
Introduction
Black male patients with lung cancer are 1.2 times more likely to die from their disease compared to white male patients, a modest improvement from 1.4 times in the 1990s [1]. In others cancer, a higher mortality rate can be partially explained by factors such as a higher incidence of more aggressive disease among black patients. For example, women with African ancestry are known to develop triple-negative breast cancer at higher rates [2]. A similar link has not been found for lung cancer. While investigation into the molecular composition of lung cancer among black patients has been limited, it continues to be essential to address mortality disparities.
Best practice for the treatment of advanced, non-squamous non-small cell lung cancer (NSCLC) includes identification of targetable or actionable mutations such as in EGFR, ALK, ROS1 and BRAF to guide treatment selection [3]. Programmed death-ligand 1 (PD-L1) assessment is also broadly recommended, as single agent pembrolizumab can be offered as first-line therapy in patients whose tumors express high levels of PD-L1. More recently, high tumor mutational burden (TMB) has been associated with treatment response to immunotherapies in lung cancer [4]. Despite this, molecular testing remains underutilized, with reduced uptake among minorities such as black and Hispanic patients [5, 6]. While several studies have investigated the frequencies of targetable mutations in black patients with NSCLC, these studies have yielded conflicting results [7] and have not included PD-L1, TMB and actionable mutations comprehensively. It therefore remains unclear whether targeted therapies and immunotherapies disproportionately benefit non-black patients, both because of disparities in access to molecular testing as well as potentially higher prevalence of actionable mutations among non-black patients.
We sought to investigate whether differences in the molecular composition of NSCLC among our diverse patient population at an urban academic medical center impact the treatment options available for underserved patients. Since early 2016, all patients with a diagnosis of NSCLC at our institution underwent both targeted sequencing with the UCM-OncoPlus panel [7], as well as PD-L1 immunohistochemistry (IHC), even if the initial cancer diagnosis was made in the inpatient setting, or if patients transferred their care from another center. As an academic, tertiary care medical center located on the south side of Chicago, we are able to offer routine molecular testing that otherwise may not be available to underserved patients in the area. Of note, we focus in this study on “actionable” or “targetable” mutations, which we use to denote molecular alterations which are currently the targets of commercially-available drugs approved for use in NSCLC. In addition, while there is significant heterogeneity in the academic or scientific literature in the terms used to describe race or ethnicity [8], we employ the categories “black,” “white”, “Asian” and “Hispanic or Latino,” as set forth by the National Institutes of Health to describe self-reported race [9].
Results
146 patients were included as follows: 59 (40.4%) black patients, 76 (52.1%) white, 7 Asians (4.8%), 3 Hispanic (2.1%), and one patient of mixed race. Patient characteristics are outlined in Table 1. The majority of patients were stage IV at the time of molecular testing (91 patients, 62.3%). 27 (25.3%) patients were light or never smokers compared to 96 (65.7%) heavy former or current smokers. A higher prevalence of any smoking history was noted among black patients, with 48/53 (90.6%) black patients reporting a smoking history versus 53/87 (60.9%) non-black patients reporting a smoking history (p = 0.003).
Table 1: Patient characteristics
| Characteristic | Black | Non-black | Total number (%) |
|---|---|---|---|
| Gender | |||
| Male | 22 | 44 | 66 (45.2) |
| Female | 37 | 43 | 80 (54.8) |
| Median age at diagnosis | 66 | 67 | 66 years |
| Stage | |||
| I or II | 5 | 15 | 20 (13.7) |
| III | 6 | 24 | 30 (20.5) |
| IV | 38 | 53 | 91 (62.3) |
| Not sufficiently reported | 4 | 1 | 5 (3.4) |
| Histology | |||
| Adenocarcinoma | 49 | 69 | 118 (80.8) |
| Squamous cell carcinoma | 2 | 8 | 10 (6.8) |
| Neuroendocrine | 1 | 1 | 2 (1.4) |
| Rare or mixed features | 4 | 2 | 6 (4.1) |
| Not further differentiated | 3 | 7 | 10 (6.8) |
| Smoking History | |||
| Never smoker | 2 | 23 | 25 (17.1) |
| Light former smoker (<10 py) | 7 | 5 | 12 (8.2) |
| Heavy former smoker (≥10 py) | 33 | 47 | 80 (54.8) |
| Current smoker | 11 | 5 | 16 (10.9) |
| Not sufficiently reported | 6 | 7 | 13 (8.9) |
| Received a TKI | 4 | 16 | 20 (13.7) |
| Received an immunotherapy | 16 | 26 | 42 (28.7) |
| Self-reported race | |||
| Black | 59 (40.4) | ||
| White | 76 (52.1) | ||
| Asian | 7 (4.8) | ||
| Hispanic/Latino | 3 (2.1) | ||
| Mixed | 1 (0.7) |
35 patients had at least one targetable mutation, with EGFR alterations seen in 21 patients, 16 of whom were white, as shown in Table 2. Two white patients had both an EGFR mutation and a CCDC6-RET fusion. Seven black patients had a targetable mutation (11.9%) compared to 24 (31.5%) white patients and 28 total non-black patients (p = 0.005, Fisher’s exact). The presence of a targetable alteration was strongly associated with light or never smoking (p < 0.0001).
Table 2: Summary of molecular alterations
| A | Black | White | Asian | Hispanic/Other | Total |
|---|---|---|---|---|---|
| Targetable Alterations | No. (%) | ||||
| EGFR | 4 | 16 | 1 | 0 | 21 (14.4) |
| BRAF | 0 | 0 | 0 | 1 | 1 (0.1) |
| ERBB2 | 1 | 3 | 0 | 0 | 4 (2.7) |
| MET exon 14 | 2 | 3 | 1 | 0 | 6 (4.1) |
| RET translocation | 0 | 3 | 0 | 0 | 3 (2.1) |
| ALK rearrangement | 0 | 0 | 1 | 0 | 1 (0.1) |
| ROS1 rearrangement | 0 | 1 | 0 | 0 | 1 (0.1) |
| No. (%) | 7 (11.9) | 26 (34.2) | 3 (42.9) | 1 (20.0) | |
| PD-L1 expression | |||||
| <1% | 35 | 37 | 1 | 4 | 77 (52.7) |
| ≥1 to 49% | 9 | 24 | 2 | 0 | 35 (24.0) |
| ≥50% | 15 | 15 | 4 | 0 | 34 (23.2) |
| TMB (mutations/Mb) | 15.3 ± 11.2 | 12.3 ± 16.1 | 6.5 ± 3.0 | 6.9 ± 6.2 | p-value 0.006 |
| Mean ± SD | n = 53 | n = 66 | n = 7 | n = 4 | |
| B | Black | Non-black | p-value | ||
| Targetable Mutations | 7 (11.9) | 28 (32.2) | 0.005 | ||
| High PD-L1 expression (≥50%) | 15 (25.4) | 19 (21.8) | 0.69 | ||
| TMB (mean ± SD) | 15.3 ± 11.2 | 11.5 ± 15.1 | 0.001 | ||
PD-L1 expression was scored as either low (<1%), medium (≥1 to 49%), or high (≥50%) tumor cell expression. Overall, 77 (52.7%) patient tumors had low expression, 35 (24.0%) medium, and 34 (23.2%) high expression. There was no difference in high PD-L1 expression between black patients and non-black patients (p = 0.69, Fisher’s exact). This remained non-significant when the threshold for high PD-L1 expression was lowered to ≥1% (p = 0.23).
Finally, the average TMB was calculated for each group (Table 2). There was a significant difference in TMB among the four racial groups (p = 0.006,). Black patients had the highest TMB, with a mean of 15.3 mutations/Mb, compared to a mean of 11.5 mutations/Mb for non-black patients (p = 0.001, Mann-Whitney U test) (Figure 1). When stratified according to smoking status, we found that the results were no longer significant. In a multivariable regression model, we found that smoking, rather than black race, was significantly associated with a higher mean TMB (p = 0.003) with a non-significant interaction between black race and smoking (p = 0.8 for the interaction coefficient).
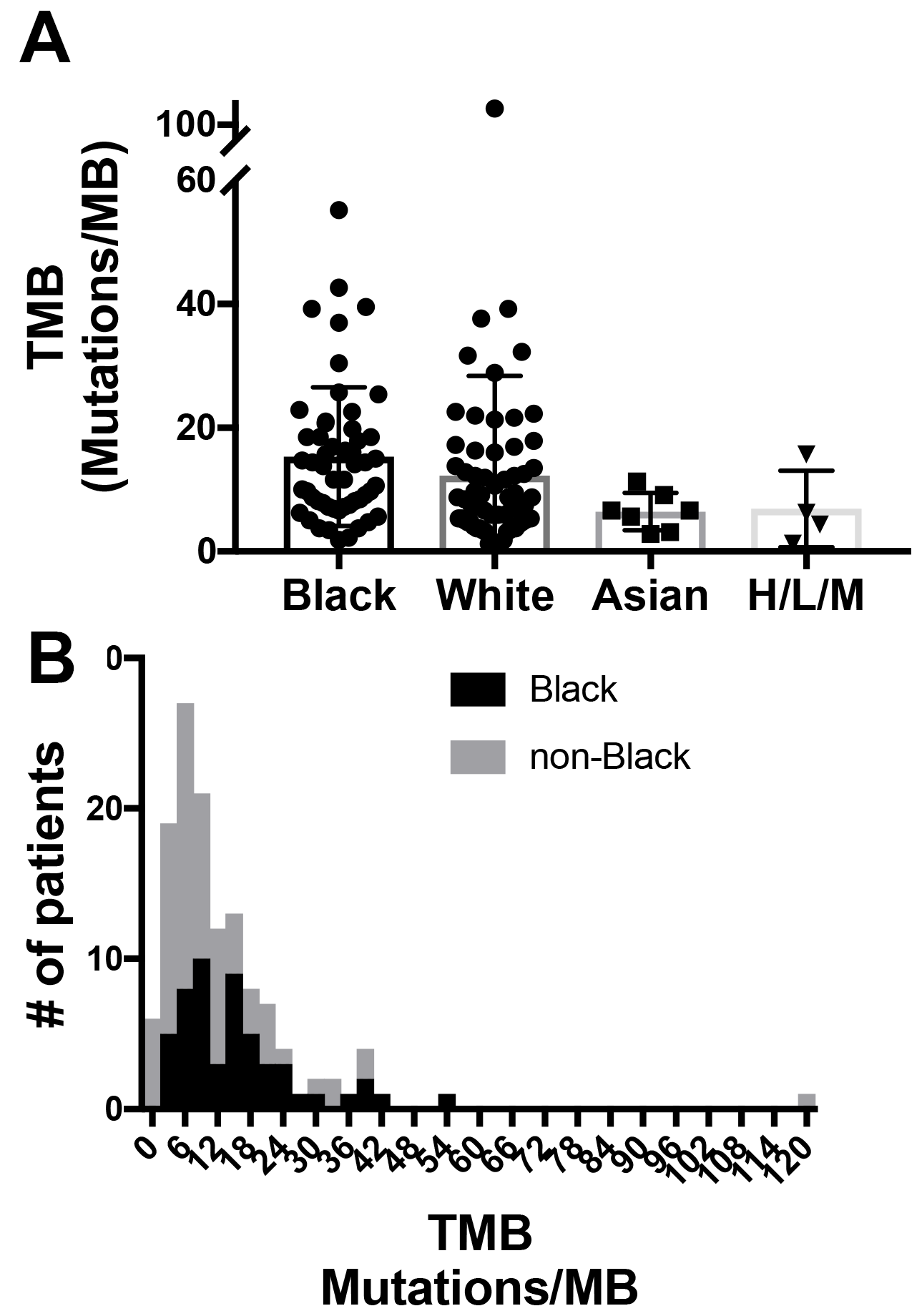
Figure 1: Distribution of tumor mutational burden. (A) demonstrates the distribution of tumor mutation burden (TMB) (mutations/ megabase or MB) for each racial group. Sample size for each group is noted on the X-axis. p = 0.006 (Kruskal-Wallis). H/M designates “Hispanic/mixed”. These categories were combined due to small numbers. (B) is a histogram of the distribution of TMB for black vs. non-black patients, with TMB on the X-axis. p = 0.001 (Mann-Whitney U test).
Given that this study included patients with all stages of disease, we sought to ascertain whether the proportion of tumors with targetable mutations or higher TMB was potentially associated with stage. We found no difference between average TMB between metastatic and non-metastatic disease groups (11.3 vs. 16.3, p = 0.25 by Mann-Whitney U), or in the proportion of tumors with a targetable mutation. 8/50 (16.0%) patients with non-metastatic disease had a targetable mutation, compared to 27/91 (29.6%) patients with metastatic disease (p = 0.07).
DISCUSSION
Our study incorporates PD-L1 testing, TMB quantification and clinically actionable mutation analysis together, which best reflects the comprehensive molecular testing recommended to guide treatment decisions. With fewer actionable mutations, the implications of our study are that black patients have less opportunity to benefit from targeted therapies that are commercially available, which significantly extend survival for eligible patients. Black and non-black patients, conversely, may be similarly eligible for immunotherapies. In fact, only 4/59 (6.8%) black patients among our patients received a tyrosine-kinase inhibitor among our patients, compared to 14 (18.4%) white patients in the cohort. In comparison, nearly equal proportions received immunotherapies (27% of black patients and 25% of white patients). Of note, some patients with actionable mutations or high PD-L1 expression may not have received a targeted therapy or immunotherapy if they presented with localized disease as this was not the standard of care at the time. Furthermore, fewer patients in our cohort at the time of data collection received an immunotherapy than would today, since the period of data collection preceded expanded U. S. Food and Drug Administration (FDA) approval for the use of immunotherapies in NSCLC. The expanded indications for using immunotherapies in NSCLC available today are likely to benefit both black and non-black patients.
Characterizing the frequencies of targetable mutations in NSCLC tumors from black patients has been of significant interest, with EGFR the most commonly investigated. Several studies report a lower frequency of EGFR mutations in tumors from black patients [10–12], even after correcting for smoking status [13], while others did not show a difference [14–16]. Compared to several of these studies, our study directly compares patients from different racial groups using synchronous testing from a single institution, which reduces potential sources of error. Similar methodology was employed in a 2017 study by Campbell, et al. [17].
The molecular differences in our study population appear to be driven by a higher prevalence of smoking in our urban black population compared to other groups. In fact, the discrepancy in mutation frequency reported among published studies are likely due to variable proportions of smokers in each study [7]. Smoking prevalence will undoubtedly vary across institutions and regions and the patterns of smoking in our population do not necessarily reflect nationwide trends.
Our study has several limitations, including smaller sample size, especially of Asian and Hispanic patients. Because of this, our study is not meant to conclusively demonstrate differences in molecular composition among patients. In addition, the retrospective nature of our study curtailed the ability to precisely correlate molecular alterations to treatment response, especially as patients may have received combination or sequential therapies. However, even with a smaller sample size, differences in molecular alterations between black and non-black patients were still elucidated. Furthermore, our sample confirmed several trends that have been demonstrated by multiple larger studies and which are embraced in the literature, including that higher TMB is associated with smoking [18], and that targetable mutations are found more commonly in non-smokers [19]. These findings offer assurance of the validity of our sample, despite its smaller size.
Methods
The University of Chicago Institutional Review Board granted an exemption for this retrospective study. All patients of any tumor stage at any point of their treatment with a pathological diagnosis of NSCLC who had a UCM-OncoPlus performed from March 2016 to October 2017 were screened. Patients were included if they had PD-L1 IHC as well as UCM-OncoPlus results. Electronic medical records (EMR) were reviewed with clinical data extracted and identifying personal information removed. Smoking history was characterized by current vs. former use and heavy (smoking history ≥ 10 pack-years) vs. light use. Of note, race was self-reported by patients. “Hispanic or Latino” is listed as a category for race in our EMR. Patients can choose to further specify ethnicity as a separate category, but fewer do so. Stage was also determined as the stage denoted in the EMR at the time molecular testing was performed.
Targeted next-generation sequencing was ordered by clinicians directly caring for patients. This is performed on tumor samples using the University of Chicago’s validated panel, the UCM-OncoPlus, which covers 1,213 cancer-related genes [20]. We defined “targetable” mutations as druggable alterations in EGFR (exon 18–21 alterations), BRAF (V600E), ERBB2, MET exon 14 skip mutations, RET translocations, and ALK and ROS1 rearrangements that are sensitizing to FDA-approved agents. TMB was quantified as mutations/Mb using UCM-OncoPlus results. Briefly, variants were restricted to genes with >10% variant allele frequency. Inherited SNPs were removed using 1000 Genome and EXAC databases. Genes with pseudogene noise and sequencing artifacts were removed from the analysis. Finally, a COSMIC rescue was performed using a >10 COSMIC entry threshold on variants with lower than 0.1% ExAC frequency. Tumor samples also underwent IHC with the Dako PD-L1 clone 28.8 antibody (Agilent, Santa Clara, CA, USA), with expression quantified by two pathologists (ME and AH).
Statistical analysis was carried out by a biostatistician (JC) using SAS software, version 9.4. All p-values are two-sided with significance cut off of ≤0.05.
Conclusions
Our study demonstrates a lower frequency of actionable mutations but a higher TMB among black patients in our urban, racially diverse population. The driving factors behind this pattern is likely the higher prevalence of smoking among black patients compared to non-black patients in our population. Our results do not suggest that black patients should be profiled as smokers or empirically offered immunotherapies. Due to our smaller sample size, our results are also not intended to be used as a definitive synopsis of the difference in molecular alterations between black and non-black patients. Instead, our study instead serves as a proof of concept that differences in molecular alterations between black and non-black patients with NSCLC exist and do impact the opportunities of patients to receive novel therapies. These results also demonstrate the necessity of improving access to guideline-directed molecular testing for all patients, especially those who may not have had access to such testing in underserved communities. Addressing sociodemographic inequalities, including access to guideline-directed molecular testing, inclusion in biomarker-discovery and therapeutic clinical trials, and continued investigation into the molecular analysis of NSCLC in black patients, is essential to reducing the excess mortality from NSCLC that black patients experience.
Abbreviations
PD-L1: Programmed death-ligand 1; NSCLC: non-small cell lung cancer; TMB: tumor mutational burden; IHC: immuno-histochemistry; EMR: electronic medical records; FDA: U.S. Food and Drug Administration.
CONFLICTS OF INTEREST
The authors have no conflicts of interest, financial or otherwise, to disclose.
FUNDING
This work was supported by the University of Chicago Comprehensive Cancer Center.
References
1. Society AC. Cancer Facts & Figures 2017. American Cancer Society. Atlanta (GA). 2017.
2. Huo D, Ikpatt F, Khramtsov A, Dangou JM, Nanda R, Dignam J, Zhang B, Grushko T, Zhang C, Oluwasola O, Malaka D, Malami S, Odetunde A, et al. Population differences in breast cancer: survey in indigenous African women reveals over-representation of triple-negative breast cancer. J Clin Oncol. 2009; 27:4515–21. https://doi.org/10.1200/JCO.2008.19.6873. [PubMed].
3. Lindeman NI, Cagle PT, Aisner DL, Arcila ME, Beasley MB, Bernicker EH, Colasacco C, Dacic S, Hirsch FR, Kerr K, Kwiatkowski DJ, Ladanyi M, Nowak JA, et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. J Mol Diagn. 2018; 20:129–59. https://doi.org/10.1016/j.jmoldx.2017.11.004. [PubMed].
4. Hellmann MD, Ciuleanu TE, Pluzanski A, Lee JS, Otterson GA, Audigier-Valette C, Minenza E, Linardou H, Burgers S, Salman P, Borghaei H, Ramalingam SS, Brahmer J, et al. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. N Engl J Med. 2018; 378:2093–104. https://doi.org/10.1056/NEJMoa1801946. [PubMed].
5. Lynch JA, Berse B, Rabb M, Mosquin P, Chew R, West SL, Coomer N, Becker D, Kautter J. Underutilization and disparities in access to EGFR testing among Medicare patients with lung cancer from 2010 - 2013. BMC Cancer. 2018; 18:306. https://doi.org/10.1186/s12885-018-4190-3. [PubMed].
6. Riaz F, Presley CJ, Chiang AC, Longtine JA, Soulos PR, Adelson KB, Herbst RS, Nussbaum NC, Sorg RA, Abernethy AP, Agarwala V, Gross CP. Disparities in broad-based genomic sequencing for patients with advanced non-small cell lung cancer. J Geriatr Oncol. 2019; 10:669–72. https://doi.org/10.1016/j.jgo.2019.01.016. [PubMed].
7. Clifford BT, Fu P, Pennell NA, Halmos B, Leidner RS. EGFR molecular testing in African-American non-small cell lung cancer patients - a review of discrepant data. Transl Lung Cancer Res. 2013; 2:251–55. https://doi.org/10.3978/j.issn.2218-6751.2013.01.04. [PubMed].
8. Zhang F, Finkelstein J. Inconsistency in race and ethnic classification in pharmacogenetics studies and its potential clinical implications. Pharm Genomics Pers Med. 2019; 12:107–23. https://doi.org/10.2147/PGPM.S207449. [PubMed].
9. Health NCfCaI. Racial and Ethnic Categories and Definitions for NIH Diversity Programs and for Other Reporting Purposes. National Institutes of Health. Bethesada (Maryland). 2015.
10. Leidner RS, Fu P, Clifford B, Hamdan A, Jin C, Eisenberg R, Boggon TJ, Skokan M, Franklin WA, Cappuzzo F, Hirsch FR, Varella-Garcia M, Halmos B. Genetic abnormalities of the EGFR pathway in African American Patients with non-small-cell lung cancer. J Clin Oncol. 2009; 27:5620–26. https://doi.org/10.1200/JCO.2009.23.1431. [PubMed].
11. Yang SH, Mechanic LE, Yang P, Landi MT, Bowman ED, Wampfler J, Meerzaman D, Hong KM, Mann F, Dracheva T, Fukuoka J, Travis W, Caporaso NE, et al. Mutations in the tyrosine kinase domain of the epidermal growth factor receptor in non-small cell lung cancer. Clin Cancer Res. 2005; 11:2106–10. https://doi.org/10.1158/1078-0432.CCR-04-1853. [PubMed].
12. Araujo LH, Lammers PE, Matthews-Smith V, Eisenberg R, Gonzalez A, Schwartz AG, Timmers C, Shilo K, Zhao W, Natarajan TG, Zhang J, Yilmaz AS, Liu T, et al. Somatic Mutation Spectrum of Non-Small-Cell Lung Cancer in African Americans: A Pooled Analysis. J Thorac Oncol. 2015; 10:1430–36. https://doi.org/10.1097/JTO.0000000000000650. [PubMed].
13. Bauml J, Mick R, Zhang Y, Watt CD, Vachani A, Aggarwal C, Evans T, Langer C. Frequency of EGFR and KRAS mutations in patients with non small cell lung cancer by racial background: do disparities exist? Lung Cancer. 2013; 81:347–53. https://doi.org/10.1016/j.lungcan.2013.05.011. [PubMed].
14. Yamaguchi N, Vanderlaan PA, Folch E, Boucher DH, Canepa HM, Kent MS, Gangadharan SP, Majid A, Kocher ON, Goldstein MA, Huberman MS, Costa DB. Smoking status and self-reported race affect the frequency of clinically relevant oncogenic alterations in non-small-cell lung cancers at a United States-based academic medical practice. Lung Cancer. 2013; 82:31–37. https://doi.org/10.1016/j.lungcan.2013.07.013. [PubMed].
15. Reinersman JM, Johnson ML, Riely GJ, Chitale DA, Nicastri AD, Soff GA, Schwartz AG, Sima CS, Ayalew G, Lau C, Zakowski MF, Rusch VW, Ladanyi M, Kris MG. Frequency of EGFR and KRAS mutations in lung adenocarcinomas in African Americans. J Thorac Oncol. 2011; 6:28–31. https://doi.org/10.1097/JTO.0b013e3181fb4fe2. [PubMed].
16. Cote ML, Haddad R, Edwards DJ, Atikukke G, Gadgeel S, Soubani AO, Lonardo F, Bepler G, Schwartz AG, Ethier SP. Frequency and type of epidermal growth factor receptor mutations in African Americans with non-small cell lung cancer. J Thorac Oncol. 2011; 6:627–30. https://doi.org/10.1097/JTO.0b013e31820a0ec0. [PubMed].
17. Campbell JD, Lathan C, Sholl L, Ducar M, Vega M, Sunkavalli A, Lin L, Hanna M, Schubert L, Thorner A, Faris N, Williams DR, Osarogiagbon RU, et al. Comparison of Prevalence and Types of Mutations in Lung Cancers Among Black and White Populations. JAMA Oncol. 2017; 3:801–09. https://doi.org/10.1001/jamaoncol.2016.6108. [PubMed].
18. Alexandrov LB, Ju YS, Haase K, Van Loo P, Martincorena I, Nik-Zainal S, Totoki Y, Fujimoto A, Nakagawa H, Shibata T, Campbell PJ, Vineis P, Phillips DH, Stratton MR. Mutational signatures associated with tobacco smoking in human cancer. Science. 2016; 354:618–22. https://doi.org/10.1126/science.aag0299. [PubMed].
19. Singal G, Miller PG, Agarwala V, Li G, Kaushik G, Backenroth D, Gossai A, Frampton GM, Torres AZ, Lehnert EM, Bourque D, O’Connell C, Bowser B, et al. Association of Patient Characteristics and Tumor Genomics With Clinical Outcomes Among Patients With Non-Small Cell Lung Cancer Using a Clinicogenomic Database. JAMA. 2019; 321:1391–99. https://doi.org/10.1001/jama.2019.3241. [PubMed].
20. Kadri S, Long BC, Mujacic I, Zhen CJ, Wurst MN, Sharma S, McDonald N, Niu N, Benhamed S, Tuteja JH, Seiwert TY, White KP, McNerney ME, et al. Clinical Validation of a Next-Generation Sequencing Genomic Oncology Panel via Cross-Platform Benchmarking against Established Amplicon Sequencing Assays. J Mol Diagn. 2017; 19:43–56. https://doi.org/10.1016/j.jmoldx.2016.07.012. [PubMed].