
INTRODUCTION
Primary liver cancer, which consists predominantly of hepatocellular carcinoma (HCC), has the seventh highest age-adjusted cancer incidence rate in the world, with approximately 0.8 million diagnosed cases worldwide in 2012 [1]. A recent Canadian burden of illness study showed that the prevalence of advanced liver disease, including HCC is increasing [2]. There are a number of disease, environmental and genetic risk factors for HCC, including viral hepatitis (B and C), cirrhosis, alcoholic liver disease, non-alcoholic fatty liver disease, aflatoxin intake, diabetes, obesity and hereditary hemochromatosis [3, 4].
Of particular interest with respect to HCC incidence is its link from chronic Hepatitis C (CHC), where the incidence is generally increased in cirrhotic liver at rates ranging from 1 to 8% per year [4–8]. Individuals with CHC are treated with anti-viral therapy including interferon (INF)/pegylated interferon (peg-INF)-based therapy in combination with ribavirin and more recently direct-acting anti-viral agents (DAAs) with the most current options of all oral IFN-free combinations. The primary objective for anti-viral therapy is to completely eradicate the virus to obtain sustained virological response (SVR), defined as continued absence of detectable hepatitis C virus (HCV) RNA (≤25 IU/mL) at least 12 weeks after the end of treatment [9, 10]. The goal of achievement of SVR is the reduction of all-cause mortality and liver-related complications [11]. Therefore, long-term data on the effect of SVR on the development of HCC has been an important topic of interest [12, 13].
Given the rapidly changing environment in new anti-viral agents over the last several years with increasing SVR rates (potentially over 95% of certain CHC patient populations), the long-term effects of SVR will eventually need to be determined as more data becomes available. Two older systematic review/meta-analyses and a small review with IFN as the sole treatment agent or IFN + ribavirin have been performed looking at the effects on the development in HCC concluding a reduction in HCC for those who achieved SVR [12–14]. In view of the long-term follow-up of patients that needs to occur to detect an outcome such as HCC and the changing landscape in antiviral treatments (introduction of DAAs), we thought it would be important to re-review the literature and open up the inclusion criteria to include both mono and co-infect patients as well as all fibrosis stages, recognizing that cirrhotic patients who received regimens which included IFN tended to be more complicated and were less likely to achieve SVR. The objective of this meta-analysis was to assess the incidence of HCC in all adult CHC patients receiving antiviral therapy who achieved SVR and to compare with those who did not achieve SVR.
RESULTS
Selected studies
A total of 1095 published articles were obtained through the literature search. After review using the inclusion criteria, 72 articles were chosen for full publication review and analysis and 4 additional studies found on Google Scholar were also included. After a thorough review of the published articles, with careful attention to ensuring that HCC incidence rates were recorded in both SVR and non-SVR groups, a total of 42 articles were chosen for further review and analysis. There was an attempt to contact one author who did not separate out the HCC incidence rates between SVR and non-SVR groups, however this attempt failed and the study was excluded [17]. Of the 42 articles that were chosen for further analysis, 4 of these (2 each) reported on the same cohort of patients (i.e. duplicates); one did not have enough information between SVR and non-SVR groups and thus were excluded from the final analysis. In addition, one of the studies excluded due to duplication of the cohort in another publication [18]. Therefore, there were 37 studies included in the final analysis. Figure 1 provides information on the flow of the study selection process.
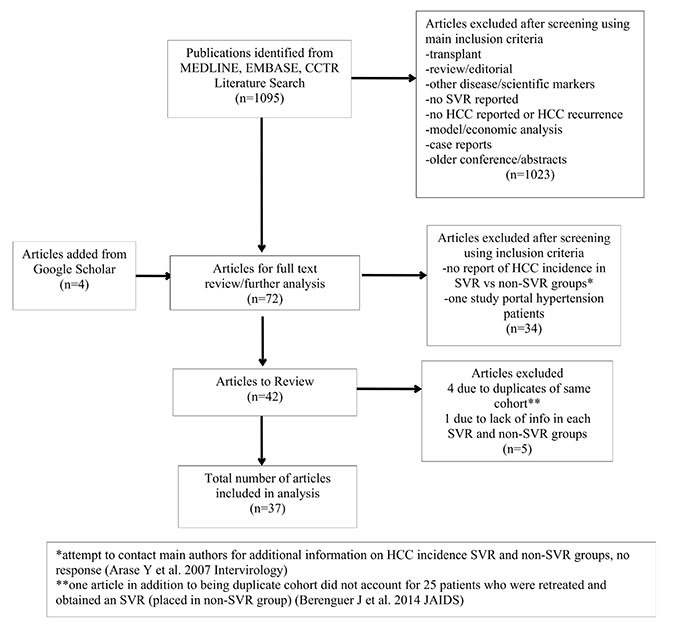
Figure 1: Literature search and study selection (MEDLINE, EMBASE, CCTR, Google Scholar).
Risk of bias quality assessment
The 37 studies chosen for review and analysis were assessed through the Newcastle-Ottawa scale, and all had good quality scores with star ratings ranging from 5–8 (i.e. mid to low risk of bias). The rating of each study is found in Table 1.
Table 1: Risk of bias quality assessment based on Newcastle-Ottawa scale (star rating)
Study/Year |
Selection |
Comparability |
Outcome |
Total Rating |
|---|---|---|---|---|
Alfaleh FZ et al. Liver Intl'/2013 [30] |
*** |
* |
*** |
7 |
Aleman S et al. Clinical Infec. Dis./2013 [31] |
**** |
* |
*** |
8 |
Berenguer J et al. J of Hepatology/2013 [32] |
*** |
* |
** |
6 |
Braks R El et al. World J of Gastro/2007 [33] |
*** |
* |
*** |
7 |
Bruno S et al. Hepatology/2007 [26] |
** |
* |
*** |
6 |
Cardoso AC et al. Journal of Hepatology/2010 [34] |
*** |
* |
*** |
7 |
Cardoso-Ruiz P et al. AGA abstract Sa1300/2014 [35] |
*** |
* |
* |
5 |
Chang KC et al. BJC/2013 [27] |
*** |
* |
* |
5 |
Cheinquer N et al. Brazil J Infec. Dis./2010 [36] |
**** |
* |
** |
7 |
Coverdale S et al. Am J of Gastro/2004 [37] |
*** |
* |
** |
6 |
Fenkel JM et al. Hepatology Suppl./2014 [38] |
**** |
* |
*** |
8 |
Florcani A et al. J Clin. Gastroennterol/2008 [39] |
*** |
* |
*** |
7 |
Hasegawa et al. Hepatology Research/2007 [40] |
*** |
* |
* |
5 |
Hung CH et al. Antiviral Therapy/2011 [41] |
**** |
* |
** |
7 |
Hung CH et al. J of Viral Hepatitis/2006 [42] |
**** |
* |
*** |
8 |
Iacobellis A et al. Clinical Gastro and Hepatol/2011 [43] |
**** |
* |
*** |
8 |
Ikeda K et al. Intervirology/2006 [44] |
**** |
* |
*** |
8 |
Imazeki F et al. Liver Intl./2005 [45] |
*** |
* |
** |
6 |
Kim JH et al Yonsei Medical Journal/2006 [46] |
**** |
* |
* |
6 |
Kobayashi S et al. Liver Intl/2007 [47] |
**** |
* |
*** |
8 |
Kurokawa M et al. Hepatology Research/2009 [48] |
**** |
* |
* |
6 |
Lee MH et al. Hepatology AASLD Abstracts/2014 [49] |
**** |
* |
* |
6 |
Mallet V et al. Annals of internal Medicine/2008 [50] |
**** |
* |
** |
7 |
Maruoka D et al. J of Gastro and Hepatol/2012 [51] |
**** |
* |
** |
7 |
Moon et al. Digestive Disease/2015 [52] |
**** |
* |
* |
6 |
Morgan et al. Hepatology/2010 [53] |
**** |
* |
*** |
8 |
Ogawa E et al. Journal of Hepatology/2013 [54] |
**** |
* |
* |
6 |
Osaki Y et al. J Gastroenterol/2012 [55] |
**** |
* |
* |
6 |
Rutter et al. Alimenatary Pharmacology and Therapeutics/2015 [56] |
**** |
* |
** |
7 |
Shiratori et al. Annals of Internal Medicine/2005 [57] |
**** |
* |
** |
7 |
Tanaka H et al. Int. J. Cancer/2000 [58] |
**** |
* |
** |
7 |
van der Meer AJP et al. JAMA/2012 [11] |
**** |
* |
*** |
8 |
Velosa J et al. Dig. Dis. Sci./2011 [59] |
**** |
* |
*** |
8 |
Wang CH et al. Hepatol Int. (conference abstract)/2013 [60] |
**** |
* |
** |
7 |
Yoshida et al. Gut/2004 [61] |
**** |
* |
** |
7 |
Yu ML et al. BMC Infectious Diseases/2005 [20] |
**** |
* |
** |
7 |
Yu ML et al. Antiviral Therapy/2006 [19] |
**** |
* |
** |
7 |
Studies characteristics
All of the studies included in the analysis were long-term follow-up cohorts, with 12 prospective and 25 retrospective in nature. Further information on the characteristics of the studies and patient population are summarized in Table 2. Three studies were conference abstracts. Two studies included HIV co-infect patients, one study HBV co-infect and the rest were CHC mono-infect patients. Twenty-one studies were published from Asia, eleven from Europe, one of these included Canada as part of the cohort, two from the United States, and one study each came from Brazil, Saudi Arabia and Australia reflecting the fact that the prevalence of CHC is worldwide.
Table 2: Key patient characteristics of study population: hepatitis C treated with antiviral therapy (IFN, peg-IFN mono or with Ribavirin (n = 36) or boceprevir/telaprevir triple therapy (n = 1)
Author/Year |
Country |
Type of cohort/Population |
Mean age (years) |
Males (%) |
Follow-up weighted mean (years) |
Total sample size (N) |
SVR/non-SVR (%) |
HCC incidence SVR/non-SVR (%) |
Fibrosis F0-2/F3-4 (%) |
|---|---|---|---|---|---|---|---|---|---|
Alfaleh FZ/2013 [30] |
Saudi Arabia |
retrospective/mono |
48 ± 11.8 |
47.8 |
5.3 |
157 |
39.5/60.5 |
0.0/4.2 |
46.5/1.9* |
Aleman S/2013 [31] |
Sweden |
prospective/mono |
51 ± 9 |
69.0 |
8.6 |
303 |
36.3/63.7 |
5.5/13.5 |
0/100 |
Berenguer J/2013 [32] |
Spain |
retrospective/HIV co-infect |
40.5 |
74.8 |
4.6 |
1599 |
36.5/63.5 |
0.34/2.3 |
61.1/38.9 |
Braks R/2007 [33] |
France |
retrospective/mono |
54.1 ± 11.2 |
61.1 |
7.7 |
113 |
32.7/67.3 |
2.7/31.6 |
0/100 |
Bruno S/2007 [26] |
Italy |
retrospective/HIV co-infect |
54.7 ± 8.6 |
63.1 |
8,0 |
883 |
14.0/86.0 |
5.6/16.1 |
0/100 |
Cardoso AC/2010 [34] |
France |
retrospective/mono |
55 ± 10 |
67 |
9.5 |
307 |
33.6/66.4 |
5.8/19.6 |
0/100 |
Cordero-Ruiz P/2014 [35] |
Spain |
retrospective/mono |
NR |
NR |
13 |
182 |
46.7/53.3 |
3.5/12.4 |
87.3/12.7 |
Chang KC/2013 [27] |
Taiwan |
retrospective/mono |
NR** |
45.6 |
NR |
1879 |
68.0/32.0 |
7.3/24.8 |
55/45 |
Cheinquer N/2010 [36] |
Brazil |
prospective/mono |
51.85 |
65.5 |
2.4 |
85 |
44.7/55.3 |
2.6/17.0 |
0/100 |
Coverdale S/2004 [37] |
Australia |
prospective/mono |
40.5 |
67.0 |
9.4 |
343 |
14.6/85.4 |
2.0/10.1 |
NR |
Fenkel JM/2014 [38] |
USA |
retrospective/mono |
NR |
53.3 |
NR |
190 |
51.6/48.4 |
1.0/8.7 |
55.3/44.7 |
Floreani A/2008 [39] |
Italy |
prospective/mono |
50.1 |
51.4 |
2.0 |
365 |
61.1/38.9 |
0.0/3.5 |
76/24 |
Hasegawa E/2007 [40] |
Japan |
retrospective/mono |
57.95 |
64.95 |
7.3 |
105 |
45.7/54.3 |
6.25/33.3 |
0/100 |
Hung CH/2011 [41] |
Taiwan |
prospective/HBV co-infect |
|||||||
HBV co-infect |
53 ± 11.2 |
60.7 |
5.8 |
135 |
71.1/28 |
4.2/28.2 |
67.5/32.5 |
||
Mono |
51.8 ± 11.2 |
52.1 |
1470 |
69.9/30.1 |
3.2/12.2 |
||||
Hung CH/2006 [42] |
Taiwan |
prospective/mono |
56.25 |
52.3 |
3.1 |
132 |
55.3/44.7 |
6.8/18.6 |
0/100 |
Iacobellis A/2011 [43] |
Italy |
prospective/mono |
60.5 |
62.6 |
4.2 |
75 |
32.0/68.0 |
12.5/21.6 |
0/100 |
Ikeda K/2006 [44] |
Japan |
retrospective/mono |
44.0 |
60.7 |
10.4 |
1654 |
37.0/63.0 |
18.3/8.1 |
62.2/37.8 |
Imazeki F/2005 [45] |
Japan |
retrospective/mono |
50.1 ± 12 |
61.0 |
8.9 |
355 |
32.7/67.3 |
3.4/18.8 |
72.6/27.4 |
Kim JH/2006 [46] |
Korea |
retrospective/mono |
49.8 ± 11.8 |
60.1 |
3.2 |
138 |
41.3/58.7 |
0.0/37.0 |
NR |
Kobayashi S/2007 [47] |
Japan |
retrospective/mono |
49.3 |
50.5 |
5.8 |
1124 |
33.2/66.8 |
3.5/8.1 |
NR |
Kurokawa M/2009 [48] |
Japan |
prospective/mono |
55.8 ± 10.9 |
63.8 |
2.8 |
403 |
34.5/65.5 |
2.9/7.95 |
54.5/45.5 |
Lee MH/2014 [49] |
Taiwan |
retrospective/mono |
55.4 |
49.6 |
5.0 |
1778 |
86.7/13.3 |
2.4/5.1 |
86.2/13.8 |
Mallet V/2008 [50] |
France |
retrospective/mono |
46.0 |
60.0 |
9.3 |
96 |
40.6/59.4 |
7.7/24.6 |
0/100 |
Maruoka D/2012 [51] |
Japan |
retrospective/mono |
50.4 ± 12.1 |
52.1 |
9.9 |
577 |
38.3/61.7 |
2.3/22.5 |
81.8/18.2 |
Moon C/2015 [52] |
Korea |
retrospective/mono |
50.9 ± 11.5 |
47.7 |
4.66 |
463 |
64.8/35.2 |
1.0/5.5 |
82.2/17.8 |
Morgan TR/2010 [53] |
USA |
prospective/mono |
49.8 ± 8.2 |
72.1 |
7.1 |
526 |
26.6/73.4 |
1.43/8.5 |
64.8/35.2 |
Ogawa E/2013 [54] |
Japan |
prospective/mono |
63.66 |
49.0 |
3.65 |
1013 |
55.0/45.0 |
2.3/7.5 |
85.2/14.8 |
Osaki Y/2012 [55] |
Japan |
retrospective/mono |
49.5 |
50.3 |
4.24 |
382 |
48.4/51.6 |
0.5/11.2 |
NR |
Rutter K/2015 [56] |
Austria |
retrospective/mono |
51.4 ± 12 |
61.3 |
11.05 |
714 |
77.2/22.8 |
1.80/11.7 |
61.2/38.8 |
Shiratori Y/2005 [57] |
Japan |
prospective/mono |
55.5 |
37.6 |
6.8 |
271 |
23.6/76.4 |
17.2/35.3 |
0/100 |
Tanaka H/2000 [58] |
Japan |
retrospective/mono |
5.17 ± 10.4 |
69.0 |
4.76 |
594 |
29.5/70.5 |
1.7/7.2 |
56.6/2.9* |
van der Meer AJP/2012 [11] |
EU and Canada |
retrospective/mono |
49.0 |
70.0 |
8.9 |
530 |
23.6/76.4 |
5.6/18.8 |
0/100 |
Velosa J/2011 [59] |
EU |
retrospective/mono |
51.7 ± 10.2 |
71.0 |
6.4 |
130 |
30.0/70.0 |
2.6/21.97 |
0/100 |
Wang CH/2013 [60] |
Taiwan |
retrospective/mono |
56.4 ± 9.5 |
54.3 |
8.0 |
138 |
80.4/19.6 |
13.5/22.2 |
NR |
Yoshida H/2004 [61] |
Japan |
retrospective/mono |
49.1 |
63.8 |
7.1 |
2392 |
35.0/65.0 |
3.2/13.8 |
67.6/32.4 |
Yu ML/2005 [20] |
Taiwan |
prospective/mono |
45.9 |
51.5 |
5.7 |
200 |
32.0/68,0 |
1.6/8/8 |
65/35 |
Yu ML/2006 [19] |
Taiwan |
retrospective-prospective/mono |
46.9 ± 11.49 |
60.5 |
5.2 |
1057 |
67.6/32.4 |
1.7/11.4 |
84.4/15.6 |
Total |
22,858 |
48.2/51.8 |
3.2/12.4 |
*Fibrosis score was not recorded in a substantial proportion of patients.
**Recorded as <60 (46.41–47.04%), 60–69 (34.11–36.52%), and ≥70 (17.07–18.85%).
NR = not recorded; mon, mono-infect.
In all, but one study, anti-viral therapy was IFN or peg-INF with or without monotherapy. One study included patients on DAAs, Boceprevir and Telaprevir triple-based therapy regimen. Sample sizes for the patients ranged from 75–1879 patients with a total sample size number of 22,858 patients. Median age of the study participants ranged from 41–63 years and 38–70% were males. Table 2 also lists the key characteristics for the main outcome of HCC incidence in SVR and non-SVR groups as well as the meta-regression covariates (fibrosis stage, year of publication, and follow-up). There was almost an even split for the SVR and non-SVR groups (48.2% vs 51.8%). The HCC incidence rates were 3.2% and 12.4% for the SVR and non-SVR groups.
Statistical results
From the 37 studies, pooled data on the incidence in HCC among patients taking antiviral therapy who achieved SVR compared to those who did not achieve SVR showed a RR of 0.214 (95% CI: 0.168–0.273; p = 0.001) in favour of the SVR group (Figure 2). The statistical analysis showed moderate heterogeneity (X2 = 80.929, 37 df; p = 0.001), with the percent of heterogeneity in the system, I2 = 54.281 and the between study variance, Tau2= 0.250 (SE 0.131; variance 0.017; Tau 0.500).
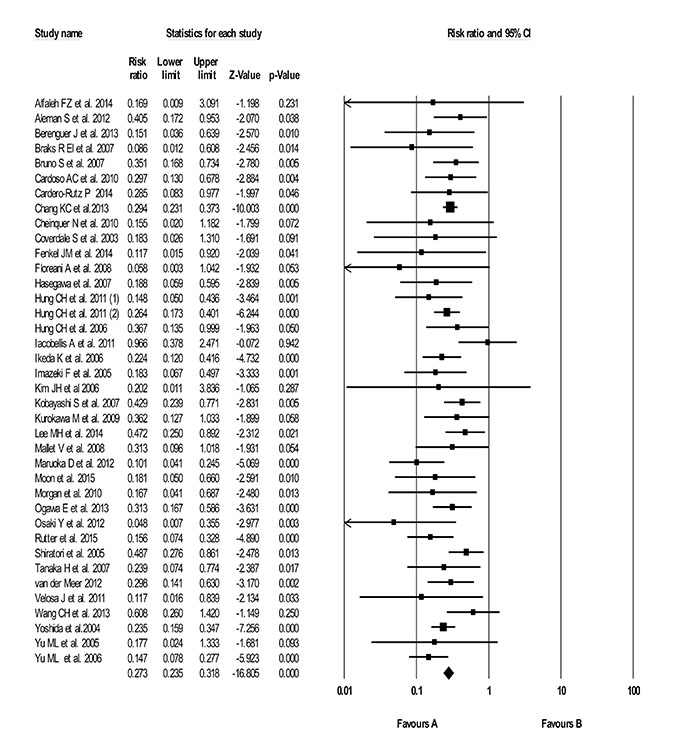
Figure 2: Forest plot for HCC incidence in hepatitis C patients who received antiviral therapy (FN/Peg-IFN ± Ribivirn/Boceprevir or Telaprevir triple therapy) and achieved a sustained virologic response (SVR) compared to those that did not achieve an SVR (non-SVR).
While the data from the random effects analysis did not point to major differences in effect size or a different direction in effect size, there were a few covariates that we wanted to assess through meta-regression to determine if they may have contributed to some of the heterogeneity. The decision to perform meta-regression analysis was based on the review of the raw data in which there was a large variation range of the covariates. The first variable was bridging fibrosis/cirrhosis (F3:F4). In the case of fibrosis staging, most of the older antiviral treatment regimens (i.e. INF-based) tended to have patients who achieved SVR at an earlier stage of disease (i.e. fibrosis stage F0-F2) so this was important to account for. Meta-regression analysis found the variable “bridging fibrosis/cirrhosis” to be significantly associated to the RR (p-value < 0.0001). After adjusting for bridging fibrosis/cirrhosis, the adjusted RR was 0.245. A table of adjusted RRs is shown in Table 3 to illustrate the impact on each study estimate.
Table 3: Meta-regression of adjusted risk ratio’s (RR) on the impact of bridging fibrosis/cirrhosis (F3:F4)
Study |
Adjusted risk ratio |
95% Confidence interval lower bound |
95% Confidence interval upper bound |
|---|---|---|---|
Alfaleh FZ et al. 2014 |
0.204 |
0.200 |
0.210 |
Aleman S et al. 2012 |
0.284 |
0.273 |
0.292 |
Berenguer J et al. 2013 |
0.232 |
0.228 |
0.235 |
Braks R El et al. 2007 |
0.284 |
0.273 |
0.292 |
Bruno S et al. 2007 |
0.284 |
0.273 |
0.292 |
Cardoso AC et al. 2010 |
0.284 |
0.273 |
0.292 |
Cordero-Rutz P et al. 2014 |
0.212 |
0.208 |
0.217 |
Chang KC et al.2013 |
0.237 |
0.232 |
0.239 |
Cheinquer N et al. 2010 |
0.284 |
0.273 |
0.292 |
Fenkel JM et al. 2014 |
0.235 |
0.232 |
0.239 |
Floreani A et al. 2008 |
0.221 |
0.217 |
0.223 |
Hasegawa et al. 2007 |
0.284 |
0.273 |
0.292 |
Hung CH et al. 2011 |
0.225 |
0.223 |
0.230 |
Hung CH et al. 2006 |
0.284 |
0.273 |
0.292 |
Iacobellis A et al. 2011 |
0.284 |
0.273 |
0.292 |
Ikeda K et al. 2006 |
0.230 |
0.228 |
0.235 |
Imazeki F et al. 2005 |
0.223 |
0.219 |
0.225 |
Kurokawa M et al. 2009 |
0.237 |
0.232 |
0.239 |
Lee MH et al. 2014 |
0.212 |
0.208 |
0.217 |
Mallet V et al. 2008 |
0.284 |
0.273 |
0.292 |
Maruoka D et al. 2012 |
0.217 |
0.212 |
0.219 |
Moon et al. 2015 |
0.214 |
0.212 |
0.219 |
Morgan et al. 2010 |
0.228 |
0.225 |
0.232 |
Ogawa E et al. 2013 |
0.212 |
0.210 |
0.217 |
Rutter et al. 2015 |
0.230 |
0.228 |
0.235 |
Shiratori et al. 2005 |
0.284 |
0.273 |
0.292 |
Two other covariates of interest included the year of publication, and length of follow-up in the study. The results of the meta-regression analysis showed that although there is large variability between the studies for effect size, none of the two covariates tested were significantly associated with the effect size. Table 4 lists the meta-regression analysis of the two other covariates. Mean follow-up time showed no significant association on the magnitude of the effect (coefficient = −0.0725, SE = 0.436, p = 0.096) as well as year of publication (coefficient = −0.0301, SE = 0.0478, p = 0.5284).
Table 4: Meta-regression of variables that could explain heterogeneity
Covariate |
Coefficient |
Standard error |
85% lower |
85% upper |
z-value |
2-sided p-value |
|---|---|---|---|---|---|---|
Intercept |
−1.0562 |
0.3386 |
−1.7198 |
−0.3926 |
−3.12 |
0.0018 |
Mean Follow-up |
−0.0725 |
0.0436 |
−0.1579 |
0.0129 |
−1.66 |
0.096 |
Intercept |
58.9456 |
95.9971 |
−129.2053 |
247.0964 |
0.61 |
0.5392 |
Study Year |
−0.0301 |
0.0478 |
−0.1237 |
0.0635 |
−0.63 |
0.5284 |
Test of the model (Follow-up): Simultaneous test that all coefficients (excluding intercept) are zero.
Q = 2.77, df = 1, p = 0.0960.
Goodness of fit: Test that unexplained variance is zero.
Tau² = 0.1721, Tau = 0.4149, I² = 38.94%, Q = 45.86, df = 28, p = 0.0180.
Comparison of model 2 with the null model.
Total between-study variance (intercept only).
Tau² = 0.3296, Tau = 0.5741, I² = 58.86%, Q = 70.49, df = 29, p = 0.0000.
Proportion of total between-study variance explained by model 2.
R² analog = 0.48.
Test of the model: Simultaneous test that all coefficients (excluding intercept) are zero.
Q = 0.40, df = 1, p = 0.5284.
Goodness of fit: Test that unexplained variance is zero.
Tau² = 0.2986, Tau = 0.5464, I² = 54.07%, Q = 60.97, df = 28, p = 0.0003.
Comparison of model 3 with the null model.
Total between-study variance (intercept only).
Tau² = 0.3296, Tau = 0.5741, I² = 58.86%, Q = 70.49, df = 29, p = 0.0000.
Proportion of total between-study variance explained by model 3.
R² analog = 0.09.
DISCUSSION
To the best of our knowledge, this systematic review and meta-analysis is the largest to date with more than 1000 articles were screened and 37 studies were included in the final analysis. We included papers that studied CHC patients treated with any type of antiviral therapy (IFN, peg-IFN with or without ribavirin and DAA’s), all fibrosis stages and both mono and co-infect patients. The random effects model on RR showed 78.6% reduction in risk of the incidence of HCC for patients who achieved SVR compared to those who did not achieve SVR whether they were treated treatment naïve or experienced. Based on previous publications on HCC and antiviral therapy, we expected that the SVR group would show a significant reduction in the risk of HCC, but the question was at what magnitude. Meta-regression analysis was performed to determine whether bridging fibrosis/cirrhosis (F3-F4) had any effect on the RR. This variable was significantly associated with RR with a reduction in risk of HCC in SVR patients of 75.5%. It was thought that two other covariates (publication year, and follow-up time in study) might have helped to explain some of the heterogeneity and variability between studies, however neither of these covariates showed a significant association and thus the variation cannot be explained by the tested covariates.
It has been documented that HCC incidence increases in later stage of disease as the virus persists [2, 4, 6]. In addition, response rates with antiviral therapies in those patients with cirrhosis tend to be lower than those patients at an earlier stage of disease. Our analysis includes twelve studies in which the patient population were bridging fibrosis/cirrhosis and response rates ranged from 14% (HIV co-infect study) to 55.3% in the SVR group compared to 44.7–76.4% in the non-SVR group showing overlap of SVR in the two groups, but a tendency towards lower response rates in the SVR group. This could explain some of the heterogeneity in the pooled data. Meta-regression analysis adjusting for later stage fibrosis F3-F4 did show statistical significance on the RR.
Results of any long-term follow-up studies with the new generation of all oral DAA’s (NS3/4A protease inhibitors, NS5A polymerase inhibitors and NS5B nuc and non-nuc polymerase inhibitors) which show very high sustained virologic response rates (over 90%) are just starting to be available, but little is still known about the effects of these new therapies on the development of HCC. Previous studies analyzing the HCC development and recurrence with all oral DAA’s have been published [19–22]. While one study directly compares HCC incidence in patients who received IFN-based therapy to those who received IFN-free therapy, there are apparent differences in baseline characteristics between the two groups, whereby those in the IFN-free group were older have a higher percent of cirrhosis which could account for the higher estimated annual incidence (0.28% in IFN based arm vs 0.62% in IFN free arm) (56). High rates of HCC are noted to include those with a history of previous HCC and other risk factors included more advanced liver disease and platelet count [22–25]. In the future, these long-term studies with the new oral antiviral agents will be of high importance, hopefully further uncovering which patients may not need long term continuance of HCC surveillance.
Some of the limitations of this analysis include the fact that none of the studies were RCT’s, they were mostly retrospective, but prospective cohorts were also included. Four conference abstracts, including one with first generation DAA’s (Boceprevir/Telaprevir) lacked some baseline characteristics (e.g. age and gender), however given the variation in the studies, this information most likely would not have changed the results. Quality assessment for risk of bias (Newcastle Ottawa Scale) was not different for the conference abstracts (range of 5–7 stars). In addition, baseline laboratory and other clinical parameters (diabetes, alcohol intake, methadone use, weight and body mass index) were reported in a variety of ways and only some of the studies, thus were not included as a covariate in the analysis. There were only three co-infect studies (two HIV and one HBV) therefore sub-group analysis was not performed on this somewhat different patient population. HIV co-infect patients are known to have higher HCV RNA levels and more rapid progression of hepatic fibrosis along with differing social and medical characteristics (e.g. drug and alcohol use, psychiatric disease) than mono infect patients, there were no red flags seen in terms of major baseline characteristics [21]. SVR rates were not significantly different than the mono-infect studies, however one study did report one of the lower SVR rates (14%) also similarly reported in one mono infect study [26, 27]. Finally, the information from this systematic analysis may help to better inform which patients would benefit from HCC screening program. The American Association for the Study of Liver (AASLD) practice guidance on the management of HCC notes that surveillance is cost effective if the expected risk of HCC exceeds 1.5% per year in patients with CHC [15]. If enough patients are screened, referred and treated for CHC, the effects of decreasing the incidence of HCC could be profound [4, 16].
CONCLUSIONS
In conclusion, CHC patients who receive anti-viral therapy and achieve SVR show a highly protective effect against the incidence of HCC with a reduction in risk of 78.6%. When adjusting for the variable bridging fibrosis/cirrhosis the reduction of risk is 75.5%.
MATERIALS AND METHODS
Search strategy
An electronic database literature search was performed by an experienced librarian (EU) in Medline, EMBASE and CCTR to July 2015. To capture any other studies that may be missed, a Google Scholar search for the top 200 hits was also be performed as well as consultation with a medical expert in the area of CHC treatment. In addition, published systematic and meta-analyses studies were reviewed for cross-reference of publications. The used search terms included CHC, hepatocellular carcinoma, all of the antiviral regimens first and second generation (e.g. IFN based regimens, first generation DAA’s and second generation DAA’s), and SVR.
Study selection and data abstraction
In order to analyze the effect of achieving SVR versus not achieving SVR with antiviral therapy on HCC risk in CHC patients, the following criteria was used to determine included publications:
Type of studies
Studies abstracted for review included those that were prospective or retrospective (randomized or single-arm studies). We reviewed studies not limited to English language (however no non-English publications were found that met all inclusion criteria). Conference abstracts that were presented within the last 2 years (i.e. 2013–2015) were included. Any publications that were reviews, comments, editorials or conference abstracts older than 2013 were excluded from this review.
Studies participants and intervention
Adults (>18 years old), diagnosed with CHC, with all fibrosis scores (F0-F4) (i.e. non-cirrhotic and cirrhotic), HIV or hepatitis B (HBV) co-infect patients were included. In terms of antiviral therapy, patients could be treatment naïve and experienced (those being retreated after not obtaining SVR) with any type of CHC antiviral therapy (e.g. IFN-based, DAA’s). Follow-up of patients had to be at least a mean or median of 1 year after study enrollment. Patients with HCC recurrence or have been transplanted were excluded.
Studies outcome
All studies included must have HCC incidence rates (number of cases) recorded in two groups of patients receiving antiviral therapy, 1) those that have obtained SVR, and 2) those that did not achieve SVR within the defined follow-up period in the study.
Method of review
The main author (AN) along with two independent reviewers (AH and TH) reviewed the electronic database and other means of abstraction (i.e. Google scholar, systematic/meta-analysis, expert opinion to assess the studies that were included in the analysis using in inclusion and exclusion criteria checklist. Any conflict between the reviewers was resolved by consensus.
Studies quality assessment
Study quality to assess the validity and risk of bias was evaluated using the Newcastle-Ottawa scale (NOS) cohort studies checklist [28]. The NOS uses a star system in which studies are judged in three broad categories, the selection of study groups (i.e. CHC patient receiving anti-viral therapy in which HCC incidence is measured), the comparability of the groups (SVR and non-SVR) and the ascertainment of the outcome. The main author (AN) and the two independent reviewers (AH and TH) assessed each included study for risk of bias using the NOS rating scale. The reviewers resolved any conflict of the ratings by consensus.
Data abstraction
Study data abstraction and collection was performed by entering all information on a data spreadsheet (Excel). The main author (AN) entered the data onto the spreadsheet and the two reviewers (AH and TH) reviewed all content for accuracy. The key data entered included the number of patients treated with antiviral therapy (sample size), the number achieving SVR, the number that did not achieve SVR (non-SVR), and incidence of HCC for each of the two groups being compared, SVR and non-SVR. Additional information that was abstracted and entered into the spreadsheet included author name/year, country, type of study (RCT, prospective, retrospective), whether the study included mono, HIV or HBV co-infect patients, type of antivirals, duration of follow-up, mean or median age, gender, ethnicity, fibrosis stage separated by two groups: F0-F2 and F3-F4, genotype, laboratory values (platelets and alpha fetoprotein), presence of other co-morbidities and weight or body mass index (BMI), whichever was recorded. Whenever possible, data was separated for SVR and non-SVR groups, however the studies were not excluded unless the main endpoint of measurement for the analysis, HCC incidence rates was not reported separately for the two groups.
Statistical analysis
Data was entered into the software Comprehensive Meta-analysis (Biostat, Englewood, NJ) and SAS Version 9.3 (SAS Institute, Cary, NC, USA). Main statistical analysis included the incidence of HCC in the SVR vs non-SVR groups. The risk ratio (RR) using a random effects model on the difference between the two groups (SVR vs non-SVR) in HCC incidence with 95% confidence intervals (CI’s) was analyzed. The random effects model was chosen to ensure the variances in effect size between the studies were accounted for. A Meta-regression was carried out to assess the potential impact of the variable bridging fibrosis/cirrhosis (F3-F4) on the RRs for the studies under examination. Meta-regression was also performed to determine if additional factors showed a large increase or decrease in effect size for two covariates, year of publication, and length of follow-up in the study. To assess the variation of the treatment effect than what would be expected by chance across studies the Cochran’s Chi-squared test (X2) was used (with significance level of p < 0.10). An estimate between study variance was assessed through Tau squared (Tau2). In order to measure the extent of inconsistency, the proportion of total variation in study estimates that is due to heterogeneity rather than sampling error (chance) the I2 statistic was used [29].
Author contributions
Conception and design: Arlene Nugent. Development of methodology: All authors. Acquisition of data: Arlene Nugent, Ali Hosni and Tawnya Hansen. Analysis and interpretation of data: All authors. Writing, review and/or revision of the manuscript: All authors. Final approval of the version to be published: All authors. Agreement to be accountable for all aspects of the work: All authors.
CONFLICTS OF INTEREST
No conflicts of interest
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J Carcinog. 2017; 16:1. https://doi.org/10.4103/jcar.JCar_9_16.
2. Myers RP, Krajden M, Bilodeau M, Kaita K, Marotta P, Peltekian K, Ramji A, Estes C, Razavi H, Sherman M. Burden of disease and cost of chronic hepatitis C infection in Canada. Can J Gastroenterol Hepatol. 2014; 28:243–50.
3. Gomaa AI, Khan SA, Toledano MB, Waked I, Taylor-Robinson SD. Hepatocellular carcinoma: epidemiology, risk factors and pathogenesis. World J Gastroenterol. 2008; 14:4300–8.
4. Venook AP, Papandreou C, Furuse J, de Guevara LL. The incidence and epidemiology of hepatocellular carcinoma: a global and regional perspective. Oncologist. 2010; 4:5–13. https://doi.org/10.1634/theoncologist.2010-S4-05.
5. Hajarizadeh B, Grebely J, Dore GJ. Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol. 2013; 10:553–62. https://doi.org/10.1038/nrgastro.2013.107.
6. Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology. 2004; 127:S35–50.
7. El-Serag HB, Kanwal F. Epidemiology of hepatocellular carcinoma in the United States: where are we? Where do we go? Hepatology. 2014; 60:1767–75. https://doi.org/10.1002/hep.27222.
8. El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012; 142:1264–73.e1. https://doi.org/10.1053/j.gastro.2011.12.061.
9. European Association for Study of L. EASL Recommendations on Treatment of Hepatitis C 2015. J Hepatol. 2015; 63:199–236. https://doi.org/10.1016/j.jhep.2015.03.025.
10. Myers RP, Shah H, Burak KW, Cooper C, Feld JJ. An update on the management of chronic hepatitis C: 2015 Consensus guidelines from the Canadian Association for the Study of the Liver. Can J Gastroenterol Hepatol. 2015; 29:19–34.
11. van der Meer AJ, Veldt BJ, Feld JJ, Wedemeyer H, Dufour JF, Lammert F, Duarte-Rojo A, Heathcote EJ, Manns MP, Kuske L, Zeuzem S, Hofmann WP, de Knegt RJ, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012; 308:2584–93. https://doi.org/10.1001/jama.2012.144878.
12. Qu LS, Chen H, Kuai XL, Xu ZF, Jin F, Zhou GX. Effects of interferon therapy on development of hepatocellular carcinoma in patients with hepatitis C-related cirrhosis: A meta-analysis of randomized controlled trials. Hepatol Res. 2012; 42:782–9. https://doi.org/10.1111/j.1872-034X.2012.00984.x.
13. Singal AK, Singh A, Jaganmohan S, Guturu P, Mummadi R, Kuo YF, Sood GK. Antiviral therapy reduces risk of hepatocellular carcinoma in patients with hepatitis C virus-related cirrhosis. Clin Gastroenterol Hepatol. 2010; 8:192–9. https://doi.org/10.1016/j.cgh.2009.10.026.
14. Ng V, Saab S. Effects of a sustained virologic response on outcomes of patients with chronic hepatitis C. Clin Gastroenterol Hepatol. 2011; 9:923–30. https://doi.org/10.1016/j.cgh.2011.05.028.
15. Bruix J, Sherman M, American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology. 2011; 53:1020–2. https://doi.org/10.1002/hep.24199.
16. Veldt BJ, Heathcote EJ, Wedemeyer H, Reichen J, Hofmann WP, Zeuzem S, Manns MP, Hansen BE, Schalm SW, Janssen HL. Sustained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med. 2007; 147:677–84.
17. Arase Y, Ikeda K, Suzuki F, Suzuki Y, Saitoh S, Kobayashi M, Akuta N, Someya T, Koyama R, Hosaka T, Sezaki H, Kobayashi M, Kumada H. Long-term outcome after interferon therapy in elderly patients with chronic hepatitis C. Intervirology. 2007; 50:16–23. https://doi.org/10.1159/000096308.
18. Berenguer J, Zamora FX, Carrero A, Von Wichmann MA, Crespo M, Lopez-Aldeguer J, Aldamiz-Echevarria T, Montes M, Quereda C, Tellez MJ, Galindo MJ, Sanz J, Santos I, et al. Effects of sustained viral response in patients with HIV and chronic hepatitis C and nonadvanced liver fibrosis. J Acquir Immune Defic Syndr. 2014; 66:280–7. https://doi.org/10.1097/QAI.0000000000000156.
19. Yu ML, Lin SM, Chuang WL, Dai CY, Wang JH, Lu SN, Sheen IS, Chang WY, Lee CM, Liaw YF. A sustained virological response to interferon or interferon/ribavirin reduces hepatocellular carcinoma and improves survival in chronic hepatitis C: a nationwide, multicentre study in Taiwan. Antivir Ther. 2006; 11:985–94.
20. Yu ML, Dai CY, Chen SC, Lee LP, Hsieh MY, Lin ZY, Hsieh MY, Wang LY, Tsai JF, Chang WY, Chuang WL. High versus standard doses interferon-alpha in the treatment of naive chronic hepatitis C patients in Taiwan: a 10-year cohort study. BMC Infect Dis. 2005; 5:27. https://doi.org/10.1186/1471-2334-5-27.
21. Sulkowski MS, Benhamou Y. Therapeutic issues in HIV/HCV-coinfected patients. J Viral Hepat. 2007; 14:371–86. https://doi.org/10.1111/j.1365-2893.2006.00816.x.
22. Toyoda H, Kumada T, Tada T. Changes in patient backgrounds may increase the incidence of HCC after SVR in the era of IFN-free therapy for HCV. Hepatology. 2016; 64:1818–9. https://doi.org/10.1002/hep.28632.
23. Buonfiglioli F, Conti F, Andreone P, Crespi C, Foschi FG, Lenzi M, Mazzella G, Verucchi G, Brillanti S. Development of Hepatocellular Carcinoma in HCV Cirrhotic Patients Treated with Direct Acting Antivirals. Journal of Hepatology. 2016; 64:S215. https://doi.org/10.1016/S0168-8278(16)00183-5.
24. Kozbial K, Stern R, Freissmuth C, Beinhardt S, Stättermayer AF, Munda P, Trauner M, Ferenci P, Hofer H; Viral Hepatitis. High Risk for Hepatocellular Carcinoma in Cirrhotic Patients with SVR following IFN-Free Daa Treatment within 1 Year Follow-Up. Journal of Hepatology. 2016; 64:S617–8. https://doi.org/10.1016/S0168-8278(16)01146-6.
25. Reig M, Marino Z, Perello C, Inarrairaegui M, Ribeiro A, Lens S, Diaz A, Vilana R, Darnell A, Varela M, Sangro B, Calleja JL, Forns X, et al. Unexpected high rate of early tumor recurrence in patients with HCV-related HCC undergoing interferon-free therapy. J Hepatol. 2016; 65:719–26. https://doi.org/10.1016/j.jhep.2016.04.008.
26. Bruno S, Stroffolini T, Colombo M, Bollani S, Benvegnu L, Mazzella G, Ascione A, Santantonio T, Piccinino F, Andreone P, Mangia A, Gaeta GB, Persico M, et al. Sustained virological response to interferon-alpha is associated with improved outcome in HCV-related cirrhosis: a retrospective study. Hepatology. 2007; 45:579–87. https://doi.org/10.1002/hep.21492.
27. Chang KC, Wu YY, Hung CH, Lu SN, Lee CM, Chiu KW, Tsai MC, Tseng PL, Huang CM, Cho CL, Chen HH, Hu TH. Clinical-guide risk prediction of hepatocellular carcinoma development in chronic hepatitis C patients after interferon-based therapy. Br J Cancer. 2013; 109:2481–8. https://doi.org/10.1038/bjc.2013.564.
28. Wells GA SB, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analysis. Available from URL: http://wwwohrica/programs/clinical_epidemiology/oxfordasp. Accessed May 2015.
29. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557–60. https://doi.org/10.1136/bmj.327.7414.557.
30. Alfaleh FZ, Alswat K, Helmy A, Al-hamoudi W, El-sharkawy M, Omar M, Shalaby A, Bedewi MA, Hadad Q, Ali SM, Alfaleh A, Abdo AA. The natural history and long-term outcomes in patients with chronic hepatitis C genotype 4 after interferon-based therapy. Liver Int. 2013; 33:871–83. https://doi.org/10.1111/liv.12127.
31. Aleman S, Rahbin N, Weiland O, Davidsdottir L, Hedenstierna M, Rose N, Verbaan H, Stal P, Carlsson T, Norrgren H, Ekbom A, Granath F, Hultcrantz R. A risk for hepatocellular carcinoma persists long-term after sustained virologic response in patients with hepatitis C-associated liver cirrhosis. Clin Infect Dis. 2013; 57:230–6. https://doi.org/10.1093/cid/cit234.
32. Berenguer J, Alvarez-Pellicer J, Carrero A, Von Wichmann MA, Lopez-Aldeguer J, Mallolas J, Galindo MJ, Van Den Eynde E, Tellez MJ, Quereda C, Tural C, Sanz J, Barros C, et al. Clinical effects of viral relapse after interferon plus ribavirin in patients co-infected with human immunodeficiency virus and hepatitis C virus. J Hepatol. 2013; 58:1104–12. https://doi.org/10.1016/j.jhep.2013.01.042.
33. Braks RE, Ganne-Carrie N, Fontaine H, Paries J, Grando-Lemaire V, Beaugrand M, Pol S, Trinchet JC. Effect of sustained virological response on long-term clinical outcome in 113 patients with compensated hepatitis C-related cirrhosis treated by interferon alpha and ribavirin. World J Gastroenterol. 2007; 13:5648–53.
34. Cardoso AC, Moucari R, Figueiredo-Mendes C, Ripault MP, Giuily N, Castelnau C, Boyer N, Asselah T, Martinot-Peignoux M, Maylin S, Carvalho-Filho RJ, Valla D, Bedossa P, et al. Impact of peginterferon and ribavirin therapy on hepatocellular carcinoma: incidence and survival in hepatitis C patients with advanced fibrosis. J Hepatol. 2010; 52:652–7. https://doi.org/10.1016/j.jhep.2009.12.028.
35. Cordero-Ruiz P, Carmona-Soria I, Caunedo-Alvarez A, Herrerias JM, Vilches-Arenas A. Long-Term Impact of Antiviral Therapy in the Natural History of Chronic Hepatitis C. Gastroenterology. 2014; 146:S–256. https://doi.org/10.1016/S0016-5085(14)60902-1.
36. Cheinquer N, Cheinquer H, Wolff FH, Coelho-Borges S. Effect of sustained virologic response on the incidence of hepatocellular carcinoma in patients with HCV cirrhosis. Braz J Infect Dis. 2010; 14:457–61.
37. Coverdale SA, Khan MH, Byth K, Lin R, Weltman M, George J, Samarasinghe D, Liddle C, Kench JG, Crewe E, Farrell GC. Effects of interferon treatment response on liver complications of chronic hepatitis C:9–year follow-up study. Am J Gastroenterol. 2004; 99:636–44. https://doi.org/10.1111/j.1572-0241.2004.04085.x.
38. Fenkel JFG, Chan D, De Marzio D, Sass D, Herrine S, Civan J. First generation protease inhibitor-based triple therapy and risk of hepatocellular carcinoma. Hepatology. 2014; 60:847A.
39. Floreani A, Baldo V, Rizzotto ER, Carderi I, Baldovin T, Minola E. Pegylated interferon alpha-2b plus ribavirin for naive patients with HCV-related cirrhosis. J Clin Gastroenterol. 2008; 42:734–7. https://doi.org/10.1097/MCG.0b013e318046ea75.
40. Hasegawa E, Kobayashi M, Kawamura Y, Yatsuji H, Sezaki H, Hosaka T, Akuta N, Suzuki F, Suzuki Y, Arase Y, Ikeda K, Kumada H. Efficacy and anticarcinogenic activity of interferon for hepatitis C virus-related compensated cirrhosis in patients with genotype 1b low viral load or genotype 2. Hepatol Res. 2007; 37:793–800. https://doi.org/10.1111/j.1872-034X.2007.00140.x.
41. Hung CH, Lu SN, Wang JH, Hu TH, Chen CH, Huang CM, Lee CM. Sustained HCV clearance by interferon-based therapy reduces hepatocellular carcinoma in hepatitis B and C dually-infected patients. Antivir Ther. 2011; 16:959–68. https://doi.org/10.3851/IMP1842.
42. Hung CH, Lee CM, Lu SN, Wang JH, Hu TH, Tung HD, Chen CH, Chen WJ, Changchien CS. Long-term effect of interferon alpha-2b plus ribavirin therapy on incidence of hepatocellular carcinoma in patients with hepatitis C virus-related cirrhosis. J Viral Hepat. 2006; 13:409–14. https://doi.org/10.1111/j.1365-2893.2005.00707.x.
43. Iacobellis A, Perri F, Valvano MR, Caruso N, Niro GA, Andriulli A. Long-term outcome after antiviral therapy of patients with hepatitis C virus infection and decompensated cirrhosis. Clin Gastroenterol Hepatol. 2011; 9:249–53. https://doi.org/10.1016/j.cgh.2010.10.036.
44. Ikeda K, Arase Y, Saitoh S, Kobayashi M, Someya T, Hosaka T, Sezaki H, Akuta N, Suzuki F, Suzuki Y, Kumada H. Anticarcinogenic impact of interferon on patients with chronic hepatitis C: a large-scale long-term study in a single center. Intervirology. 2006; 49:82–90. https://doi.org/10.1159/000087268.
45. Imazeki F, Yokosuka O, Fukai K, Kawai S, Kanda T, Kojima H, Saisho H. Lower incidence of hepatic failure than hepatocellular carcinoma in Japanese patients with chronic hepatitis C. Liver Int. 2005; 25:772–8. https://doi.org/10.1111/j.1478-3231.2005.01062.x.
46. Kim JH, Han KH, Lee KS, Park YN, Ahn SH, Chon CY, Moon YM. Efficacy and long-term follow up of combination therapy with interferon alpha and ribavirin for chronic hepatitis C in Korea. Yonsei Med J. 2006; 47:793–8. https://doi.org/10.3349/ymj.2006.47.6.793.
47. Kobayashi S, Takeda T, Enomoto M, Tamori A, Kawada N, Habu D, Sakaguchi H, Kuroda T, Kioka K, Kim SR, Kanno T, Ueda T, Hirano M, et al. Development of hepatocellular carcinoma in patients with chronic hepatitis C who had a sustained virological response to interferon therapy: a multicenter, retrospective cohort study of 1124 patients. Liver Int. 2007; 27:186–91. https://doi.org/10.1111/j.1478-3231.2006.01406.x.
48. Kurokawa M, Hiramatsu N, Oze T, Mochizuki K, Yakushijin T, Kurashige N, Inoue Y, Igura T, Imanaka K, Yamada A, Oshita M, Hagiwara H, Mita E, et al. Effect of interferon alpha-2b plus ribavirin therapy on incidence of hepatocellular carcinoma in patients with chronic hepatitis. Hepatol Res. 2009; 39:432–8. https://doi.org/10.1111/j.1872-034X.2008.00477.x.
49. Lee MYY, Yu M, Chuang W, Kao J, Liu C, Lu S, Sheen I, L’Italien G, Yang H, Chen C. Significant Reduction of Hepatocellular Carcinoma Risk in Chronic Hepatitis C Patients with Peg-interferon plus Ribavirin Therapy: A Five-year Clinical Cohort Study. Hepatology. 2014; 60:659A.
50. Mallet V, Gilgenkrantz H, Serpaggi J, Verkarre V, Vallet-Pichard A, Fontaine H, Pol S. Brief communication: the relationship of regression of cirrhosis to outcome in chronic hepatitis C. Ann Intern Med. 2008; 149:399–403.
51. Maruoka D, Imazeki F, Arai M, Kanda T, Fujiwara K, Yokosuka O. Long-term cohort study of chronic hepatitis C according to interferon efficacy. J Gastroenterol Hepatol. 2012; 27:291–9. https://doi.org/10.1111/j.1440-1746.2011.06871.x.
52. Moon C, Jung KS, Kim DY, Baatarkhuu O, Park JY, Kim BK, Kim SU, Ahn SH, Han KH. Lower incidence of hepatocellular carcinoma and cirrhosis in hepatitis C patients with sustained virological response by pegylated interferon and ribavirin. Dig Dis Sci. 2015; 60:573–81. https://doi.org/10.1007/s10620-014-3361-6.
53. Morgan TR, Ghany MG, Kim HY, Snow KK, Shiffman ML, De Santo JL, Lee WM, Di Bisceglie AM, Bonkovsky HL, Dienstag JL, Morishima C, Lindsay KL, Lok AS, et al. Outcome of sustained virological responders with histologically advanced chronic hepatitis C. Hepatology. 2010; 52:833–44. https://doi.org/10.1002/hep.23744.
54. Ogawa E, Furusyo N, Kajiwara E, Takahashi K, Nomura H, Maruyama T, Tanabe Y, Satoh T, Nakamuta M, Kotoh K, Azuma K, Dohmen K, Shimoda S, et al. Efficacy of pegylated interferon alpha-2b and ribavirin treatment on the risk of hepatocellular carcinoma in patients with chronic hepatitis C: a prospective, multicenter study. J Hepatol. 2013; 58:495–501. https://doi.org/10.1016/j.jhep.2012.10.017.
55. Osaki Y, Ueda Y, Marusawa H, Nakajima J, Kimura T, Kita R, Nishikawa H, Saito S, Henmi S, Sakamoto A, Eso Y, Chiba T. Decrease in alpha-fetoprotein levels predicts reduced incidence of hepatocellular carcinoma in patients with hepatitis C virus infection receiving interferon therapy: a single center study. J Gastroenterol. 2012; 47:444–51. https://doi.org/10.1007/s00535-011-0505-8.
56. Rutter K, Stattermayer AF, Beinhardt S, Scherzer TM, Steindl-Munda P, Trauner M, Ferenci P, Hofer H. Successful anti-viral treatment improves survival of patients with advanced liver disease due to chronic hepatitis C. Aliment Pharmacol Ther. 2015; 41:521–31. https://doi.org/10.1111/apt.13085.
57. Shiratori Y, Ito Y, Yokosuka O, Imazeki F, Nakata R, Tanaka N, Arakawa Y, Hashimoto E, Hirota K, Yoshida H, Ohashi Y, Omata M, Tokyo-Chiba Hepatitis Research G. Antiviral therapy for cirrhotic hepatitis C: association with reduced hepatocellular carcinoma development and improved survival. Ann Intern Med. 2005; 142:105–14.
58. Tanaka H, Tsukuma H, Kasahara A, Hayashi N, Yoshihara H, Masuzawa M, Kanda T, Kashiwagi T, Inoue A, Kato M, Oshima A, Kinoshita Y, Kamada T. Effect of interferon therapy on the incidence of hepatocellular carcinoma and mortality of patients with chronic hepatitis C: a retrospective cohort study of 738 patients. Int J Cancer. 2000; 87:741–9.
59. Velosa J, Serejo F, Marinho R, Nunes J, Gloria H. Eradication of hepatitis C virus reduces the risk of hepatocellular carcinoma in patients with compensated cirrhosis. Dig Dis Sci. 2011; 56:1853–61. https://doi.org/10.1007/s10620-011-1621-2.
60. Wang CH CK, Lin RC and Kuo JJ. Insights into hepatocellular carcinoma occurrence and long-term outcomes in patients with chronic hepatitis C infection after successful antiviral treatment. Hepatology International. 2013; 7:367.
61. Yoshida H, Tateishi R, Arakawa Y, Sata M, Fujiyama S, Nishiguchi S, Ishibashi H, Yamada G, Yokosuka O, Shiratori Y, Omata M. Benefit of interferon therapy in hepatocellular carcinoma prevention for individual patients with chronic hepatitis C. Gut. 2004; 53:425–30.