
INTRODUCTION
Lung cancer has become a leading cause of cancer-related mortality all over the world in recent years [1]. A lot of efforts have been made to its early detection and treatment; nonetheless, the five-year survival rate for lung cancer is less than 15% after being diagnosed [2, 3]. Currently, surgical resection remains the most effective treatment for early-stage lung cancer. However, approximately 30% patients develop tumour recurrence even after resection [4]. Typically, tumour morphology has been regarded as a prognostic factor for lung cancer since the publication of the 2011 IASLC/ATS/ERS classification in 2011 [5]. For instance, it is suggested that the solid or micropapillary pattern is always linked with poor prognosis [6]. However, there is an urgent need to classify lung cancer according to prognosis in a more precise way.
According to the 2015 WHO classification, tumour spread through air spaces (STAS) is defined as the ‘spread of lung cancer cells into the air spaces in lung parenchyma beyond the edge of the main tumour’, which represents an additional invasive pattern of lung adenocarcinoma [7, 8]. Many studies have shown that STAS is correlated with the poor recurrence-free survival (RFS) and overall survival (OS) in adenocarcinoma and squamous cell carcinoma of lung [9–14]. Howeve, no affirmative conclusion is available about the association of STAS with malignancies. Besides, the existence of STAS is still controversial, making it even more complicated. Thus, it is necessary to evaluate the relationship of STAS with the clinicopathological characteristics and prognosis for patients with lung cancer, so as to clarify the relationship of STAS with the malignant properties.
To evaluate the prognostic role of STAS in lung cancer, a meta-analysis was carried out on all eligible studies, so as to determine the clinicopathological and prognostic significance of STAS in patients with lung cancer.
RESULTS
Characteristics of the included studies
The complete study selection procedure was shown in Figure 1. In brief, a total of 112 articles had been identified from 7 electronic databases using our initial retrieval strategy, including 26 citations from PubMed, 64 from EMBASE, 21 from Web of Science, and 1 from Wanfang database. 30 duplicates of them were removed, and the remaining 82 publications were preliminarily filtered by screening titles and abstracts. Additionally 65 of them were excluded, including 6 reviews, 3 experimental studies, 11 duplicates, and 45 irrelevant studies. Subsequently, the full texts of the remaining 17 studies were read for further filtration. 8 of these 17 studies were excluded due to the lack of an outcome of interest. The remaining 9 articles had met all of the eligibility criteria and were finally enrolled in our meta-analysis [9–17]. The studies analyzed were from Germany, America, Japan, and China, which had involved a total of 3346 patients. Of these 9 studies, 1 had addressed all histological subtypes of lung cancer; 2 had discussed SCC alone and 6 had studied ADC alone. Later, the incorporative ORs were extrapolated from the reported demographical details from eligible studies, so as to evaluate the association of STAS with the clinicopathological characteristics of patients with lung cancer. As for distance or locoregional recurrence, only 1 study [16] reported the statistics of RFS from multivariate and univariate analyses. Additionally, 3 studies [12, 13, 15] had published survival data using the K-M curves, which were used to extrapolate the HR outcomes based on univariate analysis. With regard to RFS and OS, 4 studies [9–14] had reported the statistics from multivariate analysis, respectively. The complete details of estimations were listed in Table 1, and the mean NOS score ranged from 6 to 8, which suggested a good quality level of our meta-analysis.
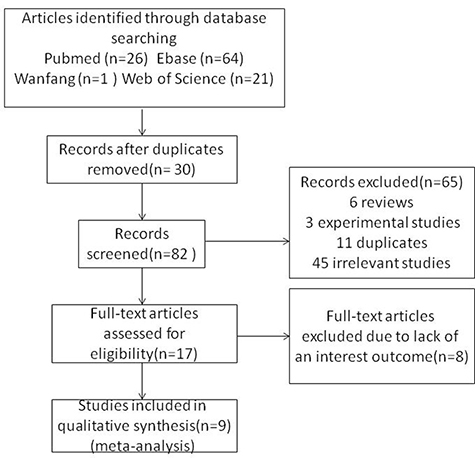
Figure 1: A flow chart of the study design. A systematic literature search yielded a total of 112 articles related to the relationship between STAS and lung cancer. After the screening of titles, abstracts and full texts, 103 articles were excluded for reasons detailed in the main text. A meta-analysis was then performed on 9 studies to assess the clinicopathological and prognostic significance of STAS in patients with lung cancer.
Table 1: NOS scoring records of the included studies
Authors [year] (Ref.) |
Selection |
Comparability |
Exposure |
Total score |
||
|---|---|---|---|---|---|---|
Assessment of outcome |
follow-up long enough for outcomes |
Adequacy of follow-up of cohorts |
||||
Masai K. [2017] |
4 |
2 |
1 |
0 |
1 |
8 |
Kadota K. [2015] |
4 |
2 |
1 |
1 |
0 |
8 |
Kadota K. [2017] |
4 |
2 |
1 |
0 |
1 |
8 |
Lu S. [2017] |
4 |
2 |
1 |
0 |
0 |
7 |
Shiono S. [2016] |
4 |
2 |
1 |
1 |
0 |
8 |
Warth A. [2015] |
4 |
2 |
0 |
0 |
1 |
7 |
Sun PL. [2017] |
4 |
2 |
0 |
0 |
0 |
6 |
Dai C. [2017] |
4 |
2 |
0 |
1 |
0 |
8 |
Uruga H. [2017] |
4 |
2 |
1 |
0 |
0 |
7 |
Association of STAS with the clinicopathological features of lung cancer
In this meta-analysis, the common clinicopathological parameters of lung cancer included gender, age, smoking status, tumor necrosis, TNM stage, as well as vascular, pleural or lymph invasion, and pathological pattern. Results of pooled analyses indicated that the presence of STAS was remarkably associated with male sex (OR = 1.43, 95% CI (1.10–1.87), P < 0.001, I2 = 63%), smoking status (OR = 1.67, 95% CI (1.35–2.06), P < 0.001, I2 = 57%), more advanced TNM stages (OR = 2.52, 95% CI (1.95–3.24), P < 0.001, I2 = 0%), more tumor necroses (OR = 2.37, 95% CI (1.78–3.17), P < 0.001, I2 = 0%), as well as more vascular (OR = 2.73, 95% CI (1.58–4.72), P < 0.001, I2 = 84%), pleural (OR = 3.07, 95% CI (1.45–6.51), P = 0.003, I2 = 84%) or lymph (OR = 3.70, 95% CI (2.39–5.72), P < 0.001, I2 = 77%) invasion, more micropapillary (OR = 14.35, 95% CI (9.22–22.34), P < 0.001, I2 = 22%) and papillary (OR = 1.71, 95% CI (1.18–2.46), P = 0.004, I2 = 49%) pattern, and less lepidic (OR = 0.29, 95% CI (0.21–0.40), P < 0.001, I2 = 79%) pattern. However, no evident relationship was observed between STAS and age of >65 years (OR = 1.01, 95% CI (0.68–1.48), P = 0.98, I2 = 51%) as well as the solid pattern (OR = 1.96, 95% CI (0.95–4.05), P = 0.07, I2 = 90%). The detailed results were listed in Table 2 and Figure 2.
Table 2: Detailed results of meta-analyses for clinicopathological parameters
Characteristics |
N |
No. samples |
Heterogeneity (I2, P) |
Model |
OR [95% CI] |
P value |
Conclusion |
||
|---|---|---|---|---|---|---|---|---|---|
Total |
Stas+ |
Stas- |
|||||||
Gender (male vs. female) |
9 |
3346 |
1178 |
2168 |
63%, 0.006 |
Random |
1.43 [1.10, 1.87] |
<0.001 |
Significant |
Age (>65 vs. ≦65 years) |
3 |
1116 |
426 |
690 |
51%, 0.13 |
Random |
1.01 [0.68, 1.48] |
0.98 |
Not significant |
Smoking (Yes vs. No) |
8 |
2851 |
942 |
1909 |
57%, 0.02 |
Random |
1.67 [1.35, 2.06] |
<0.001 |
Significant |
Vascular invasion (Yes vs. No) |
6 |
2076 |
727 |
1349 |
84%,<0.001 |
Random |
2.73 [1.58, 4.72] |
<0.001 |
Significant |
Pleural invasion (Yes vs. No) |
5 |
1733 |
555 |
1178 |
84%, <0.001 |
Random |
3.07 [1.45, 6.51] |
0.003 |
Significant |
Lymph invasion (Yes vs. No) |
7 |
2394 |
774 |
1620 |
77%, <0.001 |
Random |
3.70 [2.39, 5.72] |
<0.001 |
Significant |
Necrosis (Yes vs. No) |
4 |
1449 |
485 |
964 |
0%, 0.63 |
Fixed |
2.37 [1.78, 3.17] |
<0.001 |
Significant |
Stage (III-IV vs. I-II) |
4 |
1518 |
685 |
833 |
0%, 0.83 |
Fixed |
2.52 [1.95, 3.24] |
<0.001 |
Significant |
Pathological pattern (Micropapillary vs. Others) |
5 |
2159 |
758 |
1401 |
22%, 0.27 |
Fixed |
14.35 [9.22, 22.34] |
<0.001 |
Significant |
Pathological pattern (Lepidic vs. Others) |
3 |
1363 |
559 |
804 |
79%, <0.001 |
Random |
0.29 [0.21, 0.40] |
<0.001 |
Significant |
Pathological pattern (Papillary vs. Others) |
4 |
1651 |
737 |
914 |
49%, 0.004 |
Random |
1.71 [1.18, 2.46] |
0.004 |
Significant |
Pathological pattern (Solid vs. Others) |
5 |
2159 |
813 |
1346 |
90%, <0.001 |
Random |
1.96 [0.95, 4.05] |
0.07 |
Not Significant |
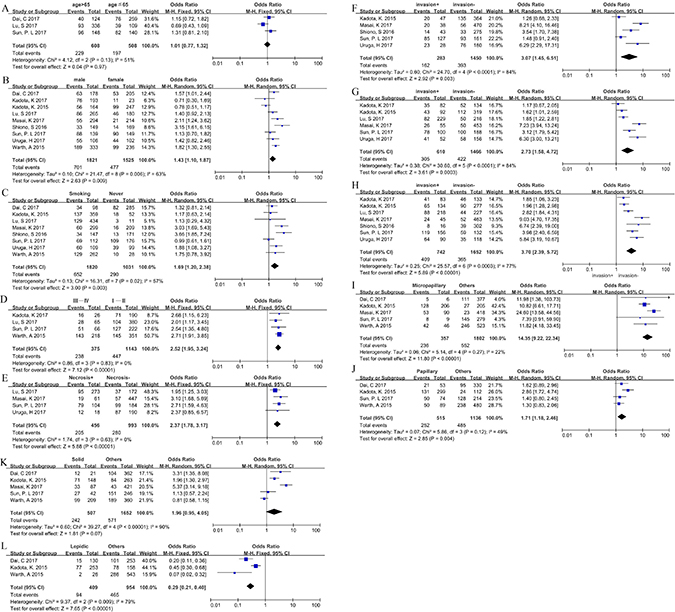
Figure 2: Association between STAS and the clinicopathological characteristics including (A) age, (B) gender, (C) smoking, (D) TNM stage, (E) necrosis, (F) pleural invasion, (G) vascular invasion, (H) lymph invasion, (I) micropapillary, (J) papillary, (K) solid, (L) lepidic.
The prognostic effect of STAS
The pooled HR values revealed that STAS was dramatically correlated with a shorter RFS in patients with lung cancer (HR = 1.69, 95% CI (1.36–2.11), P < 0.001, I2 = 0%). Moreover, it was also found that STAS could serve as a prognostic indicator of locoregional recurrence (HR = 1.91, 95% CI (1.11–3.28) P = 0.02, I2 = 0%) and distant recurrence (HR = 2.16, 95% CI (1.37–3.39), P = 0.001, I2 = 0%). Furthermore, the pooled HR values demonstrated that STAS was also associated with a shorter OS in patients with lung cancer (HR = 1.64, 95% CI (1.31, 2.05), P < 0.001, I2 = 1%). The detailed results were listed in Table 3 and Figure 3.
Table 3: Detailed results of meta-analyses for Recurrence, RFS and OS
Characteristics |
N |
No. samples |
Heterogeneity (I2, P) |
Model |
HR (95% CI) |
P value |
Conclusion |
||
|---|---|---|---|---|---|---|---|---|---|
Total |
Stas+ |
Stas− |
|||||||
Locoregional Recurrence |
3 |
781 |
265 |
516 |
0%, 0.65 |
Fixed |
1.91 [1.11, 3.28] |
0.02 |
Significant |
Distant Recurrence |
4 |
1289 |
341 |
948 |
0%, 0.47 |
Fixed |
2.16 [1.37, 3.39] |
0.001 |
Significant |
RFS |
4 |
1362 |
382 |
980 |
0%, 0.64 |
Fixed |
1.69 [1.36, 2.11] |
<0.001 |
Significant |
OS |
4 |
1558 |
629 |
929 |
1%, 0.38 |
Fixed |
1.64 [1.31, 2.05] |
<0.001 |
Significant |
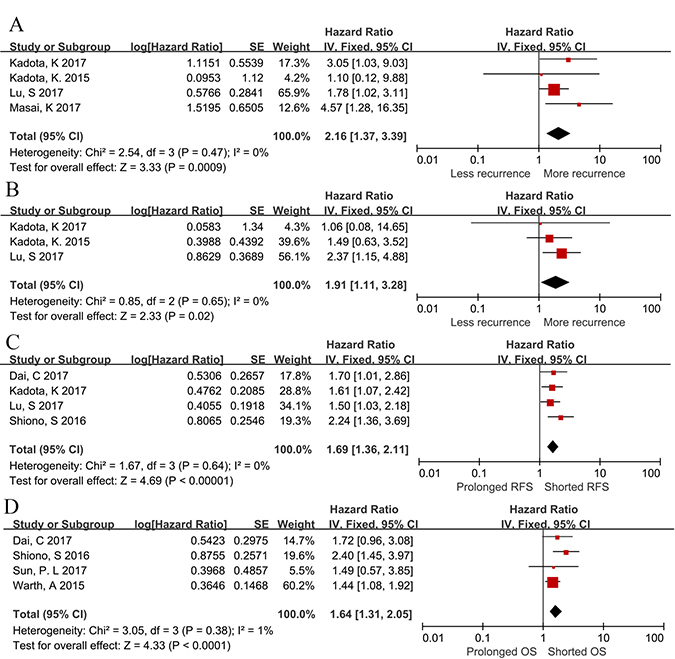
Figure 3: Forest plots evaluating the maximally adjusted association between STAS and prognosis. (A) A Forest plot assessing the effect of STAS on locoregional recurrence in lung cancer. (B) A Forest plot assessing the effect of STAS on distant recurrence in lung cancer. (C) A Forest plot assessing the effect of STAS on RFS in lung cancer. (D) A Forest plot assessing the effect of STAS on OS in lung cancer.
Sensitivity analyses
Sensitivity analyses were carried out in the current meta-analysis to test the robustness of the pooled results. The results suggested that the pooled OR value was not markedly affected when any individual study was removed. Additionally, the pooled HR value was not greatly altered when any individual study was removed, except for the “locoregional recurrence group”. Specifically, the pooled HR value of locoregional recurrence was outstandingly changed after removing 1 study [12].
DISCUSSION
According to the 2015 WHO classification, STAS is defined as “micropapillary clusters, solid nests, or single cells spreading within the air spaces beyond the edge of the main tumor” [7]. Meanwhile, STAS is regarded as the fourth category for defining adenocarcinoma invasion in the existing criteria for invasion, which is deemed as a histological subtype other than a lepidic, pleural or vascular invasion, and pattern myofibroblastic stroma associated with invasive tumor cells. Prior to the definition of STAS, aerogenous tumor spread and free floating cell clusters from ADC, as well as colorectal cancer metastases, are indicated to be unfavorable prognostic features in previous reports [18–20]. In 2013, Onozato et al. [21] reported that, the presence of tumour islands was dramatically linked with smoking, high-grade pathological pattern, higher nuclear grade and KRAS mutations. More importantly, tumor islands were found to be markedly related to a shorter RFS. However, this study is not included in our meta-analysis, which can be attributed to its slightly different definition of tumour islands to the STAS definition [7, 8].
STAS is a brand new concept, which is still in a controversial stage of development. Different definitions of STAS have been applied in different studies (Table 4). Interestingly, high comparability of the associations of clinicopathological features with the prognostic impact of STAS is noticed among all studies, in spite of the more or less different definitions. Kadota et al. [15] first reported that the presence of STAS was an independent predictor of recurrence in patients with lung adenocarcinoma undergoing limited surgical resection, but it was not markedly associated with recurrence in the lobectomy group. Warth et al. [9] demonstrated that the presence of tumour STAS was related to both the reduced OS and disease-free survival (DFS) in patients with adenocarcinomas receiving lobectomy, but it was not independent of stage. Shiono and Yanagawa [10] reported that STAS was closely correlated with dismal prognosis and recurrence. Furthermore, Lu et al. [13] and Kadota et al. [12] discovered that STAS was not limited to ADC, but was also a significant prognostic parameter for SCC. In the meantime, it was also an independent prognostic factor for both recurrence and survival in lung squamous cell carcinoma.
Table 4: Studies applied divergent defnitions of STAS and artifacts separation method
Author [year] (Ref.) |
Definition of STAS |
Criteria to separate artifacts |
|---|---|---|
Masai K. [2017] |
Noncontinuous cells less than one alveolus away from the edge of the main tumor: single cells, small cell clusters, and large nests, and must be distinguished from tumor spread through the mucus |
Not report |
Kadota K. [2015] |
Micropapillary clusters, solid nests, or single cells spreading within air spaces beyond the edge of the main tumor |
The presence of jagged edges of tumor cell clusters suggested tumor fragmentation or edges of a knife cut during specimen processing rather than STAS. Linear strips of cells that were lifted off of alveolar walls also favored the presence of artifact. |
Kadota K. [2017] |
small clusters of tumor cell nests within air spaces in the lung parenchyma beyond the edge of the main tumor |
Haphazardly distributed fragments of tumor with sharp jagged edges were regarded as artifacts |
Lu S. [2017] |
small clusters of tumor cell nests within air spaces in the lung parenchyma beyond the edge of the main tumor |
Haphazardly distributed fragments of tumor with sharp jagged edges were regarded as artifacts |
Shiono S. [2016] |
Tumor cell clusters lying freely within the alveolar space at a distance of at least 0.5 mm from the main tumor |
Not report |
Warth A. [2015] |
Detachment of small cell nests (at least 5 tumor cells) <3 alveoli away from the main tumor mass (limited STAS) and tumor cell nests >3 alveoli away from the main tumor mass (extensive STAS) |
tumor cells were only considered if they were arranged in loose small groups, and the distribution was consistent with the overall configuration of the circumferential tumor edge. |
Sun PL. [2017] |
Micropapillary clusters, solid nests, or single cells spreading within air spaces beyond the edge of the main tumor |
Not report |
Dai C. [2017] |
Tumor cells observed within air spaces in the surrounding lung parenchyma beyond the edge of the main tumor. It was classified into three morphologic subtypes: (I) single cells, (II) micropapillary clusters, and (III) solid nests |
The presence of jagged edges of tumor cell clusters suggested tumor fragmentation or edges of a knife cut during specimen processing rather than STAS. Linear strips of cells that were lifted off of alveolar walls also favored the presence of artifact. |
Uruga H. [2017] |
Micropapillary clusters, solid nests, or single cells spreading within air spaces beyond the edge of the main tumor. Cases were further classified as no STAS, low STAS (1–4 clusters of micropapillary or solid nest-predominant STAS), or high STAS (≥5 clusters of STAS) |
Not report |
Most recent studies indicate that STAS is related to the malignancy of lung cancer; nevertheless, whether STAS exists in any instances remains a source of controversy. First of all, it remains unclear whether STAS is induced by the process of cutting through a tumor with a knife? Blaauwgeers H et al. [22] reported that the number of free tumor cells within the air spaces would be increased by cutting, indicating that at least a certain proportion of STAS might be caused by the pathologist during specimen processing. Furthermore, it is found that a certain portion of the solid type STAS is the direct extension of tumor cells from the main tumor by 3D reconstruction [23]. Secondly, whether STAS spreads through a surgeon is also unclear? Mechanical stress may be possibly apply to a tumor during the operation, which would prompt the tumor periphery into the adjacent air spaces [24]. Thirdly, it remains controversial whether STAS spreads through bronchoscopic or transthoracic tumor biopsies? Single tumor cells or cell clusters may be detached during tumor biopsies, which may then reach the adjacent air spaces. However, no studies have specifically assessed intrapulmonary tumor spread after bronchoscopic or transthoracic tumor biopsies up to now. Nevertheless, the clinicopathological associations and the prognostic impact of STAS are highly comparable across all studies. As a result, it is difficult to explain the significant association of STAS with prognosis and recurrence, if STAS would only be an artifact induced by the above circumstances.
The outcome data from all the currently available studies are integrated into our meta-analysis, the results of which indicate that STAS can serve as a biomarker for the dismal prognosis for lung cancer. Besides, the current meta-analysis also attempts to estimate the relationship between STAS and several major clinicopathological features of lung cancer. Specifically, the presence of STAS is found to be evidently associated with the worse conditions of tumor invasion, TNM stage, tumor necrosis and pathological pattern, all of which were critical factors resulting in the negative prognosis for lung cancer. We speculate that the clinicopathological significance of the presence of STAS may potentially interpret its prognostic roles in lung cancer to some extent.
However, the accuracy of our summarized outcomes may be more or less reduced by the following bias risks from the statistical sources.
Firstly, in this meta-analysis, no multivariate OR statistics are reported to assess the relationship between the presence of STAS and the clinicopathological features of lung cancer. Furthermore, there are 5 HR statistics extrapolated from the published survival details based on the univariate analysis, which are also incorporated into the prognostic assessments of locoregional and distance recurrence. In addition, it is also realized that, some studies do not include the stage together with STAS in a multivariate Cox model [9–11], despite that multivariate HR statistics have been used to summarize the association between STAS and RFS or OS of lung cancer. Warth et al. [9] reported that stage itself was a highly prognostic STAS-independent parameter in this setting. Thus, we are afraid that the accuracy of the overall pooled estimates for these issues may be slightly attenuated by some insufficiently eliminated confounders, which may affect the prognosis of lung cancer. Therefore, the validity and accuracy of all the summarized outcomes should be further verified and modified in the future multivariate analyses, in the absence of any bias risk from other confounding factors.
Secondly, there is huge heterogeneity within the definitions and/or related morphological features for the presence of STAS. Therefore, an unavoidable deviation originated from the heterogeneous criteria of evaluation can negatively affect the validity of the pooled estimates. Additionally, the different criteria (Table 4) used to identify artifacts from STAS are worthy of our attention. Besides, lacking the unified criteria may also cause adverse effects on the homogeneity level of the included studies [25]. On this account, these limitations must be judiciously evaluated when interpreting our summarized outcomes correctly.
Thirdly, it is also noticed that many operation methods are included in the enrolled studies, including limited resection, lobectomy or more. Nevertheless, only available data from limited resection can be found in some studies [15, 16]. What’s more, Kadota et al. [15] reported that the association of STAS with recurrence was different between limited resection group and lobectomy group, and that STAS was not outstandingly associated with the recurrence in the lobectomy group. Our results of sensitivity analysis indicate that, the strong robustness of the prognostic significance of STAS in lung cancer is reduced by removing 1 study [12]. Therefore, the variations of operation method may be one important source of bias when synthesizing the current evidence in our meta-analysis.
Fourthly, the enrolled patients are not stratified according to their nations or histological subtypes. Only 2 studies for SCC patients and 1 for NSCLC patients have contained different histological subtypes. Consequently, subgroup analyses have not been performed to further evaluate the potential ethnic or histological differences in the prognostic roles of STAS in lung cancer. What’s more, the number of studies under each nation or histological subgroup is small and the quality of evidence is low, resulting in a lack of confidence in the combined results. Therefore, more large scale studies are urgently required to analyze the presence of STAS in each subtype of NSCLC.
Finally, studies reporting the beneficial intervention effects or a larger effect size are more likely to be published, while those with the same amount of data towards the other directions may remain unpublished [26]. In addition, when less than 10 studies are included in a meta-analysis, it may lead to a large decline on the efficacy of publication bias tests, thus resulting in potentially misleading evidence for publication bias [27]. As for our meta-analysis, only 9 studies are included into the analysis; as a result, Begg’s test or Egger’s test is not conducted to detect the publication bias. Therefore, we doubt that potential publication bias may exist across the included studies.
In conclusion, our meta-analysis demonstrates that the presence of STAS is dramatically correlated with the unfavorable outcomes of tumor invasion, tumor necrosis, tumour stage and ADC growth patterns. Furthermore, STAS can serve as an independent predictor for the poor prognosis of lung cancer. Nevertheless, some controversies and limitations have not yet been well resolved in this meta-analysis. First of all, a more precise definition of STAS should be developed. Secondly, more precise criteria are also required separate artifacts from STAS effects. Thirdly, more high-quality worldwide studies with large sample size performing a multivariate analysis will be helpful to further verify and modify our current findings in the future.
METHODS
Literature retrieval
In this meta-analysis, literature was retrieved from October 7th, 2017, to December 30th, 2017. Altogether, 7 universal electronic databases were used for searching the full-text literature reports published up to December 30th, 2017, including PubMed, EMBASE, Web of Science, Cochrane database, China National Knowledge Internet database, Wanfang database and VIP database. These search terms were listed as follows: (1) “spread through air spaces” or “STAS” and “lung cancer” or “lung carcinoma” or “lung neoplasm” or “lung tumour”. Meanwhile, additional studies were also identified from references listed in the retrieved articles through manual searching.
Selection criteria
The literature inclusion and exclusion criteria were listed as follows. Inclusion criteria (I) studies with the target disease of lung cancer; (II) studies in which STAS was defined according to 2015 World Health Organization (WHO); and (III) studies in which at least one of the outcome measures of interest was reported or calculated from published data. Exclusion criteria (I) reviews, preclinical experiments, letters and abstracts; (II) studies provided insufficient data; or (III) repeated studies based on the same database or patients.
Data extraction and assessment of study quality
The following information was collected (Table 5): (I) publication data including authors and publication years; (II) experimental data including study design, detection methods, study period, investigating categories, and endpoints; and (III) demographical data, including the number of patients, data origin, gender, age, histological types, surgical method, and stage. In addition, the Newcastle–Ottawa Scale (NOS) was employed to evaluate the quality level of the original non-randomized studies [28]. In the meantime, 3 perspectives, involving selection, comparability and exposure, were considered for a semiquantitative estimation. Furthermore, a ‘‘star system’’ with a maximum of 9 stars was employed as the assessment tool.
Table 5: Characteristics and design variables of the including studies
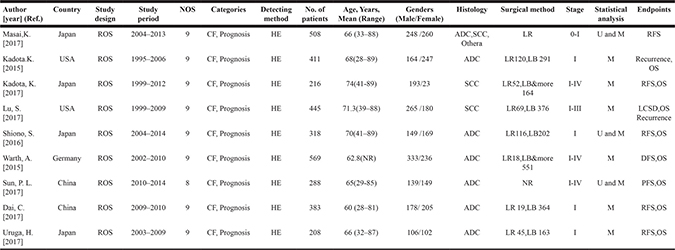
a: Other includes seven small cell carcinomas, seven large cell neuroendocrine carcinomas, five adenosquamous carcinomas, four large cell carcinomas, and one typical carcinoid tumor. ADC, adenocarcinoma; SCC, squamous cell carcinoma; ROS, retrospective observational study; CF, clinicopathological features; OS, overall survival; LR, limited resection; LB, lobectomy; WR, Wedge resection; LCSD, lung cancer–specific death; M, multivariate; U, univariate; NR, not report; RFS, Recurrence-free survival; DFS, disease free survival; PFS, Progress Free Survival
Statistical analysis
Statistical analysis was conducted using Review Manager 5.1.2 software. Briefly, the estimated OR was used to summarize the association of STAS with the clinicopathological characteristics of lung cancer. Meanwhile, the estimated HR was applied in evaluating the prognostic effects (locoregional recurrence, distant recurrence, OS and RFS). HR and its variance that were not reported directly in the original study were calculated from the available reported data, according to a practical method described by Tierney et al. [29]. All statistical values were combined with the associated 95% confidence intervals (CIs). In addition, the level of heterogeneity within this meta-analysis was determined using Q-test and I2-statistic. Typically, a fixed-effects model was applied in the initial analysis, and a confirmed random-effects model would also be employed in the presence of significant heterogeneity (I2 ≥ 40% or P ≤ 0.1). Besides, an additional sensitivity analysis was performed to further examine the robustness of our meta-analysis. Nonetheless, publication bias tests were no longer required according to Cochrane Handbook, since less than 10 studies were enrolled into the current meta-analysis [26]. On this account, Begg’s test or Egger’s test was not carried out to detect the potential publication bias in this meta-analysis.
Abbreviations
CI: confidence intervals; STAS: spread through air spaces; ADC: adenocarcinoma; SCC: squamous cell carcinoma; HR: hazard ratio; NOS: Newcastle-Ottawa scale; OR: odds ratio; OS: overall survival; RFS: recurrence-free survival.
ACKNOWLEDGMENTS
This work was supported by two project grants (No.2014SZ0148 and No. 2015SZ0158) from the Foundation of Science and Technology support plan, Department of Sichuan Province, China. We are grateful for this funding support.
CONFLICTS OF INTEREST
There are no potential conflicts of interest to disclose.
REFERENCES
1. Zou Z. Cancer statistics, 2014. Ca A Cancer Journal for Clinicians. 2015; 65:5–29.
2. Brundage MD, Davies D, Mackillop WJ. Prognostic factors in non-small cell lung cancer: a decade of progress. Chest. 2002; 122:1037.
3. Berrino F, Angelis RD, Sant M, Rosso S, Lasota MB, Coebergh JW, Santaquilani M. Survival for eight major cancers and all cancers combined for European adults diagnosed in 1995–99: results of the EUROCARE-4 study. Lancet Oncology. 2007; 8:773.
4. Hung JJ, Jeng WJ, Hsu WH, Chou TY, Huang BS, Wu YC. Predictors of death, local recurrence, and distant metastasis in completely resected pathological stage-I non-small-cell lung cancer. Journal of Thoracic Oncology Official Publication of the International Association for the Study of Lung Cancer. 2012; 7:1115.
5. Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. The Journal of Evidence-Based Medicine. 2011; 6:244–85.
6. Warth A, Muley T, Meister M, Stenzinger A, Thomas M, Schirmacher P, Schnabel PA, Budczies J, Hoffmann H, Weichert W. The novel histologic International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification system of lung adenocarcinoma is a stage-independent predictor of survival. Journal of Clinical Oncology. 2012; 30:1438.
7. Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Jhm A, Beasley MB, Chirieac LR, Dacic S, Duhig E, Flieder DB. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. Journal of Thoracic Oncology. 2015; 10:1243.
8. Morales-Oyarvide V, Mino-Kenudson M. Tumor islands and spread through air spaces: Distinct patterns of invasion in lung adenocarcinoma. Pathology International. 2016; 66:1.
9. Warth A, Muley T, Kossakowski CA, Goeppert B, Schirmacher P, Dienemann H, Weichert W. Prognostic Impact of Intra-alveolar Tumor Spread in Pulmonary Adenocarcinoma. American Journal of Surgical Pathology. 2015; 39:793–801.
10. Shiono S, Yanagawa N. Spread through air spaces is a predictive factor of recurrence and a prognostic factor in stage I lung adenocarcinoma. Interactive Cardiovascular & Thoracic Surgery. 2016; 23:ivw211.
11. Dai C, Xie H, Su H, She Y, Zhu E, Fan Z, Zhou F, Ren Y, Xie D, Zheng H, Kadeer X, Chen D, Zhang L, et al. Tumor Spread through Air Spaces Affects the Recurrence and Overall Survival in Patients with Lung Adenocarcinoma >2 to 3 cm. J Thorac Oncol. 2017; 12:1052–60. https://doi.org/10.1016/j.jtho.2017.03.020.
12. Kadota K, Kushida Y, Katsuki N, Ishikawa R, Ibuki E, Motoyama M, Nii K, Yokomise H, Bandoh S, Haba R. Tumor Spread Through Air Spaces Is an Independent Predictor of Recurrence-free Survival in Patients With Resected Lung Squamous Cell Carcinoma. American Journal of Surgical Pathology. 2017; 41:1077–86.
13. Lu S, Tan KS, Kadota K, Eguchi T, Bains S, Rekhtman N, Adusumilli PS, Travis WD. Spread through Air Spaces (STAS) Is an Independent Predictor of Recurrence and Lung Cancer-Specific Death in Squamous Cell Carcinoma. Journal of Thoracic Oncology. 2017; 12:223.
14. Sun PL, Liu JN, Cao LQ, Yao M, Gao HW. [To evaluate the clinicopathologic characteristics and outcome of tumor cells spreading through air spaces in patients with adenocarcinoma of lung]. Zhonghua bing li xue za zhi = Chinese journal of pathology. 2017; 46:303.
15. Kadota K, Nitadori J, Sima CS, Ujiie H, Rizk NP, Jones DR, Adusumilli PS, Travis WD. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J Thorac Oncol. 2015; 10:806–14. https://doi.org/10.1097/jto.0000000000000486.
16. Masai K, Sakurai H, Sukeda A, Suzuki S, Asakura K, Nakagawa K, Asamura H, Watanabe SI, Motoi N, Hiraoka N. Prognostic Impact of Margin Distance and Tumor Spread Through Air Spaces in Limited Resection for Primary Lung Cancer. Journal of Thoracic Oncology Official Publication of the International Association for the Study of Lung Cancer. 2017.
17. Uruga H, Fujii T, Fujimori S, Kohno T, Kishi K. Semi-quantitative Assessment of Tumor Spread Through Air Spaces (STAS) in Early Stage Lung Adenocarcinomas. Journal of Thoracic Oncology. 2017; 12:1046–51.
18. Clayton F. Bronchioloalveolar carcinomas. Cell types, patterns of growth, and prognostic correlates. Cancer. 2015; 57:1555–64.
19. Shiono S, Ishii G, Nagai K, Yoshida J, Nishimura M, Murata Y, Tsuta K, Kim YH, Nishiwaki Y, Kodama T. Predictive factors for local recurrence of resected colorectal lung metastases. Annals of Thoracic Surgery. 2005; 80:1040–5.
20. Shiono S, Ishii GK, Yoshida J, Nishimura M, Murata Y, Tsuta K, Nishiwaki Y, Kodama T, Ochiai A. Histopathologic Prognostic Factors in Resected Colorectal Lung Metastases - The Annals of Thoracic Surgery. Annals of Thoracic Surgery. 2005; 79:278–82.
21. Onozato ML, Kovach AE, Yeap BY, Morales-Oyarvide V, Klepeis VE, Tammireddy S, Heist RS, Mark EJ, Dias-Santagata D, Iafrate AJ. Tumor islands in resected early-stage lung adenocarcinomas are associated with unique clinicopathologic and molecular characteristics and worse prognosis. American Journal of Surgical Pathology. 2013; 37:287–94.
22. Thunnissen E, Blaauwgeers HJ, de Cuba EM, Yick CY, Flieder DB. Ex Vivo Artifacts and Histopathologic Pitfalls in the Lung. Archives of Pathology & Laboratory Medicine. 2016; 140:212.
23. Onozato ML, Klepeis VE, Yagi Y, Minokenudson M. A Role of Three-Dimensional (3D)-Reconstruction in the Classification of Lung Adenocarcinoma. Analytical Cellular Pathology. 2016; 35:79–84.
24. Warth A. Spread through air spaces (STAS): a comprehensive update. Translational Lung Cancer Research. 2017; 6:501.
25. Li S, Lai Y, Fan J, Shen C, Che G. Clinicopathological and prognostic significance of Nestin expression in patients with non-small cell lung cancer: a systematic review and meta-analysis. Clinical & Experimental Medicine. 2016; 5:1–14.
26. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Naunyn-Schmiedebergs Archiv für experimentelle Pathologie und Pharmakologie. 2008; 5:S38.
27. Li SJ, Chen DL, Zhang WB, Shen C, Che GW. Prognostic value of stromal decorin expression in patients with breast cancer: a meta-analysis. Journal of Thoracic Disease. 2015; 7:1939.
28. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. European Journal of Epidemiology. 2010; 25:603–5.
29. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007; 8:16.