
INTRODUCTION
Hepatocellular carcinoma (HCC) is the fifth most common cancer and the second most common cause of cancer-related mortality [1]. Portal vein tumor thrombus (PVTT) is a poor prognostic factor of survival as it leads to portal hypertension, tumor spread, liver failure and death [2]. The Barcelona Clinic Liver Cancer (BCLC) group recommended sorafenib as the standard therapy for these patients [3, 4]. In Asian countries, liver resection has been proposed as an option that offers a chance of cure if the lesion is resectable [5, 6]. The optimal treatment for patients with HCC and PVTT remains controversial.
Recently, transarterial chemoembolization (TACE) has become the most popular palliative treatment for patients with unresectable HCC and is no longer considered as an absolute contraindication to patients with HCC with PVTT [7, 8]. Advanced radiotherapies (RT) including three-dimensional conformal radiotherapy (3D-CRT), stereotactic body radiotherapy (SBRT) and intensity-modulated radiotherapy (IMRT), have produced promising results in HCC patients with PVTT [9-11]. The combination of TACE and radiotherapy for HCC patients with PVTT significantly improved survival outcomes when compared with TACE or radiotherapy alone [12-19]. While most of these studies used TACE followed by RT, some applied RT before TACE [17]. In this study, the survival outcomes and adverse events of a cohort of HCC patients with different extent of PVTT underwent TACE either before or after IMRT were compared. In addition, a propensity score matching (PSM) analysis was done to minimize potential bias inherent to this retrospective, nonrandomized study. Independent prognostic factors associated with survival were also investigated.
RESULTS
Study population
Of 164 patients with unresectable HCC with PVTT who underwent combined TACE and IMRT during the study period, 52 patients were excluded because they met the exclusion criteria. Thus, 112 patients (the TACE-RT group, n=76; and the RT-TACE group, n=36) were included in this study. Of these, 75 patients with HCC with PVTT (the TACE-RT group, n=50; the RT-TACE group, n=25) were selected in the propensity score analysis (Figure 1).
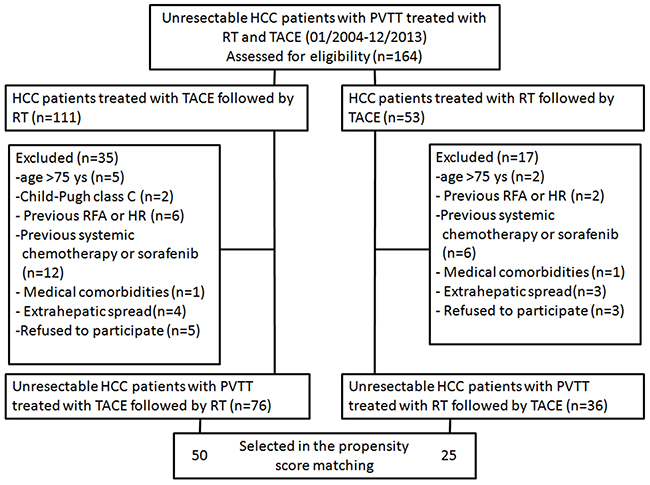
Figure 1: A flow chart of this study. RFA = radiofrequency ablation; HR = hepatic resection.
The two groups showed no significant difference in all the baseline characteristics, which included age, sex, Child-Pugh score, total bilirubin (TBIL), albumin (ALB), alanine aminotransferase (ALT), HBsAg positivity, ascites, AFP level, tumor number, maximum lesion diameter, and extent of PVTT before and after propensity score matching (Table 1).
Table 1: Baseline characteristics of the two groups of patients before and after propensity score matching
Variable |
Before propensity score matching |
After propensity score matching |
||||
|---|---|---|---|---|---|---|
TACE-RT Group (n=76) |
RT-TACE |
P value |
TACE-RT Group (n=50) |
RT-TACE Group (n=25) |
P value |
|
Sex |
|
|
1.000 |
|
|
1.000 |
Age, yr a |
53.5 (45.3, 59.0) |
52.0 (41.3, 60.8) |
0.434 |
49.5 (42.5, 57.0) |
46.0 (37.5, 56.0) |
0.229 |
Child-Pugh score |
|
|
0.296 |
|
|
1.000 |
Baseline laboratory test result a |
|
|
|
|
|
|
HBsAg |
|
|
1.000 |
|
|
1.000 |
HBV-DNA, copies/ml |
|
|
0.697 |
|
|
0.662 |
Ascites |
|
|
0.981 |
|
|
1.000 |
AFP, ng/ml |
|
|
0.309 |
|
|
0.731 |
Tumor number |
|
|
0.821 |
|
|
1.000 |
Maximum lesion diameter, cm |
|
|
0.406 |
|
|
1.000 |
PVTT location |
|
|
0.278 |
|
|
1.000 |
a Data are shown as median (interquartile range).
AFP, α-fetoprotein; ALB, Albumin; ALT, Alanine aminotransferase; HBsAg, Hepatitis B surface antigen; PVTT, Portal vein tumor thrombus; nMT-PVTT, non main trunk portal vein tumor thrombus; MT-PVTT, main trunk portal vein tumor thrombus; RT-TACE, radiotherapy followed by transarterial chemoembolization; TACE-RT, transarterial chemoembolization followed by radiotherapy; TBIL, Total bilirubin.
The median follow-up was 11 months (range, 2-48 months) for the TACE-RT group and 14 months (range, 2-55 months) for the RT-TACE group. Collectively, all of the patients in the RT-TACE and TACE-RT group died during the study period. Thirty-eight (50.0%) of the 76 patients in the TACE-RT group and 25 (69.4%) of the 36 patients in the RT-TACE group underwent repeated TACE, with a mean of 1.9 (range, 1–9) and 3.1 (range, 1–12) TACE procedures per patient in the two groups of patients, respectively.
Tumor and PVTT response
The tumor and PVTT responses in patients with different extents of PVTT are shown in Table 2. For the liver tumors, the response rates for all patients were not significantly different between the TACE-RT and RT-TACE groups (59.2% vs. 72.2%, P = 0.182). On subgroup analysis, the response rate of the patients with main portal vein trunk tumor thrombus (main trunk-PVTT, MT-PVTT) in the RT-TACE group was 81.0%, which was significantly higher than the 50.0% in the TACE-RT group (P = 0.021). However, in patients without main portal vein trunk tumor thrombus (non-main trunk-PVTT, nMT-PVTT), the response rates between the two groups were not significantly different (67.5% in the TACE-RT group vs. 60.0% in the RT-TACE group, P = 0.602).
Table 2: Tumor and PVTT responses for patients with different extents of PVTT in the two treatment groups
CR (n) |
PR (n) |
SD (n) |
PD (n) |
RR (%) |
P value |
||
|---|---|---|---|---|---|---|---|
Tumor response |
|||||||
nMT-PVTT (n=55) |
TACE-RT (n=40) |
8 |
19 |
11 |
2 |
67.5 |
0.602 |
RT-TACE (n=15) |
2 |
7 |
5 |
1 |
60.0 |
||
MT-PVTT (n=57) |
TACE-RT (n=36) |
2 |
16 |
14 |
4 |
50.0 |
0.021 |
RT-TACE (n=21) |
5 |
12 |
3 |
1 |
81.0 |
||
All patients |
TACE-RT (n=76) |
10 |
35 |
25 |
6 |
59.2 |
0.182 |
RT-TACE (n=36) |
7 |
19 |
8 |
2 |
72.2 |
||
PVTT response |
|||||||
nMT-PVTT (n=55) |
TACE-RT (n=40) |
8 |
21 |
9 |
2 |
72.5 |
0.928 |
RT-TACE (n=15) |
3 |
7 |
4 |
1 |
66.7 |
||
MT-PVTT (n=57) |
TACE-RT (n=36) |
3 |
15 |
15 |
3 |
50.0 |
0.007 |
RT-TACE (n=21) |
6 |
12 |
2 |
1 |
85.7 |
||
All patients |
TACE-RT (n=76) |
11 |
36 |
24 |
5 |
61.8 |
0.094 |
RT-TACE (n=36) |
9 |
19 |
6 |
2 |
77.8 |
||
a Response rate (RR) was calculated with the following equation: RR = (CR+PR)/N.
b CR is number of patients with complete response, PR is number of patients with partial response, SD is number of patients with stable disease, and PD is number of patients with progressive disease.
PVTT, Portal vein tumor thrombus; nMT-PVTT, non main trunk portal vein tumor thrombus; MT-PVTT, main trunk portal vein tumor thrombus; RT-TACE, radiotherapy followed by transarterial chemoembolization; TACE-RT, transarterial chemoembolization followed by radiotherapy.
For PVTT, the response rates of all patients were not significantly different between the TACE-RT and RT-TACE groups (61.8% vs. 77.8%, P = 0.094). On subgroup analysis, the response rate of patients with MT-PVTT in the RT-TACE group was 85.7%, which was significantly higher than the 50% rate in the TACE-RT group (P = 0.007). However, in patients with nMT-PVTT, the response rates between the two groups were not significantly different (72.5% in the TACE-RT group vs. 66.7% in the RT-TACE group, P = 0.928).
Survival analysis of whole population with different extents of PVTT
The overall survival (OS) was similar between the TACE-RT and RT-TACE groups in all patients (P = 0.053; Figure 2A). The 1-, 2-, and 3-year OS rates were 38.2%, 18.4%, and 9.2% vs. 61.1%, 27.8%, and 16.7%, for the TACE-RT and RT-TACE groups, respectively. On subgroup analysis of OS in patients with different extents of PVTT, the TACE-RT group had similar OS as the RT-TACE group in patients with nMT-PVTT, (P = 0.867; Figure 3A). The 1-, 2-, and 3-year OS rates were 50.0%, 25.0%, and 10.0% vs. 66.7%, 26.7%, and 13.3%, for the TACE-RT and RT-TACE groups, respectively. In patients with MT-PVTT, the RT-TACE group had significantly better OS than the TACE-RT group (P = 0.014; Figure 3C). The 1-, 2-, and 3-year OS rates were 25.0%, 11.1%, and 8.3% vs. 57.1%, 28.6%, and 19.0%, for the TACE-RT and RT-TACE groups, respectively.
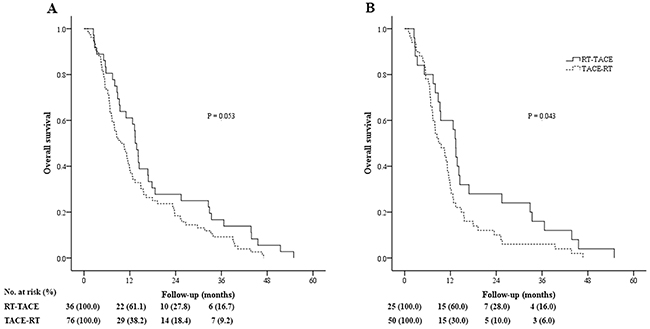
Figure 2: Kaplan-Meier curves of overall survival in patients with hepatocellular carcinoma (HCC) with portal vein tumor thrombus (PVTT) who underwent transarterial chemoembolization followed by radiotherapy (TACE-RT) or radiotherapy followed by transarterial chemoembolization (RT-TACE). (A) Whole study population (the TACE-RT group: n = 76, median OS = 9.6 months; the RT-TACE group: n = 36, median OS = 13.4 months; P = 0.053). (B) Patients selected in the propensity score analysis (the TACE-RT group: n = 50, median OS = 8.9 months; the RT-TACE group: n = 25, median OS = 13.4 months; P = 0.043).
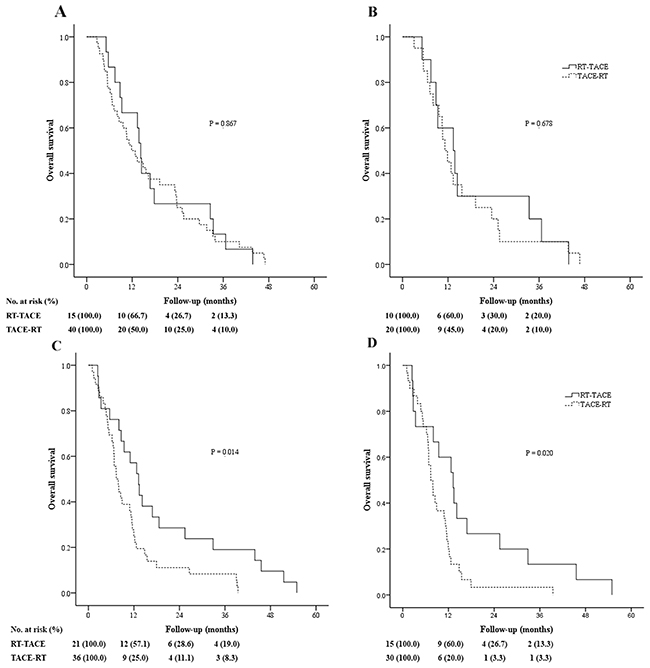
Figure 3: Kaplan-Meier curves of overall survival on subgroup analysis of patients with hepatocellular carcinoma (HCC) with different extents of portal vein tumor thrombus (PVTT) who underwent transarterial chemoembolization followed by radiotherapy (TACE-RT) or radiotherapy followed by transarterial chemoembolization (RT-TACE). (A) Whole study population of patients without main trunk PVTT (nMT-PVTT) (TACE-RT group: n = 40, median OS = 11.9 months; the RT-TACE group: n = 15, median OS = 14.2 months; P = 0.867). (B) Patients with nMT-PVTT selected in the propensity score analysis (the TACE-RT group: n = 20, median OS = 11.2 months; the RT-TACE group: n = 10, median OS = 13.4 months; P = 0.678). (C) Whole study population of patients with main trunk PVTT (MT-PVTT) (the TACE-RT group: n = 36, median OS = 7.4 months; the RT-TACE group: n = 21, median OS = 13.2 months; P = 0.014). (D) Patients with MT-PVTT selected in the propensity score analysis (TACE-RT group: n = 30, median OS = 7.4 months; RT-TACE group: n = 15, median OS = 13.2 months; P = 0.020).
Survival analysis of patients selected in the propensity score analysis with different extents of PVTT
For all patients selected in propensity score matching, the RT-TACE group had better OS than that of the TACE-RT group (P = 0.043; Figure 2B). The 1-, 2-, and 3-year OS rates were 30.0%, 10.0%, and 6.0% vs. 60.0%, 28.0%, and 16.0%, for the TACE-RT and RT-TACE groups, respectively. On subgroup analysis of OS in patients with different extents of PVTT, for patients with nMT-PVTT, the TACE-RT group had similar OS as the RT-TACE group (P = 0.678; Figure 3B). The 1-, 2-, and 3-year OS rates were 45.0%, 20.0%, and 10.0% vs. 60.0%, 30.0%, and 20.0%, for the TACE-RT and RT-TACE groups, respectively. In patients with MT-PVTT, the RT-TACE group had significantly better OS than the TACE-RT group (P = 0.020; Figure 3D). The 1-, 2-, and 3-year OS rates were 20.0%, 3.3%, and 3.3% vs. 60.0%, 26.7%, and 13.3%, for the TACE-RT and RT-TACE groups, respectively.
Factors associated with overall survival
On univariable analysis for OS before PSM, maximum lesion diameter > 5 cm was associated with decreased long-term survival rates (P = 0.008, Table 3). In the Cox proportional hazards model, one independent prognostic predictor of poor survival was a maximum lesion diameter > 5 cm (HR: 2.004, 95% CI: 1.183-3.396, P =0.010).
Table 3: Univariable and multivariable analyses of survival for patients with hepatocellular carcinoma (HCC) with portal vein tumor thrombus (PVTT) before and after propensity score matching
Univariable analysis |
Multivariable analysis |
|||||
|---|---|---|---|---|---|---|
N |
Median OS (mo) |
P value |
HR |
95% CI |
P value |
|
All patients (n = 112) |
||||||
Sex (male/female) |
104/8 |
11.5/5.6 |
0.065 |
|||
Age (>60/≤60 yrs) |
25/87 |
13.8/10.4 |
0.257 |
|||
Child-Pugh class (A/B) |
105/7 |
11.2/8.6 |
0.781 |
|||
TBIL (≤34/>34 μmol/L) |
102/10 |
11.5/5.2 |
0.480 |
|||
ALB (>35/≤35 g/L) |
103/9 |
11.2/14.2 |
0.646 |
|||
ALT (≤40/>40 U/L) |
45/67 |
12.7/10.6 |
0.132 |
|||
HBsAg (negative /positive) |
13/99 |
14.9/11.0 |
0.080 |
|||
Ascites (absent/present) |
101/11 |
11.2/8.6 |
0.370 |
|||
AFP (≤400/>400 ng/ml) |
45/67 |
12.2/11.0 |
0.133 |
|||
Tumor number (1/>1) |
92/20 |
10.9/14.8 |
0.074 |
|||
Maximum lesion diameter (≤5/>5 cm) |
20/92 |
16.3/10.4 |
0.008 |
2.004 |
1.183-3.396 |
0.010 |
Main trunk PVTT (absent/present) |
55/57 |
13.4/8.9 |
0.301 |
|||
Treatment (RT-TACE/TACE-RT) |
36/76 |
13.4/9.6 |
0.053 |
|||
Patients selected in the propensity score analysis (n = 75) |
||||||
Sex (male/female) |
72/3 |
10.6/7.9 |
0.230 |
|||
Age (>60/≤60 yrs) |
10/65 |
10.9/10.4 |
0.677 |
|||
Child-Pugh class (A/B) |
72/3 |
10.6/5.2 |
0.137 |
|||
TBIL (≤34/>34 μmol/L) |
70/5 |
10.6/9.4 |
0.154 |
|||
ALB (>35/≤35 g/L) |
69/6 |
10.6/7.4 |
0.658 |
|||
ALT (≤40/>40 U/L) |
32/43 |
11.9/8.9 |
0.035 |
0.737 |
0.445-1.221 |
0.236 |
HBsAg (negative /positive) |
2/73 |
8.1/10.9 |
0.441 |
|||
Ascites (absent/present) |
68/7 |
10.6/9.6 |
0.964 |
|||
AFP (≤400/>400 ng/ml) |
26/49 |
11.5/9.6 |
0.210 |
|||
Tumor number (1/>1) |
68/7 |
10.9/8.0 |
0.126 |
|||
Maximum lesion diameter (≤5/>5 cm) |
5/70 |
15.5/9.4 |
0.026 |
2.444 |
0.849-7.037 |
0.098 |
Main trunk PVTT (absent/present) |
30/45 |
11.9/8.5 |
0.122 |
|||
Treatment (RT-TACE/TACE-RT) |
25/50 |
13.4/8.9 |
0.043 |
0.655 |
0.396-1.082 |
0.098 |
95% CI, 95% confidence interval; AFP, α-fetoprotein; ALB, Albumin; ALT, Alanine aminotransferase; HBsAg, Hepatitis B surface antigen; HR, Hazard radio; OS, Overall survival; PVTT, Portal vein tumor thrombus; RT-TACE, radiotherapy followed by transarterial chemoembolization; TACE-RT, transarterial chemoembolization followed by radiotherapy; TBIL, Total bilirubin.
On univariable analysis of OS for patients after PSM, maximum lesion diameter > 5 cm, TACE-RT treatment, and ALT > 40 U/L were associated with a decreased survival (all P < 0.05). In the Cox proportional hazards model, no independent prognostic predictor was identified (Table 3).
Adverse events
Table 4 shows the adverse events profile. During the period and between 1 and 3 months after treatment, worsening of liver function was observed in 22.4% (17/76) and 11.1% (4/36) of the patients in the TACE-RT and RT-TACE groups. The rate of liver function worsening in the TACE-RT group was higher when compared with the RT-TACE group, but there was no significant difference between the two groups (P = 0.154). On subgroup analysis of adverse events in the patients with different extents of PVTT, for patients with nMT-PVTT, the rates of liver function worsening were similar between the two groups (12.5% vs. 13.3%, P = 1.000). For patients with MT-PVTT, the rate of liver function worsening in the TACE-RT group was significantly higher than the RT-TACE group (33.3% vs. 9.5%, P = 0.044). Fever, gastrointestinal disorders, and acute bone marrow suppression were observed in 14.5% (11/76), 25.0% (19/76), and 25.0% (19/76), respectively, in patients in the TACE-RT group, and 13.9% (5/36), 22.2% (8/36), and 27.7% (10/36), respectively, in patients in the RT-TACE group. There were no significant differences between the two groups for these adverse events (P = 0.934, 0.748, and 0.754, respectively). All the disorders returned to baseline values within 3 weeks. No patients required discontinuation in treatment because of serious adverse reactions.
Table 4: Adverse events related to the two treatments in the different subgroups
Worsening of liver function |
Fever |
Gastrointestinal disorders |
Acute bone marrow suppression |
||||
|---|---|---|---|---|---|---|---|
A to B |
B to C |
A to C |
Sum |
||||
nMT-PVTT |
|||||||
TACE-RT (n=40) |
4 |
1 |
- |
5 (12.5%) |
6 (15.0%) |
10 (25.0%) |
9 (22.5%) |
RT-TACE (n=15) |
2 |
- |
- |
2 (13.3%) |
2 (13.3%) |
3 (20.0%) |
4 (26.7%) |
P value |
1.000 |
1.000 |
0.974 |
1.000 |
|||
mPVTT |
|||||||
TACE-RT (n=36) |
10 |
1 |
1 |
12 (33.3%) |
5 (13.9%) |
9 (25.0%) |
10 (27.8%) |
RT-TACE (n=21) |
2 |
- |
- |
2 (9.5%) |
3 (14.3%) |
5 (23.8%) |
6 (28.6%) |
P value |
0.044 |
1.000 |
0.920 |
0.949 |
|||
All Patients |
|||||||
TACE-RT (n=76) |
14 |
2 |
1 |
17 (22.4%) |
11 (14.5%) |
19 (25.0%) |
19 (25.0%) |
RT-TACE (n=36) |
4 |
- |
- |
4 (11.1%) |
5 (13.9%) |
8 (22.2%) |
10 (27.7%) |
P value |
0.154 |
0.934 |
0.748 |
0.754 |
|||
nMT-PVTT, non-main trunk portal vein tumor thrombus; MT-PVTT, main trunk portal vein tumor thrombus; RT-TACE, radiotherapy followed by transarterial chemoembolization; TACE-RT, transarterial chemoembolization followed by radiotherapy.
DISCUSSION
Accumulating evidences suggest that combined of TACE and RT is safe and effective to treat patients with unresctable HCC with PVTT [12-19]. Unfortunately, there are little data to suggest whether TACE should be given before or after external radiotherapy. Kang J et al [17] reported that there were no significant differences in response rate, survival rate, and α-fetoprotein level normalization rate between the SBRT-TACE group and the TACE-SBRT group. However, the latter regimen exerted a more severe negative effect on liver function when compared with the former one. For the whole population, our study showed similar results as reported by Kang J et al. On subgroup analysis using the extent of PVTT, for the first time our study showed that IMRT followed by TACE provided better survival outcomes and lower rates of worsening of liver function when compared with TACE followed by IMRT in HCC patients with main trunk PVTT. Using propensity score matching analysis which reduced selection biases and increased reliability of the study, this study also substantiated the above observations.
When PVTT extends to the main portal vein, the prognosis is extremely bad because (1) shedding of HCC cells leads to extensive intra-hepatic metastases; (2) complete obstruction of the main portal vein causes further deterioration in liver function. In a recent review article on the role of radiotherapy as a treatment modality for patients with HCC and PVTT, main PVTT serves as a main obstacle to liver function maintenance and a source of metastasis, and IMRT can be an effective treatment for main PVTT [20]; (3) aggravation of portal hypertension results in intractable ascites and esophageal bleeding [21]. Many HCC patients with main trunk PVTT die of esophageal bleeding or liver failure caused by obstruction of the main portal vein, rather than from the liver tumor. The placement of a portal vein stent in patients with HCC with main PVTT to keep the main portal vein patent has been shown to play a prominent role in improving hepatic function, in preventing liver failure and variceal bleeding due to portal hypertension [22]. Thus, timely radiotherapy to control PVTT may be beneficial for these patients.
For patients with main trunk PVTT, TACE before IMRT can lead to hepatic ischemia and cellular damage, which can worsen liver function, reduce some effects of IMRT as tumor hypoxia caused by TACE, and enhance radioresistance in HCC [23]. On the other hand, IMRT before TACE can shrink the PVTT. Subsequently increased blood flow through the main portal vein can reduce the negative embolic effects of TACE, and the worsening effects on liver function caused by the combined treatment. Liver function is recognized to be an independent prognostic factor of survival of HCC patients with PVTT [24, 25]. These may help to explain why IMRT followed by TACE resulted in less worsening of liver function and significantly better survival outcomes for HCC patients with main trunk PVTT when compared with TACE followed by IMRT.
Our study had limitations. First, this is a retrospective study carried out in a single-center which have potential selection biases. However, we attempted to use propensity score matching analysis to overcome this limitation. Second, the aetiology of patients with HCC and PVTT in our study is mainly due to chronic hepatitis B. The results of this study may not be applied to HCC due to other aetiologies. Finally, a prospective randomized trial with considerable population is necessary to confirm our findings.
In conclusion, for HCC patients with main trunk PVTT, IMRT followed by TACE produced better survival outcomes and caused less worsening of liver function than TACE followed by IMRT.
MATERIALS AND METHODS
Patients
The study was approved by the Ethics Committee of the Eastern Hepatobiliary Surgery Hospital of the Second Military Medical University (Shanghai, China). Written informed consent was obtained from all the patients for their data to be used for clinical research.
Between January 2004 and December 2013, all consecutive patients with unresectable HCC with PVTT who were treated by combined TACE and IMRT at the Eastern Hepatobiliary Surgery Hospital of the Second Military Medical University (Shanghai, China) were retrospectively studied. The inclusion criteria were: (a) age between 18 and 75 years, (b) HCC with major portal vein invasion, (c) the tumor was considered to be unresectable by two senior hepatic surgeons, (d) Child-Pugh A or B liver function. The exclusion criteria were: (a) Child-Pugh C liver function, (b) extra-hepatic metastasis, (c) previously treated by hepatic resection (HR), radiofrequency ablation (RFA), sorafenib or systemic chemotherapy, (d) serious associated medical diseases.
HCC was diagnosed according to the non-invasive criteria of the European Association for the Study of Liver/American Association Guidelines [26]. The presence and extent of PVTT were assessed on multiphase dynamic CT scans using the following criteria: a low-attenuation intraluminal mass which expanded the portal vein or as filling defects in the main portal vein trunk, portal venous branches, or both. The patients were divided into two subgroups according to whether the tumor thrombus had extended to the main portal vein trunk: Subgroup 1, extent of PVTT not involving the main portal vein (Cheng’s classification I and II; Japanese Classification vP1 to vP3); and Subgroup 2, PVTT had extended to the main portal vein (Cheng’s classification III and IV; Japanese Classification vP4) [27].
The treatment decision was made by our multi-disciplinary team that the patients were suitable for treatment with either TACE before (TACE-RT) or after IMRT (RT-TACE). Patients were considered to be suitable for TACE only if they had good liver function and there were adequate venous collaterals around the blocked main portal veins [28, 29]. The final decision on the treatment was made by the patient after full explanation was given to the patient.
The TACE procedure
Using the Seldinger technique, a vascular catheter was inserted through a femoral artery to the hepatic artery. After hepatic angiography, the catheter was selectively inserted into the tumor-feeding artery whenever technically possible. An emulsion of 5-fluorouracil (1 g), mitomycin C (20 mg), cisplatin (5 mg), and lipiodol 10 to 30 ml (1 to 2 ml/cm diameter of the tumor) was injected. Gelfoam fragments were then injected to embolise the tumor-feeding vessel. The treatment was repeated at 6 to 8 weeks intervals until complete disappearance of viable intrahepatic tumor, provided that hepatic function was preserved.
Radiotherapy procedure
IMRT was used for radiotherapy. The patient was scanned during the arterial phase and portal phase, from carina to the fifth lumbar vertebra with a thickness slice of 5.0 mm. The images and related data were delivered to the treatment plan system (TPS). The PVTT was outlined as a clinical target volume (CTV), and the plan target volume (PTV) was expanded 1.0 cm in the XY axis, and 0.5 cm in the Z axis (head direction). The prescribed doses to the initial PTV ranged from 50 to 67 Gy (median 58 Gy), given in daily doses of 2.0-2.2 Gy. The biologically effective dose (BED) ranged from 61.0 Gy to 82.5 Gy (median 68.2 Gy, α/β=10). A dose volume histogram (DVH) was used for dose optimization, with 90% of the dose curve being completely covered by the PTV. The internal dose to the PVTT was uniform, and the dose change was never more than 5%. The radiation doses to the organs such as the gastrointestinal tract and the spinal cord were all acceptably low and the dose limit of a high dose was never more than 10%.
Combination treatment process
All patients received treatment within 1 week of diagnosis of HCC with PVTT. The group assignment was: for group TACE-RT, 76 patients were treated with TACE followed by IMRT within the next 2-4 weeks, and for group RT-TACE, 36 patients were treated with IMRT followed by TACE within the next 2-4 weeks, depending on recovery of liver function. Patients with a high viral load (≥ 104 copies/ml) of HBV-DNA were given nucleotide/nucleoside analog (NA) treatment [30].
Evaluation
All patients were followed-up by the same multidisciplinary team after treatment. This study was censored on June 30, 2017. The baseline characteristics of the two groups were compared before and after propensity score matched analysis. The short-term therapeutic effects on liver tumors and PVTT were evaluated separately according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST) [31, 32] within 1 month after treatment. A complete response (CR) was defined as disappearance of intratumoral arterial enhancement in all target lesions; a partial response (PR) was at least 30% decrease in the sum of diameters of viable (contrast enhancement in the arterial phase) target lesions, taking as reference the baseline sum of the diameters of the target lesions; a progressive disease (PD) was an increase of at least 20% in the sum of the diameters of viable (enhancing) target lesions, taking as reference the smallest sum of the diameters of viable (enhancing) target lesions recorded since treatment started; a stable disease (SD) was any cases that do not qualify for either partial response or progressive disease. The response rate (RR) was estimated based on the combined number of patients with CR and PR. In addition to the size of the PVTT, other factors like recanalization of any part of the blocked portal vein were also taken into consideration.
For long-term survival outcomes, OS was compared between the two groups before and after propensity score matched analysis. OS was measured from the date of first treatment (either TACE or IMRT) to the date of death or the last follow-up. The prognostic factors for overall survival were explored using univariable and multivariable analyses before and after propensity score matched analysis. A subgroup analysis was performed on patients with different extents of PVTT.
The adverse events were evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE; version3.0) [33].
Statistical methods
All statistical analyses were performed using SPSS 20.0 (IBM, New York, NY). Continuous variables were expressed as mean ± sd or median (interquartile range) as appropriate. Categorical variables were compared by the χ2 test or the Fisher exact test, and continuous variables by the student’s t test or the non-parametric test. Overall survival curves were constructed using the Kaplan-Meier method and compared with the log-rank test. Univariable analyses were performed with the log-rank test. Variables with a P value of < 0.05 were then entered into a multivariable analysis. Multivariable analyses were performed with a Cox proportional hazard regression model.
To investigate the association between treatment and outcomes in an observational database rather than in a randomized, controlled trial, a propensity score matching analysis was used in an attempt to reduce biases in patient selection. The R version 2.12.1 (The R Foundation for Statistical Computing) and the MatchIt package were used to produce the propensity score graphs. PSM was performed via binary logistic regression to generate a propensity score for each patient. The co-variables entered into the model included age, sex, Child-Pugh score, HBsAg positivity, AFP, PVTT extent, tumor size, and tumor number. Subsequently, a one-to-two match between the RT-TACE group and the TACE-RT group on patients with HCC with PVTT was obtained by use of the nearest-neighborhood matching using a caliper width of 0.02 without replacement.
All statistical tests were two tailed, and a P value < 0.05 indicated a significant difference.
CONFLICTS OF INTEREST
There is no conflicts of interest.
FUNDING
This work was supported by the grants of The National Key Basic Research Program “973 project” (No: 2015CB554000); the Science Fund for Creative Research Groups (No: 81521091); Shanghai Science and Technology Committee (No: 134119a0200); Shanghai Shenkang Project (SHDC12015106); SMMU Innovation Alliance for Liver Cancer Diagnosis and Treatment (2012); Collaborative Innovation Center for Cancer Medicine.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87–108.
2. Llovet JM, Bustamante J, Castells A, Vilana R, Ayuso MC, Sala M, Brú C, Rodés J, Bruix J. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology. 1999; 29:62–67.
3. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, et al, and SHARP Investigators Study Group. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008; 359:378–90.
4. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS, Xu J, Sun Y, Liang H, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009; 10:25–34.
5. Shi J, Lai EC, Li N, Guo WX, Xue J, Lau WY, Wu MC, Cheng SQ. Surgical treatment of hepatocellular carcinoma with portal vein tumor thrombus. Ann Surg Oncol. 2010; 17:2073–80.
6. Liu PH, Lee YH, Hsia CY, Hsu CY, Huang YH, Chiou YY, Lin HC, Huo TI. Surgical resection versus transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombosis: a propensity score analysis. Ann Surg Oncol. 2014; 21:1825–33.
7. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003; 37:429–42.
8. Xue TC, Xie XY, Zhang L, Yin X, Zhang BH, Ren ZG. Transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus: a meta-analysis. BMC Gastroenterol. 2013; 13:60.
9. Wada H, Sasaki Y, Yamada T, Ohigashi H, Miyashiro I, Murata K, Doki Y, Ishikawa O, Nishiyama K, Imaoka S. Successful preoperative treatment for hepatocellular carcinoma with tumor thrombus in the major portal branch by three-dimensional conformal radiation therapy--two case reports. Hepatogastroenterology. 2005; 52:343–7.
10. Kim DY, Park W, Lim DH, Lee JH, Yoo BC, Paik SW, Kho KC, Kim TH, Ahn YC, Huh SJ. Three-dimensional conformal radiotherapy for portal vein thrombosis of hepatocellular carcinoma. Cancer. 2005; 103:2419–26.
11. Lin CS, Jen YM, Chiu SY, Hwang JM, Chao HL, Lin HY, Shum WY. Treatment of portal vein tumor thrombosis of hepatoma patients with either stereotactic radiotherapy or three-dimensional conformal radiotherapy. Jpn J Clin Oncol. 2006; 36:212–17.
12. Tazawa J, Maeda M, Sakai Y, Yamane M, Ohbayashi H, Kakinuma S, Miyasaka Y, Nagayama K, Enomoto N, Sato C. Radiation therapy in combination with transcatheter arterial chemoembolization for hepatocellular carcinoma with extensive portal vein involvement. J Gastroenterol Hepatol. 2001; 16:660–65.
13. Ishikura S, Ogino T, Furuse J, Satake M, Baba S, Kawashima M, Nihei K, Ito Y, Maru Y, Ikeda H. Radiotherapy after transcatheter arterial chemoembolization for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Clin Oncol. 2002; 25:189–93.
14. Yamada K, Izaki K, Sugimoto K, Mayahara H, Morita Y, Yoden E, Matsumoto S, Soejima T, Sugimura K. Prospective trial of combined transcatheter arterial chemoembolization and three-dimensional conformal radiotherapy for portal vein tumor thrombus in patients with unresectable hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2003; 57:113–19.
15. Choi BO, Choi IB, Jang HS, Kang YN, Jang JS, Bae SH, Yoon SK, Chai GY, Kang KM. Stereotactic body radiation therapy with or without transarterial chemoembolization for patients with primary hepatocellular carcinoma: preliminary analysis. BMC Cancer. 2008; 8:351.
16. Yoon SM, Lim YS, Won HJ, Kim JH, Kim KM, Lee HC, Chung YH, Lee YS, Lee SG, Park JH, Suh DJ. Radiotherapy plus transarterial chemoembolization for hepatocellular carcinoma invading the portal vein: long-term patient outcomes. Int J Radiat Oncol Biol Phys. 2012; 82:2004–11.
17. Kang J, Nie Q, Du R, Zhang L, Zhang J, Li Q, Li J, Qi W. Stereotactic body radiotherapy combined with transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombosis. Mol Clin Oncol. 2014; 2:43–50.
18. Lu DH, Fei ZL, Zhou JP, Hu ZT, Hao WS. A comparison between three-dimensional conformal radiotherapy combined with interventional treatment and interventional treatment alone for hepatocellular carcinoma with portal vein tumour thrombosis. J Med Imaging Radiat Oncol. 2015; 59:109–14.
19. Li XL, Guo WX, Hong XD, Yang L, Wang K, Shi J, Li N, Wu MC, Cheng SQ. Efficacy of the treatment of transarterial chemoembolization combined with radiotherapy for hepatocellular carcinoma with portal vein tumor thrombus: A propensity score analysis. Hepatol Res. 2016; 46:1088–98.
20. Yu JI, Park HC. Radiotherapy as valid modality for hepatocellular carcinoma with portal vein tumor thrombosis. World J Gastroenterol. 2016; 22:6851–63.
21. Tang QH, Li AJ, Yang GM, Lai EC, Zhou WP, Jiang ZH, Lau WY, Wu MC. Surgical resection versus conformal radiotherapy combined with TACE for resectable hepatocellular carcinoma with portal vein tumor thrombus: a comparative study. World J Surg. 2013; 37:1362–70.
22. Ishikawa T, Kubota T, Abe H, Nagashima A, Hirose K, Togashi T, Seki K, Honma T, Yoshida T, Kamimura T. Percutaneous transhepatic portal vein stent placement can improve prognosis for hepatocellular carcinoma patients with portal vein tumor thrombosis. Hepatogastroenterology. 2014; 61:413–16.
23. Piao LS, Hur W, Kim TK, Hong SW, Kim SW, Choi JE, Sung PS, Song MJ, Lee BC, Hwang D, Yoon SK. CD133+ liver cancer stem cells modulate radioresistance in human hepatocellular carcinoma. Cancer Lett. 2012; 315:129–37.
24. Yu JI, Park HC, Lim DH, Park W, Yoo BC, Paik SW, Koh KC, Lee JH. Prognostic index for portal vein tumor thrombosis in patients with hepatocellular carcinoma treated with radiation therapy. J Korean Med Sci. 2011; 26:1014–22.
25. Liu L, Zhang C, Zhao Y, Qi X, Chen H, Bai W, He C, Guo W, Yin Z, Fan D, Han G. Transarterial chemoembolization for the treatment of advanced hepatocellular carcinoma with portal vein tumor thrombosis: prognostic factors in a single-center study of 188 patients. Biomed Res Int. 2014; 2014:194278.
26. Bruix J, Sherman M, and Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208–36.
27. Shuqun C, Mengchao W, Han C, Feng S, Jiahe Y, Guanghui D, Wenming C, Peijun W, Yuxiang Z. Tumor thrombus types influence the prognosis of hepatocellular carcinoma with the tumor thrombi in the portal vein. Hepatogastroenterology. 2007; 54:499–502.
28. Chung GE, Lee JH, Kim HY, Hwang SY, Kim JS, Chung JW, Yoon JH, Lee HS, Kim YJ. Transarterial chemoembolization can be safely performed in patients with hepatocellular carcinoma invading the main portal vein and may improve the overall survival. Radiology. 2011; 258:627–34.
29. Luo J, Guo RP, Lai EC, Zhang YJ, Lau WY, Chen MS, Shi M. Transarterial chemoembolization for unresectable hepatocellular carcinoma with portal vein tumor thrombosis: a prospective comparative study. Ann Surg Oncol. 2011; 18:413–20.
30. Yin J, Li N, Han Y, Xue J, Deng Y, Shi J, Guo W, Zhang H, Wang H, Cheng S, Cao G. Effect of antiviral treatment with nucleotide/nucleoside analogs on postoperative prognosis of hepatitis B virus-related hepatocellular carcinoma: a two-stage longitudinal clinical study. J Clin Oncol. 2013; 31:3647–55.
31. Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, Sherman M, Schwartz M, Lotze M, Talwalkar J, Gores GJ, and Panel of Experts in HCC-Design Clinical Trials. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008; 100:698–711.
32. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009; 45:228–47.
33. NCI. CTCAE v3.0. Available from: URL: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf.