
Introduction
NETs are a rare and diverse group of tumors with variable survival outcomes and behaviors [1], defined by tissue-based characteristics that include Ki67 index, grade, and morphology [2]. The annual incidence of NET has been reported to be around 3.65 per 100,000 people, however, due to better diagnostic tools and increased lifespan, the incidence and prevalence of these tumors is on the rise [3, 4]. Although there have been substantial advances in the treatment of NET over the past decade [5], challenges still exist with regard to patient selection and prediction of response. The classification of these tumors is based on tumor grade (assessed by mitotic rate and Ki-67 index) and differentiation: well-differentiated NETs, which are mostly low or intermediate grade, poorly differentiated NECs, which are high grade and aggressive, and the discordant tumors (well differentiated with high tumor grades) [6]. Poorly differentiated NECs often involve multiple sites of metastases, and rarely produce symptoms related to secretion of bioactive substances. Accurate distinction of well-differentiated, indolent tumors from poorly differentiated, aggressive tumors is important since treatment approaches are different with substantial difference in prognosis [7]. The majority of NET are diagnosed at a late stage with around 60–80% presenting with distant metastasis at diagnosis [8]. The 5-year overall survival of patients with NET ranges between 35–82% in well-to moderately differentiated NET and between 4–38% in poorly differentiated NET [3, 9].
With the complexity of the classification, novel biomarkers are required to assist in clinical decision making and ultimately improve patient outcomes [10]. Identification of biomarkers that could be used to guide targets for therapy is an unmet need [11]. Mutational alterations have changed the landscape of treatment in multiple cancers and improved the survival of cancer patients [12–18]. Recently, there has been an increasing interest in circulating tumor DNA (ctDNA) on the basis of studies performed in a range of other cancers [2]. As opposed to traditional tissue biopsies, liquid biopsies are faster, less invasive, have the potential to reflect all metastatic sites (ie tumor heterogeneity), and can indicate therapeutic response or progression through serial sampling [2]. Furthermore, considering the potential of genomic analysis, liquid biopsies offer a facilitated means of detecting genomic alterations and can be easily repeated over time [19–22]. ctDNA testing is now recommended to guide the treatment of lung cancer [23]. A potential challenge that exists with the application of ctDNA in the NEN field is the relative lack of recurrent and/or actionable mutations [2] and this is reported in multiple small studies [2]. Novel technologies such as next generation sequencing (NGS) revealed new molecular aspects of NET over the last years [1, 24]. In a study conducted by Gleeson et al, alterations in MEN1 chromatin remodeling genes and mammalian target of rapamycin (mTOR) pathway genes were found to be the most frequent molecular events identified in pancreatic NET, but it remains unclear whether these biomarkers and other less frequently observed alterations possess predictive value [24]. In this report, analysis of ctDNA through blood-based Guardant360® NGS from patients with a diagnosis of NEN across various histologies is evaluated. The aim was to confirm the feasibility of NGS using ctDNA in NEN and characterize common alterations in the genomic profile. Furthermore, we aimed to identify whether the molecular alterations lead to the identification of potential actionable targets.
Results
Patient demographics
Between the years 2016 and 2019, a total of 320 NEN patients underwent Guardant360® testing using clinical-grade NGS of ctDNA across multiple institutions, and 280 (87.5%) patients had at least one sample with alterations. The median age was 63 years (range: 8-93), with a male preponderance (57%). Tumor type included pancreatic NET (N = 165, 52%), NEC/NET not otherwise specified (NOS) (N = 64, 20%), gastrointestinal NEC (N = 52, 16%), large cell lung NEC (N = 21, 7%) and nasopharyngeal NEC (N = 16, 5%) (Figure 1). ctDNA NGS testing was performed on 338 plasma samples; 14 patients had testing performed twice and 2 patients had testing performed three times. A total of 1,012 genomic alterations were identified after excluding variants of uncertain significance (VUSs) and synonymous mutations. Chemotherapy was documented in 48 patients (Supplementary Table 1). The sequence of testing to treatment is unknown. Pathology was obtained in 144 patients and KI-67 score was obtained in 71 patients. KI-67 scores ranged from < 1% to > 99%. Of the 144 patients with documented pathology, 43 patients (30%) were high grade, 8 were intermediate grade (6%), and 3 were low grade.
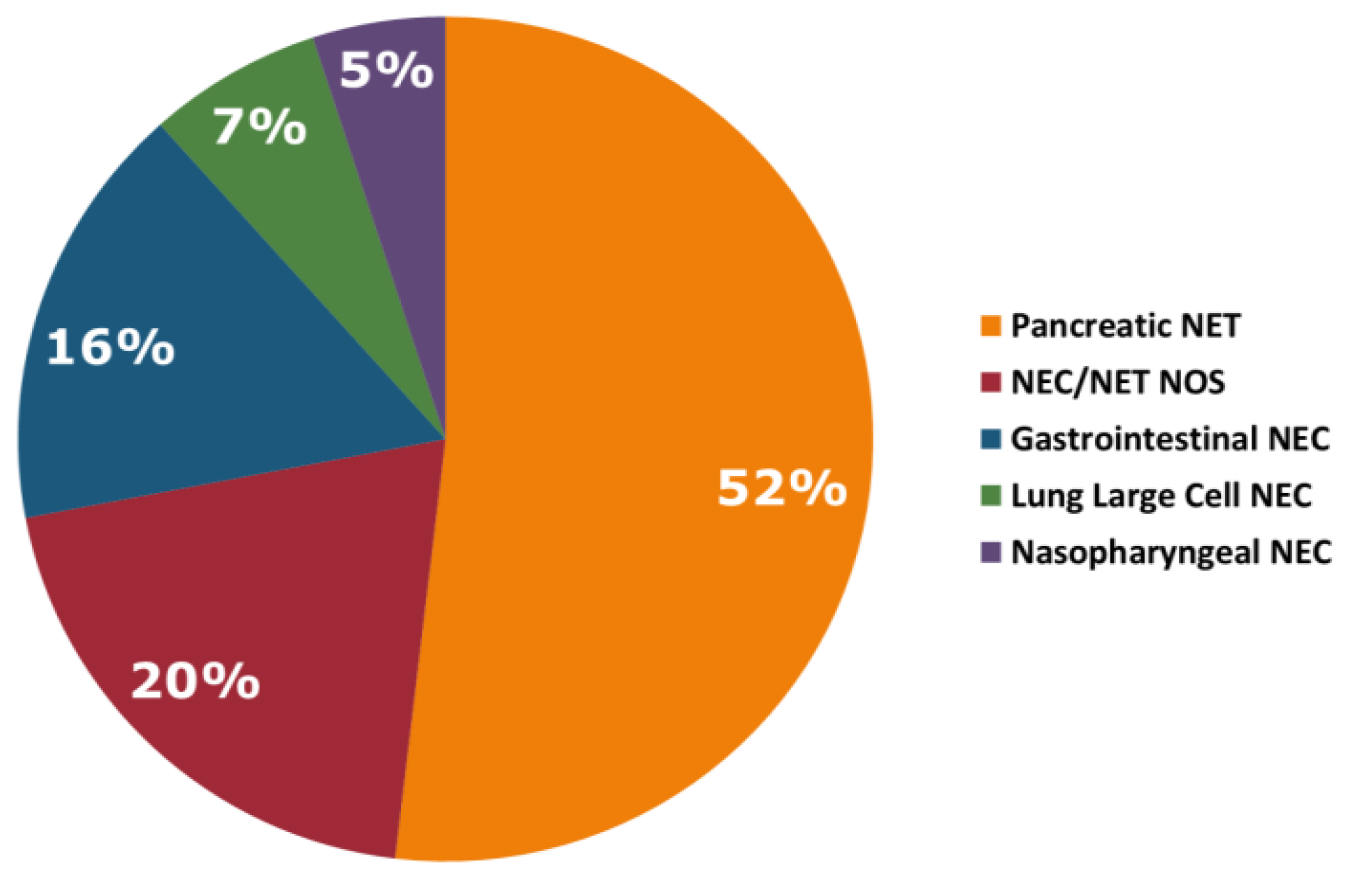
Figure 1: Tumor types.
Molecular alterations
In the total cohort of NEN patients, TP53 associated genes were most commonly altered (N = 145, 52%), followed by KRAS (N = 61, 22%), EGFR (N = 33, 12%), PIK3CA (N = 30, 11%), BRAF (N = 28, 10%), MYC (N = 28, 10%), CCNE1 (N = 28, 10%), CDK6 (N = 22, 8%), RB1 (N = 19, 7%), NF1 (N = 19, 7%), MET (N = 19, 7%), FGFR1 (N = 19, 7%), APC (N = 19, 7%), ERBB2 (N = 16, 6%) and PTEN (N = 14, 5%) (Figure 2). Alteration frequency by gene and alteration type are shown in Figure 3. Of the 28 patients with BRAF mutations, 3 patients had the V600E alteration. For PNET patients, TP53 was the most commonly altered mutation (N = 125), followed by KRAS (N = 63), APC (N = 49), NF1 (N = 46), EGFR (N = 43), MET (N = 42), BRCA1 (N = 32), MYC (N = 30), BRCA2 (N = 29), CDK6 (N = 25), ERBB2 (N = 22), BRAF (N = 20), CCNE1 (N = 19), PIK3CA (N = 17), MTOR (N = 15), FGFR1 (N = 14), RB1 (N = 13) and PTEN (N = 11). For gastrointestinal NEC patients, TP53 associated genes were most commonly altered (N = 54), followed by APC (N = 28), EGFR (N = 18), ERBB2 (N = 11), NF1 (N = 11), KRAS (N = 10), CCNE1 (N = 10), BRCA2 (N = 10), BRCA1 (N = 9), PIK3CA (N = 9), RB1 (N = 8), MYC (N = 7), BRAF (N = 7), CDK6 (N = 5), MTOR (N = 4), MET (N = 3), and FGFR1 (N = 3). For large cell lung NEC patients, TP53 mutation was most commonly altered (N = 48), followed by BRAF (N = 11), PIK3CA (N = 10), APC (N = 10), MET (N = 9), FGFR1 (N = 9), EGFR (N = 8), KRAS (N = 8), MYC (N = 7), BRCA2 (N = 5), ERBB2 (N = 5), CCNE1 (N = 5), RB1 (N = 5), CDK6 (N = 4), NF1 (N = 3), MTOR (N = 2), BRCA1 (N = 1) and PTEN (N = 1). Genomic alterations stratified by tumor type are shown in Figure 4.
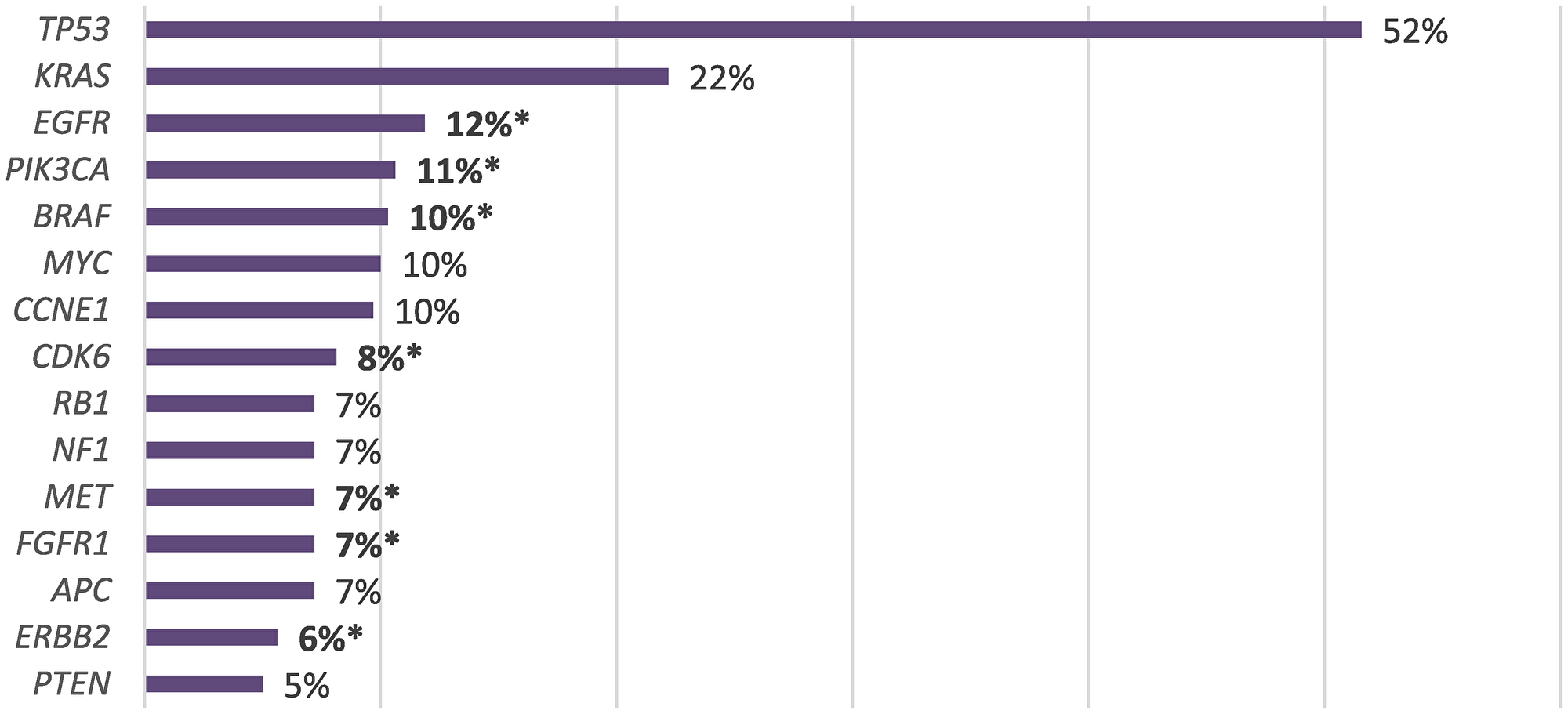
Figure 2: Prevalence of genomic alterations (SM and VUSs excluded) with therapeutic implications (*).
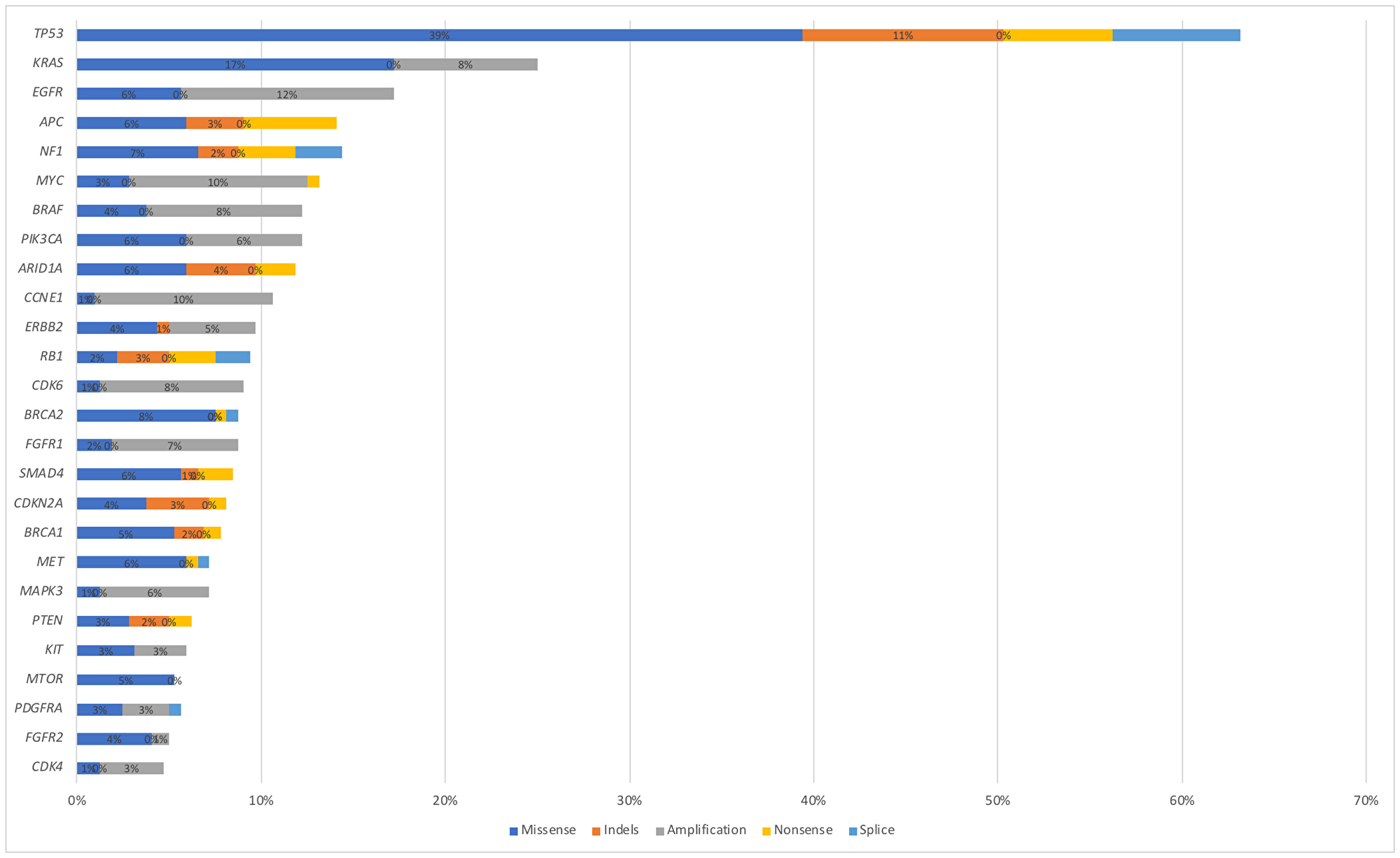
Figure 3: Alteration frequency by gene and alteration type (synonymous alterations excluded).
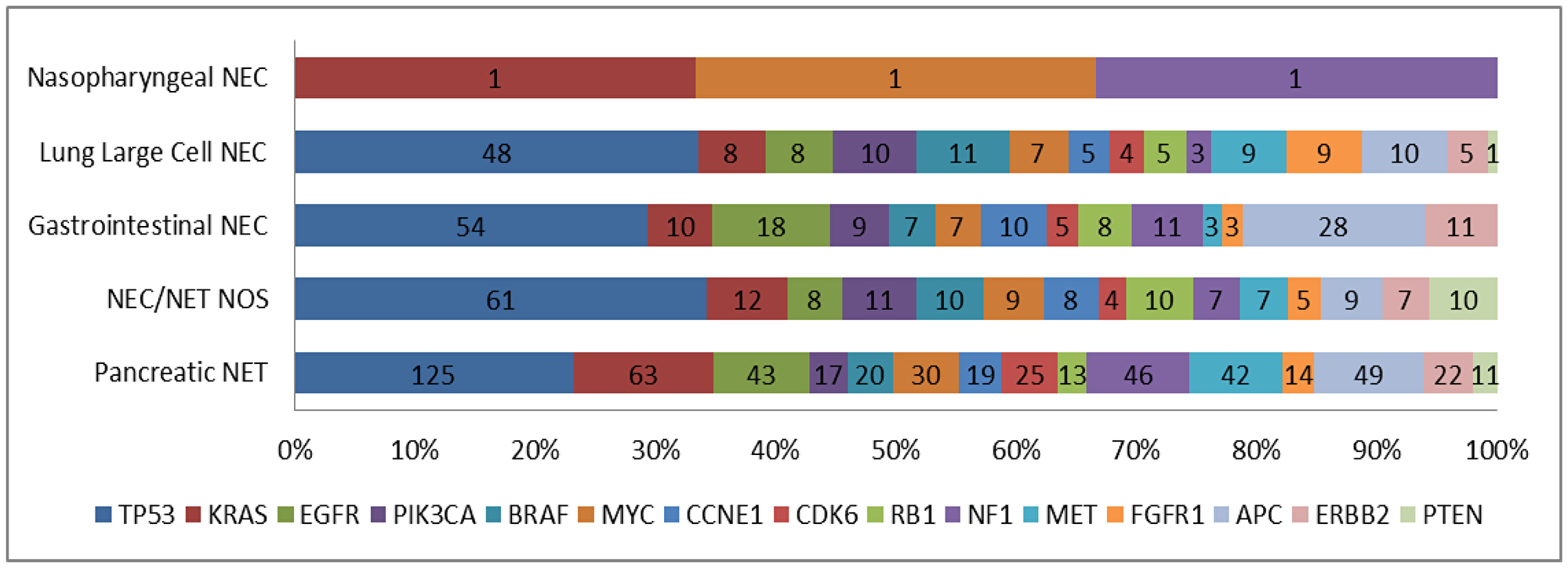
Figure 4: Genomic alterations stratified by tumor type.
Relationship between age and gender
KRAS mutations occurred more commonly among males (66%) with a mean age of 59.3 years. Prevalence of BRAF mutations occurred more frequently in males (60%) with a mean age of 61.5 years. Seven ATM mutations were detected and occurred more frequently in males (57%) with a mean age of 67.1 years. In this study, BRCA1 and BRCA2 mutations were seen in males more frequently (82% and 65%) with a mean age of 54.7 years and 58.9 years, respectively. MTOR mutations occurred more commonly in females (56%) with a mean age of 63.4 years and 47 PIK3CA mutations were detected, of which 51% were male and mean age was 58.4 years (Table 1). These results need to be validated by a larger sample size in future studies to reach a statistically significant correlation.
Table 1: Correlation between age and gender with respect to KRAS/BRAF/ATM/BRCA/MTOR/PIK3CA
| Gene | Count of Gene | Male | Female | Mean Age (Years) |
|---|---|---|---|---|
| KRAS | 94 | 62/94 (66%) | 32/94 (34%) | 59.3 |
| BRAF | 48 | 29/48 (60%) | 19/48 (40%) | 61.5 |
| ATM | 7 | 4/7 (57%) | 3/7 (43%) | 67.1 |
| BRCA 1 | 45 | 37/45 (82%) | 8/45 (18%) | 54.7 |
| BRCA 2 | 48 | 31/48 (65%) | 17/48 (35%) | 58.9 |
| MTOR | 27 | 12/27 (44%) | 15/27 (56%) | 63.4 |
| PIK3CA | 47 | 24/47 (51%) | 23/47 (49%) | 58.4 |
Plasma-Derived ctDNA for longitudinal disease monitoring
Among the 320 patients studied, 14 patients had testing performed twice and 2 patients had testing performed three times. By analyzing these longitudinal blood samples, we found that new mutations can be gained over time that could potentially be targeted in 11 patients. With serial testing, we identified 1 patient that gained a mutation in FGFR2, 1 patient that gained a mutation in ATM and 1 patient that gained a mutation in BRCA1, which could all be targeted. Loss of mutations was identified in 6 of the 11 patients. These include TP53, KIT, RAF1, ERBB2, CDK6, PIK3CA, DDR2, CCNE1, NF1, BRCA2, PDGFRA, and NOTCH1 (Supplementary Table 3).
DISCUSSION
NEN represent a heterogeneous group of malignancies varying in biology and behavior. In the era of next generation sequencing the characterization of NEN has led to a better understanding of the molecular underpinnings of these neoplasms [25–28]. As a result, research can be geared towards exploring new pathways to target with both research-based and existing therapies. The current selection of therapies for NETs include somatostatin analogs [29], peptide receptor radionuclide therapy [30], mTOR inhibitors (everolimus), chemotherapy combinations [31] (ie capecitabine/temozolomide) and multi-kinase inhibitors [32] (ie sunitinib, pazopanib, cabozantinib). None of these agents are tailored to select patients on the basis of the presence or absence of molecular alterations, and limited predictive or prognostic biomarkers have been identified other than the location of the primary tumor and the Ki67%. Several translational studies have provided convincing data that epigenetic profiling can identify potential prognostic biomarkers, and some of these have demonstrated preliminary success as serum biomarkers that can be used clinically [33].
With current technology the genome of a tumor can be analyzed by studying the tumor tissue as well as the DNA shed by the tumor (ctDNA). A significant challenge for the use of ctDNA in the NEN field is the relative lack of recurrent mutations in comparison with other tumors. Requirements for accurate ctDNA analysis include adequate tumor DNA being shed into the blood stream and a PCR primer based assay that detects the mutations of interest [34]. Unfortunately, these conditions are only present in a small subset of NET patients population [34]. In small bowel NET, tissue-based genomic sequencing revealed that the majority of recurrent mutations were in cyclin-dependent kinase inhibitor CDKN1B (8% of cases) [35]. Pancreatic NET also exhibit recurrent mutations in a relatively limited number of genes, including the tumor suppressor gene MEN1, as well as ATRX and DAXX, genes implicated in chromatin remodeling [36]. Interestingly, mutations in MEN1, DAXX/ATRX or the combination of both MEN1 and DAXX/ATRX were associated with prolonged survival in a study conducted by Jiao et al. relative to those patients whose tumors lacked these mutations [36]. The mutational status of DAXX, ATRX and mTOR pathway genes could be used to stratify the prognosis of pancreatic NETs [37]. However, Chan et al. demonstrated contradictory results, whereby mutations in DAXX, ATRX, and MEN1 were associated with adverse clinical outcome in comparison to those without these mutations [38]. This discrepancy between the data could be attributed to a different composition of the tumors. Use of ctDNA analysis in this disease has been inconsistent. Pipinikas et al. established that the ctDNA detected in the blood of 9 tissue samples from 3 pancreatic NET patients had variable concordance with tissue somatic variants [the same tissue somatic variants were detected in ctDNA from cases 1 (NEBL) and 3 (DAXX)] [39], while Beltran et al. demonstrated that ctDNA and matched tissue biopsies from 64 patients with prostate NET showed approximately 80% concordance [40].
The analysis of ctDNA may be useful for multiple purposes including early detection of residual or recurrent disease, monitoring tumor burden, assessing molecular heterogeneity targeted treatments, prognostic and predictive implications [41]. Recently, Wang et al. demonstrated an ALK translocation revealed by ctDNA analysis in a patient with metastatic atypical carcinoid tumor of the lung [42]. The patient was treated with the second-generation ALK inhibitor alectinib with rapid and lasting shrinkage of his disease, supporting the hypothesis that the ALK translocation was the driver mutation. In another case report, a patient with high-grade, large cell neuroendocrine cervical carcinoma was successfully treated with nivolumab combined with stereotactic body radiation therapy, based on blood ctDNA results targetting alterations suspicious for high tumor burden [43].
The present analysis is the first and largest population-based study exploring the genetic mutations in patients with NEN utilizing ctDNA derived from liquid biopsy. Some of the alterations reported here are in clinical development as potential targets. In our population of NEN patients, alterations were identified with therapeutic implications that could potentially be targeted by drugs approved for other cancers. Examples of these mutations with their respective frequency of alterations include with possible drug examples: EGFR (12%, erlotinib), PIK3CA (11%, alpelisib), BRAF (10%, vermurafenib), CDK6 (8%, palbociclib), MET (7%, cabozantinib), FGFR1 (7%, pazopanib, erdafitinib), ERBB2 (6%, trastuzumab, pertuzumab), and BRCA1/2 (15%, olaparib). Repeat sampling is a unique advantage of liquid biopsies over tissue based assays. In this series, 16 patients had serial profiling of ctDNA. Analysis showed gain and loss of mutations with time. Some of the gained mutations are targetable including FGFR2, ATM and BRCA1.
There are several limitations to our study inherent to all retrospective analyses. First, genomics data were obtained from a de-identified database and, hence, only limited clinical information was available. There was no data available regarding whether samples were obtained prior to or after medical treatment/surgery, which limits the interpretation of the analysis. Furthermore, the gene panel is restricted to 73 genes failing to test for MEN1, ATRX or DAXX, which are clinically important in pancreatic NET (Supplementary Table 2). In addition, no survival data was available and the data was limited by the coding of physicians at the different institutions. KI67% and pathology data was lacking in around 50% of patients. It worth noting that our subset of patients did not include specifically small intestinal NETs, which represent the most common NET. It is likely that the majority of the gastrointestinal and the “not otherwise specified” NETs are small intestinal in origin. There is no data to compare tissue genomics to liquid testing in this analysis. Despite these limitations, our findings have important implications. Our study demonstrated that evaluation of ctDNA is feasible among individuals with NEN. Theoretically, as more oncogenic pathways are discovered and more targeted therapies are approved, personalized treatments based on identified unique molecular mutations could lead to improved patient outcomes [44].
Despite the identification of ctDNA as circulating biomarkers capable of providing prognostic information and personalized treatment options in patients with NEN, they have not yet been incorporated into routine clinical practice. More prospective evaluations are required to better understand the role of these biomarkers in NEN, therefore incorporation of ctDNA analysis into clinical trials is highly recommended.
Materials and Methods
This is a retrospective review evaluating the molecular alterations in 338 ctDNA samples from 320 patients who had a diagnosis of NEN and underwent Guardant360® clinical-grade NGS across multiple institutions. The test detects single nucleotide variants in 54–73 genes, copy number amplifications, fusions, and indels in selected genes. Samples from NEN patients between the years 2016 and 2019 were analyzed. Patient-specific covariates included gender and age. Ethical approval was not required for the study; patient identity protection was maintained throughout the study in a de-identified database through a data transfer agreement between Guardant Health and Emory University, and existing data was collected in accordance with the Emory University Institutional Review Board (IRB) guidelines.
Next generation sequencing
NGS of plasma cfDNA (liquid biopsy) was done by Guardant Health (Guardant360®), a College of American Pathologists (CAP)-accredited and Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory. The Guardant360® assay detects single-nucleotide variants (SNV), indels, fusions, and copy number alterations in 73 genes, including the most prevalent tumor suppressor genes in human cancers, with a reportable range of ≥ 0.04%, ≥ 0.02%, ≥ 0.04%, and ≥ 2.12 copies, respectively, as well as microsatellite instability. It does not report tumor mutation burden (TMB). This is a highly analytically/clinically sensitive and specific test, able to detect single molecules of tumor DNA in 10 mL blood samples with an analytic specificity of > 99.9999% [45].
cfDNA was extracted from plasma using the QIAmp Circulating Nucleic Acid Kit (Qiagen, Inc.). Hybrid-capture sequencing libraries were prepared from up to 30ng cfDNA and labeled with nonrandom oligonucleotide barcodes (IDT, Inc.), followed by library preparation, hybrid capture enrichment (Agilent Technologies, Inc.), and sequencing at 15,000 × read depth of the critical exons in the targeted panel by paired-end synthesis (NextSeq 500 and/or HiSeq 2500, Illumina, Inc.). Bioinformatics analysis and variant detection were performed as previously described [46]. NGS data were interpreted by N-of-One, Inc. (Lexington, MA, USA).
Abbreviations
NENs: Neuroendocrine neoplasms; NETs: Neuroendocrine tumors; NECs: Neuroendocrine carcinomas; NGS: Next generation sequencing; DNA: Circulating tumor; VUSs: Variants of uncertain significance; mTOR: Mammalian target of rapamycin; IRB: Institutional Review Board; SNV: Single-nucleotide variants.
ACKNOWLEDGMENTS
Part of data presented in this study was presented at the 2019 American Society of Clinical Oncology in Chicago, Illinois. The manuscript’s abstract was published in “Abstracts” in Journal of Clinical Oncology: Shaib et al. Journal of Clinical Oncology. May 20, 2019; 37(15_suppl):4110. DOI: 10.1200/JCO.2019.37.15_suppl.4110.
CONFLICTS OF INTEREST
The authors declare no potential conflicts of interest.
FUNDING
There was no specific funding for this study and there are no competing financial disclosures.
References
1. Di Domenico A, Wiedmer T, Marinoni I, Perren A. Genetic and epigenetic drivers of neuroendocrine tumours (NET). Endocr Relat Cancer. 2017; 24:R315–34. https://doi.org/10.1530/ERC-17-0012. [PubMed].
2. Rizzo FM, Meyer T. Liquid Biopsies for Neuroendocrine Tumors: Circulating Tumor Cells, DNA, and MicroRNAs. Endocrinol Metab Clin North Am. 2018; 47:471–83. https://doi.org/10.1016/j.ecl.2018.04.002. [PubMed].
3. Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, Abdalla EK, Fleming JB, Vauthey JN, Rashid A, Evans DB. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008; 26:3063–72. https://doi.org/10.1200/JCO.2007.15.4377. [PubMed].
4. Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin North Am. 2011; 40:1–18, vii. https://doi.org/10.1016/j.ecl.2010.12.005. [PubMed].
5. Cives M, Strosberg J. Treatment Strategies for Metastatic Neuroendocrine Tumors of the Gastrointestinal Tract. Curr Treat Options Oncol. 2017; 18:14. https://doi.org/10.1007/s11864-017-0461-5. [PubMed].
6. Kim JY, Hong SM. Recent Updates on Neuroendocrine Tumors From the Gastrointestinal and Pancreatobiliary Tracts. Arch Pathol Lab Med. 2016; 140:437–48. https://doi.org/10.5858/arpa.2015-0314-RA. [PubMed].
7. Oronsky B, Ma PC, Morgensztern D, Carter CA. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia. 2017; 19:991–1002. https://doi.org/10.1016/j.neo.2017.09.002. [PubMed].
8. Modlin IM, Gustafsson BI, Moss SF, Pavel M, Tsolakis AV, Kidd M. Chromogranin A—biological function and clinical utility in neuro endocrine tumor disease. Ann Surg Oncol. 2010; 17:2427–43. https://doi.org/10.1245/s10434-010-1006-3. [PubMed].
9. Pape UF, Böhmig M, Berndt U, Tiling N, Wiedenmann B, Plöckinger U. Survival and clinical outcome of patients with neuroendocrine tumors of the gastroenteropancreatic tract in a german referral center. Ann N Y Acad Sci. 2004; 1014:222–33. https://doi.org/10.1196/annals.1294.025. [PubMed].
10. Oberg K, Modlin IM, De Herder W, Pavel M, Klimstra D, Frilling A, Metz DC, Heaney A, Kwekkeboom D, Strosberg J, Meyer T, Moss SF, Washington K, et al. Consensus on biomarkers for neuroendocrine tumour disease. Lancet Oncol. 2015; 16:e435–46. https://doi.org/10.1016/S1470-2045(15)00186-2. [PubMed].
11. Shaw A, Bradley MD, Elyan S, Kurian KM. Tumour biomarkers: diagnostic, prognostic, and predictive. BMJ. 2015; 351:h3449. https://doi.org/10.1136/bmj.h3449. [PubMed].
12. Overman MJ, Lonardi S, Wong KY, Lenz HJ, Gelsomino F, Aglietta M, Morse MA, Van Cutsem E, McDermott R, Hill A, Sawyer MB, Hendlisz A, Neyns B, et al. Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J Clin Oncol. 2018; 36:773–79. https://doi.org/10.1200/JCO.2017.76.9901. [PubMed].
13. Le DT, Kim TW, Van Cutsem E, Geva R, Jäger D, Hara H, Burge M, O’Neil B, Kavan P, Yoshino T, Guimbaud R, Taniguchi H, Elez E, et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J Clin Oncol. 2020; 38:11–19. https://doi.org/10.1200/JCO.19.02107. [PubMed].
14. Bang YJ, Kang YK, Catenacci DV, Muro K, Fuchs CS, Geva R, Hara H, Golan T, Garrido M, Jalal SI, Borg C, Doi T, Yoon HH, et al. Pembrolizumab alone or in combination with chemotherapy as first-line therapy for patients with advanced gastric or gastroesophageal junction adenocarcinoma: results from the phase II nonrandomized KEYNOTE-059 study. Gastric Cancer. 2019; 22:828–37. https://doi.org/10.1007/s10120-018-00909-5. [PubMed].
15. Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, Dechaphunkul A, Imamura F, Nogami N, Kurata T, Okamoto I, Zhou C, Cho BC, et al, and FLAURA Investigators. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2018; 378:113–25. https://doi.org/10.1056/NEJMoa1713137. [PubMed].
16. Zhou Y, Lin Z, Zhang X, Chen C, Zhao H, Hong S, Zhang L. First-line treatment for patients with advanced non-small cell lung carcinoma and high PD-L1 expression: pembrolizumab or pembrolizumab plus chemotherapy. J Immunother Cancer. 2019; 7:120. https://doi.org/10.1186/s40425-019-0600-6. [PubMed].
17. Amatu A, Sartore-Bianchi A, Siena S. NTRK gene fusions as novel targets of cancer therapy across multiple tumour types. ESMO Open. 2016; 1:e000023. https://doi.org/10.1136/esmoopen-2015-000023. [PubMed].
18. Cheng L, Lopez-Beltran A, Massari F, MacLennan GT, Montironi R. Molecular testing for BRAF mutations to inform melanoma treatment decisions: a move toward precision medicine. Mod Pathol. 2018; 31:24–38. https://doi.org/10.1038/modpathol.2017.104. [PubMed].
19. Gerlinger M, Rowan AJ, Horswell S, Math M, Larkin J, Endesfelder D, Gronroos E, Martinez P, Matthews N, Stewart A, Tarpey P, Varela I, Phillimore B, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012; 366:883–92. https://doi.org/10.1056/NEJMoa1113205. [PubMed].
20. Martelotto LG, Ng CK, Piscuoglio S, Weigelt B, Reis-Filho JS. Breast cancer intra-tumor heterogeneity. Breast Cancer Res. 2014; 16:210. https://doi.org/10.1186/bcr3658. [PubMed].
21. Bidard FC, Weigelt B, Reis-Filho JS. Going with the flow: from circulating tumor cells to DNA. Sci Transl Med. 2013; 5:207ps14. https://doi.org/10.1126/scitranslmed.3006305. [PubMed].
22. De Mattos-Arruda L, Cortes J, Santarpia L, Vivancos A, Tabernero J, Reis-Filho JS, Seoane J. Circulating tumour cells and cell-free DNA as tools for managing breast cancer. Nat Rev Clin Oncol. 2013; 10:377–89. https://doi.org/10.1038/nrclinonc.2013.80. [PubMed].
23. Wang W, Song Z, Zhang Y. A Comparison of ddPCR and ARMS for detecting EGFR T790M status in ctDNA from advanced NSCLC patients with acquired EGFR-TKI resistance. Cancer Med. 2017; 6:154–62. https://doi.org/10.1002/cam4.978. [PubMed].
24. Gleeson FC, Voss JS, Kipp BR, Kerr SE, Van Arnam JS, Mills JR, Marcou CA, Schneider AR, Tu ZJ, Henry MR, Levy MJ. Assessment of pancreatic neuroendocrine tumor cytologic genotype diversity to guide personalized medicine using a custom gastroenteropancreatic next-generation sequencing panel. Oncotarget. 2017; 8:93464–75. https://doi.org/10.18632/oncotarget.18750. [PubMed].
25. Mafficini A, Scarpa A. Genetics and Epigenetics of Gastroenteropancreatic Neuroendocrine Neoplasms. Endocr Rev. 2019; 40:506–36. https://doi.org/10.1210/er.2018-00160. [PubMed].
26. Raj N, Shah R, Stadler Z, Mukherjee S, Chou J, Untch B, Li J, Kelly V, Saltz LB, Mandelker D, Ladanyi M, Berger MF, Klimstra DS, et al. Real-Time Genomic Characterization of Metastatic Pancreatic Neuroendocrine Tumors Has Prognostic Implications and Identifies Potential Germline Actionability. JCO Precis Oncol. 2018; 2018:1–18. https://doi.org/10.1200/PO.17.00267. [PubMed].
27. Pipinikas CP, Dibra H, Karpathakis A, Feber A, Novelli M, Oukrif D, Fusai G, Valente R, Caplin M, Meyer T, Teschendorff A, Bell C, Morris TJ, et al. Epigenetic dysregulation and poorer prognosis in DAXX-deficient pancreatic neuroendocrine tumours. Endocr Relat Cancer. 2015; 22:L13–18. https://doi.org/10.1530/ERC-15-0108. [PubMed].
28. Vijayvergia N, Boland PM, Handorf E, Gustafson KS, Gong Y, Cooper HS, Sheriff F, Astsaturov I, Cohen SJ, Engstrom PF. Molecular profiling of neuroendocrine malignancies to identify prognostic and therapeutic markers: a Fox Chase Cancer Center Pilot Study. Br J Cancer. 2016; 115:564–70. https://doi.org/10.1038/bjc.2016.229. [PubMed].
29. Igaz P. [Efficacy of somatostatin analogues in the treatment of neuroendocrine tumours based on the results of recent clinical trials]. [Article in Hungarian]. Orv Hetil. 2014; 155:1908–12. https://doi.org/10.1556/OH.2014.30048. [PubMed].
30. Zhang J, Kulkarni HR, Singh A, Baum RP. Delayed Response (Partial Remission) 3 Years After Peptide Receptor Radionuclide Therapy in a Patient Participating in the NETTER-1 Trial. Clin Nucl Med. 2019; 44:223–26. https://doi.org/10.1097/RLU.0000000000002456. [PubMed].
31. Ramirez RA, Beyer DT, Chauhan A, Boudreaux JP, Wang YZ, Woltering EA. The Role of Capecitabine/Temozolomide in Metastatic Neuroendocrine Tumors. Oncologist. 2016; 21:671–75. https://doi.org/10.1634/theoncologist.2015-0470. [PubMed].
32. Imbulgoda A, Heng DY, Kollmannsberger C. Sunitinib in the treatment of advanced solid tumors. Recent Results Cancer Res. 2014; 201:165–84. https://doi.org/10.1007/978-3-642-54490-3_9. [PubMed].
33. Finnerty BM, Gray KD, Moore MD, Zarnegar R, Fahey Iii TJ. Epigenetics of gastroenteropancreatic neuroendocrine tumors: A clinicopathologic perspective. World J Gastrointest Oncol. 2017; 9:341–53. https://doi.org/10.4251/wjgo.v9.i9.341. [PubMed].
34. Herrera-Martínez AD, Hofland LJ, Gálvez Moreno MA, Castaño JP, de Herder WW, Feelders RA. Neuroendocrine neoplasms: current and potential diagnostic, predictive and prognostic markers. Endocr Relat Cancer. 2019; 26:R157–79. https://doi.org/10.1530/ERC-18-0354. [PubMed].
35. Francis JM, Kiezun A, Ramos AH, Serra S, Pedamallu CS, Qian ZR, Banck MS, Kanwar R, Kulkarni AA, Karpathakis A, Manzo V, Contractor T, Philips J, et al. Somatic mutation of CDKN1B in small intestine neuroendocrine tumors. Nat Genet. 2013; 45:1483–86. https://doi.org/10.1038/ng.2821. [PubMed].
36. Jiao Y, Shi C, Edil BH, de Wilde RF, Klimstra DS, Maitra A, Schulick RD, Tang LH, Wolfgang CL, Choti MA, Velculescu VE, Diaz LA Jr, Vogelstein B, et al. DAXX/ATRX, MEN1, and mTOR pathway genes are frequently altered in pancreatic neuroendocrine tumors. Science. 2011; 331:1199–203. https://doi.org/10.1126/science.1200609. [PubMed].
37. Scarpa A, Chang DK, Nones K, Corbo V, Patch AM, Bailey P, Lawlor RT, Johns AL, Miller DK, Mafficini A, Rusev B, Scardoni M, Antonello D, et al, and Australian Pancreatic Cancer Genome Initiative. Whole-genome landscape of pancreatic neuroendocrine tumours. Nature. 2017; 543:65–71. https://doi.org/10.1038/nature21063. [PubMed].
38. Chan CS, Laddha SV, Lewis PW, Koletsky MS, Robzyk K, Da Silva E, Torres PJ, Untch BR, Li J, Bose P, Chan TA, Klimstra DS, Allis CD, Tang LH. ATRX, DAXX or MEN1 mutant pancreatic neuroendocrine tumors are a distinct alpha-cell signature subgroup. Nat Commun. 2018; 9:4158. https://doi.org/10.1038/s41467-018-06498-2. [PubMed].
39. Abstracts of the 13th Annual ENETS Conference for the Diagnosis and Treatment of Neuroendocrine Tumor Disease. March 9-11, 2016, Barcelona, Spain: abstracts. Neuroendocrinology. 2016; 103:1–128. https://doi.org/10.1159/000448725. [PubMed].
40. Beltran H, Romanel A, Casiraghi N, Sigouros M, Benelli M, Xiang J, Demichelis F. Whole exome sequencing (WES) of circulating tumor DNA (ctDNA) in patients with neuroendocrine prostate cancer (NEPC) informs tumor heterogeneity. Journal of Clinical Oncology. 2017; 35:5011. https://doi.org/10.1200/JCO.2017.35.15_suppl.5011.
41. Francis G, Stein S. Circulating Cell-Free Tumour DNA in the Management of Cancer. Int J Mol Sci. 2015; 16:14122–42. https://doi.org/10.3390/ijms160614122. [PubMed].
42. Wang VE, Young L, Ali S, Miller VA, Urisman A, Wolfe J, Bivona TG, Damato B, Fogh S, Bergsland EK. A Case of Metastatic Atypical Neuroendocrine Tumor with ALK Translocation and Diffuse Brain Metastases. Oncologist. 2017; 22:768–73. https://doi.org/10.1634/theoncologist.2017-0054. [PubMed].
43. Sharabi A, Kim SS, Kato S, Sanders PD, Patel SP, Sanghvi P, Weihe E, Kurzrock R. Exceptional Response to Nivolumab and Stereotactic Body Radiation Therapy (SBRT) in Neuroendocrine Cervical Carcinoma with High Tumor Mutational Burden: Management Considerations from the Center For Personalized Cancer Therapy at UC San Diego Moores Cancer Center. Oncologist. 2017; 22:631–37. https://doi.org/10.1634/theoncologist.2016-0517. [PubMed].
44. Borazanci E, Millis SZ, Kimbrough J, Doll N, Von Hoff D, Ramanathan RK. Potential actionable targets in appendiceal cancer detected by immunohistochemistry, fluorescent in situ hybridization, and mutational analysis. J Gastrointest Oncol. 2017; 8:164–72. https://doi.org/10.21037/jgo.2017.01.14. [PubMed].
45. Lanman RB, Mortimer SA, Zill OA, Sebisanovic D, Lopez R, Blau S, Collisson EA, Divers SG, Hoon DS, Kopetz ES, Lee J, Nikolinakos PG, Baca AM, et al. Analytical and Clinical Validation of a Digital Sequencing Panel for Quantitative, Highly Accurate Evaluation of Cell-Free Circulating Tumor DNA. PLoS One. 2015; 10:e0140712. https://doi.org/10.1371/journal.pone.0140712. [PubMed].
46. Odegaard JI, Vincent JJ, Mortimer S, Vowles JV, Ulrich BC, Banks KC, Fairclough SR, Zill OA, Sikora M, Mokhtari R, Abdueva D, Nagy RJ, Lee CE, et al. Validation of a Plasma-Based Comprehensive Cancer Genotyping Assay Utilizing Orthogonal Tissue- and Plasma-Based Methodologies. Clin Cancer Res. 2018; 24:3539–49. https://doi.org/10.1158/1078-0432.CCR-17-3831. [PubMed].