
Introduction
The mTOR (Target of Rapamycin) pathway is involved in both cancer and aging. Furthermore, common cancers are age-related diseases, and their incidence increases exponentially with age. Rapamycin (sirolimus) and other rapalogs (temsirolimus, everolimus) may delay cancer by targeting directly pre-cancerous cells and by slowing down organism aging.
Rapamycin delays tobacco-related and lung cancer in mice
In 2007, it was demonstrated that rapamycin prevents lung cancer in mice caused by the tobacco-specific carcinogen NNK [1]. Mice were treated with NNK at the age of 6 weeks. In one of experiments, treatment with rapamycin (every-other-day) was started one week after NNK exposure. Rapamycin decreased tumor multiplicity by 90%. Phenotypic progression of tumors was slowed, tumors were smaller in size by 74% due to decreased cell proliferation. Granville et al. envisioned a clinical trial of rapamycin for smokers at high risk of lung cancer [1].
Supporting these results, Patlolla et al. showed that rapamycin delayed (or prevented) development of NNK-induced lung adenoma and progression from lung adenoma to adenocarcinoma in mice [2]. When treatment with rapamycin was started early (three weeks after NNK), rapamycin suppressed development of lung adenoma and adenocarcinoma [2]. For late intervention (rapamycin treatment was started 20 weeks after NNK exposure) rapamycin suppressed progression from lung adenoma to lung cancer. The authors concluded that rapamycin is effective even after dysplastic adenoma or early adenocarcinoma stages and may be useful for high-risk lung cancer people [2].
Yan et al. found that treatment with rapamycin for 14 weeks, beginning 12 weeks after administration of a polycyclic aromatic hydrocarbon [benzo(a)pyrene] (BP), decreased lung tumor load by 84% [3].
In a model of EGFR mutant lung cancer in mice, rapamycin prevented or slowed down tumor development. Median overall survival was prolonged by more than three-fold [4].
In a different mouse model, 4-nitroquinoline-1 oxide (a surrogate of tobacco exposure) caused head and neck squamous cell carcinoma (HNSCC). This tobacco-mimicking carcinogen leads to the appearance of preneoplastic and tumoral lesions, with 100% incidence. Many of these lesions progressed into highly malignant squamous cell carcinomas few weeks after carcinogen withdrawal. The Akt-mTOR was overactivated as an early event in dysplastic lesions. Rapamycin delayed the onset and slowed progression of tumorigenesis [5]. Chronic administration of rapamycin prevented the malignant conversion of precancerous lesions [5]. It was suggested to use rapamycin for chemoprevention of upper aerodigestive tract cancers [5, 6].
Rapamycin prevents cancer and extends lifespan in cancer-prone mice
In transgenic HER-2/neu cancer-prone mice, rapamycin treatment (started 2 months after birth) decreased rate of aging, increased lifespan, and suppressed carcinogenesis. Rapamycin delayed tumor onset, decreased the number of tumors per animal and tumor size, increasing maximal lifespan by 12.4% [7]. In the follow-up work in these mice, some degree of cancer prevention can be achieved by low doses of rapamycin [8].
In highly tumor-prone p53−/− mice, rapamycin extended the mean lifespan by 30% and delayed tumor development [9].
In heterozygous p53+/− mice, rapamycin also extended the mean lifespan when treatment started early in life and decreased the incidence of tumors [10].
In Rb1+/− mice, rapamycin extended lifespan and delayed the onset and/or progression of neuroendocrine tumors [11].
In cancer-prone germline PTEN mutant mice, long-term treatment (started at the age of 6 week) with low doses of rapamycin extended lifespan and delayed tumor development [12].
In male mice with prostate epithelium-specific Pten-knockout mouse prostate cancer model, low dose of rapamycin (formulated as Rapatar) was effective in suppressing proliferation of prostate epithelial cells and prevention of prostate cancer. A higher dose activated feedback circuits that decreased the drug’s tumor preventive efficacy [13].
Deletions of transforming growth factor-β receptor I and PTEN in oral mucosa resulted in spontaneous development of HNSCC with 100% penetrance. Rapamycin treatment delayed progression of papilloma and the onset of squamous cell carcinoma in the head and neck region as well as the oral cavity and increased life span and median survival almost two-fold [14].
Apc(Min/+) mice exhibit multiple intestinal neoplasia (MIN), which causes death by 6 months. Short-term treatment with everolimus and rapamycin reduced the number of polyps and their size [15, 16]. Importantly, chronic rapamycin improved survival of Apc(Min/+) mice in a dose-dependent manner [17]. A high dose of enterically targeted rapamycin (eRapa) extended the median lifespan beyond normal median lifespan of wild-type syngeneic mice. Based on these results it was suggested that rapamycin may be effective for cancer prevention in people with familial adenomatous polyposis [17, 18].
Everolimus (RAD001) delays tumor onset and progression in a transgenic mouse model of ovarian cancer [19]. Tumor burden was decreased by 84%. Approximately 30% of everolimus-treated mice developed early ovarian carcinoma confined within the ovary, whereas all placebo-treated mice developed advanced ovarian carcinoma [19]. The authors suggested rapamycin for women at high familial risk of ovarian cancer [19].
Rapamycin delays cancer in normal mice
In numerous studies, rapamycin extended lifespan in normal strains and genetically heterogeneous mice and wild mice (see for references [20]). Cancers are the leading cause of death in most mouse strains used for these studies [21, 22]. Presumably, when death was delayed, then the cause of death (mostly cancer) was delayed too. Some studies investigated this assumption specifically.
In genetically heterogeneous mice, administration of rapamycin started at the age of 9 and 20 months extended lifespan and delayed cancer [21, 22]. It was even speculated that “longevity extension in these mice might reflect inhibition of multiple forms of neoplastic disease” [23]. Alternatively, it was suggested that, by slowing and delaying aging, rapamycin delayed cancer [23, 24]. Similarly, lifelong administration of rapamycin (starting from age of 2 months) increased lifespan and delayed spontaneous cancer in mice [24]. Neff et al. detected several cancers in aged mice, including lymphoma, hepatocellular carcinoma, histiocytic sarcoma, and bronchoalveolar adenocarcinoma, as well as precancerous lesions in male C57BL/6J mice [25]. Rapamycin significantly reduced the proportion of aged mice presenting with cancers and/or precancerous lesions in the 16-month cohort (control, 4 of 10; rapamycin, 0 of 15), but not at the older ages of 25-month and 34-month. The authors concluded that rapamycin delayed cancer and cancer-caused death in male C57BL/6J mice [25].
Cancer prevention in humans
Solid organ (kidney, liver, lung, heart) transplantation is associated with increased risk of cancer and especially of non-melanoma skin cancer.
Starting from 2004, numerous studies demonstrated that rapamycin and everolimus reduced the incidence of various cancers in organ transplant patients [26–34].
For example, Mathew et al. showed that Sirolimus (rapamycin) protected renal transplant patients from skin cancer even when given in combination with CsA (CsA increases incidence of skin cancer) [26].
Kauffman et al. also demonstrated that sirolimus and everolimus treatment is associated with a significantly decreased risk of any de novo malignancy and non-skin solid malignancy [27].
Piselli et al. also found that use of mTOR inhibitors significantly reduced the risk (by 46%) of all cancers combined [30].
mTOR inhibition was associated with a reduced risk of basal cell carcinoma of the skin after kidney transplantation [31]. Rapamycin (sirolimus) treatment was associated with decreased incidence of lymphoproliferative disorder after heart transplantation [34].
Rapamycin and its analogs for cancer therapy
Rapamycin analogs (temsirolimus and everolimus) are approved for various cancers: renal, breast, lung and others.
On May 30, 2007, temsirolimus (Torisel) was approved for the treatment of advanced renal cell carcinoma (RCC) [35, 36]. In comparison with treatment with interferon-a (the best treatment in 2007), temsirolimus further increased overall survival in patients with metastatic renal-cell carcinoma. Median overall survival in the interferon group, the temsirolimus group, and the combination-therapy group were 7.3, 10.9, and 8.4 months, respectively. There was also a statistically significant longer progression-free survival (PFS) time for the temsirolimus arm than for the IFN-alpha: 5.5 months versus 3.1 months [36].
On Mar 30, 2009, everolimus (rapamycin analog) was approved by the FDA as a first treatment for patients with advanced kidney cancer after failure of either sunitinib or sorafenib. Treatment with everolimus prolonged progression-free survival relative to placebo in patients with metastatic renal cell carcinoma that had progressed on other targeted therapies. Median progression-free survival was 4.0 vs. 1.9 months [37].
On July 20, 2012, everolimus was approved by the FDA for use in combination with exemestane to treat women with advanced hormone receptor-positive, HER2-negative breast cancer [38]. At the interim analysis, median progression-free survival was 6.9 months with everolimus plus exemestane and 2.8 months with placebo plus exemestane. Median progression-free survival was 10.6 months and 4.1 months, respectively, according to central assessment. Everolimus combined with an aromatase inhibitor improved progression-free survival in patients with hormone receptor-positive advanced breast cancer previously treated with nonsteroidal aromatase inhibitors [38].
On February 26, 2016, the FDA approved everolimus (Afinitor) for the treatment of adult patients with progressive, well-differentiated, non-functional neuroendocrine tumors (NET) of gastrointestinal or lung origin with unresectable, locally advanced or metastatic disease. Median PFS were 11 months and 3.9 months in the everolimus and placebo arms [39].
Delaying (prevention) vs. treating cancer
To be a highly effective cancer-preventive drug, rapamycin does not need to cure cancer or even be effective in treating advanced, heterogeneous and metastatic tumors, harboring numerous oncogenic mutations and failed previous therapy. To prevent cancer, rapamycin does not need to kill cancer cells (rapamycin does not kill cells) or stop tumor progression (it merely slows it down).
As we discussed earlier, rapamycin slows cell proliferation and tumor progression, thus delaying the onset of cancer in tobacco-carcinogen-treated mice, in both genetically cancer-prone and normal mice (Figure 1). (In cell culture, rapamycin slows cell proliferation 2–10 fold and slows geroconversion to cell senescence 3-fold [40]). Rapamycin figuratively slows down time [41].
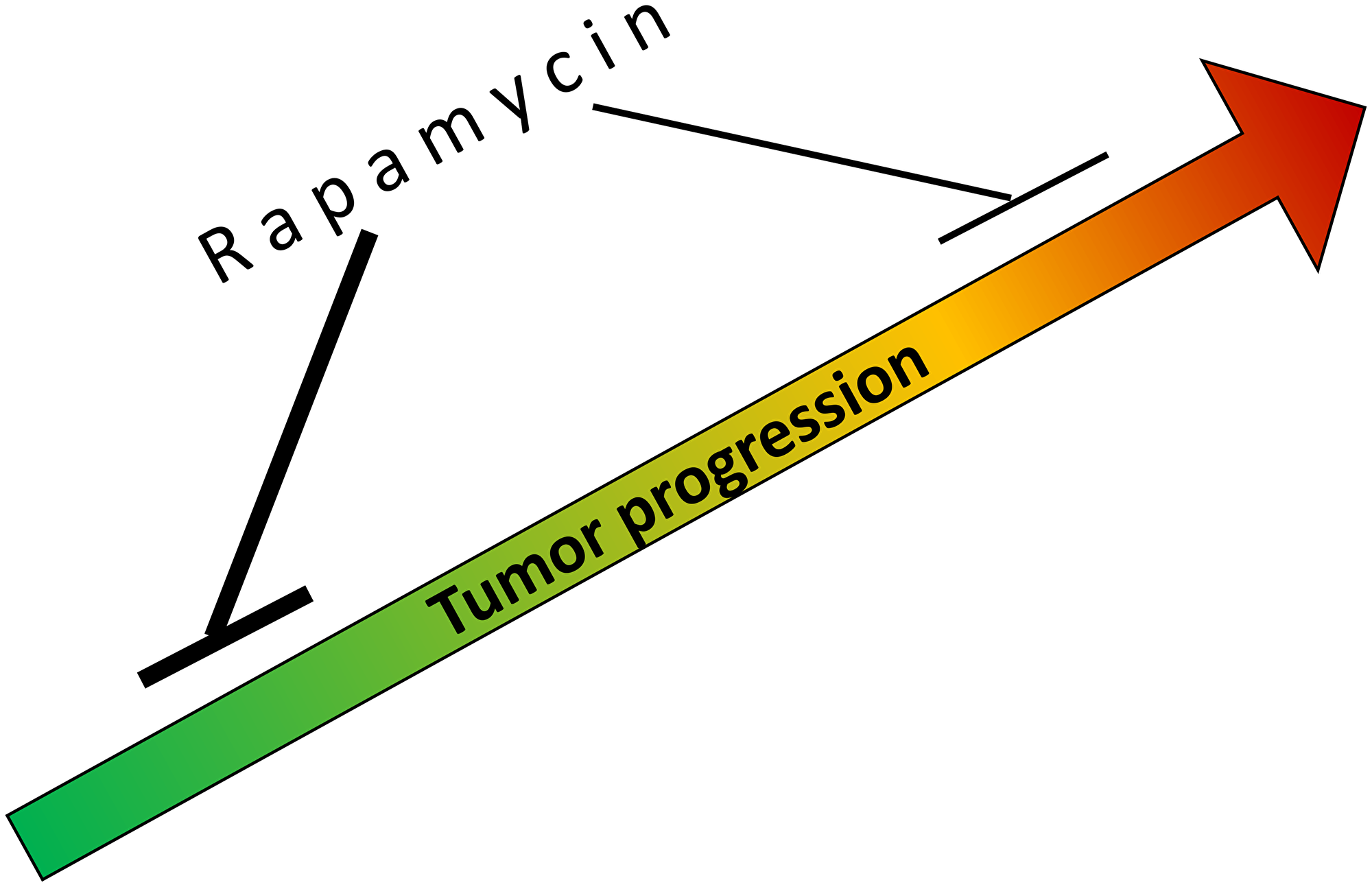
Figure 1: Rapamycin slows tumorigenesis, tumor progression and growth. Rapamycin is more potent at early stage of tumorigenesis (green color) than in advanced and pre-treated cancer (red color).
For cancer prevention, treatment with rapamycin should last many years (in humans). In numerous studies, mice were treated for almost a lifetime. It was not only well-tolerated but also improved healthspan and lifespan (see for references [42, 43]).
If, hypothetically, in humans, a low dose of rapamycin would slow pre-cancer cell proliferation and tumor progression just 2-fold, and a person would be treated for 40 years, then the onset of cancer would be delayed for 20 years. Then this person may die later in life from another age-related disease, for example CVD. Such a significant cancer delay can be viewed as cancer prevention (Figure 2).
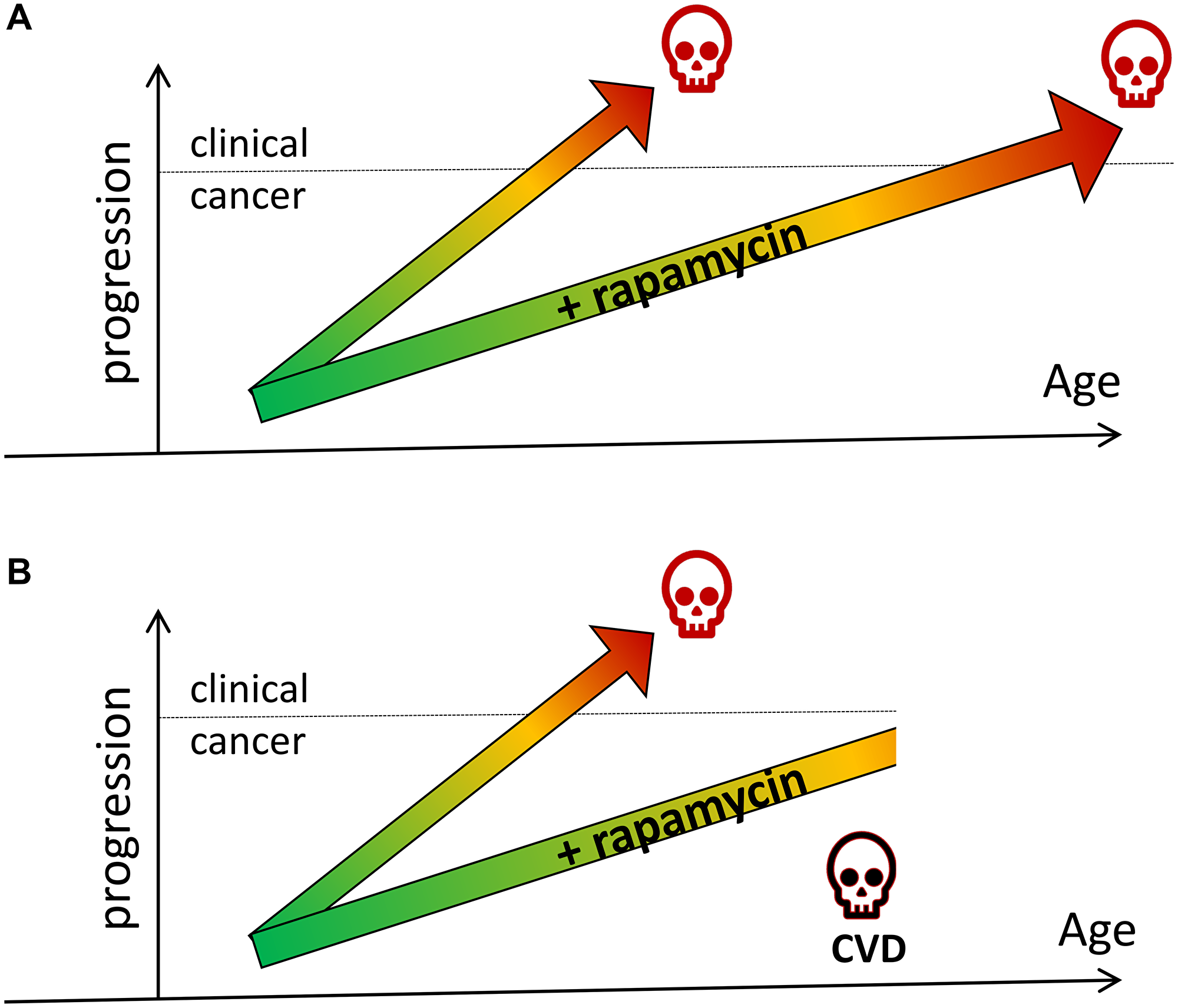
Figure 2: Rapamycin prevents cancer by slowing tumor progression (hypothetical schema). (A) Rapamycin slows tumor progression and delays cancer and death from cancer. (B) Rapamycin slows tumor progression and delays cancer. A person dies from another cause (e.g., cardiovascular disease, CVD) before cancer developed.
In humans, lung cancer may take 20 years to develop, with smoking driving mutations, even 20 years after quitting [44].
In tobacco-carcinogen-induced lung tumorigenesis in mice, rapamycin delays tumors by slowing down tumor progression and cell proliferation. When treatment is started early, rapamycin decreases not only the size of tumors and tumor burden, but also the number of tumors per animal. When treatment is started later (after tumors develop), rapamycin does not decrease tumor multiplicity but slows tumor progression and growth, making them smaller [1–3].
Using a two-stage skin carcinogenesis protocol with DMBA (carcinogen) and TPA (tumor promoter), rapamycin (given topically 30 minutes prior to TPA) exerted a powerful anti-promoting effect, reducing both tumor incidence and tumor multiplicity [45]. Furthermore, rapamycin abolished tumor development when administered prior to both DMBA and TPA [46].
Rapamycin protects HPV-E6/E7 expressing tissues from developing of squamous cell carcinoma [46].
It was concluded that rapamycin is a potent chemopreventive agent [47, 48]. “Rapamycin suspends progression of low-grade cancers, preventing invasive conversion of in situ malignancy, or delaying malignant transformation of established pre-malignant conditions” [48].
Rapamycin slows aging, thus delaying cancer further
Rapamycin can delay cancer not only by targeting precancerous/cancerous cells directly, but also by slowing down organismal aging [49]. It is theoretically predictable that rapamycin delays age-related diseases in part by slowing aging [50]. Certainly, rapamycin extends lifespan in other ways beyond preventing cancer.
Rapamycin delays numerous age-related diseases other than cancer. For example, rapamycin (sirolimus) or its analog (everolimus) attenuate atherosclerosis in rabbits [51], mice [52] and humans [53]. Thus, a prospective randomized trial showed that rapamycin (sirolimus) decreased carotid atherosclerosis in organ-transplant patients [53].
Rapamycin extends lifespan in species that do not have cancer: the C. elegans worm [54], the freshwater cnidarian Hydra [55], and Daphnia magna [56]. Rapamycin also extends the lifespan of yeast [57].
A brief treatment with rapamycin very early in life extends lifespan in mice [56, 58, 59]. There are no pre-cancer cells so early in life, and the treatment with rapamycin is brief. One explanation is that by re-programming development-driven aging, rapamycin retards aging and therefore delays cancer [20].
Rapamycin slows geroconversion (acquisition of the senescent phenotype) in mammalian cells. First, geroconversion may be linked to organism aging [60]. Second, senescent stroma stimulates tumor growth [61–63]. Reversing the aging stromal phenotype with rapamycin prevents carcinoma initiation [61], and rapamycin suppressed the ability of senescent fibroblasts to stimulate tumor growth in mice [64, 65].
Conclusion
In several dozen murine models, rapamycin robustly and reproducibly delays cancer and, in some cases, prevents cancer over a lifetime. It was repeatably proposed that clinical trials in high-risk populations are warranted. A decade-long treatment with rapamycin may be employed to prevent lung cancer in smokers and former smokers. However, decades-long trails are unlikely to be started in the near future. Accidental data on the use of rapamycin (Sirolimus) and everolimus in organ-transplant patients is consistent with their cancer-preventive effects. However, in these patients, their use in combination with other immunosuppressants makes interpretations difficult.
The experience of treatment of cancer patients with mTOR inhibitors is also in agreement with their cancer-preventive effects. Although rapalogs do not cure cancer and infrequently cause remission, they can slow down progression even in advanced tumors, and this activity is sufficient for cancer prevention. Also, long-term treatment with rapamycin slows down aging, a major risk factor for cancer (Figure 3). Notably, delaying cancer is form of cancer prevention. Consider a scenario: rapamycin delays cancer for 2 years, during which this person dies from myocardial infarction (Figure 2). In this case postponing cancer is cancer prevention.
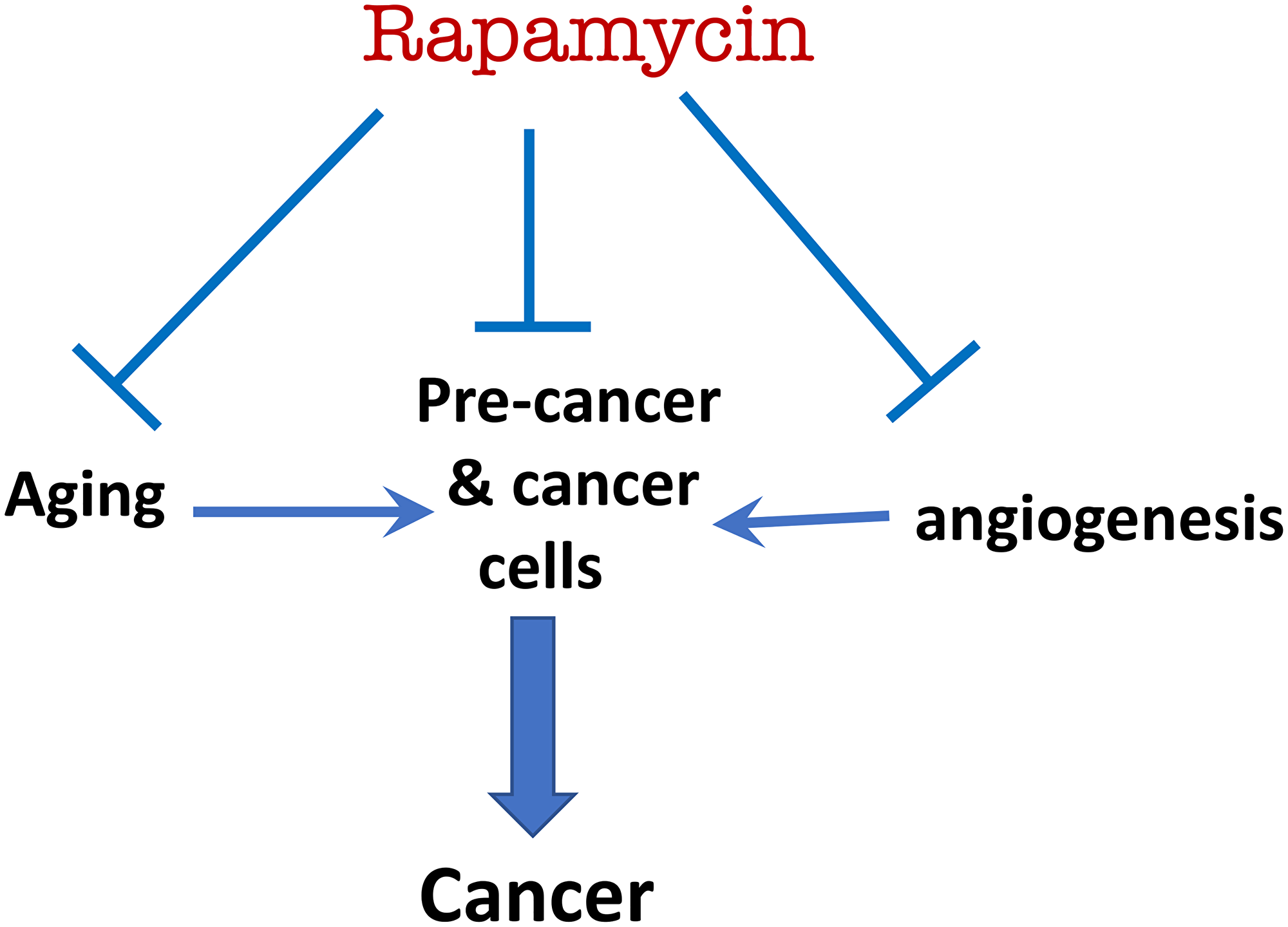
Figure 3: Rapamycin prevents cancer by direct (suppressing pre-cancerous/cancer cell) and indirect mechanisms (suppressing aging and angiogenesis).
Currently, an increasing number of healthy people use rapamycin off-label to slow down aging. Perhaps in ten or twenty years from now, data will accumulate for retrospective analysis of cancer-prevention with rapamycin in humans.
CONFLICTS OF INTEREST
Author has no conflicts of interest to declare.
References
1. Granville CA, Warfel N, Tsurutani J, Hollander MC, Robertson M, Fox SD, Veenstra TD, Issaq HJ, Linnoila RI, Dennis PA. Identification of a highly effective rapamycin schedule that markedly reduces the size, multiplicity, and phenotypic progression of tobacco carcinogen-induced murine lung tumors. Clin Cancer Res. 2007; 13:2281–89. https://doi.org/10.1158/1078-0432.CCR-06-2570. [PubMed].
2. Patlolla JM, Kopelovich L, Qian L, Zhang Y, Kumar G, Madka V, Mohammed A, Biddick L, Sadeghi M, Lightfoot S, Rao CV. Early and delayed intervention with rapamycin prevents NNK-induced lung adenocarcinoma in A/J mice. Oncol Rep. 2015; 34:2925–34. https://doi.org/10.3892/or.2015.4277. [PubMed].
3. Yan Y, Wang Y, Tan Q, Hara Y, Yun TK, Lubet RA, You M. Efficacy of polyphenon E, red ginseng, and rapamycin on benzo(a)pyrene-induced lung tumorigenesis in A/J mice. Neoplasia. 2006; 8:52–58. https://doi.org/10.1593/neo.05652. [PubMed].
4. Kawabata S, Mercado-Matos JR, Hollander MC, Donahue D, Wilson W 3rd, Regales L, Butaney M, Pao W, Wong KK, Jänne PA, Dennis PA. Rapamycin prevents the development and progression of mutant epidermal growth factor receptor lung tumors with the acquired resistance mutation T790M. Cell Rep. 2014; 7:1824–32. https://doi.org/10.1016/j.celrep.2014.05.039. [PubMed].
5. Czerninski R, Amornphimoltham P, Patel V, Molinolo AA, Gutkind JS. Targeting mammalian target of rapamycin by rapamycin prevents tumor progression in an oral-specific chemical carcinogenesis model. Cancer Prev Res (Phila). 2009; 2:27–36. https://doi.org/10.1158/1940-6207.CAPR-08-0147. [PubMed].
6. Dennis PA. Rapamycin for chemoprevention of upper aerodigestive tract cancers. Cancer Prev Res (Phila). 2009; 2:7–9. https://doi.org/10.1158/1940-6207.CAPR-08-0215. [PubMed].
7. Anisimov VN, Zabezhinski MA, Popovich IG, Piskunova TS, Semenchenko AV, Tyndyk ML, Yurova MN, Antoch MP, Blagosklonny MV. Rapamycin extends maximal lifespan in cancer-prone mice. Am J Pathol. 2010; 176:2092–97. https://doi.org/10.2353/ajpath.2010.091050. [PubMed].
8. Popovich IG, Anisimov VN, Zabezhinski MA, Semenchenko AV, Tyndyk ML, Yurova MN, Blagosklonny MV. Lifespan extension and cancer prevention in HER-2/neu transgenic mice treated with low intermittent doses of rapamycin. Cancer Biol Ther. 2014; 15:586–92. https://doi.org/10.4161/cbt.28164. [PubMed].
9. Comas M, Toshkov I, Kuropatwinski KK, Chernova OB, Polinsky A, Blagosklonny MV, Gudkov AV, Antoch MP. New nanoformulation of rapamycin Rapatar extends lifespan in homozygous p53−/− mice by delaying carcinogenesis. Aging (Albany NY). 2012; 4:715–22. https://doi.org/10.18632/aging.100496. [PubMed].
10. Komarova EA, Antoch MP, Novototskaya LR, Chernova OB, Paszkiewicz G, Leontieva OV, Blagosklonny MV, Gudkov AV. Rapamycin extends lifespan and delays tumorigenesis in heterozygous p53+/− mice. Aging (Albany NY). 2012; 4:709–14. https://doi.org/10.18632/aging.100498. [PubMed].
11. Livi CB, Hardman RL, Christy BA, Dodds SG, Jones D, Williams C, Strong R, Bokov A, Javors MA, Ikeno Y, Hubbard G, Hasty P, Sharp ZD. Rapamycin extends life span of Rb1+/− mice by inhibiting neuroendocrine tumors. Aging (Albany NY). 2013; 5:100–10. https://doi.org/10.18632/aging.100533. [PubMed].
12. Tibarewal P, Rathbone V, Constantinou G, Pearce W, Adil M, Varyova Z, Folkes L, Hampson A, Classen GAE, Alves A, Carvalho S, Scudamore CL, Vanhaesebroeck B. Long-term treatment of cancer-prone germline PTEN mutant mice with low-dose rapamycin extends lifespan and delays tumour development. J Pathol. 2022; 258:382–94. https://doi.org/10.1002/path.6009. [PubMed].
13. Antoch MP, Wrobel M, Gillard B, Kuropatwinski KK, Toshkov I, Gleiberman AS, Karasik E, Moser MT, Foster BA, Andrianova EL, Chernova OV, Gudkov AV. Superior cancer preventive efficacy of low versus high dose of mTOR inhibitor in a mouse model of prostate cancer. Oncotarget. 2020; 11:1373–87. https://doi.org/10.18632/oncotarget.27550. [PubMed].
14. Sun ZJ, Zhang L, Hall B, Bian Y, Gutkind JS, Kulkarni AB. Chemopreventive and chemotherapeutic actions of mTOR inhibitor in genetically defined head and neck squamous cell carcinoma mouse model. Clin Cancer Res. 2012; 18:5304–13. https://doi.org/10.1158/1078-0432.CCR-12-1371. [PubMed].
15. Fujishita T, Aoki K, Lane HA, Aoki M, Taketo MM. Inhibition of the mTORC1 pathway suppresses intestinal polyp formation and reduces mortality in ApcDelta716 mice. Proc Natl Acad Sci U S A. 2008; 105:13544–49. https://doi.org/10.1073/pnas.0800041105. [PubMed].
16. Koehl GE, Spitzner M, Ousingsawat J, Schreiber R, Geissler EK, Kunzelmann K. Rapamycin inhibits oncogenic intestinal ion channels and neoplasia in APC(Min/+) mice. Oncogene. 2010; 29:1553–60. https://doi.org/10.1038/onc.2009.435. [PubMed].
17. Hasty P, Livi CB, Dodds SG, Jones D, Strong R, Javors M, Fischer KE, Sloane L, Murthy K, Hubbard G, Sun L, Hurez V, Curiel TJ, Sharp ZD. eRapa restores a normal life span in a FAP mouse model. Cancer Prev Res (Phila). 2014; 7:169–78. https://doi.org/10.1158/1940-6207.CAPR-13-0299. [PubMed].
18. Parihar M, Dodds SG, Hubbard G, Javors MA, Strong R, Hasty P, Sharp ZD. Rapamycin Extends Life Span in Apc(Min/+) Colon Cancer FAP Model. Clin Colorectal Cancer. 2021; 20:e61–70. https://doi.org/10.1016/j.clcc.2020.08.006. [PubMed].
19. Mabuchi S, Altomare DA, Connolly DC, Klein-Szanto A, Litwin S, Hoelzle MK, Hensley HH, Hamilton TC, Testa JR. RAD001 (Everolimus) delays tumor onset and progression in a transgenic mouse model of ovarian cancer. Cancer Res. 2007; 67:2408–13. https://doi.org/10.1158/0008-5472.CAN-06-4490. [PubMed].
20. Blagosklonny MV. Rapamycin treatment early in life reprograms aging: hyperfunction theory and clinical practice. Aging (Albany NY). 2022; 14:8140–49. https://doi.org/10.18632/aging.204354. [PubMed].
21. Harrison DE, Strong R, Sharp ZD, Nelson JF, Astle CM, Flurkey K, Nadon NL, Wilkinson JE, Frenkel K, Carter CS, Pahor M, Javors MA, Fernandez E, Miller RA. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature. 2009; 460:392–95. https://doi.org/10.1038/nature08221. [PubMed].
22. Miller RA, Harrison DE, Astle CM, Baur JA, Boyd AR, de Cabo R, Fernandez E, Flurkey K, Javors MA, Nelson JF, Orihuela CJ, Pletcher S, Sharp ZD, et al. Rapamycin, but not resveratrol or simvastatin, extends life span of genetically heterogeneous mice. J Gerontol A Biol Sci Med Sci. 2011; 66:191–201. https://doi.org/10.1093/gerona/glq178. [PubMed].
23. Wilkinson JE, Burmeister L, Brooks SV, Chan CC, Friedline S, Harrison DE, Hejtmancik JF, Nadon N, Strong R, Wood LK, Woodward MA, Miller RA. Rapamycin slows aging in mice. Aging Cell. 2012; 11:675–82. https://doi.org/10.1111/j.1474-9726.2012.00832.x. [PubMed].
24. Anisimov VN, Zabezhinski MA, Popovich IG, Piskunova TS, Semenchenko AV, Tyndyk ML, Yurova MN, Rosenfeld SV, Blagosklonny MV. Rapamycin increases lifespan and inhibits spontaneous tumorigenesis in inbred female mice. Cell Cycle. 2011; 10:4230–36. https://doi.org/10.4161/cc.10.24.18486. [PubMed].
25. Neff F, Flores-Dominguez D, Ryan DP, Horsch M, Schröder S, Adler T, Afonso LC, Aguilar-Pimentel JA, Becker L, Garrett L, Hans W, Hettich MM, Holtmeier R, et al. Rapamycin extends murine lifespan but has limited effects on aging. J Clin Invest. 2013; 123:3272–91. https://doi.org/10.1172/JCI67674. [PubMed].
26. Mathew T, Kreis H, Friend P. Two-year incidence of malignancy in sirolimus-treated renal transplant recipients: results from five multicenter studies. Clin Transplant. 2004; 18:446–49. https://doi.org/10.1111/j.1399-0012.2004.00188.x. [PubMed].
27. Kauffman HM, Cherikh WS, Cheng Y, Hanto DW, Kahan BD. Maintenance immunosuppression with target-of-rapamycin inhibitors is associated with a reduced incidence of de novo malignancies. Transplantation. 2005; 80:883–89. https://doi.org/10.1097/01.tp.0000184006.43152.8d. [PubMed].
28. Campistol JM, Eris J, Oberbauer R, Friend P, Hutchison B, Morales JM, Claesson K, Stallone G, Russ G, Rostaing L, Kreis H, Burke JT, Brault Y, et al. Sirolimus therapy after early cyclosporine withdrawal reduces the risk for cancer in adult renal transplantation. J Am Soc Nephrol. 2006; 17:581–89. https://doi.org/10.1681/ASN.2005090993. [PubMed].
29. Euvrard S, Morelon E, Rostaing L, Goffin E, Brocard A, Tromme I, Broeders N, del Marmol V, Chatelet V, Dompmartin A, Kessler M, Serra AL, Hofbauer GF, et al. Sirolimus and secondary skin-cancer prevention in kidney transplantation. N Engl J Med. 2012; 367:329–39. https://doi.org/10.1056/NEJMoa1204166. [PubMed].
30. Piselli P, Serraino D, Segoloni GP, Sandrini S, Piredda GB, Scolari MP, Rigotti P, Busnach G, Messa P, Donati D, Schena FP, Maresca MC, Tisone G, et al. Risk of de novo cancers after transplantation: results from a cohort of 7217 kidney transplant recipients, Italy 1997-2009. Eur J Cancer. 2013; 49:336–44. https://doi.org/10.1016/j.ejca.2012.09.013. [PubMed].
31. Opelz G, Unterrainer C, Süsal C, Döhler B. Immunosuppression with mammalian target of rapamycin inhibitor and incidence of post-transplant cancer in kidney transplant recipients. Nephrol Dial Transplant. 2016; 31:1360–67. https://doi.org/10.1093/ndt/gfw088. [PubMed].
32. Dantal J, Morelon E, Rostaing L, Goffin E, Brocard A, Tromme I, Broeders N, Del Marmol V, Chatelet V, Dompmartin A, Kessler M, Serra A, Hofbauer GFL, et al. Sirolimus for Secondary Prevention of Skin Cancer in Kidney Transplant Recipients: 5-Year Results. J Clin Oncol. 2018; 36:2612–20. https://doi.org/10.1200/JCO.2017.76.6691. [PubMed].
33. Murray SL, Daly FE, O’Kelly P, O’Leary E, Deady S, O’Neill JP, Dudley A, Rutledge NR, McCormick A, Houlihan DD, Williams Y, Morris PG, Ni Raghallaigh S, et al. The impact of switching to mTOR inhibitor-based immunosuppression on long-term non-melanoma skin cancer incidence and renal function in kidney and liver transplant recipients. Ren Fail. 2020; 42:607–12. https://doi.org/10.1080/0886022X.2020.1785499. [PubMed].
34. Asleh R, Vucicevic D, Petterson TM, Kremers WK, Pereira NL, Daly RC, Edwards BS, Steidley DE, Scott RL, Kushwaha SS. Sirolimus-Based Immunosuppression Is Associated with Decreased Incidence of Post-Transplant Lymphoproliferative Disorder after Heart Transplantation: A Double-Center Study. J Clin Med. 2022; 11:322. https://doi.org/10.3390/jcm11020322. [PubMed].
35. Kwitkowski VE, Prowell TM, Ibrahim A, Farrell AT, Justice R, Mitchell SS, Sridhara R, Pazdur R. FDA approval summary: temsirolimus as treatment for advanced renal cell carcinoma. Oncologist. 2010; 15:428–35. https://doi.org/10.1634/theoncologist.2009-0178. [PubMed].
36. Hudes G, Carducci M, Tomczak P, Dutcher J, Figlin R, Kapoor A, Staroslawska E, Sosman J, McDermott D, Bodrogi I, Kovacevic Z, Lesovoy V, Schmidt-Wolf IG, et al, and Global ARCC Trial. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med. 2007; 356:2271–81. https://doi.org/10.1056/NEJMoa066838. [PubMed].
37. Motzer RJ, Escudier B, Oudard S, Hutson TE, Porta C, Bracarda S, Grünwald V, Thompson JA, Figlin RA, Hollaender N, Urbanowitz G, Berg WJ, Kay A, et al. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet. 2008; 372:449–56. https://doi.org/10.1016/S0140-6736(08)61039-9. [PubMed].
38. Baselga J, Campone M, Piccart M, Burris HA 3rd, Rugo HS, Sahmoud T, Noguchi S, Gnant M, Pritchard KI, Lebrun F, Beck JT, Ito Y, Yardley D, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012; 366:520–29. https://doi.org/10.1056/NEJMoa1109653. [PubMed].
39. Yao JC, Fazio N, Singh S, Buzzoni R, Carnaghi C, Wolin E, Tomasek J, Raderer M, Lahner H, Voi M, Pacaud LB, Rouyrre N, Sachs C, et al. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study. Lancet. 2016; 387:968–77. https://doi.org/10.1016/S0140-6736(15)00817-X. [PubMed].
40. Demidenko ZN, Zubova SG, Bukreeva EI, Pospelov VA, Pospelova TV, Blagosklonny MV. Rapamycin decelerates cellular senescence. Cell Cycle. 2009; 8:1888–95. https://doi.org/10.4161/cc.8.12.8606. [PubMed].
41. Blagosklonny MV. Does rapamycin slow down time? Oncotarget. 2018; 9:30210–12. https://doi.org/10.18632/oncotarget.25788. [PubMed].
42. Johnson SC, Kaeberlein M. Rapamycin in aging and disease: maximizing efficacy while minimizing side effects. Oncotarget. 2016; 7:44876–78. https://doi.org/10.18632/oncotarget.10381. [PubMed].
43. Blagosklonny MV. Rapamycin for longevity: opinion article. Aging (Albany NY). 2019; 11:8048–67. https://doi.org/10.18632/aging.102355. [PubMed].
44. de Bruin EC, McGranahan N, Mitter R, Salm M, Wedge DC, Yates L, Jamal-Hanjani M, Shafi S, Murugaesu N, Rowan AJ, Grönroos E, Muhammad MA, Horswell S, et al. Spatial and temporal diversity in genomic instability processes defines lung cancer evolution. Science. 2014; 346:251–56. https://doi.org/10.1126/science.1253462. [PubMed].
45. Checkley LA, Rho O, Moore T, Hursting S, DiGiovanni J. Rapamycin is a potent inhibitor of skin tumor promotion by 12-O-tetradecanoylphorbol-13-acetate. Cancer Prev Res (Phila). 2011; 4:1011–20. https://doi.org/10.1158/1940-6207.CAPR-10-0375. [PubMed].
46. Callejas-Valera JL, Iglesias-Bartolome R, Amornphimoltham P, Palacios-Garcia J, Martin D, Califano JA, Molinolo AA, Gutkind JS. mTOR inhibition prevents rapid-onset of carcinogen-induced malignancies in a novel inducible HPV-16 E6/E7 mouse model. Carcinogenesis. 2016; 37:1014–25. https://doi.org/10.1093/carcin/bgw086. [PubMed].
47. Kopelovich L, Fay JR, Sigman CC, Crowell JA. The mammalian target of rapamycin pathway as a potential target for cancer chemoprevention. Cancer Epidemiol Biomarkers Prev. 2007; 16:1330–40. https://doi.org/10.1158/1055-9965.EPI-07-0045. [PubMed].
48. O’Shea AE, Valdera FA, Ensley D, Smolinsky TR, Cindass JL, Kemp Bohan PM, Hickerson AT, Carpenter EL, McCarthy PM, Adams AM, Vreeland TJ, Clifton GT, Peoples GE. Immunologic and dose dependent effects of rapamycin and its evolving role in chemoprevention. Clin Immunol. 2022; 245:109095. https://doi.org/10.1016/j.clim.2022.109095. [PubMed].
49. Blagosklonny MV. Prevention of cancer by inhibiting aging. Cancer Biol Ther. 2008; 7:1520–24. https://doi.org/10.4161/cbt.7.10.6663. [PubMed].
50. Blagosklonny MV. Aging and immortality: quasi-programmed senescence and its pharmacologic inhibition. Cell Cycle. 2006; 5:2087–102. https://doi.org/10.4161/cc.5.18.3288. [PubMed].
51. Chen WQ, Zhong L, Zhang L, Ji XP, Zhang M, Zhao YX, Zhang C, Zhang Y. Oral rapamycin attenuates inflammation and enhances stability of atherosclerotic plaques in rabbits independent of serum lipid levels. Br J Pharmacol. 2009; 156:941–51. https://doi.org/10.1111/j.1476-5381.2008.00102.x. [PubMed].
52. Mueller MA, Beutner F, Teupser D, Ceglarek U, Thiery J. Prevention of atherosclerosis by the mTOR inhibitor everolimus in LDLR−/− mice despite severe hypercholesterolemia. Atherosclerosis. 2008; 198:39–48. https://doi.org/10.1016/j.atherosclerosis.2007.09.019. [PubMed].
53. Silva AL, Fusco DR, Nga HS, Takase HM, Bravin AM, Contti MM, Valiatti MF, de Andrade LGM. Effect of sirolimus on carotid atherosclerosis in kidney transplant recipients: data derived from a prospective randomized controlled trial. Clin Kidney J. 2018; 11:846–52. https://doi.org/10.1093/ckj/sfy041. [PubMed].
54. Robida-Stubbs S, Glover-Cutter K, Lamming DW, Mizunuma M, Narasimhan SD, Neumann-Haefelin E, Sabatini DM, Blackwell TK. TOR signaling and rapamycin influence longevity by regulating SKN-1/Nrf and DAF-16/FoxO. Cell Metab. 2012; 15:713–24. https://doi.org/10.1016/j.cmet.2012.04.007. [PubMed].
55. Tomczyk S, Suknovic N, Schenkelaars Q, Wenger Y, Ekundayo K, Buzgariu W, Bauer C, Fischer K, Austad S, Galliot B. Deficient autophagy in epithelial stem cells drives aging in the freshwater cnidarian Hydra. Development. 2020; 147:dev177840. https://doi.org/10.1242/dev.177840. [PubMed].
56. Shindyapina AV, Cho Y, Kaya A, Tyshkovskiy A, Castro JP, Deik A, Gordevicius J, Poganik JR, Clish CB, Horvath S, Peshkin L, Gladyshev VN. Rapamycin treatment during development extends life span and health span of male mice and Daphnia magna. Sci Adv. 2022; 8:eabo5482. https://doi.org/10.1126/sciadv.abo5482. [PubMed].
57. Powers RW 3rd, Kaeberlein M, Caldwell SD, Kennedy BK, Fields S. Extension of chronological life span in yeast by decreased TOR pathway signaling. Genes Dev. 2006; 20:174–84. https://doi.org/10.1101/gad.1381406. [PubMed].
58. Aiello G, Sabino C, Pernici D, Audano M, Antonica F, Gianesello M, Ballabio C, Quattrone A, Mitro N, Romanel A, Soldano A, Tiberi L. Transient rapamycin treatment during developmental stage extends lifespan in Mus musculus and Drosophila melanogaster. EMBO Rep. 2022; 23:e55299. https://doi.org/10.15252/embr.202255299. [PubMed].
59. Juricic P LY, Leech T, Drews LF, Paulitz J, Lu J, Nespital T, Azami S, Regan JC, Funk E, Fröhlich J, Grönke S, Partridge L. Long-lasting geroprotection from brief rapamycin treatment in early adulthood by persistently increased intestinal autophagy. Nat Aging. 2022; 2:824–36. https://doi.org/10.1038/s43587-022-00278-w.
60. Blagosklonny MV. Cell senescence, rapamycin and hyperfunction theory of aging. Cell Cycle. 2022; 21:1456–67. https://doi.org/10.1080/15384101.2022.2054636. [PubMed].
61. Lewis DA, Travers JB, Machado C, Somani AK, Spandau DF. Reversing the aging stromal phenotype prevents carcinoma initiation. Aging (Albany NY). 2011; 3:407–16. https://doi.org/10.18632/aging.100318. [PubMed].
62. Marongiu F, Serra MP, Doratiotto S, Sini M, Fanti M, Cadoni E, Serra M, Laconi E. Aging promotes neoplastic disease through effects on the tissue microenvironment. Aging (Albany NY). 2016; 8:3390–99. https://doi.org/10.18632/aging.101128. [PubMed].
63. Smit MA, Peeper DS. Epithelial-mesenchymal transition and senescence: two cancer-related processes are crossing paths. Aging (Albany NY). 2010; 2:735–41. https://doi.org/10.18632/aging.100209. [PubMed].
64. Laberge RM, Sun Y, Orjalo AV, Patil CK, Freund A, Zhou L, Curran SC, Davalos AR, Wilson-Edell KA, Liu S, Limbad C, Demaria M, Li P, et al. MTOR regulates the pro-tumorigenic senescence-associated secretory phenotype by promoting IL1A translation. Nat Cell Biol. 2015; 17:1049–61. https://doi.org/10.1038/ncb3195. [PubMed].
65. Mercier I, Camacho J, Titchen K, Gonzales DM, Quann K, Bryant KG, Molchansky A, Milliman JN, Whitaker-Menezes D, Sotgia F, Jasmin JF, Schwarting R, Pestell RG, et al. Caveolin-1 and accelerated host aging in the breast tumor microenvironment: chemoprevention with rapamycin, an mTOR inhibitor and anti-aging drug. Am J Pathol. 2012; 181:278–93. https://doi.org/10.1016/j.ajpath.2012.03.017. [PubMed].