
INTRODUCTION
Hepatic resection for metastatic disease has improved oncologic outcomes in various solid organ malignancies [1]. Despite advances in technique [2] and appropriate oncologic resections [3] for these patients, perioperative inflammatory stimuli [4] and management strategies such as volatile anesthetic agents [5] and opioid analgesia [6] have been implicated in poor oncologic outcomes [7–9]. These factors are associated with suppression of cell mediated immunity, shift from Th1 to Th2 signaling, augmented tumor growth, and pro-metastatic systemic signaling [10]. In some cancers, use of regional analgesia in surgical oncology procedures has been associated with increased disease-free survival (DFS) and overall survival (OS) compared to traditional post-operative opioid-based analgesia [7, 9, 11, 12]. The mechanism for these improved oncologic outcomes, however, remains unclear.
Current literature evaluating the impact of epidural analgesia on lymphocyte function [13–15], Th1 vs. Th2 balance [16], and systemic markers of inflammation [17–20] has yielded mixed results. Furthermore, oncological relevant biomarkers to measure the impact of regional anesthesia on the response to surgery have not been established. Herein, we evaluated the longitudinal postoperative impact of thoracic epidural analgesia (TEA) on a comprehensive systemic biomarker panel from patients undergoing elective hepatic resection for metastatic disease as part of a randomized controlled trial comparing TEA and intravenous patient controlled analgesia (IV-PCA). In addition to established perioperative biomarkers, a novel set of oncological relevant systemic markers involved in Th1 immune response (CXCL10) [21]; tumor associated macrophages (CXCL12) [22]; tumor suppression (Omentin-1) [23]; pro-metastatic signaling (Galectin-3) [24]; and tumor associated inflammation (Pentraxin-3) [25] were evaluated. Our hypothesis was that TEA would dampen the inflammatory response, preserve Th1 biomarkers, and decrease pro-metastatic signaling in the postoperative period in comparison to IV-PCA.
RESULTS
Table 1 demonstrates that clinicopathologic variables were overall similar between patients in the TEA (n = 45) and IV-PCA (n = 16) groups. Metastatic pathology was also similar between groups and consisted predominantly of colorectal liver metastasis (75 vs. 93%, p = 0.070). Additional metastatic disease pathology included neuroendocrine tumor (n = 2), sarcoma (n = 1), adrenocortical carcinoma (n = 1), ovarian carcinoma (n = 1), medullar thyroid cancer (n = 1), and breast cancer (n = 1) distributed between the two groups. During the hospitalization, the IV-PCA group had an increased opioid consumption compared to the TEA group (386.3 [233.8–588.5] vs. 154.3 [99.4–264.2] mg, p = 0.012).
Table 1: Clinicopathologic, operative, and recovery variables of patients in all patients, as well as PCA and TEA groups
Epidural vs. PCA |
|||||
|---|---|---|---|---|---|
PCA n = 16 |
TEA n = 45 |
||||
n or median |
% or IQR |
n or median |
% or IQR |
p |
|
Age |
61 |
52–64 |
55 |
48–61 |
0.166 |
Male |
8 |
50% |
27 |
60% |
0.563 |
ASA = 3 |
13 |
81% |
41 |
91% |
0.365 |
BMI |
24 |
23-30 |
27 |
24-30 |
0.425 |
Received Pre-operative Chemotherapy |
11 |
69% |
39 |
89% |
0.112 |
Portal Vein Embolization |
0 |
0% |
5 |
11% |
0.313 |
Major Hepatectomy |
9 |
56% |
30 |
66% |
0.568 |
Midline Incision |
9 |
56% |
31 |
68% |
0.376 |
Operative Time (min) |
259 |
220–316 |
260 |
206–306 |
0.516 |
Estimated Blood Loss (mL) |
200 |
150–375 |
200 |
100–300 |
0.343 |
Perioperative Transfusion |
2 |
12% |
4 |
9% |
0.648 |
Postoperative Complication |
5 |
31% |
16 |
36% |
0.999 |
Length of Stay (days) |
5 |
5–6 |
6 |
5–7 |
0.663 |
PCA or Epidural Duration (days) |
3 |
3–4 |
4 |
3–4 |
0.857 |
Colorectal Liver Metastasis |
12 |
75% |
42 |
93% |
0.070 |
Opioid Consumption (mg) |
386.3 |
233.8–588.5 |
154.3 |
99.4–264.2 |
0.012 |
Inadequate Pain Control |
8 |
50% |
17 |
38% |
0.555 |
Patients in the TEA group had lower opioids requirement during their hospitalization, but the groups were otherwise similar.
Preoperative concentrations of biomarkers are shown in Table 2. IL-6 (35.2 vs. 10.1, p = 0.048) was noted to be higher in the IV-PCA group, while the remainder of the biomarkers were similar between the two groups prior to surgery. Of note, poor signal quality outside of the standard’s concentration range was noted in IL-1b, IL-2, IL-4, IL-5, IL-7, IL-10, IL-13, IL-17, VEGF, GM-CSF, and G-CSF before surgery and throughout the experiment in most patients.
Table 2: Preoperative plasma biomarker levels in all patients
Analgesic Technique |
|||
|---|---|---|---|
PCA (n = 16) |
Epidural (n = 45) |
P value |
|
Median (IQR) |
Median (IQR) |
||
IL6 |
35.2 (12.5, 52.1) |
10.1 (6.4, 20.7) |
0.048 |
IL8 |
93.9 (35.7, 158.5) |
82.8 (50.9, 96.0) |
0.432 |
IL12p70 |
4.8 (3.4, 8.5) |
7.7, (4.8, 13.1) |
0.899 |
CXCL10 |
108.9 (58.4–355.1) |
94.9 (62.5, 178.4) |
0.679 |
CXCL12 |
1432.8 (529.9, 5006.3) |
958.5 (666.2, 1370.3) |
0.163 |
INFg |
26.7 (11.0, 71.3) |
6.9 (2.8, 14.3) |
0.137 |
TNFa |
116.5 (72.9, 201.3) |
128.6 (96.7, 199.6) |
0.433 |
TGFb1 |
4078.9 (2961.3, 8302.6) |
2056.8 (478.1, 4294.1) |
0.087 |
TGFb2 |
417.6 (272.7, 512.0) |
271.9 (102.9, 409.9) |
0.181 |
TGFb3 |
173.9 (41.7, 908.9) |
57.5 (48.8, 151.4) |
0.164 |
MIP1b |
80.4 (49.3, 173.1) |
98.3 (64.6, 137.3) |
0.794 |
MCP1 |
280.1 (174.6, 396.4) |
254.6 (182.7, 418.7) |
0.681 |
Resistin |
8650.2 (6040.7, 10705.6) |
5705.9 (4196.3, 8461.1) |
0.160 |
Omentin1 |
352746.9 (129012.2, 484118.7) |
512229.7 (94982.9, 829895.6) |
0.351 |
Pentraxin3 |
1191.0 (811.4, 2273.2) |
1531.8 (683.4, 3579.1) |
0.456 |
Galactin3 |
8572.8 (6224.2, 16169.2) |
13568.6 (11411.1, 16902.5) |
0.176 |
sLeptinR |
10208.3 (1702.8, 15521.7) |
10687.7 (2835.3, 13680.6) |
0.341 |
Vaspin |
87.0 (46.7, 300.3) |
111.9 (62.1, 288.5) |
0.856 |
FGF21 |
138.9 (41.9, 595.9) |
131.2 (65.4, 201.3) |
0.221 |
FGF23 |
88.3 (42.2, 195.2) |
91.7 (59.4, 149.6) |
0.276 |
PON1 |
2710100.0 (1831150.0, 7488825.0) |
6833800.0 (3983625.0, 9489499.0) |
0.069 |
IL-6 was elevated in the PCA group. Of note biomarkers IL1b, IL2, IL4, IL5, IL7, IL10, IL13, IL17, VEGF, GMCSF, GCSF demonstrated poor signal quality at baseline and throughout the experiment.
Considering the concentrations of biomarkers throughout the study, statistically significant differences between groups were noted in TGFb1/2/3 and IL-12p70 as demonstrated in Figure 1. Compared to the IV-PCA group, the TEA group had significantly lower TGFb3 levels on POD1 (243.2 vs. 86.0 pg/mL, p = 0.005), POD3 (132.2 vs. 77.8 pg/mL, p = 0.028), POD5 (306.5 vs. 92.2 pg/mL, p = 0.032). On POD3, TGFb1 (6558.0 vs. 2063.3 pg/mL, p = 0.004) and TGFb2 (468.3 vs. 368.9 pg/mL, p = 0.036) were also significantly lower in TEA group. The POD1 IL-12p70 was significantly higher in TEA patients (8.3 vs. 1.6 pg/mL, p = 0.024).
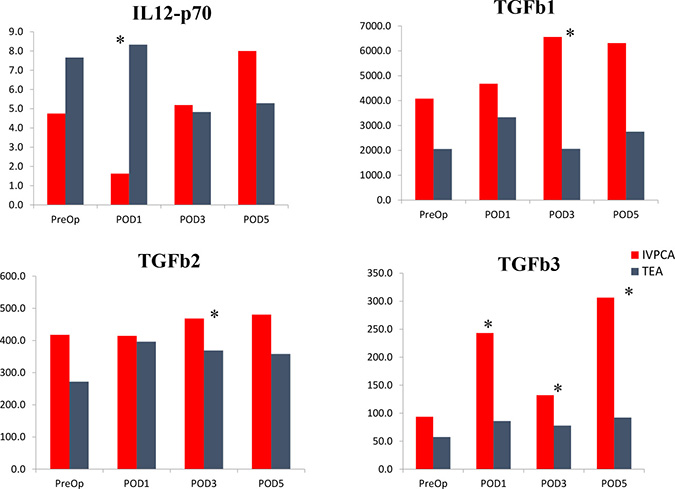
Figure 1: Concentrations (pg/mL) of the biomarkers which were significantly different between TEA and PCA groups in the postoperative time period. There were no significant differences between postoperative levels of remaining biomarkers. PreOp - preoperative. POD – postoperative day. *indicates significant differences between TEA and IVPCA patients (p < 0.05).
In order to evaluate significant variation from preoperative values and fold change in all detectable biomarkers, we compared the concentrations of the biomarkers on POD1, POD3, and POD5 to preoperative values in all patients as seen in Table 3. Of note MIP1b, INFγ, TNFα, IL-17, IL-12p70, CXCL12, Omentin1, sLeptinR, Vaspin, Galactin3, FGF23, PON1, FGF21, TGFb1, TGFb2, and TGFb3 did not vary significantly from preoperative concentrations. The peak fold changes for most biomarkers occurred on POD1, with the largest median fold changes noted in IL-6 (14 folds) and Pentraxin-3 (12 folds). CXCL10 values decreased below baseline (0.48 folds) on POD1. Most biomarker values began to trend back to baseline by POD3.
Table 3: Levels of fold change in detectable biomarkers in all patients
PreOp |
POD1 |
POD3 |
POD5 |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
Median (IQR) |
Median (IQR) |
Fold |
p |
Median |
Fold |
p |
Median |
Fold |
p |
|
IL6 |
13.0 (8.0, 34.7) |
73.6 (30.4, 202.9) |
14.852 |
0.052 |
32.2 (16.7, 49.9) |
5.857 |
0.041 |
16.6 (12.5, 31.3) |
2.582 |
0.320 |
IL8 |
82.75 (48.6, 118.5) |
151.0 (93.9, 280.9) |
2.554 |
0.000 |
112.4 (83.3, 158.6) |
1.726 |
0.046 |
115.4 (88.9, 156.4) |
1.638 |
0.052 |
IL12p70 |
7.2 (3.7, 12.5) |
7.7 (3.2, 10.2) |
0.773 |
0.137 |
4.8 (2.8, 10.0) |
0.678 |
0.918 |
6.5 (1.8, 10.1) |
1.063 |
0.135 |
CXCL10 |
101.1 (61.5, 232.2) |
51.5 (36.2, 116.1) |
0.487 |
0.040 |
79.2 (51.9, 136.4) |
0.946 |
0.209 |
97.7 (41.7, 203.5) |
0.857 |
0.492 |
CXCL12 |
965.15 (614.3, 1539.0) |
894.8 (534.4, 1255.4) |
0.730 |
0.362 |
1207.4 (628.6, 1925.9) |
1.022 |
0.854 |
1068.9 (614.1, 1824.6) |
1.039 |
0.965 |
INFg |
11.0 (3.4, 23.6) |
11.1 (6.3, 22.6) |
1.734 |
0.549 |
10.7 (5.9, 22.2) |
1.492 |
0.640 |
12.7 (4.7, 41.8) |
2.523 |
0.259 |
TNFa |
126.0 (92.9, 202.6) |
126.0 (81.9, 198.6) |
0.974 |
0.459 |
135.1 (101.9, 227.5) |
1.104 |
0.989 |
156.4 (95.5, 202.1) |
1.090 |
0.805 |
TGFb1 |
3003.15 (1189.3, 5068.0) |
3454.7 (2009.3, 5282.4) |
2.788 |
0.376 |
2703.7 (1198.7, 6157.2) |
2.224 |
0.926 |
2966.9 (1650.8, 4558.1) |
1.299 |
0.639 |
TGFb2 |
306.2 (203.8, 442.1) |
396.3 (206.1, 579.7) |
1.485 |
0.545 |
402.9 (242.5, 543.7) |
1.296 |
0.544 |
368.6 (238.1, 569.8) |
1.114 |
0.503 |
TGFb3 |
63.3 (46.4, 210.5) |
97.0 (77.4, 203.7) |
1.010 |
0.556 |
94.9 (62.3, 186.1) |
0.932 |
0.338 |
138.2 (65.0, 306.5) |
0.904 |
0.643 |
MIP1b |
95.7 (59.0, 143.9) |
67.0 (48.9, 142.3) |
0.962 |
0.645 |
95.8 (53.6, 141.9) |
1.020 |
0.960 |
81.7 (55.0, 137.1) |
1.083 |
0.558 |
MCP1 |
273.1 (182.7, 412.9) |
451.9 (240.2, 782.5) |
2.213 |
0.001 |
432.9 (288.7, 630.5) |
2.017 |
0.015 |
341.1 (241.7, 564.3) |
1.600 |
0.086 |
Resistin |
6224.6 (4342.7, 9855.6) |
13281.9 (7821.4, 20317.2) |
2.420 |
0.000 |
7221.3 (5229.1, 10051.4) |
1.357 |
0.201 |
7617.2 (4906.9, 11754.5) |
1.360 |
0.050 |
Omentin1 |
435901.4 (115754.4, 771727.2) |
504943.7 (133695.5, 932574.1) |
1.303 |
0.321 |
318922.5 (45931.7, 604216.9) |
0.695 |
0.703 |
129172.2 (14563.6, 346332.3) |
0.613 |
0.534 |
Pentraxin3 |
1438.9 (677.6, 3385.8) |
16795.8 (7074.2, 29856.8) |
12.094 |
0.001 |
5185.2 (3203.2, 10193.4) |
4.077 |
<0.001 |
4148.5 (1578.8, 8617.8) |
2.497 |
0.124 |
Galactin3 |
12861.8 (8025.9, 16893.3) |
13766.9 (10171.8, 17631.9) |
1.148 |
0.683 |
12268.2 (8340.8, 15990.7) |
1.037 |
0.297 |
11069.9 (6249.1, 16756.0) |
1.114 |
0.498 |
sLeptinR |
10687.72 (2290.0, 13971.2) |
9570.9 (2053.1, 14689.6) |
1.125 |
0.410 |
10503.6 (2535.6, 17330.9) |
1.069 |
0.756 |
11196.5 (1928.2, 19685.4) |
1.019 |
0.538 |
Vaspin |
97.9 (56.9, 294.8) |
39.7 (21.1, 92.0) |
0.426 |
0.283 |
99.5 (56.7, 270.4) |
0.986 |
0.455 |
121.7 (62.4, 231.5) |
0.775 |
0.599 |
FGF21 |
131.2 (59.0, 335.9) |
67.3 (27.5, 257.3) |
1.267 |
0.867 |
117.3 (45.4, 347.7) |
1.353 |
0.702 |
107.1 (48.5, 402.9) |
1.313 |
0.890 |
FGF23 |
91.7 (49.6, 173.8) |
76.8 (33.8, 181.8) |
1.060 |
0.376 |
93.0 (51.423, 171.9) |
0.956 |
0.520 |
122.6 (50.1, 361.7) |
1.303 |
0.296 |
PON1 |
6567750.0 (2181700.0, 8901800.0) |
5904950.0 (2512325.0, 8260475.0) |
1.019 |
0.818 |
6009250.0 (3126650.0, 9958075.0) |
1.132 |
0.582 |
3761700.0 (869938.9, 6759850.0) |
0.844 |
0.479 |
IL-6, IL-8, MCP-1, Resistin, Pentraxin3, and CXCL10 were noted to be significantly different from baseline. Remainder of cytokines did not vary significantly from baseline. PreoOp: preoperative. POD: postoperative day.
Of those biomarkers which varied significantly from baseline, Figure 2 illustrates that the TEA patients on POD1 had relatively lower mean fold changes from baseline compared to IV-PCA patients in IL-6 (13.5 vs. 19.1), MCP-1 (1.9 vs 3.0), IL-8 (2.4 vs 3.0), and Pentraxin-3 (10.8vs15.6) as well as similar increases in Resistin (2.4 vs. 2.4) and decrease in CXCL10 (0.47 vs. 0.53). Though most biomarkers trended back to baseline with similar fold changes in both groups on POD3 and POD5, the TEA group maintained IL-6, IL-8, MCP-1, and Pentraxin-3 levels that were significantly above baseline at these time points.
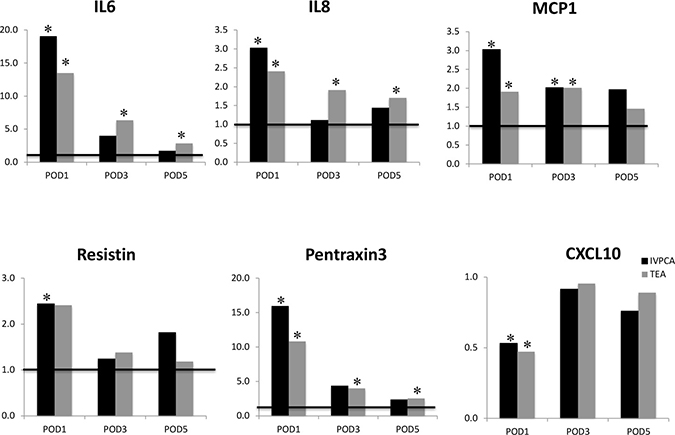
Figure 2: Mean fold change in biomarkers with significant variation from baseline in the IVPCA and TEA groups. *indicates significant difference from baseline in the TEA or the IVPCA group.
DISCUSSION
In this comprehensive and longitudinal systemic biomarker analysis of patients undergoing elective hepatic resection for metastatic disease in a randomized controlled trial comparing TEA to IV-PCA, we demonstrated that patients with epidural analgesia had a favorable postoperative biomarker profile for oncologic surgery with reduction in TGFb concentrations, dampened response to surgery in fold changes of IL-6, IL-8, MCP-1 and Pentraxin-3, as well as increased values of IL-12p70. The remaining novel markers including CXCL12, Omentin-1, and Galectin-3 did not vary significantly from baseline and were not significantly different between the epidural and IV-PCA groups in the postoperative period.
The increase in Pentraxin3 is a novel finding in the elective perioperative setting, and to the authors knowledge, this is the first study to demonstrate an impact from regional analgesia in the postoperative fold change of this biomarker. Pentraxin3 is an important prognostic marker in sepsis [26] as well as colorectal cancer [25], and it is involved in the propagation of inflammation, tissue remodeling, angiogenesis, and tumor related inflammation [27]. Interestingly, Pentraxin3 demonstrated significant elevations relative to preoperative values in the postoperative period with large fold changes similar to IL6. IL6, IL8, and MCP1, followed the previously demonstrated postoperative kinetics with peak values on POD1 [28–31]. Beyond the immune response to injury, these are pluripotent biomarkers and also have significant oncologic impact as each has been associated with tumor burden in clinical studies [25, 32, 33, 65] as well as mechanisms involved in tumor progression in preclinical experiments [34–36].
While some studies have demonstrated that epidural analgesia is associated with lower postoperative levels of these biomarkers in various surgical procedures [18–20, 37–42], our data and supporting literature suggests that the overall concentrations of these proinflammatory markers were not different between TEA and IV-PCA patients [17, 28, 43]. These mixed results are likely associated with the large variations in inflammatory marker measurements prior to surgery and potential individual patient response to any intervention or stimuli. Interestingly, when considering the variations from baseline and fold change in these biomarkers, epidural analgesia was associated with an initial dampened proinflammatory response in IL6, IL8, MCP1, and Pentraxin3 on POD1, but also persistent elevation of these biomarkers above baseline on POD3 and POD5. This finding is unlikely due to postoperative inflammatory events given the similar complication rate, but rather this is in keeping with clinical findings suggesting that epidural analgesia is associated with early benefits of patient experience and pain control, but it may not decrease hospital length of stay and in some cases may slow patient recovery [44].
In concert with the inflammatory reaction to surgical trauma, TGFb is among the immunosuppressive signals produced early in the postoperative period to regulate inflammation [45]. In the setting of resection of metastatic disease, this surge in TGFb likely has both pro- and anti-oncogenic properties in various tissues in that it can induce apoptosis in cancer cells in early metastatic niches, but can also suppress macrophage phagocytic function [46], promote epithelial mesenchymal transition [47], stimulate angiogenesis and stromal proliferation in more established metastatic disease [19, 47–50]. Within the TGFb super family, TGFb1, TGFb2, and TGFb3 play roles in these oncogenic processes and elevated systemic TGFb levels have been found to be correlate to poor prognosis factor in colorectal cancer [51–53]. Though TGFb levels overall did not vary significantly from baseline in this study, TGFb1 demonstrated a median fold change >2 in the postoperative period and the levels were significantly lower in the TEA group. These findings are consistent with a similar randomized control trial, in which patients with epidural analgesia undergoing elective colon cancer resections had significantly lower TGFb1 levels early in the postoperative period [19]. Interestingly, the postoperative TGFb2 and TGFb3 levels remained relatively close to preoperative values, however, unique to this study we have demonstrated that the levels of TGFb3 remained significantly lower in the TEA group through POD5 suggesting that overall the TEA group had lower systemic levels of immunosuppressive signaling in these patients.
The response to surgical insult also includes suppression of cell mediated immunity. The early postoperative period is characterized by a reduction in number and function of natural killer cells and cytotoxic T-cells [54], as well as a shift in Th1/Th2 signaling with suppression of Th1 cytokines [55]. Surrogate systemic markers for this process include IL12p70 [56–58] and CXCL10 [21]. Herein we found the expected suppression of CXCL10 in all patients and IL12p70 in the IV-PCA patients with preservation of IL12p70 systemic values on POD1 in TEA patients. The available literature suggests that compared to opioid based pain management, epidural analgesia does not maintain baseline IL12 levels [16, 18]. These studies, however, evaluated systemic IL12 levels including both the active heterodimer IL12p70 component involved in Th1 signaling and the less active IL12 subunits including IL12p40 and IL12p35. Hence we believe our specific analysis of IL12p70 is suggestive of preservation of Th1 signaling, and this is in keeping with data from other pre-clinical experiments [14] and randomized controlled trial demonstrating the preservation of cell mediated immunity with epidural analgesia [46, 47, 59, 60].
There are several limitations to this study. This is a subset analysis from a randomized controlled trial which included a smaller number of patients in the IV-PCA group compared to epidural group. This was in part due to the 2.5:1 randomization favoring epidural patients, but also limited by patients with available blood samples and further limited in the selection of patients with similar pathology and successful oncologic resection. This selection was prompted in order to have similar biomarker baselines values between patients with metastatic disease and comparable responses to inflammatory stimuli given the impact of tumor load on immune function [61]. The resulting subset analysis compared two groups with similar preoperative and postoperative factors associated with the inflammatory response, as demonstrated in Table 1, allowing for distinct evaluation of the effect of TEA vs. IV-PCA on the studied biomarkers in the postoperative period. Further analysis to consider the impact of alternative sources of inflammatory stimuli on comprehensive biomarker panels, such as the Charlson’s comorbidity index or postoperative infectious complications, should be considered, but are beyond the scope of this study [62]. In addition, previously published data from the original RCT (https://clinicaltrials.gov/ NCT01438476) demonstrated no differences in postoperative complications between patients allocated to the TEA or IV-PCA group.
Due to limited understanding of threshold values for pathologic significance of the studied biomarkers a sample size analysis based on meaningful change in these biomarkers could not be performed prior to this investigation [30]. The number of patients included in this analysis, however, is similar to other prospective trials investigating the impacts of regional analgesia on biomarker panels [17–19, 41]. Additional limitations include the poor signal quality noted in 11 of the 32 biomarkers. These assay deficits were unexpected given the well-established biomarker platform utilized in this study, particularly for biomarkers with known impacts from epidural analgesia in the perioperative setting such as VEGF [19] and IL10 [28]. Measurable time points may have been missed the temporal profile of some biomarkers given known early (<24 hours) postoperative peaks, and future biomarker studies should consider evaluation of biomarkers on the evening of surgery. Of note, the remaining traditional biomarkers (IL6, IL8, and MCP1) demonstrated reliable results with appropriate signal quality and predictable postoperative temporal variation based on literature review. Further, the comprehensive biomarker panel yielded novel impacts of epidural analgesia on biomarkers Pentraxin-3, IL12p70, and TGFb which support existing literature demonstrating that epidural analgesia may preserve postoperative oncological relevant immune function. Future studies to correlate these markers to other known markers of physiologic recovery from surgery are underway and will aid in further understanding of the mechanisms associated with regional analgesia.
MATERIALS AND METHODS
Patient selection
The patients in this study were part of the randomized controlled trial (RCT) conducted at University of Texas MD Anderson Cancer Center (https://clinicaltrials.gov/ NCT01438476) evaluating outcomes in patients undergoing liver resection with TEA vs. IV-PCA [63]. From the original trial database, patients were selected for this correlative study if they consented for additional blood draws and completed perioperative blood sample collection. In order to compare relative changes at each time point for individual perioperative biomarker levels, this subset analysis further selected patients with metastatic disease undergoing complete (R1 or R0) oncologic resection.
Epidural and patient controlled analgesia regimens
Perioperative analgesia regimens for the TEA and IV-PCA groups have been previously described [63]. In brief, patients in the TEA group underwent preoperative epidural placement between the 5th and 10th thoracic intervertebral space and after a test dose, received epidural hydromorphone and lidocaine prior to incision, and then received continuous epidural infusion of bupivacaine and hydromorphone. This continued until the patient was tolerating a regular diet and could be transitioned to oral pain medications. Patients in the IV-PCA group underwent intra-operative and postoperative intravenous (IV) hydromorphone based analgesia. Additional non-opioid pain medications could be administered by the patient’s primary team or acute pain service.
Clinicopathologic variables and postoperative recovery variables
Patient data including age, gender, American Society of Anesthesiologist physical status classification system (ASA) score, body mass index (BMI), receipt of preoperative chemotherapy within 90 days of surgery, portal vein embolization, extent of hepatectomy, surgical incision, operative time, estimated blood loss (EBL), perioperative transfusion, post-operative complication, histology of metastatic disease, opioid consumption (measured in morphine mg equivalents) and quality of pain control were collected. Major hepatectomy was defined by resection of 3 or more Couinaud segments [64]. Pain scores were recorded throughout the postoperative time period by numeric/visual pain scale (0–10), and inadequately controlled pain in the early post-operative period was defined as a pain score of 7 or greater reported in the first 48 hours.
Biomarkers
Patients who agreed to blood draws underwent collection of venous blood at the preoperative visit (T0) within 2 weeks before surgery, as well as collection of venous blood on the mornings of postoperative day (POD) 1, POD 3, and POD5. Plasma samples were prepared and levels (pg/mL) were assessed using multiplex bead assay (Bio-Rad Laboratories, Hercules, CA, USA and EMD, Bioscience Research Reagents, Temecula, CA, USA) as previously described [65]. The 27 biomarkers (MIP-1b, IL-6, INFγ, IL-5, GM-CSF, TNFα, IL-2, IL-1b, IL-13, IL-4, MCP-1, IL-8, IL-10, G-CSF, VEGF, Resistin, IL-7, IL-12p70, IL-17, CXCL12, CXCL10, Omentin-1, Pentraxin-3, Galactin-3, TGFb1, TGFb2, and TGFb3) were selected by literature review for analysis given known variation with inflammatory stimuli and oncologic relevance in signaling pathways. The biomarkers sLeptin R, Vaspin, FGF-21, FGF-23, and PON-1 were included as portions of the multiplex bead assay. Acceptable signal quality to calculate the values (pg/mL) for these biomarkers was determined only by the values within the standards concentration range for each assay. To confirm reliability, all biomarker values were performed in duplicate on the established assay by a single research team member and all patient’s time point samples were arranged on to a single plate.
Statistical analysis
Demographic, intraoperative, and postoperative data were analyzed and summarized using medians (interquartile ranges [IQRs]) or means (standard deviations or 95% confidence intervals) to account for outliers and non-normality in our description of study variables. Chi-squared test was used for categorical clinicopathologic variables, and Wilcoxon rank-sum tests were used for continuous clinicopathologic variables as well as to compare time point values of biomarkers between groups. Given that the oncological relevant value or “biologic effect size” of the studied biomarkers in the perioperative setting has not been established per systemic concentration or relative fold change to baseline with respect to the impact of analgesic modalities, the postoperative biomarker values were compared in traditional fashion according to systemic concentration [pg/mL] between groups at each time point as well as by considerations of individual patient fold change at each time point relative to preoperative baseline [66–68]. A p value < 0.05 was considered statistically significant. Data were analyzed using SPSS software (version 23).
CONCLUSIONS
In this subset analysis of a randomized controlled trial comparing TEA vs. IV-PCA, circulating biomarker concentrations in patients undergoing TEA demonstrated a dampened early pro-inflammatory response to surgery as well as maintenance of markers of cell mediated immunity, while also demonstrating persistently lower levels of immunosuppressive signaling throughout the postoperative period in patients with epidural analgesia. These results add to a growing body of literature to support further investigation of systemic biomarkers with oncologic mechanisms and known variation with inflammatory stimuli to further understand how perioperative inflammation impacts oncologic outcomes. Novel to this study, Pentraxin3 demonstrated significant variation with both surgical stress and anesthetic technique and could be considered for future investigations aimed at evaluating techniques to dampen perioperative inflammation.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Tzeng CW, Aloia TA. Colorectal liver metastases. J Gastrointest Surg. 2013; 17:195–201; quiz p.-2. https://doi.org/10.1007/s11605-012-2022-3.
2. Zimmitti G, Vauthey JN, Shindoh J, Tzeng CW, Roses RE, Ribero D, Capussotti L, Giuliante F, Nuzzo G, Aloia TA. Systematic use of an intraoperative air leak test at the time of major liver resection reduces the rate of postoperative biliary complications. J Am Coll Surg. 2013; 217:1028–37. https://doi.org/10.1016/j.jamcollsurg.2013.07.392.
3. Andreou A, Aloia TA, Brouquet A, Dickson PV, Zimmitti G, Maru DM, Kopetz S, Loyer EM, Curley SA, Abdalla EK, Vauthey JN. Margin status remains an important determinant of survival after surgical resection of colorectal liver metastases in the era of modern chemotherapy. Ann Surg. 2013; 257:1079–88. https://doi.org/10.1097/SLA.0b013e318283a4d1.
4. Govaert KM, Jongen JMJ, Kranenburg O, Borel Rinkes IHM. Surgery-induced tumor growth in (metastatic) colorectal cancer. Surg Oncol. 2017; 26:535–43. https://doi.org/10.1016/j.suronc.2017.10.004.
5. Sekandarzad MW, van Zundert AAJ, Lirk PB, Doornebal CW, Hollmann MW. Perioperative Anesthesia Care and Tumor Progression. Anesth Analg. 2017; 124:1697–708. https://doi.org/10.1213/ANE.0000000000001652.
6. Gupta K, Kshirsagar S, Chang L, Schwartz R, Law PY, Yee D, Hebbel RP. Morphine stimulates angiogenesis by activating proangiogenic and survival-promoting signaling and promotes breast tumor growth. Cancer Res. 2002; 62:4491–8.
7. de Oliveira GS Jr, Ahmad S, Schink JC, Singh DK, Fitzgerald PC, McCarthy RJ. Intraoperative neuraxial anesthesia but not postoperative neuraxial analgesia is associated with increased relapse-free survival in ovarian cancer patients after primary cytoreductive surgery. Reg Anesth Pain Med. 2011; 36:271–7. https://doi.org/10.1097/AAP.0b013e318217aada.
8. Lin L, Liu C, Tan H, Ouyang H, Zhang Y, Zeng W. Anaesthetic technique may affect prognosis for ovarian serous adenocarcinoma: a retrospective analysis. Br J Anaesth. 2011; 106:814–22. https://doi.org/10.1093/bja/aer055.
9. Biki B, Mascha E, Moriarty DC, Fitzpatrick JM, Sessler DI, Buggy DJ. Anesthetic technique for radical prostatectomy surgery affects cancer recurrence: a retrospective analysis. Anesthesiology. 2008; 109:180–7. https://doi.org/10.1097/ALN.0b013e31817f5b73.
10. McSorley ST, Watt DG, Horgan PG, McMillan DC. Postoperative Systemic Inflammatory Response, Complication Severity, and Survival Following Surgery for Colorectal Cancer. Ann Surg Oncol. 2016; 23:2832–40. https://doi.org/10.1245/s10434-016-5204-5.
11. Zimmitti G, Soliz J, Aloia TA, Gottumukkala V, Cata JP, Tzeng CW, Vauthey JN. Positive Impact of Epidural Analgesia on Oncologic Outcomes in Patients Undergoing Resection of Colorectal Liver Metastases. Ann Surg Oncol. 2016; 23:1003–11. https://doi.org/10.1245/s10434-015-4933-1.
12. Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology. 2006; 105:660–4.
13. Cata JP, Bauer M, Sokari T, Ramirez MF, Mason D, Plautz G, Kurz A. Effects of surgery, general anesthesia, and perioperative epidural analgesia on the immune function of patients with non-small cell lung cancer. J Clin Anesth. 2013; 25:255–62. https://doi.org/10.1016/j.jclinane.2012.12.007.
14. Wada H, Seki S, Takahashi T, Kawarabayashi N, Higuchi H, Habu Y, Sugahara S, Kazama T. Combined spinal and general anesthesia attenuates liver metastasis by preserving TH1/TH2 cytokine balance. Anesthesiology. 2007; 106:499–506.
15. Conrick-Martin I, Kell MR, Buggy DJ. Meta-analysis of the effect of central neuraxial regional anesthesia compared with general anesthesia on postoperative natural killer T lymphocyte function. J Clin Anesth. 2012; 24:3–7. https://doi.org/10.1016/j.jclinane.2011.09.001.
16. Ahlers O, Nachtigall I, Lenze J, Goldmann A, Schulte E, Hohne C, Fritz G, Keh D. Intraoperative thoracic epidural anaesthesia attenuates stress-induced immunosuppression in patients undergoing major abdominal surgery. Br J Anaesth. 2008; 101:781–7. https://doi.org/10.1093/bja/aen287.
17. Fant F, Tina E, Sandblom D, Andersson SO, Magnuson A, Hultgren-Hornkvist E, Axelsson K, Gupta A. Thoracic epidural analgesia inhibits the neuro-hormonal but not the acute inflammatory stress response after radical retropubic prostatectomy. Br J Anaesth. 2013; 110:747–57. https://doi.org/10.1093/bja/aes491.
18. Moselli NM, Baricocchi E, Ribero D, Sottile A, Suita L, Debernardi F. Intraoperative epidural analgesia prevents the early proinflammatory response to surgical trauma. Results from a prospective randomized clinical trial of intraoperative epidural versus general analgesia. Ann Surg Oncol. 2011; 18:2722–31. https://doi.org/10.1245/s10434-011-1700-9.
19. Xu YJ, Chen WK, Zhu Y, Wang SL, Miao CH. Effect of thoracic epidural anaesthesia on serum vascular endothelial growth factor C and cytokines in patients undergoing anaesthesia and surgery for colon cancer. Br J Anaesth. 2014; 113:i49–55. https://doi.org/10.1093/bja/aeu148.
20. Chen JQ, Wu Z, Wen LY, Miao JZ, Hu YM, Xue R. Preoperative and postoperative analgesic techniques in the treatment of patients undergoing transabdominal hysterectomy: a preliminary randomized trial. BMC Anesthesiol. 2015; 15:70. https://doi.org/10.1186/s12871-015-0046-4.
21. Mohty AM, Grob JJ, Mohty M, Richard MA, Olive D, Gaugler B. Induction of IP-10/CXCL10 secretion as an immunomodulatory effect of low-dose adjuvant interferon-alpha during treatment of melanoma. Immunobiology. 2010; 215:113–23. https://doi.org/10.1016/j.imbio.2009.03.008.
22. Mota JM, Leite CA, Souza LE, Melo PH, Nascimento DC, de-Deus-Wagatsuma VM, Temporal J, Figueiredo F, Noushmehr H, Alves-Filho JC, Cunha FQ, Rego EM. Post-Sepsis State Induces Tumor-Associated Macrophage Accumulation through CXCR4/CXCL12 and Favors Tumor Progression in Mice. Cancer Immunol Res. 2016; 4:312–22. https://doi.org/10.1158/2326-6066.CIR-15-0170.
23. Li D, Zhao X, Xiao Y, Mei H, Pu J, Xiang X, Jiao W, Song H, Qu H, Huang K, Zheng L, Tong Q. Intelectin 1 suppresses tumor progression and is associated with improved survival in gastric cancer. Oncotarget. 2015; 6:16168–82. https://doi.org/10.18632/oncotarget.3753.
24. Xin M, Dong XW, Guo XL. Role of the interaction between galectin-3 and cell adhesion molecules in cancer metastasis. Biomed Pharmacother. 2015; 69:179–85. https://doi.org/10.1016/j.biopha.2014.11.024.
25. Di Caro G, Carvello M, Pesce S, Erreni M, Marchesi F, Todoric J, Sacchi M, Montorsi M, Allavena P, Spinelli A. Circulating Inflammatory Mediators as Potential Prognostic Markers of Human Colorectal Cancer. PLoS One. 2016; 11:e0148186. https://doi.org/10.1371/journal.pone.0148186.
26. Lee YT, Gong M, Chau A, Wong WT, Bazoukis G, Wong SH, Lampropoulos K, Xia Y, Li G, Wong MCS, Liu T, Wu WKK, Tse G. Pentraxin-3 as a marker of sepsis severity and predictor of mortality outcomes: A systematic review and meta-analysis. J Infect. 2018; 76:1–10. https://doi.org/10.1016/j.jinf.2017.10.016.
27. Garlanda C, Bottazzi B, Bastone A, Mantovani A. Pentraxins at the crossroads between innate immunity, inflammation, matrix deposition, and female fertility. Annu Rev Immunol. 2005; 23:337–66. https://doi.org/10.1146/annurev.immunol.23.021704.115756.
28. Siekmann W, Eintrei C, Magnuson A, Sjolander A, Matthiessen P, Myrelid P, Gupta A. Surgical and not analgesic technique affects postoperative inflammation following colorectal cancer surgery: a prospective, randomized study. Colorectal Dis. 2017; 19:O186–O95. https://doi.org/10.1111/codi.13643.
29. Strey CW, Marquez-Pinilla RM, Markiewski MM, Siegmund B, Oppermann E, Lambris JD, Bechstein WO. Early post-operative measurement of cytokine plasma levels combined with pre-operative bilirubin levels identify high-risk patients after liver resection. Int J Mol Med. 2011; 27:447–54. https://doi.org/10.3892/ijmm.2010.592.
30. Bradley MJ, Vicente DA, Bograd BA, Sanders EM, Leonhardt CL, Elster EA, Davis TA. Host responses to concurrent combined injuries in non-human primates. J Inflamm (Lond). 2017; 14:23. https://doi.org/10.1186/s12950-017-0170-7.
31. Cata JP, Velasquez JF, Ramirez MF, Vauthey JN, Gottumukkala V, Conrad C, Kim BJ, Aloia T. Inflammation and pro-resolution inflammation after hepatobiliary surgery. World J Surg Oncol. 2017; 15:152. https://doi.org/10.1186/s12957-017-1220-6.
32. Guthrie GJ, Roxburgh CS, Richards CH, Horgan PG, McMillan DC. Circulating IL-6 concentrations link tumour necrosis and systemic and local inflammatory responses in patients undergoing resection for colorectal cancer. Br J Cancer. 2013; 109:131–7. https://doi.org/10.1038/bjc.2013.291.
33. Krzystek-Korpacka M, Diakowska D, Kapturkiewicz B, Bebenek M, Gamian A. Profiles of circulating inflammatory cytokines in colorectal cancer (CRC), high cancer risk conditions, and health are distinct. Possible implications for CRC screening and surveillance. Cancer Lett. 2013; 337:107–14. https://doi.org/10.1016/j.canlet.2013.05.033.
34. Cavassani KA, Carson WF 4th, Moreira AP, Wen H, Schaller MA, Ishii M, Lindell DM, Dou Y, Lukacs NW, Keshamouni VG, Hogaboam CM, Kunkel SL. The post sepsis-induced expansion and enhanced function of regulatory T cells create an environment to potentiate tumor growth. Blood. 2010; 115:4403–11. https://doi.org/10.1182/blood-2009-09-241083.
35. Matsumoto Y, Tsujimoto H, Ono S, Shinomiya N, Miyazaki H, Hiraki S, Takahata R, Yoshida K, Saitoh D, Yamori T, Yamamoto J, Hase K. Abdominal Infection Suppresses the Number and Activity of Intrahepatic Natural Killer Cells and Promotes Tumor Growth in a Murine Liver Metastasis Model. Ann Surg Oncol. 2016; 23:S257–65. https://doi.org/10.1245/s10434-015-4466-7.
36. Hotchkiss RS, Monneret G, Payen D. Sepsis-induced immunosuppression: from cellular dysfunctions to immunotherapy. Nat Rev Immunol. 2013; 13:862–74. https://doi.org/10.1038/nri3552.
37. Caputo M, Alwair H, Rogers CA, Ginty M, Monk C, Tomkins S, Mokhtari A, Angelini GD. Myocardial, inflammatory, and stress responses in off-pump coronary artery bypass graft surgery with thoracic epidural anesthesia. Ann Thorac Surg. 2009; 87:1119–26. https://doi.org/10.1016/j.athoracsur.2008.12.047.
38. Ezhevskaya AA, Mlyavykh SG, Anderson DG. Effects of continuous epidural anesthesia and postoperative epidural analgesia on pain management and stress response in patients undergoing major spinal surgery. Spine (Phila Pa 1976). 2013; 38:1324–30. https://doi.org/10.1097/BRS.0b013e318290ff26.
39. Fares KM, Mohamed SA, Hamza HM, Sayed DM, Hetta DF. Effect of thoracic epidural analgesia on pro-inflammatory cytokines in patients subjected to protective lung ventilation during Ivor Lewis esophagectomy. Pain Physician. 2014; 17:305–15.
40. Kun L, Tang L, Wang J, Yang H, Ren J. Effect of Combined General/Epidural Anesthesia on Postoperative NK Cell Activity and Cytokine Response in Gastric Cancer Patients Undergoing Radical Resection. Hepatogastroenterology. 2014; 61:1142–7.
41. Marta GN, Riera R, Bossi P, Zhong LP, Licitra L, Macedo CR, de Castro G, Carvalho AL, William WN, Kowalski LP. Induction chemotherapy prior to surgery with or without postoperative radiotherapy for oral cavity cancer patients: Systematic review and meta-analysis. European Journal of Cancer. 2015; 51:2596–603. https://doi.org/10.1016/j.ejca.2015.08.007.
42. Zhao J, Mo H. The Impact of Different Anesthesia Methods on Stress Reaction and Immune Function of the Patients with Gastric Cancer during Peri-Operative Period. J Med Assoc Thai. 2015; 98:568–73.
43. Chloropoulou P, Iatrou C, Vogiatzaki T, Kotsianidis I, Trypsianis G, Tsigalou C, Paschalidou E, Kazakos K, Touloupidis S, Simopoulos K. Epidural anesthesia followed by epidural analgesia produces less inflammatory response than spinal anesthesia followed by intravenous morphine analgesia in patients with total knee arthroplasty. Med Sci Monit. 2013; 19:73–80.
44. Guay J, Nishimori M, Kopp SL. Epidural Local Anesthetics Versus Opioid-Based Analgesic Regimens for Postoperative Gastrointestinal Paralysis, Vomiting, and Pain After Abdominal Surgery: A Cochrane Review. Anesth Analg. 2016; 123:1591–602. https://doi.org/10.1213/ane.0000000000001628.
45. Menger MD, Vollmar B. Surgical trauma: hyperinflammation versus immunosuppression? Langenbecks Arch Surg. 2004; 389:475–84. https://doi.org/10.1007/s00423-004-0472-0.
46. Ayala A, Meldrum DR, Perrin MM, Chaudry IH. The release of transforming growth factor-beta following haemorrhage: its role as a mediator of host immunosuppression. Immunology. 1993; 79:479–84.
47. Pudova EA, Kudryavtseva AV, Fedorova MS, Zaretsky AR, Shcherbo DS, Lukyanova EN, Popov AY, Sadritdinova AF, Abramov IS, Kharitonov SL, Krasnov GS, Klimina KM, Koroban NV, et al. HK3 overexpression associated with epithelial-mesenchymal transition in colorectal cancer. BMC Genomics. 2018; 19:113. https://doi.org/10.1186/s12864-018-4477-4.
48. Bachman KE, Park BH. Duel nature of TGF-beta signaling: tumor suppressor vs. tumor promoter. Curr Opin Oncol. 2005; 17:49–54.
49. Wang JL, Qi Z, Li YH, Zhao HM, Chen YG, Fu W. TGFbeta induced factor homeobox 1 promotes colorectal cancer development through activating Wnt/beta-catenin signaling. Oncotarget. 2017; 8:70214–25. https://doi.org/10.18632/oncotarget.19603.
50. Fukuchi M, Masuda N, Miyazaki T, Nakajima M, Osawa H, Kato H, Kuwano H. Decreased Smad4 expression in the transforming growth factor-beta signaling pathway during progression of esophageal squamous cell carcinoma. Cancer. 2002; 95:737–43. https://doi.org/10.1002/cncr.10727.
51. Bellone G, Carbone A, Tibaudi D, Mauri F, Ferrero I, Smirne C, Suman F, Rivetti C, Migliaretti G, Camandona M, Palestro G, Emanuelli G, Rodeck U. Differential expression of transforming growth factors-beta1, -beta2 and -beta3 in human colon carcinoma. Eur J Cancer. 2001; 37:224–33.
52. Kuczynski EA, Viloria-Petit AM, Coomber BL. Colorectal carcinoma cell production of transforming growth factor beta decreases expression of endothelial cell vascular endothelial growth factor receptor 2. Cancer. 2011; 117:5601–11. https://doi.org/10.1002/cncr.26247.
53. Huang X, Lee C. From TGF-beta to cancer therapy. Curr Drug Targets. 2003; 4:243–50.
54. Goldfarb Y, Sorski L, Benish M, Levi B, Melamed R, Ben-Eliyahu S. Improving postoperative immune status and resistance to cancer metastasis: a combined perioperative approach of immunostimulation and prevention of excessive surgical stress responses. Ann Surg. 2011; 253:798–810. https://doi.org/10.1097/SLA.0b013e318211d7b5.
55. Hensler T, Hecker H, Heeg K, Heidecke CD, Bartels H, Barthlen W, Wagner H, Siewert JR, Holzmann B. Distinct mechanisms of immunosuppression as a consequence of major surgery. Infect Immun. 1997; 65:2283–91.
56. Del Prete G. The concept of type-1 and type-2 helper T cells and their cytokines in humans. Int Rev Immunol. 1998; 16:427–55.
57. Athie-Morales V, Smits HH, Cantrell DA, Hilkens CM. Sustained IL-12 signaling is required for Th1 development. J Immunol. 2004; 172:61–9.
58. Oth T, Vanderlocht J, Van Elssen CH, Bos GM, Germeraad WT. Pathogen-Associated Molecular Patterns Induced Crosstalk between Dendritic Cells, T Helper Cells, and Natural Killer Helper Cells Can Improve Dendritic Cell Vaccination. Mediators Inflamm. 2016; 2016:5740373. https://doi.org/10.1155/2016/5740373.
59. Volk T, Schenk M, Voigt K, Tohtz S, Putzier M, Kox WJ. Postoperative epidural anesthesia preserves lymphocyte, but not monocyte, immune function after major spine surgery. Anesth Analg. 2004; 98:1086–92, table of contents.
60. Wei L, Meng QG, Bi ZG. Result of a randomized clinical trial comparing different types of anesthesia on the immune function of patients with osteosarcoma undergoing radical resection. Panminerva Med. 2013; 55:211–6.
61. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014; 15:e493–503. https://doi.org/10.1016/s1470-2045(14)70263-3.
62. Tan WP, Talbott VA, Leong QQ, Isenberg GA, Goldstein SD. American Society of Anesthesiologists class and Charlson’s comorbidity index as predictors of postoperative colorectal anastomotic leak: a single-institution experience. J Surg Res. 2013; 184:115–9. https://doi.org/10.1016/j.jss.2013.05.039.
63. Aloia TA, Kim BJ, Segraves-Chun YS, Cata JP, Truty MJ, Shi Q, Holmes A, Soliz JM, Popat KU, Rahlfs TF, Lee JE, Wang XS, Morris JS, et al. A Randomized Controlled Trial of Postoperative Thoracic Epidural Analgesia Versus Intravenous Patient-controlled Analgesia After Major Hepatopancreatobiliary Surgery. Ann Surg. 2017; 266:545–54. https://doi.org/10.1097/SLA.0000000000002386.
64. Couinaud C. [The anatomy of the liver]. [Article in French]. Ann Ital Chir. 1992; 63:693–7.
65. Chen ZY, Raghav K, Lieu CH, Jiang ZQ, Eng C, Vauthey JN, Chang GJ, Qiao W, Morris J, Hong D, Hoff P, Tran H, Menter DG, et al. Cytokine profile and prognostic significance of high neutrophil-lymphocyte ratio in colorectal cancer. Br J Cancer. 2015; 112:1088–97. https://doi.org/10.1038/bjc.2015.61.
66. Namas RA, Vodovotz Y, Almahmoud K, Abdul-Malak O, Zaaqoq A, Namas R, Mi Q, Barclay D, Zuckerbraun B, Peitzman AB, Sperry J, Billiar TR. Temporal Patterns of Circulating Inflammation Biomarker Networks Differentiate Susceptibility to Nosocomial Infection Following Blunt Trauma in Humans. Ann Surg. 2016; 263:191–8. https://doi.org/10.1097/sla.0000000000001001.
67. Henry NL, Hayes DF. Cancer biomarkers. Mol Oncol. 2012; 6:140–6. https://doi.org/10.1016/j.molonc.2012.01.010.
68. Ioannidis JP, Panagiotou OA. Comparison of effect sizes associated with biomarkers reported in highly cited individual articles and in subsequent meta-analyses. JAMA. 2011; 305:2200–10. https://doi.org/10.1001/jama.2011.713.