
Introduction
Locally advanced oropharyngeal cancers possess a unique challenge. The anatomical location along with multiple physiological functions associated with this structure makes open surgical resection a difficult and moribund procedure [1]. Hence in locally advanced oropharyngeal cancers, concurrent chemoradiation is used primarily for management. The prognosis of these tumors is heavily dependent on the Human Papilloma Virus (HPV) status [2]. Patients with HPV positive disease have a favorable prognosis as opposed to HPV negative disease [2]. The incidence of HPV positive disease is variable across the globe with the incidence in North America in the range of 48–81.4% [3], and 15–22.8% in the Indian subcontinent [4].
Efforts to improve outcomes in locally advanced oropharyngeal cancer have met with limited success [5, 6]. Recently a phase 3 randomized study was reported by us, in locally advanced head and neck cancers, testing the role of concurrent nimotuzumab in addition to weekly cisplatin and definitive radiation. The study met its primary endpoint of progression-free survival [7]. However, a similar study exploring the role of Cetuximab (RTOG 0522) was negative [8]. We had hypothesized that an improvement in outcomes in our study was seen due to the differential patient population in our study when compared to the RTOG 0552 study. We had a younger cohort of patients and a predominantly HPV negative disease [7]. This population, even in RTOG 0522 showed a trend towards improvement with the addition of cetuximab [8]. Another phase 3 study, exploring the role of cetuximab along with carboplatin -5 FU with radiation, reported improvement in outcomes with the addition of cetuximab [9]. The probable reason for this was probably due to the predominant HPV negative disease.
Taking this into consideration, we decided to perform a subgroup analysis of the HPV negative oropharyngeal cancer cohort, to study the absolute improvement in 2-year outcomes with the addition of nimotuzumab. We compared 2 year progression free survival (PFS), disease free survival (DFS), locoregional control (LRC) and overall survival (OS) between both arms.
Results
Patient selection and baseline characteristics
We had 536 patients in the study, out of which 269 had primary in the oropharynx. P16 testing was feasible in 212 patients and 187 patients were p16 negative. These 187 patients are included in the current analysis. There were 91 patients in the cisplatin radiotherapy (CRT) arm and 97 in nimotuzumab-cisplatin radiation (NCRT) arm. The baseline characteristics were balanced between the 2 arms (Table 1).
Table 1: Baseline characteristics
| Variable | Cisplatin-radiotherapy arm (n = 91) | Nimotuzumab-cisplatin-radiotherapy arm (n = 96) | P-value |
|---|---|---|---|
| Age, years | |||
| Median age (range) | 53 (31–75) | 56 (34–70) | |
| Age > 60 years | 23 (25.3) | 30 (31.2) | 0.272* |
| Gender | |||
| Male | 83 (91.2) | 83 (86.5) | 0.359 |
| Female | 8 (8.8) | 13 (13.5) | |
| ECOG PS | |||
| 0 | 20 (22) | 14 (14.6) | 0.255 |
| 1 | 71 (78) | 82 (85.4) | |
| Tobacco use | |||
| Yes | 85 (93.4) | 88 (91.7) | 0.783 |
| No | 6 (6.6) | 8 (9.3) | |
| Subsite of malignancy | |||
| Base of tongue | 52 (57.1) | 57 (59.4) | 0.959 |
| Tonsil | 25 (27.5) | 27 (28.1) | |
| Soft palate | 10 (11) | 9 (9.4) | |
| Posterior pharyngeal wall | 4 (4.4) | 3 (3.1) | |
| T category† | |||
| T1–T2 | 25 (27.5) | 16 (16.7) | 0.08 |
| T3–T4 | 66 (72.5) | 80 (83.3) | |
| N category† | |||
| N0–N1 | 35 (38.5) | 35 (36.5) | 0.88 |
| N2–N3 | 56 (61.5) | 61 (63.5) | |
| TNM Stage grouping† | |||
| Stage III | 14 (15.4) | 18 (18.8) | 0.794 |
| Stage IVA | 74 (81.3) | 74 (77.1) | |
| Stage IVB | 3 (3.3) | 4 (4.2) | |
| Histological Grade | |||
| Grade 1–2 | 68 (74.4) | 66 (68.8) | 0.418 |
| Grade 3 | 23 (25.3) | 30 (31.2) |
Outcomes
The interaction test for HPV status (positive & negative) was significant for PFS (p = 0.000), LRC (p = 0.007) and OS (p = 0.002) but not for DFS (p = 0.072), suggesting a differential impact of the addition of nimotuzumab with respect to HPV status.
Progression-free survival
At the time of data censoring 103 events had occurred, 60 in CRT arm and 43 in the NCRT arm. The median PFS was 12.9 months (95%CI 8.47–17.3) versus 35.3 months (95%CI 22.10-NA) (P-value = 0.0015) in the CRT and NCRT arm respectively. The 2 year PFS was 31.5% (95%CI 21.5–42) in CRT arm versus 57.2% (95%CI 45.8–67.1) in NCRT arm (Figure 1). The unadjusted hazard ratio was 0.53 (95%CI 0.36–0.79, P-value = 0.002). The multivariate analysis for PFS is shown in Table 2. The adjusted hazard ratio was 0.53 (95%CI 0.36–0.8, P-Value = 0.002). The results of sensitivity analysis performed for PFS using a composite endpoint of progression or death was in line with the above-mentioned analysis. The unadjusted and adjusted hazard ratios were 0.62 (95%CI 0.43–0.88, P-value = 0.008) and 0.62 (95%CI 0.43–0.89, P-value = 0.009), respectively. The site of failure was locoregional in 45 patients (49.5%), locoregional with distant failure in 3 patients (3.3%) and distant failure in 12 patients (13.2%) in CRT arm. The patients with corresponding sites of failure in the NCRT arm were 32 (33.3%), 6 (6.2%) and 5 (5.2%), respectively.
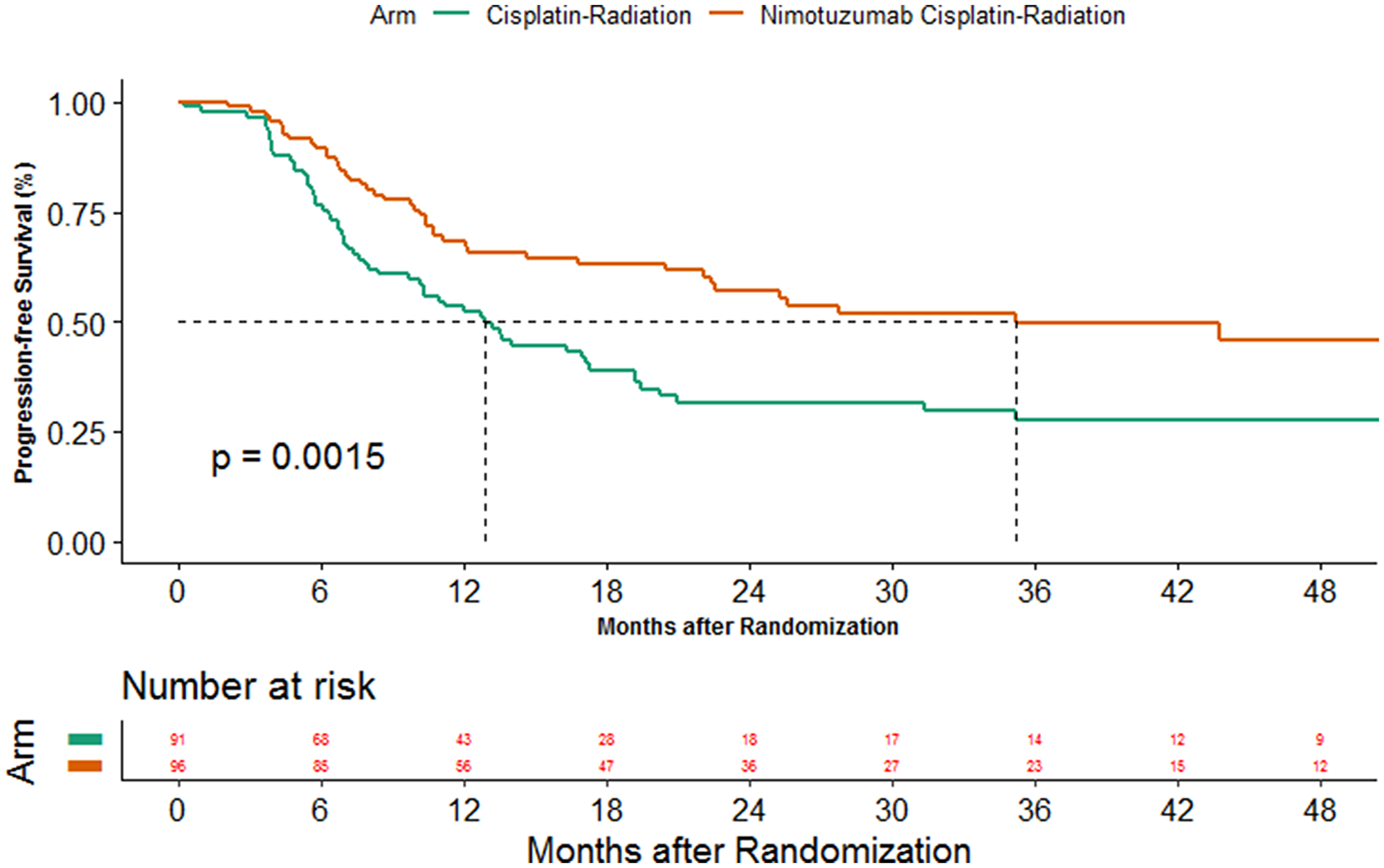
Figure 1: Kaplan Meier estimates of progression-free survival between the 2 arms.
Table 2: Table depicting the result of multivariate cox regression analysis for progression-free survival and locoregional control
| Variables | Variable type | Reference | Hazard ratio (HR) | 95%CI of HR | P-value |
|---|---|---|---|---|---|
| Progression-free analysis | |||||
| Arm | Binary | Cisplatin arm | 0.5352 | 0.3588–0.7983 | 0.00218* |
| Age | Binary | Below 60 years | 0.7138 | 0.4573–1.1141 | 0.13776 |
| Stage | Binary | Stage III | 1.7770 | 0.9587–3.2937 | 0.06786 |
| ECOG PS | Binary | ECOG PS 0 | 0.8501 | 0.5337–1.3541 | 0.49418 |
| Grade | Binary | Grade 1–2 | 1.2734 | 0.8227–1.9710 | 0.27816 |
| Subsite | Binary | Non base of tongue | 1.0607 | 0.7106–1.5835 | 0.77303 |
| Time to locoregional control | |||||
| Arm | Binary | Cisplatin arm | 0.6311 | 0.4094–0.9728 | 0.0371* |
| Age | Binary | Below 60 years | 0.7268 | 0.4453–1.1861 | 0.2016 |
| Stage | Binary | Stage III | 2.0823 | 1.0250–4.2303 | 0.0425* |
| ECOG PS | Binary | ECOG PS 0 | 0.6850 | 0.4203–1.1165 | 0.1290 |
| Grade | Binary | Grade 1–2 | 1.1278 | 0.6967–1.8256 | 0.6245 |
| Subsite | Binary | Non base of tongue | 0.9464 | 0.6121–1.4631 | 0.8042 |
Locoregional control
The improvement in PFS with the addition of nimotuzumab is largely contributed by an improvement in locoregional control. The median time to locoregional failure was 17.3 months (95%CI 12.0–56.3) and 60.3 months (95%CI 22.6-NA) in cisplatin arm and cisplatin-nimotuzumab arm respectively (P-value = 0.023). The 2-year LRC was 41.4% (95%CI 29.8–52.6) in CRT arm versus in 60.4% (95%CI 48.7–70.2) in NCRT arm (Figure 2). The unadjusted hazard ratio was 0.61 (95%CI 0.4–0.94, P-value = 0.024) while the adjusted hazard ratio was 0.63 (95%CI 0.41–0.97, P-value = 0.037). These results were confirmed in the sensitivity analysis. The unadjusted and adjusted hazard ratios were 0.68 (95%CI 0.48–0.99, P-value = 0.0358) and 0.69 (95%CI 0.43–0.89, P-value = 0.0494) in favor of the cisplatin-nimotuzumab arm, with the use of composite endpoint of locoregional failure or death.
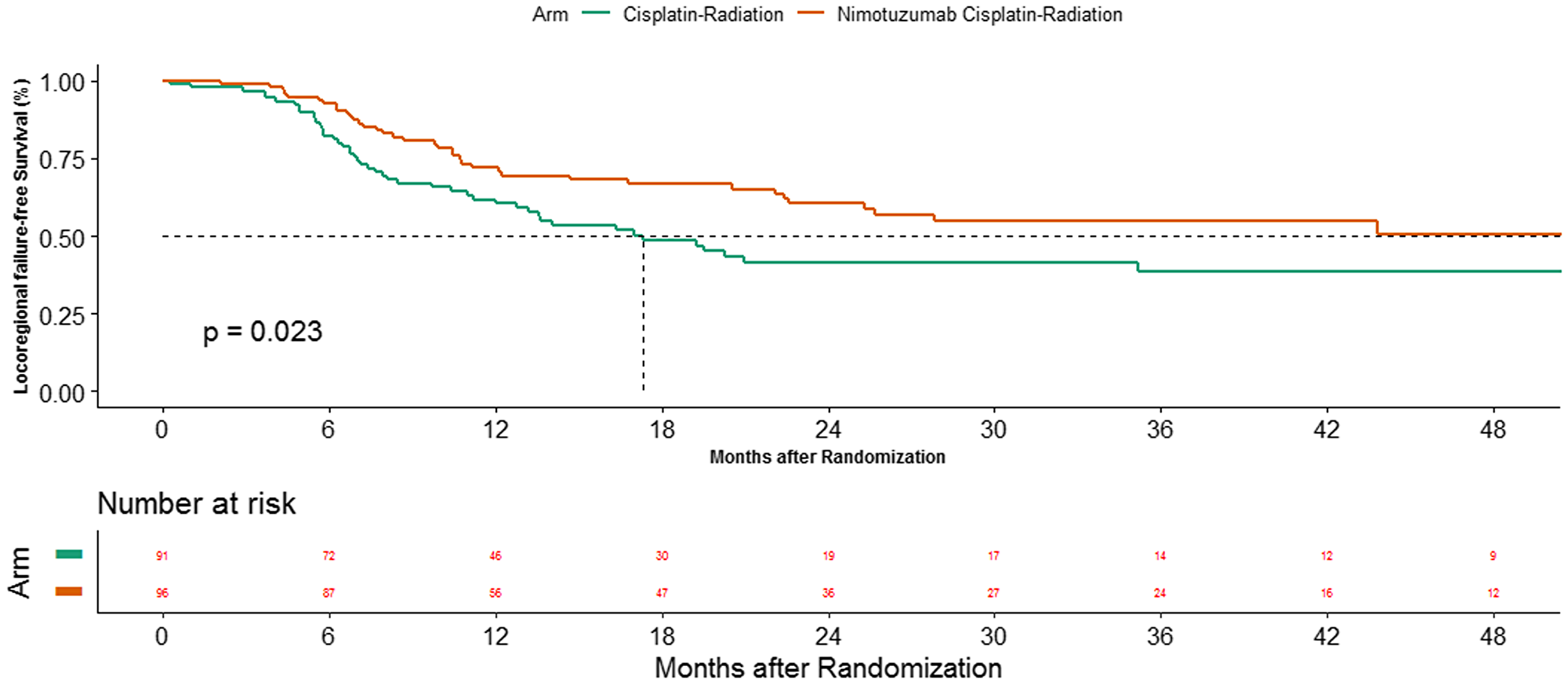
Figure 2: Kaplan Meier estimates of time to locoregional control between the 2 arms.
Overall survival
The median follow up was 38.5 months (95%CI 36.2–46.3). At the data cutoff, 105 deaths had happened; 57 in cisplatin arm and 48 in the cisplatin-nimotuzumab arm. The median OS was 19.0 months (95%CI 14.2–23.4) in cisplatin arm while it was 35.9 months (95%CI 22.8–53.7) in the cisplatin-nimotuzumab arm (P-value = 0.017). The addition of nimotuzumab also led to an improvement in 2 year OS from 39.0% (95%CI 28.4–49.6) to 57.6% (95%CI 46.3–67.4) (Figure 3). The assumption for proportional hazard was violated (Supplementary Table 1) and hence, COX regression analysis was found to be an unsuitable method for comparison. Alternatively, restricted mean survivals were calculated for both arms and compared. The restricted mean survival estimated in cisplatin and cisplatin-nimotuzumab arm using data up to 65 months was 37.62 months (95%CI 32.5–42.74) and 29.45 months (95%CI 24.12–34.77), respectively (Figure 4), a difference of 8.17 months (95%CI 0.79–15.56; P-value = 0.03).
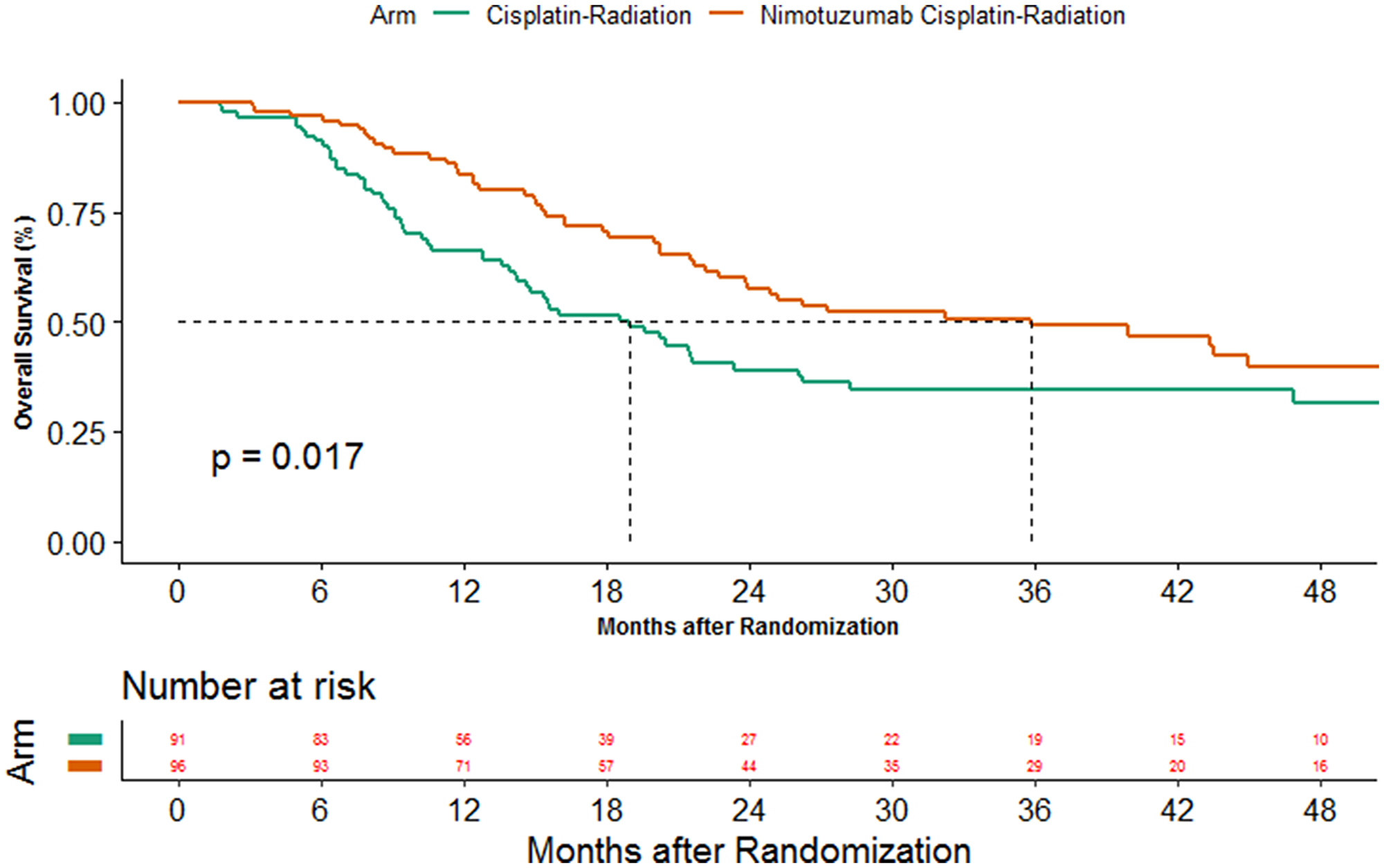
Figure 3: Kaplan Meier estimates overall survival between the 2 arms.
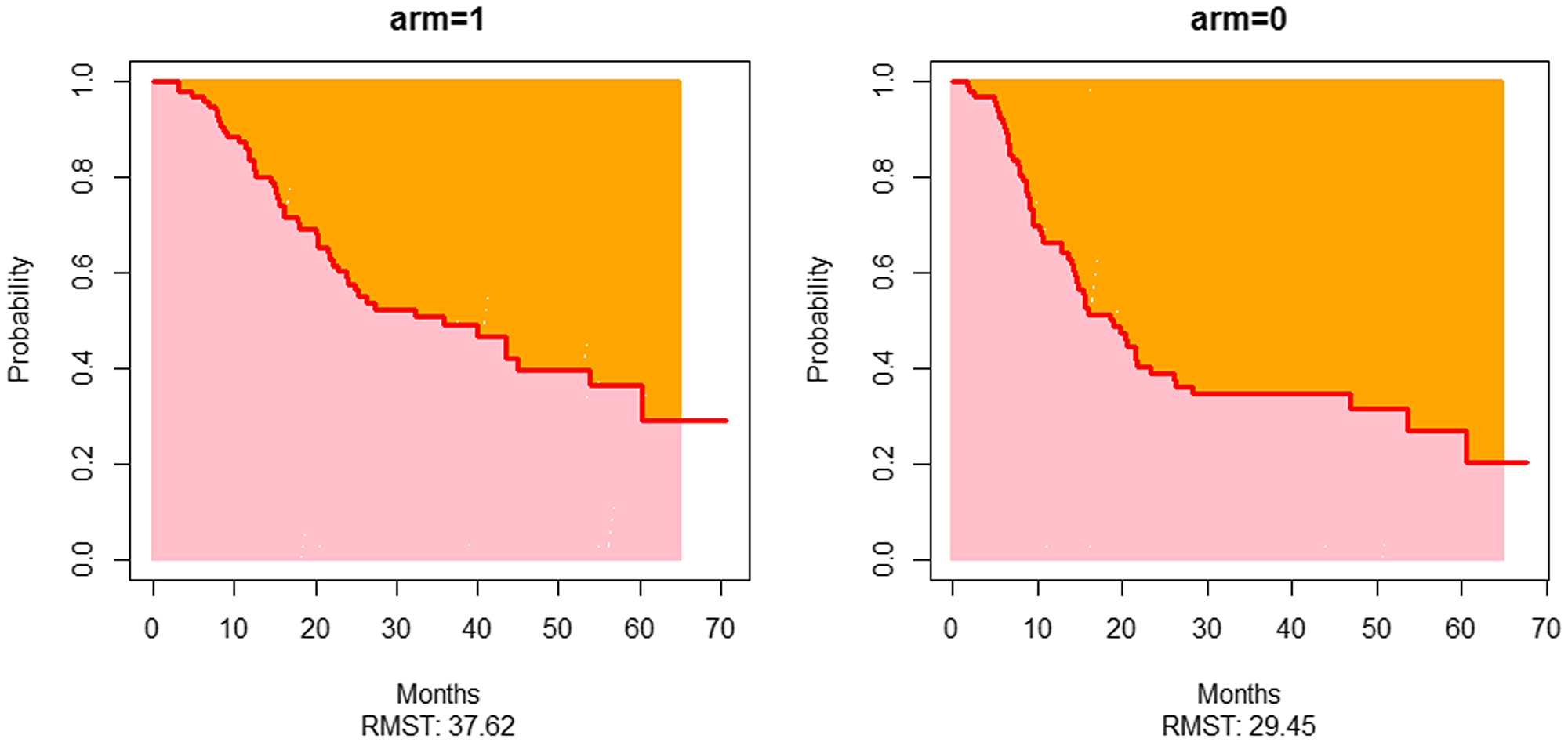
Figure 4: Restricted mean overall survival plots of both arms. arm = 0 represents the plot of the cisplatin radiotherapy arm while arm = 1 represents the plot of the Nimotuzumab-cisplatin radiotherapy arm.
Compliance to treatment
The data for treatment compliance and radiation technique are shown in Table 3. There was no difference in these factors between the 2 arms.
Table 3: Compliance data for radiation and cisplatin
| Variable | Cisplatin-radiotherapy arm | Nimotuzumab-cisplatin- radiotherapy arm | P-value |
|---|---|---|---|
| (n = 91) | (n = 96) | ||
| Radiotherapy compliance | |||
| Radiotherapy dose | |||
| Median dose | 70 (IQR 70–70) | 70 (IQR 70–70) | – |
| 100% | 86 (94.5) | 84 (87.5) | 0.127 |
| ≥95% | 86 (94.5) | 85 (88.5) | 0.193 |
| Radiotherapy technique | |||
| 2-Dimensional | 83 (91.2) | 86 (89.6) | |
| IMRT | 8 (8.8) | 9 (9.4) | 1.0 |
| Not started | – | 1 (1.0) | |
| Median package time in days | 52 (IQR 49–55) | 51 (IQR 49–54) | – |
| Treatment completed within 63 days | |||
| Yes | 88 (96.7) | 93 (96.9) | 1.0 |
| No | 3 (3.3) | 3 (3.1) | |
| Gaps | |||
| 1 day or more | 30 (33) | 36 (37.5) | 0.543 |
| ≥3 days cumulative duration | 24 (26.4) | 32 (33.3) | 0.34 |
| Systemic therapy compliance | |||
| Cisplatin cycles | |||
| Median | 7 (IQR 7–7) | 7 (IQR 7–7) | |
| 7 or more | 74 (81.3) | 83 (86.5) | 0.426 |
| Cumulative dose 200 mg/m2 or above of cisplatin | 0.858 | ||
| Yes | 72 (79.1) | 77 (80.2) | |
| No | 19 (20.9) | 19 (19.8) | |
| Cisplatin dose reduction | |||
| Yes | 7 (7.7) | 11 (11.5) | 0.461 |
| No | 84 (92.3) | 85 (88.5) | |
| Nimotuzumab | – | – | |
| Median | 7 (IQR 7–7) | ||
Adverse events
The clinical adverse events were captured in 180 patients while laboratory adverse events were captured in 182 patients. The adverse events details between the 2 arms are shown in Supplementary Table 2.
DISCUSSION
The results of the current study clarify the importance of treatment intensification in HPV negative oropharyngeal cancers. Locoregional control, progression-free survival and overall survival were improved with the addition of nimotuzumab to cisplatin and radiation. The absolute improvement in the 2 years LRC and PFS were around 20–25 percent. The corresponding improvement in OS was 18 percent. These improvements, in accordance with the ESMO magnitude of clinical benefit scale for curative treatment would classify as “A” [10].
As opposed to HPV related oropharyngeal cancer, HPV negative oropharyngeal cancers have worse prognosis. The median PFS, LRC, and OS in the current study are however, lower than reported in literature from the western world [8, 11, 12], [13–15]. The patient population in the current study had a history of tobacco use (90 percent) with the predominance of stage IV disease (80 percent), which probably resulted in lower survival. Both tobacco and stage IV are known bad prognostic factors [2, 16]. Another factor responsible for poorer outcomes would be the use of weekly cisplatin. However, it is unlikely as the cumulative dose of cisplatin received was 200 mg per M2 or more in nearly 3/4th of the patients. Dose intensification above 200 mg/m2 has questionable benefit [17]. These results in the control arm are similar to the results we previously reported [16].
Addition of nimotuzumab as a radiosensitizer to weekly cisplatin and addition of cetuximab to carboplatin 5-FU resulted in an improvement in outcomes over weekly cisplatin and carboplatin-5 FU in locally advanced head and neck cancers [7, 9]. However, a similar study of the addition of cetuximab to 3 weekly cisplatin was associated with negative results [8]. The probable reason for this discrepancy was the nature of the population in these 3 studies. In our study and the french study, the predominant population was HPV negative while, in the RTOG 0552, the predominant population was HPV positive. We feel that dose intensification would work if the population had poor prognostic factors like HPV negative. Hence, this analysis was performed to study whether addition of nimotuzumab would have larger incremental benefits in a HPV negative population. And indeed it leads to larger incremental benefits as opposed to the whole cohort Supplementary Table 3.
The current study is not without limitations. It is a subgroup analysis. However, an interaction test was performed prior to doing the subgroup analysis, to determine whether nimotuzumab had a differential impact or not. The study had used weekly cisplatin and not 3 weekly cisplatin, and so, the outcomes of the analysis are only applicable for weekly regimen.
Materials and Methods
Patient population and design of the study
This was a phase 3 randomized superiority study conducted between 2012–2018. The study protocol was approved by the institutional ethics committee and the study was conducted in accordance with national (Indian Council of Medical Research) and international guidelines (Good Clinical Practice and Declaration of Helsinki) on human research. The detailed inclusion-exclusion criteria with study protocol are already published [7]. The study enrolled patients with locally advanced head and neck cancer who were planned for curative intent therapy, had normal organ functions, no uncontrolled comorbidities and ECOG PS 0–2. Patients with primary in salivary gland, nasopharynx or thyroid were excluded. For the current analysis, we selected locally advanced oropharyngeal cancer patients who were considered as p16 negative on immunohistochemistry.
Intervention in both arms
The standard arm received radical radiation to a dose of 66–70 Gy with conventional fractionation over 6–7 weeks. Altered fractionation schedules were allowed in both arms if the Biologically equivalent dose (BED) was around 70Gy10. The chemosensitizer used was weekly cisplatin –30 mg/m2. The dose of 30 mg/m2 was selected as it was considered as standard at our centre and had been proven effective compared to radical radiation in a randomized study [18]. In the experimental arm, in addition to cisplatin and radiation, nimotuzumab was administered as a flat dose of 200 mg, over 1 hour in 0.9% normal saline without any premedication. Cisplatin in both arms was administered over 1 hour with adequate antiemetic cover and hydration.
HPV testing
HPV testing was done using p16 IHC. The procedure for performing HPV testing has been already published in the literature [19]. Interpretation of p16 was done in accordance with American pathologist consensus guidelines. Both negative and positive controls were performed while performing p16 IHC for each batch for quality assurance.
Study conduct
All patients, post consenting, underwent screening procedures, which were complete blood count, renal function tests, liver function test, viral serology, pure tone audiometry, dental examination, speech – swallowing function testing, nutritional status examination and evaluation by a social worker for compliance. All patients underwent an examination under anesthesia for mucosal disease assessment and a contrast enhanced computed tomography (CECT) neck with upper thorax for staging. In patients who had N2 nodes, the imaging used as positron emission tomography (PET). The radiation was administered either via conventional 2-D technique or 3-D technique. Use of intensity-modulated radiotherapy was permitted as per physician’s discretion. The patients were assessed each week during the treatment phase. Post-treatment completion at 8 weeks, patients were assessed in a joint clinic with a PET. Further follow up was according to the study protocol. The patients were followed up until death.
Endpoint definition
The primary endpoint was PFS. It was defined as the time in months from randomization until progression. Progression was defined as per RECIST version 1.1. The secondary endpoints were LRC, DFS and OS. Locoregional control was defined as the time in months from randomization till loco-regional progression. Overall survival was defined as the time in months from randomization till death.
Statistical analysis
Descriptive statistics were performed. Nominal and ordinal data between both arms were compared using Fischer’s test. An interaction test was performed between HPV status and outcomes (PFS, DFS, LRC, and OS). Only if the interaction test was positive (P-value of 0.05 or below), which suggested that the addition of nimotuzumab had a differential impact on outcome in accordance with HPV status, further analysis was done on HPV negative patients.
The subgroup had 187 patients. Considering a type 1 error of 5% and a type 2 of 20%, this subgroup was powered to rule out a 20% absolute improvement at 2 years in PFS, which was the primary endpoint.
Kaplan Meier method was used for estimation of the probability of PFS, LRC, and OS in each arm. The median estimates with the 95% confidence interval (CI) were reported. The 95%CI was calculated in accordance with Brookmeyer and Crowley method. The unadjusted hazard ratio (HR) and adjusted HR (adjusted for prognostic factors) with its 95%CI interval were calculated using the COX regression analysis with Efron’s method of tie handling, with CRT arm being considered as reference. The assumptions of proportional hazard model were checked using Schoenfeld residuals and assumptions were met for PFS and LRC. However, the assumption was violated for OS. Hence mean overall survival between the 2 arms were calculated using the restricted mean survival method. The difference between the restricted means between the 2 arms with its 95%CI were calculated. A p-value of 0.05 or below was considered as significant.
Conclusions
The addition of nimotuzumab to weekly cisplatin-radiation improves outcomes inclusive of OS in HPV negative oropharyngeal cancers and this regimen should be considered as standard if 3 weekly cisplatin 100 mg/m2 regimen is not used.
CONFLICTS OF INTEREST
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests. Dr. Noronha reports research grants from Dr. Reddy’s Laboratories Inc, Amgen, Sanofi India Ltd., Intas Pharmaceuticals and Astra Zeneca Pharma India Ltd., outside the submitted work. Dr. Prabhash reports grants from Biocon Ltd, grants from Dr. Reddy’s Laboratories Inc, grants from Fresenius Kabi India Pvt Ltd, grants from Alkem Laboratories, grants from Natco Pharma Ltd, grants from BDR Pharmaceuticals Intl Pvt Ltd, grants from Roche Holding AG, outside the submitted work. All grants were paid to the institution. None of the other authors have anything to declare that may be considered as potential competing interests.
FUNDING
We thank Biocon Ltd and the Tata Memorial Center Research Administration Council for funding this study. The funding agency had no role in design and conduct of the study, collection, management, analysis, and interpretation of the data, preparation, review or approval of the manuscript, and decision to submit the manuscript for publication.
References
1. Parsons JT, Mendenhall WM, Stringer SP, Amdur RJ, Hinerman RW, Villaret DB, Moore-Higgs GJ, Greene BD, Speer TW, Cassisi NJ, Million RR. Squamous cell carcinoma of the oropharynx: surgery, radiation therapy, or both. Cancer. 2002; 94:2967–80. https://doi.org/10.1002/cncr.10567. [PubMed].
2. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tân PF, Westra WH, Chung CH, Jordan RC, Lu C, Kim H, Axelrod R, Silverman CC, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010; 363:24–35. https://doi.org/10.1056/NEJMoa0912217. [PubMed].
3. Stein AP, Saha S, Kraninger JL, Swick AD, Yu M, Lambert PF, Kimple RJ. Prevalence of Human Papillomavirus in Oropharyngeal Cancer: A Systematic Review. Cancer J. 2015; 21:138–46. https://doi.org/10.1097/PPO.0000000000000115. [PubMed].
4. Murthy V, Calcuttawala A, Chadha K, d’Cruz A, Krishnamurthy A, Mallick I, Nair S, Teni T, Pawar S, Talapatra K, Patil A, Bhatt A, Chatterjee S, et al. Human papillomavirus in head and neck cancer in India: current status and consensus recommendations. South Asian J Cancer. 2017; 6:93–98. https://doi.org/10.4103/sajc.sajc_96_17. [PubMed].
5. Pignon JP, Baujat B, Bourhis J. [Individual patient data meta-analyses in head and neck carcinoma: what have we learnt?]. [Article in French]. Cancer Radiother. 2005; 9:31–36. https://doi.org/10.1016/j.canrad.2004.11.002. [PubMed].
6. Nguyen-Tan PF, Zhang Q, Ang KK, Weber RS, Rosenthal DI, Soulieres D, Kim H, Silverman C, Raben A, Galloway TJ, Fortin A, Gore E, Westra WH, et al. Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol. 2014; 32:3858–66. https://doi.org/10.1200/JCO.2014.55.3925. [PubMed].
7. Patil VM, Noronha V, Joshi A, Agarwal J, Ghosh-Laskar S, Budrukkar A, Murthy V, Gupta T, Mahimkar M, Juvekar S, Arya S, Mahajan A, Agarwal A, et al. A randomized phase 3 trial comparing nimotuzumab plus cisplatin chemoradiotherapy versus cisplatin chemoradiotherapy alone in locally advanced head and neck cancer. Cancer. 2019; 125:3184–97. https://doi.org/10.1002/cncr.32179. [PubMed].
8. Ang KK, Zhang Q, Rosenthal DI, Nguyen-Tan PF, Sherman EJ, Weber RS, Galvin JM, Bonner JA, Harris J, El-Naggar AK, Gillison ML, Jordan RC, Konski AA, et al. Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma: RTOG 0522. J Clin Oncol. 2014; 32:2940–50. https://doi.org/10.1200/JCO.2013.53.5633. [PubMed].
9. Tao Y, Auperin A, Sire C, Martin L, Khoury C, Maingon P, Bardet E, Kaminsky MC, Lapeyre M, Chatellier T, Alfonsi M, Pointreau Y, Jadaud E, et al. Improved Outcome by Adding Concurrent Chemotherapy to Cetuximab and Radiotherapy for Locally Advanced Head and Neck Carcinomas: Results of the GORTEC 2007-01 Phase III Randomized Trial. J Clin Oncol. 2018 Jun 7. https://doi.org/10.1200/JCO.2017.76.2518. [Epub ahead of print]. [PubMed]
10. Cherny NI, Dafni U, Bogaerts J, Latino NJ, Pentheroudakis G, Douillard JY, Tabernero J, Zielinski C, Piccart MJ, de Vries EG. ESMO-Magnitude of Clinical Benefit Scale version 1.1. Ann Oncol. 2017; 28:2340–66. https://doi.org/10.1093/annonc/mdx310. [PubMed].
11. Cohen EE, Karrison TG, Kocherginsky M, Mueller J, Egan R, Huang CH, Brockstein BE, Agulnik MB, Mittal BB, Yunus F, Samant S, Raez LE, Mehra R, et al. Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J Clin Oncol. 2014; 32:2735–43. https://doi.org/10.1200/JCO.2013.54.6309. [PubMed].
12. Haddad R, O’Neill A, Rabinowits G, Tishler R, Khuri F, Adkins D, Clark J, Sarlis N, Lorch J, Beitler JJ, Limaye S, Riley S, Posner M. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised phase 3 trial. Lancet Oncol. 2013; 14:257–64. https://doi.org/10.1016/S1470-2045(13)70011-1. [PubMed].
13. Ghi MG, Paccagnella A, Ferrari D, Foa P, Alterio D, Codecà C, Nolè F, Verri E, Orecchia R, Morelli F, Parisi S, Mastromauro C, Mione CA, et al, and GSTTC (Gruppo di Studio Tumori della Testa e del Collo) Italian Study Group. Induction TPF followed by concomitant treatment versus concomitant treatment alone in locally advanced head and neck cancer. A phase II-III trial. Ann Oncol. 2017; 28:2206–12. https://doi.org/10.1093/annonc/mdx299. [PubMed].
14. Bonner JA, Harari PM, Giralt J, Cohen RB, Jones CU, Sur RK, Raben D, Baselga J, Spencer SA, Zhu J, Youssoufian H, Rowinsky EK, Ang KK. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol. 2010; 11:21–28. https://doi.org/10.1016/S1470-2045(09)70311-0. [PubMed].
15. Rischin D, Peters LJ, O’Sullivan B, Giralt J, Fisher R, Yuen K, Trotti A, Bernier J, Bourhis J, Ringash J, Henke M, Kenny L. Tirapazamine, cisplatin, and radiation versus cisplatin and radiation for advanced squamous cell carcinoma of the head and neck (TROG 02.02, HeadSTART): a phase III trial of the Trans-Tasman Radiation Oncology Group. J Clin Oncol. 2010; 28:2989–95. https://doi.org/10.1200/JCO.2009.27.4449. [PubMed].
16. Agarwal JP, Mallick I, Bhutani R, Ghosh-Laskar S, Gupta T, Budrukkar A, Murthy V, Sengar M, Dinshaw KA. Prognostic factors in oropharyngeal cancer—analysis of 627 cases receiving definitive radiotherapy. Acta Oncol. 2009; 48:1026–33. https://doi.org/10.1080/02841860902845839. [PubMed].
17. Ang KK. Concurrent radiation chemotherapy for locally advanced head and neck carcinoma: are we addressing burning subjects? J Clin Oncol. 2004; 22:4657–59. https://doi.org/10.1200/JCO.2004.07.962. [PubMed].
18. Ghosh-Laskar S, Kalyani N, Gupta T, Budrukkar A, Murthy V, Sengar M, Chaukar D, Pai P, Chaturvedi P, D’Cruz A, Agarwal J. Conventional radiotherapy versus concurrent chemoradiotherapy versus accelerated radiotherapy in locoregionally advanced carcinoma of head and neck: results of a prospective randomized trial. Head Neck. 2016; 38:202–07. https://doi.org/10.1002/hed.23865. [PubMed].
19. Bhosale PG, Pandey M, Desai RS, Patil A, Kane S, Prabhash K, Mahimkar MB. Low prevalence of transcriptionally active human papilloma virus in Indian patients with HNSCC and leukoplakia. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016; 122:609–618.e7. https://doi.org/10.1016/j.oooo.2016.06.006. [PubMed].