
Introduction
Colorectal cancer (CRC) is the second most common cause of cancer death in the United States and rectal cancer comprise 44% of CRC [1]. Standard treatment for locally advanced rectal cancer (LARC) consists in neoadjuvant (preoperative) chemoradiotherapy (nCRT) combined with surgery [2], with the aim to reduce local recurrence and to increase the sphincter preservation rate. However, only a minority of patients achieve a complete response after nCRT treatment [3].
Antitumor activity of Radiation therapy (RT), and chemoradiotherapy (CRT), is thought to be partly due to the activation of tumor-specific adaptive immunity [4, 5]. Upon radiation, there is upregulation of up- major histocompatibility complex molecules [6, 7] and release of tumor associated antigens [8] which in turns leads to release of inflammatory cytokines, especially interferon-γ (IFN-γ) from tumor and immune cells [9]. As results, the immunologic equilibrium of the tumor microenvironment (TME) is shifted towards a more immunogenic one [10, 11]. However, activation of immune suppressive pathways, including PD-1/PD-L1 pathway also happens, limiting the potential beneficial effects of this increased immunogenicity [12–16].
Recent preclinical studies showed that combining PD-1/PD-L1 inhibitors with CRT improved both local and systemic tumor control in animal models [17–20]. The synergistic effects of CRT and PD-1/PD-L1 immunotherapy has been supported by several retrospective analyses in different cancer types, including esophageal cancer, bladder cancer, and lung cancer also support [14, 21, 22]. However, the role of nCRT to interact synergistically with for immune checkpoint inhibitor treatment to improve tumor control in rectal cancer remain uncertain. Additionally, controversies exist regarding the prognostic value of PD-L1 expression in rectal cancer. The aim of this study was to evaluate nCRT-induced alterations in the TME of post-CRT resected specimens of rectal cancer, with a particular focus on PD-L1 expression and the density of CD8+ tumor-infiltrating lymphocytes (TILs). We used rectal cancer cases where nCRT was not delivered as control cases. We also examined the densities of CD8+TILs and PD-L1 expression on the basis of their localization. Finally, we aimed to analyze mucin expression within the tumor, as mucins might play an important role in inflammation and immune responses.
Results
Clinicopathologic characteristics
From 2008 and 2014, 79 patients with rectal adenocarcinoma were included in this analysis who were treated with surgery with or without nCRT at the Johns Hopkins Hospital and had resection specimens available for analysis. Baseline patient and tumor-related characteristics of the study group are given in Table 1. The median age was 52 years (range, 21–88 years), with majority of male patients (70%) were men. Most patients (58%) had pT3 tumors. At time of diagnosis 50 patients (63%) had node-positive disease and 41 patients (52%) had pathologically positive nodal status.
Table 1: Clinicopathologic characteristics
| Characteristic | n (%) |
|---|---|
| Age (y) | |
| Median (range) | 52 (21–88) |
| <52 | 38 (48) |
| ≥52 | 41 (52) |
| Sex | |
| Male | 55 (70) |
| Female | 24 (30) |
| Tumor location | |
| Rectum | 62 (78) |
| Recto-sigmoid | 17 (21) |
| Unknown | 1 (1) |
| Clinical Stage at Diagnosis | |
| Stage 1 | 7 (9) |
| Stage 2 | 9 (11) |
| Stage 3 | 50 (63) |
| Stage 4 | 13 (17) |
| Tumor grade (resected) | |
| Well to moderately differentiated | 60 (76) |
| Poorly- differentiated | 9 (11) |
| NE (no residual tumor) | 10 (13) |
| pT stage | |
| T0 | 3 (4) |
| T1 | 3 (4) |
| T2 | 17 (21) |
| T3 | 46 (58) |
| T4 | 7 (9) |
| NA | 3 (4) |
| pN Stage | |
| Nx | 3 (4) |
| N0 | 35 (44) |
| N1 | 25 (32) |
| N2 | 16 (20) |
| N3 | 0 (0) |
| Downstage of after CRT, n = 61 | |
| Yes | 25 (41) |
| No | 31 (51) |
| NE | 5 (8) |
| Lymphatic Invasion | |
| Yes | 24 (30) |
| No | 32 (40) |
| Unknown | 18 (23) |
| Vascular Invasion | |
| Yes | 7 (9) |
| No | 57 (72) |
| Unknown | 15 (19) |
| Microsatellite instability | |
| MSS/MSI-Low | 42 (53) |
| MSI-H | 1 (1) |
| Unknown | 36 (46) |
Significant differences were found between the two groups in terms of clinical stage at the time of diagnosis: patients in the nCRT arm had more advanced stage at the time of diagnosis, with 50 patients (92.6%) diagnosed with stage 3 or 4 disease and 4 (4,2%) with stage 1 or 2 cancer. In the groups that did not receive nCRT (N = 17), 7 patients had stage 3 or 4 disease, while 10 (58.8%) were diagnosed with stage 1 or 2 cancer (p = 0) (Table 2). Other clinical features were assessed for imbalance, and arms were well matched.
Table 2: Stage at the time of diagnosis, PD-L1, CD8+TILs and mucin expression by radiation therapy
| NO nCRT | nCRT | p-Value | |
|---|---|---|---|
| Stage at Diagnosis, n (%) | N = 17 | N = 54 | 0 |
| 1, 2 | 10 (58.8) | 4 (7.4) | |
| 3,4 | 7 (41.2) | 50 (92.6) | |
| PD-L1 TC, n (%) | N = 17 | N = 61 | 0.329 |
| neg | 17 (100) | 55 (90.2) | |
| pos | 0 (0) | 6 (9.8) | |
| PD-L1 IF | N = 17 | N = 61 | 0.942 |
| median | 25 | 10 | |
| mean | 30.9 | 30.2 | |
| PD-L1 TS, n (%) | N = 17 | N = 61 | 0.559 |
| Neg | 6 (35.3) | 17 (27.9) | |
| Pos | 11 (64.7) | 44 (72.1) | |
| PD-L1 Interface, n (%) | N = 17 | N = 61 | 0.558 |
| Neg | 4 (23.5) | 21 (34.4) | |
| Pos | 13 (76.5) | 40 (65.6) | |
| CD8+ Intratumor, | N = 15 | N = 49 | 0.793 |
| Median | 105.8 | 99.5 | |
| Mean | 229.3 | 207.1 | |
| CD8 inner interface, N | N = 9 | N = 29 | 0.47 |
| Median | 131 | 173.5 | |
| Mean | 348.8 | 220.9 | |
| CD8 outer interface, N | N = 7 | N = 28 | 0.2156 |
| Median | 330 | 202 | |
| Mean | 634 | 283.3 | |
| Mucin ratio | N = 2 | N = 9 | 0.02 |
| Median | 0 | 0.3 | |
| Mean | 0 | 0.2 |
nCRT consisted of fluoropyrimidines- based chemotherapy administered concomitant with RT. Radiotherapy consisted of 50.4 Gy radiation in 28 fractions delivered to the primary tumor and the mesorectal, pre-sacral and internal iliac lymph nodes. The median time interval between n CRT and surgery (total mesorectal excision) was 63.3 days. Pathologic downstaging was observed in 25 patients (41%). Mismatch repair status was available for 43 patients (53%) and only one patient was found to have microsatellite unstable diseases (1%).
PD-L1, CD8+ TILs and mucin expression with and without neoadjuvant radiochemotherapy
PD-L1 expression in rectal adenocarcinoma cells and immune cells was evaluated in the surgical specimens of the two patient cohorts: patients who did receive nCRT before surgery (n = 61) and patients who had surgery without nCRT (n = 17). One patient received only chemotherapy and not radiation before surgery and was excluded from analysis. PD-L1 expression was studied according to spatial localization: tumor cells (TC), tumor stroma (TS) and invasive front (IF). Figure 1A–1C shows the representative slide views. Considering the overall population, both the maximum staining intensity and the proportion of PD-L1-expressing cells were more pronounced in the TS (70.5%) and IF (67.9%).
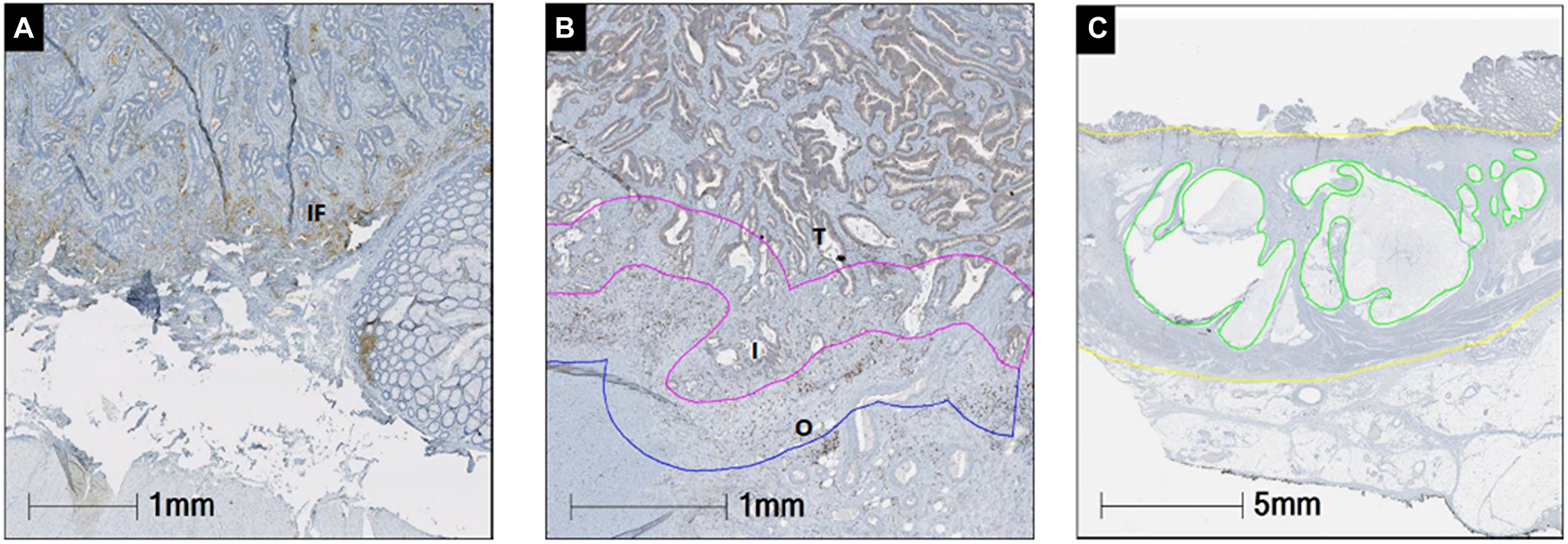
Figure 1: Representative images of PD-L1 (A), CD8 (B) and mucin (C) and staining. The percentage of PD-L1 membranous expression was manually counted in tumor cells tumor stroma and invasive front. The prevalence of CD8+ TILs was recorded in tumor, interface tumor side (inner), interface background rectal side (outer). Mucin expression (green) was determined as percentage of the mucin area in the whole tumor area mass (yellow). Abbreviations: I: inner; IF: invasive front; O: outer front; T: tumor.
PD-L1 expression on TCs was identified in only 7.7 % (6/79) of specimens. All 6 cases had received nCRT (p = 0.33) (Table 2). Generalized estimating equation (GEE) was used to account for the repeated measures obtained from the same patient. The results of GEE are consistent with what we found using Chi-square test, except for PD-L1: comparisons between the patient groups with and without nCRT showed a significant difference in PD-L1+ rectal cancer cells (p = 0) (Table 3).
Table 3: PD-L1 expression by radiation therapy using GEE (generalized estimating equations) analysis
| NO nCRT (N = 17) | nCRT (N = 61) | p-Value | |
|---|---|---|---|
| PD-L1 TC, n (%) | 0* | ||
| Neg | 17 (100) | 55 (90.2) | |
| Pos | 0 (0) | 6 (9.8) | |
| PD-L1 IF | 0.94 | ||
| Median | 25 | 10 | |
| Mean | 30.9 | 30.2 | |
| PD-L1 TS, n (%) | 0.56 | ||
| NEG | 6 (35.3) | 17 (27.9) | |
| Pos | 11 (64.7) | 44 (72.1) | |
CD8+ tumor-infiltrating T cells, were evaluated by IHC staining within the tumor and the interface (inner and outer interface). No significant differences in CD8+T cells density by location (tumor or interface) were observed in the two cohorts of patients (Table 2).
Differences in CD8+T cells infiltrated between surgery-alone and nCRT cases were observed, although not statistically significant: the median density (cells/mm2) of CD8+ TILs was 319.66 (range, 20.76–978.08) in the surgery alone group and 787.05 (range, 101.39–2100.85) in the nCRT, respectively.
Mucin ratio, defined as mucin area versus total tumor area (Figure 1C), was evaluable in a total of 11 specimens, and was significantly higher in the cohort of patient who received nCRT (median 0.3 versus 0, p = 0.02) (Table 2).
Independent prognostic risk factors
Among 79 patients who underwent curative surgery, 21 (31.8%) had postoperative recurrences. Primary recurrence was found in, lung, liver, lymph node, and local sites for 7, 6, 5, and 5 patients, respectively. The majority of these patients received further treatment but, due the retrospective nature of this study we did not have access to full data regarding post recurrence treatment. As post recurrence therapy could have impacted on overall survival rates., we decided to focus our analysis on relapse free survival (RFS).
In the univariate analysis of RFS, the following parameters were associated with patients’ outcome: pathological stage (and not clinical stage at diagnosis) (hazard ratio (HR) = 2.31, 95% CI:1.02, 5.20, p = 0.0435), margins status at the time of resection (HR = 5.63; 95% CI: 1.87,16.96, p = 0.0021) and post nCRT neutrophil to lymphocyte ratio (NLR) (HR = 1.04, 95% CI: 1.00, 1.08, p = 0.0348).
On the basis of the results obtained in the univariable analyses, pathological stage, margins status and post CRT NLR were included in the multivariable Cox regression model for RFS. Margins status and post nCRT NLR confirmed the statistically significant association with survival. Neither PD-L1 expression nor CD8+ TILs density was significant predictive factors (Table 4).
Table 4: Univariate and multivariate analysis of clinicopathologic parameters on RFS
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| All patients (N = 79) | ||||||
| PD-L1 TS (positive vs. negative) | 1.15 | 0.53–2.50 | 0.7238 | NA | NA | NA |
| PD-L1 IF (positive vs. negative) | 0.92 | 0.43–1.95 | 0.8192 | NA | NA | NA |
| CD8-interface (high vs. low) | 1.00 | 1.00–1.00 | 0.1785 | NA | NA | NA |
| Pre CRT NLR (high vs. low) | 0.80 | 0.56–1.12 | 0.1966 | NA | NA | NA |
| Post CRT NLR (high vs. low) | 1.04 | 1.00–1.08 | 0.0348 | 1.04 | 1.00–1.09 | 0.0415 |
| Age (≥52 vs. <52) | 1.23 | 0.60–2.51 | 0.5780 | NA | NA | NA |
| Sex (male vs female) | 0.57 | 0.28–1.18 | 0.1290 | NA | NA | NA |
| Margins (positive vs negative) | 5.63 | 1.87–16.96 | 0.0021 | 13.59 | 2.32–79.57 | 0.0038 |
| Stage at diagnosis (3,4 vs. 1–2) | 2.19 | 0.28–17.35 | 0.456 | 1.04 | 0.00-Inf | 1.0000 |
| Interaction between Stage at diagnosis and Radiation | NA | NA | NA | NA | 0.85-Inf | 1.0000 |
| Pathological stage (3,4 vs. 0–2) | 2.31 | 1.02–5.20 | 0.0435 | 1.47 | 0.49–4.40 | 0.4862 |
DISCUSSION
Within the recent years, immunotherapy with immune checkpoint inhibitors (ICIs) has revolutionized the field of oncology [23–26]. However, despite the current success of immunotherapy, not all patients respond similarly and the benefits of this approach have been limited in non-immunogenic, “cold, tumors [27]. This natural resistance is in part due to various immunosuppressive factors present in the TME that prevent infiltration of CD8+ T cells, unlike in immunogenic tumors. Therefore, to unleash an optimal antitumor immune response, combinatorial approaches that combine immune checkpoints with other modalities, have been investigated and developed [22, 28]. Salient to our work, studies have investigated the immunomodulatory impact of radiation therapy and its ability to alter the immunogenicity of the TME and increase T cell infiltration and antigen processing and presentation [19, 29]. This has paved the way for investigation of combinatorial approaches with immune checkpoint inhibition in different cancer types, and numerous reports have shown clinical benefit of the combination of RT and PD-1/PD-L1 blockade in melanoma [30], non-small cell lung cancer (NSCLC) [31], Hodgkin lymphoma [32], renal cell carcinoma (RCC) [33].
Durable responses, including in non-radiated areas with the use of low dose radiation in combination with ICI therapy, have also been reported in microsatellite stable (MSS) CRC [34].
However, the clinical significance of PD-1(L)1 pathway upregulation in rectal cancers remains controversial and it is important to acknowledge that PD-L1 is an imperfect biomarker and that different analyses have highlighted how immunohistochemistry staining cut off differ among studies and how PD-L1 expression is not uniform, which could induce possible biased results related to sampling [35–38]. However, our findings are consistent with other studies in rectal cancer patients looking at matched pre and post radiation specimens [39–41]. In our analysis, tumor cell PD-L1 expression was overall low (7.7%), which is in line with results presented by other groups [39, 41, 42]. For instance, Hecht et al. reported that the percentage of tumor PD-L1 high expression was 2.1% in rectal cancer [39]. Lee et al. reported that high tumor PD-L1 expression was identified in only 4.8% of the total cohort of rectal cancer [43].
We showed that nCRT exposure was associated with a higher PD-L1 expression in tumor cells as compared to non-nCRT cases. Moreover, although not significant, we observed also an increased overall PD-L1 expression on TS and IF in the nCRT group as compared to patients who had surgery only. CD8+ T cell and their spatial distribution remains a crucial component in eliciting an antitumor immune response [40–42]. Paired analysis of PD-L1 expression and density of CD8+ TILs showed that CRT induce an immunologic shift toward increases in both PD-L1 expression and density of CD8+TILs in rectal cancer patients [43–46]. For this purpose, we developed an IHC approach incorporating both an image analysis approach and a manual approach to quantitate the density of each immune cells’ subsets in different areas of the TME. We applied this approach in this study and were able to assess CD8-TILs in the whole tumor, and in the tumor margins (tumor interface, inner and outer interface). Although no statistically significant differences between the two cohorts were observed, there was a trend toward higher CD8+ cell density in the nCRT cohorts compared to surgery-alone cases, suggesting a different immunological milieu between the two cohorts based on radiation exposure.
Mucins are a class of glycoproteins that play a role in suppressing inflammation abnormal expression of mucins has been observed in various adenocarcinomas, including CRC [47, 48]. Studies have supported mucins’ role in regulating T cells function and modulating immune response, for instance through interaction with intercellular adhesion molecule-1 (ICAM-1) and other inhibitory receptors on T-cells, leading to impaired antigen recognition, [49–51]. Cancer cells can exploit the immune-modulatory ability of mucins to evade immune surveillance [52–55]. We observed a higher mucin concentration in patients who underwent nCRT, as compared to the surgery alone cases. These findings suggest a novel way through which radiation therapy can impact the immune TME towards a more immunosuppressive phenotype.
Finally, our results for both univariate and multivariate analyses indicated that higher post-treatment NLR was an independent predictor of relapse free survival (RFS). Other studies in rectal cancer have focused on pretreatment NLR and showed that elevated higher NLR was associated with higher T stage, inferior RFS, and poorer pathological response to nCRT. These studies have not looked at post treatment NLR. Thus, our findings suggest a possible prognostic role of posttreatment NLR and might help personalizing adjuvant treatments, for instance by intensifying systemic treatment in patients with an elevated NLR after nCRT.
Our study has few limitations that need to be acknowledged. First, we did not have access to pretreatment tumor tissues and the analysis include a limited number of patients, which is a consequence of the retrospective design. It is also important to note that in our study, patients in the nCRT group had a more advanced tumor stage at the time of diagnosis, as compared to the group who received surgery upfront. A possible association between PD-L1 expression and higher TNM stage at diagnosis (regardless of radiation exposure) cannot be excluded, as it has been showed in other tumor types [35–37]. Finally, the variability in test cutoffs and standards for PD-L1 testing should be considered. However, we previously shown that different clones of PD-L1 antibodies, including 5H1, SP142, 28–8, 22C3, and SP263, have similar performance characteristics when used in a standardized IHC assay [38].
In conclusion, our study provides further data on the immunologic impact of nCRT in rectal cancer. We evaluated the effect of nCRT on CD8+TILsPDL-1 expression by spatial localization as well as on mucin expression, and their clinical implications in rectal cancer patients, comparing data from non-CRT cases. Matched pre- and postsurgical specimen analysis with further mechanistic investigations are needed in order to better evaluate the immune milieu of rectal cancer and to expand the applicability of checkpoint inhibitors in this setting.
Materials and Methods
Patients selection and evaluation
In this retrospective study, we collected surgical specimens from patients with rectal adenocarcinoma treated with surgery with or without nCRT at the Johns Hopkins between 2008 and 2014. We included patients with more evidence of distant metastasis at time of diagnosis, for which we had access to postsurgical tumor tissues obtained and clinicopathologic information. For patient who underwent nCRT further eligibility criteria was the completion of the planned course of preoperative CRT with conventional fractionation plus total mesorectal excision.
Clinical (at the time of diagnosis) and pathologic tumor stages were classified according to the 8th edition of the American Joint Committee on Cancer staging system. Dworak system was used to assess the pathologic regression grade, from 0 (no regression) to 4 (complete pathologic regression). Histological details of the tumors were retrieved from the archived pathological reports. Clinical data were obtained from patient records. The study was approved by the Johns Hopkins Institutional Research Board.
Immunohistochemical analysis
For immunohistochemistry tissue sections were stained with CD8 and PD-L1 antibodies. Whole slides images were acquired at 20× magnification. The prevalence of positive CD8 stained cells was recorded in the tumor-stroma interface was identified and drew by the pathologist (RAA) based on the H&E staining image and transferred to the analyzed images afterwards in Halo digital analysis software.
To assess if CD8+ cells have been enriched in tissue compartments, we measured the CD8+ cell density in different tissue compartments separately (tumor, interface tumor side, and interface background rectal side); each region was defined as 400 micrometers on both sides of the interface.
The density (# of cells/surface area analyzed) of CD8 expressing lymphocytes was assess via image analysis (HALO Indica Labs). Additionally, before we performed the digital analysis, we first did a quality check by eye with all the images and we didn’t observe a clear cluster pattern of CD8+ cell distribution [56].
PD-L1 membranous expression was manually counted in tumor cells (TC), tumor stroma (TS) and invasive front (IF), as previously described [34, 56]. Two 5 μm-thick sections were cut from one FFPE specimen and mounted on glass slides. After deparaffinization and antigen retrieval, the anti-PD-L1 antibody (SP142, Spring Bioscience) or a concentration matched isotype control were applied and allowed to incubate at 4°C for 22 hours. Signals were developed by using an Avidin Biotin Complex (ABC) Method (Vector Laboratory) combined with the TSA system (PerkinElmer) [56].
The study pathologist (RAA) estimated the percentage of PD-L1 stained cells was estimated on tumor cells (membranous staining), stroma (all the inflammatory, fibroblast and vascular cells, cytoplasm and membranous pattern) and invasive front (stroma between tumor cells and non-tumor tissue). Mucin expression was determined as the percentage of the mucin area in the whole tumor mass area.
Signal quantitation
Slides were scanned at 20× objective equivalent (0.49 microns/pixel) with Hamamatsu NanoZoomer XR slide scanner. Each image was annotated for regions of tumor, invasive front (400 micron area toward the center of the tumor and 400 micron area outside the tumor edge) and non-tumor regions by the study pathologist (RAA). Positive signals were reported as cell density per mm2 tissue area by digital analysis (Halo, Indicalab) [56].
Statistical analysis
Density and other continuous variables were tested with Student’s t-test. Association between categorical variables were analyzed using Fisher exact test with continuity correction. The median value of multiple slides for the same patient were used for analysis.
Pretreatment and post treatment absolute neutrophil count (ANC) absolute and lymphocyte count (ALC) from the peripheral blood were also collected. Pretreatment ANC and ALC values were obtained between the time of cancer diagnosis and treatment initiation (nCRT or surgery). The lab values closest to the time of treatment initiation were used. Post treatment ANC and ALC values were obtained within 60 days from surgery. A pretreatment and post treatment neutrophil-lymphocyte ratio (NLR), NLR was calculated for each patient, defined as the ANC divided by the ALC. NLR was evaluated as a continuous variable. Generalized estimating equations (GEE) were used (assuming a compound symmetry correlation structure) for model estimation and hypothesis testing. Specifically, we modeled the vector of expression from samples among patients as a function of sample location, treatment group, and the interaction of the two. Recurrence free survival (RFS) and overall survival (OS) were analyzed with the Kaplan-Meier method. Univariate and multivariate regression analyses of RFS were performed using Cox’s proportional hazard model. P-Values <0.05 were considered to be statistically significant. All the statistical analyses were performed using R 3.5.1.
Abbreviations
ANC: absolute neutrophil count; ALC: absolute and lymphocyte count; CRC: colorectal cancer; CRT: chemoradiotherapy; CT: chemotherapy; GEE: generalized estimating equations; HPF: high-power fields; HR: hazard ratio; ICI: immune checkpoint inhibitors; IF: invasive front; IFN-γ: interferon-γ; IHC: immunohistochemistry; ICAM: intercellular adhesion molecule-1; LARC: locally advanced rectal cancer; MSI: microsatellite instable; MSS: microsatellite stable; N: lymph node; nCRT: neoadjuvant chemoradiotherapy; NLR: neutrophil to lymphocytes ratio; NSCLC: non-small cell lung cancer; OS: overall survival; PD-1: programmed death 1; PD-L1: programmed death ligand-1; RCC: renal cell carcinoma; RFS: recurrence-free survival; RT: radiation therapy; TC: tumor cells; TILs: tumor-infiltrating lymphocytes; TME: tumor microenvironment; TRG: tumor regression grade; TS: tumor stroma.
ACKNOWLEDGMENTS
The study was supported by the Johns Hopkins Colorectal Cancer Research Center of Excellence.
Ethics approval and consent to participate
The study was approved by the Johns Hopkins Institutional Research Board.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
CONFLICTS OF INTEREST
The authors have no conflict of interests to declare.
References
1. Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020; 70:145–64. https://doi.org/10.3322/caac.21601. [PubMed].
2. Rödel C, Liersch T, Becker H, Fietkau R, Hohenberger W, Hothorn T, Graeven U, Arnold D, Lang-Welzenbach M, Raab HR, Sülberg H, Wittekind C, Potapov S, et al, and German Rectal Cancer Study Group. Preoperative chemoradiotherapy and postoperative chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced rectal cancer: initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet Oncol. 2012; 13:679–87. https://doi.org/10.1016/S1470-2045(12)70187-0. [PubMed].
3. Zhu S, Brodin NP, English K, Ohri N, Chuy JW, Rajdev LN, Narang R, Kalnicki S, Guha C, Garg MK, Kabarriti R. Comparing outcomes following total neoadjuvant therapy and following neoadjuvant chemoradiation therapy in patients with locally advanced rectal cancer. EClinicalMedicine. 2019; 16:23–29. https://doi.org/10.1016/j.eclinm.2019.09.009. [PubMed].
4. Walle T, Martinez Monge R, Cerwenka A, Ajona D, Melero I, Lecanda F. Radiation effects on antitumor immune responses: current perspectives and challenges. Ther Adv Med Oncol. 2018; 10:1758834017742575. https://doi.org/10.1177/1758834017742575. [PubMed].
5. Gupta A, Probst HC, Vuong V, Landshammer A, Muth S, Yagita H, Schwendener R, Pruschy M, Knuth A, van den Broek M. Radiotherapy promotes tumor-specific effector CD8+ T cells via dendritic cell activation. J Immunol. 2012; 189:558–66. https://doi.org/10.4049/jimmunol.1200563. [PubMed].
6. Gulley JL, Arlen PM, Bastian A, Morin S, Marte J, Beetham P, Tsang KY, Yokokawa J, Hodge JW, Ménard C, Camphausen K, Coleman CN, Sullivan F, et al. Combining a recombinant cancer vaccine with standard definitive radiotherapy in patients with localized prostate cancer. Clin Cancer Res. 2005; 11:3353–62. https://doi.org/10.1158/1078-0432.CCR-04-2062. [PubMed].
7. Reits EA, Hodge JW, Herberts CA, Groothuis TA, Chakraborty M, Wansley EK, Camphausen K, Luiten RM, de Ru AH, Neijssen J, Griekspoor A, Mesman E, Verreck FA, et al. Radiation modulates the peptide repertoire, enhances MHC class I expression, and induces successful antitumor immunotherapy. J Exp Med. 2006; 203:1259–71. https://doi.org/10.1084/jem.20052494. [PubMed].
8. Golden EB, Frances D, Pellicciotta I, Demaria S, Helen Barcellos-Hoff M, Formenti SC. Radiation fosters dose-dependent and chemotherapy-induced immunogenic cell death. Oncoimmunology. 2014; 3:e28518. https://doi.org/10.4161/onci.28518. [PubMed].
9. Lugade AA, Sorensen EW, Gerber SA, Moran JP, Frelinger JG, Lord EM. Radiation-induced IFN-gamma production within the tumor microenvironment influences antitumor immunity. J Immunol. 2008; 180:3132–39. https://doi.org/10.4049/jimmunol.180.5.3132. [PubMed].
10. Burnette BC, Liang H, Lee Y, Chlewicki L, Khodarev NN, Weichselbaum RR, Fu YX, Auh SL. The efficacy of radiotherapy relies upon induction of type i interferon-dependent innate and adaptive immunity. Cancer Res. 2011; 71:2488–96. https://doi.org/10.1158/0008-5472.CAN-10-2820. [PubMed].
11. Formenti SC, Demaria S. Systemic effects of local radiotherapy. Lancet Oncol. 2009; 10:718–26. https://doi.org/10.1016/S1470-2045(09)70082-8. [PubMed].
12. Kachikwu EL, Iwamoto KS, Liao YP, DeMarco JJ, Agazaryan N, Economou JS, McBride WH, Schaue D. Radiation enhances regulatory T cell representation. Int J Radiat Oncol Biol Phys. 2011; 81:1128–35. https://doi.org/10.1016/j.ijrobp.2010.09.034. [PubMed].
13. Price JG, Idoyaga J, Salmon H, Hogstad B, Bigarella CL, Ghaffari S, Leboeuf M, Merad M. CDKN1A regulates Langerhans cell survival and promotes Treg cell generation upon exposure to ionizing irradiation. Nat Immunol. 2015; 16:1060–68. https://doi.org/10.1038/ni.3270. [PubMed].
14. Wu CT, Chen WC, Chang YH, Lin WY, Chen MF. The role of PD-L1 in the radiation response and clinical outcome for bladder cancer. Sci Rep. 2016; 6:19740. https://doi.org/10.1038/srep19740. [PubMed].
15. Zou W, Chen L. Inhibitory B7-family molecules in the tumour microenvironment. Nat Rev Immunol. 2008; 8:467–77. https://doi.org/10.1038/nri2326. [PubMed].
16. Keir ME, Butte MJ, Freeman GJ, Sharpe AH. PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol. 2008; 26:677–704. https://doi.org/10.1146/annurev.immunol.26.021607.090331. [PubMed].
17. Schaue D, Comin-Anduix B, Ribas A, Zhang L, Goodglick L, Sayre JW, Debucquoy A, Haustermans K, McBride WH. T-cell responses to survivin in cancer patients undergoing radiation therapy. Clin Cancer Res. 2008; 14:4883–90. https://doi.org/10.1158/1078-0432.CCR-07-4462. [PubMed].
18. Deng L, Liang H, Burnette B, Beckett M, Darga T, Weichselbaum RR, Fu YX. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J Clin Invest. 2014; 124:687–95. https://doi.org/10.1172/JCI67313. [PubMed].
19. Dovedi SJ, Adlard AL, Lipowska-Bhalla G, McKenna C, Jones S, Cheadle EJ, Stratford IJ, Poon E, Morrow M, Stewart R, Jones H, Wilkinson RW, Honeychurch J, Illidge TM. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014; 74:5458–68. https://doi.org/10.1158/0008-5472.CAN-14-1258. [PubMed].
20. Sharabi AB, Lim M, DeWeese TL, Drake CG. Radiation and checkpoint blockade immunotherapy: radiosensitisation and potential mechanisms of synergy. Lancet Oncol. 2015; 16:e498–509. https://doi.org/10.1016/S1470-2045(15)00007-8. [PubMed].
21. Lim SH, Hong M, Ahn S, Choi YL, Kim KM, Oh D, Ahn YC, Jung SH, Ahn MJ, Park K, Zo JI, Shim YM, Sun JM. Changes in tumour expression of programmed death-ligand 1 after neoadjuvant concurrent chemoradiotherapy in patients with squamous oesophageal cancer. Eur J Cancer. 2016; 52:1–9. https://doi.org/10.1016/j.ejca.2015.09.019. [PubMed].
22. Twyman-Saint Victor C, Rech AJ, Maity A, Rengan R, Pauken KE, Stelekati E, Benci JL, Xu B, Dada H, Odorizzi PM, Herati RS, Mansfield KD, Patsch D, et al. Radiation and dual checkpoint blockade activate non-redundant immune mechanisms in cancer. Nature. 2015; 520:373–77. https://doi.org/10.1038/nature14292. [PubMed].
23. Brahmer JR, Drake CG, Wollner I, Powderly JD, Picus J, Sharfman WH, Stankevich E, Pons A, Salay TM, McMiller TL, Gilson MM, Wang C, Selby M, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010; 28:3167–75. https://doi.org/10.1200/JCO.2009.26.7609. [PubMed].
24. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012; 366:2443–54. https://doi.org/10.1056/NEJMoa1200690. [PubMed].
25. Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, Biedrzycki B, Donehower RC, Zaheer A, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015; 372:2509–20. https://doi.org/10.1056/NEJMoa1500596. [PubMed].
26. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M, Rutkowski P, Ferrucci PF, Hill A, Wagstaff J, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med. 2015; 373:23–34. https://doi.org/10.1056/NEJMoa1504030. [PubMed].
27. Poschke I, Mougiakakos D, Kiessling R. Camouflage and sabotage: tumor escape from the immune system. Cancer Immunol Immunother. 2011; 60:1161–71. https://doi.org/10.1007/s00262-011-1012-8. [PubMed].
28. Gasser S, Orsulic S, Brown EJ, Raulet DH. The DNA damage pathway regulates innate immune system ligands of the NKG2D receptor. Nature. 2005; 436:1186–90. https://doi.org/10.1038/nature03884. [PubMed].
29. Chajon E, Castelli J, Marsiglia H, De Crevoisier R. The synergistic effect of radiotherapy and immunotherapy: A promising but not simple partnership. Crit Rev Oncol Hematol. 2017; 111:124–32. https://doi.org/10.1016/j.critrevonc.2017.01.017. [PubMed].
30. Ahmed KA, Stallworth DG, Kim Y, Johnstone PA, Harrison LB, Caudell JJ, Yu HH, Etame AB, Weber JS, Gibney GT. Clinical outcomes of melanoma brain metastases treated with stereotactic radiation and anti-PD-1 therapy. Ann Oncol. 2016; 27:434–41. https://doi.org/10.1093/annonc/mdv622. [PubMed].
31. Golden EB, Chhabra A, Chachoua A, Adams S, Donach M, Fenton-Kerimian M, Friedman K, Ponzo F, Babb JS, Goldberg J, Demaria S, Formenti SC. Local radiotherapy and granulocyte-macrophage colony-stimulating factor to generate abscopal responses in patients with metastatic solid tumours: a proof-of-principle trial. Lancet Oncol. 2015; 16:795–803. https://doi.org/10.1016/S1470-2045(15)00054-6. [PubMed].
32. Brody JD, Ai WZ, Czerwinski DK, Torchia JA, Levy M, Advani RH, Kim YH, Hoppe RT, Knox SJ, Shin LK, Wapnir I, Tibshirani RJ, Levy R. In situ vaccination with a TLR9 agonist induces systemic lymphoma regression: a phase I/II study. J Clin Oncol. 2010; 28:4324–32. https://doi.org/10.1200/JCO.2010.28.9793. [PubMed].
33. Sun X, Gan L, Na A, Ge L, Chen B, Liu J. Combination with Stereotactic Body Radiotherapy Offers a Promising Strategy to Overcome Resistance to Immunotherapy in Advanced Renal Cell Cancer. J Oncol. 2019; 2019:1483406. https://doi.org/10.1155/2019/1483406. [PubMed].
34. Parikh AR, Clark JW, Wo JYL, Yeap BY, Allen JN, Blaszkowsky LS, Ryan DP, Giantonio BJ, Weekes CD, Zhu AX, Van Seventer EE, Matlack L, Foreman B, et al. A phase II study of ipilimumab and nivolumab with radiation in microsatellite stable (MSS) metastatic colorectal adenocarcinoma (mCRC). J Clin Oncol. 2019; 37:3514. https://doi.org/10.1200/JCO.2019.37.15_suppl.3514.
35. Choueiri TK, Figueroa DJ, Fay AP, Signoretti S, Liu Y, Gagnon R, Deen K, Carpenter C, Benson P, Ho TH, Pandite L, de Souza P, Powles T, Motzer RJ. Correlation of PD-L1 tumor expression and treatment outcomes in patients with renal cell carcinoma receiving sunitinib or pazopanib: results from COMPARZ, a randomized controlled trial. Clin Cancer Res. 2015; 21:1071–77. https://doi.org/10.1158/1078-0432.CCR-14-1993. [PubMed].
36. Song M, Chen D, Lu B, Wang C, Zhang J, Huang L, Wang X, Timmons CL, Hu J, Liu B, Wu X, Wang L, Wang J, Liu H. PTEN loss increases PD-L1 protein expression and affects the correlation between PD-L1 expression and clinical parameters in colorectal cancer. PLoS One. 2013; 8:e65821. https://doi.org/10.1371/journal.pone.0065821. [PubMed].
37. Baptista MZ, Sarian LO, Derchain SF, Pinto GA, Vassallo J. Prognostic significance of PD-L1 and PD-L2 in breast cancer. Hum Pathol. 2016; 47:78–84. https://doi.org/10.1016/j.humpath.2015.09.006. [PubMed].
38. Sunshine JC, Nguyen PL, Kaunitz GJ, Cottrell TR, Berry S, Esandrio J, Xu H, Ogurtsova A, Bleich KB, Cornish TC, Lipson EJ, Anders RA, Taube JM. PD-L1 Expression in Melanoma: A Quantitative Immunohistochemical Antibody Comparison. Clin Cancer Res. 2017; 23:4938–44. https://doi.org/10.1158/1078-0432.CCR-16-1821. [PubMed].
39. Hecht M, Büttner-Herold M, Erlenbach-Wünsch K, Haderlein M, Croner R, Grützmann R, Hartmann A, Fietkau R, Distel LV. PD-L1 is upregulated by radiochemotherapy in rectal adenocarcinoma patients and associated with a favourable prognosis. Eur J Cancer. 2016; 65:52–60. https://doi.org/10.1016/j.ejca.2016.06.015. [PubMed].
40. Lim YJ, Koh J, Kim S, Jeon SR, Chie EK, Kim K, Kang GH, Han SW, Kim TY, Jeong SY, Park KJ, Wu HG. Chemoradiation-Induced Alteration of Programmed Death-Ligand 1 and CD8+ Tumor-Infiltrating Lymphocytes Identified Patients With Poor Prognosis in Rectal Cancer: A Matched Comparison Analysis. Int J Radiat Oncol Biol Phys. 2017; 99:1216–24. https://doi.org/10.1016/j.ijrobp.2017.07.004. [PubMed].
41. Ogura A, Akiyoshi T, Yamamoto N, Kawachi H, Ishikawa Y, Mori S, Oba K, Nagino M, Fukunaga Y, Ueno M. Pattern of programmed cell death-ligand 1 expression and CD8-positive T-cell infiltration before and after chemoradiotherapy in rectal cancer. Eur J Cancer. 2018; 91:11–20. https://doi.org/10.1016/j.ejca.2017.12.005. [PubMed].
42. Teng F, Meng X, Kong L, Mu D, Zhu H, Liu S, Zhang J, Yu J. Tumor-infiltrating lymphocytes, forkhead box P3, programmed death ligand-1, and cytotoxic T lymphocyte-associated antigen-4 expressions before and after neoadjuvant chemoradiation in rectal cancer. Transl Res. 2015; 166:721–32.e1. https://doi.org/10.1016/j.trsl.2015.06.019. [PubMed].
43. Lee Y, Auh SL, Wang Y, Burnette B, Wang Y, Meng Y, Beckett M, Sharma R, Chin R, Tu T, Weichselbaum RR, Fu YX. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: changing strategies for cancer treatment. Blood. 2009; 114:589–95. https://doi.org/10.1182/blood-2009-02-206870. [PubMed].
44. Shinto E, Hase K, Hashiguchi Y, Sekizawa A, Ueno H, Shikina A, Kajiwara Y, Kobayashi H, Ishiguro M, Yamamoto J. CD8+ and FOXP3+ tumor-infiltrating T cells before and after chemoradiotherapy for rectal cancer. Ann Surg Oncol. 2014 (Suppl 3); 21:S414–21. https://doi.org/10.1245/s10434-014-3584-y. [PubMed].
45. Naito Y, Saito K, Shiiba K, Ohuchi A, Saigenji K, Nagura H, Ohtani H. CD8+ T cells infiltrated within cancer cell nests as a prognostic factor in human colorectal cancer. Cancer Res. 1998; 58:3491–94. [PubMed].
46. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pagès C, Tosolini M, Camus M, Berger A, Wind P, Zinzindohoué F, Bruneval P, Cugnenc PH, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006; 313:1960–64. https://doi.org/10.1126/science.1129139. [PubMed].
47. Hollingsworth MA, Swanson BJ. Mucins in cancer: protection and control of the cell surface. Nat Rev Cancer. 2004; 4:45–60. https://doi.org/10.1038/nrc1251. [PubMed].
48. Byrd JC, Bresalier RS. Mucins and mucin binding proteins in colorectal cancer. Cancer Metastasis Rev. 2004; 23:77–99. https://doi.org/10.1023/a:1025815113599. [PubMed].
49. Agrawal B, Krantz MJ, Parker J, Longenecker BM. Expression of MUC1 mucin on activated human T cells: implications for a role of MUC1 in normal immune regulation. Cancer Res. 1998; 58:4079–81. [PubMed].
50. Agrawal B, Longenecker BM. MUC1 mucin-mediated regulation of human T cells. Int Immunol. 2005; 17:391–99. https://doi.org/10.1093/intimm/dxh219. [PubMed].
51. Correa I, Plunkett T, Vlad A, Mungul A, Candelora-Kettel J, Burchell JM, Taylor-Papadimitriou J, Finn OJ. Form and pattern of MUC1 expression on T cells activated in vivo or in vitro suggests a function in T-cell migration. Immunology. 2003; 108:32–41. https://doi.org/10.1046/j.1365-2567.2003.01562.x. [PubMed].
52. Agrawal B, Gupta N, Konowalchuk JD. MUC1 Mucin: A Putative Regulatory (Checkpoint) Molecule of T Cells. Front Immunol. 2018; 9:2391. https://doi.org/10.3389/fimmu.2018.02391. [PubMed].
53. Lindén SK, Florin TH, McGuckin MA. Mucin dynamics in intestinal bacterial infection. PLoS One. 2008; 3:e3952. https://doi.org/10.1371/journal.pone.0003952. [PubMed].
54. Cornelissen LA, Van Vliet SJ. A Bitter Sweet Symphony: Immune Responses to Altered O-glycan Epitopes in Cancer. Biomolecules. 2016; 6:26. https://doi.org/10.3390/biom6020026. [PubMed].
55. Bhatia R, Gautam SK, Cannon A, Thompson C, Hall BR, Aithal A, Banerjee K, Jain M, Solheim JC, Kumar S, Batra SK. Cancer-associated mucins: role in immune modulation and metastasis. Cancer Metastasis Rev. 2019; 38:223–36. https://doi.org/10.1007/s10555-018-09775-0. [PubMed].
56. Baretti M, Zhu Q, Zahurak M, Bhaijee F, Xu H, Engle EL, Kotte A, Pawlik TM, Anders RA, De Jesus-Acosta A. Prognostic Implications of the Immune Tumor Microenvironment in Patients With Pancreatic and Gastrointestinal Neuroendocrine Tumors. Pancreas. 2021; 50:719–26. https://doi.org/10.1097/MPA.0000000000001831. [PubMed].