
INTRODUCTION
The 3rd edition of the Japanese Classification of Gastric Carcinoma defines remnant gastric cancer (RGC) as all cancers arising in the remnant stomach, regardless of the initial disease or operation [1]. Several studies have reported that in patients who had a previous gastrectomy, the incidence of RGC is 2–3%, representing 1.8% of all stomach cancers [3–5]. Recently, the prevalence of RGC has risen due to the improved survival of patients who received a distal gastrectomy for a peptic ulcer or primary gastric cancer [6] and an increase in endoscopy screening, which improves early diagnosis and treatment. Moreover, patients with Billroth II anastomosis, a constant irritation caused by bile acid reflux that results in mucosal inflammation and degeneration, have a higher prevalence of RGC than those with Billroth I anastomosis [7–11]. Therefore, RGC is a malignancy that will continue to require clinical attention.
Standard surgery for RGC involves removing the entire remnant stomach and dissecting the lymph node [2]. Laparoscopic gastrectomy is gaining popularity because it is minimally invasive and has a shorter postoperative recovery time, among other benefits. The main target of the procedure is early primary gastric cancer [12–15]. In RGC cases, severe adhesion, regional anatomical modification and the variation in lymphatic flow resulting from the initial surgery make laparoscopy difficult. In addition, the low incidence rate of RGC makes it difficult to conduct randomized controlled trials, leading to controversy over surgical selection. To date, only a few retrospective studies focusing on early stage disease have demonstrated the feasibility and safety of laparoscopic gastrectomy to treat RGC [16–21]. The short-term surgical efficacy and long-term survival outcomes of advanced RGC have not been reported.
This study investigated the surgical outcomes of laparoscopic-assisted total gastrectomy (LATG) as well as its impact on long-term survival on both early and advanced RGC. This was accomplished by comprehensively reviewing the oncologic outcomes of this technique. To the best of our knowledge, this study is one of the largest studies of its kind to date.
RESULTS
Clinicopathological characteristics of patients
The data extraction process is depicted in Figure 1. Patient characteristics are shown in Table 1. There were 18 patients in the open total gastrectomy (OTG) cohort and 12 in the LATG cohort that suffered from preoperative comorbidity. In the OTG group, 5 patients had diabetes, 5 had hypertension, 1 had diabetes with hypertension, 1 had hypertension and coronary heart disease, and the remaining 6 had hepatic lipidosis, hepatic dysfunction, atrial fibrillation, coronary heart disease, hyperthyroidism and bronchial asthma. In the LATG group, there were 6 cases of hypertension, 2 cases of diabetes and 2 cases of hepatitis B. Additionally, 1 patient had diabetes with hypertension, atrial fibrillation and alcoholic liver cirrhosis. The anastomotic site was the most common area for RGC. Pathological analysis revealed that the tumor location, tumor size, depth of invasion, lymph node metastasis and TNM stage were not significantly different between the two groups (p > 0.05); however, histology revealed that the number of undifferentiated tumors was significantly higher in the OTG group than in the LATG group (n = 28, p = 0.022).
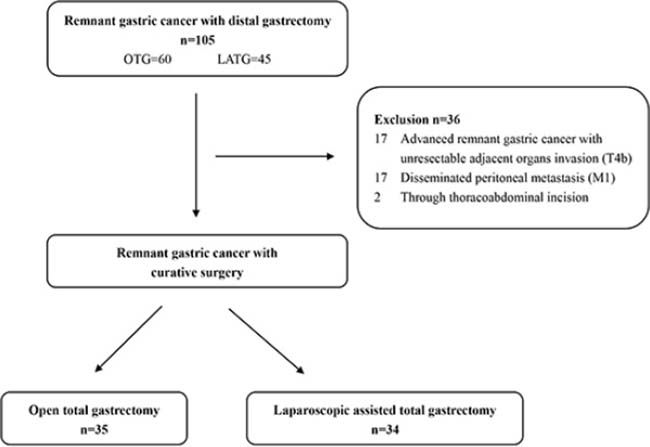
Figure 1: Study design.
Table 1: Clinicopathological parameters of patients with remnant gastric cancer
Characteristic |
OTG (n = 35) |
LATG (n = 34) |
χ2/t |
P value |
|---|---|---|---|---|
Age (year) |
62.86 ± 9.74 |
63.82 ± 8.65 |
0.435 |
0.665 |
BMI (kg/m2) |
20.83 ± 2.24 |
21.12 ± 3.44 |
0.426 |
0.672 |
Time Interval (year) |
26.06 ± 11.29 |
25.35 ± 10.18 |
0.272 |
0.787 |
Gender |
0.403 |
0.734 |
||
Female |
6 (17.1%) |
4 (11.8%) |
||
Male |
29 (82.9%) |
30 (88.2%) |
||
Previous Disease |
0.336 |
0.752 |
||
Benign |
28 (80.0%) |
29 (85.3%) |
||
Malignant |
7 (20.0%) |
5 (17.7%) |
||
Previous Reconstruction |
0.359 |
0.611 |
||
Billroth I |
10 (28.6%) |
12 (35.3%) |
||
Billroth II |
25 (71.4%) |
22 (64.7%) |
||
Preoperative Comorbidity |
1.827 |
0.293 |
||
Positive |
18 (51.4%) |
12 (35.3%) |
||
Negative |
17 (48.6%) |
22 (64.7%) |
||
Tumor Location |
2.502 |
0.227 |
||
Anastomosis Site |
21 (60.0%) |
14 (41.2%) |
||
Cardia |
8 (22.9%) |
12 (35.3%) |
||
Fundus |
1 (2.9%) |
2 (5.9%) |
||
Body |
5 (14.2%) |
6 (17.6%) |
||
Tumor Size (mm) |
44.31 ± 18.81 |
41.18 ± 17.76 |
0.712 |
0.479 |
Type of Histology |
5.682 |
0.022 |
||
Differentiated |
7 (20.0%) |
16 (47.1%) |
||
Undifferentiated |
28 (80.0%) |
18 (52.9%) |
||
Tumor Invasion |
0.519 |
0.521 |
||
T1 |
6 (17.1%) |
5 (14.7%) |
||
T2 |
6 (17.1%) |
6 (17.6%) |
||
T3 |
7 (20.0%) |
12 (35.3%) |
||
T4a |
16 (45.7%) |
11 (32.4%) |
||
Lymph Node Metastasis |
3.694 |
0.301 |
||
N0 |
20 (57.1%) |
16 (47.1%) |
||
N1 |
3 (8.6%) |
3 (8.8%) |
||
N2 |
8 (22.9%) |
5 (14.7%) |
||
N3 |
4 (11.4%) |
10 (29.4%) |
||
TNM Stage |
3.998 |
0.151 |
||
I |
8 (22.9%) |
9 (26.5%) |
||
II |
16 (45.7%) |
8 (23.5%) |
||
III |
11 (31.4%) |
17 (50.0%) |
All continuous values are means ± deviation.
OTG Open total gastrectomy LATG Laparoscopic-assisted total gastrectomy BMI Body mass index.
Surgical and short-term postoperative outcomes
As shown in Table 2, the LATG group had more dissected lymph nodes (14.3 vs. 19.4, p = 0.048), less blood loss (192.9 vs. 98.5 ml, p = 0.002), shorter operation times (236.7 vs. 195.3 min, p = 0.001) and shorter hospital stays (18.0 vs. 13.9 days, p = 0.012) than the OTG group. There was no significant difference in the time to first flatus between the two groups (p = 0.765). Regarding severe postoperative complications (Clavien-Dindo classification≥IIIa) [24], the discrepancy in morbidity was not statistically significant, with rates of 14.29% and 8.82% in the OTG and LATG groups, respectively.
Table 2: Short-term postoperative outcomes
Characteristic |
OTG (n = 35) |
LATG (n = 34) |
χ2/t |
P value |
|---|---|---|---|---|
No. of Retrieved LNs |
14.31 ± 7.824 |
19.41 ± 12.71 |
2.013 |
0.048 |
Blood Loss (ml) |
192.9 ± 149.10 |
98.53 ± 78.09 |
3.278 |
0.002 |
Hospital Stay (days) |
18.03 ± 6.27 |
13.88 ± 7.01 |
2.590 |
0.012 |
Time of Operation (mins) |
236.7 ± 50.74 |
195.3 ± 48.44 |
3.466 |
0.001 |
Time to First Flatus (days) |
3.800 ± 1.13 |
3.882 ± 1.15 |
0.300 |
0.765 |
Severe Complication* |
5 (14.29%) |
3 (8.82%) |
0.502 |
0.710 |
Intraperitoneal Infection |
3 |
1 |
||
Anastomotic Leakage |
1 |
|||
Chylous Leakage |
1 |
|||
Bowel Obstruction |
1 |
|||
Intraperitoneal Bleeding |
1 |
*The Clavien-Dindo classification Grade ≥ IIIa.
All continuous values are means ± deviation.
OTG, Open total gastrectomy; LATG, Laparoscopic-assisted total gastrectomy.
Survival analysis
Median follow-up times were 39 months (95% CI 25–56 months) and 35 months (95% CI 21–43 months) in the OTG and LATG groups, respectively. The median survival time was 31 months (95% CI 23–39 months) in the OTG group and 28 months (95% CI 20–35 months) in the LATG group.
Kaplan-Meier analysis revealed no significant difference in cumulative survival rates between the two groups (p = 0.957), with rates of 45.31% in the OTG group and 37.96% in the LATG group (Figure 2). Of the thirteen factors identified using univariate analysis, serosal invasion (p = 0.002), lymph node metastasis (p = 0.009) and TNM stage (p = 0.002) were relevant to the prognosis. Using a Cox proportional hazards regression model, serosal invasion (p = 0.036) and TNM stage (p = 0.039) were identified as independent prognostic factors for RGC (Table 3).
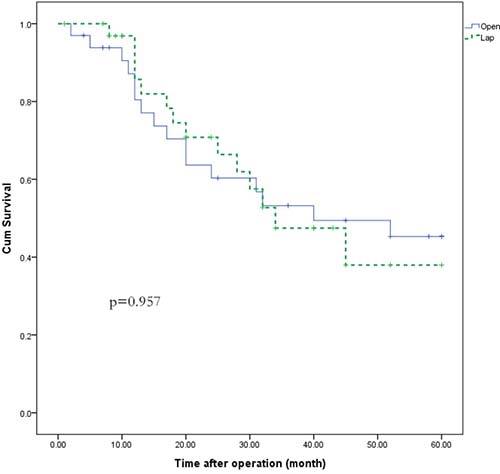
Figure 2: Patient survival curve for RGC by laparoscopic or open surgery.
Table 3: Univariate and multivariable prognostic analysis of remnant gastric cancer
Characteristic |
Total (n = 69) |
Univariate |
Multivariate analysis |
|
|---|---|---|---|---|
HR (95 % CI) |
p value |
|||
Age |
0.202 |
|||
<60 |
27 (39.1%) |
|||
≥60 |
42 (60.9%) |
|||
Gender |
0.251 |
|||
Female |
10 (14.5%) |
|||
Male |
59 (85.5%) |
|||
BMI (kg/m2) |
0.461 |
|||
<25 |
63 (91.3%) |
|||
≥25 |
6 (8.7%) |
|||
Tumor Size (mm) |
0.691 |
|||
<50 |
36 (52.2%) |
|||
≥50 |
33 (46.8%) |
|||
Previous Disease |
0.569 |
|||
Benign |
57 (82.6%) |
|||
Malignant |
12 (16.4%) |
|||
Previous Reconstruction |
0.691 |
|||
Billroth I |
22 (31.9%) |
|||
Billroth II |
47 (68.1%) |
|||
Approach |
0.957 |
|||
Open |
35 (50.7%) |
|||
Lap |
34 (49.3%) |
|||
Tumor Location |
0.955 |
|||
Anastomosis Site |
33 (47.8%) |
|||
Others |
36 (52.2%) |
|||
No. of Retrieved LNs |
0.180 |
|||
<15 |
29 (42.0%) |
|||
≥15 |
40 (58.0%) |
|||
Type of Histology |
0.267 |
|||
Differentiated |
23 (33.3%) |
|||
Undifferentiated |
46 (66.7%) |
|||
Serosal Invasion |
0.002 |
|||
Positive |
42 (60.9%) |
2.343 (1.095–5.186) |
0.036 |
|
Negative |
27 (39.1%) |
|||
Lymph Node Metastasis |
0.009 |
|||
Positive |
34 (49.3%) |
1.581 (0.916–3.228) |
0.068 |
|
Negative |
35 (50.7%) |
|||
TNM Stage |
0.002 |
|||
I+II |
41 (59.4%) |
|||
III |
28 (40.6%) |
2.276 (1.041–4.975) |
0.039 |
|
Adjuvant chemotherapy |
0.068 |
|||
Yes |
43 (62.3%) |
|||
No |
26 (37.7%) |
|||
We compared the cumulative survival between the two cohorts by grouping the patients by tumor stage. The survival time was not significantly different between the LATG and OTG groups for either stage I + II or the stage III subgroups (p = 0.542 and p = 0.774, respectively, Figure 3).
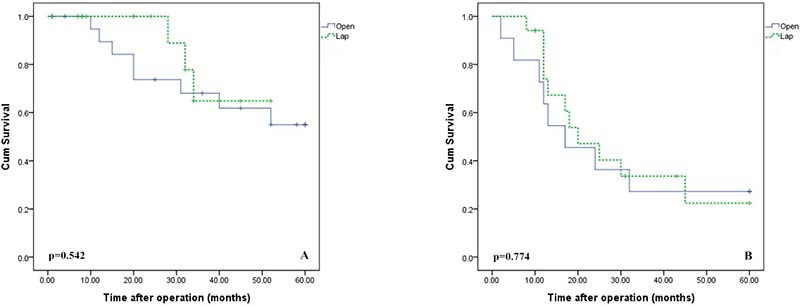
Figure 3: Survival curve for stage I+II (A) and stage III (B) RGC patients by laparoscopic or open surgery.
Of the 58 cases of advanced RGC, 29 were enrolled in each group. There was no significant difference in 5-year cumulative survival rates between the two cohorts, with a rate of 37.82% in the OTG group and 33.12% in the LATG group (p = 0.821).
Literature review
All of the case-control studies examining laparoscopic gastrectomy for RGC are listed in Table 4. Of the five investigations, four assessed based on early RGC. Regarding short-term intraoperative and postoperative efficacy, all five studies reported that LATG required a longer operation time but resulted in shorter postoperative hospital stays. Additionally, most studies reported more blood loss in the open cohorts than the laparoscopy cohorts. The results varied by study and were influenced by previous surgery in terms of the number of lymph nodes dissected, making it difficult to draw conclusions. The studies by Nagai, Son and Kwon all demonstrated similar 5-year cumulative survival rates between OTG and LATG cohorts; however, most of those patients presented with early stage disease.
Table 4: Summary of studies comparing open and laparoscopic gastrectomy for remnant gastric cancer
Author (year) |
Country |
Approach |
No. of Patients |
Early/Advanced Stage |
Overall 5-year Survival (%) |
No. of Retrieved LNs |
Blood Loss (g or ml) |
Time of Operation (mins) |
Hospital Stay (days) |
|---|---|---|---|---|---|---|---|---|---|
Nagai (2013) |
Japan |
Open |
10 |
5/5 |
72.9 |
15.9 |
746.3 |
270.5 |
24.9 |
Lap |
12 |
10/2 |
77.8 |
23.7 |
65.8 |
362.3 |
11.3 |
||
Son (2014) |
Korea |
Open |
17 |
4/13 |
60.3 |
22.3 |
184.1 |
170 |
9.3 |
Lap |
17 |
11/6 |
66.7 |
18.8 |
227.6 |
234.4 |
9.3 |
||
Kwon (2014) |
Korea |
Open |
58 |
35/23 |
100 |
7 |
193.1 |
203.3 |
9 |
Lap |
18 |
15/3 |
94.9 |
8 |
182.2 |
266.2 |
6 |
||
Kim (2014) |
Korea |
Open |
50 |
— |
— |
— |
— |
149.3 |
13.8 |
Lap |
17 |
13/4 |
— |
12.9 |
— |
197.2 |
11.1 |
||
Tsunoda (2014) |
Japan |
Open |
6 |
1/5 |
— |
7 |
893 |
289 |
24 |
Lap |
10 |
7/3 |
— |
22 |
55 |
325 |
13 |
||
Current Study |
China |
Open |
35 |
6/29 |
45.31 |
14.31 |
192.9 |
236.7 |
18.03 |
Lap |
34 |
5/29 |
37.96 |
19.41 |
98.53 |
195.3 |
13.88 |
DISCUSSION
Since Kitano [25] performed the first laparoscopic-assisted distal gastrectomy (LADG) in 1991, the procedure has been refined for over two decades. This technique has been increasingly adopted by surgeons as a treatment option for gastric cancer, especially for early stage disease. In 2005, Yamada [26] applied the technique to remnant stomach carcinoma by conducting the first laparoscopic-assisted gastrectomy for RGC. However, due to its low incidence and rapid disease progression [27] together with the adhesion and variation in regional anatomical structures and lymphatic flow [5, 28], the use of the laparoscopic approach has been limited. Nevertheless, there have been several retrospective studies reporting the feasibility of laparoscopic gastrectomy to treat RGC [16–21], with limited cases of minimally invasive surgery. In this investigation, we included 34 cases of laparoscopic-assisted gastrectomy for RGC, which is to date the largest laparoscopic sample included in a single-center retrospective clinical study.
Son et al. [16] reported more blood loss in the laparoscopic cohort with fewer dissected lymph nodes. This result was primarily due to eight open conversions in the laparoscopy. Other researchers [16–17, 19–21] reported that laparoscopic surgery requires a longer operating time. Our study observed less blood loss, shorter operation times and shorter postoperative hospital stays in the LATG group, and we believe the contradictory operation times were caused by the following reasons. First, there is a learning curve. Many surgeons are new to performing laparoscopic gastrectomy (LG) and accept the lengthy operation time because they perceive LG to be a complicated technique with a learning curve [29]. A study by Kunisaki et al. [30] focused on one surgeon’s learning curve with LDG and found that the operating time reduced to 230 min after 60 cases. Our department began performing laparoscopic surgery for primary gastric cancer in 2007. When the first laparoscopy for RGC was performed in May 2008, our team overcame the learning curve with increased technical skill. After ‘‘climbing’’ the learning curve, we observed that the operation time gradually decreased. The average operation time was 237 min after 218 patients and decreased to 196 min after completing 1380 cases [31]. Second, as previously mentioned, all 35 patients received OTG from 2007 to 2011; however, most patients received LTG after 2011. In addition, all of the laparoscopic surgeries were performed by the same team. A stable and knowledgeable team is important for performing LG, making the operation easier and faster. Furthermore, a possible reason that more lymph nodes were dissected using the minimally invasive approach was that laparoscopy provided clearer surgical vision, allowing the surgeon to access deeper regions for lymphadenectomy, such as the spleen hilum and suprapancreatic region. Of note, LATG patients had more No. 9, No. 11, and No. 10 LNs than did the OTG group (3.4 ± 1.5 vs. 2.6 ± 1.9, p = 0.085; 3.6 ± 1.8 vs. 3.1 ± 1.5, p = 0.167; 2.7 ± 1.1 vs. 2.0 ± 1.2, p = 0.231; respectively), but the differences were not statistically significant due to the small number of cases. Moreover, minimally invasive surgery causes minimal interference to the intestine and other non-operative areas, which might lead to faster postoperative recovery times and shorter hospital stays.
The disparity in 5-year cumulative survival rates was not statistically significant between the two cohorts, consistent with the results reported by Nagai, Son and Kwon. One point to note is that our 5-year cumulative survival rate was lower than other Japanese and Korean retrospective analyses [16–17, 19–21], primarily because the rate of advanced RGC in this study was 84.1%. By analyzing survival rates in 58 advanced RGC patients, we discovered that open and laparoscopic approaches yielded similar oncologic outcomes, providing preliminary clinical evidence for the efficacy and safety of laparoscopic surgery.
This study had some limitations. The nature of retrospective analysis inevitably results in patient selection bias. Research at a single medical center restricted the patient sample size and made it impossible to eliminate discrepancies between groups by using a propensity scoring match system. Short follow-up times in some cases may impact long-term survival rates. Furthermore, gastric cancer in China is more prevalent than in western countries and occurs in a population that is typically thinner. Experience is necessary before taking on this approach, as the same results would not be expected if the surgery were performed by less experienced surgeons or in an obese patient population. This situation is particularly true given the male predominance of this disease, as foregut surgery is more challenging in obese men than in obese women. Broad application of this approach without appropriate training could cause patient harm. However, we collected all of the RGC cases in our center within a relatively short period, which might reduce some selection bias. To provide stronger clinical evidence, multi-center, well-designed randomized controlled trials comparing short-term and long-term outcomes between laparoscopy-assisted gastrectomy and open gastrectomy in a larger number of patients are required.
MATERIALS AND METHODS
Patients
A database search of patients who received surgery for RGC at Fujian Medical University Union Hospital between Dec 2007 and Apr 2014 was performed using the hospital’s retrospective gastric cancer database and electronic medical records. As shown in Figure 1, 105 cases were selected based on the following inclusion criteria: 1. RGC was diagnosed preoperatively by endoscopy and pathology. 2. There was no evidence of metastasis in the lung, liver or peritoneum by chest or abdominal computed tomography (CT) scan or abdominal ultrasonography. 3. Radical total gastrectomy with lymph node dissection was performed. 4. Complete information from the electronic medical records related to surgery and perioperative data were obtained. The exclusion criteria were as follows: 1. advanced RGC with unresectable adjacent organ invasion of the liver, spleen, transverse colon or pancreas; 2. peritoneal or distant metastasis; and 3. surgery was performed using the thoracoabdominal approach. All 69 patients enrolled in this study were categorized into either the laparoscopic group (34 cases) or the open group (35 cases) based on the procedure performed. Adjuvant chemotherapy with 5-fluorouracil (5-FU)-based regimens was recommended to all eligible patients except those with stage Ia or Ib cancer. Collectively, 43 patients (62.3%) received 5-FU-based adjuvant chemotherapy. The Ethics Committee of Fujian Medical University Union Hospital approved this study, and all of the patients provided signed informed consent preoperatively.
Surgical procedure
All of the patients were treated by a single experienced surgeon who performed more than 2,000 cases of laparoscopic gastrectomy for gastric cancer between 2007 and 2014. All of the patients received a remnant gastrectomy with lymph node dissection. Roux-en-Y esophagojejunostomy was performed after the completion of a total gastrectomy.
We began performing LADG for gastric cancer in 2007. We expanded our indications to LATG in 2008 and to complete laparoscopic total remnant gastrectomy (LTRG) for early RGC in May 2008. We began performing LTRG for preoperative stage II to IIIA RGC [American Joint Committee on Cancer (AJCC), 7th edition] in 2011. Thereafter, LTRG was indicated for all operable RGC. The remaining 35 patients received OTG between 2007 and 2011. Preoperative endoscopic ultrasonography and abdominal computed tomography were performed to diagnose invasion depth and lymph node staging.
A five-port approach was used for the laparoscopy group. First, a 12-mm trocar was placed in the left lateral abdomen to avoid intestinal injury during CO2 insufflation of the abdominal cavity to a pressure of 12–14 mmHg. The intestines or greater omentum often adhered to the previous surgical incision scar. After insufflation, a 10-mm trocar was inserted into the infra-umbilical area as an observation port, and a 5-mm trocar was placed in the left hypochondriac region without adhesions. These three trocars were used to perform adhesiolysis at the previous incision site and the right upper abdominal wall. An ultrasonically activated coagulating scalpel (Harmonic Scalpel, Ethicon Endo Surgery Inc.) was used for adhesiolysis and radical lymphadenectomy. After completing the total gastrectomy, extracorporeal Roux-en-Y esophagojejunostomy was performed via an 8-cm upper midline abdominal incision. The lymph node dissection procedure is described in detail elsewhere [22, 23].
Follow-up
Patients returned every 3 or 6 months for regular physical examinations, laboratory blood tests, and chest and abdominal X-rays. Patients received CT and/or abdominal ultrasound (US) every 6 months. Patients received upper gastrointestinal endoscopies annually. If necessary, further evaluation, such as positron emission tomography or magnetic resonance imaging, was initiated to better clarify recurrence.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Categorical data were compared using Chi-square tests and means using Student’s t-test. Survival rate was calculated according to the Kaplan-Meier method via the log-rank test. A Cox proportional hazards model was constructed for multivariate analysis of prognosis. P < 0.05 was considered to be statistically significant.
Literature search
Through the PubMed database, a literature search was conducted to identify English studies reporting clinical research related to laparoscopic gastrectomy for remnant gastric cancer before December 2014. The search terms used were as follows: laparoscopic AND gastrectomy (“remnant gastric cancer” or “gastric stump cancer”).
CONCLUSIONS
In summary, our study demonstrated that laparoscopic gastrectomy for RGC led to better short-term outcomes and similar oncologic results as open surgery. We also found that the same results were achieved for advanced RGC. For experienced surgeons, laparoscopic surgery may be a reasonable approach for managing RGC.
ACKNOWLEDGMENTS
This study was supported by grants Scientific and technological innovation joint capital projects of Fujian Province (2016Y9031), National Key Clinical Specialty Discipline Construction Program of China (No. [2012]649),Youth scientific research subject of Fujian provincial health and family planning commission (No. 2015-1-37), and QIHANG funds of Fujian Medical University (No.2016QH025).
CONFLICTS OF INTEREST
All of the authors declare that they have no potential commercial conflicts of interest relevant to this article.
REFERENCES
1. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–12.
2. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011; 14:113–23.
3. Welvaart K, Warnsinck HM. The incidence of carcinoma of the gastric remnant. J Surg Oncol. 1982; 21:104–106.
4. Nozaki I, Nasu J, Kubo Y, Tanada M, Nishimura R, Kurita A. Risk factors for metachronous gastric cancer in the remnant stomach after early cancer surgery. World J Surg. 2010; 34:1548–1554.
5. Kaneko K, Kondo H, Saito D, Shirao K, Yamaguchi H, Yokota T, Yamao G, Sano T, Sasako M, Yoshida S. Early gastric stump cancer following distal gastrectomy. Gut. 1998; 43:342–344.
6. Sinning C, Schaefer N, Standop J, Hirner A, Wolff M. Gastric stump carcinoma - epidemiology and current concepts in pathogenesis and treatment. Eur J Surg Oncol. 2007; 33:133–139.
7. Lundegardh G, Adami HO, Helmick C, Zack M, Meirik O. Stomach cancer after partial gastrectomy for benign ulcer disease. N Engl J Med. 1988; 319:195–200.
8. Arnthorsson G, Tulinius H, Egilsson V, Sigvaldason H, Magnusson B, Thorarinsson H. Gastric cancer after gastrectomy. Int J Cancer. 1988; 42:365–367.
9. Caygill CP, Hill MJ, Kirkham JS, Northfield TC. Mortality from gastric cancer following gastric surgery for peptic ulcer. Lancet. 1986; 1:929–931.
10. Tersmette AC, Offerhaus GJ, Tersmette KW, Giardiello FM, Moore GW, Tytgat GN, Vandenbroucke JP. Meta-analysis of the risk of gastric stump cancer: detection of high risk patient subsets for stomach cancer after remote partial gastrectomy for benign conditions. Cancer Res. 1990; 50:6486–6489.
11. Mezhir JJ, Gonen M, Ammori JB, Strong VE, Brennan MF, Coit DG. Treatment and outcome of patients with gastric remnant cancer after resection for peptic ulcer disease. Ann Surg Oncol. 2011; 18:670–676.
12. Adachi Y, Shiraishi N, Shiromizu A, Bandoh T, Aramaki M, Kitano S. Laparoscopy-assisted Billroth I gastrectomy compared with conventional open gastrectomy. Arch Surg. 2000; 135:806–810.
13. Shimizu S, Uchiyama A, Mizumoto K, Morisaki T, Nakamura K, Shimura H, Tanaka M. Laparoscopically assisted distal gastrectomy for early gastric cancer: is it superior to open surgery? Surg Endosc. 2000; 14:27–31.
14. Lee SI, Choi YS, Park DJ, Kim HH, Yang HK, Kim MC. Comparative study of laparoscopy-assisted distal gastrectomy and open distal gastrectomy. J Am Coll Surg. 2006; 202:874–880.
15. Kodera Y, Fujiwara M, Ohashi N, Nakayama G, Koike M, Morita S, Nakao A. Laparoscopic surgery for gastric cancer: a collective review with meta-analysis of randomized trials. J Am Coll Surg. 2010; 211:677–686.
16. Son SY, Lee CM, Jung DH, Lee JH, Ahn SH, Park do J, Kim HH. Laparoscopic completion total gastrectomy for remnant gastric cancer: a single-institution experience. Gastric Cancer. 2015; 18:177–182.
17. Nagai E, Nakata K, Ohuchida K, Miyasaka Y, Shimizu S, Tanaka M. Laparoscopic total gastrectomy for remnant gastric cancer: feasibility study. Surg Endosc. 2014; 28:289–296.
18. Jiang X, Hiki N, Nunobe S, Nohara K, Kumagai K, Sano T, Yamaguchi T. Laparoscopy-assisted subtotal gastrectomy with very small remnant stomach: a novel surgical procedure for selected early gastric cancer in the upper stomach. Gastric Cancer. 2011; 14:194–199.
19. Kwon IG, Cho I, Guner A, Choi YY, Shin HB, Kim HI, An JY, Cheong JH, Noh SH, Hyung WJ. Minimally invasive surgery for remnant gastric cancer: a comparison with open surgery. Surg Endosc. 2014; 28:2452–2458.
20. Kim HS, Kim BS, Lee IS, Lee S, Yook JH, Kim BS. Laparoscopic gastrectomy in patients with previous gastrectomy for gastric cancer: a report of 17 cases. Surg Laparosc Endosc Percutan Tech. 2014; 24:177–182.
21. Tsunoda S, Okabe H, Tanaka E, Hisamori S, Harigai M, Murakami K, Sakai Y. Laparoscopic gastrectomy for remnant gastric cancer: a comprehensive review and case series. Gastric Cancer. 2016; 19:287–92.
22. Huang CM, Chen QY, Lin JX, Zheng CH, Li P, Xie JW, Wang JB, Lu J, Yang XT. Laparoscopic Suprapancreatic Lymph Node Dissection for Advanced Gastric Cancer Using a Left-Sided Approach. Ann Surg Oncol. 2015; 22:2351.
23. Jia-Bin W, Chang-Ming H, Chao-Hui Z, Ping L, Jian-Wei X, Jian-Xian L. Laparoscopic spleen-preserving No. 10 lymph node dissection for advanced proximal gastric cancer in left approach: a new operation procedure. World J Surg Oncol. 2012; 10:241.
24. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004; 240:205–213.
25. Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994; 4:146–148.
26. Yamada H, Kojima K, Yamashita T, Kawano T, Sugihara K, Nihei Z. Laparoscopy-assisted resection of gastric remnant cancer. Surg Laparosc Endosc Percutan Tech. 2005; 15:226–229.
27. Imada T, Rino Y, Hatori S, Shiozawa M, Takahashi M, Amano T, Kondo J, Kobayashi O, Sairenji M, Motohashi H. Clinicopathologic differences between early gastric remnant cancer and early primary gastric cancer in the upper third of the stomach. Hepatogastroenterology. 2000; 47:1186–1188.
28. Inomata M, Shiraishi N, Adachi Y, Yasuda K, Aramaki M, Kitano S. Gastric remnant cancer compared with primary proximal gastric cancer. Hepatogastroenterology. 2003; 50:587–591.
29. Jung DH, Son SY, Park YS, Shin DJ, Ahn HS, Ahn SH, Park DJ, Kim HH. The learning curve associated with laparoscopic total gastrectomy. Gastric Cancer. 2016; 19:264–272.
30. Kunisaki C, Makino H, Yamamoto N, Sato T, Oshima T, Nagano Y, Fujii S, Akiyama H, Otsuka Y, Ono HA, Kosaka T, Takagawa R, Shimada H. Learning curve for laparoscopy-assisted distal gastrectomy with regional lymph node dissection for early gastric cancer. Surg Laparosc Endosc Percutan Tech. 2008; 18:236–41.
31. Lin JX, Huang CM, Zheng CH, Li P, Xie JW, Wang JB, Jun L, Chen QY, Lin M, Tu R. Evaluation of laparoscopic total gastrectomy for advanced gastric cancer: results of a comparison with laparoscopic distal gastrectomy. Surg Endosc. 2016; 30:1988–98.