
INTRODUCTION
In recent decades we have witnessed significant improvements in medical care and continuous development of medical technology. As a result, a higher life expectancy can be observed in most populations [1]. The elderly constitute a high-risk group of candidates for surgery, most commonly with accompanying comorbidities and reduced health capacity [2]. In addition, age is one of the main risk factors for cancer development, including pancreatic neoplasms [3]. A 2016 report by Ferlay et al. suggested that in EU countries more people annually from pancreatic cancer than breast cancer [4]. After lung and colorectal cancers, pancreatic cancer may soon become the third most common cause of cancer-related death in the European Union. According to statistics, more than ¾ of patients with pancreatic cancer and other periampullary neoplasms are older than 60 years of age and more than a half are above 70 years of age. This means that the number of elderly patients seeking help from surgery will inevitably continue to rise [5, 10–53].
Improvements in the operative technique of pancreatoduodenectomy (PD), along with improvements in perioperative care, have led to reduced mortality [6]. The rate, however, of postoperative complications of 40% or above is still relatively high [7]. Increased overall mortality among elderly population remains the greatest concern. In fact, due to the aggressive nature of the tumor (median survival in unresected pancreatic cancer is less than 12 months), a lack of alternative treatment options, and an ageing population, there is less reluctance to perform PD in elderly candidates than might otherwise be expected [8, 9]. Therefore, it is important to evaluate the risk of mortality, morbidity and adverse events in elderly patients undergoing PD. We aimed to review systematically the available published literature and conduct a meta-analysis comparing the outcomes of PD in the elderly with the young.
RESULTS
An initial reference search yielded 2,043 articles. After removing 503 duplicates, 1,540 articles were evaluated through titles and abstracts. This produced 143 articles suitable for full-text review. Finally, 45 articles were studies eligible for data extraction, with a combined total of 21,295 patients (3,824 from the older population and 17,471 from the younger population) [5, 10–53]. A flowchart of the analyzed studies is presented in Figure 1. Since the majority of studies scored at least 6 out of 9 in Newcastle-Ottawa Scale (NOS), the average quality of studies included is high. Baseline information about the analyzed studies is presented in Supplementary Table 1. The funnel plot of publication bias is presented in Supplementary Figure 1. The cone is asymmetrical which may suggest a publication bias for studies regarding <70 vs. >70 groups. This possible bias, however, is only associated with articles that had a small numbers of participants, and therefore, would have had little impact on results in general.
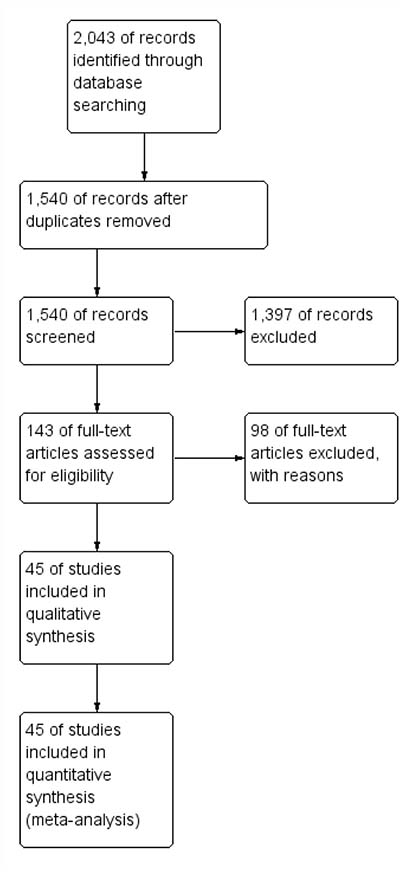
Figure 1: PRISMA flowchart.
Mortality was reported in 42 studies, with a total of 11,615 patients (2,180 patients from the elderly population and 9,435 patients from the younger population). There was a significantly lower rate of mortality among younger patients: 213/9435 (2.26%) vs. 99/2180 (4.54%) among older patients, RR: 2.23; 95% CI 1.74–2.87, p < 0.001 (Figure 2). Subgroup analysis revealed a similar pattern for the age cut-offs 80, 75, and 70, but not 65; however, the 65-year old cut-off was used in only 2 studies, with a low number of patients responsible for 1.2% of the total effect.
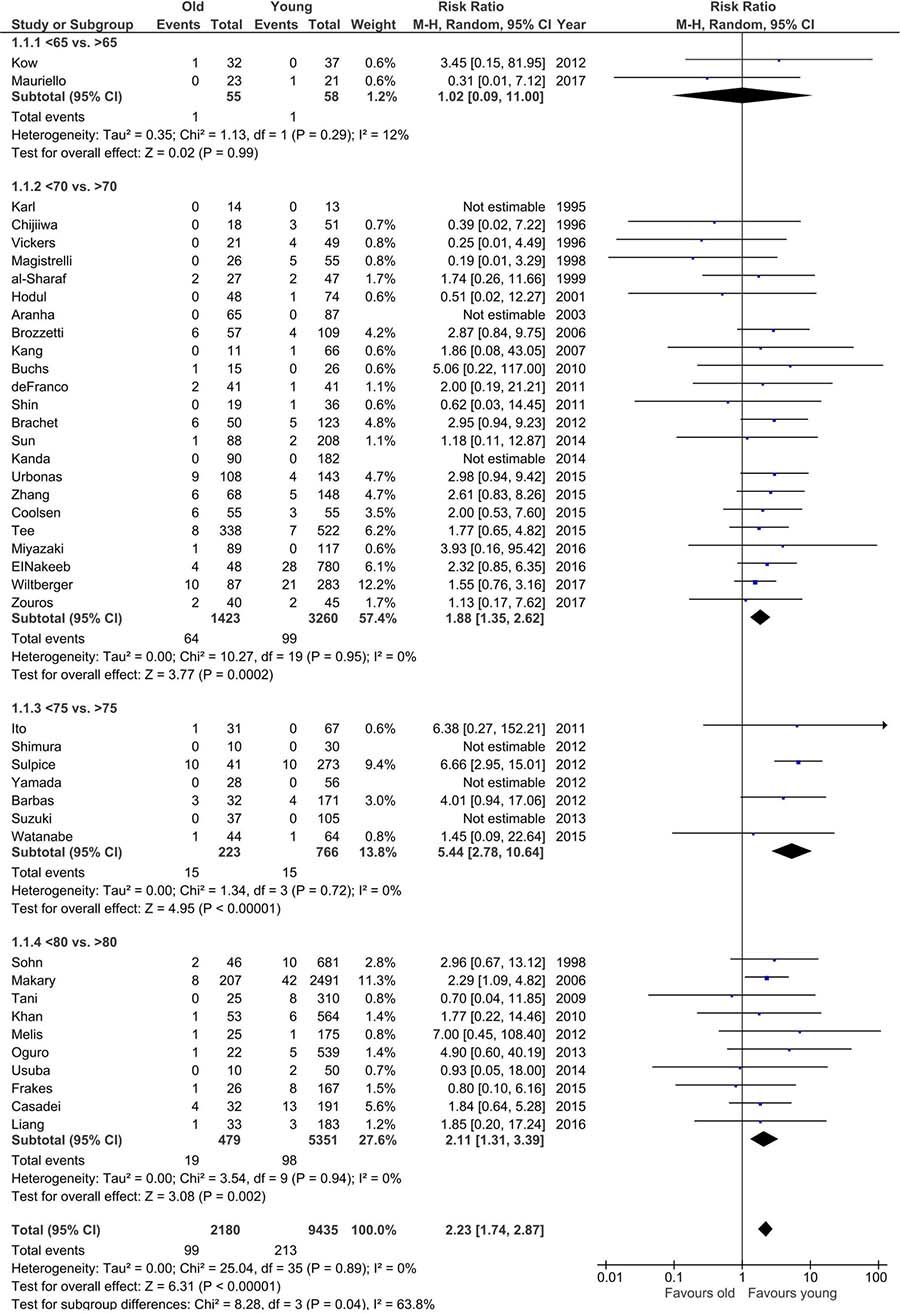
Figure 2: Pooled estimates of mortality comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Overall morbidity was reported in 38 studies, involving 19,043 patients (3,301 older patients and 15,742 younger patients). A significant difference was found between older and younger patients: 1,559/3,301 (47.23%) vs. 6,194/15,742 (39.35%): RR 1.17; 95% CI 1.12–1.24, p < 0.001. There were no differences in studies using age cut-offs of 65 or 75 years (Figure 3).
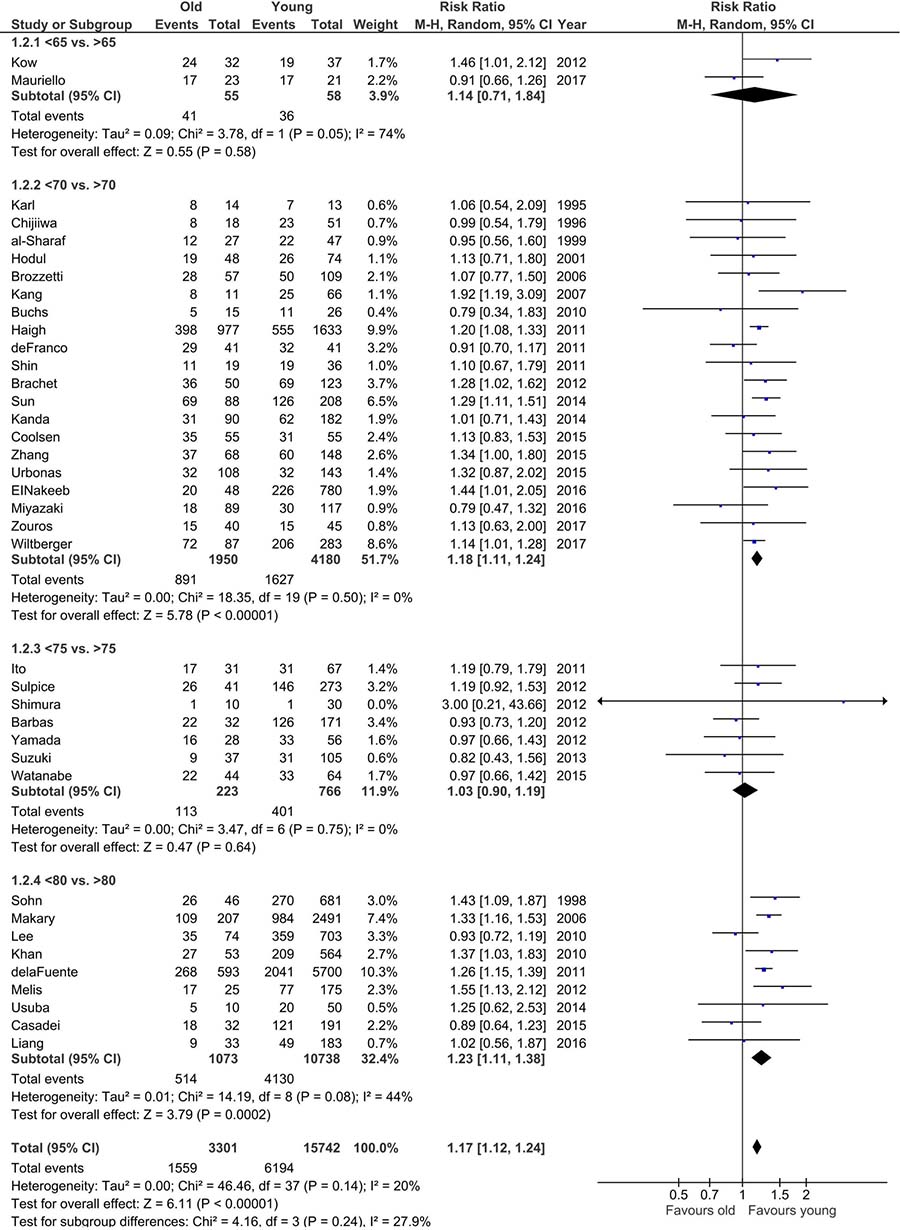
Figure 3: Pooled estimates of overall morbidity comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Pancreatic fistula occurrence was reported in 37 studies. No significant differences between older and younger populations were found: 372/2,001 (18.59%) vs. 1,399/9,141 (15.3%), p = 0.27; 95% CI 0.95–1.20 (Figure 4). Heterogeneity was low except for studies that had 65 years old as the age cutoff (I2 = 90%).
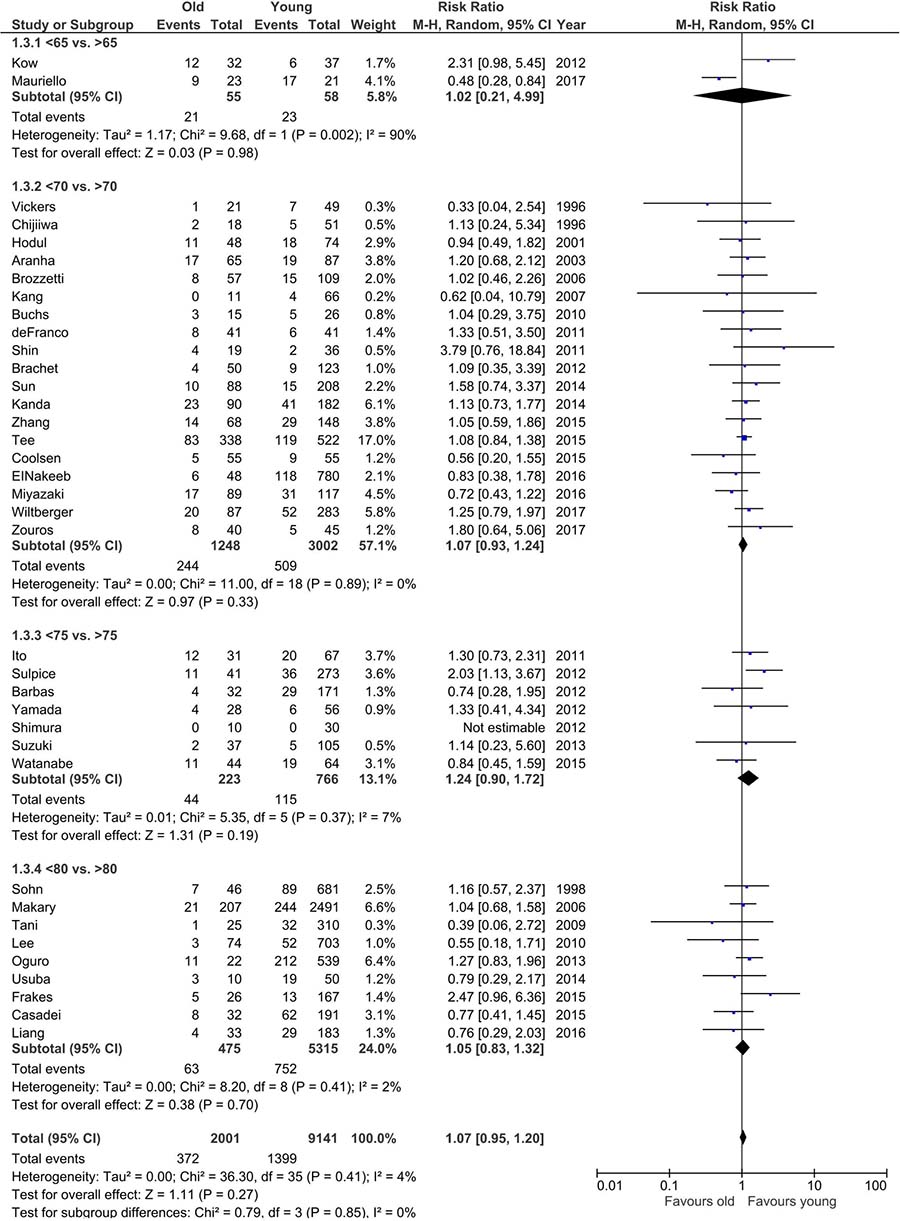
Figure 4: Pooled estimates of pancreatic fistula comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Bile leakage was reported in 26 studies. Older patients did not differ significantly from younger patients: 30/1,157 (2.59%) vs. 232/6,899 (3.36%), p = 0.81; 95% CI 0.71–1.54; the same was true for subgroup analysis (Figure 5). There was no heterogeneity across studies.
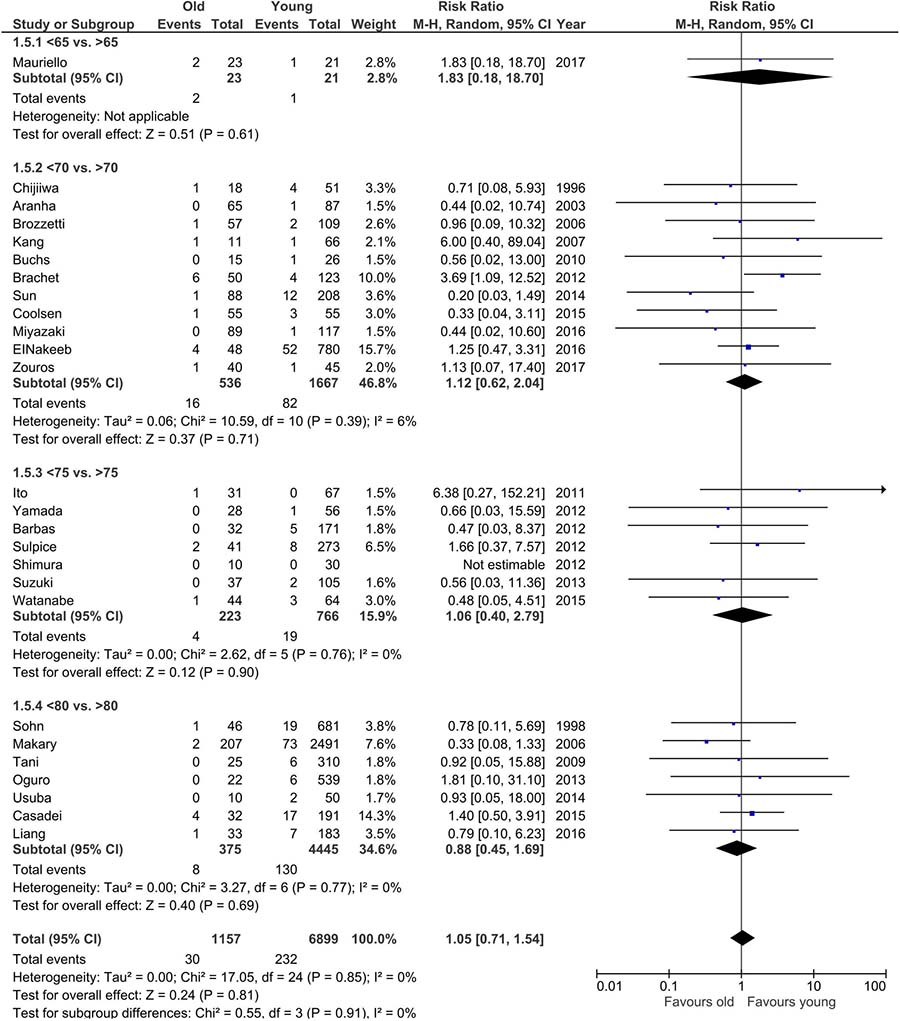
Figure 5: Pooled estimates of bile leakage comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Delayed gastric emptying (DGE) was reported in 33 studies, looking at a total of 9,748 patients. It occurred more frequently among older patients: 345/1,807 (19.09%) vs. 1,328/7,941 (16.72%); RR = 1.17 95% CI 1.03–1.33, p = 0.01. Heterogeneity in general was low, although it was moderate (I2 = 52%) for the highest age cut-off. Subgroup analysis showed that the difference was significant only for the age cut-off of 70 years old (Figure 6).
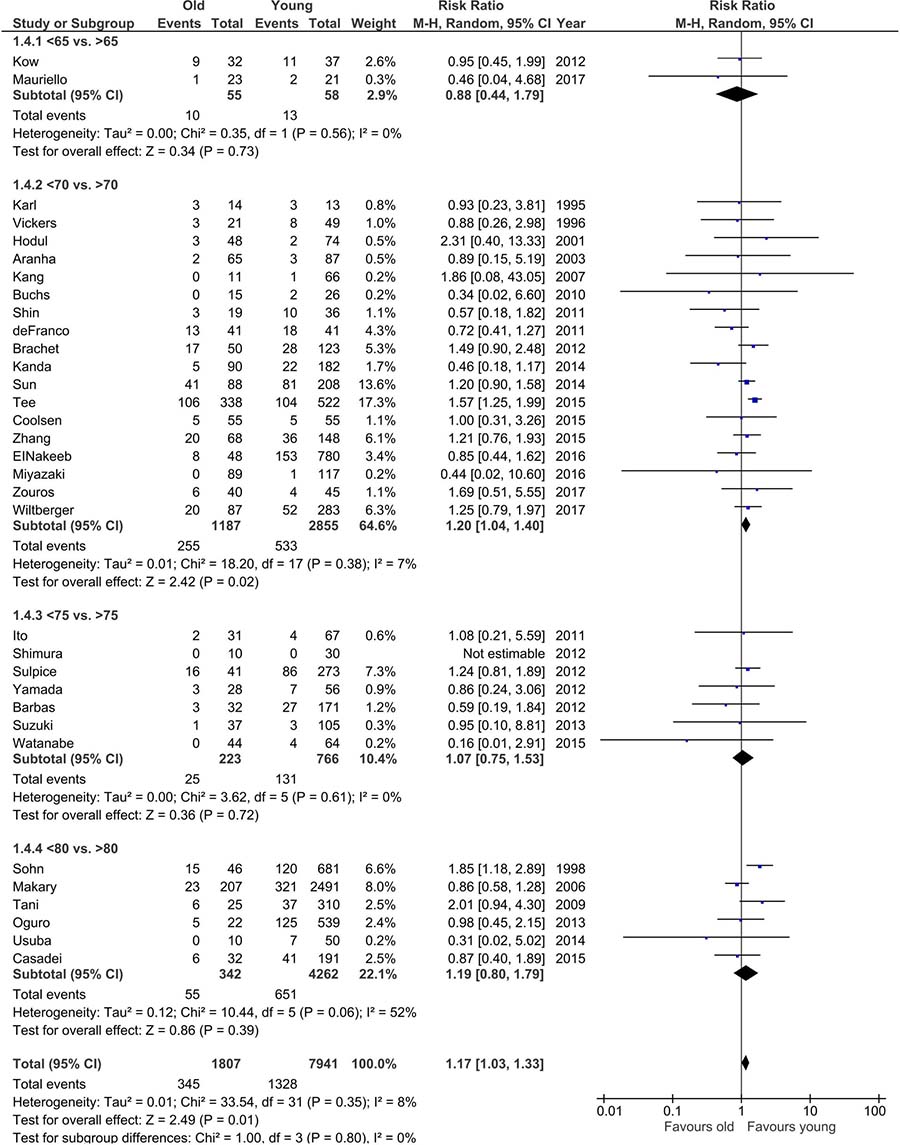
Figure 6: Pooled estimates of delayed gastric emptying comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Postoperative hemorrhage was reported in 28 studies and no significant differences were observed: 108/1,474 (7.33%) vs. 276/4,623 (5.97%), p = 0.08; 95% CI 0.98–1.52 (Figure 7).
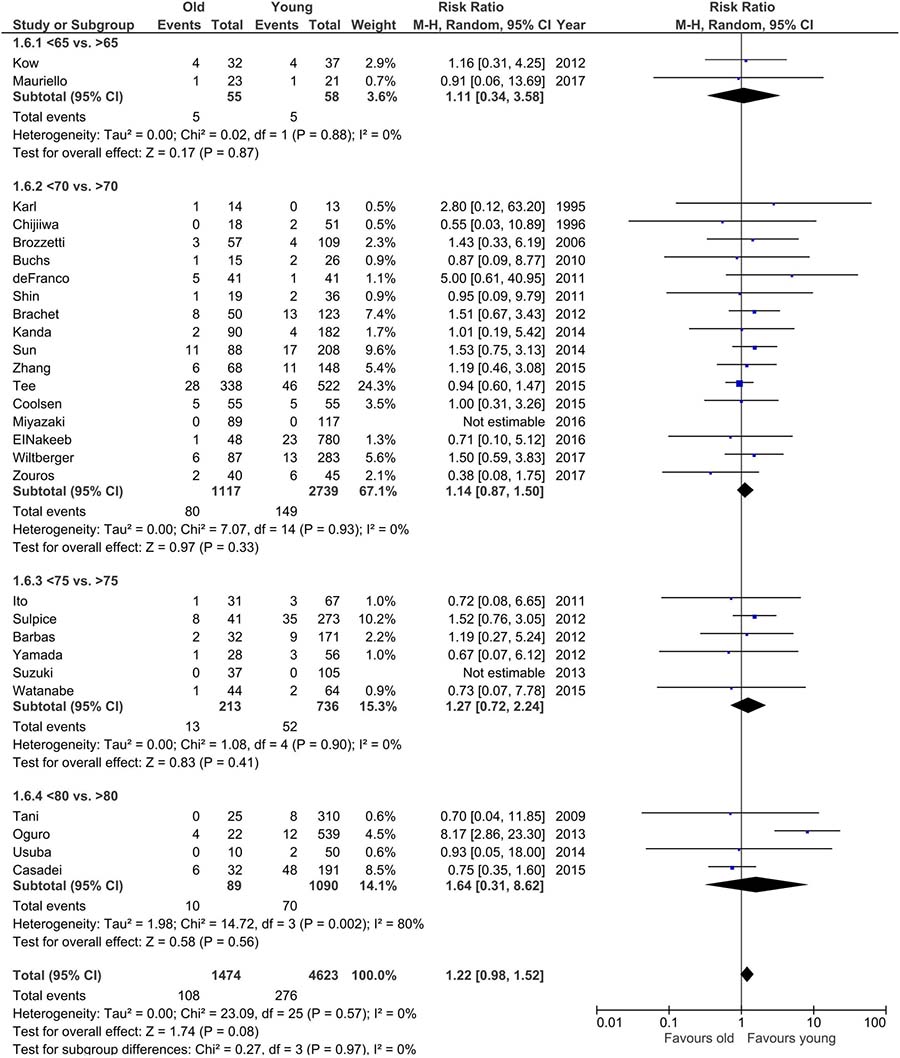
Figure 7: Pooled estimates of postoperative hemorrhage comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Surgical site infections (SSI) were reported in 26 studies and occurred more frequently in older patients 220/1,336 (16.47%) vs. 669/6,652 (10.06%): RR 1.21; 95% CI 1.05–1.41, p = 0.009. Subgroup analysis revealed a significant difference only for the age cut-off of 70 years old. This group comprised almost 70% of analyzed patients. There was no heterogeneity within age cut-off subgroups or across them (Figure 8).
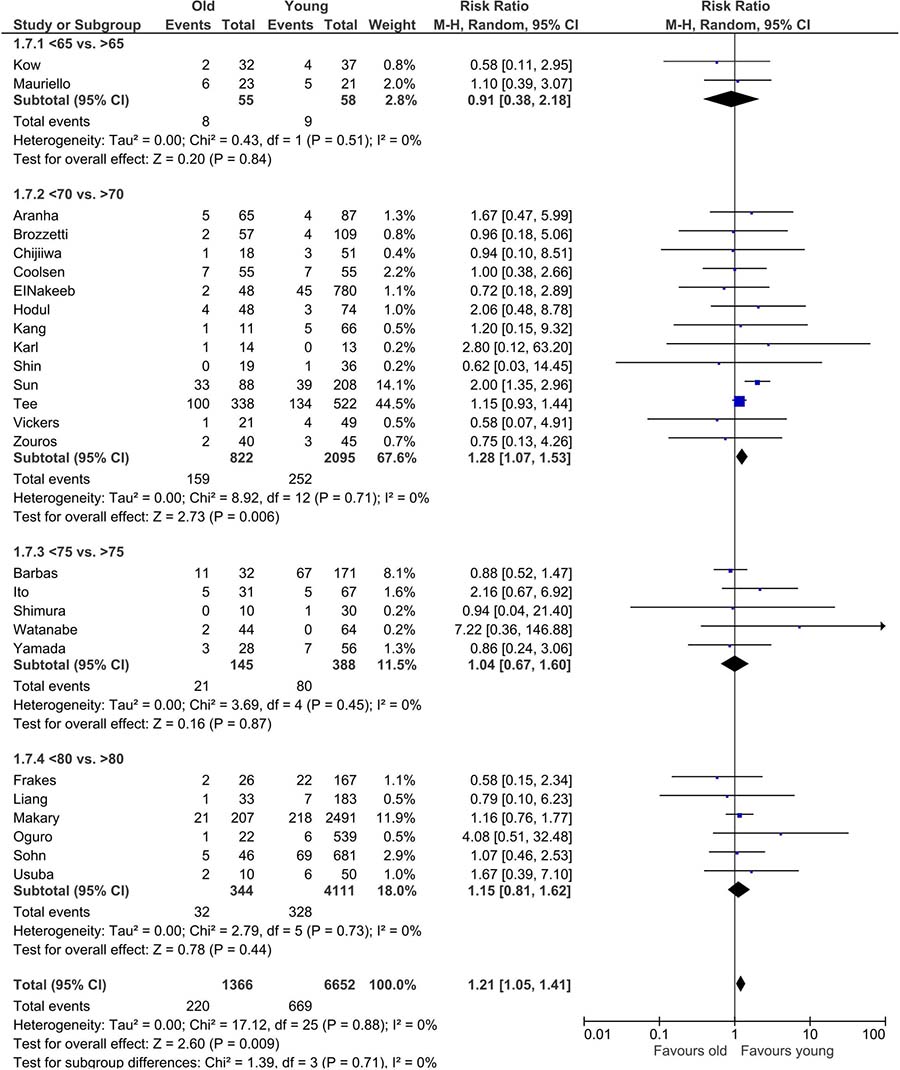
Figure 8: Pooled estimates of surgical site infection comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Pulmonary complications were reported in 31 studies and cardiovascular complications were reported in 23 studies. There were significant differences in the prevalence of pulmonary complications: 144/1,755 (8.21%) among older patients vs. 281/8,411 (3.34%) younger patients, RR: 1.71; 95% CI 1.39–2.11, p < 0.001. Subgroup analysis revealed no differences in studies with an age cut-off of 65 years old. There was no heterogeneity within the subgroups; however, a moderate heterogeneity was present across them. Cardiovascular complications occurred more frequently among older patients (172/2,019 [8.52%] vs. 248/11,402 [2.18%]); RR: 2.62; 95% CI 2.12–3.23, p < 0.001. Subgroup analysis revealed significant differences for the age cut-offs of 70 and 80 years old; heterogeneity was low (Figures 9 and 10).
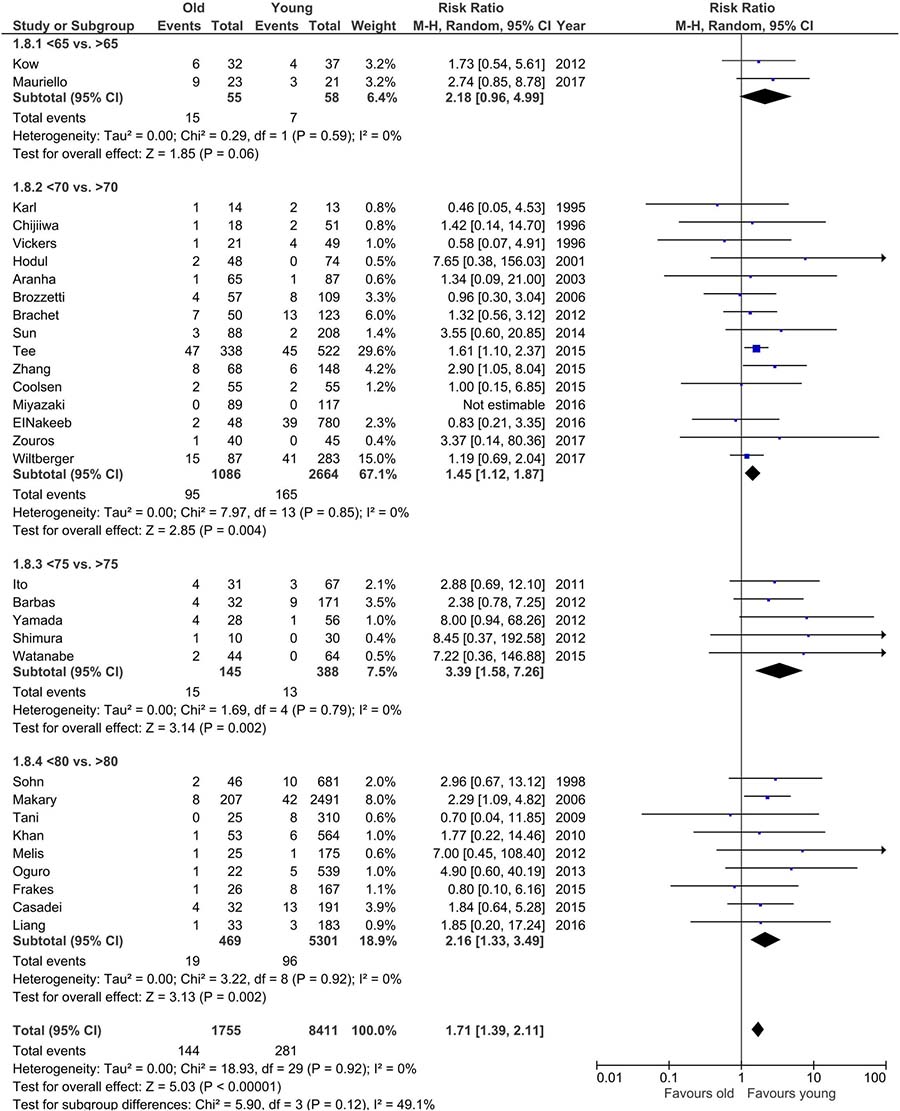
Figure 9: Pooled estimates of pulmonary complications comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
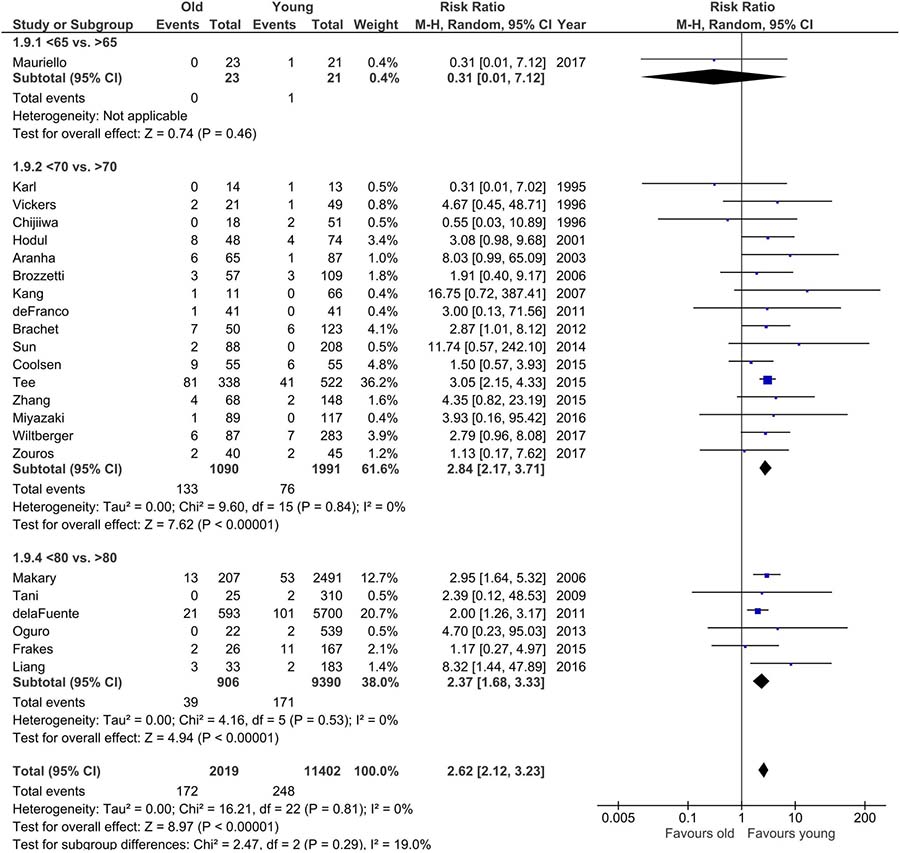
Figure 10: Pooled estimates of cardiovascular comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Length of hospital stay (LOS) was reported in 35 studies; however, 6 of these compared more than 2 groups, rendering them ineligible for meta-analysis. We therefore decided to exclude these studies from our evaluation of this parameter. In the end, our analysis of LOS covered 13,986 patients and revealed significant differences among studied groups. LOS of elderly patients was longer than younger patients: MD: 1.21; 95% CI 0.51–1.91, p < 0.001. Subgroup analysis revealed significant differences for the age cut-offs of 65 and 80 years old. Heterogeneity within subgroups ranged from low to high, with the overall heterogeneity being high, I2 = 77% (Figure 11).
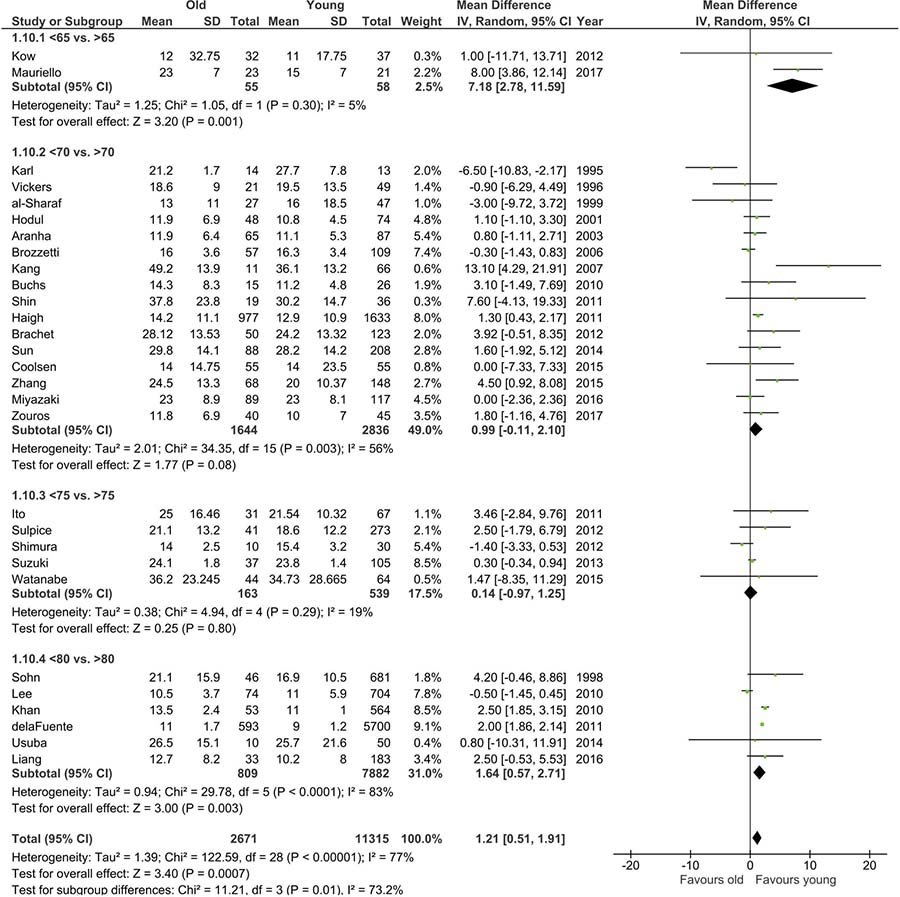
Figure 11: Pooled estimates of length of hospital stay comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom LOS.
R0 for pancreatic ductal adenocarcinoma was only reported in 13 studies. There were no differences between older and younger patients, 427/588 (72.62%) vs. 1,794/2,476 (72.46%), p = 0.92; 95% CI 0.82–1.25. Heterogeneity was moderate, I2 = 51% (Figure 12).
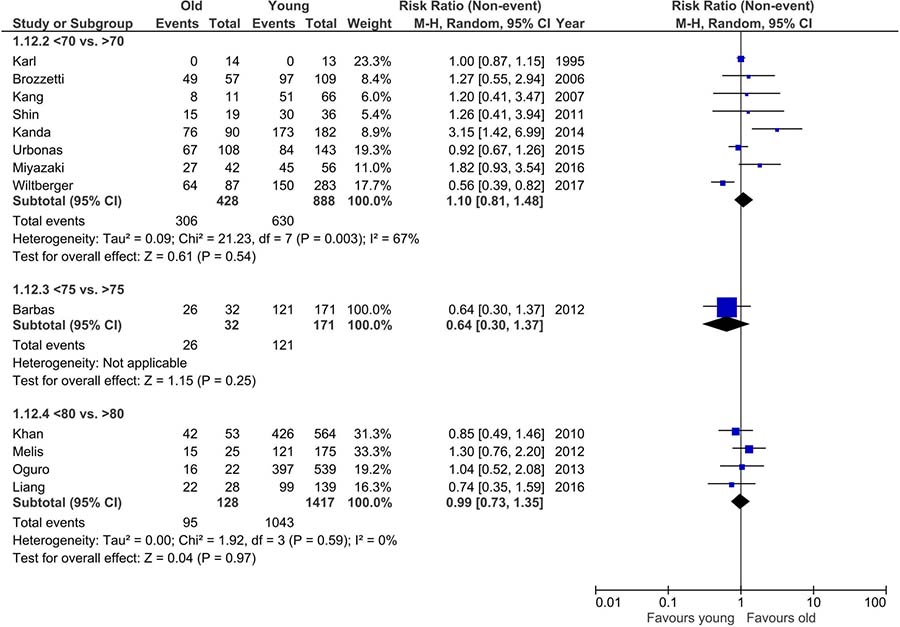
Figure 12: Pooled estimates of R0 resection rate comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
Readmission was reported in only 8 studies and no age-related differences were observed (Figure 13).
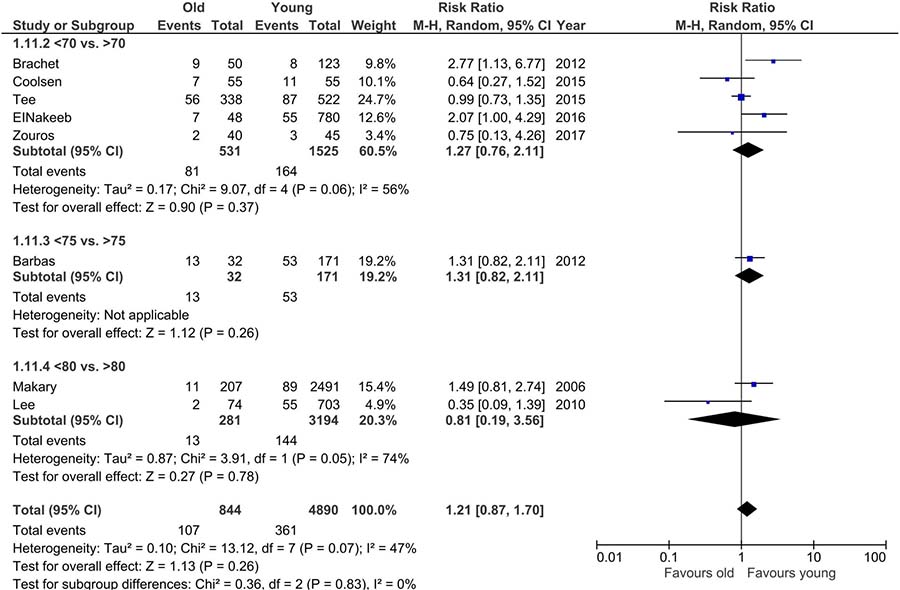
Figure 13: Pooled estimates of readmissions comparing elderly population vs. younger population. CI confidence interval, df degrees of freedom.
DISCUSSION
Changes in global demographics and an increase in the prevalence of gastrointestinal tumors lead to a rise in the number of extensive surgeries on older patients. This is particularly evident for pancreatic cancer. As long as other treatment strategies remain insufficient, we rely on radical surgery, the only potential cure of pancreatic head malignancies. For this reason, surgery ought to be considered as a valid treatment option for every patient with pancreatic head malignancy, regardless of age.
Our systematic review of 45 studies has shown that among pancreatoduodenectomy patients both postoperative mortality and postoperative morbidity are higher for older patients. An increased rate of non-surgical complications and a prolonged LOS were observed among older patients. The patient’s age does not seem to influence surgical complications related to the procedure itself, such as the rate of fistula, bile leakage, or postoperative hemorrhage. Higher rates of DGE and SSI, however, were observed in the older population.
Patients were eligible based on pancreatic cancer, other tumors and other indications. When analyzing these indications for pancreatoduodenectomy, a slightly larger portion of the elderly candidates (59%/36%/5%) had cancer in comparison to the younger candidates (52%/39%/9%). However, this difference was not statistically significant. Meta-analysis of all studies reporting mortality confirmed that the risk of perioperative death among older patients is more than twice as high as compared to younger patients (4.54% vs. 2.26%). This was also observed in the subgroup analysis, when different age cut-off points were set. This should be raised during pre-surgery consultations with older patients. Despite the clear difference, mortality among older patients is still considerably low, confirming the current theory that pancreatoduodenectomy is associated with relatively low mortality, even in high-risk patients, despite being one of the most complex and extensive abdominal surgeries, it. On the other hand, the low mortality rate in the included studies is not in line with the data from national databases. According to these databases the mortality rate in the elderly population is usually higher, exceeding even 10% [54, 55]. This disparity is probably due to the inclusion of low-volume centers reporting increased mortality, whereas most of the included studies in our meta-analysis originated from high-volume centers. It is well established that the annual patient volume of institutions and surgeons is strongly correlated with postoperative mortality [56–58]. Unfortunately, the data on the annual volume was only provided in the minority of included studies and none of them specified the surgeon’s annual volume. In addition, a large proportion of the studies were comprised of patients from relatively low volume centers (Supplementary Table 1). On one hand this may bias the results (lower volume = more complications); on the other, it reflects the real clinical situation worldwide, where the majority of PDs are being operated in low volume centres. Even while taking these findings into consideration it seems, that in terms of mortality, the benefits of undergoing surgery for pancreatic head malignancy regardless of age still outweigh the risks. The median survival time in unresected cancer patients can be as low as 12 months, and this is only when palliative chemotherapy is administered [8, 59–61]. Unfortunately, the majority of elderly patients are not, in any way, fit for the most aggressive regimens of chemotherapy. At best, the dose must be reduced due to its toxicity [62–64]. Higher mortality among the elderly should also be taken into consideration in preoperative evaluation of patients with tumors that have low or undefined malignant potential. The best treatment strategy for these older patients is yet to be established.
Although postoperative mortality has decreased over the last two decades, morbidity related to pancreatoduodenectomy still remains a serious problem. In our meta-analysis we have shown that the overall complication rate was higher in the elderly (47.23% vs 39.35%). Interestingly, when specific complications were analyzed, it was observed that older age is associated mainly with non-surgical complications as well as DGE and SSI, whereas the rate of all other complications typical for pancreatoduodenectomy (fistula, bile leakage, and postoperative hemorrhage) remained comparable. The relationship between pulmonary disease, cardiovascular disease, and the elderly can help explain differences in postoperative deaths in our analysis [65]. This increase in postoperative deaths is probably associated with a higher prevalence of comorbidities (mainly coronary artery disease, chronic obstructive pulmonary disease, hypertension, liver disease and vascular disease) among the elderly and reduced preoperative care combined with great surgical trauma related to PD [42]. We did not perform an in depth comparison of serious comorbidities between groups; however, they all may result in cardiorespiratory failure, leading to ICU admission in a significant proportion of cases [2, 65]. On the other hand, the insignificant difference in surgical complications may encourage surgeons to perform PD in patients regardless of age. As with every complex and extensive surgical procedure, it is all about common sense and patients’ quality of life. Since the outcomes are mainly influenced by non-surgical morbidity, other strategies to improve outcomes should be favored. There is, for instance, strong evidence that the implementation of enhanced recovery after surgery (ERAS) protocols help reduce postoperative surgical trauma [41, 66–68]. ERAS is a multimodal, multidisciplinary approach to the care of the surgical patient that incorporates several pre-, intra-, and postoperative items. When combined together, these are beneficial in terms of LOS, as well as, non-surgical morbidity as seen in other surgical disciplines [69–71]. Although a majority of the changes in ERAS protocol run counter to surgical dogmas and common beliefs, strong scientific evidence supports this modern perioperative approach. In our review, some aspects of perioperative care and resection technique were not investigated. Although there is still a lot of controversy over the use of minimally invasive surgery in pancreatic head resection, it is an alternative strategy that should be investigated specifically in relation to elderly patients [7, 72–75].
A 1.2-days longer LOS was observed in the older group. However, this small difference could be a result of multiple variables and, in fact, seems to be of little clinical relevance, considering the fact that PD is associated with LOS as high as 20 days. What seems to be more important is that once the elderly patient is discharged from surgical ward the risk of readmission is similar to the younger group. In this meta-analysis, readmissions were comparable between groups. However, this finding was based on a limited number of studies and the heterogeneity was moderate.
Our review has some limitations. Apart from the age, we did not precisely analyze demographic differences between groups, such as co-morbidities, ASA score, etc. It is very likely, or even certain, that the elderly group had more co-morbidities. In addition, we did not compare the indications for surgery (pancreatic cancer vs. other periampullary neoplasms). It is well established that the indication for surgery may also have impact on outcomes–for instance patients undergoing PD for advanced pancreatic cancer have a different prognosis than those with other tumors or benign diseases. The proportion of pancreatic cancer patients in older group was slightly higher (although not statistically significant). Other indications for surgery were duodenal cancer, ampullary carcinoma, distal cholangiocarcinoma, metastasis in the head of pancreas, intraductal papillary mucinous neoplasms, neuroendocrine tumor and chronic pancreatitis We were not able to perform subgroup analysis distinguishing different indications for surgery due to lack of patient level data. So, this limitation also has to be taken into consideration when analyzing results of our meta-analysis. Additionally, the fact that the number of elderly patients receiving adjuvant chemotherapy is lower, one can assume might have influenced survival. Lastly, papers included in the meta-analysis were published over the last two decades during which there have been major changes in pancreatic surgery. That said, in our opinion these aspects did not play a major role in the results.
CONCLUSIONS
Our review confirms that in the case of PD, advanced age is a risk factor for increased non-surgical morbidity and, by extension, higher mortality. These findings are based on a number of moderate or high-quality comparative studies; it is very unlikely that future comparisons will undermine them. Unless other treatment strategies are implemented, the elderly will continue to constitute a group of patients for whom worse outcomes can be expected. However, as long as PD remains the only way to cure periampullary neoplasms, or at least prolongs survival, age should never be the sole contraindication to surgery.
METHODS
Study selection
A systematic review of the literature was performed using the Medline, Embase and Cochrane databases to identify all eligible studies that compared patients undergoing PD for periampullary tumors in terms of age. The used search terms included: “pancreatoduodenectomy”, “pancreaticoduodenectomy”, “Whipple”, “Traverso”, “pancreatic head resection”, “pancreatic head tumour”, “duodenopancreatectomy”, “older”, “elderly”, “octagenarian”, “nonagenarian”, “septuagenarian”, “age”, “70”, “75”, “80” and “65”. These terms were combined using Boolean operators “AND” and “OR”. Some references of the acquired articles were also located manually. The most recent search was performed on 10th of April, 2017. Ovid search strategy is available in Supplementary Figure 2.
Studies eligible for further analysis had to fulfill the following criteria: (1) a comparison of the characteristics and perioperative outcomes of older patients vs. younger patients undergoing pancreatoduodenectomy; (2) an objective evaluation of mortality or overall morbidity; (3) publication in English. Studies were excluded when there was: (1) a lack of comparative data; (2) a lack of primary outcomes or insufficient data to analyze; (3) a focus on procedures other than pancreatoduodenectomy; or (4) an extraction of data specifically concerning pancreatoduodenectomy was not possible.
Outcomes of interest
Older patients were compared with younger patients on the basis of postoperative complications, oncologic safety (R0 rate), and length of hospital stay (LOS). All-cause mortality was defined as the number of deaths during the longest follow-up period. Overall morbidity was defined as the number of patients with at least one complication during the longest follow-up period. Complications included pancreatic fistula, delayed gastric emptying (DGE), postoperative hemorrhage, bile leakage, surgical site infection (SSI), pulmonary complications, and cardiovascular complications.
Data extraction and quality assessment
All references were reviewed and evaluated by three teams of two researchers. In case of any doubts about eligibility for inclusion, an attempt was made to reach consensus within the group. If no resolution was possible, an arbitrary decision was made by another reviewer. Data from the included studies were extracted independently by all teams. Only full-length articles were eligible for extraction. When available, the following data was extracted: first author, year of publication, number of operated subjects, type of surgery, age cut-off point, and short-term outcomes.
Non-randomized studies were evaluated according to the Newcastle–Ottawa Scale (NOS), which consists of three factors: patient selections, comparability of study groups, and assessment of outcomes. A score of 0 to 9 was assigned to each study and studies achieving a score of 6 or higher were considered high-quality. This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) consensus statement. The study was registered in the PROSPERO Database and the assigned number is CRD42017070692.
Data analysis
Analysis was performed using RevMan 5.3 (freeware from The Cochrane Collaboration). Statistical heterogeneity and inconsistency were measured using Cochran’s Q tests and I2, respectively. Qualitative outcomes from individual studies were analyzed to assess individual and pooled risk ratios (RR) with 95% confidence intervals (CI) favoring older populations undergoing pancreatoduodenectomy, and by using the Mantel-Haenszel random-effects method. For positive outcomes, RR was calculated for “non-event” occurrence. When appropriate, mean and standard deviation were calculated from medians and interquartile ranges using a method proposed by Hozo et al. [76]. Weighted mean differences (WMD) with a 95% CI are presented for quantitative variables using the inverse variance random-effects method. Statistical significance was observed with a two-tailed 0.05 level for hypotheses and with 0.10 for heterogeneity testing, while unadjusted p-values were reported accordingly. Each analysis involved subgroup analysis with cut-off points set at 65, 70, 75, and 80 years old. For studies that reported more than two age groups, only qualitative outcomes were analyzed (3 groups were divided into 2 to provide a dichotomous outcome, e.g. groups <70 vs. 71–80 vs. >80 were transformed to <80 vs. >80).
Abbreviations
PD: pancreatoduodenectomy; WMD: Weighted mean differences; RR: risk ratio; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; MOOSE: Meta-Analysis of Observational Studies in Epidemiology; NOS: Newcastle–Ottawa Scale; SSI: surgical site infection ; DGE: delayed gastric emptying ; LOS: length of stay.
Author contributions
Michał Pędziwiatr–idea conception, manuscript preparation, screening and data extraction, data interpretation, final revision of the manuscript; Piotr Małczak–screening supervisor, extraction supervisor, data synthesis, figure and table preparation, data interpretation
Magdalena Mizera–screening and data extraction, data interpretation' Jan Witowski - screening and data extraction, data interpretation; Grzegorz Torbicz - screening and data extraction; Piotr Major - screening and data extraction; Magdalena Pisarska - screening supervisor, extraction supervisor, data synthesis; Michał Wysocki–figure and table preparation; Miłosz Jankowski–data interpretation; Mateusz Rubinkiewicz - data interpretation, screening and data extraction; Anna Lasek–language correction; Jan Kulawik–manuscript preparation, screening and data extraction; Andrzej Budzyński–final revision of the manuscript.
CONFLICTS OF INTEREST
Authors declare no conflicts of interest.
REFERENCES
1. Mackenbach JP. Convergence and divergence of life expectancy in Europe: a centennial view. Eur J Epidemiol. 2013; 28:229–40. https://doi.org/10.1007/s10654-012-9747-x.
2. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet (London, England). England; 2012; 380:37–43. https://doi.org/10.1016/S0140-6736(12)60240-2.
3. Midha S, Chawla S, Garg PK. Modifiable and non-modifiable risk factors for pancreatic cancer: A review. Cancer Lett. Elsevier; 2016; 381:269–77. https://doi.org/10.1016/j.canlet.2016.07.022.
4. Ferlay J, Partensky C, Bray F. More deaths from pancreatic cancer than breast cancer in the EU by 2017. Acta Oncol (Madr). Taylor & Francis; 2016; 55:1158–60. https://doi.org/10.1080/0284186X.2016.1197419.
5. Hodul P, Tansey J, Golts E, Oh D, Pickleman J, Aranha GV. Age is not a contraindication to pancreaticoduodenectomy. Am Surg. 2001; 67:270–5; discussion 275—6. Available from http://europepmc.org/abstract/MED/11270888.
6. Cameron JL, He J. Two thousand consecutive pancreaticoduodenectomies. J Am Coll Surg. United States; 2015; 220:530–6. https://doi.org/10.1016/j.jamcollsurg.2014.12.031.
7. Pędziwiatr M, Małczak P, Pisarska M, Major P, Wysocki M, Stefura T, Budzyński A. Minimally invasive versus open pancreatoduodenectomy—systematic review and meta-analysis. Langenbeck’s Arch Surg. Berlin/Heidelberg: Springer Berlin Heidelberg; 2017; 402:841–51. https://doi.org/10.1007/s00423-017-1583-8.
8. Vincent A, Herman J, Schulick R, Hruban RH, Goggins M. Pancreatic cancer. Lancet (London, England). England; 2011; 378:607–20. https://doi.org/10.1016/S0140-6736(10)62307-0.
9. Liu C, Lu Y, Luo G, Cheng H, Guo M, Liu Z, Xu J, Long J, Liu L, Fu D, Ni Q, Li M, Yu X. Which patients with para-aortic lymph node (LN16) metastasis will truly benefit from curative pancreaticoduodenectomy for pancreatic head cancer? Oncotarget. United States; 2016; 7:29177–86. https://doi.org/10.18632/oncotarget.8690.
10. Karl RC, Smith SK, Fabri PJ. Validity of major cancer operations in elderly patients. Ann Surg Oncol. United States; 1995; 2:107–13.
11. Vickers SM, Kerby JD, Smoot TM, Shumate CR, Halpern NB, Aldrete JS, Gleysteen JJ. Economics of pancreatoduodenectomy in the elderly. Surgery. United States; 1996; 120:620–6.
12. Chijiiwa K, Yamaguchi K, Yamashita H, Ogawa Y, Yoshida J, Tanaka M. ASA physical status and age are not factors predicting morbidity, mortality, and survival after pancreatoduodenectomy. Am Surg. United States; 1996; 62:701–5.
13. Sohn TA, Yeo CJ, Cameron JL, Lillemoe KD, Talamini MA, Hruban RH, Sauter PK, Coleman J, Ord SE, Grochow LB, Abrams RA, Pitt HA. Should pancreaticoduodenectomy be performed in octogenarians? J Gastrointest Surg. United States; 1998; 2:207–16.
14. Magistrelli P, Masetti R, Coppola R, Riccioni ME, Crucitti A, Nuzzo G, Picciocchi A. Pancreatic resection for periampullary cancer in elderly patients. Hepatogastroenterology. Greece; 1998; 45:242–7.
15. Al-Sharaf K, Andren-Sandberg A, Ihse I. Subtotal pancreatectomy for cancer can be safe in the elderly. Eur J Surg. England; 1999; 165:230–5. https://doi.org/10.1080/110241599750007090.
16. Aranha G V, Hodul PJ, Creech S, Jacobs W. Zero mortality after 152 consecutive pancreaticoduodenectomies with pancreaticogastrostomy. J Am Coll Surg. United States; 2003; 197:222–3. https://doi.org/10.1016/S1072-7515(03)00331-4.
17. Brozzetti S, Mazzoni G, Miccini M, Puma F, De Angelis M, Cassini D, Bettelli E, Tocchi A, Cavallaro A. Surgical treatment of pancreatic head carcinoma in elderly patients. Arch Surg. United States; 2006; 141:137–42. https://doi.org/10.1001/archsurg.141.2.137.
18. Makary MA, Winter JM, Cameron JL, Campbell KA, Chang D, Cunningham SC, Riall TS, Yeo CJ. Pancreaticoduodenectomy in the very elderly. J Gastrointest Surg. United States; 2006; 10:347–56. https://doi.org/10.1016/j.gassur.2005.12.014.
19. Kang CM, Kim JY, Choi GH, Kim KS, Choi JS, Lee WJ, Kim BR. Pancreaticoduodenectomy of pancreatic ductal adenocarcinoma in the elderly. Yonsei Med J. Korea (South); 2007; 48:488–94. https://doi.org/10.3349/ymj.2007.48.3.488.
20. Tani M, Kawai M, Hirono S, Ina S, Miyazawa M, Nishioka R, Shimizu A, Uchiyama K, Yamaue H. A pancreaticoduodenectomy is acceptable for periampullary tumors in the elderly, even in patients over 80 years of age. J Hepatobiliary Pancreat Surg. Japan; 2009; 16:675–80. https://doi.org/10.1007/s00534-009-0106-6.
21. Buchs NC, Addeo P, Bianco FM, Gangemi A, Ayloo SM, Giulianotti PC. Outcomes of robot-assisted pancreaticoduodenectomy in patients older than 70 years: a comparative study. World J Surg. United States; 2010; 34:2109–14. https://doi.org/10.1007/s00268-010-0650-x.
22. Khan S, Sclabas G, Lombardo KR, Sarr MG, Nagorney D, Kendrick ML, Donohue JH, Que FG, Farnell MB. Pancreatoduodenectomy for ductal adenocarcinoma in the very elderly; is it safe and justified? J Gastrointest Surg. United States; 2010; 14:1826–31. https://doi.org/10.1007/s11605-010-1294-8.
23. Lee MK, Dinorcia J, Reavey PL, Holden MM, Genkinger JM, Lee JA, Schrope BA, Chabot JA, Allendorf JD. Pancreaticoduodenectomy can be performed safely in patients aged 80 years and older. J Gastrointest Surg. United States; 2010; 14:1838–46. https://doi.org/10.1007/s11605-010-1345-1.
24. de Franco V, Frampas E, Wong M, Meurette G, Charvin M, Leborgne J, Regenet N. Safety and feasibility of pancreaticoduodenectomy in the elderly: a matched study. Pancreas. United States; 2011; 40:920–4. https://doi.org/10.1097/MPA.0b013e31821fd70b.
25. Haigh PI, Bilimoria KY, DiFronzo LA. Early postoperative outcomes after pancreaticoduodenectomy in the elderly. Arch Surg. United States; 2011; 146:715–23. https://doi.org/10.1001/archsurg.2011.115.
26. Shin JW, Ahn KS, Kim YH, Kang KJ, Lim TJ. The impact of old age on surgical outcomes after pancreaticoduodenectomy for distal bile duct cancer. Korean J hepato-biliary-pancreatic Surg. Korea (South); 2011; 15:248–53. https://doi.org/10.14701/kjhbps.2011.15.4.248.
27. Ito Y, Kenmochi T, Irino T, Egawa T, Hayashi S, Nagashima A, Kitagawa Y. The impact of surgical outcome after pancreaticoduodenectomy in elderly patients. World J Surg Oncol. BioMed Central; 2011; 9:102. https://doi.org/10.1186/1477-7819-9-102.
28. de la Fuente SG, Bennett KM, Pappas TN, Scarborough JE. Pre- and intraoperative variables affecting early outcomes in elderly patients undergoing pancreaticoduodenectomy. HPB (Oxford). Blackwell Publishing Ltd; 2011; 13:887–92. https://doi.org/10.1111/j.1477-2574.2011.00390.x.
29. Kow AWC, Sadayan NA, Ernest A, Wang B, Chan CY, Ho CK, Liau KH. Is pancreaticoduodenectomy justified in elderly patients? Surgeon. Scotland; 2012; 10:128–36. https://doi.org/10.1016/j.surge.2011.02.005.
30. Sulpice L, Rayar M, D’Halluin PN, Harnoy Y, Merdrignac A, Bretagne JF, Meunier B, Boudjema K. Impact of age over 75 years on outcomes after pancreaticoduodenectomy. J Surg Res. United States; 2012; 178:181–7. https://doi.org/10.1016/j.jss.2012.03.075.
31. Yamada S, Shimada M, Utsunomiya T, Morine Y, Imura S, Ikemoto T, Mori H, Kanamoto M, Hanaoka J, Iwahashi S, Saitoh Y. Surgical results of pancreatoduodenectomy in elderly patients. Surg Today. 2012; 42:857–62. https://doi.org/10.1007/s00595-012-0169-x.
32. Barbas AS, Turley RS, Ceppa EP, Reddy SK, Blazer DG 3rd, Clary BM, Pappas TN, Tyler DS, White RR, Lagoo SA. Comparison of outcomes and the use of multimodality therapy in young and elderly people undergoing surgical resection of pancreatic cancer. J Am Geriatr Soc. United States; 2012; 60:344–50. https://doi.org/10.1111/j.1532-5415.2011.03785.x.
33. Melis M, Marcon F, Masi A, Pinna A, Sarpel U, Miller G, Moore H, Cohen S, Berman R, Pachter HL, Newman E. The safety of a pancreaticoduodenectomy in patients older than 80 years: risk vs. benefits. HPB (Oxford). Oxford, UK: Blackwell Publishing Ltd; 2012; 14:583–8. https://doi.org/10.1111/j.1477-2574.2012.00484.x.
34. Brachet D, Lermite E, Vychnevskaia-Bressollette K, Mucci S, Hamy A, Arnaud JP. Should pancreaticoduodenectomy be performed in the elderly? Hepatogastroenterology. Greece; 2012; 59:266–71. https://doi.org/10.5754/hge10047.
35. Shimura T, Morinaga N, Suzuki H, Araki K, Kobayashi T, Koyama Y, Yashima R, Shibata M, Takenoshita S, Kuwano H. Description of pylorus-preserving pancreaticoduodenectomy in elderly patients. Hepatogastroenterology. Greece; 2012; 59:903–6. https://doi.org/10.5754/hge10735.
36. Suzuki S, Kaji S, Koike N, Harada N, Suzuki M. Pancreaticoduodenectomy can be safely performed in the elderly. Surg Today. Japan; 2013; 43:620–4. https://doi.org/10.1007/s00595-012-0383-6.
37. Oguro S, Shimada K, Kishi Y, Nara S, Esaki M, Kosuge T. Perioperative and long-term outcomes after pancreaticoduodenectomy in elderly patients 80 years of age and older. Langenbeck’s Arch Surg. Germany; 2013; 398:531–8. https://doi.org/10.1007/s00423-013-1072-7.
38. Sun JW, Zhang PP, Ren H, Hao JH. Pancreaticoduodenectomy and pancreaticoduodenectomy combined with superior mesenteric-portal vein resection for elderly cancer patients. Hepatobiliary Pancreat Dis Int. Singapore; 2014; 13:428–34.
39. Kanda M, Fujii T, Suenaga M, Takami H, Inokawa Y, Yamada S, Kobayashi D, Tanaka C, Sugimoto H, Nomoto S, Fujiwara M, Kodera Y. Pancreatoduodenectomy with portal vein resection is feasible and potentially beneficial for elderly patients with pancreatic cancer. Pancreas. United States; 2014; 43:951–8. https://doi.org/10.1097/MPA.0000000000000136.
40. Usuba T, Takeda Y, Murakami K, Tanaka Y, Hanyu N. Clinical outcomes after pancreaticoduodenectomy in elderly patients at middle-volume center. Hepatogastroenterology. Greece; 2014; 61:1762–6.
41. Coolsen MME, Bakens M, van Dam RM, Olde Damink SWM, Dejong CHC. Implementing an enhanced recovery program after pancreaticoduodenectomy in elderly patients: is it feasible? World J Surg. United States; 2015; 39:251–8. https://doi.org/10.1007/s00268-014-2782-x.
42. Tee MC, Croome KP, Shubert CR, Farnell MB, Truty MJ, Que FG, Reid-Lombardo KM, Smoot RL, Nagorney DM, Kendrick ML. Laparoscopic pancreatoduodenectomy does not completely mitigate increased perioperative risks in elderly patients. HPB (Oxford). England; 2015; 17:909–18. https://doi.org/10.1111/hpb.12456.
43. Urbonas K, Gulbinas A, Smailyte G, Pranys D, Jakstaite A, Pundzius J, Barauskas G. Factors influencing survival after pancreatoduodenectomy for ductal adenocarcinoma depend on patients’ age. Dig Surg. Switzerland; 2015; 32:60–7. https://doi.org/10.1159/000371856.
44. Casadei R, Taffurelli G, Silvestri S, Ricci C, Campra D, Minni F. Is age a barrier to pancreaticoduodenectomy? An Italian dual-institution study. Updates Surg. Italy; 2015; 67:439–47. https://doi.org/10.1007/s13304-015-0337-9.
45. Frakes JM, Strom T, Springett GM, Hoffe SE, Balducci L, Hodul P, Malafa MP, Shridhar R. Resected pancreatic cancer outcomes in the elderly. J Geriatr Oncol. Netherlands; 2015; 6:127–32. https://doi.org/10.1016/j.jgo.2014.11.005.
46. Zhang D, Gao J, Li S, Wang F, Zhu J, Leng X. Outcome after pancreaticoduodenectomy for malignancy in elderly patients. Hepatogastroenterology. Greece; 2015; 62:451–4.
47. Watanabe J, Hanaki T, Arai Y, Tokuyasu N, Sakamoto T, Honjo S, Otani S, Ikeguchi M. Perioperative Outcomes after Pancreaticoduodenectomy in Elderly Patients. Hepatogastroenterology. Greece; 2015; 62:590–4.
48. Miyazaki Y, Kokudo T, Amikura K, Kageyama Y, Takahashi A, Ohkohchi N, Sakamoto H. Age does not affect complications and overall survival rate after pancreaticoduodenectomy: Single-center experience and systematic review of literature. Biosci Trends. Japan; 2016; 10:300–6. https://doi.org/10.5582/bst.2016.01093.
49. El Nakeeb A, Atef E, El Hanafy E, Salem A, Askar W, Ezzat H, Shehta A, Abdel Wahab M. Outcomes of pancreaticoduodenectomy in elderly patients. Hepatobiliary Pancreat Dis Int. Singapore; 2016; 15:419–27.
50. Liang DH, Shirkey BA, Rosenberg WR, Martinez S. Clinical outcomes of pancreaticoduodenectomy in octogenarians: a surgeon’s experience from 2007 to 2015. J Gastrointest Oncol. China; 2016; 7:540–6. https://doi.org/10.21037/jgo.2016.03.04.
51. Mauriello C, Polistena A, Gambardella C, Tartaglia E, Orditura M, De Vita F, Santini L, Avenia N, Conzo G. Pancreatic stump closure after pancreatoduodenectomy in elderly patients: a retrospective clinical study. Aging Clin Exp Res. Germany; 2017; 29:35–40. https://doi.org/10.1007/s40520-016-0657-8.
52. Zouros E, Liakakos T, Machairas A, Patapis P, Tzerbinis H, Manatakis DK, Papadimitriou-Olivgeris M, Dervenis C. Fast-Track Pancreaticoduodenectomy in the Elderly. Am Surg. United States; 2017; 83:239–49.
53. Wiltberger G, Muhl B, Benzing C, Hau HM, Bartels M, Krenzien F. Pancreaticoduodenectomy in the Elderly Patient: Age-Adapted Risk Assessment. Dig Surg. Switzerland; 2017; 34:43–51. https://doi.org/10.1159/000448059.
54. Krautz C, Nimptsch U, Weber GF, Mansky T, Grutzmann R. Effect of Hospital Volume on In-hospital Morbidity and Mortality Following Pancreatic Surgery in Germany. Ann Surg. United States; 2018; 267:411–7. https://doi.org/10.1097/SLA.0000000000002248.
55. Coe TM, Fong ZV, Wilson SE, Talamini MA, Lillemoe KD, Chang DC. Outcomes Improvement Is Not Continuous Along the Learning Curve for Pancreaticoduodenectomy at the Hospital Level. J Gastrointest Surg. United States; 2015; 19:2132–7. https://doi.org/10.1007/s11605-015-2967-0.
56. Nienhuijs SW, van den Akker SA, de Vries E, de Hingh IH, Visser O, Lemmens VE. Nationwide improvement of only short-term survival after resection for pancreatic cancer in the Netherlands. Pancreas. United States; 2012; 41:1063–6. https://doi.org/10.1097/MPA.0b013e31824c3dbf.
57. Birkmeyer JD, Warshaw AL, Finlayson SR, Grove MR, Tosteson AN. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Surgery. United States; 1999; 126:178–83.
58. Lemmens VEPP, Bosscha K, van der Schelling G, Brenninkmeijer S, Coebergh JWW, de Hingh IHJT. Improving outcome for patients with pancreatic cancer through centralization. Br J Surg. England; 2011; 98: 1455–62. https://doi.org/10.1002/bjs.7581.
59. Opendro SS, Satoi S, Yanagimoto H, Yamamoto T, Toyokawa H, Hirooka S, Yamaki S, Inoue K, Matsui Y, Kwon AH. Role of adjuvant surgery in initially unresectable pancreatic cancer after long-term chemotherapy or chemoradiation therapy: survival benefit? J Hepatobiliary Pancreat Sci. Japan; 2014; 21:695–702. https://doi.org/10.1002/jhbp.119.
60. Gurusamy KS, Kumar S, Davidson BR, Fusai G. Resection versus other treatments for locally advanced pancreatic cancer. Cochrane database Syst Rev. England; 2014; CD010244. https://doi.org/10.1002/14651858.CD010244.pub2.
61. Wangjam T, Zhang Z, Zhou XC, Lyer L, Faisal F, Soares KC, Fishman E, Hruban RH, Herman JM, Laheru D, Weiss M, Li M, De Jesus-Acosta A, et al. Resected pancreatic ductal adenocarcinomas with recurrence limited in lung have a significantly better prognosis than those with other recurrence patterns. Oncotarget. Impact Journals LLC; 2015; 6:36903–10. Available from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4742219/
62. Nagrial AM, Chang DK, Nguyen NQ, Johns AL, Chantrill LA, Humphris JL, Chin VT, Samra JS, Gill AJ, Pajic M, Pinese M, Colvin EK, Scarlett CJ, et al. Adjuvant chemotherapy in elderly patients with pancreatic cancer. Br J Cancer. England; 2014; 110:313–9. https://doi.org/10.1038/bjc.2013.722.
63. Sehgal R, Alsharedi M, Larck C, Edwards P, Gress T. Pancreatic cancer survival in elderly patients treated with chemotherapy. Pancreas. United States; 2014; 43:306–10. https://doi.org/10.1097/MPA.0000000000000091.
64. Cooper AB, Holmes HM, des Bordes JKA, Fogelman D, Parker NH, Lee JE, Aloia TA, Vauthey JN, Fleming JB, Katz MHG. Role of neoadjuvant therapy in the multimodality treatment of older patients with pancreatic cancer. J Am Coll Surg. United States; 2014; 219:111–20. https://doi.org/10.1016/j.jamcollsurg.2014.02.023.
65. Casadei R, Zanini N, Morselli-Labate AM, Calculli L, Pezzilli R, Poti O, Grottola T, Ricci C, Minni F. Prognostic factors in periampullary and pancreatic tumor resection in elderly patients. World J Surg. United States; 2006; 30:1992–3. https://doi.org/10.1007/s00268-006-0122-5.
66. Coolsen MME, van Dam RM, van der Wilt AA, Slim K, Lassen K, Dejong CHC. Systematic review and meta-analysis of enhanced recovery after pancreatic surgery with particular emphasis on pancreaticoduodenectomies. World J Surg. United States; 2013; 37:1909–18. https://doi.org/10.1007/s00268-013-2044-3.
67. Barton JG. Enhanced Recovery Pathways in Pancreatic Surgery. Surg Clin North Am. United States; 2016; 96:1301–12. https://doi.org/10.1016/j.suc.2016.07.003.
68. Deng X, Cheng X, Huo Z, Shi Y, Jin Z, Feng H, Wang Y, Wen C, Qian H, Zhao R, Qiu W, Shen B, Peng C. Modified protocol for enhanced recovery after surgery is beneficial for Chinese cancer patients undergoing pancreaticoduodenectomy. Oncotarget. Impact Journals LLC; 2017; 8:47841–8. https://doi.org/10.18632/oncotarget.18092.
69. Pisarska M, Malczak P, Major P, Wysocki M, Budzynski A, Pedziwiatr M. Enhanced recovery after surgery protocol in oesophageal cancer surgery: Systematic review and meta-analysis. PLoS One. United States; 2017; 12:e0174382. https://doi.org/10.1371/journal.pone.0174382.
70. Pedziwiatr M, Matlok M, Kisialeuski M, Migaczewski M, Major P, Winiarski M, Budzynski P, Zub-Pokrowiecka A, Budzynski A. Short hospital stays after laparoscopic gastric surgery under an Enhanced Recovery After Surgery (ERAS) pathway: experience at a single center. Eur Surg. Austria; 2014; 46:128–32. https://doi.org/10.1007/s10353-014-0264-x.
71. Pedziwiatr M, Pisarska M, Kisielewski M, Major P, Mydlowska A, Rubinkiewicz M, Winiarski M, Budzynski A. ERAS protocol in laparoscopic surgery for colonic versus rectal carcinoma: are there differences in short-term outcomes? Med Oncol. United States; 2016; 33:56. https://doi.org/10.1007/s12032-016-0772-6.
72. Pedziwiatr M, Malczak P, Major P, Witowski J, Kusnierz-Cabala B, Ceranowicz P, Budzynski A. Minimally invasive pancreatic cancer surgery: What is the current evidence? Med Oncol. United States; 2017; 34:125. https://doi.org/10.1007/s12032-017-0984-4.
73. Zhang S, Lan Z, Zhang J, Chen Y, Xu Q, Jiang Q, Zhao Y, Wang C, Bi X, Huang X. Duct-to-mucosa versus invagination pancreaticojejunostomy after pancreaticoduodenectomy: a meta-analysis. Oncotarget. United States; 2017; 46449–60. https://doi.org/10.18632/oncotarget.17503.
74. Liu D, Lv A, Tian Z, Tian X, Guan X, Dong B, Zhao M, Hao C. Superior mesenteric artery margin in pancreaticoduodenectomy for pancreatic adenocarcinoma. Oncotarget. Impact Journals LLC; 2017; 8:7766–76. https://doi.org/10.18632/oncotarget.13950.
75. Pędziwiatr M, Małczak P, Pisarska M, Major P, Wysocki M, Stefura T, Budzyński A. Minimally invasive versus open pancreatoduodenectomy—systematic review and meta-analysis. Langenbeck’s Arch Surg. Berlin/Heidelberg: Springer Berlin Heidelberg; 2017; 402:841–51. https://doi.org/10.1007/s00423-017-1583-8.
76. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005; 5:13. https://doi.org/10.1186/1471-2288-5-13.