
INTRODUCTION
Since Huggins first reported that surgical castration is an effective treatment for advanced prostate cancer [1], hormonal therapy has become an established intervention for previously untreated patients with this disease. In 1982, Labrie et al. indicated the need for anti-androgen drug administration concomitant with surgical or medical castration [2]. Since then, androgen deprivation therapy (ADT) and combined androgen blockade (CAB) have been commonly used for the treatment of locally advanced or metastatic prostate cancer. CAB was not found to be superior to ADT monotherapy in Western countries [3]; however, controlled trials in Japan found that CAB led to significantly longer overall survival (OS) than ADT monotherapy (hazard ratio [HR]: 0.78) in patients with stages C and D1 disease, although not in those with stage D2 disease [4, 5]. As a result, CAB is frequently administered to Japanese prostate cancer patients [6]. In Western countries, the Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy (STAMPEDE) trial found that the failure-free survival in patients receiving ADT monotherapy was only 11 months [7]. Moreover, OS following ADT monotherapy was 24 months among patients with prostate cancer who had bone metastasis at initial diagnosis and 16 months among those who had visceral metastasis; the median OS of those who had both types of metastasis was 14 months [8]. Since these data indicate that ADT is not sufficiently effective for patients with metastatic prostate cancer, new treatment methods have been explored. Some studies showed that docetaxel or abiraterone in combination with initial hormonal therapy was more effective for high-risk prostate cancer patients than ADT monotherapy [9–12]. In these studies, however, ADT monotherapy was used in all the control groups, whereas in Japan, CAB is often used as the initial hormonal therapy. Therefore, it remains unclear whether ADT combined with docetaxel or abiraterone is beneficial for Japanese patients.
Few studies have investigated the time to progression to castration-resistant prostate cancer (CRPC) following the initiation of hormonal therapy. In the ‘Chemo-Hormonal Therapy versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer’ (CHAARTED) trial [9], Sweeny et al. found that the median time to biochemical, symptomatic, or radiographic progression was 11.7 months in patients receiving ADT monotherapy. Hinotsu et al. reported clinically acceptable progression-free survival and OS in prostate cancer patients treated with ADT [13]. However, they did not investigate the time to transition from hormone-naive prostate cancer to CRPC.
Therefore, in our current study, we focused on prostate cancer patients who initially underwent hormonal therapy (particularly CAB) and examined their prognoses and time to progression to CRPC. Furthermore, we evaluated these same endpoints specifically in high-risk prostate cancer patients to determine the effectiveness of CAB.
RESULTS
Table 1 summarizes the patients’ characteristics. The 10-year and 15-year OS rates were 74.0% and 50.4%, respectively (median: not reached). Forty-eight patients died of any cause during the follow-up period. Furthermore, the 10-year and the 15-year disease-specific survival rates were both 86.8% (median: not reached). Twenty-one patients died during the follow-up period due to prostate cancer.
Table 1: Patients characteristics (N = 387)
Age in years, median (range) |
77 |
(49–95) |
Observation period in months, median (range) |
33.3 |
(0.4–230.1) |
PSA at initial diagnosis in ng/mL, median (range) |
41 |
(2.2–9675) |
Gleason score at initial diagnosis (%) |
||
≤6 |
32 |
(8.2) |
7 |
71 |
(18.3) |
≥8 |
265 |
(68.5) |
unknown |
19 |
(5.0) |
T stage (%) |
||
1 |
31 |
(8.0) |
2 |
164 |
(42.4) |
3 |
122 |
(31.5) |
4 |
61 |
(15.8) |
unknown |
9 |
(2.3) |
Presence of metastatic lesion(s) (%) |
||
Yes |
159 |
(41.1) |
No |
228 |
(58.9) |
Metastatic site |
||
Bone |
151 |
|
Distal lymph node |
23 |
|
Lung |
20 |
|
Others |
3 |
|
Extent of disease of bone metastasis |
||
1 |
74 |
|
(<3 bone lesions) |
(52) |
|
(≥3 bone lesions) |
(22) |
|
2 |
54 |
|
3 |
19 |
|
4 |
5 |
Abbreviations: PSA, prostate-specific antigen.
Disease-specific survival was stratified by the prostate-specific antigen (PSA) level at diagnosis (<20 vs. ≥20 ng/mL), Gleason score (GS) (≤7 vs. ≥8), and the presence of metastatic foci (Figure 1). Disease-specific survival was significantly shorter among patients with initial PSA ≥20 ng/mL, those with a GS ≥8, and those with metastasis at initial diagnosis. Multivariate analysis revealed that the presence of metastasis at initial diagnosis was an independent negative prognostic factor (Table 2).
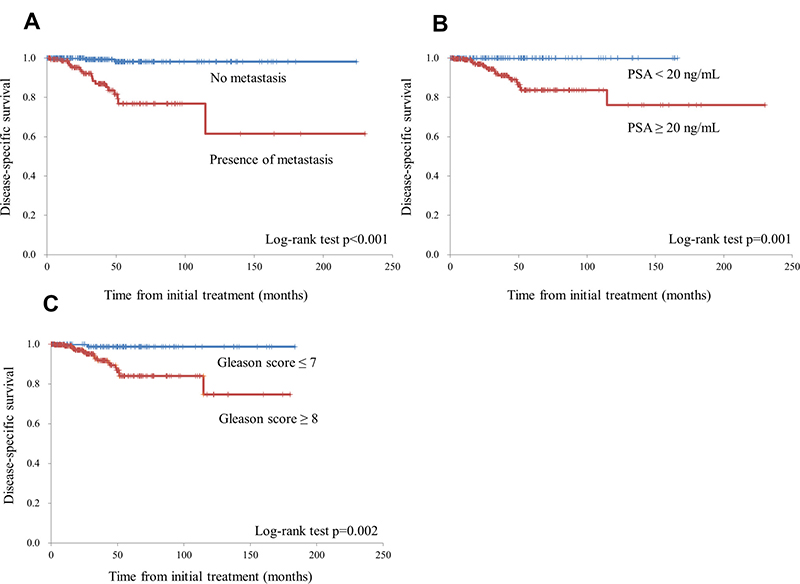
Figure 1: The disease-specific survival rate was stratified by the presence of metastatic foci (A), prostate-specific antigen (PSA) levels at diagnosis (<20 ng/mL vs. ≥20 ng/mL) (B), and the Gleason score (≤7 vs. ≥8) (C).
Table 2: Cox proportional stepwise multivariate analysis for the association between the variables and disease-specific survival
Unadjusted |
Adjusted |
||||||||
|---|---|---|---|---|---|---|---|---|---|
Comparison |
Ten-year disease-specific survival in months |
HR (95% CI) |
p-value |
HR (95% CI) |
p-value |
||||
Presence of metastasis at initial diagnosis |
vs |
No metastasis |
61.5% |
vs |
98.2% |
17.7 (4.1–76.2) |
<0.001 |
13.4 (3.0–59.1) |
<0.001 |
PSA ≥20 ng/mL |
vs |
PSA <20 ng/mL |
76.1% |
vs |
100.0% |
NA |
NA |
NA |
|
Gleason score ≥8 |
vs |
Gleason score ≤7 |
74.7% |
vs |
98.7% |
12.2 (1.6–90.9) |
0.015 |
7.2 (0.9–56.2) |
0.059 |
Abbreviations: HR, hazard ratio; CI, confidence interval; NA, not applicable; PSA, prostate-specific antigen.
A total of 105 of the 387 patients progressed to CRPC; the median time to CRPC development was 140.7 months (Figure 2). The time to CRPC development was stratified by PSA levels, GS, and the presence of metastatic foci as described above. The time to CRPC was significantly shorter in patients with PSA ≥20 ng/mL, those with a GS ≥8, and those with metastasis at initial diagnosis (Figure 3); all these variables were found to be independent prognostic factors on multivariate analysis (Table 3).
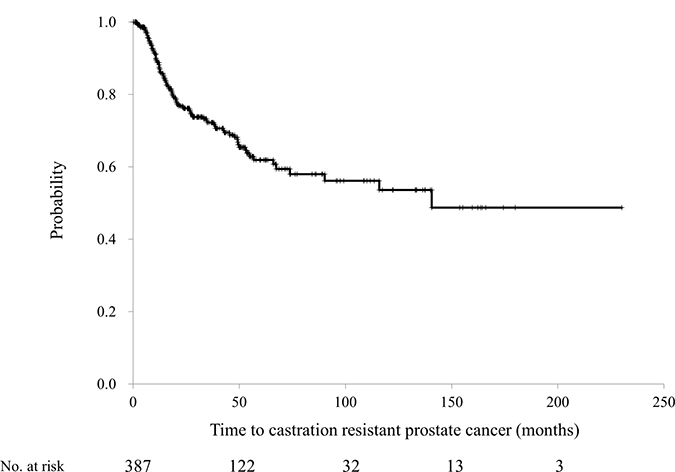
Figure 2: The time to developing castration-resistant prostate cancer among the 387 patients with prostate cancer treated by combined androgen blockade.
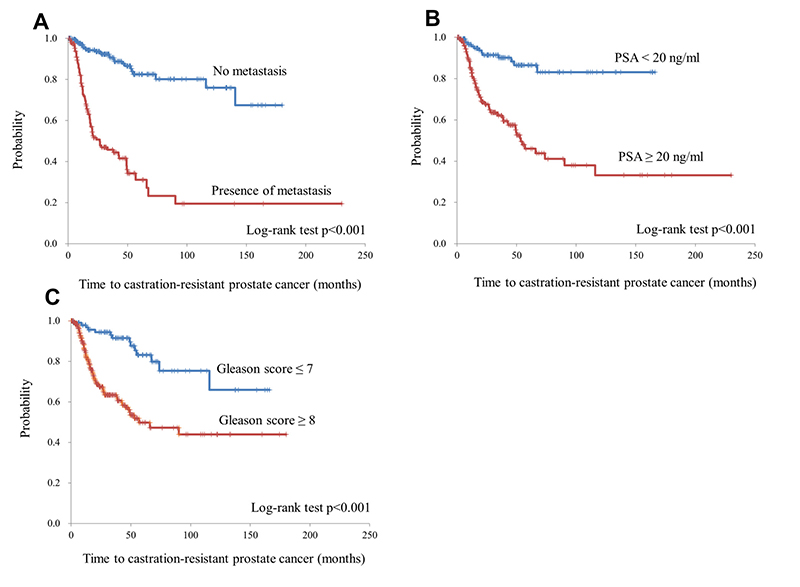
Figure 3: The time to developing castration-resistant prostate cancer was stratified by the presence of metastatic foci (A), prostate-specific antigen (PSA) levels at diagnosis (<20 ng/mL vs. ≥20 ng/mL) (B), and Gleason score (≤7 vs. ≥8) (C).
Table 3: Cox proportional stepwise multivariate analysis for the association between the variables and time to CRPC
Unadjusted |
Adjusted |
||||||||
|---|---|---|---|---|---|---|---|---|---|
Comparison |
Time to CRPC in months (median) |
HR (95% CI) |
p-value |
HR (95% CI) |
p-value |
||||
Presence of metastasis at initial diagnosis |
vs |
No metastasis |
26.6 |
vs |
not reached |
7.00 (4.47–10.97) |
<0.001 |
4.79 (2.93–7.83) |
<0.001 |
PSA ≥20 ng/mL |
vs |
PSA <20 ng/mL |
53.5 |
vs |
not reached |
4.93 (2.75–8.84) |
<0.001 |
2.48 (1.29–4.73) |
0.006 |
Gleason score ≥8 |
vs |
Gleason score ≤7 |
56.8 |
vs |
not reached |
3.88 (2.19–6.85) |
<0.001 |
2.17 (1.20–3.91) |
0.010 |
Abbreviations: CRPC, castration resistant prostate cancer; HR, hazard ratio; CI, confidence interval; NA, not applicable; PSA, prostate-specific antigen.
The extent of disease (EOD) of bone metastasis has previously been shown to be closely correlated with OS [14]. Therefore, we analyzed the disease-specific survival rate and time to CRPC development in patients stratified according to EOD grade (0, 1, or ≥2). The Kaplan–Meier curves generated for patients with no bone metastasis and those with EOD grade 1 were similar (Figure 4). Next, we stratified the patients according to EOD grade ≤1 vs. ≥2, and found that disease-specific survival was significantly shorter in patients of the latter group (EOD grades ≤1: median not reached; EOD grades ≥2: median 114.6 months, HR 20.4; 95% confidence interval [CI]: 7.3–56.9; p < 0.001). The same was true for patients with CRPC (EOD grades ≤1: median not reached; EOD grades ≥2: median 15.0 months, HR 6.4; 95% CI: 4.3–9.6; p < 0.001).
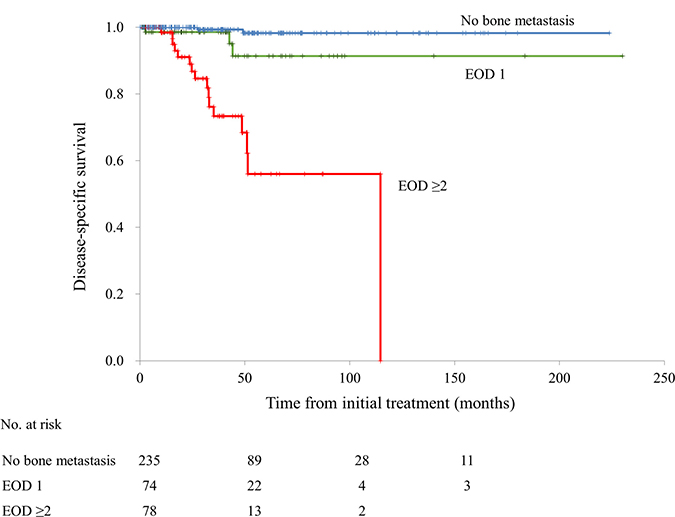
Figure 4: The disease-specific survival rate classified by the extent of disease (EOD) grade (0, 1, or ≥2).
In terms of patients with high-risk disease, 72 patients (48.6%) had EOD grade ≥2, metastasis at initial diagnosis, and a GS ≥8; 6 patients (4.1%) had EOD grade ≥2 and metastasis at initial diagnosis; and 70 patients (47.3%) had metastasis at diagnosis and a GS ≥8. Disease-specific survival among patients in this high-risk group was significantly shorter than those in the low-risk group (median: 114.6 months vs. not reached; HR 23.3, 95% CI: 5.3–102.5; p < 0.001) (Figure 5A). Similarly, the time to CRPC development was significantly shorter in the high-risk group than in the low-risk group (median: 20.5 months vs. not reached; HR 8.2, 95% CI: 5.3–12.8; p < 0.001) (Figure 5B).
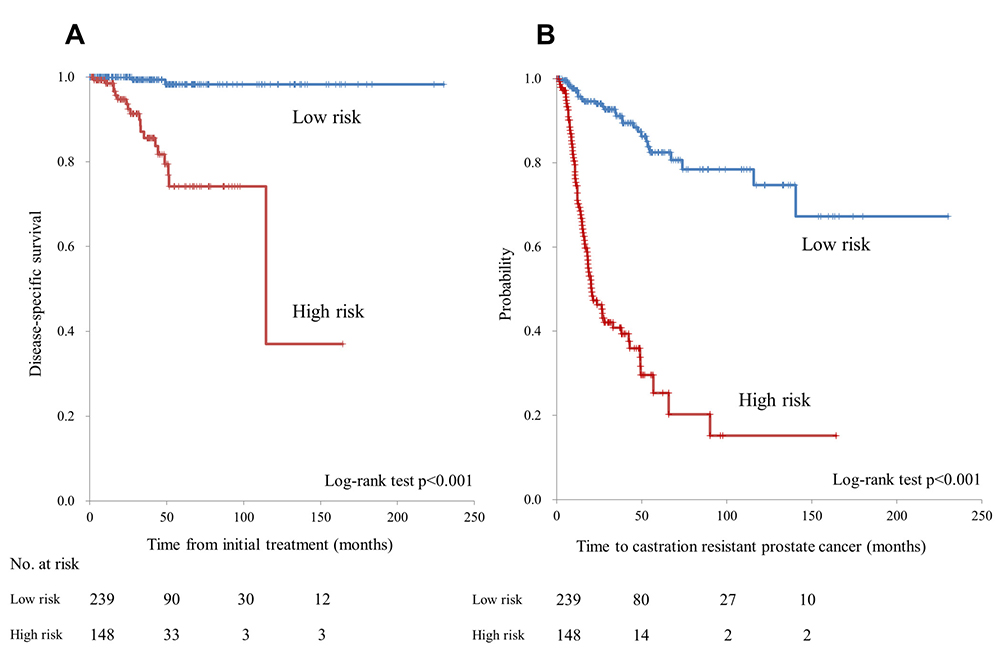
Figure 5: (A) Disease-specific survival in the low- and high-risk patient groups. (B) Time to progression to castration-resistant prostate cancer in the low- and high-risk patient groups.
Eighty-nine patients (84.8%) proceeded to the next treatment step after being diagnosed with CRPC; they were administered flutamide (n = 60), enzalutamide (n = 48), abiraterone (n = 14), docetaxel (n = 17), cabazitaxel (n = 8), steroids (n = 22), or other drugs (n = 5).
DISCUSSION
To our knowledge, ours is the first study to determine the time to CRPC development in patients who underwent CAB as the initial hormonal therapy for prostate cancer. Overall, the effectiveness of CAB was long-lasting (140 months), but varied markedly according to various risk factors.
Serum PSA level ≥20 ng/mL, a GS ≥8, and presence of metastasis at initial diagnosis were all independent prognostic factors for faster progression to CRPC. In particular, patients with metastasis at initial diagnosis developed castration-resistant disease after a median of 26.6 months, which indicated that the efficacy period of CAB was very short in this population. Since most metastatic foci at initial diagnosis were found in the bones, we also investigated the relationship between the volume of bone metastasis and time to CRPC development. Generally, the volume of bone metastatic foci is expressed on a 5-/point EOD scale [14]. Accordingly, a significant difference in the time to CRPC development was observed between patients with EOD grade 1 and those with EOD grades ≥2. Among patients with bone metastasis, those who have a huge volume of bone metastatic foci may not respond to CAB treatment and may therefore require alternative therapies. Recent studies found that administering docetaxel or abiraterone to early stage hormone-sensitive patients with metastatic prostate cancer prolonged OS [9, 11, 12]. These clinical trials were characteristic in that they all focused on metastatic or high-risk patients, although their definitions of “high-risk” were not consistent. Before our analysis, therefore, we defined “high-risk” patients as those who satisfied at least two of the following three criteria, which were independent risk factors determined using multivariable analysis: the presence of metastasis (visceral and/or bone metastasis) at initial diagnosis, a GS ≥8, and bone metastasis EOD grade ≥2. Serum PSA level was excluded from the analysis because none of the patients with PSA <20 ng/mL died of cancer. We found that both disease-specific survival and time to CRPC development were significantly shorter in the high-risk group than in the low-risk group. In particular, the median time to CRPC development in the high-risk group was a remarkably short 20.5 months. Although comparisons are difficult, these data may indicate that the time to CRPC development following CAB treatment may be shorter than that observed in abiraterone-treated patients in the STAMPEDE and LATITUDE trials [12, 15]. The median age of this study population was 77 years, and the median age of the high-risk group was 75 years. This is an older group than the LATTITUDE trial population. Nevertheless, time to CRPC development was short in the high-risk group; therefore, age may not affect time to CRPC development. Another study examined whether the time to CRPC development could be prolonged by using zoledronic acid in combination with CAB for prostate cancer patients who had bone metastasis at initial diagnosis, but found that the combinational effect was very weak [16]. Taken together, high-risk patients as defined by our criteria may require alternatives to CAB.
The time to CRPC development in the entire high-risk group (20.5 months) was longer than that in patients specifically with EOD grade ≥2 (15.0 months). This is because patients who had both metastasis at initial diagnosis and a GS ≥8 accounted for approximately half of the high-risk group. In other words, the difference can be attributable to the fact that approximately half of the high-risk group comprised patients who had smaller volumes of bone metastatic foci (EOD grade ≤1).
We found that metastasis at initial diagnosis was an independent risk factor of disease-specific survival. Moreover, patients with a GS ≥8 had poorer prognoses than those with a GS ≤7. These findings were similar to those in a controlled trial conducted in Japan to compare CAB and castration monotherapy [5], and supports the possibility that CAB may not be as effective for patients with metastases discovered at initial diagnosis.
Analyses such as ours usually investigate OS; however, we used disease-specific survival because our patients were of older age, with a median age of 77 years, and the death rate from other causes was high (56%). Furthermore, due to the relatively high survival rates, these results should be interpreted with caution. In fact, the median OS was long even in the high-risk patient group (114 months). However, this may partly be because a relatively large number of high-risk patients were lost to follow-up. It should also be noted that the data from high-risk patients were immature because disease-specific death occurred less often. However, since it has been reported that a longer time to CRPC development may correlate with improved OS [17], a longer follow-up period is required.
In summary, the time to CRPC development in patients who underwent CAB as initial therapy and who had metastasis at initial diagnosis was short, as it was for high-risk patients as defined by our criteria. We conclude that CAB treatment is not sufficiently effective for such patients. While the effectiveness of new hormonal drugs to treat CRPC is becoming increasingly evident [18, 19], it remains unknown whether using these drugs for untreated metastatic prostate cancer at an early stage can prolong OS compared to their use at a later stage. Thus, a future prospective study is warranted in this regard.
PATIENTS AND METHODS
A total of 387 patients who were pathologically diagnosed with adenocarcinoma of the prostate at the Osaka City University Hospital and the Bell Land General Hospital between May 2007 and December 2017 (a 10-year period), were judged not to be candidates for local treatment, and consequently underwent combination therapy as first-line treatment were enrolled in our study. These therapies included gonadotropin-releasing hormone agonists (3.75 mg leuprolide acetate or 3.6 mg goserelin acetate every 4 weeks or 11.25 mg leuprolide acetate or 10.8 mg goserelin acetate every 12 weeks) or gonadotropin-releasing hormone antagonists (initial dose of 240 mg and maintenance dose of 80 mg of degarelix every 4 weeks) as well as anti-androgen drugs (80 mg of bicalutamide orally once a day or 125 mg of flutamide orally 3 times a day) (CAB). Degarelix was discontinued due to adverse events, and a gonadotropin-releasing hormone agonist (leuprorelin acetate or goserelin acetate) was used for maintenance therapy [20]. We examined OS, disease-specific survival, and time to CRPC development in these patients. Disease-specific survival and time to CRPC were stratified by PSA levels at diagnosis (<20 ng/mL vs. ≥20 ng/mL), GS (≤7 or ≥8), and the presence of metastatic foci before performing comparative analyses.
Furthermore, we focused on “high-risk” prostate cancer patients, who were defined as those satisfying two of the following three criteria: EOD of bone metastasis grade ≥2; presence of metastasis at diagnosis (visceral and/or bone metastasis); and a GS ≥8. Patients not meeting at least two of these criteria were considered “low-risk.” On the basis of the number or extent of metastases, patients were divided into five EOD grades based on bone scintigraphy scans as follows: 0, normal or abnormal due to benign bone disease; 1, number of bony metastases less than 6, each of which is less than 50% the size of a vertebral body (one lesion about the size of a vertebral body would be counted as two lesions); 2, number of bone metastases between 6 and 20, size of lesions as described above; 3, number of metastases more than 20 but less than a “super scan”; and 4, “super scan” or its equivalent, i.e., metastasis to more than 75% of the ribs, vertebrae, and pelvic bones [14].
Clinical and histological staging were based on the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (version 3, 2016). The definition of CRPC was based on meeting the following European Association of Urology Guidelines criteria: serum testosterone level <50 ng/dL plus 1) successive increases in PSA level during three consecutive measurements obtained ≥1 week apart, an increase of ≥25% on two PSA readings, and a PSA level ≥2.0 ng/mL; or 2) the exacerbation of an existing lesion or development of a new lesion on imaging. OS, disease-specific survival, and the time to CRPC development were estimated using the Kaplan–Meier method, with differences determined using the log-rank test. Cox proportional stepwise multivariate analysis was used to evaluate associations of PSA, GS, and presence of metastatic lesions at initial diagnosis with cause-specific survival and time to CRPC development. A two-sided p-value of < 0.05 was considered statistically significant. All statistical analyses were performed using Microsoft Excel® (Microsoft, Redmond, WA, USA). Permission to access the database for a review of the medical records of the patients was obtained from the local research ethics committee at Osaka City University (approval number 4011).
Abbreviations
ADT: androgen deprivation therapy; CAB: combined androgen blockade; CRPC: castration-resistant prostate cancer; EOD: extent of disease; GS: Gleason score; HR: hazard ratio; OS: overall survival; PSA: prostate-specific antigen.
Author contributions
Conception and design, drafting of the manuscript: Satoshi Tamada. Acquisition of data: Taro Iguchi, Minoru Kato, Takeshi Yamasaki, Jumpei Asakawa, Kazuaki Kita, Yudai Matsuoka, Kazuyuki Yamaguchi, Kentaro Matsumura, Ishun Go, Tetsuji Ohmachi. Analysis and interpretation of data: Satoshi Tamada, Sayaka Yasuda. Final approval of the manuscript: Tatsuya Nakatani.
ACKNOWLEDGMENTS
We would like to thank Ms. Ayako Akagi for data collection, as well as Mr. Maehira (https://www.igaku-honyaku.jp/) and Editage (https://www.editage.jp) for English language editing.
CONFLICTS OF INTEREST
T. Iguchi and T. Nakatani have received research funding from Astellas Japan (Tokyo, Japan), Bayer Yakuhin. Ltd (Osaka, Japan). The remaining authors have declared no conflict of interest.
FUNDING
None.
REFERENCES
1. Huggins C, Hodges CV. Studies on prostatic cancer. I. The effect of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res. 1941; 1:293–97.
2. Labrie F, Dupont A, Belanger A, Cusan L, Lacourciere Y, Monfette G, Laberge JG, Emond JP, Fazekas AT, Raynaud JP, Husson JM. New hormonal therapy in prostatic carcinoma: combined treatment with an LHRH agonist and an antiandrogen. Clin Invest Med. 1982; 5:267–75.
3. Prostate Cancer Trialists Collaborative Group. Maximum androgen blockade in advanced prostate cancer: an overview of the randomised trials. Prostate Cancer Trialists’ Collaborative Group. Lancet. 2000; 355:1491–98.
4. Akaza H, Yamaguchi A, Matsuda T, Igawa M, Kumon H, Soeda A, Arai Y, Usami M, Naito S, Kanetake H, Ohashi Y. Superior anti-tumor efficacy of bicalutamide 80 mg in combination with a luteinizing hormone-releasing hormone (LHRH) agonist versus LHRH agonist monotherapy as first-line treatment for advanced prostate cancer: interim results of a randomized study in Japanese patients. Jpn J Clin Oncol. 2004; 34:20–28.
5. Akaza H, Hinotsu S, Usami M, Arai Y, Kanetake H, Naito S, Hirao Y, and Study Group for the Combined Androgen Blockade Therapy of Prostate Cancer. Combined androgen blockade with bicalutamide for advanced prostate cancer: long-term follow-up of a phase 3, double-blind, randomized study for survival. Cancer. 2009; 115:3437–45.
6. Onozawa M, Hinotsu S, Tsukamoto T, Oya M, Ogawa O, Kitamura T, Suzuki K, Naito S, Namiki M, Nishimura K, Hirao Y, Akaza H. Recent trends in the initial therapy for newly diagnosed prostate cancer in Japan. Jpn J Clin Oncol. 2014; 44:969–81.
7. James ND, Spears MR, Clarke NW, Dearnaley DP, De Bono JS, Gale J, Hetherington J, Hoskin PJ, Jones RJ, Laing R, Lester JF, McLaren D, Parker CC, et al. Survival with Newly Diagnosed Metastatic Prostate Cancer in the “Docetaxel Era”: Data from 917 Patients in the Control Arm of the STAMPEDE Trial (MRC PR08, CRUK/06/019). Eur Urol. 2015; 67:1028–38.
8. Gandaglia G, Karakiewicz PI, Briganti A, Passoni NM, Schiffmann J, Trudeau V, Graefen M, Montorsi F, Sun M. Impact of the Site of Metastases on Survival in Patients with Metastatic Prostate Cancer. Eur Urol. 2015; 68:325–34.
9. Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, Wong YN, Hahn N, Kohli M, Cooney MM, Dreicer R, Vogelzang NJ, Picus J, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015; 373:737–46.
10. Gravis G, Boher JM, Joly F, Soulié M, Albiges L, Priou F, Latorzeff I, Delva R, Krakowski I, Laguerre B, Rolland F, Théodore C, Deplanque G, et al, and GETUG. Androgen Deprivation Therapy (ADT) Plus Docetaxel Versus ADT Alone in Metastatic Non castrate Prostate Cancer: Impact of Metastatic Burden and Long-term Survival Analysis of the Randomized Phase 3 GETUG-AFU15 Trial. Eur Urol. 2016; 70:256–62.
11. James ND, Sydes MR, Clarke NW, Mason MD, Dearnaley DP, Spears MR, Ritchie AW, Parker CC, Russell JM, Attard G, de Bono J, Cross W, Jones RJ, et al, and STAMPEDE investigators. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016; 387:1163–77.
12. Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Özgüroğlu M, Ye D, Feyerabend S, Protheroe A, De Porre P, Kheoh T, Park YC, et al, and LATITUDE Investigators. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2017; 377:352–60.
13. Hinotsu S, Akaza H, Usami M, Ogawa O, Kagawa S, Kitamura T, Tsukamoto T, Naito S, Namiki M, Hirao Y, Murai M, Yamanaka H, and Japan Study Group of Prostate Cancer (J-CaP). Current status of endocrine therapy for prostate cancer in Japan analysis of primary androgen deprivation therapy on the basis of data collected by J-CaP. Jpn J Clin Oncol. 2007; 37:775–81.
14. Soloway MS, Hardeman SW, Hickey D, Raymond J, Todd B, Soloway S, Moinuddin M. Stratification of patients with metastatic prostate cancer based on extent of disease on initial bone scan. Cancer. 1988; 61:195–202.
15. James ND, de Bono JS, Spears MR, Clarke NW, Mason MD, Dearnaley DP, Ritchie AW, Amos CL, Gilson C, Jones RJ, Matheson D, Millman R, Attard G, et al, and STAMPEDE Investigators. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N Engl J Med. 2017; 377:338–51.
16. Kamba T, Kamoto T, Maruo S, Kikuchi T, Shimizu Y, Namiki S, Fujimoto K, Kawanishi H, Sato F, Narita S, Satoh T, Saito H, Sugimoto M, et al, and ZAPCA Study Group. A phase III multicenter, randomized, controlled study of combined androgen blockade with versus without zoledronic acid in prostate cancer patients with metastatic bone disease: results of the ZAPCA trial. Int J Clin Oncol. 2017; 22:166–73.
17. Frees S, Akamatsu S, Bidnur S, Khalaf D, Chavez-Munoz C, Struss W, Eigl BJ, Gleave M, Chi KN, So A. The impact of time to metastasis on overall survival in patients with prostate cancer. World J Urol. 2018; 36:1039–46.
18. Ryan CJ, Smith MR, de Bono JS, Molina A, Logothetis CJ, de Souza P, Fizazi K, Mainwaring P, Piulats JM, Ng S, Carles J, Mulders PF, Basch E, et al, and COU-AA-302 Investigators. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013; 368:138–48.
19. Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, Iversen P, Bhattacharya S, Carles J, Chowdhury S, Davis ID, de Bono JS, Evans CP, et al, and PREVAIL Investigators. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014; 371:424–33.
20. Asakawa J, Iguchi T, Tamada S, Yasuda S, Ninomiya N, Kato M, Yamasaki T, Ohmachi T, Nakatani T. A change from gonadotropin releasing hormone antagonist to gonadotropin releasing hormone agonist therapy does not affect the oncological outcomes in hormone sensitive prostate cancer. Basic Clin Androl. 2018; 28:9.