
INTRODUCTION
Triple negative breast cancer (TNBC) includes a heterogeneous subgroup of tumors accounting for approximately 15-20% of all breast cancers. TNBC is clinically defined by the absence of expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) amplification/overexpression. TNBC presents a more aggressive natural history and worse disease-specific outcomes than other breast cancer subtypes. Anthracycline and taxane-based chemotherapy has been traditionally the mainstay of therapy for TNBC patients. Nevertheless, platinum-based chemotherapy, with a DNA-damaging mechanism of action, has been incorporated into the neoadjuvant and metastatic settings. Patients with TNBC do not benefit from targeted therapies such as endocrine therapy or trastuzumab, and no appropriate molecular targets have been identified yet [1, 2].
Neoadjuvant chemotherapy has been historically used to downstage unresectable tumors for better loco-regional control and higher conservative surgery rate. The neoadjuvant approach also represents an excellent in vivo test of tumors´ biological sensitivity and of drugs´ clinical efficacy. Therefore, it facilitates cancer research and works towards personalized medicine [3, 4]. After receiving neoadjuvant chemotherapy, about 30% of TNBC patients present a complete absence of residual invasive tumor or pathologic complete response (pCR). Achieving a pCR improves these patients´ prognoses to the point that their disease-free survival and overall survival are similar to patients with less aggressive tumors. However, TNBC patients with residual disease after chemotherapy have worse survival and prognosis than those non-triple negative [5-7]. In TNBC, pCR is therefore considered a potential surrogate marker for survival [7].
Gene expression analysis studies have contributed to unveil TNBC heterogeneity by demonstrating that it is composed of all the intrinsic subtypes, being basal-like the most common subtype (70%) [8]. Thus, not all triple negative are basal-like by gene expression and not all basal-like are triple negative by immunohistochemistry. Recently, Lehmann and colleagues performed a more thorough dissection of TNBC into 7 distinct subtypes based on gene expression profiling. This classification included 6 stable subtypes consisting in: two basal-like (BL1 and BL2), an immunomodulatory (IM), a mesenchymal (M), a mesenchymal stem-like (MSL), and a luminal androgen receptor (LAR) subtype; and an unstable (UNS) subtype. These subtypes were reproduced and pharmacologically targeted in breast cancer cell lines as proof of concept that they can inform therapy selection [9]. However, the clinical relevance of the subtyping defined by Lehmann et al. is still unclear and more research is needed to clarify its impact on TNBC treatment decisions.
We believe there is a need for proper validation of the value of TNBC subtyping regarding response to treatment and survival outcome. Thus, a first highly valuable step would be testing how Lehmann´s classification predicts tumor pCR in the neoadjuvant setting. The main aim of this study was to assess the clinical relevance of these 7 molecular subtypes by ascertaining their correlation with pCR, as a surrogate marker for overall survival, in a cohort of 125 TNBC patients treated with anthracyclines and/or taxanes +/- carboplatin in the neoadjuvant setting. In addition, we evaluated the activity of platinum salts in BL subtypes, given that drugs with DNA-damaging mechanisms of action have proven to be effective in tumors with DNA repair defects that characterize these subtypes [9].
RESULTS
Characteristics of the TNBC population
Patients’ clinicopathological characteristics in the global population (N=125) are shown in Table 1. Patients were mainly pre-menopausal (56%), with positive lymph nodes (59%), high histological grade (63% had grade 3) and high proliferation (median Ki-67 index of 65%, range 5-100%). Close to a third of the patients (27%) received carboplatin in the global population, being this percentage substantially higher in patients from the GEICAM/2006-03 clinical trial (56%). The pCR rate in the global population was 37% although it was unevenly distributed across Lehmann subtypes.
Table 1: Patients’ characteristics
Characteristics |
N (%) |
|---|---|
Age at diagnosis (years) |
|
Median |
48 |
Range |
29-76 |
Tumor size (cm) |
|
<2 |
9 (7.2%) |
2-5 |
90 (72%) |
>5 |
24 (19.2%) |
NA |
2 (1.6%) |
Lymph node status |
|
N0 |
38 (30.4%) |
N+ |
74 (59.2%) |
NA |
13 (10.4%) |
Histological grade |
|
1 |
3 (2.4%) |
2 |
28 (22.4%) |
3 |
79 (63.2%) |
NA |
15 (12%) |
Ki-67 (%) |
|
≤50 |
39 (31.2%) |
>50 |
83 (66.4%) |
NA |
3 (2.4%) |
Intrinsic subtypes |
|
Basal |
104 (83.2%) |
Non-basal |
6 (4.8%) |
NA |
15 (12%) |
Lehmann subtypes |
|
BL1 |
17 (13.6%) |
BL2 |
15 (12%) |
M |
22 (17.6%) |
MSL |
9 (7.2%) |
IM |
25 (20%) |
LAR |
14 (11.2%) |
UNS |
17 (13.6%) |
NA |
6 (4.8%) |
Treatment |
|
A and/or T |
91 (72.8%) |
A+T+Cb |
34 (27.2%) |
pCR |
|
Yes |
46 (36.8%) |
No |
79 (63.2%) |
Abbreviations: N0, No node involvement; N+, node involvement; NA, not available; A, anthracyclines; T, taxanes; Cb, carboplatin.
TNBC subtyping and clinicopathological variables
Lehmann subtypes
Of the 125 TNBC patients with evaluable pathologic response after neoadjuvant chemotherapy, RNA with sufficient quantity and quality for Lehmann subtyping was collected from 119 (95%) of them. Of these, 102 (86%) were classified as stable and 17 (14%) as unstable (UNS) (Table 1). A more detailed description of the clinicopathological variables in every Lehmann subtype is shown in Table 2. Ki-67 index (dichotomized using a cut-off >50%) was associated with Lehmann subtyping (p=0.002). BL1 samples had the highest proliferation rates (88.2% of BL1 patients vs. 63.7% of patients with other subtypes had Ki-67>50%, p=0.02) and LAR the lowest (71% of LAR patients vs. 27% of patients with other subtypes had Ki-67≤50%, p=0.002).
Table 2: Patients’ characteristics by Lehmann subtype, N (%) and p-values of the comparison between all subtypes and all subtypes except MSL
Characteristics |
BL1(N=17) |
BL2(N=15) |
M(N=22) |
MSL(N=9) |
IM(N=25) |
LAR(N=14) |
UNS(N=17) |
p all subtypes |
p excluding MSL |
|---|---|---|---|---|---|---|---|---|---|
Age (years) |
|||||||||
<50 |
10 (58.8%) |
9 (60%) |
12 (54.5%) |
3 (33.3%) |
20 (80%) |
6 (42.9%) |
10 (58.8%) |
||
≥50 |
7 (41.2%) |
6 (40%) |
10 (45.5%) |
6 (66.7%) |
5 (20%) |
8 (57.1%) |
7 (41.2%) |
0.1791 |
0.2686 |
Tumor size (cm) |
|||||||||
<2 |
3 (17.6%) |
0 |
3 (13.6%) |
0 |
2 (8%) |
0 |
1 (5.9%) |
||
2-5 |
13 (76.5%) |
13 (86.7%) |
16 (72.7%) |
7 (77.8%) |
17 (68%) |
9 (64.3%) |
11 (64.7%) |
||
>5 |
1 (5.9%) |
2 (13.3%) |
2 (9.1%) |
2 (22.2%) |
6 (24%) |
4 (28.6%) |
5 (29.4%) |
0.5033 |
0.3979 |
NA |
0 |
0 |
1 (4.6%) |
0 |
0 |
1 (7.1%) |
0 |
||
Lymph node status |
|||||||||
N0 |
8 (47.1%) |
4 (26.7%) |
5 (22.7%) |
4 (44.4%) |
7 (28%) |
3 (21.4%) |
6 (35.3%) |
||
N+ |
8 (47.1%) |
8 (53.3%) |
12 (54.6%) |
5 (55.6%) |
16 (64%) |
10 (71.4%) |
10 (58.8%) |
||
NA |
1 (5.8%) |
3 (20%) |
5 (22.7%) |
0 |
2 (8%) |
1 (7.2%) |
1 (5.9%) |
0.7903 |
0.7449 |
Histological grade |
|||||||||
1 |
0 |
1 (6.7%) |
0 |
0 |
0 |
1 (7.1%) |
1 (5.9%) |
||
2 |
5 (29.4%) |
0 |
7 (31.8%) |
2 (22.2%) |
5 (20%) |
5 (35.7%) |
3 (17.6%) |
||
3 |
10 (58.8%) |
13 (86.6%) |
11 (50%) |
4 (44.5%) |
18 (72%) |
7 (50.1%) |
11 (64.7%) |
||
NA |
2 (11.8%) |
1 (6.7%) |
4 (18.2%) |
3 (33.3%) |
2 (8%) |
1 (7.1%) |
2 (11.8%) |
0.1438 |
0.0912 |
Ki-67 (%) |
|||||||||
≤50 |
1 (5.9%) |
4 (26.7%) |
9 (40.9%) |
5 (55.6%) |
4 (16%) |
10 (71.4%) |
5 (29.4%) |
||
>50 |
15 (88.2%) |
11 (73.3%) |
13 (59.1%) |
4 (44.4%) |
21 (84%) |
4 (28.6%) |
12 (70.6%) |
||
NA |
1 (5.9%) |
0 |
0 |
0 |
0 |
0 |
0 |
0.0015* |
<0.001* |
Intrinsic subtypes |
|||||||||
basal |
16 (94.1%) |
15 (100%) |
20 (90.9%) |
8 (88.9%) |
25 (100%) |
5 (35.7%) |
12 (70.6%) |
||
non-basal |
0 |
0 |
0 |
0 |
0 |
5 (35.7%) |
1 (5.9%) |
||
NA |
1 (5.9%) |
0 |
2 (9.1%) |
1 (11.1%) |
0 |
4 (28.6%) |
4 (23.5%) |
<0.001* |
<0.001* |
Treatment |
|||||||||
A and/or T |
12 (70.6%) |
12 (80%) |
18 (81.8%) |
7 (77.8%) |
17 (68%) |
10 (71.4%) |
12 (70.6%) |
||
A+T+Cb |
5 (29.4%) |
3 (20%) |
4 (18.2%) |
2 (22.2%) |
8 (32%) |
4 (28.6%) |
5 (29.4%) |
0.9447 |
0.8916 |
pCR |
|||||||||
Yes |
8 (47.1%) |
7 (46.7%) |
9 (40.9%) |
3 (33.3%) |
10 (40%) |
2 (14.3%) |
7 (41.2%) |
||
No |
9 (52.9%) |
8 (53.3%) |
13 (59.1%) |
6 (66.7%) |
15 (60%) |
12 (85.7%) |
10 (58.8%) |
0.5714 |
0.4539 |
Abbreviations: NA, not available; N0, No node involvement, N+, node involvement. NA, not available A, anthracyclines; T, taxanes; Cb, carboplatin.
* p≤0.05.
Intrinsic subtypes
We further classified 110 (88%) of the tumor samples into intrinsic subtypes. Of these, 104 (94.5%) were classified as basal-like and 6 (5.4%) as non-basal-like (Table 1). Non-basal-like samples included 5 HER2-enriched and 1 luminal A; due to this low number we combined these 6 samples into a group of non-basal-like samples for further analyses. As highlighted in the methodology, 36% of the tumors in this study were collected as part of the GEICAM/2006-03 trial, which eligibility criteria included the core basal definition, a more restrictive triple negative definition (triple negative status plus EGFR-positive and/or CK5/6-positive). The fact that all these samples were already basal by immunohistochemistry could have caused an overrepresentation of basal-like tumors compared to the triple negative-only definition. However, we observed a comparable proportion of samples classified as basal-like when excluding this subset of core basal samples defined by immunohistochemistry (94.5% of basal-like samples in the global cohort vs. 92.2% in the triple negative-only cohort, p=0.56).
Correlation between Lehmann and intrinsic subtyping
We found a strong concordance between Lehmann and intrinsic subtyping (p<0.001, Table 2) mainly because the only stable group with non-basal-like samples is the LAR subtype. The distribution of Lehmann subtypes into basal-like and non-basal-like intrinsic subtypes is shown in Figure 1. Of the 5 LAR samples classified as non-basal-like, 4 were HER2-enriched and 1 was luminal A. We had enough tumor tissue to successfully determine the expression of the androgen receptor (AR) in the luminal A and three out of four HER2-enriched tumors; all overexpressed AR and were histopathologically consistent with apocrine carcinomas.
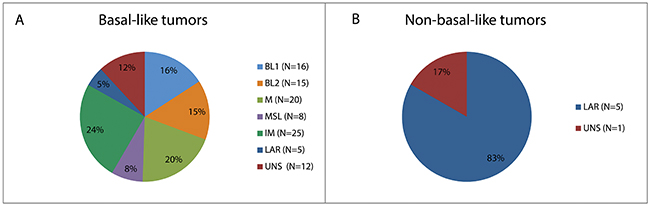
Figure 1: Distribution of Lehmann subtypes within intrinsic subtypes. (A) Distribution of Lehmann subtypes in molecular basal-like tumors. (B) Distribution of Lehmann subtypes in molecular non-basal-like tumors.
Pathological complete response to different neoadjuvant treatments
We first analyzed the association between the different clinicopathological variables and the pathological complete response (pCR) to neoadjuvant treatment in the global sample. High expression of Ki-67 (using a cut-off >50%, p=0.037) and bigger clinical tumor size (≤2cm vs. >2cm, p=0.024) were associated with higher number of pCRs achieved. Clinical tumor size was the only variable that remained associated with pCR when performing a multivariate analysis (p=0.002).
pCR to overall neoadjuvant treatment by Lehmann subtype
Next, we analyzed the pCR rates achieved by Lehmann subtype (see Figure 2). As recently Prat and colleagues highlighted that Lehmann subtyping ignores TNBC samples that are highly contaminated with normal breast tissue, which are mostly classified as MSL [10], we performed all analyses with and without the MSL group to avoid missing relevant associations between clinicopathological variables and Lehmann subtypes.
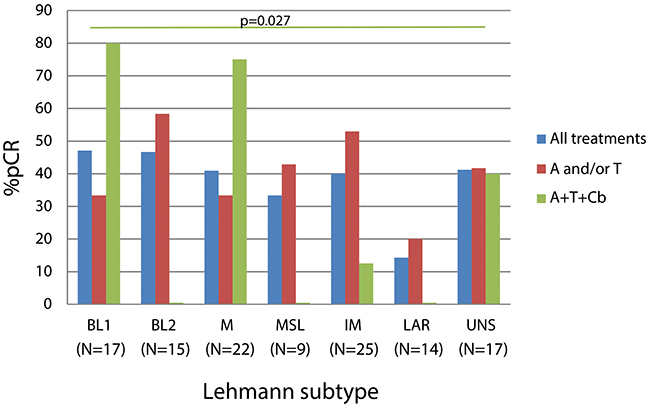
Figure 2: Percentage of pCR associated to the different Lehmann subtypes by treatment. The green horizontal line represents the comparison of the percentage of pCR to sequential anthracyclines and taxanes plus carboplatin of BL1 versus the rest of patients and its associated p-value. The number of patients receiving every treatment within each Lehmann subtype can be found at Table 2. Abbreviations: A, anthracyclines; T, taxanes; Cb, carboplatin.
We found no statistically significant association between Lehmann subtypes and pCR to overall neoadjuvant treatment (p=0.571) in spite of the wide range of pCR observed (from 47.1% in BL1 to 14.3% in LAR). LAR patients were the most chemoresistant (14.3% of pCR in LAR vs. 41.9% in the remaining subtypes combined, p=0.077) and when excluding MSL samples, this difference in response appeared to be more pronounced (14.3% of pCR in LAR patients vs. 42.7% in the remaining groups except MSL, p=0.046).
pCR to the different treatments in overall sample and by Lehmann subtype
We found no differences in pCR rates in the global population (without subtyping) when comparing patients treated with and without carboplatin (40.9% vs. 32.3% of pCR, respectively; p=0.521).
When analyzing the pCR response to the different treatments received by Lehmann subtype, we did not observe a difference in pCR rates to standard chemotherapy (sequential anthracyclines and/or taxanes) by Lehmann subtypes (p=0.556). When comparing the pCR rates in patients treated with carboplatin in each of the Lehmann subtypes, we observed that patients with BL1 tumors were the most benefited of the addition of carboplatin (80% of pCR in BL1 patients vs. 23% of pCR in the remaining groups, p=0.027).
DISCUSSION
Triple negative breast cancer (TNBC) is a commonly used umbrella term for a histologic group of tumors which, from a molecular perspective, are vastly heterogeneous. In fact, TNBC includes a wide range of entities differing in biology and response to chemotherapy and targeted therapies, and, thus, leading to different clinical outcomes. Recently, several TNBC classifications have been published illustrating the existing inconsistencies both in the definition of disease subgroups and of their corresponding clinical outcomes [9, 11-13]; only the subtypes termed as LAR appear to be consistent across all the studies, though it is unclear whether these classifications are predictive of treatment efficacy.
In this report, we analyzed a combined dataset of TNBC patients treated with anthracyclines and/or taxanes +/- carboplatin in the neoadjuvant setting. First, we classified them into the TNBC Lehmann subtypes and evaluated their clinicopathological characteristics and, second, we explored the chemosensitivity of these subtypes to the different neoadjuvant treatments administrated. To our knowledge, this is the first study evaluating the prognostic role of Lehmann TNBC subtypes in the neoadjuvant setting of patients treated with and without platinum salts.
Based on our results, LAR is the least proliferative tumor subtype and the most chemoresistant one. Despite its significantly lower response to neoadjuvant chemotherapy in comparison to the other subtypes, LAR has been associated with a favorable prognosis when defined by immunohistochemistry as AR-positive [14-16]. This may be, in part, because LAR is the only subtype including non-basal-like tumors [17, 18] which could explain the low proliferation and pCR rates observed in our study. However, there are controversial results in the literature when LAR is defined by gene-expression, having the best [19, 20] or worse prognosis [9, 21] within TNBC and when analyzing all breast cancer subtypes [22]. As expected, our LAR samples expressed AR and were histologically consistent with apocrine carcinomas [23]. Recently published early phase II clinical trials results suggest that antiandrogen therapy may target the AR-positive subset of TNBCs [24-26].
In our study, BL1 subtype appeared to be particularly sensitive to chemotherapy regimens including a platinum agent. This is of major significance because in the past few decades there has been considerable interest in platinum salts as treatment for TNBC given that homologous recombination deficiency (HRD) sensitizes tumor cells to these agents inducing cell death. Although, results from phase II studies involving unselected TNBC patients in the neoadjuvant setting have been conflicting [27-29], TNBC tumors harboring a high HRD score seem to benefit from platinum-based therapy [30].
The results of this study should be interpreted in the context of its limitations. First, the actual number of samples analyzed under each Lehmann subtype is limiting; second, we used formalin-fixed paraffin-embedded (FFPE) samples for gene expression analysis, which could present differences when compared to analysis performed in fresh/frozen tissue; and, third, patients did not receive homogeneous neoadjuvant treatments, although all patients did receive anthracyclines and/or taxanes +/- carboplatin regimes.
In conclusion, our results confirm the high genetic diversity within TNBC tumors, although, rather than falling into discreet categories, TNBC disease may be considered a spectrum of tumors with varying clinically-relevant characteristics. On one extreme of this spectrum, we would have BL1 tumors, a highly proliferative subtype with its likely deficiencies in HRD resulting in a high pCR to platinum salts-based therapies. On the other side, we would find LAR, a tumor subtype characterized by a low proliferation and a low response to standard chemotherapy. In between, we would find patients with TNBC tumors that cannot be classified into any subgroup further than the standard definition of TNBC. These results may have important implications in the design, implementation, and evaluation of future clinical trials aimed at further exploration of the clinical utility of TNBC subtyping.
MATERIALS AND METHODS
Patients and samples
We performed a retrospective analysis on 125 patients with invasive TNBC including 45 (36%) from a randomized phase II trial (GEICAM/2006-03, ClinicalTrials.gov: NCT00432172) with a prospective collection of FFPE tumor samples and associated clinical data, and 80 (64%) patients for whom we had retrospectively collected FFPE tumor samples and data from four collaborating hospitals. GEICAM/2006-03 study was the first to investigate whether adding carboplatin to one of the most commonly used standard chemotherapy combinations (neoadjuvant epirubicin/cyclophosphamide followed by docetaxel) increased the pCR rate in basal-like breast cancer patients. Further information about this trial can be found elsewhere [27].
To be included in this retrospective study, patients had to be over 18-years old females with histologically confirmed invasive TNBC (ER-negative, PR-negative, HER2-negative). All patients received standard neoadjuvant chemotherapy consisting of anthracyclines and/or taxanes with or without carboplatin. Patients included in the study had already undergone surgery during which data on their pathological response was assessed and collected in every collaborating hospital from the restrospective cohort and centrally in the GEICAM cohort. pCR was defined as the absence of invasive carcinoma in the breast and lymph nodes according to the Miller & Payne criteria [31]. Samples were managed and/or provided by the Málaga Hospital-IBIMA Biobank and GEICAM Biobank. All patients participating in the study provided written informed consent and study protocols were approved by the corresponding institutional ethical committees.
Samples processing
Immunohistochemistry
Analyses were performed with FFPE biopsies obtained before neoadjuvant treatment. Immunostaining was performed and assessed in every collaborating hospital using estrogen receptor (ER, Clone SP1), progesterone receptor (PR, Clone Y85), cytokeratin 5/6 (CK5/6, Clone D5/16B4), Ki-67 (Clone SP6) (Master Diagnóstica, Granada, Spain), epidermal growth factor receptor (EGFR, Clone 2-18C9), androgen receptor (AR, Clone AR441), and human epidermal growth factor receptor 2 (HER2, HercepTest) (DakoCytomation, Glostrup, Denmark). Samples from all patients were defined as triple negative by immunohistochemistry as ER-negative, PR-negative, and HER2-negative. AR status was assessed only in the samples classified as non-basal-like by PAM50 in order to evaluate if they were compatible with apocrine carcinomas. ER, PR and AR status were considered negative if <1% of cells stained positively [32]. HER2 status was considered negative if either immunohistochemical results were 0 to +1, or were +2 and FISH results were negative [33]. All GEICAM/2006-03 samples were CK5/6-positive and/or EGFR-positive by immunohistochemistry and therefore defined as core basal [34]. CK5/6 and EGFR tumor immunoreactivity was determined only in the GEICAM cohort and categorized as negative (immunohistochemical score 0), and positive (immunohistochemical score 1-3). Information about Ki-67 was collected as a continuous variable as well as a dichotomized variable defined by a cut-off point of 50% [35].
RNA extraction
Hematoxylin and eosin staining of a slide-mounted tumor section were reviewed, by independent pathologists for the GEICAM and non-GEICAM collections, to identify the area of invasive breast carcinoma. Tumor area was manually macrodissected to obtain an enriched tumor RNA. Extraction and purification was performed with the RNeasy FFPE Kit (Qiagen) from 3-6 sections of 10μm and quality assessment was conducted using a 2100 Bioanalyzer (Agilent Technologies) and a Nanodrop spectrophotometer (Thermo Scientific).
TNBC subtyping
Gene expression analyses to classify samples into 1 of the 4 intrinsic subtypes (luminal A, luminal B, HER2-enriched, basal-like) were performed on an nCounter Analysis System (NanoString Technologies). For further analyses, we grouped samples as basal-like and non-basal-like (luminal A, luminal B and HER2-enriched); as the majority of triple negative breast tumors are basal-like we expected a low number of the remaining subtypes. Samples from the GEICAM/2006-03 clinical trial were profiled using the PAM50 classifier and analyzed by means of a clinical algorithm for subtype prediction [36], discarding samples classified as normal-like. The retrospective collection of patients was classified according the Prosigna assay [37], which includes a proprietary algorithm based on the PAM50 gene signature [38].
RNA processing and microarray analysis performed to classify the samples into Lehmann TNBC subtypes were performed at the Microarray Analysis Service (SAM) core facility from Hospital del Mar Medical Research Institute (IMIM), using exclusively Affymetrix Technology (Affymetrix, Santa Clara, CA). RNA was amplified and labelled using the SensationPlus™ FFPE Amplification and WT Labeling kit. The resulting cDNA was hybridized to the GeneChip® Human Transcriptome Array 2.0. Data were normalized with the Robust Multichip Analysis (RMA) algorithm in the Affymetrix Expression Console (EC, v.1.4.1). Data were annotated in the statistical computing environment R (v.3.2.3) using hg19 human genome built and duplicated genes were mean summarized. Gene expression data are available in the GEO repository (accession GSE106977), at https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE106977. Subtypes were identified with the web-based tool TNBCtype [39].
Statistical analyses
Pearson’s chi-square test was used to perform contingency table and goodness-of-fit tests, and Fisher’s exact test when any of expected values in cells were less than 5. Student’s t-test was also used to test the null hypothesis under the assumption of the two populations having equal means. A logistic regression multivariate analysis was performed, using a stepwise forward and backward selection procedure to select the most important variables of the model based on the Akaike information criterion (AIC). All statistical analyses were conducted in the statistical computing environment R (v. 3.3.1). Because the Lehmann’s MSL subtype can have an overrerpresentation of normal breast tissue [10], we performed all analysis both including and excluding the MSL subtype to avoid missing relevant associations.
Abbreviations
AR Androgen receptor
BL1 Basal-like 1
BL2 Basal-like 2
CK5/6 Cytokeratin 5/6
EGFR Epidermal growth factor receptor
ER Estrogen receptor
FFPE Formalin-fixed paraffin-embedded
HER2 Human epidermal growth factor receptor 2
HRD Homologous recombination deficiency
IM Immunomodulatory
LAR Luminal-androgen receptor
M Mesenchymal
MSL Mesenchymal stem-like
pCR Pathological complete response
PR Progesterone receptor
TNBC Triple negative breast cancer
UNS Unstable.
Author contributions
EA and ASM conceived the study; EA was the lead investigator and the study supervisor; the project was managed by ASM and AS and samples and data were managed by AS, MRCP and RC. AS, MRCP, CEFDS and VdL were involved in sample processing and data acquisition; LV performed the pathology review, JMJ was in charge of statistical analysis. Data was also analyzed and interpreted by AS, MRCP, MA and RC. ASM, AL, JA, JIC, SA, JdlH, YP, CLRT, CL, IZP and MM were involved in sample and data acquisition and management. AS and ASM wrote the first manuscript draft, that underwent major revisions by EC, RC and EA. All authors read and approved the final manuscript.
ACKNOWLEDGMENTS
We gratefully acknowledge the technical advice of Genologica, the technical and data analysis support of the Microarray Analysis Service (SAM) core facility’s team (IMIM), the statistical support of Maribel Casas, the artwork edition of Jose M. Roldán and the language editing and critical revision of the manuscript of Hossana Soler.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
This work was supported by Centro de Investigación Biomédica en Red de Cáncer (CIBERONC) from Instituto de Salud Carlos III (ISCIII) (CB16/12/00241, CB16/12/00471, CB16/12/00481) and by research grants from ISCIII (PI13/00730), Mutua Madrileña 2013 and Sociedad Española de Oncología Médica (SEOM) 2013. The authors acknowledge support through grant TIN2017-88728-C2-1-R from MICINN-SPAIN. Angela Santonja has a predoctoral grant PFIS-ISCIII (FI12/00489).
REFERENCES
1. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P, Narod SA. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007; 13: 4429–34.
2. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010; 363: 1938–48.
3. von Minckwitz G, Loibl S, Maisch A, Untch M. Lessons from the neoadjuvant setting on how best to choose adjuvant therapies. The Breast. 2011; 20: S142–5.
4. Wang-Lopez Q, Chalabi N, Abrial C, Radosevic-Robin N, Durando X, Mouret-Reynier MA, Benmammar KE, Kullab S, Bahadoor M, Chollet P, Penault-Llorca F, Nabholtz JM. Can pathologic complete response (pCR) be used as a surrogate marker of survival after neoadjuvant therapy for breast cancer? Crit Rev Oncol Hematol. 2015; 95: 88–104.
5. Liedtke C, Mazouni C, Hess KR, André F, Tordai A, Mejia JA, Symmans WF, Gonzalez-Angulo AM, Hennessy B, Green M, Cristofanilli M, Hortobagyi GN, Pusztai L. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008; 26: 1275–81.
6. Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, Collichio F, Ollila DW, Sartor CI, Graham ML, Perou CM. The triple negative paradox: primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. 2007; 13: 2329–34.
7. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L, Valagussa P, Swain SM, Prowell T, Loibl S, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014; 384: 164–72.
8. Prat A, Perou CM. Deconstructing the molecular portraits of breast cancer. Mol Oncol. 2011; 5: 5–23.
9. Lehmann BD, Bauer JA, Chen X, Sanders ME, Chakravarthy AB, Shyr Y, Pietenpol JA. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest. 2011; 121: 2750–67.
10. Prat A, Fan C, Fernández A, Hoadley KA, Martinello R, Vidal M, Viladot M, Pineda E, Arance A, Muñoz M, Paré L, Cheang MCU, Adamo B, et al. Response and survival of breast cancer intrinsic subtypes following multi-agent neoadjuvant chemotherapy. BMC Med. 2015; 13: 303.
11. Lehmann BD, Jovanović B, Chen X, Estrada MV., Johnson KN, Shyr Y, Moses HL, Sanders ME, Pietenpol JA. Refinement of triple-negative breast cancer molecular subtypes: implications for neoadjuvant chemotherapy selection. PLoS One. 2016; 11: e0157368.
12. Burstein MD, Tsimelzon A, Poage GM, Covington KR, Contreras A, Fuqua SAW, Savage MI, Osborne CK, Hilsenbeck SG, Chang JC, Mills GB, Lau CC, Brown PH. Comprehensive genomic analysis identifies novel subtypes and targets of triple-negative breast cancer. Clin Cancer Res. 2015; 21: 1688–98.
13. Liu YR, Jiang YZ, Xu XE, Yu KD, Jin X, Hu X, Zuo WJ, Hao S, Wu J, Liu GY, Di GH, Li DQ, He XH, et al. Comprehensive transcriptome analysis identifies novel molecular subtypes and subtype-specific RNAs of triple-negative breast cancer. Breast Cancer Res. 2016; 15: 18–33.
14. Rakha EA, El-Sayed ME, Green AR, Lee AHS, Robertson JF, Ellis IO. Prognostic markers in triple-negative breast cancer. Cancer. 2007; 109: 25–32.
15. Agoff SN, Swanson PE, Linden H, Hawes SE, Lawton TJ. Androgen receptor expression in estrogen receptor-negative breast cancer immunohistochemical, clinical, and prognostic associations. Am J Clin Pathol. 2003; 120: 725–31.
16. Loibl S, Müller BM, von Minckwitz G, Schwabe M, Roller M, Darb-Esfahani S, Ataseven B, du Bois A, Fissler-Eckhoff A, Gerber B, Kulmer U, Alles JU, Mehta K, et al. Androgen receptor expression in primary breast cancer and its predictive and prognostic value in patients treated with neoadjuvant chemotherapy. Breast Cancer Res Treat. 2011; 130: 477–87.
17. Prat A, Lluch A, Albanell J, Barry WT, Fan C, Chacón JI, Parker JS, Calvo L, Plazaola A, Arcusa A, Seguí-Palmer MA, Burgues O, Ribelles N, et al. Predicting response and survival in chemotherapy-treated triple-negative breast cancer. Br J Cancer. 2014; 111: 1532–41.
18. Lehmann BD, Pietenpol JA. Identification and use of biomarkers in treatment strategies for triple-negative breast cancer subtypes. J Pathol. 2014; 232: 142–50.
19. Masuda H, Baggerly KA, Wang Y, Zhang Y, Gonzalez-Angulo AM, Meric-Bernstam F, Valero V, Lehmann BD, Pietenpol JA, Hortobagyi GN, Symmans WF, Ueno NT. Differential response to neoadjuvant chemotherapy among 7 triple-negative breast cancer molecular subtypes. Clin Cancer Res. 2013; 19: 5533–40.
20. Yu KD, Zhu R, Zhan M, Rodriguez AA, Yang W, Wong S, Makris A, Lehmann BD, Chen X, Mayer I, Pietenpol JA, Shao ZM, Symmans WF, Chang JC. Identification of prognosis-relevant subgroups in patients with chemoresistant triple-negative breast cancer. Clin Cancer Res. 2013; 19: 2723–33.
21. Bareche Y, Venet D, Ignatiadis M, Aftimos P, Piccart M, Rothe F, Sotiriou C. Unravelling triple-negative breast cancer molecular heterogeneity using an integrative multiomic analysis. Ann Oncol. 2018; 29:895–902. https://doi.org/10.1093/annonc/mdy024.
22. Guedj M, Marisa L, de Reynies A, Orsetti B, Schiappa R, Bibeau F, MacGrogan G, Lerebours F, Finetti P, Longy M, Bertheau P, Bertrand F, Bonnet F, et al. A refined molecular taxonomy of breast cancer. Oncogene. 2012; 31: 1196–206.
23. Pareja F, Geyer FC, Marchiò C, Burke KA, Weigelt B, Reis-Filho JS. Triple-negative breast cancer: the importance of molecular and histologic subtyping, and recognition of low-grade variants. NPJ Breast Cancer. 2016; 2: 16036.
24. Gucalp A, Tolaney S, Isakoff SJ, Ingle JN, Liu MC, Carey LA, Blackwell K, Rugo H, Nabell L, Forero A, Stearns V, Doane AS, Danso M, et al. Phase II trial of bicalutamide in patients with androgen receptor-positive, estrogen receptor-negative metastatic breast cancer. Clin Cancer Res. 2013; 19: 5505–12.
25. Traina TA, Miller K, Yardley DA, O’Shaughnessy J, Cortes J, Awada A, Kelly CM, Trudeau ME, Schmid P, Gianni L, García-Estevez L, Nanda R, Ademuyiwa FO, et al. Results from a phase 2 study of enzalutamide (ENZA), an androgen receptor (AR) inhibitor, in advanced AR+ triple-negative breast cancer (TNBC). J Clin Oncol. 2015 (Suppl 15); 33:1003.
26. Bonnefoi H, Grellety T, Tredan O, Saghatchian M, Dalenc F, Mailliez A, L’Haridon T, Cottu P, Abadie-Lacourtoisie S, You B, Mousseau M, Dauba J, Del Piano F, et al. A phase II trial of abiraterone acetate plus prednisone in patients with triple-negative androgen receptor positive locally advanced or metastatic breast cancer (UCBG 12-1). Ann Oncol. 2016; 27: 812–8.
27. Alba E, Chacon JI, Lluch A, Anton A, Estevez L, Cirauqui B, Carrasco E, Calvo L, Segui MA, Ribelles N, Alvarez R, Sanchez-Muñoz A, Sanchez R, et al. A randomized phase II trial of platinum salts in basal-like breast cancer patients in the neoadjuvant setting. Results from the GEICAM/2006-03, multicenter study. Breast Cancer Res Treat. 2012; 136: 487–93.
28. von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M, Blohmer JU, Jackisch C, Paepke S, Gerber B, Zahm DM, Kümmel S, Eidtmann H, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol. 2014; 15: 747–56.
29. Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM, Kuzma CS, Pluard TJ, Somlo G, Port ER, Golshan M, Bellon JR, Collyar D, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603. J Clin Oncol. 2015; 33: 13–21.
30. Telli ML, Timms KM, Reid J, Hennessy B, Mills GB, Jensen KC, Szallasi Z, Barry WT, Winer EP, Tung NM, Isakoff SJ, Ryan PD, Greene-Colozzi A, et al. Homologous Recombination Deficiency (HRD) score predicts response to platinum-containing neoadjuvant chemotherapy in patients with triple-negative breast cancer. Clin Cancer Res. 2016; 22: 3764–73.
31. Ogston KN, Miller ID, Payne S, Hutcheon AW, Sarkar TK, Smith I, Schofield A, Heys SD. A new histological grading system to assess response of breast cancers to primary chemotherapy: prognostic significance and survival. Breast. 2003; 12: 320–7.
32. Hammond MEH, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, Fitzgibbons PL, Francis G, Goldstein NS, Hayes M, Hicks DG, Lester S, Love R, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch Pathol Lab Med. 2010; 134: e48–72.
33. Wolff AC, Hammond MEH, Hicks DG, Dowsett M, McShane LM, Allison KH, Allred DC, Bartlett JMS, Bilous M, Fitzgibbons P, Hanna W, Jenkins RB, Mangu PB, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: american society of clinical oncology/college of american pathologists clinical practice guideline update. J Clin Oncol. American Society of Clinical Oncology; 2013; 31: 3997–4013.
34. Nielsen TO, Hsu FD, Jensen K, Cheang M, Karaca G, Hu Z, Hernandez-Boussard T, Livasy C, Cowan D, Dressler L, Akslen LA, Ragaz J, Gown AM, et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res. 2004; 10: 5367–74.
35. Alba E, Lluch A, Ribelles N, Anton-Torres A, Sanchez-Rovira P, Albanell J, Calvo L, Garcia-Asenjo JAL, Palacios J, Chacon JI, Ruiz A, De la Haba-Rodriguez J, Segui-Palmer MA, et al. High proliferation predicts pathological complete response to neoadjuvant chemotherapy in early breast cancer. Oncologist. 2016; 21: 150–5.
36. Parker JS, Mullins M, Cheang MCU, Leung S, Voduc D, Vickery T, Davies S, Fauron C, He X, Hu Z, Quackenbush JF, Stijleman IJ, Palazzo J, et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. J Clin Oncol. 2009; 27: 1160–7.
37. Prosigna [Package Insert]. Seattle, WA: NanoString Technologies, Inc.; 2015. Available from http://prosigna.com/docs/Prosigna_Packet_Insert_US.pdf.
38. Perou CM, Sørlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA, Fluge O, Pergamenschikov A, Williams C, et al. Molecular portraits of human breast tumours. Nature. 2000; 406: 747–52.
39. Chen X, Li J, Gray WH, Lehmann BD, Bauer JA, Shyr Y, Pietenpol JA. TNBCtype: a subtyping tool for triple-negative breast cancer. Cancer Inform. 2012; 11: 147–56.