
INTRODUCTION
Production of carbapenemases are main mechanism underlying resistance to carbapenems which are first-line agents with proven efficacy for treatment of severe infections caused by multi-drugs resistant bacteria [1]. Carbapenemase-producing Enterobacteriaceae isolates are usually extensively drug resistant, and infections caused by these pathogens with significant morbidity and mortality present a serious clinical challenge, especially for pediatric patients [2]. Because genes mediated carbapenemase usually located in transferable plasmids and it can potentially spread rapidly, infections caused by carbapenemase-producing Enterobacteriaceae may prove difficult to control once they emerge [3]. For this purpose, rapid and reliable identification of carbapenemase producers in the clinical microbiology laboratory is urgently needed to affect infection treatment. Currently, although several commercial tests are available for detection of carbapenem resistance including phenotypic or genotypic tests, none is ideal for all possible carbapenemase genes [4]. In 2017, modified carbapenem inactivation method (mCIM) testing was recommended by Clinical and Laboratory Standard Institute (CLSI) for detection of carbapenemase among Enterobacteriaceae clinical isolates [5]. This method is simple, low-cost to assess phenotypic carbapenemase activity in Enterobacteriaceae and has been demonstrated a sensitivity >99% and specificity >99% for detection of KPC, NDM, VIM, IMP, SPM, SME and OXA-type carbapenemase [1]. In this study, we described a mCIM method with some modification for the identification of carbapenemase-producing Enterobacteriaceae clinical isolates.
MATERIALS AND METHODS
Strains
A panel of 145 clinical strains including 77 blaKPC-2-positive K. pneumoniae, 31 blaNDM-1-positive K. pneumoniae, 4 blaNDM-1-positive E.coli, 5 blaOXA-232-positive K. pneumoniae, and 28 carbapenem-susceptible K. pneumoniae were collected from four hospitals in China for evaluating the mCIM for suspected carbapenemase. All isolates were identified by vitek 2 compact system (BioMerieux, France), and the presence of carbapenemase genes was confirmed by specific PCR and sequence analysis. E. coli ATCC25922 was used as quality control strain in antimicrobial susceptibility testing. E. coli NCTC-13476 (blaIMP positive) and K. pneumoniae NCTC-13440 (blaVIM-1 positive) were also used for positive control for mCIM.
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing were performed by microbroth dilution and minimum inhibitory concentrations (MICs) were interpreted according to CLSI guidelines [5].
mCIM for suspected carbapenemase
mCIM for detection of carbapenemases among 145 Enterobacteriaceae clinical isolates were performed as described by CLSI [5]. The zone of inhibition of meropenem was recorded after incubating time for 6 h, 18 h, and 24 h, respectively.
RESULTS
Antimicrobial susceptibility testing
The results of antimicrobial agents susceptibility for all of 117 carbapenem-resistant Enterobacteriaceae isolates were detailed in Table 1. All strains were resistant to ertapenem with high MIC50 and MIC90 (64 mg/L and >128 mg/L), meropenem with high MIC50 and MIC90 (32 mg/L and 128 mg/L), however, 23.1%–49.6% of them were susceptible to ciprofloxacin, gentamicin and amikacin, respectively.
Table 1: Activities of various antimicrobial agents against 117 carbapenem-resistant Enterobacteriaceae clinical isolates
Antibiotic name |
MIC Range (mg/L) |
MIC50 (mg/L) |
MIC90 (mg/L) |
Resistant (%) |
Susceptible (%) |
|---|---|---|---|---|---|
Cefoperazone/Sulbactam |
4 –>128 |
>128 |
>128 |
94.9 |
4.3 |
Piperacillin/Tazobactam |
4 –>256 |
>256 |
>256 |
96.6 |
2.6 |
Cefazolin |
64 –>128 |
>128 |
>128 |
100 |
0 |
Cefuroxime |
32 –>128 |
>128 |
>128 |
100 |
0 |
Ceftazidime |
1 –>128 |
>128 |
>128 |
97.4 |
2.6 |
Cefotaxime |
1 –>128 |
>128 |
>128 |
97.4 |
1.7 |
Cefepime |
4 –>128 |
128 |
>128 |
96.6 |
0 |
Ertapenem |
1 –>128 |
64 |
>128 |
98.3 |
0 |
Imipenem |
0.5 – 64 |
32 |
32 |
93.2 |
0.9 |
Meropenem |
0.25 –>128 |
32 |
128 |
96.6 |
1.7 |
Amikacin |
0.5 –>128 |
>128 |
>128 |
50.4 |
49.6 |
Gentamicin |
0.25 –>128 |
128 |
>128 |
63.2 |
35 |
Ciprofloxacin |
0.06 –>128 |
32 |
128 |
73.5 |
23.1 |
mCIM for suspected carbapenemase production
Results obtained from mCIM indicated (Figures 1 and 2), for blaNDM-1-positive and blaOXA-232-positive strains, the zone of inhibition of meropenem were all 6 mm despite the incubation time of 6 h, 18 h or 24 h. For 18 h or 24 h, because of presence of colonies within a 16–18 mm meropenem zone for several blaKPC-2 producing K. pneumoniae isolates, mCIM can also differentiate successfully between carbapenemase-positive and carbapenemase-negative Enterobacteriaceae isolates. For 6 h, the zone of meropenem inhibition for all of carbapenemase-positive isolates were meet the positive criteria 6–15 mm. However, for carbapenemase-negative isolates, the zone of meropenem inhibition were 16–18 mm after 6 h incubation which should be considered indeterminate for standard incubating time such as 18 h or 24 h. After incubating for 18 h or 24 h, the zone of meropenem inhibition were 22–25 mm for carbapenemase-negative isolates and meet the negative criteria.
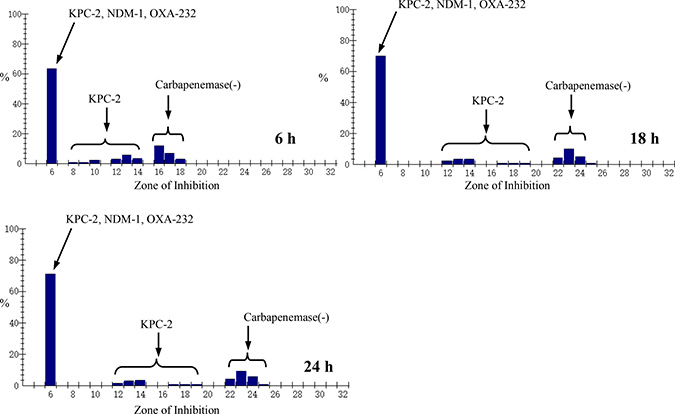
Figure 1: Zone of Inhibition distribution of meropenem for Enterobacteriacae clinical isolates at different incubating time.
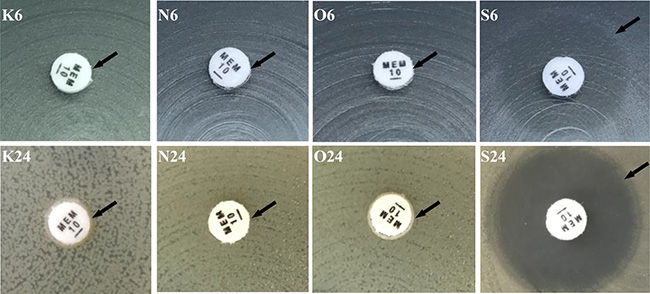
Figure 2: Modified carbapenem inactivation method for suspected carbapenemase production in enterobacteriaceae. 1. K6, blakpc-2 positive K. pneumoniae incubating 6 h (zone 6 mm); K24, blakpc-2 positive K. pneumoniae incubating 24 h (zone 6 mm) (arrow indicated); 2. N6, blaNDM-1 positive K. pneumoniae incubating 6 h (zone 6 mm); N24, blaNDM-1 positive K. pneumoniae incubating 24 h (zone 6 mm) (arrow indicated); 3. O6, blaOXA-232 positive K. pneumoniae incubating 6 h (zone 6 mm); O24, blaOXA-232 positive K. pneumoniae incubating 24 h (zone 6 mm) (arrow indicated); 4. S6, meropenem-susceptible K. pneumoniae incubating 6 h (zone 18 mm); S24, meropenem-susceptible K. pneumoniae incubating 24 h (zone 22 mm) (arrow indicated).
DISCUSSION
In the past 10 years, the world-wide increase in carbapenem-resistant organisms has made it even more important to use these “last line” antibiotics which are the most broad-spectrum agents known and are often life-saving therapies for severe infections [6, 7]. According to CHINET surveillance, the resistance rate of K. pneumoniae isolates to carbapenem was increasing rapidly from 2005 to 2015 [1, 8]. Rapid and effective detection of carbapenemases is important for clinicians treating patients with these infections and for infection preventionists to limit the spread of carbapenem-resistant organisms [9]. mCIM recommended by CLSI in 2017 is a simple and inexpensive method to perform and is well established in many clinical microbiology laboratories based on its high sensitivity and specificity to detect carbapenemase-producing Enterobacteriaceae isolates compared with the current published or available phenotype method such as modified hodge testing and Craba-NP method [5]. Modified hodge testing is very simple to perform and no special reagents or media necessary. however, false-positive results can occur in isolates that produce ESBL or AmpC enzymes coupled with porin loss, and false-negative results are occasionally noted for some strains producing NDM carbapenemase. Carba_NP is a rapid method for detection of suspected carbapenemases among Enterobacteriaceae, but special reagents are needed, some of which necessitate inhouse preparation (and have a short shelf life). Given the rapid international spread of carbapenemase-producing isolates and the urgent need of treatment for the infection due to these isolates, a simple and effective mCIM for detection of KPC-2, NDM-1 and OXA-232-type carbapenemases which were the most common carbapenemases among Enterobacteriacece isolates in China [10, 11] is important.
In CLSI studies [5], one OXA-232-producing K.pneumoniae isolate was negative by mCIM at 4 out of validation sites, however, in this study, all of 5 OXA-232-producing K.pneumoniae isolates were positive by mCIM at different incubating time including 6 h, 18 h and 24 h. In this study, for 6 h, 18 h or 24 h, mCIM demonstrated a sensitivity 100% and specificity 100% for detection of KPC-2, NDM-1, OXA-232-type carbapenemases among Enterobacteriaceae isolates. For 6 h, the indeterminate results occurred for all of carbapenemase-negative Enterobacteriaceae isolates and the results indicated “testing inconclusive for the presence of carbapenemase”. So, for carbapenemase-negative Enterobacteriaceae isolates, it is necessary to extend the incubating time for confirming the production of carbapenemase.
Although carbapenemases involving in this study are only three type of carbapenemase. However, according to the previous studies, blaKPC and blaNDM-1 are the main carbapenemase genes in our country [12]. Other genes including blaOXA-48, blaIPM and blaVIM are rare among Enterobacterieceae clinical isolates [13]. In some cases, especilly for pediatries infected by CRE, early and rapid detection of carbapenemase among Enterobacterieceae clinical isolates with 6 h incubation probably is vital the treatment with antimicrobial agents because the infection caused by carbapenem-resistant Enterobacterieceae clinical isolates are associated with significant morbidity and mortality [14, 15].
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING
This work was supported by the National Natural Science Foundation of China (grant no. 81273559 to Fupin Hu). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
REFERENCES
1. Hawkey PM, Livermore DM. Carbapenem antibiotics for serious infections. BMJ. 2012; 344:e3236.
2. Zhu J, Sun L, Ding B, Yang Y, Xu X, Liu W, Zhu D, Yang F, Zhang H, Hu F. Outbreak of NDM-1-producing Klebsiella pneumoniae ST76 and ST37 isolates in neonates. Eur J Clin Microbiol Infect Dis. 2016; 35:611–618.
3. Pournaras S, Protonotariou E, Voulgari E, Kristo I, Dimitroulia E, Vitti D, Tsalidou M, Maniatis AN, Tsakris A, Sofianou D. Clonal spread of KPC-2 carbapenemase-producing Klebsiella pneumoniae strains in Greece. J Antimicrob Chemother. 2009; 64:348–352.
4. Pantel A, Souzy D, Sotto A, Lavigne JP. Evaluation of Two Phenotypic Screening Tests for Carbapenemase-Producing Enterobacteriaceae. J Clin Microbiol. 2015; 53:3359–3362.
5. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 27th ed. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute. 2017.
6. Vardakas KZ, Tansarli GS, Rafailidis PI, Falagas ME. Carbapenems versus alternative antibiotics for the treatment of bacteraemia due to Enterobacteriaceae producing extendedspectrum β-lactamases: a systematic review and meta-analysis. J Antimicrob Chemother. 2012; 67:2793–2803.
7. Yang K, Guglielmo BJ. Diagnosis and treatment of extended-spectrum and AmpC β-lactamase-producing organisms. Ann Pharmacother. 2007; 41:1427–1435.
8. Hu FP, Guo Y, Zhu DM, Wang F, Jiang XF, Xu YC, Zhang XJ, Zhang CX, Ji P, Xie Y, Kang M, Wang CQ, Wang AM, et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005–2014. Clin Microbiol Infect. 2016; 22:S9–14.
9. Hu FP, Zhu DM, Wang F, Jiang XF, Xu YC, Zhang XJ, Zhang ZX, Ji P, Xie Y, Kang M, Wang CQ, Wang AM, Xu YH, et al. Report of CHINET Antimicrobial Resistance Surveillance Program in 2015. Chinese Journal of Infection and Chemotherapy. 2016; 16:685–694.
10. Lutgring JD, Limbago BM. The Problem of Carbapenemase-Producing-Carbapenem-Resistant-Enterobacteriaceae Detection. J Clin Microbiol. 2016; 54:529–534.
11. Qin X, Yang Y, Hu F, Zhu D. Hospital clonal dissemination of Enterobacter aerogenes producing carbapenemase KPC-2 in a Chinese teaching hospital. J Med Microbiol. 2014; 63:222–228.
12. Zhang R, Liu L, Zhou H, Chan EW, Li J, Fang Y, Li Y, Liao K, Chen S. Nationwide Surveillance of Clinical Carbapenem-resistant Enterobacteriaceae (CRE) Strains in China. EBioMedicine. 2017; 19:98–106.
13. Yin D, Dong D, Li K, Zhang L, Liang J, Yang Y, Wu N, Bao Y, Wang C, Hu F. Clonal Dissemination of OXA-232 Carbapenemase-Producing Klebsiella pneumoniae in Neonates. Antimicrob Agents Chemother. 2017; 61:e00385–17.
14. Centers for Disease Control and Prevention (CDC). Guidance for control of infections with carbapenem-resistant or carbapenemase-producing Enterobacteriaceae in acute care facilities. MMWR Morb Mortal Wkly Rep. 2009; 58:256–60.
15. Logan LK. Carbapenem-resistant Enterobacteriaceae: an emerging problem in children. Clin Infect Dis. 2012; 55:852–859.