
Introduction
Breast cancer is the most commonly diagnosed cancer and the second leading cause of cancer death in women [1]. Conventional treatment options for metastatic breast cancer (MBC) include endocrine therapy, targeted therapy and cytotoxic chemotherapy, all of which have demonstrated limited treatment response and duration. More recently, there has been increasing recognition of the key role of the host immune response in tumor response. Immune checkpoint inhibitors (ICI) have found increasing use since the first FDA approval of ipilumumab for metastatic melanoma in 2011. Multiple ICIs have now been developed and approved in other disease sites. Tremelimumab is a fully humanized monoclonal antibody targeting the checkpoint receptor CTLA-4.
Despite the remarkable activity of ICI in some settings, most patients fail to respond. In triple negative breast cancer (TNBC), overall response rates (ORR) for pembrolizumab, avelumab, and atezolizumab are in the range of 2.8%–26%, although durable responses have been reported [2–5]. Preclinical studies suggest that ionizing radiation (IR) can enhance the systemic antitumor immune response through multiple mechanisms. IR leads to cell death and subsequent release of tumor antigens as well as upregulation of MHC class I molecules, which may augment the activation of tumor-specific cytotoxic T cell and NK cell responses [6–9]. IR induced cytoplasmic double-stranded DNA is sensed by the cyclic GMP-AMP synthase (cGAS)-stimulator of interferon genes (STING) pathway to induce IFN-I, a key mediator of dendritic cell recruitment and maturation [10]. In the tumor microenvironment, proinflammatory chemotactic factors induced by IR also enhance recruitment of effector T cells [11, 12] and antigen presenting cells [7, 13–15]. In preclinical models of breast cancer, tumors unresponsive to anti-CTLA4 antibody are sensitized following IR [16]. These preclinical studies provide a strong rationale for combining radiotherapy (RT) and ICI to overcome immunotherapy resistance in MBC. We therefore performed an investigator-initiated phase I study to further evaluate the safety of this combination strategy in human subjects with MBC.
Results
Patient characteristics
From July 2010 to October 2011, 6 female patients were enrolled. Their characteristics are summarized in Table 1. Median age was 45 years. None had significant comorbidities at study entry. Five patients had hormone receptor-positive MBC, 1 had recurrent metastatic triple negative breast cancer (TNBC) with an original diagnosis of hormone receptor-positive breast cancer. HER2-positive disease was seen in 1 patient; 2 patients had unknown HER2 status (their pathology specimens were obtained externally in 1997 and 2001 and were unavailable for review). Two patients presented with de novo metastatic disease; 4 had recurrent metastatic disease, with a median time to relapse of 9.0 years.
Table 1: Baseline characteristics at study enrollment
| Clinicopathologic features | n = 6 |
|---|---|
| Median age | 45.0 [range 42.6, 60.2] |
| Family history for breast or ovarian cancer | |
| No | 4 |
| Yes | 2 |
| De novo metastatic disease | |
| No | 4 |
| Median time to metastatic relapse* | 9.0 years [range 2.9, 12.6] |
| Yes | 2 |
| ECOG performance status at enrollment | |
| 0 | 0 |
| 1 | 6 |
| 2 | 0 |
| 3 | 0 |
| 4 | 0 |
| Histology | |
| Ductal | 6 |
| Lobular | 0 |
| Histopathology grade | |
| 1 | 0 |
| 2 | 2 |
| 3 | 2 |
| Unknown | 2 |
| ER/PR | |
| Positive | 5 |
| Negative | 1 |
| HER2 | |
| Positive | 1 |
| Negative | 3 |
| Unknown | 2 |
| Number of metastatic sites | |
| 1 | 0 |
| 2 | 2 |
| 3 | 3 |
| 4 | 1 |
| Presence of visceral metastases | 5 |
| Previous radiotherapy | |
| No | 2 |
| Yes | 4 |
| Previous endocrine therapy | |
| No | 4 |
| Yes | 2 |
| Previous lines of palliative chemotherapy | |
| 0 | 1 |
| 1 | 0 |
| 2 | 3 |
| ≥3 | 2 |
Most patients had visceral organ involvement and received prior chemotherapy such as taxane, capecitabine, epirubicin, platinum and cyclophosphamide. One patient received sunitinib plus herceptin as part of a clinical trial prior to enrollment. Two patients previously received endocrine therapy (tamoxifen). The number of subsequent therapies ranged from 0-6, and included endocrine and chemotherapy regimens, such as vinorelbine, gemcitabine, capecitabine and cyclophosphamide.
Dose escalation and determination of MTD
Three subjects received tremelimumab at dose level 1 (3 mg/kg). As no DLTs occurred at this level, the trial escalated to the next dose level. Among the 3 patients dosed at level 2 (6 mg/kg), 1 developed grade 3 confusion and presyncope, which constituted a DLT. According to the study protocol, cohort expansion with another 3 patients at dose level 2 would be required to determine MTD. Unfortunately, this trial was not able to meet target accrual. One patient (subject 4) received a subsequent dose of tremelimumab at dose level 2 at the investigator’s discretion for ongoing stable disease (SD), 90 days after the first dose.
Toxicities
Toxicities are shown in Table 2. Four patients (67%) developed grade >3 toxicity, which included fatigue, pathological fracture, confusion/presyncope and asymptomatic lymphopenia. Two of these 4 patients were dosed at level 1 (pathological fracture, lymphopenia, and fatigue); the other 2 were dosed at level 2 (confusion and presyncope, lymphopenia). There were no grade 4 or 5 adverse events. One patient discontinued the study due to a pathologic fracture 7.1 weeks after receiving tremelimumab, requiring urgent surgery. One patient experienced grade 3 confusion and presyncope (DLT)approximately 3 weeks following therapy, which required intravenous hydration in hospital.
Table 2: Adverse events
| Adverse events | Grade 1 n | Grade 2 n | Grade 3 n | Grade 4 n |
|---|---|---|---|---|
| Diarrhea | 1 | 0 | 0 | 0 |
| Rash | 2 | 0 | 0 | 0 |
| Fatigue | 2 | 0 | 1 | 0 |
| Pathologic fracture from radiated site | 0 | 0 | 1 | 0 |
| Dyspnea | 1 | 0 | 0 | 0 |
| Anemia | 0 | 1 | 0 | 0 |
| Neutropenia | 0 | 1 | 0 | 0 |
| Lymphopenia | 1 | 1 | 3 | 0 |
| Confusion, presyncope* | 0 | 0 | 1 | 0 |
Five of 6 patients developed grade 1-3 lymphopenia within a median of 0.9 weeks (range 0.7, 1.7) following tremelimumab, whereas neutropenia occurred in only 1 patient. There were no transaminitis, renal dysfunction or endocrinopathies following treatment. Other common toxicities included fatigue (50%) and rash (33%), occurring within 8 weeks following therapy. Grade 1 diarrhea and dyspnea each occurred in 1 patient approximately 1 week after receiving tremelimumab.
Efficacy
As shown in Table 3, overall disease control rate was 33%; however, there were no objective responses. One patient (subject 4) had SD for more than 6 months. At data cutoff (January 1, 2019), median follow up after tremelimumab administration was 27.0 months (4.8–101.7). For the 3 patients who were alive at the last visit, median follow up was 41.6 months (37.3–101.7). Median PFS was 1.5 months, and Median OS was 50.8 months from date of MBC diagnosis, and 27.0 months from tremelimumab administration.
Table 3: Treatment outcomes of the study cohort
| Subject # | Receptor status | Previous therapy | Trial RT | Study drug | Efficacy | Worst AE | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ER/PR | HER2 | RT | Systemic therapy regimen | Surg | Site | Dose (Gy) | # | Time to trial discontinuation (mo) | Dose mg (mg/kg) | Number of doses | Reason for DC | Best OR+ | OS1* (mo) | OS2** (mo) | PFS** (mo) | Grade | Type | |
| 1 | + | NA | Yes | None | Yes | right humerus | 2000 | 5 | 2.2 | 195.0 (3) | 1 | PD | SD | 103.4 | 94.0 | 2.8 | 1 | Diarrhea, rash, fatigue |
| 2 | + | NA | Yes | Tamoxifen Docetaxel, capecitabine | Yes | T4 | 2000 | 5 | 1.4 | 140.7 (3) | 1 | SAE | PD | 53.9 | 36.9 | 1.7 | 3 | T4 pathologic fracture, lymphopenia |
| 3 | + | + | No | Sutent + herceptin (trial), docetaxel + herceptin, adrimaycin, taxol + HKI-272 (trial), tamoxifen | No | T spine | 2000 | 5 | 1.5 | 239. 1 (3) | 1 | PD | PD | 53.9 | 16.7 | 1.6 | 3 | Fatigue |
| 4 | + | - | No | Docetaxel Abraxane | Yes | right ribs | 2000 | 5 | 6.1 | 385.2 (6), 360.6 (6) | 2 | PD | SD | 47.7 | 41.6 | 6.1 | 2 | Neutropenia |
| 5 | -^ | - | Yes | Cisplatin + gemcitabine, Cyclophosphamide+ veliparib (trial) | Yes | left chest nodule | 2000 | 5 | 1.3 | 357.6 (6) | 1 | PD | PD | 9.7 | 4.8 | 1.5 | 3 | Lymphopenia |
| 6 | + | - | Yes | Tamoxifen capecitabine | No | left femur | 2000 | 5 | 0.9 | 414.6 (6) | 1 | PD | PD | 32.5 | 16.2 | 0.9 | 3 | Lymphopenia, confusion and presyncope; grade 2 anemia |
Subject 1 survived more than 8 years (101 months) after receiving tremelimumab. Following disease progression (PD), this patient received endocrine therapy (letrozole for 6 years then tamoxifen for more than 2 years) and remains on tamoxifen at the last follow up. Unlike other subjects, subject 1 did not receive any palliative systemic therapy prior to enrollment.
Correlative immune profiling
Immune profiling by flow cytometry was performed on prospectively collected peripheral blood mononuclear cells. No consistent changes in CD4+ or CD8+ T cell populations were seen across the baseline, week 1, week 2, week 3 and week 4 samples. CD28 expression remained largely stable on CD8+ T cells, however in patient 6, CD28 expression decreased from 92% at baseline to 62% at week 4. The percentage of Ki67+ proliferating regulatory T cells (Tregs: CD3+CD4+FOXP3+ CD25+ CD127–) seemed to increase at week 1 for patients 1–5 (from <12% to up to 36%) then decreased close to baseline in most patients (Figure 1). Overall, there were no notable trends in our flow cytometric analyses that were associated with SD versus PD.
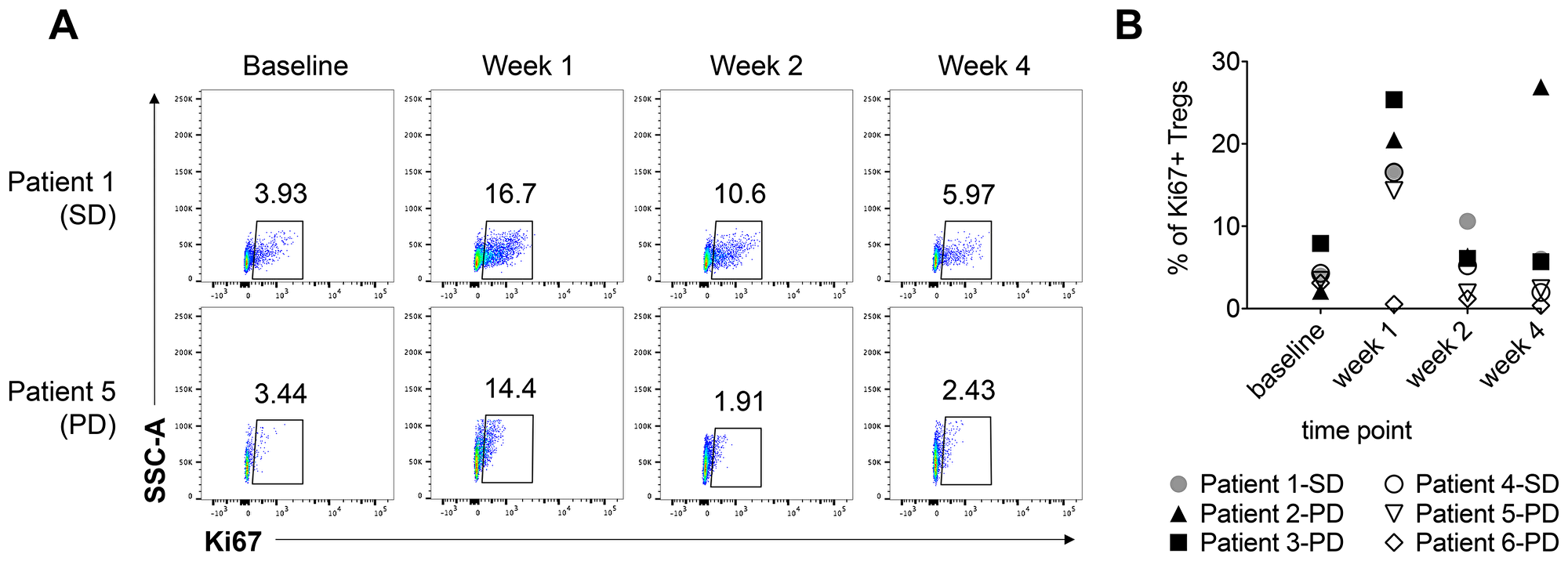
Figure 1: The percentage of Ki67+ regulatory T cells increases at 1 week post-radiation therapy and tremelimumab treatment. The percentage of Ki67+ Tregs (CD3+CD4+FOXP3+CD25+CD127-) in PBMCs isolated from serial blood samples was analyzed by flow cytometry. (A) Representative Ki67 staining in the Treg compartment at baseline, week 1, week 2, and week 4 is presented for two patients, and the percentage of Ki67+ cells is indicated for each time point. (B) The percentage of Ki67+ Tregs at the indicated timepoints is shown for all six patients. The best response for each patient is indicated in the figure legend. SD = stable disease; PD = progressive disease.
Neutrophil to lymphocyte ratio (NLR) was also explored. Interestingly, 3 subjects (subject 2, 5 and 6) had relatively higher pretreatment NLR (>4) and developed significant elevation of NLR (>10) within 3 weeks following tremelimumab therapy, and all 3 patients developed PD. The 2 patients who achieved SD had lower pretreatment NLRs (1.8 in subject 1; 1.1 in subject 4) than others (2.6 to 6.3), and maintained NLR <2 through week 4 following tremelimumab.
DISCUSSION
In 2012, Postow et al first described a patient whose metastatic melanoma regressed upon treatment with ipilimumab and concurrent palliative RT of 28.5 Gy [17]. Since this publication, other similar series have emerged [18–20]. To our knowledge, the only phase III study using this combination strategy with published results is CA184-043. This trial demonstrated that ipilimumab (anti-CTLA4 antibody) plus to a conservative dose of palliative bone-directed RT (8 Gy × 1), which did not improve overall survival (OS) in heavily pre-treated metastatic prostate cancer patients, however treatment was tolerable [21].
With the ongoing interest in this combination strategy, the safety profile of ICI plus higher dose RT requires systematic and prospective evaluation. Although our study was unable to meet target accrual to determine the MTD, tremelimumab at 3 mg/kg did not induce any DLTs and therefore appears safe and feasible to combine with RT. Existing studies also report acceptable safety profile [22, 23], with grade 3 or 4 toxicity [21, 24, 25] similar to ICI monotherapy [26]. Follow up of prior studies was generally 6 months or less [22, 23]. Our longer follow up provides additional assurance that this combination approach is feasible.
The most common toxicity was lymphopenia, all occurring within 2 weeks following tremelimumab. In 3 of the 5 patients, lymphopenia was grade 3. Lymphocytes are radiosensitive [27]. Interestingly, subject 1 did not develop lymphopenia and had prolonged OS, with ongoing disease stability with endocrine therapy 8 years post-progression from study treatment. Subject 4, who had only grade 1 lymphopenia, had the longest duration of disease control. All other patients with grade >1 lymphopenia had PD within 1.5 months of therapy. Severe radiation-induced lymphopenia [28–30], high NLR pre- and post-treatment [31, 32] are known to correlate with poor prognosis. Lymphopenia and high NLR may be markers of poor T cell reserve and therefore associate with lower response to ICI. Other toxicities included a T4 pathological fracture at 7 weeks in subject 2, highlighting the need for special caution in treating large spinal metastases with this combination approach, especially when considering stereotactic body radiation therapy. No new safety signals were detected otherwise.
The best ORR was SD, and no abscopal effects were observed. One patient had SD over 6 months, which suggests durable responses are possible with this combination strategy. Although our sample size was too small to discern any definitive association, ICI may be more effective in earlier treatment settings. Notably, subject 1 with the exceptionally long OS had no prior therapies at enrollment, unlike other subjects. Subject 4 had more prolonged disease control, and received only 2 lines of prior therapy. As chemotherapy suppresses the immune system, patients who are less pre-treated likely have a more intact repertoire of immune cells which are sensitive to activation by ICI. Post ICI therapy, chemotherapy may produce superior antitumor activity via an increased number of antigen-specific CD8+ T cells within the tumor microenvironment [33, 34]. Retrospective studies suggest chemotherapy has a higher response rate pre-ICI relative to the post-ICI setting [35, 36]. In the Keynote-086 trial, pembrolizumab showed a much higher ORR in TNBC patients who were previously untreated (21.4%, cohort B), compared with those who received prior chemotherapy (5.3%, cohort A) [37, 38]. Similar findings of favorable responses in treatment-naïve patients were also seen with atezolizumab [3]. Interestingly, although the CA184-043 trial did not demonstrate improved OS overall, there was a significant benefit in patients with low burden, non-visceral metastatic disease, suggesting RT plus ICI may be more effective in less advanced disease [21]. Further research is warranted to elucidate the optimal treatment setting of this combination strategy.
Following PD on study, 3 subjects were alive at the last follow up. Subject 1 survived at leastmore than 8 years on endocrine therapies, subject 2 and 3 had ≥ 5 lines of subsequent therapies and survived for at leastmore than 48 months after since diagnosis of MBC. This is compared to a median of 3 lines of palliative therapy [39] and median OS of 27-37 months in other contemporary series [39, 40]. This could reflectThere could be some selection bias for younger patients with excellent performance status and more favorable disease biology, as evident from the exceptionally long median time to recurrence in those with recurrent MBC. However, despite short PFS on study treatment, it is unknown whether the combination strategy of ICI plusand RT contributed to the long median OS by augmenting disease activity or response post progression.
We did not identify any major trends in the correlative analysis of PBMCs, however patients 1–5 exhibited a notable increase in the percentage of proliferating (Ki67+) Tregs at week 1 post-treatment. Although PBMCs may not be representative of the immune response in the tumor, preclinical experiments have found more robust Treg proliferation in comparison to other T cell subsets in the tumor microenvironment [41]. Tregs are more radio-resistant than other T cells [42], and increasing Treg populations in peripheral blood following chemotherapy and RT has been observed [43, 44]. The radio-resistance of Tregs may preferentially select for survival of these cells post-radiotherapy, which could result in an increased proportion of proliferating Tregs at week 1. These Tregs are able to not only survive the effect of IR, but also retain proliferative potential given the expression of Ki67. Whether the increased percentage of proliferating Tregs at week 1 reflects other factors such as activation of immunosuppression pathways by RT, and the non-immunogenic phenotype of the tumor itself, remains unclear. Interestingly, the percentage and number of reconstituting Tregs in the peripheral blood have been negatively associated with treatment response [45, 46]. Consistent with the increased proportion of Ki67+ cells in the Treg compartment post-treatment, the overall frequency of Tregs increased post-treatment in patients 1, 3, and 4; but not by more than two-fold. There is data to suggest that hyper-activation of Tregs can result in Treg-specific apoptosis in the tumor microenvironment [47]. It is possible then that these Ki67+ Tregs go on to die, but we cannot make this conclusion based on our immune profiling data alone. In patients 1–5, where we observed an increase in the percentage of Ki67+ Tregs, the proportion of Tregs in the peripheral blood does not decrease below baseline levels by week 4. Furthermore, higher tumor-infiltrating CD8/Treg ratios have been linked with better outcomes in some breast cancers [48, 49]. We observed less than two-fold increases in the proportion of Tregs in patients 1, 3 and 4, and accordingly, less than two-fold decreases in the CD8/Treg ratio (as percentages of CD3+ T cells). The proliferation and frequency of Tregs within the tumor microenvironment – in addition to the tumor-infiltrating CD8/Treg ratio – after treatment with radiation and tremelimumab, would be an interesting biomarker to evaluate in future studies.
Future investigations are also needed to define the optimal strategy of combining RT and immunotherapy. Current evidence suggests fractionated RT [8, 50, 51] and RT doses >10Gy, such as those used in our study, achieve enhanced systemic antitumor immune responses [17, 52, 53]. Concurrent ICI and RT is favored over sequential administration [54, 55], and multiple doses of ICI are likely required to mount a meaningful systemic immune response [56]. In our study, most patients received only 1 dose of tremelimumab, which may be insufficient to produce synergy. Proton radiation, which spares surrounding normal tissue better than photon therapy, and hypofractionation of RT (used in this study) may better preserve peripheral lymphocytes and synergize better with ICI [57, 58]. Irradiation of pathologic draining LNs compared with other sites might also improve cross-presentation of tumor associated epitopes by dendritic cells [8].
This trial had some important limitations. Patient accrual was challenging and limited our ability to determine MTD and draw meaningful conclusions. This deficiency highlights the need for cross-disciplinary collaboration in such combination trials. At the time of trial initiation, immune-oncology was still at its infancy. Investigators lacked knowledge of irRECIST criteria and treatment beyond progression. Our patient population was not selected to enrich response. We now know that the tumor mutational load might correlate with ICI response [59–62], and unselected MBC typically displays lower numbers of somatic mutations, and less engagement with T cells [63]. However, certain breast cancer subtypes have higher degree of immune infiltration and PD-L1 expression, such as TNBC and HER2-positive MBC [64–69]. In a phase II study of TNBC using a similar treatment protocol with pembrolizumab given within 3 days of RT delivered over 5 daily fractions, ORR reached 33%, and ongoing responses were still present after 20 weeks [56].
Taken together, our results with relatively long follow up demonstrate safety profile which support testing ICI in combination with RT in future prospective trials.
Materials and Methods
Study design and patients
In this investigator-initiated, open-label phase 1 dose escalation trial, we enrolled women aged 18 years or older with incurable, histologically confirmed MBC requiring palliative radiation therapy (RT). Patients were enrolled between July 2010 and October 2011 at the Princess Margaret Cancer Centre. Other inclusion criteria included Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 and adequate organ function. There were no restrictions on previous lines of therapy (≥4 weeks must have elapsed since the last dose of systemic therapy). Patients were excluded if they had contraindications to RT, previous treatment with any anti-CTLA4 agent, history of chronic inflammatory, gastrointestinal or autoimmune disorder, insulin-dependent diabetes, active diarrhea at baseline, planned radiation to pelvic masses (to minimize the risk of colitis), history of congestive heart failure, stroke, myocardial infarction or thromboembolic event, untreated brain metastases, or concurrent or planned immunosuppressive dose of corticosteroid therapy or other immunosuppressive medication (e,g., methotrexate, rapamycin) for longer than 10 days within 4 weeks prior to enrollment or while on trial. For further information regarding the trial protocol, please see Appendix.
This study was approved by the Research Ethics Board at University Health Network, and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines. All patients provided written informed consent before enrollment. Tremelimumab was provided by Pfizer Canada Inc. The study protocol, accrual process, data collection and analysis were proposed and conducted independently by study investigators.
Treatment procedures
All patients received palliative external RT of 2000cGy in 5 daily fractions at one tumor site using 6-18 MV photons. The rationale for choosing this radiation dose was: 1) ability to induce sufficient cell kill in the majority of tumors and provide appropriate signals for enhancing the anti-tumor T cell response [8, 50]; and 2) 2000cGy is a standard dose for palliative radiation with low risk of toxicities [70]. On the third day of RT, tremelimumab was administered intravenously at 3, 6, 10, or 15 mg/kg, as per dose escalation rules outlined below. We chose the third day of RT to dose tremelimumab given that 1) the effect of radiation on promoting tumor antigen cross-presentation and MHC upregulation can occur as early as one day after radiation [6], and 2) subsequent CTLA4 upregulation on activated effector T cells is detectable 2 days after an antigenic signal [71]. The starting dose of tremelimumab was 3mg/kg, a dose shown to be safe as a single agent in previous trials [72, 73]. Given the long half-life of tremelimumab (22 days) [74], patients with a clinical response (or clinical benefit at the investigator’s discretion) following the first tremelimumab dose were eligible to receive a subsequent dose at 90 days, for a maximum of 4 cycles in total. Combination of subsequent cycles with radiation were not permitted.
Evaluation of endpoints
The primary objective of this study was to assess safety and define the maximum tolerated dose (MTD) of tremelimumab in combination with radiation therapy. The MTD was the dose at which no subject experienced a life-threatening adverse event, and at which 0-1 out of 6 patients (<33%) experienced a dose limiting toxicity (DLT) within 12 weeks of tremelimumab administration. DLT was defined as any of the following: 1) any Grade 4 toxicity, 2) other grade >3 toxicities that do not recover to ≤ Grade 1 or baseline within 7 days of maximal management (including skin toxicities), or 3) other Grade >2 or greater treatment-related autoimmune toxicity of critical organs (lung, heart, kidney, bowel, bone marrow and nervous system, eye except anterior uveitis). Dose escalation rules followed a classic 3 + 3 design, with assessment of DLT at 12 weeks. If no patient experienced a DLT, the trial would proceed to the next dose level cohort. If a DLT was encountered in one of three patients, 3 additional patients would be treated at the same dose for a total of 6 patients. If one of the six patients experienced a DLT, the trial would escalate to the next dose level. If DLT was encountered in more than one patient, the MTD would be declared as having been exceeded, and dose escalation was discontinued.
Patients were evaluated for toxicity with clinical visits, bloodwork and urine analysis weekly in the first month, and every two weeks following treatment. Thyroid function tests, autoantibody panel and human antihuman antibody (HAHA) were assessed at 4 and 12 weeks. Adverse events and other symptoms were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 3.0, as per trial protocol.
Our secondary objective was to explore clinical efficacy. ORR was assessed 6-8 weeks following tremelimumab dosing, defined according to RECIST v1.0, as per trial protocol [75]. Complete response (CR) was defined as disappearance of all target and non-target lesions. Partial response (PR) was defined as at least 30% decrease in the sum of the tumor measurements (TM) of target lesions compared to baseline. Non-target lesions could persist, provided there was no unequivocal progression in these lesions. CR and PR were confirmed by repeat assessments performed within 4–6 weeks. Progressive disease (PD) was defined as >20% increase in the sum TM of the target lesions from the smallest sum TM recorded since baseline or the appearance of one or more new lesions or unequivocal progression of existing non-target lesions. If the changes in sizes of the target and nontarget lesions did not qualify as either PR or PD, then the patient would be deemed to have stable disease (SD). Routine assessment of response with CT imaging was performed 8 weeks following tremelimumab, and every 6–8 weeks thereafter. Overall survival was defined from the date of metastatic breast cancer diagnosis (OS1) and from date of first dose of tremelimumab initiation (OS2).
Peripheral blood mononuclear cells (PBMCs) were collected at baseline, and at 1, 2, and 4 weeks following tremelimumab dosing. Cryopreserved PBMCs were thawed and stained for flow cytometric analysis. Staining was performed using antibodies purchased from BD Biosciences (CD3 (clone UCHT1), CD4 (RPA-T4)), Thermo Fisher Scientific (FOXP3 (clone 236A/E7), CD25 (BC96), CD127 (eBioRDR5), Ki67 (20Raj1), TCRγδ (B1.1), CD28 (CD28.2), and CD19 (HIB19)), and BioLegend (CD56 (clone HCD56). Data were acquired using a 5-laser LSR Fortessa X-20 (BD) and analyzed using FlowJo v.10 (Treestar).
ACKNOWLEDGMENTS
We thank James Seongjun Han and Dr. Aras Toker for scientific discussions. We thank Patty Yen, Jessica Nie and Michael Fyrsta for technical assistance. PSO holds a Tier 1 Canada Research Chair in Autoimmunity and Tumour Immunity and Canadian Institutes of Health Research (CIHR) Foundation award.
CONFLICTS OF INTEREST
Dr. Neel: Co-founder, member of board of directors, consulting and equity in Northern Biologics Co-founder, chair of scientific advisory board, consulting and equity in Navire pharma Spouse has equity in Pfizer.
Dr. Sacher: Consultant/advisory board for AstraZeneca, Pfizer, Bayer, Gritstone Oncology, Merck, Genentech-Roche Honoraria from AstraZeneca, Pfizer, Bayer, Merck, Genentech-Roche.
FUNDING
This study was made possible with grant funding from Pfizer.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018; 68:7–30. https://doi.org/10.3322/caac.21442. [PubMed].
2. Nanda R, Chow LQ, Dees EC, Berger R, Gupta S, Geva R, Pusztai L, Pathiraja K, Aktan G, Cheng JD, Karantza V, Buisseret L. Pembrolizumab in patients with advanced triple-negative breast cancer: Phase Ib keynote-012 study. J Clin Oncol. 2016; 34:2460–7. https://doi.org/10.1200/JCO.2015.64.8931. [PubMed].
3. Schmid P, Cruz C, Braiteh FS, Eder JP, Tolaney S, Kuter I, Nanda R, Chung C, Cassier P, Delord JP, Gordon M, Li Y, Liu B, et al. Abstract 2986: Atezolizumab in metastatic TNBC (mTNBC): Long-term clinical outcomes and biomarker analyses. Cancer Res. 2017; 77:2986–2986. https://doi.org/10.1158/1538-7445.AM2017-2986.
4. Dirix LY, Takacs I, Jerusalem G, Nikolinakos P, Arkenau HT, Forero-Torres A, Boccia R, Lippman ME, Somer R, Smakal M, Emens LA, Hrinczenko B, Edenfield W, et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: a phase 1b JAVELIN Solid Tumor study. Breast Cancer Res Treat. 2017; 167:1–16. https://doi.org/10.1007/s10549-017-4537-5. [PubMed].
5. Rugo H, Huang L, Petrenciuc O, Zaccarini P, Coleman R. Abstract OT2-01-11: A phase 2 randomized, doubl-blind, placebo-controlled trial of radium-223 dichloride with exemestane and everolimus in human epidermal growth factor receptor 2–negative, hormone receptor–positive breast cancer patients with bone metast. Thirty-Eighth Annual CTRC-AACR San Antonio Breast Cancer Symposium; December 8–12, 2015; San Antonio, TX.
6. Reits EA, Hodge JW, Herberts CA, Groothuis TA, Chakraborty M, Wansley EK, Camphausen K, Luiten RM, de Ru AH, Neijssen J, Griekspoor A, Mesman E, Verreck FA, Spits H, et al. Radiation modulates the peptide repertoire, enhances MHC class I expression, and induces successful antitumor immunotherapy. J Exp Med. 2006; 203:1259–71. https://doi.org/10.1084/jem.20052494. [PubMed].
7. Sharabi AB, Nirschl CJ, Kochel CM, Nirschl TR, Francica BJ, Velarde E, Deweese TL, Drake CG. Stereotactic Radiation Therapy Augments Antigen-Specific PD-1-Mediated Antitumor Immune Responses via Cross-Presentation of Tumor Antigen. Cancer Immunol Res. 2015; 3:345–55. https://doi.org/10.1158/2326-6066.CIR-14-0196. [PubMed].
8. Lugade AA, Moran JP, Gerber SA, Rose RC, Frelinger JG, Lord EM. Local Radiation Therapy of B16 Melanoma Tumors Increases the Generation of Tumor Antigen-Specific Effector Cells That Traffic to the Tumor. J Immunol. 2005; 174:7516–23. https://doi.org/10.4049/jimmunol.174.12.7516. [PubMed].
9. Chakraborty M, Abrams SI, Camphausen K, Liu K, Scott T, Coleman CN, Hodge JW. Irradiation of Tumor Cells Up-Regulates Fas and Enhances CTL Lytic Activity and CTL Adoptive Immunotherapy. J Immunol. 2003; 170:6338–47. https://doi.org/10.4049/jimmunol.170.12.6338. [PubMed].
10. Deng L, Liang H, Xu M, Yang X, Burnette B, Arina A, Li X, Mauceri H, Beckett M, Darga T, Huang X, Gajewski TF, Chen ZJ. Article STING-Dependent Cytosolic DNA Sensing Promotes Radiation-Induced Type I Interferon-Dependent Antitumor Immunity in Immunogenic Tumors. Immunity. 2014; 41:843–52. https://doi.org/10.1016/j.immuni.2014.10.019. [PubMed].
11. Matsumura S, Wang B, Kawashima N, Braunstein S, Badura M, Cameron TO, Babb JS, Schneider RJ, Formenti SC, Dustin ML, Demaria S, Matsumura S, Wang B, et al. Radiation-Induced CXCL16 Release by Breast Cancer Cells Attracts Effector T Cells. J Immunol. 2008; 181:3099–107. https://doi.org/10.4049/jimmunol.181.5.3099. [PubMed].
12. Kunkel EJ, Butcher EC. Chemokines and the Tissue-Specific Migration of Lymphocytes. Immunity. 2002; 16:1–4. https://doi.org/10.1016/s1074-7613(01)00261-8. [PubMed].
13. Ganss R, Ryschich E, Klar E, Arnold B, Hämmerling GJ. Combination of T-cell therapy and trigger of inflammation induces remodeling of the vasculature and tumor eradication. Cancer Res. 2002; 62:1462–70. https://doi.org/10.1078/0171-2985-00078. [PubMed].
14. Multhoff G, Radons J. Radiation, Inflammation, and Immune Responses in Cancer. Front Oncol. 2012; 2:1–18. https://doi.org/10.3389/fonc.2012.00058. [PubMed].
15. Demaria S, Formenti SC. Sensors of ionizing radiation effects on the immunological microenvironment of cancer. Int J Radiat Biol. 2007; 83:819–25. https://doi.org/10.1080/09553000701481816. [PubMed].
16. Demaria S, Kawashima N, Yang AM, Devitt ML, Babb JS, Allison JP, Formenti SC. Immune-Mediated Inhibition of Metastases after Treatment with Local Radiation and CTLA-4 Blockade in a Mouse Model of Breast Cancer Immune-Mediated Inhibition of Metastases after Treatment with Local Radiation and CTLA-4 Blockade in a Mouse Model of Breas. Clin Cancer Res. 2005; 11:728–34. https://doi.org/10.1016/s0360-3016(04)01159-9. [PubMed].
17. Postow MA, Callahan MK, Barker CA, Yamada Y, Yuan J, Kitano S. Effect in a Patient with Melanoma. N Engl J Med. 2012; 366:925–31. https://doi.org/10.1056/NEJMc1203984. [PubMed].
18. Hiniker SM, Chen DS, Reddy S, Chang DT, Jones JC, Mollick JA, Swetter SM, Knox SJ. A Systemic Complete Response of Metastatic Melanoma to Local Radiation and Immunotherapy. Transl Oncol. 2012; 5:404–7. https://doi.org/10.1593/tlo.12280. [PubMed].
19. Slovin SF, Higano CS, Hamid O, Tejwani S, Harzstark A, Alumkal JJ, Scher HI, Chin K, Gagnier P, McHenry MB, Beer TM. Ipilimumab alone or in combination with radiotherapy in metastatic castration-resistant prostate cancer: Results from an open-label, multicenter phase i/ii study. Ann Oncol. 2013; 24:1813–21. https://doi.org/10.1093/annonc/mdt107. [PubMed].
20. Golden EB, Demaria S, Schiff PB, Chachoua A, Formenti SC. An Abscopal Response to Radiation and Ipilimumab in a Patient with Metastatic Non-Small Cell Lung Cancer. Cancer Immunol Res. 2013; 1:365–72. https://doi.org/10.1158/2326-6066.CIR-13-0115. [PubMed].
21. Kwon ED, Drake CG, Scher HI, Fizazi K, Bossi A, Van den Eertwegh AJ, Krainer M, Houede N, Santos R, Mahammedi H, Ng S, Maio M, Franke FA, et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): A multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014; 15:700–12. https://doi.org/10.1016/S1470-2045(14)70189-5. [PubMed].
22. Bang A, Wilhite TJ, Pike LRG, Cagney DN, Aizer AA, Taylor A, Spektor A, Krishnan M, Ott PA, Balboni TA, Hodi FS, Schoenfeld JD. Multicenter Evaluation of the Tolerability of Combined Treatment With PD-1 and CTLA-4 Immune Checkpoint Inhibitors and Palliative Radiation Therapy. Int J Radiat Oncol Biol Phys. 2017; 98:344–51. https://doi.org/10.1016/j.ijrobp.2017.02.003. [PubMed].
23. Luke JJ, Lemons JM, Karrison TG, Pitroda SP, Melotek JM, Zha Y, Al-Hallaq HA, Arina A, Khodarev NN, Janisch L, Chang P, Patel JD, Fleming GF, et al. Safety and Clinical Activity of Pembrolizumab and Multisite Stereotactic Body Radiotherapy in Patients With Advanced Solid Tumors. J Clin Oncol. 2018; 36:1611–1618. https://doi.org/10.1200/JCO.2017.76.2229. [PubMed].
24. Shaverdian N, Lisberg AE, Bornazyan K, Veruttipong D, Goldman JW, Formenti SC, Garon EB, Lee P. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 phase 1 trial. Lancet Oncol. 2017; 18:895–903. https://doi.org/10.1016/S1470-2045(17)30380-7. [PubMed].
25. Tang C, Welsh JW, De Groot P, Massarelli E, Chang JY, Hess KR, Basu S, Curran MA, Cabanillas ME, Subbiah V, Fu S, Tsimberidou AM, Karp D, et al. Ipilimumab with stereotactic ablative radiation therapy: Phase i results and immunologic correlates from peripheral T cells. Clin Cancer Res. 2017; 23:1388–96. https://doi.org/10.1158/1078-0432.CCR-16-1432. [PubMed].
26. Wolchok J, Neyns B, Linette G, Negrier S, Lutzky J, Thomas L, Waterfield W, Schadendorf D, Smylie M, Guthrie TJ, Grob J, Chesney J, Chin K, et al. Ipilimumab monotherapy in patients with pretreated advanced melanoma: a randomised, double-blind, multicentre, phase 2, dose- ranging study. Lancet Oncol. 2010; 11:155–64. https://doi.org/10.1016/S1470-2045(09)70334-1. [PubMed].
27. Sage EK, Schmid TE, Sedelmayr M, Gehrmann M, Geinitz H, Duma MN, Combs SE, Multhoff G. Comparative analysis of the effects of radiotherapy versus radiotherapy after adjuvant chemotherapy on the composition of lymphocyte subpopulations in breast cancer patients. Radiother Oncol. 2016; 118:176–80. https://doi.org/10.1016/j.radonc.2015.11.016. [PubMed].
28. Grossman S, Ellsworth S, Campian J, Wild A, Herman J, Laheru D, Brock M, Balmanoukian A, Ye X. Survival in Patients With Severe Lymphopenia Following Treatment With Radiation and Chemotherapy for Newly Diagnosed Solid Tumors. J Natl Compr Canc Netw. 2015; 13:1225–31. https://doi.org/10.6004/jnccn.2015.0151. [PubMed].
29. Tang C, Liao Z, Gomez D, Levy L, Zhuang Y, Gebremichael RA, Hong DS, Komaki R, Welsh JW. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int J Radiat Oncol Biol Phys. 2014; 89:1084–1091. https://doi.org/10.1016/j.ijrobp.2014.04.025. [PubMed].
30. Venkatesulu BP, Mallick S, Lin SH, Krishnan S. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Crit Rev Oncol Hematol. 2018; 123:42–51. https://doi.org/10.1016/j.critrevonc.2018.01.003. [PubMed].
31. Wei B. The neutrophil lymphocyte ratio is associated with breast cancer prognosis: an updated systematic review and meta-analysis. Onco Targets Ther. 2016; 9:5567–75. https://doi.org/10.2147/OTT.S108419. [PubMed].
32. Ethier JL, Desautels D, Templeton A, Shah PS, Amir E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: a systematic review and meta-analysis. Breast Cancer Res. 2017; 19:2. https://doi.org/10.1186/s13058-016-0794-1. [PubMed].
33. Peng J, Hamanishi J, Matsumura N, Abiko K, Murat K. Chemotherapy Induces Programmed Cell Death-Ligand 1 Overexpression via the Nuclear Factor- k B to Foster an Immunosuppressive Tumor Microenvironment in Ovarian Cancer. Cancer Res. 2015; 75:1–12. https://doi.org/10.1158/0008-5472.CAN-14-3098. [PubMed].
34. Fridlender ZG, Sun J, Singhal S, Kapoor V, Cheng G, Suzuki E, Albelda SM. Chemotherapy Delivered After Viral Immunogene Therapy Augments Antitumor Efficacy Via Multiple Immune-mediated Mechanisms. Mol Ther. 2009; 18:1947–59. https://doi.org/10.1038/mt.2010.159. [PubMed].
35. Schvartsman G, Peng SA, Bis G, Lee JJ, Benveniste MFK, Zhang J, Roarty EB, Lacerda L, Swisher S, Heymach JV, Fossella FV, William WN. Lung Cancer Response rates to single-agent chemotherapy after exposure to immune checkpoint inhibitors in advanced non-small cell lung cancer. Lung Cancer. 2017; 112:90–5. https://doi.org/10.1016/j.lungcan.2017.07.034. [PubMed].
36. Park SE, Lee SH, Ahn JS, Ahn M, Park K, Sun J. Increased Response Rates to Salvage Chemotherapy Administered after PD-1 / PD-L1 Inhibitors in Patients with Non – Small Cell Lung Cancer. J Thorac Oncol. 2018; 13:106–11. https://doi.org/10.1016/j.jtho.2017.10.011. [PubMed].
37. Adams S, Schmid P, Rugo HS, Winer EP, Loirat D, Awada A, Cescon DW, Iwata H. Pembrolizumab monotherapy for previously treated metastatic triple-negative breast cancer: cohort A of the phase II KEYNOTE-086 study. Ann Oncol. 2019; 30:397–404. https://doi.org/10.1093/annonc/mdy517. [PubMed].
38. Adams S, Loi S, Toppmeyer D, Cescon DW, De Laurentiis M, Nanda R, Winer EP, Mukai H, Tamura K, Armstrong A, Liu MC, Iwata H, Ryvo L, et al. Pembrolizumab monotherapy for previously breast cancer: cohort B of the phase II KEYNOTE-086 study. Ann Oncol. 2019; 30:405–411. https://doi.org/10.1093/annonc/mdy518. [PubMed].
39. Bonotto M, Gerratana L, Iacono D, Minisini AM, Rihawi K, Fasola G, Puglisi F. Treatment of Metastatic Breast Cancer in a Real-World Scenario: Is Progression-Free Survival With First Line Predictive of Benefit From Second and Later Lines? Oncologist. 2015; 20:719–24. https://doi.org/10.1634/theoncologist.2015-0002. [PubMed].
40. Dawood S, Broglio K, Ensor J, Hortobagyi GN, Giordano SH. Survival differences among women with de novo stage IV and relapsed breast cancer. Ann Oncol. 2010; 21:2169–74. https://doi.org/10.1093/annonc/mdq220. [PubMed].
41. Muroyama Y, Nirschl TR, Kochel CM, Lopez-Bujanda Z, Theodros D, Mao W, Carrera-Haro MA, Ghasemzadeh A, Marciscano AE, Velarde E, Tam AJ, Thoburn CJ, Uddin M, et al. Stereotactic radiotherapy increases functionally suppressive regulatory T cells in the tumor microenvironment. Cancer Immunol Res. 2017; 5:992–1004. https://doi.org/10.1158/2326-6066.CIR-17-0040. [PubMed].
42. Qu Y, Jin S, Zhang A, Zhang B, Shi X, Wang J, Zhao Y. Gamma-Ray Resistance of Regulatory CD4 + CD25 + Foxp3 + T Cells in Mice. Radiat Res. 2010; 173:148–57. https://doi.org/10.1667/RR0978.1. [PubMed].
43. Schuler PJ, Harasymczuk M, Schilling B, Saze Z, Strauss L, Lang S, Johnson JT, Whiteside TL. Effects of adjuvant chemoradiotherapy on the frequency and function of Regulatory T cells in patients with head and neck cancer. Clin Cancer Res. 2013; 19:6585–96. https://doi.org/10.1158/1078-0432.CCR-13-0900. [PubMed].
44. Fadul CE, Fisher JL, Gui J, Hampton TH, Côté AL, Ernstoff MS. Immune modulation effects of concomitant temozolomide and radiation therapy on peripheral blood mononuclear cells in patients with glioblastoma multiforme. Neuro Oncol. 2011; 13:393–400. https://doi.org/10.1093/neuonc/noq204. [PubMed].
45. Yao X, Ahmadzadeh M, Lu YC, Liewehr DJ, Dudley ME, Liu F, Schrump DS, Steinberg SM, Rosenberg SA, Robbins PF. Levels of peripheral CD4 +FoxP3 + regulatory T cells are negatively associated with clinical response to adoptive immunotherapy of human cancer. Blood. 2012; 119:5688–96. https://doi.org/10.1182/blood-2011-10-386482. [PubMed].
46. Vacchelli E, Semeraro M, Enot DP, Chaba K, Colame VP, Dartigues P, Perier A, Villa I, Rusakiewicz S, Gronnier C, Goéré D, Mariette C, Zitvogel L, et al. Negative prognostic impact of regulatory T cell infiltration in surgically resected esophageal cancer post-radiochemotherapy. Oncotarget. 2015; 6:20840–50. https://doi.org/10.18632/oncotarget.4428. [PubMed].
47. Hirschhorn-Cymerman D, Rizzuto GA, Merghoub T, Cohen AD, Avogadri F, Lesokhin AM, Weinberg AD, Wolchok JD, Houghton AN. OX40 engagement and chemotherapy combination provides potent antitumor immunity with concomitant regulatory T cell apoptosis. J Exp Med. 2009; 206:1103–16. https://doi.org/10.1084/jem.20082205. [PubMed].
48. Takada K, Kashiwagi S, Goto W, Asano Y, Takahashi K, Takashima T. Use of the tumor-infiltrating CD8 to FOXP3 lymphocyte ratio in predicting treatment responses to combination therapy with pertuzumab, trastuzumab, and docetaxel for advanced HER2-positive breast cancer. J Transl Med. 2018; 16:1–11. https://doi.org/10.1186/s12967-018-1460-4. [PubMed].
49. Asano Y, Kashiwagi S, Goto W, Kurata K, Noda S, Takashima T, Onoda N, Tanaka S, Ohsawa M, Hirakawa K. Tumour-infiltrating CD8 to FOXP3 lymphocyte ratio in predicting treatment responses to neoadjuvant chemotherapy of aggressive breast cancer. Br J Surg. 2016; 103:845–54. https://doi.org/10.1002/bjs.10127. [PubMed].
50. Dewan MZ, Galloway AE, Kawashima N, Dewyngaert JK, Babb JS, Formenti SC, Demaria S. Fractionated but not single dose radiotherapy induces an immune-mediated abscopal effect when combined with anti- CTLA-4 antibody. Clin Cancer Res. 2010; 15:5379–88. https://doi.org/10.1158/1078-0432.CCR-09-0265. [PubMed].
51. Chandra RA, Wilhite TJ, Balboni TA, Alexander BM, Spektor A, Ott PA, Ng AK, Hodi FS, Schoenfeld JD. A systematic evaluation of abscopal responses following radiotherapy in patients with metastatic melanoma treated with ipilimumab. Oncoimmunology. 2015; 4:e1046028. https://doi.org/10.1080/2162402X.2015.1046028. [PubMed].
52. Barker CA, Postow MA, Khan SA, Beal K, Parhar PK, Yamada Y, Lee NY, Wolchok JD. Concurrent Radiotherapy and Ipilimumab Immunotherapy for Patients with Melanoma. Cancer Immunol Res. 2013; 1:92–8. https://doi.org/10.1158/2326-6066.CIR-13-0082. [PubMed].
53. Grimaldi AM, Simeone E, Giannarelli D, Muto P, Falivene S, Borzillo V, Giugliano FM, Sandomenico F, Petrillo A, Curvietto M, Esposito A, Paone M, Palla M, et al. Abscopal effects of radiotherapy on advanced melanoma patients who progressed after ipilimumab immunotherapy. Oncoimmunology. 2014; 3:e28780. https://doi.org/10.4161/onci.28780. [PubMed].
54. Dewan MZ, Galloway AE, Kawashima N, Dewyngaert JK, Babb JS, Formenti SC, Demaria S. Fractionated but not single-dose radiotherapy induces an immune-mediated abscopal effect when combined with anti-CTLA-4 antibody. Clin Cancer Res. 2009; 15:5379–88. https://doi.org/10.1158/1078-0432.CCR-09-0265. [PubMed].
55. Dovedi SJ, Lipowska-Bhalla G, Beers SA, Cheadle EJ, Mu L, Glennie MJ, Illidge TM, Honeychurch J. Antitumor Efficacy of Radiation plus Immunotherapy Depends upon Dendritic Cell Activation of Effector CD8+ T Cells. Cancer Immunol Res. 2016; 4:621–30. https://doi.org/10.1158/2326-6066.CIR-15-0253. [PubMed].
56. McArthur HL. A phase II, single arm study assessing the efficacy of pembrolizumab (Pembro) plus radiotherapy (RT) in metastatic triple negative breast cancer (mTNBC). ASCO Annual Meeting. 2018. https://doi.org/10.1200/JCO.2018.36.15_suppl.1017.
57. Yuan C, Wang Q. Comparative analysis of the effect of different radiotherapy regimes on lymphocyte and its subpopulations in breast cancer patients. Clin Transl Oncol. 2018; 20:1219–1225. https://doi.org/10.1007/s12094-018-1851-2. [PubMed].
58. Shiraishi Y, Fang P, Xu C, Song J, Krishnan S, Koay EJ, Mehran RJ, Hofstetter WL, Blum-Murphy M, Ajani JA, Komaki R, Minsky B, Mohan R, et al. Severe lymphopenia during neoadjuvant chemoradiation for esophageal cancer: A propensity matched analysis of the relative risk of proton versus photon-based radiation therapy. Radiother Oncol. 2017. https://doi.org/10.1016/j.radonc.2017.11.028. [PubMed].
59. Schumacher TN, Schreiber RD. Neoantigens in cancer immunotherapy. Science. 2015; 348:69–74. https://doi.org/10.1126/science.aaa4971. [PubMed].
60. Lawrence MS, Stojanov P, Polak P, Kryukov GV, Cibulskis K, Sivachenko A, Carter SL, Stewart C, Mermel CH, Roberts SA, Kiezun A, Hammerman PS, McKenna A, et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature. 2013; 499:214–8. https://doi.org/10.1038/nature12213. [PubMed].
61. Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Behjati S, Biankin AV, Bignell GR, Bolli N, Borg A, Børresen-Dale AL, Boyault S, Burkhardt B, Butler AP, et al. Signatures of mutational processes in human cancer. Nature. 2013; 500:415–21. https://doi.org/10.1038/nature12477. [PubMed].
62. Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, Lee W, Yuan J, Wong P, Ho TS, Miller ML, Rekhtman N, Moreira AL, et al. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015; 348:124–8. https://doi.org/10.1126/science.aaa1348. [PubMed].
63. Chalmers ZR, Connelly CF, Fabrizio D, Gay L, Ali SM, Ennis R, Schrock A, Campbell B, Shlien A, Chmielecki J, Huang F, He Y, Sun J, et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017; 9:1–14. https://doi.org/10.1186/s13073-017-0424-2. [PubMed].
64. Stanton SE, Adams S, Disis ML. Variation in the Incidence and Magnitude of Tumor-Infiltrating Lymphocytes in Breast Cancer Subtypes: A Systematic Review. JAMA Oncol. 2016; 2:1354–60. https://doi.org/10.1001/jamaoncol.2016.1061. [PubMed].
65. Wimberly H, Brown JR, Schalper K, Haack H, Silver MR, Nixon C, Bossuyt V, Pusztai L, Lannin DR, Rimm DL. PD-L1 Expression Correlates with Tumor-Infiltrating Lymphocytes and Response to Neoadjuvant Chemotherapy in Breast Cancer. Cancer Immunol Res. 2015; 3:326–32. https://doi.org/10.1158/2326-6066.CIR-14-0133. [PubMed].
66. Denkert C, von Minckwitz G, Brase JC, Sinn BV, Gade S, Kronenwett R, Pfitzner BM, Salat C, Loi S, Schmitt WD, Schem C, Fisch K, Darb-Esfahani S, et al. Tumor infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2 positive and triple negative primary breast cancers. J Clin Oncol. 2015; 33:983–91. https://doi.org/10.1200/JCO.2014.58.1967. [PubMed].
67. Mittendorf EA, Philips AV, Meric-Bernstam F, Qiao N, Wu Y, Harrington S, Su X, Wang Y, Gonzalez-Angulo AM, Akcakanat A, Chawla A, Curran M, Hwu P, et al. PD-L1 Expression in Triple-Negative Breast Cancer. Cancer Immunol Res. 2014; 2:361–70. https://doi.org/10.1158/2326-6066.CIR-13-0127. [PubMed].
68. Miller LD, Chou JA, Black MA, Print C, Chifman J, Alistar A, Putti T, Zhou X, Bedognetti D, Hendrickx W, Pullikuth A, Rennhack J, Andrechek ER, et al. Immunogenic Subtypes of Breast Cancer Delineated by Gene Classifiers of Immune Responsiveness. Cancer Immunol Res. 2016; 4:600–10. https://doi.org/10.1158/2326-6066.CIR-15-0149. [PubMed].
69. Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, Wienert S, Van den Eynden G, Baehner FL, Penault-Llorca F, Perez EA, Thompson EA, Symmans WF, et al. The evaluation of tumor-infiltrating lymphocytes (TILS) in breast cancer: Recommendations by an International TILS Working Group 2014. Ann Oncol. 2015; 26:259–71. https://doi.org/10.1093/annonc/mdu450. [PubMed].
70. Lutz S, Balboni T, Jones J, Lo S, Petit J, Rich SE, Wong R, Hahn C. Palliative radiation therapy for bone metastases: Update of an ASTRO Evidence-Based Guideline. Pract Radiat Oncol. 2017; 7:4–12. https://doi.org/10.1016/j.prro.2016.08.001. [PubMed].
71. Linsley PS, Greene JL, Tan P, Bradshaw J, Ledbetter JA, Anasetti C, Damle NK. Coexpression and functional cooperation of CTLA-4 and CD28 on activated T lymphocytes. J Exp Med. 1992; 176:1595–604. https://doi.org/10.1084/jem.176.6.1595. [PubMed].
72. Ribas A, Hanson DC, Noe DA, Millham R, Guyot DJ, Bernstein SH, Canniff PC, Sharma A, Gomez-Navarro J. Tremelimumab (CP-675,206), a Cytotoxic T Lymphocyte Associated Antigen 4 Blocking Monoclonal Antibody in Clinical Development for Patients with Cancer. Oncologist. 2007; 12:873–83. https://doi.org/10.1634/theoncologist.12-7-873. [PubMed].
73. Vonderheide RH, Lorusso PM, Khalil M, Gartner EM, Khaira D, Soulieres D, Dorazio P, Trosko JA, Rüter J, Mariani GL, Usari T, Domchek SM. Tremelimumab in combination with exemestane in patients with advanced breast cancer and treatment-associated modulation of inducible costimulator expression on patient T cells. Clin Cancer Res. 2010; 16:3485–94. https://doi.org/10.1158/1078-0432.CCR-10-0505. [PubMed].
74. Ribas A, Camacho LH, Lopez-Berestein G, Pavlov D, Bulanhagui CA, Millham R, Comin-Anduix B, Reuben JM, Seja E, Parker CA, Sharma A, Glaspy JA, Gomez-Navarro J. Antitumor Activity in Melanoma and Anti-Self Responses in a Phase I Trial With the Anti-Cytotoxic T Lymphocyte – Associated Antigen 4 Monoclonal Antibody CP-675,206. J Clin Oncol. 2005; 23:8968–77. https://doi.org/10.1200/JCO.2005.01.109. [PubMed].
75. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT, Christian MC, Gwyther SG. New guidelines to evaluate the response to treatment in solid Tumors. J Natl Cancer Inst. 2000; 92:205–16. https://doi.org/10.1093/jnci/92.3.205. [PubMed].