
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC), otherwise known as pancreatic carcinoma or pancreatic cancer, is a highly aggressive malignancy characterized by local and vascular invasion, extensive regional lymph node metastasis, and distant metastases [1]. PDAC is the ninth most common malignancy in western countries, but represents the fourth leading cause of cancer related death [2, 3]. Approximately 80% of patients have either unresectable locally advanced or metastatic disease at the time of diagnosis and three-quarter of those who undergo curative surgical resection develop recurrent disease [4–7]. As such, pancreatic cancer is considered to be a systemic disease in the majority of patients at the time of diagnosis.
Unfortunately, PDAC typically demonstrates innate resistance to conventional chemotherapeutics, due in part to multiple molecular aberrations, dense desmoplastic reaction, poor angiogenesis and tumor microenvironment hypoxia [8–10]. Responses are often short-lived and prognosis is dismal. Primary resection with subsequent adjuvant chemotherapy yields a median survival of 20–22 months in resectable disease [6, 7, 11, 12]. With current chemotherapy regimens, the median survival for patients with unresectable/metastatic tumors is 9–11 months [13–15].
A better understanding of the molecular basis of pancreatic carcinogenesis has led to the development of strategies targeting dysregulated signaling pathways implicated in the development and progression of this devastating cancer. These targeted therapies include small-molecule inhibitors of signaling proteins such as Hedgehog, MEK, RAS, and SRC [16–21]; as well as cell-membrane proteins such as EGFR [22]. This review discusses new targeted therapies that have progressed from preclinical studies into clinical trials for the treatment of patients with advanced pancreatic cancer either as monotherapy or in combination with cytotoxic agents in an attempt to achieve better responses and improve survival.
CONVENTIONAL APPROACHES
In newly diagnosed patients with advanced unresectable/metastatic pancreatic cancer, gemcitabine- and fluoropyrimidine-based chemotherapy have been established as the preferred initial treatment options for most patients with the goal of prolonging survival and improving the quality of life. Specifically, gemcitabine plus nab-paclitaxel and FOLFIRINOX (combination of 5-fluorouracil, folinic acid, irinotecan and oxaliplatin) demonstrated high response rates and modest improvement in overall survival [14, 15]. In contrast, the combination of gemcitabine with other cytotoxic agents including oxaliplatin, irinotecan, cisplatin, fluorouracil/leucovorin, pemetrexed or capecitabine failed to show a survival benefit over gemcitabine alone in prospective phase II/III studies (Table 1) [23–29]. Similarly, gemcitabine with monoclonal antibodies (e.g bevacizumab, cetuximab, ganitumab) did not reveal improvement in survival when compared to gemcitabine alone in phase III CALGB, SWOG, and GAMMA trials (Table 2) [30–32]. Recent trials employing gemcitabine plus small molecule inhibitors such as sorafenib, tipifarnib, rigosertib, trametinib, aflibercept, sunitinib, everolimus, or axitinib failed to show better survival in comparison with gemcitabine monotherapy in randomized placebo-controlled phase II/III studies in previously untreated patients with advanced pancreatic cancer (Table 3) [33–39]. Nevertheless, Moore et al reported that gemcitabine plus erlotinib conferred significant survival advantage with improved overall survival (OS) and progression free survival (PFS) rates [40]. These findings underscore further development of targeted agents in the treatment of patients with advanced unresectable and metastatic pancreatic adenocarcinoma.
NOVEL MONOCLONAL ANTIBODIES
Tigatuzumab (CS-1008)
Tigatuzumab, also known as CS-1008, is an intravenously bioavailable, humanized murine IgG1 monoclonal antibody with a molecular weight of 144.6kDA, and composed of the complementarity determining region (CDR) of the murine monoclonal antibody TRA-8 and the variable region framework and constant regions of human immunoglobulin IgG-1mAb58′CL [41, 42]. The antibody demonstrates potent agonist property against TRAIL (tumor necrosis factor-related apoptosis-inducing ligand) receptor 2 (TR-2)/death receptor 5 (DR5). This antibody induces tumor cell apoptosis and growth inhibition by triggering both extrinsic and intrinsic apoptotic, caspase-mediated signaling pathways [43, 44]. In vitro studies showed that tigatuzumab induces selective, dose-dependent cytotoxicity in several human pancreatic carcinoma cell lines including MIA PaCa-2 [41, 45, 46]. Tigatuzumab did not induce cell death in human primary hepatocytes. In xenografted MIA PaCa-2 mouse model of human pancreatic carcinoma, tigatuzumab dosed at 0.3 and 3 mg/kg in combination with gemcitabine at 400 mg/kg substantially inhibited tumor growth with complete tumor regression noted in two of 10 mice treated with the higher tigatuzumab dose [41].
In an initial, multi-institutional, open-label, phase I dose-escalation study, tigatuzumab at dose levels of 1, 2, 4, and 8 mg/kg was administered weekly by intravenous infusion to 17 patients with relapsed or refractory carcinomas and lymphoma [47]. After at least 2 cycles of treatment, tigatuzumab was found to be safe, well-tolerated, with no dose-limiting toxicity (DLT), and the maximal tolerated dose (MTD) was not reached. The most common adverse events were nausea, vomiting, fatigue, pyrexia, anemia, and cough. No serious treatment-related toxicities observed [47]. Stable disease was achieved in approximately 41% of patients for a prolonged period of time [47]. These results prompted a phase II trial to evaluate the efficacy of tigatuzumab administered in combination with gemcitabine to chemotherapy-naive patients diagnosed with unresectable or metastatic pancreatic cancer [48]. Sixty-five patients, predominantly Caucasians with median age of 60.6 years, received tigatuzumab intravenously on days 1, 8, 15, and 21 (8 mg/kg loading dose followed by 3 mg/kg per week) and intravenous gemcitabine on days 1, 8, and 15 (1000 mg/m2) until disease progression or unacceptable toxicity. Tolerability profile was acceptable as the most common toxicities were grade 1 or 2 nausea, fatigue, abdominal pain, constipation, and fever after a median duration of treatment of approximately 18 weeks. No new treatment-emergent adverse events were seen [47, 48]. Of 61 patients evaluated for efficacy, the overall response rate (ORR) was 13.1% with a median duration of response of 309 days. The primary endpoint, PFS at 16 weeks, was 53%, and the median PFS and OS were 3.9 months and 8.2 months respectively [48]. Tigatuzumab combined with gemcitabine was well tolerated and may improve survival outcomes in patients with unresectable or metastatic pancreatic cancer. Tigatuzumab has now entered phase II clinical trials for the treatment of patients with a variety of solid neoplasms including pancreatic cancer, non-small cell lung cancer (NSCLC), hepatocellular carcinoma, and ovarian cancer [NCT00521404, NCT00991796, NCT01033240, NCT00945191].
Table 1: Phase III trials of gemcitabine containing regimens in advanced pancreatic cancer
Trial |
Regimen |
Primary endpoint |
Reference |
MPACT |
gemcitabine + nab-paclitaxel vs. gemcitabine |
mOS: 8.5 vs. 6.7 months (p < 0.001) |
[15] |
GIP-1 |
gemcitabine + cisplatin vs. gemcitabine |
mOS: 8.3 vs. 7.2 months (p = 0.38) |
[23] |
GEM-CAP |
gemcitabine + capecitabine vs. gemcitabine |
mOS: 7.1 vs. 6.2 months (p = 0.08) |
[24] |
E6201 |
gemcitabine + oxaliplatin vs. gemcitabine |
mOS: 5.7 vs. 4.9 months (p = 0.22) |
[25] |
NCT00023972 |
gemcitabine + exatecan vs. gemcitabine |
mOS: 6.7 vs. 6.2 months (p = 0.52) |
[26] |
Stathopoulos et al. |
gemcitabine + irinotecan vs. gemcitabine |
mOS: 6.4 vs. 6.5 months (p = 0.957) |
[27] |
NCT00035035 |
gemcitabine + pemetrexed vs. gemcitabine |
mOS: 6.2 vs. 6.3 months (p = 0.8477) |
[28] |
E2297 |
gemcitabine + 5-FU vs. gemcitabine |
mOS: 6.7 vs. 5.4 months (p = 0.09) |
[29] |
Abbreviations: 5-FU – 5-fluorouracil; mOS – median overall survival.
Table 2: Phase III trials of gemcitabine with biologics in advanced pancreatic cancer
Trial |
Regimen |
Primary endpoint |
Reference |
SWOG S0205 |
gemcitabine + cetuximab vs. gemcitabine |
mOS: 6.3 vs. 5.9 months (p = 0.23) |
[30] |
CALGB 80303 |
gemcitabine + bevacizumab vs. gemcitabine |
mOS: 5.8 vs. 5.9 months (p = 0.95) |
[31] |
GAMMA |
gemcitabine + ganitumab vs. gemcitabine |
mOS: 7.1 vs. 7.0 months (p = 0.397) |
[32] |
Abbreviation: mOS – median overall survival.
Table 3: Phase II/III trials of gemcitabine with small molecule inhibitors in advanced pancreatic cancer
Trial |
Regimen |
Primary endpoint |
Reference |
BAYPAN |
gemcitabine + sorafenib vs. gemcitabine |
mPFS: 3.8 vs. 5.7 months (p = 0.902) |
[33] |
NCT00471146 |
gemcitabine + axitinib vs. gemcitabine |
mOS: 8.5 vs. 8.3 months (p = 0.5436) |
[34] |
CESAR |
gemcitabine + sunitinib vs. gemcitabine |
mPFS: 11.6 vs. 13.3 weeks (p = 0.74) |
[35] |
NCT00574275 |
gemcitabine + aflibercept vs. gemcitabine |
mOS: 6.5 vs. 7.8 months (p = 0.2034) |
[36] |
NCT00005648 |
gemcitabine + tipifarnib vs. gemcitabine |
mOS: 193 vs. 182 days (p = 0.75) |
[37] |
NCT00409292 |
gemcitabine + everolimus |
mOS: 4.5 months |
[38] |
NCT01231581 |
gemcitabine + trametinib vs. gemcitabine |
mOS: 8.4 vs. 6.7 months (p = 0.453) |
[39] |
NCIC CTG PA.3 |
gemcitabine + erlotinib vs. gemcitabine |
mOS: 6.24 vs. 5.91 months (p = 0.038) |
[40] |
Abbreviations: mOS – median overall survival; mPFS – median progression-free survival.
Dalotuzumab (MK-0646)
The insulin growth factor-1 receptor (IGF-1R) is a homodimeric transmembrane tyrosine kinase receptor. It.is over-expressed on the surface of several human malignancies including pancreatic tumor cells [49–52]. When activated by its ligands (IGF-I and -II), the receptor sends signals that exert antiapoptotic effects and confers increased tumor growth, resistance to chemotherapeutics, and motility of cancer cells via multiple signaling cascades (Figure 1) [53, 54]. Dalotuzumab is a novel, recombinant humanized IgG1 monoclonal antagonist antibody that binds to IGF-1R with high affinity (Kd = 1 nmol/L). This induces receptor internalization and degradation, and inhibits IGF-I- and IGF-II-mediated pancreatic cancer growth and metastasis [55–57]. In preclinical studies, dalotuzumab (also known as MK-0646 or h7C10) enhances gemcitabine-induced apoptosis and inhibits signaling pathways that confer increased cellular proliferation, survival and drug resistance in pancreatic cancer [56, 58]. The first-in-human study of dalotuzumab showed the agent was generally well-tolerated, exhibited positive pharmacodynamic effects, and favorable clinical activity in patients with advanced solid cancers [59]. The most common adverse event was hyperglycemia. Subsequently, a phase I/II study evaluated dalotuzumab in combination regimens. Jayle and colleagues showed that dalotuzumab (5–10 mg/kg weekly) plus gemcitabine (1000 mg/m2 weekly) or gemcitabine (100 mg/m2 weekly) and erlotinib (100 mg daily) showed favorable toxicity profile in previously untreated patients with metastatic pancreatic cancer [60]. Serious adverse events included hyperglycemia, hepatic toxicity, and cytopenia. Early efficacy data showed higher partial response (PR) in the dalotuzumab plus gemcitabine and erlotinib arm (25% versus 20%). Additional clinical data clarifying the OS benefit of this targeted agent are expected from ongoing clinical trials.
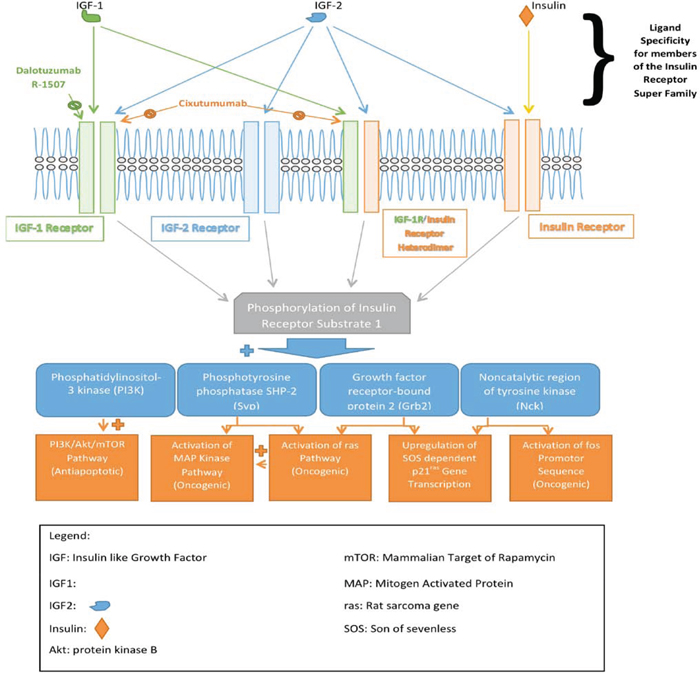
Figure 1: Signaling pathways for insulin and insulin-like growth factors. Three growth factors, insulin, insulin-like 1, and 2 signal through four major receptors—homodimeric insulin-like growth factor 1 receptor (IGF-1R), homodimeric insulin-like growth factor 2 receptor (IGF-2R), heterodimeric insulin receptor (IR)/IGF-1R, and homodimeric IR. There pathways contribute to diverse cellular functions, including proliferation, survival, apoptosis, and cell metabolism. The corresponding ligands activating these receptors are highlighted. The diverse downstream signaling proteins are indicated. Dalotuzumab, R-1507, and cixutumumab are the agents in development targeting IGF receptors.
Conatumumab (AMG-655)
Conatumumab (AMG-655) is a fully human IgG1 monoclonal antibody with antineoplastic activity mediated by agonist effect against the extracellular domain of human TR-2)/DR5 [61]. Conatumumab binds to and activates TR-2/DR5, leading to activation of downstream caspase cascades and tumor cell apoptosis. TR-2 is highly expressed by pancreatic tumor cells than normal pancreatic tissue. The TR-2 high expression makes it an attractive, druggable target for cancer therapeutics [62]. Treatment with conatumumab alone or in combination with gemcitabine demonstrated potent antitumor activity against pancreatic tumor xenograft [61]. The safety and preliminary clinical activity of conatumumab in combination with gemcitabine have been evaluated in a phase IB multicenter trial of 13 previously-untreated patients with advanced pancreatic cancer [63]. Participants received conatumumab 3 or 10 mg/kg IV day 1 and 15, and gemcitabine 1000 mg/m2 IV on day 1, 8, and 15 of every 28-day cycle. After a median treatment of 6 cycles, the combination appeared tolerable and no DLTs were observed. Thrombocytopenia, abdominal pain, and neutropenia were the most common serious adverse events. Preliminary efficacy data showed a PR of 31%, median PFS of 5.3 months, and a 6-month OS rate of 76% [63]. Given these data, conatumumab combined with gemcitabine was advanced to a placebo-controlled, randomized phase II clinical testing [64]. No new safety signal emerged after median treatment of 4 cycles. The disease control rate was 65% in the combination arm versus 40% for the placebo arm, with an improved 6-month OS rate of 59% versus and 50% respectively [64]. Additional investigation into this combination in patients with advanced/metastatic pancreatic cancer is warranted.
Cixutumumab (IMC-A12)
Cixutumumab, also known as IMC-A12, is a potent, highly selective, fully human IgG1 monoclonal blocking antibody with dual, subnanomolar inhibitory activity (IC50 = 0.6–1 nM) against IGF-1R homodimers as well as heterodimeric insulin receptor/IGF-1R in tumor cells (Figure 1) [65, 66]. Cixutumumab lacks antibody-dependent cellular cytotoxicity (ADCC). Rather, it selectively binds to IGF-1R or IR/IGF-1R with high affinity (Kd = 0.04 nM), triggers internalization and degradation of the receptor, and indirectly blocks both IGF-I and -II mediated ERK-MAPK (proliferative) as well as the PI3K-AKT-mTOR (survival) signaling pathway activation [66]. Cixutumumab exhibited broad anti-mitogenic activity on multiple tumor cell lines including breast cancer line (T47D), pancreatic cancer line (BxPC-3), and multiple myeloma cell line (RPMI-8226) [66]. In BxPC-3 pancreatic cancer xenograft models, cixutumumab induced tumor shrinkage by eighty percent at a dose of 1mg every three days [66].
Infusion reactions, anemia, rash, pruritus, dizziness, and fatigue were the common side-effects observed in the first phase I dose escalation study of 16 patients with relapsed/refractory solid neoplasms including breast, bladder, pancreatic, endometrial, hepatocellular carcinoma, and phaechromocytoma [67]. The DLT was hyperglycemia. Though no objective response was observed, nine patients experienced stable disease lasting for more than 6 weeks [67]. This preliminary evidence of activity of cixutumumab has prompted multiple early phase trials in advanced solid tumors. In a recent report of a phase IB/II SWOG S0727study, administration of cixutumumab 6 mg/kg/week intravenously in combination with erlotinib 100 mg/day orally, and gemcitabine 1000 mg/m2 intravenously on days 1, 8, and 15 of a 28-day cycle demonstrated tolerable toxicity profile in chemotherapy-naïve patients with advanced/metastatic pancreatic cancer [68]. The most common serious adverse effects were transaminitis, hyperglycemia, fatigue, and cytopenia. When compared with the control arm (erlotinib plus gemcitabine), the addition of cixutumumab to erlotinib and gemcitabine did not lead to longer PFS or OS. The median PFS and OS were 3.6 and 7.0 months respectively on the cixutumumab arm, and 3.6 and 6.7 months respectively on the control arm [68].
At this time, it is unclear how much, if any, benefit this specific agent would add to that achieved with conventional approaches. Evaluation of cixutumumab with other active agents in pancreatic cancer is warranted in future trials to determine whether or not this antibody will produce clinically, meaningful benefit in patients with PDAC.
R-1507
Like dalotuzumab, R-1507 is a humanized IgG1 monoclonal antibody with potent, highly selective, antagonist activity against the extracellular domain of IGF-1R characterized by intracellular internalization and degradation of the receptor [69]. The antibody demonstrates antitumor activity against pancreatic cell lines and delays tumor growth in xenograft models [70]. Preclinical studies by Kawanami and colleagues showed that R-1507 interacted synergistically with gemcitabine and/or metformin to inhibit proliferation and growth in human pancreatic ductal adenocarcinoma cell lines SUIT-2 and MIAPaCa-2 [71]. Treatment with R-1507 and everolimus, an mTOR inhibitor, demonstrated substantial anti-proliferative activity against pancreatic cell line BxPC-3 [72]. The agent was well-tolerated up to a dose of 9 mg/kg weekly in a phase I trial [73]. No DLTs were observed and the most common drug-related adverse effects were fatigue and nausea. Further investigations are warranted to establish whether IGF-1R inhibition with R-1507 alone or in combination with cytotoxic chemotherapy will improve outcomes in patients with advanced pancreatic cancer.
AGS-1C4D4
AGS-1C4D4 is a fully human IgG1 monoclonal antibody directed against the human prostate stem cell antigen (PSCA) with potential anti-neoplastic activity. The mechanism of action is designed to selectively bind to the extracellular domain of PSCA and triggers complement-dependent cell lysis (CDC) and ADCC in tumor cells expressing PSCA [74]. PSCA is a glycosylphosphatidylinositol (GPI)-linked cell surface protein. It is overexpressed on the cell surfaces of a variety of cancer cell types, including pancreatic cancer, and may play a key role in cell proliferation, invasion, and survival [75, 76]. Targeting PSCA has been shown as a promising anti-tumor strategy in pancreatic cancers in preclinical models [77, 78].
In phase I studies, the compound demonstrated acceptable toxicity profile with no DLTs at 48 mg/kg loading dose followed by 24 mg/kg every 3 weeks intravenously [74, 79], and this dose was carried to a randomized phase II trial in patients with advanced/metastatic pancreatic cancer [80]. In this multicenter study, previously untreated, metastatic pancreatic adenocarcinoma patients were randomly assigned 1:2 to gemcitabine (1000 mg/m2) or gemcitabine plus AGS-1C4D4 antibody [80]. The trial met its primary endpoint. The 6-month survival rate was significantly improved in the combination therapy arm compared to gemcitabine alone arm (60.9% versus 44.4%; p = 0.03), while the median OS were 7.6 months and 5.5 months in the two arms, respectively [80]. Another phase II trial is investigating the activity and safety of this regimen in the second-line therapy for chemotherapy-refractory patients with advanced/metastatic pancreatic cancer [NCT01608711].
Tarextumab (OMP-59R5)
Tarextumab (formerly OMP-59R5) is a novel, highly selective, fully human IgG2 monoclonal blocking antibody that binds to and prevents signaling through both the Notch2 and Notch3 receptors [81]. Notch signaling plays a critical role in pancreatic cancer transformation, tumor progression, and chemotherapy resistance. In preclinical models, tarextumab exhibited substantial tumor regressions in Notch3-expressing human pancreatic cancer xenografts when combined with nab-paclitaxel and gemcitabine via inhibition of cancer stem cell growth, promotion of cell differentiation, as well as disruption of tumor angiogenesis [81]. Although the anti-NOTCH agent (RO4929097) failed to improve survival [82], final data from a phase IB trial demonstrated encouraging clinical activity of tarextumab in combination with nab-paclitaxel and gemcitabine in treatment naïve pancreatic cancer patients [81, 83]. The combination was well-tolerated and no DLTs occurred. Frequently reported adverse effects were cytopenia, fatigue, GI toxicities, peripheral neuropathy, and alopecia. A phase II ALPINE study of this combination is underway [NCT01647828].
RADIOIMMUNOCONJUGATE
90Yttrium-clivatuzumab tetraxetan (90Y-hPAM4)
Yttrium (90Y) clivatuzumab tetraxetan (also known as hPAM4-Cide) is a radioimmunoconjugate composed of fully humanized monoclonal antibody HuPAM4, directed against the pancreatic cancer antigen mucin-1(MUC-1), that is conjugated to the chelating agent tetra-azacyclododecanetetra-acetic acid (DOTA), and radiolabeled with the beta-emitting radioisotope Yttrium90 [84]. MUC-1is a cell membrane surface glycoprotein with extensive O-linked glycosylation of its extracellular domain [85]. It is overexpressed in more than 85% of pancreatic adenocarcinomas and absent in normal pancreas, making it an attractive target for anti-cancer therapeutics [86–88]. Aberrant activation of the MUC-1-dependent pathways has been implicated in initiation and maintenance of malignant phenotype. Increased expression enhances beta-catenin mediated cancer invasion, and promotes both p53- and PI3K-AKT-dependent cell survival [89–91]. Clivatuzumab tetraxetan demonstrates ADCC. The compound selectively binds to tumor cells expressing MUC-1, undergoes internalization, and delivers high cytotoxic dose of beta radiation to the tumor cells [92, 93]. In athymic nude mice bearing CaPan1 human pancreatic cancer xenografts, clivatuzumab alone or in combination with gemcitabine exhibited substantial antitumor response [94–97].
A phase I dose-escalation trial of clivatuzumab teraxetan enrolled 21 patients with advanced pancreatic cancer. These patients were treated with single dose of 15, 20, or 25 mCi/m2. The radioimmunoconjugate was well-tolerated. DLTs included neutropenia and thrombocytopenia, which occurred at 25 mCi/m2. Therefore, 20 mCi/m2 was established as the MTD and chosen for further studies [98]. Notably, 2 patients developed human anti-human antibody (HAHA). Of twenty patients evaluated for response at week 4 after treatment, there were three PR and four with stable disease (SD) [98]. When clivatuzumab was administered at weekly fractionated doses together with low dose gemcitabine, no new treatment-related toxicities were noted [84]. The disease control rate was higher at 58% (6 PR, 16 SD) presumably due to the radiosensitizing effect of gemcitabine.
These encouraging results led to initiation of phase II/III clinical trials of clivatuzumab in advanced pancreatic cancer. Final results of a multicenter phase IB study of 58 heavily-pretreated patients with pancreatic cancer were recently reported at the 2014 ASCO Annual Meeting [99]. In arm A, twenty-nine patients received the combination of fractionated doses of clivatuzumab tetraxetan once-a-week for 3 weeks with gemcitabine given weekly for 4 weeks while 29 patients in arm B were treated with 4 doses of clivatuzumab tetraxetan alone. The treatment cycle was repeated every 4 weeks until unacceptable toxicity or disease progression or patient withdrawal. The median OS of patients who received combination therapy (7.9 months) was significantly longer than that of patients who received antibody alone (3.4 months) [P = 0.004] [99]. Given these favorable results, a phase III PANCRIT-1 registration trial has been initiated to confirm these findings.
SMALL MOLECULE INHIBITORS
Vismodegib (GDC-0449)
Vismodegib (GDC-0449, HhAntag-691) is an orally administered, specific, irreversible, and highly potent hedgehog pathway (Hh) inhibitor approved by the FDA in January 2012 for treatment of patients with unresectable locally advanced/metastatic basal cell carcinoma of the skin [100, 101]. The Hh pathway is activated by binding of Hh ligands (Sonic, Desert, Indian) to the transmembrane G-protein-coupled receptor (Patched), which in turn releases the suppression of signal transducing protein (Smoothened) that triggers a cascade of events resulting in expression of Hh-responsive genes [102]. Uncontrolled activation of the Hedgehog (Hh) signaling pathway has emerged as a central player in neoplastic transformation, tumor growth and cancer survival in a growing number of hematologic and solid malignancies including the skin, breast, lung, liver, and pancreatic carcinomas along with colon and brain tumors [103–108]. The components of Sonic Hh signaling pathway, including the ligand (SHh), the signaling molecules (Patched-1, Patched-2 and Smoothened) and effectors (Gli1, and Gli2) are aberrantly expressed in human pancreatic cancer cell lines and pancreatic cancer stem cells [109–111]. Vismodegib induces cell apoptosis and inhibits survival in dose-dependent manner in pancreatic cell lines by selectively binding to and downregulating the expression of Smoothened, Patched-1, and Patched-2 [112, 113]. Similarly, vismodegib inhibited the expression of transcription factor Gli1 and Gli2 [112].
Vismodegib has been assessed in a multi-center, placebo-controlled, phase IB/randomized phase II study of previously untreated patients with metastatic pancreatic cancer [114]. One hundred and six patients were randomized in 1:1 to gemcitabine (1000 mg/m2 over 30 minutes on days 1, 8, 15), every 28 days plus either placebo (GP) or vismodegib (150 mg PO daily) (GV). Toxicity between the 2 groups was similar. The most serious adverse events were cytopenia, hyponatremia, fatigue, and hyperglycemia [114]. Adding vismodegib to gemcitabine chemotherapy as frontline therapy yielded disappointing results. No improvement in median PFS (4.0/2.5 months) and median OS (6.9/6.1 months) when compared with gemcitabine alone, although 22 patients on the GP crossed over to the GV at progression, which could have complicated the outcome [114]. Interim results from an ongoing open label phase II trial of untreated pancreatic cancer patients showed that vismodegib (150mg PO daily) combined with gemcitabine (1000 mg/m2) plus nab-paclitaxel (125 mg/m2) on days 1, 8 and 15 of every 28 days cycle demonstrated acceptable toxicity profile [115]. Of forty-nine patients evaluated for response, the ORR was 43%. Data analysis showed a median PFS of 5.5 months and OS of 10 months [115].
Masitinib (AB1010)
Masitinib (AB1010) is a potent, ATP competitive, multi-tyrosine kinase inhibitor with nanomolar activity (≤ 500 nM) [116] and potential antineoplastic activity. A benzamide derivative, masitinib selectively binds to and inhibits both the wild-type and mutated forms of the stem cell factor receptor (c-Kit; SCFR); platelet-derived growth factor receptor (PDGFR); and fibroblast growth factor receptor 3 (FGFR3) [116]. The compound enhances the antiproliferative effects of gemcitabine in gemcitabine-refractory human pancreatic cell lines Mia Paca2 and Panc1 by downregulating Wnt/beta-catenin signaling pathway [117]. Substantial clinical progress has been seen with masitinib. In a phase I dose-escalation study conducted in patients with advanced and/or metastatic pancreatic cancer, the MTD was not reached but a dose of 12 mg/kg/day was found to be safe for the treatment of patients with solid cancers [118]. In a phase II trial in combination with gemcitabine, masitinib demonstrated substantial clinical activity in treatment naïve patients with advanced pancreatic cancer [119], resulting in its advancement to phase III registration study. This trial met its primary endpoint of median time-to-progression (TTP) (6.4 months) which was well beyond the threshold (2.1 months) set by the investigators [119]. The results of the first prospective, international, randomized, double-blinded clinical trial of masitinib plus gemcitabine as first line treatment in patients with advanced pancreatic cancer were presented at the 2013 American Society of Clinical Oncology (ASCO) meeting. Three hundred and fourty eight patients were randomized to receive either masitinib (9 mg/kg/day) in combination with gemcitabine (1000 mg/m2/weekly) or placebo plus gemcitabine with overall survival (OS) being the primary end point [120]. A gene expression profiling assay of whole blood samples was also conducted before initiation of treatment to identify genetic expression patterns predictive of overall survival and/or treatment benefit. Overall, no difference in OS was demonstrated (HR = 0.90; 95% CI, 0.71–1.14; p = 0.74). However, masitinib in combination with gemcitabine significantly extended median OS in two independent patient populations [120]. Firstly, median OS was significantly prolonged in patients with pain at baseline (defined as a VAS score > 20 mm on a 100 mm scale) from 5.4 months in the placebo arm to 8.1 months in the masitinib arm (p = 0.010). In another separate cohort analysis of patients with a specific deleterious genomic biomarker (GBM) indicative of aggressive disease, the median OS was superior with combination of masitinib plus gemcitabine compared with gemcitabine plus placebo (11.0 versus 5.0 months, respectively; p = 0.000038) [120].
Selumetinib (AZD-6244, ARRY-142886)
Selumetinib (also known as AZD-6244 or ARRY-142886) is an orally bioavailable, non-ATP competitive, highly selective MEK 1/2 inhibitor with potential anti-neoplastic activity at nanomolar concentration (IC50 of 14 nm) [17, 121]. In murine BxPC3 pancreatic tumor xenograft models, selumetinib significantly inhibited tumor growth [121], and its antitumor activity correlated with substantial decrease in phosphorylated ERK1/2 levels. A phase I dose escalation study of 57 patients with advanced cancers including pancreatic carcinoma identified 100mg BID as safe and well-tolerated [122]. Rash, diarrhea and hypoxia were reported as the major DLTs. Results of a recently published phase II trial showed no difference in overall survival between selumetinib and capecitabine as second-line treatment in 70 patients with advanced pancreatic cancer who had been pretreated with a gemcitabine-based regimen [20]. The median OS was 5.4 months in the selumetinib group versus 5.0 months in the capecitabine group (p = 0.92) [20]. Dual targeting of MEK/EGFR signaling with selumetinib and erlotinib in 46 previously-treated patients with advanced/metastatic pancreatic cancer demonstrated a disease control rate of 51%. The estimated median PFS and OS were 2.6 and 7.5 months respectively [123]. Additional clinical trials are currently underway to further explore this targeted agent in combination strategies [NCT01658943, NCT01061749].
Saracatinib (AZD-0530)
A quinazolinamine derivative, saracatinib (formerly AZD-0530) is an orally bioavailable, dual-specific inhibitor of Src and Abl tyrosine kinases with antitumor activity at nanomolar concentrations (IC50 = 4–10 nM) [124]. In preclinical models of pancreatic cancer, saracatinib showed great antitumor activity in orthotopic ASPC-1xenograft mice through inhibition of Src phosphorylation and induction of cell cycle arrest at G1/S [124].
In first-line setting, phase I/II trial by Renouf et al. [125] evaluated the combination of saracatinib (175 mg PO daily) and gemcitabine (1000 mg/m2) in patients with advanced pancreatic cancer and showed the combination was safe and generally well-tolerated. The phase II part of the trial did not meet its primary endpoint of objective tumor response (ORR) plus stable disease ≥ 4 months, and was closed to further accrual [125].
Pimasertib (AS-703026, MSC-1936369B)
Pimasertib, also known as AS703026, MSC1936369B, is a highly potent, ATP noncompetitive, second generation small molecule inhibitor of MEK1 and MEK2 [126]. It exhibited potent antitumor activity by selectively binding to the allosteric site on MEK1/2; induced G0-G1 cell cycle arrest via downregulation of pERK1/2; and triggered apoptosis by caspase-3 and PARP cleavage [127]. Interim safety data from an ongoing open label phase II trial showed that pimasertib was safe and well-tolerated when combined with gemcitabine in chemotherapy naïve patients with advanced pancreatic cancer [128]. The DLTs were grade 3 confusion with ataxia and disorientation, and grade 4 suicidal ideation. Asthenia, ocular disturbance, skin rash, GI toxicities, and cytopenias were the most common adverse events [128]. Further clinical data are awaited.
Refametinib (RDEA119, BAY 869766)
Refametinib is another MEK inhibitor that has progressed to early phase clinical testing in patients with advanced/metastatic pancreatic cancer. A cyclopropane-1-sulfonamide derivative, refametinib inhibits cell proliferation in several tumor cell lines including BxPC3 human pancreatic cell line [129]. The compound alone or in combination with rapamycin, an mTOR inhibitor, showed significant growth inhibition in murine xenograft models of human pancreatic cancer cells OCIP19, 21, and 23 mediated by cell cycle arrest predominantly in G1 phase [130]. The combination of refametinib and gemcitabine as first-line treatment of sixty patients with advanced pancreatic cancer showed encouraging results in a single-arm, open label, phase IIA clinical trial with stable disease and partial response shown in 38% and 35%, respectively [131]. The compound demonstrated acceptable safety profile with most common toxicities being cytopenia, transaminitis, hypertension, rash and fatigue [131].
Galunisertib (LY-2157299)
Galunisertib, also known as LY-2157299, is a novel selective small molecule inhibitor of transforming growth factor beta receptor 1(TGF-βR1) with potential antitumor activity mediated by reducing levels of active, phosphorylated SMAD [132]. A phase IB trial of this agent in combination with gemcitabine in advanced solid malignancies including pancreatic cancer demonstrated acceptable toxicity [133]. The PK profile of galunisertib was unchanged, and no DLTs were observed [133]. Galunisertib at 300 mg/day has been advanced into a randomized Phase II trial in pancreatic cancer in first-line setting to assess the antitumor activity of this combination [NCT02154646, NCT01373164].
Talazoparib (BMN-673)
Talazoparib, also known as BMN-673, is a novel, orally bioavailable inhibitor of the nuclear enzyme poly (ADP-ribose) polymerase (PARP) with potent anti-neoplastic activity at subnanomolar concentration (IC50 = 0.58 nM) [134]. It selectively binds to PARP and prevents PARP-mediated DNA repair of single strand DNA breaks via the base-excision repair pathway. As a consequence, there is accumulation of DNA strand breaks, increased genomic instability, leading to apoptosis in target cells [134]. The agent has demonstrated efficacy with acceptable toxicity in patients with BRCA-mutant solid tumors including pancreatic cancer [135]. The recommended phase II dose is 1000 μg/day, and the main DLT is thrombocytopenia [135]. Additional phase I/II trials are ongoing [NCT02286687, NCT01989546, NCT01286987].
Veliparib (ABT-888)
Veliparib (formerly ABT-888) is an orally bioavailable, carboxamide derivative with potent inhibitory property against PARP 1 and PARP 2 at concentrations (IC50) of 5.2 nM and 2.9 nM respectively [136]. Like talazoparib, ABT-888 selectively binds to PARP, inhibits DNA repair, and potentiates cytotoxicity of DNA-damaging agents such as alkylating compounds (e.g. temozolomide, platinums, cyclophosphamide) and ionizing radiation in syngeneic and xenograft tumor models [136, 137]. When combined with cisplatin and gemcitabine in a phase IB trial of untreated pancreatic cancer patients, veliparib demonstrated a tolerable toxicity profile with high clinical activity in BRCA-mutant tumors [138]. Serious adverse effects were anemia, neutropenia, thrombocytopenia, and fatigue. The recommended phase II dose was 80 mg PO BID on day 1–12 every 3 weeks with fixed doses of cisplatin (25 mg/m2 IV) and gemcitabine (600mg/m2 IV) on day three and ten [138]. Given these encouraging results, a two-part phase II trial of this compound has been initiated in this setting [NCT01585805]. In the first part, patients with untreated pancreatic cancer and BRCA and/or PALB2 mutations will be randomly assigned to receive gemcitabine and cisplatin with or without veliparib. In the other part, patients with relapses/refractory pancreatic cancer will receive veliparib alone. Patients from the first part whose cancer did not respond to gemcitabine and cisplatin treatment alone are eligible to participate in the second part of the trial.
Salirasib (FTS)
The RAS signaling pathway plays a key role in signal transduction, cell motility, proliferation, survival and malignant transformation [17]. Up to 90% of human pancreatic cancers are driven by aberrant oncogenic RAS signaling and associated with increased tumor invasion and metastasis. Unfortunately, previous attempts to directly block RAS activity by inhibition of farnesyltransferase have been ineffective, as multiple escape pathways exist that allow for alternative prenylation of RAS protein [37, 139]. Salirasib is a novel, highly potent, synthetic small molecule with distinctive inhibitory property against RAS at micromolar concentration (IC50 = 2.6 μM) in kinase assays [140]. As a farnesylcysteine mimetic, salirasib selectively binds to and dislodges RAS from its membrane anchorage domains, and eventually accelerates its degradation and abrogates multiple RAS-dependent signaling pathways accompanied by substantial tumor growth inhibition in human pancreatic cancer xenografts [140].
The development of salirasib in advanced pancreatic cancer is still in the early clinical stage [141, 142]. A recently reported phase I study involving treatment-naïve patients with advanced, metastatic pancreatic cancer demonstrated good tolerability and encouraging clinical activity [141]. In combination with standard dose and schedule of gemcitabine, salirasib at 200–800 mg orally twice daily for 21 days every 28 days showed no overlapping pharmacokinetics. The most common adverse events were hematologic and GI toxicities, and fatigue [141]. The combination regimen achieved a median OS of 6.2 months and the 1-year survival of 37% in nineteen patients enrolled in the study [141]. The recommended dose for phase II trials was 600 mg twice daily.
CONCLUSION
The survival of pancreatic cancer patients with either unresectable locally advanced or metastatic disease rarely surpasses 11 months with standard chemotherapy regimens. Recent efforts have identified multiple dysregulated signaling pathways in pancreatic cancer development and progression, many of which appear to be reasonable targets including PI3K/mTOR, SIRT1, and ALK [143–146]. The data from clinical trials on clivatuzumab, masitinib, veliparib, and salirasib are particularly encouraging. Further research into combinations of multiple targeted agents as well as mixture of these inhibitors in combination with cytotoxic agents to achieve optimal vertical or horizontal blockade will most likely improve the bleak outlook in patients with advanced/metastatic pancreatic cancer [147].
ACKNOWLEDGMENTS AND FUNDING
This study was partly supported by Henan Cancer Hospital of Zhengzhou University, Zhengzhou China.
CONFLICTS OF INTEREST
The authors have no relevant conflicts of interest.
Author contributions
DL, AA and CI designed the study and drafted the manuscript. All authors have contributed to data preparation, drafting and revising the manuscripts. All authors have read and approved the final manuscript.
REFERENCES
1. Apte MV, Park S, Phillips PA, Santucci N, Goldstein D, Kumar RK, Ramm GA, Buchler M, Friess H, McCarroll JA, Keogh G, Merrett N, Pirola R, Wilson JS. Desmoplastic reaction in pancreatic cancer: role of pancreatic stellate cells. Pancreas. 2004; 29:179–187.
2. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014; 64:9–29.
3. Jemal A. Global burden of cancer: opportunities for prevention. Lancet. 2012; 380:1797–1799.
4. Worni M, Guller U, White RR, Castleberry AW, Pietrobon R, Cerny T, Gloor B, Koeberle D. Modest improvement in overall survival for patients with metastatic pancreatic cancer: a trend analysis using the surveillance, epidemiology, and end results registry from 1988 to 2008. Pancreas. 2013; 42:1157–1163.
5. Hartwig W, Hackert T, Hinz U, Gluth A, Bergmann F, Strobel O, Buchler MW, Werner J. Pancreatic cancer surgery in the new millennium: better prediction of outcome. Ann Surg. 2011; 254:311–319.
6. Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, Beger H, Fernandez-Cruz L, Dervenis C, Lacaine F, Falconi M, Pederzoli P, Pap A, Spooner D, Kerr DJ, Buchler MW. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004; 350:1200–1210.
7. Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, Schramm H, Fahlke J, Zuelke C, Burkart C, Gutberlet K, Kettner E, Schmalenberg H, Weigang-Koehler K, Bechstein WO, Niedergethmann M, Schmidt-Wolf I, Roll L, Doerken B, Riess H. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007; 297:267–277.
8. Omary MB, Lugea A, Lowe AW, Pandol SJ. The pancreatic stellate cell: a star on the rise in pancreatic diseases. J Clin Invest. 2007; 117:50–59.
9. Pandol S, Edderkaoui M, Gukovsky I, Lugea A, Gukovskaya A. Desmoplasia of pancreatic ductal adenocarcinoma. Clin Gastroenterol Hepatol. 2009; 7:S44–47.
10. Sharma S, Green KB. The pancreatic duct and its arteriovenous relationship: an underutilized aid in the diagnosis and distinction of pancreatic adenocarcinoma from pancreatic intraepithelial neoplasia. A study of 126 pancreatectomy specimens. Am J Surg Pathol. 2004; 28:613–620.
11. Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, Padbury R, Moore MJ, Gallinger S, Mariette C, Wente MN, Izbicki JR, Friess H, Lerch MM, Dervenis C, Olah A, Butturini G, Doi R, Lind PA, Smith D, Valle JW, Palmer DH, Buckels JA, Thompson J, McKay CJ, Rawcliffe CL, Buchler MW. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA. 2010; 304:1073–1081.
12. Ueno H, Kosuge T, Matsuyama Y, Yamamoto J, Nakao A, Egawa S, Doi R, Monden M, Hatori T, Tanaka M, Shimada M, Kanemitsu K. A randomised phase III trial comparing gemcitabine with surgery-only in patients with resected pancreatic cancer: Japanese Study Group of Adjuvant Therapy for Pancreatic Cancer. Br J Cancer. 2009; 101:908–915.
13. Hidalgo M. Pancreatic cancer. N Engl J Med. 2010; 362:1605–1617.
14. Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de la Fouchardiere C, Bennouna J, Bachet JB, Khemissa-Akouz F, Pere-Verge D, Delbaldo C, Assenat E, Chauffert B, Michel P, Montoto-Grillot C, Ducreux M. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011; 364:1817–1825.
15. Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, Harris M, Reni M, Dowden S, Laheru D, Bahary N, Ramanathan RK, Tabernero J, Hidalgo M, Goldstein D, Van Cutsem E, Wei X, Iglesias J, Renschler MF. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013; 369:1691–1703.
16. Tibes R, Mesa R. Targeting hedgehog signaling in myelofibrosis and other hematologic malignancies. Journal of Hematology & Oncology. 2014; 7:18.
17. Akinleye A, Furqan M, Mukhi N, Ravella P, Liu D. MEK and the inhibitors: from bench to bedside. J Hematol Oncol. 2013; 6:27.
18. Chung EJ, Brown AP, Asano H, Mandler M, Burgan WE, Carter D, Camphausen K, Citrin D. In vitro and in vivo radiosensitization with AZD6244 (ARRY-142886), an inhibitor of mitogen-activated protein kinase/extracellular signal-regulated kinase 1/2 kinase. Clin Cancer Res. 2009; 15:3050–3057.
19. Rajeshkumar NV, Tan AC, De Oliveira E, Womack C, Wombwell H, Morgan S, Warren MV, Walker J, Green TP, Jimeno A, Messersmith WA, Hidalgo M. Antitumor effects and biomarkers of activity of AZD0530, a Src inhibitor, in pancreatic cancer. Clin Cancer Res. 2009; 15:4138–4146.
20. Bodoky G, Timcheva C, Spigel DR, La Stella PJ, Ciuleanu TE, Pover G, Tebbutt NC. A phase II open-label randomized study to assess the efficacy and safety of selumetinib (AZD6244 [ARRY-142886]) versus capecitabine in patients with advanced or metastatic pancreatic cancer who have failed first-line gemcitabine therapy. Invest New Drugs. 2012; 30:1216–1223.
21. Collins MA, Pasca di Magliano M. Kras as a key oncogene and therapeutic target in pancreatic cancer. Front Physiol. 2013; 4:407.
22. Wang T, Yang J, Xu J, Li J, Cao Z, Zhou L, You L, Shu H, Lu Z, Li H, Li M, Zhang T, Zhao Y. CHIP is a novel tumor suppressor in pancreatic cancer through targeting EGFR. Oncotarget. 2014; 5:1969–1986.
23. Colucci G, Labianca R, Di Costanzo F, Gebbia V, Carteni G, Massidda B, Dapretto E, Manzione L, Piazza E, Sannicolo M, Ciaparrone M, Cavanna L, Giuliani F, Maiello E, Testa A, Pederzoli P, Falconi M, Gallo C, Di Maio M, Perrone F. Randomized phase III trial of gemcitabine plus cisplatin compared with single-agent gemcitabine as first-line treatment of patients with advanced pancreatic cancer: the GIP-1 study. J Clin Oncol. 2010; 28:1645–1651.
24. Cunningham D, Chau I, Stocken DD, Valle JW, Smith D, Steward W, Harper PG, Dunn J, Tudur-Smith C, West J, Falk S, Crellin A, Adab F, Thompson J, Leonard P, Ostrowski J, Eatock M, Scheithauer W, Herrmann R, Neoptolemos JP. Phase III randomized comparison of gemcitabine versus gemcitabine plus capecitabine in patients with advanced pancreatic cancer. J Clin Oncol. 2009; 27:5513–5518.
25. Poplin E, Feng Y, Berlin J, Rothenberg ML, Hochster H, Mitchell E, Alberts S, O’Dwyer P, Haller D, Catalano P, Cella D, Benson AB 3rd. Phase III, randomized study of gemcitabine and oxaliplatin versus gemcitabine (fixed-dose rate infusion) compared with gemcitabine (30-minute infusion) in patients with pancreatic carcinoma E6201: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol. 2009; 27:3778–3785.
26. Abou-Alfa GK, Letourneau R, Harker G, Modiano M, Hurwitz H, Tchekmedyian NS, Feit K, Ackerman J, De Jager RL, Eckhardt SG, O’Reilly EM. Randomized phase III study of exatecan and gemcitabine compared with gemcitabine alone in untreated advanced pancreatic cancer. J Clin Oncol. 2006; 24:4441–4447.
27. Stathopoulos GP, Syrigos K, Aravantinos G, Polyzos A, Papakotoulas P, Fountzilas G, Potamianou A, Ziras N, Boukovinas J, Varthalitis J, Androulakis N, Kotsakis A, Samonis G, Georgoulias V. A multicenter phase III trial comparing irinotecan-gemcitabine (IG) with gemcitabine (G) monotherapy as first-line treatment in patients with locally advanced or metastatic pancreatic cancer. Br J Cancer. 2006; 95:587–592.
28. Oettle H, Richards D, Ramanathan RK, van Laethem JL, Peeters M, Fuchs M, Zimmermann A, John W, Von Hoff D, Arning M, Kindler HL. A phase III trial of pemetrexed plus gemcitabine versus gemcitabine in patients with unresectable or metastatic pancreatic cancer. Ann Oncol. 2005; 16:1639–1645.
29. Berlin JD, Catalano P, Thomas JP, Kugler JW, Haller DG, Benson AB 3rd. Phase III study of gemcitabine in combination with fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma: Eastern Cooperative Oncology Group Trial E2297. J Clin Oncol. 2002; 20:3270–3275.
30. Philip PA, Benedetti J, Corless CL, Wong R, O’Reilly EM, Flynn PJ, Rowland KM, Atkins JN, Mirtsching BC, Rivkin SE, Khorana AA, Goldman B, Fenoglio-Preiser CM, Abbruzzese JL, Blanke CD. Phase III study comparing gemcitabine plus cetuximab versus gemcitabine in patients with advanced pancreatic adenocarcinoma: Southwest Oncology Group-directed intergroup trial S0205. J Clin Oncol. 2010; 28:3605–3610.
31. Kindler HL, Niedzwiecki D, Hollis D, Sutherland S, Schrag D, Hurwitz H, Innocenti F, Mulcahy MF, O’Reilly E, Wozniak TF, Picus J, Bhargava P, Mayer RJ, Schilsky RL, Goldberg RM. Gemcitabine plus bevacizumab compared with gemcitabine plus placebo in patients with advanced pancreatic cancer: phase III trial of the Cancer and Leukemia Group B (CALGB 80303). J Clin Oncol. 2010; 28:3617–3622.
32. Fuchs CS, Azevedo S, Okusaka T, Van Laethem JL, Lipton LR, Riess H, Szczylik C, Moore MJ, Peeters M, Bodoky G, Ikeda M, Melichar B, Nemecek R, Ohkawa S, Świeboda-Sadlej A, Tjulandin SA, Van Cutsem E, Loberg R, Haddad V, Gansert JL, Bach BA, Carrato A. A Phase 3 Randomized, Double-Blind, Placebo-Controlled Trial of Ganitumab or Placebo in Combination With Gemcitabine as First-Line Therapy for Metastatic Adenocarcinoma of the Pancreas: the GAMMA Trial. Annals of Oncology. 2015; 26doi:10.1093/annonc/mdv1027.
33. Goncalves A, Gilabert M, Francois E, Dahan L, Perrier H, Lamy R, Re D, Largillier R, Gasmi M, Tchiknavorian X, Esterni B, Genre D, Moureau-Zabotto L, Giovannini M, Seitz JF, Delpero JR, Turrini O, Viens P, Raoul JL. BAYPAN study: a double-blind phase III randomized trial comparing gemcitabine plus sorafenib and gemcitabine plus placebo in patients with advanced pancreatic cancer. Ann Oncol. 2012; 23:2799–2805.
34. Kindler HL, Ioka T, Richel DJ, Bennouna J, Letourneau R, Okusaka T, Funakoshi A, Furuse J, Park YS, Ohkawa S, Springett GM, Wasan HS, Trask PC, Bycott P, Ricart AD, Kim S, Van Cutsem E. Axitinib plus gemcitabine versus placebo plus gemcitabine in patients with advanced pancreatic adenocarcinoma: a double-blind randomised phase 3 study. Lancet Oncol. 2011; 12:256–262.
35. Richly H, Maute L, Heil G, Russel J, Jager E, Koeberle D, Fuxius S, Weigang-Koehler K, Aulitzky W, Woehrmann B, Hartung GG, Moritz B, Burkholder I, Scheulen ME, Bergmann L. Prospective randomized phase II trial with gemcitabine versus gemcitabine plus sunitinib in advanced pancreatic cancer: A study of the CESAR Central European Society for Anticancer Drug Research-EWIV. ASCO Meeting Abstracts. 2013; 31:4035.
36. Rougier P, Riess H, Manges R, Karasek P, Humblet Y, Barone C, Santoro A, Assadourian S, Hatteville L, Philip PA. Randomised, placebo-controlled, double-blind, parallel-group phase III study evaluating aflibercept in patients receiving first-line treatment with gemcitabine for metastatic pancreatic cancer. Eur J Cancer. 2013; 49:2633–2642.
37. Van Cutsem E, van de Velde H, Karasek P, Oettle H, Vervenne WL, Szawlowski A, Schoffski P, Post S, Verslype C, Neumann H, Safran H, Humblet Y, Perez Ruixo J, Ma Y, Von Hoff D. Phase III trial of gemcitabine plus tipifarnib compared with gemcitabine plus placebo in advanced pancreatic cancer. J Clin Oncol. 2004; 22:1430–1438.
38. Wolpin BM, Hezel AF, Abrams T, Blaszkowsky LS, Meyerhardt JA, Chan JA, Enzinger PC, Allen B, Clark JW, Ryan DP, Fuchs CS. Oral mTOR inhibitor everolimus in patients with gemcitabine-refractory metastatic pancreatic cancer. J Clin Oncol. 2009; 27:193–198.
39. Infante JR, Somer BG, Park JO, Li CP, Scheulen ME, Kasubhai SM, Oh DY, Liu Y, Redhu S, Steplewski K, Le N. A randomised, double-blind, placebo-controlled trial of trametinib, an oral MEK inhibitor, in combination with gemcitabine for patients with untreated metastatic adenocarcinoma of the pancreas. Eur J Cancer. 2014; 50:2072–2081.
40. Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, Campos D, Lim R, Ding K, Clark G, Voskoglou-Nomikos T, Ptasynski M, Parulekar W. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007; 25:1960–1966.
41. Yada A, Yazawa M, Ishida S, Yoshida H, Ichikawa K, Kurakata S, Fujiwara K. A novel humanized anti-human death receptor 5 antibody CS-1008 induces apoptosis in tumor cells without toxicity in hepatocytes. Ann Oncol. 2008; 19:1060–1067.
42. Ichikawa K, Liu W, Zhao L, Wang Z, Liu D, Ohtsuka T, Zhang H, Mountz JD, Koopman WJ, Kimberly RP, Zhou T. Tumoricidal activity of a novel anti-human DR5 monoclonal antibody without hepatocyte cytotoxicity. Nat Med. 2001; 7:954–960.
43. Sprick MR, Weigand MA, Rieser E, Rauch CT, Juo P, Blenis J, Krammer PH, Walczak H. FADD/MORT1 and caspase-8 are recruited to TRAIL receptors 1 and 2 and are essential for apoptosis mediated by TRAIL receptor 2. Immunity. 2000; 12:599–609.
44. Li H, Zhu H, Xu CJ, Yuan J. Cleavage of BID by caspase 8 mediates the mitochondrial damage in the Fas pathway of apoptosis. Cell. 1998; 94:491–501.
45. DeRosier LC, Huang ZQ, Sellers JC, Buchsbaum DJ, Vickers SM. Treatment with gemcitabine and TRA-8 anti-death receptor-5 mAb reduces pancreatic adenocarcinoma cell viability in vitro and growth in vivo. J Gastrointest Surg. 2006; 10:1291–1300. discussion 1300.
46. Derosier LC, Vickers SM, Zinn KR, Huang Z, Wang W, Grizzle WE, Sellers J, Stockard CR Jr, Zhou T, Oliver PG, Arnoletti P, Lobuglio AF, Buchsbaum DJ. TRA-8 anti-DR5 monoclonal antibody and gemcitabine induce apoptosis and inhibit radiologically validated orthotopic pancreatic tumor growth. Mol Cancer Ther. 2007; 6:3198–3207.
47. Forero-Torres A, Shah J, Wood T, Posey J, Carlisle R, Copigneaux C, Luo FR, Wojtowicz-Praga S, Percent I, Saleh M. Phase I trial of weekly tigatuzumab, an agonistic humanized monoclonal antibody targeting death receptor 5 (DR5). Cancer Biother Radiopharm. 2010; 25:13–19.
48. Forero-Torres A, Infante JR, Waterhouse D, Wong L, Vickers S, Arrowsmith E, He AR, Hart L, Trent D, Wade J, Jin X, Wang Q, Austin T, Rosen M, Beckman R, von Roemeling R, Greenberg J, Saleh M. Phase 2, multicenter, open-label study of tigatuzumab (CS-1008), a humanized monoclonal antibody targeting death receptor 5, in combination with gemcitabine in chemotherapy-naive patients with unresectable or metastatic pancreatic cancer. Cancer Med. 2013; 2:925–932.
49. Liu D, Rutter WJ, Wang LH. Enhancement of transforming potential of human insulinlike growth factor 1 receptor by N-terminal truncation and fusion to avian sarcoma virus UR2 gag sequence. Journal of virology. 1992; 66:374–385.
50. Liu D, Zong CS, Wang LH. Distinctive effects of the carboxyl-terminal sequence of the insulin-like growth factor I receptor on its signaling functions. Journal of virology. 1993; 67:6835–6840.
51. Liu D, Rutter WJ, Wang LH. Modulating effects of the extracellular sequence of the human insulinlike growth factor I receptor on its transforming and tumorigenic potential. Journal of virology. 1993; 67:9–18.
52. Liu D, Wang LH. Oncogenes, Protein Tyrosine Kinases, and Signal Transduction. Journal of biomedical science. 1994; 1:65–82.
53. Liu W, Bloom DA, Cance WG, Kurenova EV, Golubovskaya VM, Hochwald SN. FAK and IGF-IR interact to provide survival signals in human pancreatic adenocarcinoma cells. Carcinogenesis. 2008; 29:1096–1107.
54. Bergmann U, Funatomi H, Yokoyama M, Beger HG, Korc M. Insulin-like growth factor I overexpression in human pancreatic cancer: evidence for autocrine and paracrine roles. Cancer Res. 1995; 55:2007–2011.
55. Broussas M, Dupont J, Gonzalez A, Blaecke A, Fournier M, Corvaia N, Goetsch L. Molecular mechanisms involved in activity of h7C10, a humanized monoclonal antibody, to IGF-1 receptor. Int J Cancer. 2009; 124:2281–2293.
56. Pandini G, Wurch T, Akla B, Corvaia N, Belfiore A, Goetsch L. Functional responses and in vivo anti-tumour activity of h7C10: a humanised monoclonal antibody with neutralising activity against the insulin-like growth factor-1 (IGF-1) receptor and insulin/IGF-1 hybrid receptors. Eur J Cancer. 2007; 43:1318–1327.
57. Scartozzi M, Bianconi M, Maccaroni E, Giampieri R, Berardi R, Cascinu S. Dalotuzumab, a recombinant humanized mAb targeted against IGFR1 for the treatment of cancer. Curr Opin Mol Ther. 2010; 12:361–371.
58. Goetsch L, Gonzalez A, Leger O, Beck A, Pauwels PJ, Haeuw JF, Corvaia N. A recombinant humanized anti-insulin-like growth factor receptor type I antibody (h7C10) enhances the antitumor activity of vinorelbine and anti-epidermal growth factor receptor therapy against human cancer xenografts. Int J Cancer. 2005; 113:316–328.
59. Atzori F, Tabernero J, Cervantes A, Prudkin L, Andreu J, Rodriguez-Braun E, Domingo A, Guijarro J, Gamez C, Rodon J, Di Cosimo S, Brown H, Clark J, Hardwick JS, Beckman RA, Hanley WD, Hsu K, Calvo E, Rosello S, Langdon RB, Baselga J. A phase I pharmacokinetic and pharmacodynamic study of dalotuzumab (MK-0646), an anti-insulin-like growth factor-1 receptor monoclonal antibody, in patients with advanced solid tumors. Clin Cancer Res. 2011; 17:6304–6312.
60. Javle M VG, et al. Randomized phase II study of gemcitabine (G) plus anti-IGF-1R antibody MK-0646, G plus erlotinib (E) plus MK-0646 and G plus E for advanced pancreatic cancer. J Clin Oncol. 29:2011.
61. Kaplan-Lefko PJ, Graves JD, Zoog SJ, Pan Y, Wall J, Branstetter DG, Moriguchi J, Coxon A, Huard JN, Xu R, Peach ML, Juan G, Kaufman S, Chen Q, Bianchi A, Kordich JJ, Ma M, Foltz IN, Gliniak BC. Conatumumab, a fully human agonist antibody to death receptor 5, induces apoptosis via caspase activation in multiple tumor types. Cancer Biol Ther. 2010; 9:618–631.
62. Ozawa F, Friess H, Kleeff J, Xu ZW, Zimmermann A, Sheikh MS, Buchler MW. Effects and expression of TRAIL and its apoptosis-promoting receptors in human pancreatic cancer. Cancer Lett. 2001; 163:71–81.
63. Kindler HL GL, Stephenson J, et al. A phase Ib study to evaluate the safety and efficacy of AMG 655 in combination with gemcitabine (G) in patients (pts) with metastatic pancreatic cancer (PC). J Clin Oncol. 2009; 27.
64. Kindler HL, Richards DA, Garbo LE, Garon EB, Stephenson JJ Jr., Rocha-Lima CM, Safran H, Chan D, Kocs DM, Galimi F, McGreivy J, Bray SL, Hei Y, Feigal EG, Loh E, Fuchs CS. A randomized, placebo-controlled phase 2 study of ganitumab (AMG 479) or conatumumab (AMG 655) in combination with gemcitabine in patients with metastatic pancreatic cancer. Ann Oncol. 2012; 23:2834–2842.
65. Rowinsky EK, Youssoufian H, Tonra JR, Solomon P, Burtrum D, Ludwig DL. IMC-A12, a human IgG1 monoclonal antibody to the insulin-like growth factor I receptor. Clin Cancer Res. 2007; 13:5549s–5555s.
66. Burtrum D, Zhu Z, Lu D, Anderson DM, Prewett M, Pereira DS, Bassi R, Abdullah R, Hooper AT, Koo H, Jimenez X, Johnson D, Apblett R, Kussie P, Bohlen P, Witte L, Hicklin DJ, Ludwig DL. A fully human monoclonal antibody to the insulin-like growth factor I receptor blocks ligand-dependent signaling and inhibits human tumor growth in vivo. Cancer Res. 2003; 63:8912–8921.
67. Higano CS YE, Whiting SH, et al. A phase I, first in man study of weekly IMC-A12, a fully human insulin-like growth factor receptor IgG1 monoclonal antibody in patients with advanced solid tumors. ASCO. 2007; A269 2009.
68. Philip PA, Goldman B, Ramanathan RK, Lenz HJ, Lowy AM, Whitehead RP, Wakatsuki T, Iqbal S, Gaur R, Benedetti JK, Blanke CD. Dual blockade of epidermal growth factor receptor and insulin-like growth factor receptor-1 signaling in metastatic pancreatic cancer: phase Ib and randomized phase II trial of gemcitabine, erlotinib, and cixutumumab versus gemcitabine plus erlotinib (SWOG S0727). Cancer. 2014; 120:2980–2985.
69. Schnitzer T KK, Rebers F, et al. Characterization of a re-combinant, fully human monoclonal antibody directed against the human insulin-like growth factor-1 receptor. 18th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics, Poster #214 2006.
70. F. Hoffmann-La Roche Ltd: IGF-1R (RO4858696) Roche Clinical Study Report-Protocol BO19373. Research Report 1027082 2009.
71. Kawanami T, Takiguchi S, Ikeda N, Funakoshi A. A humanized anti-IGF-1R monoclonal antibody (R1507) and/or metformin enhance gemcitabine-induced apoptosis in pancreatic cancer cells. Oncol Rep. 2012; 27:867–872.
72. Dragovich T BA, Pineda C, et al. Effect of R1507, an anti-IGF-1R monocolonal antibody, on sensitization of pancreatic cancer cell lines to mTOR inhibition. 2010 Gastrointestinal Cancers Symposium Abstract 177.
73. Kurzrock R, Patnaik A, Aisner J, Warren T, Leong S, Benjamin R, Eckhardt SG, Eid JE, Greig G, Habben K, McCarthy CD, Gore L. A phase I study of weekly R1507, a human monoclonal antibody insulin-like growth factor-I receptor antagonist, in patients with advanced solid tumors. Clin Cancer Res. 2010; 16:2458–2465.
74. Antonarakis ES, Carducci MA, Eisenberger MA, Denmeade SR, Slovin SF, Jelaca-Maxwell K, Vincent ME, Scher HI, Morris MJ. Phase I rapid dose-escalation study of AGS-1C4D4, a human anti-PSCA (prostate stem cell antigen) monoclonal antibody, in patients with castration-resistant prostate cancer: a PCCTC trial. Cancer Chemother Pharmacol. 2012; 69:763–771.
75. Argani P, Rosty C, Reiter RE, Wilentz RE, Murugesan SR, Leach SD, Ryu B, Skinner HG, Goggins M, Jaffee EM, Yeo CJ, Cameron JL, Kern SE, Hruban RH. Discovery of new markers of cancer through serial analysis of gene expression: prostate stem cell antigen is overexpressed in pancreatic adenocarcinoma. Cancer Res. 2001; 61:4320–4324.
76. Raff AB, Gray A, Kast WM. Prostate stem cell antigen: a prospective therapeutic and diagnostic target. Cancer Lett. 2009; 277:126–132.
77. Saffran DC, Raitano AB, Hubert RS, Witte ON, Reiter RE, Jakobovits A. Anti-PSCA mAbs inhibit tumor growth and metastasis formation and prolong the survival of mice bearing human prostate cancer xenografts. Proc Natl Acad Sci U S A. 2001; 98:2658–2663.
78. Gu Z, Yamashiro J, Kono E, Reiter RE. Anti-prostate stem cell antigen monoclonal antibody 1G8 induces cell death in vitro and inhibits tumor growth in vivo via a Fc-independent mechanism. Cancer Res. 2005; 65:9495–9500.
79. Morris MJ, Eisenberger MA, Pili R, Denmeade SR, Rathkopf D, Slovin SF, Farrelly J, Chudow JJ, Vincent M, Scher HI, Carducci MA. A phase I/IIA study of AGS-PSCA for castration-resistant prostate cancer. Ann Oncol. 2012; 23:2714–2719.
80. Wolpin BM, O’Reilly EM, Ko YJ, Blaszkowsky LS, Rarick M, Rocha-Lima CM, Ritch P, Chan E, Spratlin J, Macarulla T, McWhirter E, Pezet D, Lichinitser M, Roman L, Hartford A, Morrison K, Jackson L, Vincent M, Reyno L, Hidalgo M. Global, multicenter, randomized, phase II trial of gemcitabine and gemcitabine plus AGS-1C4D4 in patients with previously untreated, metastatic pancreatic cancer. Ann Oncol. 2013; 24:1792–1801.
81. O’Reilly E SL, Bendell J, et al. Phase Ib of anticancer stem cell antibody OMP-59R5 (anti-Notch2/3) in combination with nab-paclitaxel and gemcitabine (Nab-P+Gem) in patients (pts) with untreated metastatic pancreatic cancer (mPC). J Clin Oncol. 32, 2014.
82. De Jesus-Acosta A, Laheru D, Maitra A, Arcaroli J, Rudek MA, Dasari A, Blatchford PJ, Quackenbush K, Messersmith W. A phase II study of the gamma secretase inhibitor RO4929097 in patients with previously treated metastatic pancreatic adenocarcinoma. Invest New Drugs. 2014; 32:739–745.
83. Bendell J CA, Smith L, et al. Final results of a phase 1b of OMP-59R5 (anti-notch2/3/stem cell antibody) in combination with nab-paclitaxel and gemcitabine (Nab-P + Gem) in patients with untreated metastatic pancreatic cancer. Annals of Oncology. 2014; 25. iv210-iv253 101093/annonc/mdu334 2014.
84. Ocean AJ, Pennington KL, Guarino MJ, Sheikh A, Bekaii-Saab T, Serafini AN, Lee D, Sung MW, Gulec SA, Goldsmith SJ, Manzone T, Holt M, O’Neil BH, Hall N, Montero AJ, Kauh J, Gold DV, Horne H, Wegener WA, Goldenberg DM. Fractionated radioimmunotherapy with (90) Y-clivatuzumab tetraxetan and low-dose gemcitabine is active in advanced pancreatic cancer: A phase 1 trial. Cancer. 2012; 118:5497–5506.
85. Hollingsworth MA, Swanson BJ. Mucins in cancer: protection and control of the cell surface. Nat Rev Cancer. 2004; 4:45–60.
86. Gold DV, Karanjawala Z, Modrak DE, Goldenberg DM, Hruban RH. PAM4-reactive MUC1 is a biomarker for early pancreatic adenocarcinoma. Clin Cancer Res. 2007; 13:7380–7387.
87. Gold DV, Goggins M, Modrak DE, Newsome G, Liu M, Shi C, Hruban RH, Goldenberg DM. Detection of early-stage pancreatic adenocarcinoma. Cancer Epidemiol Biomarkers Prev. 2010; 19:2786–2794.
88. Rachagani S, Torres M, Kumar S, Haridas D, Baine M, Macha M, Kaur S, Ponnusamy M, Dey P, Seshacharyulu P, Johansson S, Jain M, Wagner K-U, Batra S. Mucin (Muc) expression during pancreatic cancer progression in spontaneous mouse model: potential implications for diagnosis and therapy. Journal of Hematology & Oncology. 2012; 5:68.
89. Schroeder JA, Adriance MC, Thompson MC, Camenisch TD, Gendler SJ. MUC1 alters beta-catenin-dependent tumor formation and promotes cellular invasion. Oncogene. 2003; 22:1324–1332.
90. Raina D, Kharbanda S, Kufe D. The MUC1 oncoprotein activates the anti-apoptotic phosphoinositide 3-kinase/Akt and Bcl-xL pathways in rat 3Y1 fibroblasts. J Biol Chem. 2004; 279:20607–20612.
91. Wei X, Xu H, Kufe D. Human MUC1 oncoprotein regulates p53-responsive gene transcription in the genotoxic stress response. Cancer Cell. 2005; 7:167–178.
92. Gold DV, Lew K, Maliniak R, Hernandez M, Cardillo T. Characterization of monoclonal antibody PAM4 reactive with a pancreatic cancer mucin. Int J Cancer. 1994; 57:204–210.
93. Gold DV, Cardillo T, Vardi Y, Blumenthal R. Radioimmunotherapy of experimental pancreatic cancer with 131I-labeled monoclonal antibody PAM4. Int J Cancer. 1997; 71:660–667.
94. Cardillo TM, Ying Z, Gold DV. Therapeutic advantage of (90)yttrium-versus (131)iodine-labeled PAM4 antibody in experimental pancreatic cancer. Clin Cancer Res. 2001; 7:3186–3192.
95. Cardillo TM, Blumenthal R, Ying Z, Gold DV. Combined gemcitabine and radioimmunotherapy for the treatment of pancreatic cancer. Int J Cancer. 2002; 97:386–392.
96. Gold DV, Modrak DE, Schutsky K, Cardillo TM. Combined 90Yttrium-DOTA-labeled PAM4 antibody radioimmunotherapy and gemcitabine radiosensitization for the treatment of a human pancreatic cancer xenograft. Int J Cancer. 2004; 109:618–626.
97. Gold DV, Schutsky K, Modrak D, Cardillo TM. Low-dose radioimmunotherapy ((90)Y-PAM4) combined with gemcitabine for the treatment of experimental pancreatic cancer. Clin Cancer Res. 2003; 9:3929S–3937S.
98. Gulec SA, Cohen SJ, Pennington KL, Zuckier LS, Hauke RJ, Horne H, Wegener WA, Teoh N, Gold DV, Sharkey RM, Goldenberg DM. Treatment of advanced pancreatic carcinoma with 90Y-Clivatuzumab Tetraxetan: a phase I single-dose escalation trial. Clin Cancer Res. 2011; 17:4091–4100.
99. Picozzi V RR, Lowery M, et al. Feasibility and results of a randomized phase lb study of fractionated 90Y-clivatuzumab tetraxetan in patients with metastatic pancreatic cancer having two or more prior therapies. J Clin Oncol. 32:5s2014.
100. Sekulic A, Migden MR, Oro AE, Dirix L, Lewis KD, Hainsworth JD, Solomon JA, Yoo S, Arron ST, Friedlander PA, Marmur E, Rudin CM, Chang AL, Low JA, Mackey HM, Yauch RL, Graham RA, Reddy JC, Hauschild A. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012; 366:2171–2179.
101. Robarge KD, Brunton SA, Castanedo GM, Cui Y, Dina MS, Goldsmith R, Gould SE, Guichert O, Gunzner JL, Halladay J, Jia W, Khojasteh C, Koehler MF, Kotkow K, La H, Lalonde RL, Lau K, Lee L, Marshall D, Marsters JC Jr., Murray LJ, Qian C, Rubin LL, Salphati L, Stanley MS, Stibbard JH, Sutherlin DP, Ubhayaker S, Wang S, Wong S, et al. GDC-0449-a potent inhibitor of the hedgehog pathway. Bioorg Med Chem Lett. 2009; 19:5576–5581.
102. Evangelista M, Tian H, de Sauvage FJ. The hedgehog signaling pathway in cancer. Clin Cancer Res. 2006; 12:5924–5928.
103. Lu JT, Zhao WD, He W, Wei W. Hedgehog signaling pathway mediates invasion and metastasis of hepatocellular carcinoma via ERK pathway. Acta Pharmacol Sin. 2012; 33:691–700.
104. Agyeman A, Mazumdar T, Houghton JA. Regulation of DNA damage following termination of Hedgehog (HH) survival signaling at the level of the GLI genes in human colon cancer. Oncotarget. 2012; 3:854–868.
105. Ajeawung NF, Wang HY, Kamnasaran D. Progress from clinical trials and emerging non-conventional therapies for the treatment of Medulloblastomas. Cancer Lett. 2013; 330:130–140.
106. Ramaswamy B, Lu Y, Teng KY, Nuovo G, Li X, Shapiro CL, Majumder S. Hedgehog signaling is a novel therapeutic target in tamoxifen-resistant breast cancer aberrantly activated by PI3K/AKT pathway. Cancer Res. 2012; 72:5048–5059.
107. Yang L, Su X, Xie J. Activation of Hedgehog pathway in gastrointestinal cancers. Vitam Horm. 2012; 88:461–472.
108. Bertrand FE, Angus CW, Partis WJ, Sigounas G. Developmental pathways in colon cancer: crosstalk between WNT, BMP, Hedgehog and Notch. Cell Cycle. 2012; 11:4344–4351.
109. Thayer SP, di Magliano MP, Heiser PW, Nielsen CM, Roberts DJ, Lauwers GY, Qi YP, Gysin S, Fernandez-del Castillo C, Yajnik V, Antoniu B, McMahon M, Warshaw AL, Hebrok M. Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis. Nature. 2003; 425:851–856.
110. Ogden SK, Ascano M Jr., Stegman MA, Robbins DJ. Regulation of Hedgehog signaling: a complex story. Biochem Pharmacol. 2004; 67:805–814.
111. Hidalgo M, Maitra A. The hedgehog pathway and pancreatic cancer. N Engl J Med. 2009; 361:2094–2096.
112. Singh BN, Fu J, Srivastava RK, Shankar S. Hedgehog signaling antagonist GDC-0449 (Vismodegib) inhibits pancreatic cancer stem cell characteristics: molecular mechanisms. PLoS One. 2011; 6:e27306.
113. Scales SJ, de Sauvage FJ. Mechanisms of Hedgehog pathway activation in cancer and implications for therapy. Trends Pharmacol Sci. 2009; 30:303–312.
114. Catenacci D BN, Nattam S, et al. Final analysis of a phase IB/randomized phase II study of gemcitabine (G) plus placebo (P) or vismodegib (V), a hedgehog (Hh) pathway inhibitor, in patients (pts) with metastatic pancreatic cancer (PC): A University of Chicago phase II consortium study. J Clin Oncol. 31, 2013.
115. De Jesus-Acosta A ODP, Ramanathan R, et al. A phase II study of vismodegib, a hedgehog (Hh) pathway inhibitor, combined with gemcitabine and nab-paclitaxel (nab-P) in patients (pts) with untreated metastatic pancreatic ductal adenocarcinoma (PDA). J Clin Oncol. 32, 2014.
116. Dubreuil P, Letard S, Ciufolini M, Gros L, Humbert M, Casteran N, Borge L, Hajem B, Lermet A, Sippl W, Voisset E, Arock M, Auclair C, Leventhal PS, Mansfield CD, Moussy A, Hermine O. Masitinib (AB1010), a potent and selective tyrosine kinase inhibitor targeting KIT. PLoS One. 2009; 4:e7258.
117. Humbert M, Casteran N, Letard S, Hanssens K, Iovanna J, Finetti P, Bertucci F, Bader T, Mansfield CD, Moussy A, Hermine O, Dubreuil P. Masitinib combined with standard gemcitabine chemotherapy: in vitro and in vivo studies in human pancreatic tumour cell lines and ectopic mouse model. PLoS One. 2010; 5:e9430.
118. Soria JC, Massard C, Magne N, Bader T, Mansfield CD, Blay JY, Bui BN, Moussy A, Hermine O, Armand JP. Phase 1 dose-escalation study of oral tyrosine kinase inhibitor masitinib in advanced and/or metastatic solid cancers. Eur J Cancer. 2009; 45:2333–2341.
119. Hammel F MF, Deplanque G, et al. Oral tyrosine kinase inhibitor masitinib in combination with gemcitabine in patients with advanced pancreatic cancer: A multicenter phase II study. J Clin Oncol. 27:15s, 2009.
120. Deplanque G DM, Hebbar M, et al. Masitinib in nonresectable pancreatic cancer: Results of a phase III randomized placebo-controlled trial. J Clin Oncol. 31, 2013.
121. Yeh TC, Marsh V, Bernat BA, Ballard J, Colwell H, Evans RJ, Parry J, Smith D, Brandhuber BJ, Gross S, Marlow A, Hurley B, Lyssikatos J, Lee PA, Winkler JD, Koch K, Wallace E. Biological characterization of ARRY-142886 (AZD6244), a potent, highly selective mitogen-activated protein kinase kinase 1/2 inhibitor. Clin Cancer Res. 2007; 13:1576–1583.
122. Adjei AA, Cohen RB, Franklin W, Morris C, Wilson D, Molina JR, Hanson LJ, Gore L, Chow L, Leong S, Maloney L, Gordon G, Simmons H, Marlow A, Litwiler K, Brown S, Poch G, Kane K, Haney J, Eckhardt SG. Phase I pharmacokinetic and pharmacodynamic study of the oral, small-molecule mitogen-activated protein kinase kinase 1/2 inhibitor AZD6244 (ARRY-142886) in patients with advanced cancers. J Clin Oncol. 2008; 26:2139–2146.
123. Ko A TM, Bekaii-Saab T, et al. Dual MEK/EGFR inhibition for advanced, chemotherapy-refractory pancreatic cancer: A multicenter phase II trial of selumetinib (AZD6244; ARRY-142886) plus erlotinib. J Clin Oncol. 31, 2013.
124. Chang YM, Bai L, Liu S, Yang JC, Kung HJ, Evans CP. Src family kinase oncogenic potential and pathways in prostate cancer as revealed by AZD0530. Oncogene. 2008; 27:6365–6375.
125. Renouf DJ, Moore MJ, Hedley D, Gill S, Jonker D, Chen E, Walde D, Goel R, Southwood B, Gauthier I, Walsh W, McIntosh L, Seymour L. A phase I/II study of the Src inhibitor saracatinib (AZD0530) in combination with gemcitabine in advanced pancreatic cancer. Invest New Drugs. 2012; 30:779–786.
126. Kim K, Kong SY, Fulciniti M, Li X, Song W, Nahar S, Burger P, Rumizen MJ, Podar K, Chauhan D, Hideshima T, Munshi NC, Richardson P, Clark A, Ogden J, Goutopoulos A, Rastelli L, Anderson KC, Tai YT. Blockade of the MEK/ERK signalling cascade by AS703026, a novel selective MEK1/2 inhibitor, induces pleiotropic anti-myeloma activity in vitro and in vivo. Br J Haematol. 2010; 149:537–549.
127. Yoon J, Koo KH, Choi KY. MEK1/2 inhibitors AS703026 and AZD6244 may be potential therapies for KRAS mutated colorectal cancer that is resistant to EGFR monoclonal antibody therapy. Cancer Res. 2011; 71:445–453.
128. Verslype C HP, Hidalgo M, et al. Pimasertib plus gemcitabine in metastatic pancreatic adenocarcinoma: Results of a safety run-in part of a phase II trial. J Clin Oncol. 31, 2013.
129. Iverson C, Larson G, Lai C, Yeh LT, Dadson C, Weingarten P, Appleby T, Vo T, Maderna A, Vernier JM, Hamatake R, Miner JN, Quart B. RDEA119/BAY 869766: a potent, selective, allosteric inhibitor of MEK1/2 for the treatment of cancer. Cancer Res. 2009; 69:6839–6847.
130. Chang Q, Chapman MS, Miner JN, Hedley DW. Antitumour activity of a potent MEK inhibitor RDEA119/BAY 869766 combined with rapamycin in human orthotopic primary pancreatic cancer xenografts. BMC Cancer. 2010; 10:515.
131. Van Laethem J JJ, Heinemann V, et al. Phase II study of refametinib (BAY 86-9766), an allosteric dual MEK 1/2 inhibitor, and gemcitabine in patients with unresectable, locally advanced, or metastatic pancreatic cancer. J Clin Oncol. 32:5s, 2014.
132. Zhou L, McMahon C, Bhagat T, Alencar C, Yu Y, Fazzari M, Sohal D, Heuck C, Gundabolu K, Ng C, Mo Y, Shen W, Wickrema A, Kong G, Friedman E, Sokol L, Mantzaris I, Pellagatti A, Boultwood J, Platanias LC, Steidl U, Yan L, Yingling JM, Lahn MM, List A, Bitzer M, Verma A. Reduced SMAD7 leads to overactivation of TGF-beta signaling in MDS that can be reversed by a specific inhibitor of TGF-beta receptor I kinase. Cancer Res. 2011; 71:955–963.
133. Kozloff M CR, Nadal T, et al. Phase Ib study evaluating safety and pharmacokinetics (PK) of the oral transforming growth factor-beta (TGF-ß) receptor I kinase inhibitor LY2157299 monohydrate (LY) when combined with gemcitabine in patients with advanced cancer. J Clin Oncol. 31, 2013.
134. Wang B CD, Feng Y, et al. Novel PARP inhibitors with potent antitumor activity as single-agent and combination therapies. Mol Cancer Ther. 2009; 8:A121. 2009.
135. De Bono J ML, Gonzalez M, et al. First-in-human trial of novel oral PARP inhibitor BMN 673 in patients with solid tumors. J Clin Oncol. 31, 2013.
136. Donawho CK, Luo Y, Penning TD, Bauch JL, Bouska JJ, Bontcheva-Diaz VD, Cox BF, DeWeese TL, Dillehay LE, Ferguson DC, Ghoreishi-Haack NS, Grimm DR, Guan R, Han EK, Holley-Shanks RR, Hristov B, Idler KB, Jarvis K, Johnson EF, Kleinberg LR, Klinghofer V, Lasko LM, Liu X, Marsh KC, McGonigal TP, Meulbroek JA, Olson AM, Palma JP, Rodriguez LE, Shi Y, et al. ABT-888, an orally active poly(ADP-ribose) poly-merase inhibitor that potentiates DNA-damaging agents in preclinical tumor models. Clin Cancer Res. 2007; 13:2728–2737.
137. De Soto J MR. The use of PARP inhibitors as single agents and as chemosensitizers in sporadic pancreatic cancer. J Clin Oncol. 29, 2011.
138. O’Reilly E LM, Segal M, et al. Phase IB trial of cisplatin (C), gemcitabine (G), and veliparib (V) in patients with known or potential BRCA or PALB2-mutated pancreas adenocarcinoma (PC). J Clin Oncol. 32:5s, 2014.
139. Rowinsky EK, Windle JJ, Von Hoff DD. Ras protein farnesyltransferase: A strategic target for anticancer therapeutic development. J Clin Oncol. 1999; 17:3631–3652.
140. Weisz B, Giehl K, Gana-Weisz M, Egozi Y, Ben-Baruch G, Marciano D, Gierschik P, Kloog Y. A new functional Ras antagonist inhibits human pancreatic tumor growth in nude mice. Oncogene. 1999; 18:2579–2588.
141. Laheru D, Shah P, Rajeshkumar NV, McAllister F, Taylor G, Goldsweig H, Le DT, Donehower R, Jimeno A, Linden S, Zhao M, Song D, Rudek MA, Hidalgo M. Integrated preclinical and clinical development of S-trans, trans-Farnesylthiosalicylic Acid (FTS, Salirasib) in pancreatic cancer. Invest New Drugs. 2012; 30:2391–2399.
142. Bustinza-Linares E, Kurzrock R, Tsimberidou AM. Salirasib in the treatment of pancreatic cancer. Future Oncol. 2010; 6:885–891.
143. Venkannagari S, Fiskus W, Peth K, Atadja P, Hidalgo M, Maitra A, Bhalla KN. Superior efficacy of co-treatment with dual PI3K/mTOR inhibitor NVP-BEZ235 and pan-histone deacetylase inhibitor against human pancreatic cancer. Oncotarget. 2012; 3:1416–1427.
144. Rooman I. Sirtainties in pancreatic cancer? Oncoscience. 2014; 1:183–184.
145. Yan HH, Jung KH, Son MK, Fang Z, Kim SJ, Ryu YL, Kim J, Kim MH, Hong SS. Crizotinib exhibits antitumor activity by targeting ALK signaling not c-MET in pancreatic cancer. Oncotarget. 2014; 5:9150–9168.
146. Iragavarapu C, Mustafa M, Akinleye A, Furqan M, Mittal V, Cang S, Liu D. Novel ALK inhibitors in clinical use and development. Journal of Hematology & Oncology. 2015; 8:17.
147. Goel G, Sun W. Novel approaches in the management of pancreatic ductal adenocarcinoma: potential promises for the future. Journal of Hematology & Oncology. 2015; 8:44.