
INTRODUCTION
Gastric cancer (GC) is among the leading causes of cancer-related mortality globally, and ranks the second of all cancer-related mortality in China, despite a declining global incidence [1, 2]. Early-stage GC is generally asymptomatic, and the majority of patients are diagnosed at advanced stage. Despite great progress of chemotherapy and radiation therapy in GC [3], accurate prognostic stratification is still an important issue in determining therapeutic strategy. Precise classification of tumor stage, including the invasive depth as well as lymph node involvement, plays a critical role in evaluating prognosis and determining the stage-specific therapeutic strategy. The AJCC/UICC TNM classification is the most well-defined indicator to predict survival, which, therefore, plays an essential role in the therapeutic strategy of GC patients. In this classification, non-metastatic (M0) GC is categorized into seven risk groups in accordance with the number of involved lymph nodes as well as pathologically invasive depth [4]. However, the outcomes of subjects with the same TNM stage and undergoing similar therapy generally vary from one to another, indicating the inadequateness of the present AJCC TNM classification in determining therapeutic strategy and assessing prognosis, because only anatomical factors are considered [5]. Other factors, including age, sex, gender, tumor size as well as differentiation should be taken into consideration for personalized survival prediction. Therefore, it is urgently needed to establish a new prognostic system that includes all these factors.
Nomogram, a statistics-based method providing the overall probability of a specific outcome, has been prevalently applied in a series of malignancies, including GC [6–12]. In recent researches, nomogram combined with the biomarkers of systemic inflammation response (SIR) has been showed to harbor more precise prediction compared to traditional stage classification in multiple malignancies [9, 13, 14]. The SIR is characterized by variations of peripheral blood cell amounts and serum biomarkers. Moreover, the systemic inflammation-based prognostic scores, including Glasgow Prognostic Score (GPS), C-reactive protein albumin (CRP/Alb) ratio [15], neutrophil lymphocyte ratio (NLR) [16], and lymphocyte monocyte ratio (LMR) [17] have emerged as prognostic factors in gastric cancer [18, 19]. The above-described factors are cost-effective, routinely performed in clinical practice, which, therefore, might be used for prognostic prediction by using accessible objective data. Nevertheless, few researches have reported on establishing a prognostic nomogram of GC by collaborating these factors. GPS, NLR as well as CRP/Alb are defined as risk factors, while LMR is defined as a protective factor. In this study, we selected monocyte lymphocyte ratio (MLR) as a risk factor and together with other inflammation-based prognostic scores (GPS, NLR and CRP/Alb) as well as clinic-pathological parameters as potential prognostic factors in order to construct a prognostic nomogram for resectable GC. Moreover, the study was also designed to assess the advantage of this nomogram over the 7th and 8th edition of AJCC TNM staging systems in terms of precise prediction of survival.
RESULTS
Patient characteristics
The clinic-pathologic characteristics in both training cohort (n=370) and validation cohort (n=101) were shown in Table 1. The median age in training set and validation set was 61 years (range, 27–85 years) and 60 years (range, 32–78 years), respectively. Over the follow-up period, 80 subjects died (median follow-up, 29.51months) in the training cohort, with the median OS not being obtained. In terms of validation set, 46 (62.2%) subjects died (median follow-up, 25.1 months), with the median OS of 33.41 months (ranging from 2 to 77 months).
Table 1: Clinical characteristics of patients with gastric cancer undergoing R0 resection
Variable |
Primary Cohort (N=370) |
Validation Cohort (N=101) |
||
|---|---|---|---|---|
No. of Patients |
% |
No. of Patients |
% |
|
Gender |
||||
Male |
264 |
71.4 |
69 |
68.3 |
Female |
106 |
28.6 |
32 |
31.7 |
Age |
||||
<62 |
183 |
49.2 |
51 |
50.5 |
≥62 |
187 |
50.3 |
50 |
49.5 |
Helicobator pylori |
||||
Negative |
130 |
35.1 |
38 |
37.6 |
Positive |
240 |
64.9 |
63 |
62.4 |
Tumor size |
||||
<5cm |
256 |
68.8 |
57 |
56.4 |
≥5cm |
114 |
30.6 |
44 |
43.6 |
Degree of differentiation |
||||
Poorly+signet ring cell |
194 |
52.2 |
59 |
58.4 |
Moderately |
165 |
44.4 |
40 |
39.6 |
Well |
11 |
3.0 |
2 |
2.0 |
Location |
||||
Upper third |
37 |
9.9 |
11 |
10.9 |
Middle third |
96 |
25.8 |
23 |
22.8 |
Lower third |
209 |
56.2 |
56 |
55.4 |
Diffuse |
28 |
7.5 |
11 |
10.9 |
Type of gastrectomy |
||||
Subtotal |
246 |
66.5 |
67 |
66.3 |
Total |
124 |
33.5 |
34 |
33.7 |
Depth of invasion |
||||
T1 |
87 |
23.5 |
7 |
6.9 |
T2 |
64 |
17.3 |
13 |
12.9 |
T3 |
120 |
32.4 |
41 |
40.6 |
T4a |
69 |
18.6 |
25 |
24.8 |
T4b |
30 |
8.1 |
15 |
14.9 |
LN status |
||||
N0 |
155 |
41.7 |
40 |
39.6 |
N1 |
58 |
15.6 |
7 |
6.9 |
N2 |
60 |
16.1 |
13 |
12.9 |
N3a |
72 |
19.4 |
31 |
30.7 |
N3b |
25 |
6.7 |
10 |
9.9 |
Metastasis |
||||
NO |
349 |
93.8 |
87 |
86.1 |
YES |
21 |
5.6 |
14 |
13.9 |
Retrieved lymph nodes |
||||
≤15 |
156 |
44.3 |
43 |
42.6 |
>15 |
214 |
55.7 |
58 |
57.4 |
Chemotherapy |
||||
NO |
207 |
55.9 |
11 |
10.9 |
Yes |
163 |
44.1 |
90 |
89.1 |
The 7th TNM stage (AJCC) |
||||
IA |
77 |
20.7 |
5 |
5.0 |
IB |
38 |
10.2 |
9 |
8.9 |
IIA |
55 |
14.8 |
21 |
20.8 |
IIB |
39 |
10.5 |
11 |
10.9 |
IIIA |
35 |
9.4 |
7 |
6.9 |
IIIB |
57 |
15.3 |
13 |
12.9 |
IIIC |
48 |
12.9 |
21 |
20.8 |
IV |
21 |
5.6 |
14 |
13.9 |
The 8th TNM stage (AJCC) |
||||
IA |
77 |
20.7 |
5 |
5.0 |
IB |
38 |
10.2 |
9 |
8.9 |
IIA |
55 |
14.8 |
21 |
20.8 |
IIB |
39 |
10.5 |
11 |
10.9 |
IIIA |
53 |
14.2 |
9 |
8.9 |
IIIB |
61 |
16.4 |
22 |
21.8 |
IIIC |
26 |
7.0 |
10 |
9.9 |
IV |
21 |
5.6 |
14 |
13.9 |
NLR |
||||
<1.83 |
124 |
33.5 |
33 |
32.7 |
≥1.83 |
246 |
66.5 |
68 |
67.3 |
MLR |
||||
<0.35 |
291 |
78.6 |
78 |
77.2 |
≥0.35 |
79 |
21.4 |
23 |
22.8 |
CRP/Alb |
||||
<0.16 |
213 |
57.3 |
65 |
64.4 |
≥0.16 |
137 |
36.8 |
33 |
32.7 |
GPS |
||||
0 |
179 |
48.4 |
50 |
49.5 |
1 |
122 |
33.0 |
16 |
15.8 |
2 |
49 |
13.2 |
35 |
34.7 |
Abbreviations: AJCC: American Joint Committee on Cancer; NLR: neutrophil lymphocyte ratio; MLR: monocyte lymphocyte ratio; CRP/Alb: C-reactive protein albumin ratio; GPS: Glasgow Prognostic Score
Associations of inflammatory response biomarkers with OS
KM survival analysis along with log-rank tests were conducted on the basis of the postoperative survival in the training cohort to assess the potential correlation. As a result, MLR (≥0.35) (P=0.002), CRP/Alb (≥0.16) (P<0.018), GPS (2 vs 0) (P=0.014), but not NLR (≥1.83) (P=0.203), were significantly related to reduced decreased OS (Figure 1A–1D).
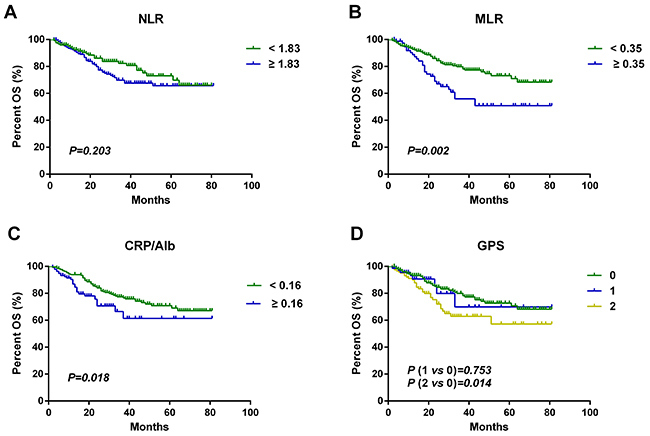
Figure 1: Kaplan–Meier curves for overall survival probability according to preoperative NLR, MLR, CRP/Alb and GPS. Kaplan–Meier analysis for OS according to (A) preoperative NLR, (B) preoperative MLR, (C) preoperative CRP/Alb, and (D) preoperative GPS.
Nomogram development and internal validation.
Cox regression model was used to further assess the inflammatory response indicators as well as clinic-pathological factors in predicting in a univariate analysis. Consequently, it revealed that gender, tumor length, degree of differentiation, location, TNM stage, chemotherapy, MLR, CRP/Alb and GPS were prognostic factors of OS, while age, type of gastrectomy, retrieved lymph nodes and NLR showed no statistical differences (Table 2). Multivariate analysis further showed tumor length, N stage, M stage, MLR and GPS as independent risk factors for OS. Although T stage was insignificance in the multivariate analysis, however, in consideration of T stage as an important prognostic factor, it was included in the nomogram as well. A nomogram integrating six factors: tumor length, T stage, N stage, M stage, MLR and GPS was ultimately established to predict 3- and 5-year OS in the training set (Figure 2). To determine the point of every prognostic factor in the nomogram, a line was drawn straight upward to the point axis, followed by sum up to obtain the total points, which were placed in the total point axis. The 3- and 5-year OS was estimated by drawing a straight line down from the total point axis. The concordance index (C-index) for OS prediction was 0.83 (95% CI, 0.78–0.88). The calibration plot for the probability of post-operative 3- and 5- year survival demonstrated a good correlation between nomogram predictions and actual outcomes (Figure 3A, 3B). In the validation set, the C-index for OS prediction was 0.83 (95% CI 0.77~0.88). The calibration curves indicated the good performance of the nomogram performed well in 3- and 5-year OS prediction (Figure 3C, 3D). Together, the above outcomes indicated that the nomogram was a more helpful and accurate approach in OS prediction for GC subjects undergoing R0 resection.
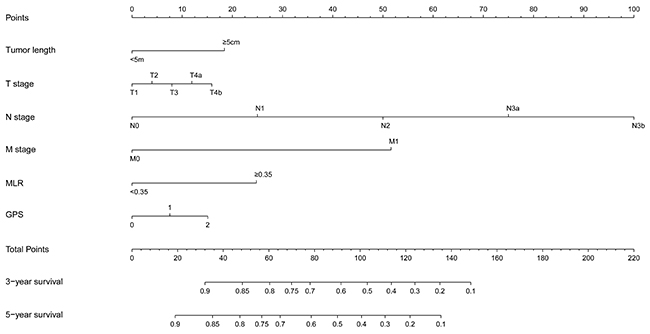
Figure 2: Nomogram for predicting 3- and 5-year OS of patients with gastric cancer undergoing R0 resection. To use the nomogram, the value attributed to an individual patient is located on each variable axis, and a line is drawn upwards to determine the number of points received for each variable value. The sum of these numbers is located on the total point axis, and a line is then drawn downwards to the survival axis to determine the likelihood of 3- and 5-year OS.
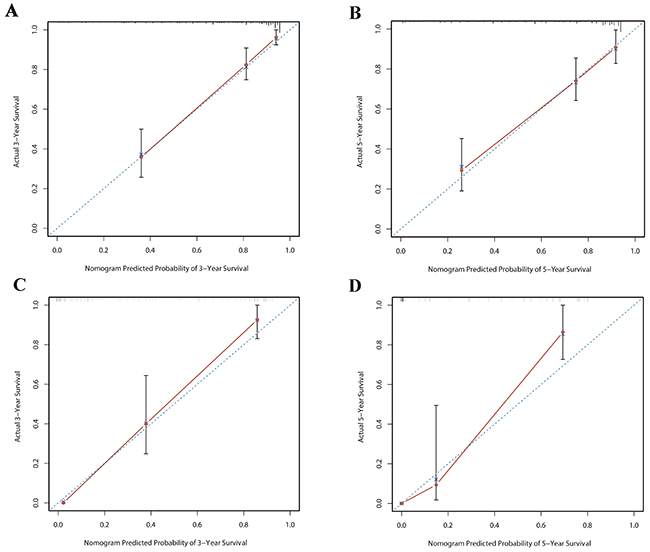
Figure 3: Validation of nomogram for 3-year and 5-year OS of patients with gastric cancer undergoing R0 resection. The calibration curve of the nomogram for predicting patient survival at 3-year (A) and 5-year (B) in the primary cohort. The calibration curve for predicting patient survival at 3-year (C) and 5-year (D) in the validation cohort. The blue dashed line represents the “ideal” line of a perfect match between predicted and observed survival. The red line indicates the performance of the proposed nomogram. Red dots are sub-cohorts of the data set. Vertical bars represent 95% confidence interval.
Table 2: Univariate and multivariate cox regression analyses for overall survival in patients with gastric cancer undergoing R0 resection
Variable |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
HR (95%CI) |
P |
HR (95%CI) |
P |
|
Gender |
||||
Male vs Female |
1.85(1.06-3.24) |
0.032 |
1.50(0.84-2.69) |
0.175 |
Age (median age: 62) |
||||
<62 vs≥62 |
1.07(0.69-1.66) |
0.780 |
- |
|
Tumor length |
||||
<5cm vs ≥5cm |
0.28(0.18-0.44) |
<0.01 |
0.48(0.29-0.79) |
0.004 |
Degree of differentiation |
||||
Poorly+signet ring cell 1 |
1 |
|||
Moderately |
0.51(0.32-0.81) |
0.004 |
0.81(0.48-1.35) |
0.417 |
Well |
0.01(0-10.11) |
0.960 |
0.02(0-11.12) |
0.973 |
Location |
||||
Upper third |
1 |
1 |
||
Middle third |
1.92(0.79-4.67) |
0.153 |
1.35(0.53-3.43) |
0.530 |
Lower third |
1.22(0.52-2.88) |
0.653 |
1.07(0.44-2.60) |
0.886 |
Diffuse |
3.83(1.41-10.40) |
0.008 |
2.12(0.74-6.03) |
0.160 |
Type of gastrectomy |
||||
Subtotal vs Total |
0.52(0.337-0.815) |
0.524 |
- |
|
T stage |
||||
T1 |
1 |
1 |
||
T2 |
2.20(0.70-6.93) |
0.178 |
1.21(0.35-4.22) |
0.763 |
T3 |
5.73(2.24-14.68) |
<0.01 |
2.22(0.77-6.41) |
0.139 |
T4a |
7.67(2.86-20.61) |
<0.01 |
1.96(0.60-6.45) |
0.267 |
T4b |
19.50(7.03-54.10) |
<0.01 |
1.74(0.49-6.16) |
0.389 |
N stage |
||||
N0 |
1 |
1 |
||
N1 |
1.60(0.64-4.02) |
0.315 |
0.91(0.34-2.41) |
0.848 |
N2 |
4.83(2.38-9.80) |
<0.01 |
3.02(1.43-6.37) |
0.004 |
N3a |
7.86(4.06-15.22) |
<0.01 |
6.62(3.23-13.59) |
<0.01 |
N3b |
22.62(10.30-49.69) |
<0.01 |
16.79(7.21-39.08) |
<0.01 |
M stage |
||||
M0 vs M1 |
0.20(0.11-0.35) |
<0.01 |
0.18(0.10-0.34) |
<0.01 |
Retrieved lymph nodes |
||||
≤15 vs >15 |
0.71(0.45-1.12) |
0.142 |
- |
|
Chemotherapy |
||||
Yes vs No |
1.89(1.21-2.95) |
0.005 |
1.52(0.89-2.60) |
0.128 |
NLR |
||||
<1.83vs ≥1.83 |
0.74(0.46-1.18) |
0.203 |
- |
|
MLR |
||||
<0.35 vs ≥0.35 |
0.49(0.31-0.77) |
0.002 |
0.39(0.23-0.65) |
<0.01 |
CRP/Alb |
||||
<0.16 vs ≥0.16 |
0.56(0.35-0.91) |
0.018 |
1.08(0.61-1.91) |
0.796 |
GPS |
||||
0 |
1 |
1 |
||
1 |
1.13(0.52-2.44) |
0.753 |
0.36(0.15-0.89) |
0.027 |
2 |
1.81(1.13-2.90) |
0.014 |
1.53(0.92-2.56) |
0.102 |
Abbreviations: AJCC: American Joint Committee on Cancer; NLR: neutrophil lymphocyte ratio; MLR: monocyte lymphocyte ratio; CRP/Alb: C-reactive protein albumin ratio; GPS: Glasgow Prognostic Score
Comparison of the OS predictive accuracy between the nomogram and present TNM classification
The major differences between the 7th and 8th editions are in the stage IIB and stage III, without any other difference among other stages. As shown in Figure 4, the 7th and 8th AJCC classifications harbored relatively good prognostic discrimination in the majority of population. Nevertheless, the 7th and 8th AJCC classifications failed to discriminate subjects between stages IB and IIA, IIB and IIIA; between stages IB and IIA, IIB and IIIA, IIIC and IV, respectively.
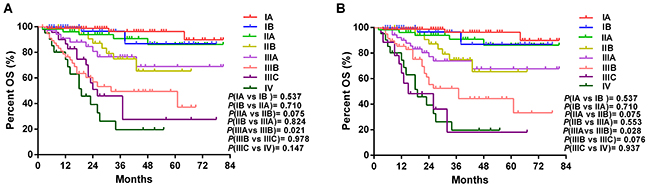
Figure 4: Comparative survival analysis on discriminatory ability and accuracy. (A), survival curves of patients according to 7th AJCC TNM staging system. (B), survival curves of patients according to 8th AJCC TNM staging system. The significance of difference between survival curves were calculated by the log-rank test.
When compared with the 7th and 8th editions TNM classification, the nomogram displayed better survival predicting value in both sets. The C-index of the nomogram (0.83) was higher than that in the 7th (0.78) and 8th editions TNM staging systems (0.80) in training set. Consistently, the C-index of the 7th (0.78) and 8th editions TNM staging systems (0.79) was lower than that of the nomogram (0.83) in validation set. The ROC curve revealed higher sensitivity and specificity for OS prediction at 3- and 5-year of follow-up in both cohorts (Figure 5). Collectively, the above-described outcomes indicate a better performance of the nomogram compared to the AJCC TNM classification in OS prediction in GC patients undergoing R0 resection.
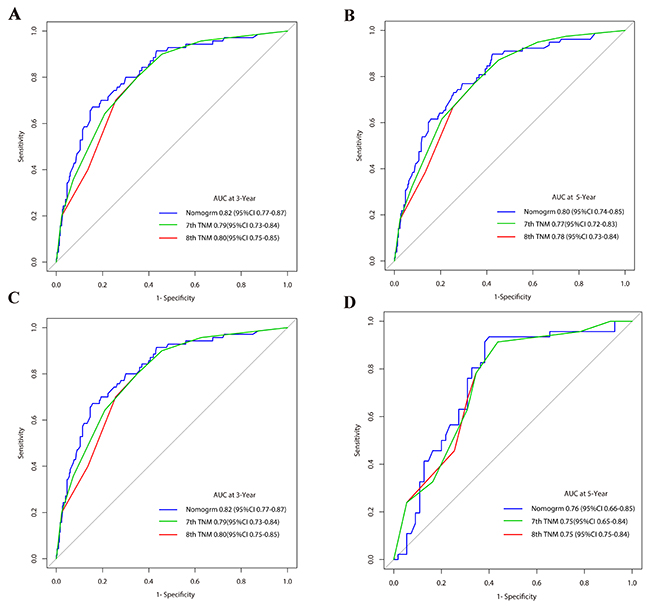
Figure 5: Validation of nomogram for 3-year and 5-year OS of patients with gastric cancer undergoing R0 resection. Time-dependent receiver operating characteristic (ROC) curves by nomogram, 7th AJCC-TNM staging system and 8th AJCC-TNM staging system for 3-year (A) and 5-year (B) OS in the primary cohort; ROC curves by nomogram, 7th AJCC-TNM staging system and 8th AJCC-TNM staging system for 3-year (C) and 5-year (D) OS in the validation cohort.
DISCUSSION
SIR has been increasingly demonstrated to be critically involved in tumorigenesis and tumor progression [20]. Cancer related inflammation is capable of reducing the antitumor activity of the host via recruitment of immunosuppressive cells, including regulatory T cells (Treg) [21] and myeloid-derived suppressor cells (MDSC) [22]. Diverse cytokines as well as chemokines in the tumor microenvironment make a contribution to tumor progression and metastasis [23]. Inflammation-based prognostic scores, such as GPS, NLR, combination of platelet count and neutrophil-lymphocyte ratio (COP-NLR), and LMR harbor prognostic significance in a series of malignancies, including GC [14, 24–26]. Notably, GPS, has been prevalently demonstrated with prognostic significance in GC, which is considered as an inflammation-based prognostic score on the basis of serum CRP and Alb levels [18, 27]. Moreover, NLR, a ratio of neutrophil to lymphocyte counts, has been revealed to be a potential independent prognostic indicator in GC [16]. Due to the absence of generally-applied prognostic model for GC subjects undergoing R0 resection, herein, we aimed at assessing the prognosis of GC subjects on the basis of inflammatory response biomarkers, followed by establishment of a nomogram for more accurate prediction.
In this research, there was a significant correlation of pre-operative MLR, CRP/Alb and GPS in the peripheral blood with OS in GC subjects. The Pre-operative MLR as well as GPS scores were independent prognostic factors. Despite the previously-reported prognostic significance of NLR NLR, however, failed to serve independent prognostic marker in our study. This phenomenon might be due the retrospective nature of this study, leading to a potential selection bias when collecting information.
Despite the significant role of single serum marker for the prognosis of tumor patients, it is insufficient for survival prediction in a clinical set. A series of combined factors in a single index is likely to enhance the predictive potential. Among them, nomogram, a combination of clinicopathological features, could enhance personalized survival prediction [12, 29]. In this research, on the basis of certain clinical characteristics and inflammatory response biomarkers, a nomogram was established for survival prediction in training and validation sets of GC subjects, which accurately predicted the 3- and 5-year OS, as indicated by calibration curves in training and validation sets. In addition, as shown by Harrell’s c-indexes and the ROC curve, this nomogram harbored significantly better capacity of OS prediction, and higher sensitivity and specificity for 3- and 5-year OS prediction than the 7th or 8th TNM classification, respectively.
In spite of the relatively good precision of this nomogram in survival prediction, there existed certain limitations in this study. To begin with, the establishment of this nomogram was only based on a single Chinese institution. Secondly, due to the retrospective nature of study, selection bias might occur when collecting data. The last but not least, in previous studies, the reported thresholds were inconsistent, which were employed in the definition of increased inflammation-based prognostic scores. To this end, large, multi-center and prospective studies are required for further validation.
Taken together, a novel nomogram integrating systemic inflammation scores, was established and internally validated for accurate prediction of 3- and 5-year OS of GC. This newly-established nomogram harbored a better discriminative ability compared to the 7th and 8th TNM staging system, which estimated personalized risk for GC subjects as well as. Further researches are warranted to assess the application of this nomogram in other patient groups.
MATERIALS AND METHODS
Patients
Between January 2010 and December 2016, clinic-pathological data from 370 cases of newly diagnosed gastric adenocarcinoma patients who underwent R0 surgical resection at the Third Affiliated Hospital of Soochow University were analyzed retrospectively. For nomogram construction and validation, all enrolled subjects were assigned to the training cohort (n=370), one third of whom were assigned to the validation cohort (n=101). Exclusion criteria included severe comorbidities, previous surgical history due to GC, lymphadenectomy not using D2, gastric stump cancer, R1 or R2 resection, preoperative radiotherapy, and/or chemotherapy. Patient demographics, surgical features, tumor characteristics as well as the number of resected and metastatic lymph nodes were collected. Patients were staged by the 7th and 8th editions of AJCC TNM classification. After collection of peripheral blood from each subject prior to surgery, neutrophils, lymphocytes, monocyte counts, serum CRP as well as Alb levels were examined. The definition and calculation of the inflammation-based prognostic scores in this study were shown in the following: (1) GPS, subjects with CRP >10 mg/L and albumin <35 g/L were given 2 scores; subjects with CRP > 10 mg/L or albumin <35 g/L were given 1 score; and subjects with both CRP <10 mg/L and albumin>35 g/L were given 0 score. (2) Optimal cutoff values, such as NLR (NLR<1.83, NLR≥1.83), MLR (MLR<0.35, MLR≥0.35) and CRP/Alb (CRP/Alb<0.16, CRP/Alb≥0.16) were detected via X-tile software (https://medicine.yale.edu/lab/rimm/research/software.aspx) [28].
Follow-Up
Follow-up was regularly conducted on each subject every three months for the first two years, every six months for the next three years, and annually thereafter. All patients received physical exmination, laboratory, imaging, as well as endoscopy examination to evaluate whether there was any relapse or metastasis. The last follow-up of survivors was carried out at the end of December 2016. Phone calls and regular mail represented two approaches of follow-up. The observation time was defined as the time from the surgical date to last follow-up or death. Survivors were assessed by the last follow-up. The median follow-up was 24.5 months (ranging from 2 to 81 months). All subjects signed provided informed consent. The study was carried out according to the Declaration of Helsinki, and gained approval from the ethics committee of the Third Affiliated Hospital of Soochow University.
Statistical analysis
SPSS 17.0 for windows (SPSS, Chicago, IL) as well as R software version 3.2.0 (http://www.r-project.org/) with Hmisc, rms, and survival ROC packages were utilized for statistical analysis. Overall survival (OS) was defined as the time from surgery to death or the last follow-up date. Kaplan–Meier (KM) method was employed to generate survival curves, followed by comparison by the log-rank test. The variables were selected based on a priori clinical hypotheses, which had been shown to be related to survival in a previous study, hence, there these variables were enrolled into prognostic characteristics. These factors included gender, age, tumor length, degree of differentiation, location, retrieved lymph nodes, TNM stage, chemotherapy, type of gastrectomy, NLR, MLR, CRP/Alb and GPS. All variables with P<0.05 in univariate analyses were further included in multivariate Cox’s proportional hazards model, based on which, the nomogram was established. A backward stepdown selection process with the AIC was used to select the final model. Both discrimination and calibration were examined to fully assess the performance of nomogram. Specifically, time-dependent receiver operating characteristics (ROC) curve as well as C-index were employed to compare the discrimination ability of OS among different models. Confidence intervals (CIs) were obtained by creating 1000 bootstrap samples from the entire dataset and replicating the estimation process. A larger C-index indicated the more accuracy of the prognostic prediction [29]. During nomogram validation, the total points of every subject of validation set were calculated in line with established nomogram, followed by Cox regression integrating the total points as a factor, as well as subsequent C-index and calibration curve on the basis of the regression analysis. Nomogram was constructed and further validated according to relevant guide. P≤0.05 was considered to be statistically significant unless otherwise specified.
ACKNOWLEDGMENTS
This study was funded by National Natural Science Foundation of China (No. 81171653, 81301960, 81302047, 81402518), Natural Science Foundation of Jiangsu Province (BK2011246, BK2011247, BK20130243), the project of Six Batch of Major Talent Summit (BRA2010037), Society Development Plans, Department of Science and Technology Changzhou (CS20102020, CZ20110024, CE20125026, CJ20112020, CJ20130010, CJ20140039), Youth Talent project of Changzhou Health Development Planning Commission (QN201703, QN201722) as well as the Innovative Talents Training Project of Changzhou Health Bureau.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87-108.
2. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66:115-132.
3. Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016; 388:2654-2664.
4. Sano T, Coit DG, Kim HH, Roviello F, Kassab P, Wittekind C, Yamamoto Y, Ohashi Y. Proposal of a new stage grouping of gastric cancer for TNM classification: international gastric cancer association staging project. Gastric Cancer. 2017; 20:217-225.
5. Liu J, Geng Q, Chen S, Liu X, Kong P, Zhou Z, Zhan Y, Xu D. Nomogram based on systemic inflammatory response markers predicting the survival of patients with resectable gastric cancer after D2 gastrectomy. Oncotarget. 2016; 7:37556-37565. https://doi.org/10.18632/oncotarget.8788.
6. Chen S, Rao H, Liu J, Geng Q, Guo J, Kong P, Li S, Liu X, Sun X, Zhan Y, Xu D. Lymph nodes ratio based nomogram predicts survival of resectable gastric cancer regardless of the number of examined lymph nodes. Oncotarget. 2017; 8:45585-45596. https://doi.org/10.18632/oncotarget.17276.
7. Tang LQ, Li CF, Li J, Chen WH, Chen QY, Yuan LX, Lai XP, He Y, Xu YX, Hu DP, Wen SH, Peng YT, Zhang L, et al. Establishment and validation of prognostic nomograms for endemic nasopharyngeal carcinoma. J Natl Cancer Inst. 2015; 108:djv291.
8. Yang Y, Zhang YJ, Zhu Y, Cao JZ, Yuan ZY, Xu LM, Wu JX, Wang W, Wu T, Lu B, Zhu SY, Qian LT, Zhang FQ, et al. Prognostic nomogram for overall survival in previously untreated patients with extranodal NK/T-cell lymphoma, nasal-type: a multicenter study. Leukemia. 2015; 29:1571-1577.
9. Shao Y, Ning Z, Chen J, Geng Y, Gu W, Huang J, Pei H, Shen Y, Jiang J. Prognostic nomogram integrated systemic inflammation score for patients with esophageal squamous cell carcinoma undergoing radical esophagectomy. Sci Rep. 2015; 5:18811.
10. Liang W, Zhang L, Jiang G, Wang Q, Liu L, Liu D, Wang Z, Zhu Z, Deng Q, Xiong X, Shao W, Shi X, He J. Development and validation of a nomogram for predicting survival in patients with resected non-small-cell lung cancer. J Clin Oncol. 2015; 33:861-869.
11. Wang Y, Li J, Xia Y, Gong R, Wang K, Yan Z, Wan X, Liu G, Wu D, Shi L, Lau W, Wu M, Shen F. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin Oncol. 2013; 31:1188-1195.
12. Han DS, Suh YS, Kong SH, Lee HJ, Choi Y, Aikou S, Sano T, Park BJ, Kim WH, Yang HK. Nomogram predicting long-term survival after d2 gastrectomy for gastric cancer. J Clin Oncol. 2012; 30:3834-3840.
13. Liu JS, Huang Y, Yang X, Feng JF. A nomogram to predict prognostic values of various inflammatory biomarkers in patients with esophageal squamous cell carcinoma. Am J Cancer Res. 2015; 5:2180-2189.
14. Gu L, Ma X, Li H, Chen L, Xie Y, Zhao C, Luo G, Zhang X. Prognostic value of preoperative inflammatory response biomarkers in patients with sarcomatoid renal cell carcinoma and the establishment of a nomogram. Sci Rep. 2016; 6:23846.
15. Liu X, Sun X, Liu J, Kong P, Chen S, Zhan Y, Xu D. Preoperative C-reactive protein/albumin ratio predicts prognosis of patients after curative resection for gastric cancer. Transl Oncol. 2015; 8:339-345.
16. Jin H, Sun J, Zhu K, Liu X, Zhang Q, Shen Q, Gao Y, Yu J. The prognostic value of neutrophil-lymphocyte ratio is superior to derived neutrophil-lymphocyte ratio in advanced gastric cancer treated with preoperative chemotherapy and sequential R0 resection: a 5-year follow-up. Onco Targets Ther 2017; 10:2655–64.
17. Zhou X, Du Y, Xu J, Huang Z, Qiu T, Wang X, Qian J, Zhu W, Liu P. The preoperative lymphocyte to monocyte ratio predicts clinical outcomes in patients with stage II/III gastric cancer. Tumour Biol. 2014; 35:11659-11666.
18. Jiang X, Hiki N, Nunobe S, Kumagai K, Kubota T, Aikou S, Sano T, Yamaguchi T. Prognostic importance of the inflammation-based Glasgow prognostic score in patients with gastric cancer. Br J Cancer. 2012; 107:275-279.
19. Proctor MJ, Horgan PG, Talwar D, Fletcher CD, Morrison DS, McMillan DC. Optimization of the systemic inflammation-based Glasgow prognostic score: a Glasgow Inflammation Outcome Study. Cancer. 2013; 119:2325-2332.
20. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011; 144:646-674.
21. Brimnes MK, Vangsted AJ, Knudsen LM, Gimsing P, Gang AO, Johnsen HE, Svane IM. Increased level of both CD4+FOXP3+ regulatory T cells and CD14+HLA-DR(-)/low myeloid-derived suppressor cells and decreased level of dendritic cells in patients with multiple myeloma. Scand J Immunol. 2010; 72:540-547.
22. Wang G, Lu X, Dey P, Deng P, Wu CC, Jiang S, Fang Z, Zhao K, Konaparthi R, Hua S, Zhang J, Li-Ning-Tapia EM, Kapoor A, et al. Targeting YAP-dependent MDSC infiltration impairs tumor progression. Cancer Discov. 2016; 6:80-95.
23. Lippitz BE. Cytokine patterns in patients with cancer: a systematic review. Lancet Oncol. 2013; 14:e218-228.
24. Lorente D, Mateo J, Templeton AJ, Zafeiriou Z, Bianchini D, Ferraldeschi R, Bahl A, Shen L, Su Z, Sartor O, de Bono JS. Baseline neutrophil-lymphocyte ratio (NLR) is associated with survival and response to treatment with second-line chemotherapy for advanced prostate cancer independent of baseline steroid use. Ann Oncol. 2015; 26:750-755.
25. Fan H, Shao ZY, Xiao YY, Xie ZH, Chen W, Xie H, Qin GY, Zhao NQ. Comparison of the Glasgow Prognostic Score (GPS) and the modified Glasgow Prognostic Score (mGPS) in evaluating the prognosis of patients with operable and inoperable non-small cell lung cancer. J Cancer Res Clin Oncol. 2016; 142:1285-1297.
26. Zhang H, Zhang L, Zhu K, Shi B, Yin Y, Zhu J, Yue D, Zhang B, Wang C. Prognostic significance of combination of preoperative platelet count and neutrophil-lymphocyte ratio (COP-NLR) in patients with non-small cell lung cancer: based on a large cohort study. PLoS One. 2015; 10:e0126496.
27. Takeno S, Hashimoto T, Shibata R, Maki K, Shiwaku H, Yamana I, Yamashita R, Yamashita Y. The high-sensitivity modified Glasgow prognostic score is superior to the modified Glasgow prognostic score as a prognostic predictor in patients with resectable gastric cancer. Oncology. 2014; 87:205-214.
28. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015; 16:e173–80.
29. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008; 26:1364-1370.