
INTRODUCTION
Breast cancer is a molecularly diverse disease, which can be mainly divided into three molecular subtypes. The first subtype is hormone receptor positive (HR-positive) breast cancer, whose tumors tend to be estrogen receptor (ER) positive or progesterone receptor (PR) positive, or both, with a normal expression of human epidermal growth factor receptor 2 (HER2-negative). The second subtype is HER2+ breast cancer, which is defined by HER2 gene amplification or overexpression. Interestingly, about 45% of this subtype breast cancer has variable expression levels of ER or PR, or both. And the third subtype is triple-negative breast cancer (TNBC), defined by the deficiency of ER, PR and HER2 [1]. Furthermore, about 80% of breast cancer patients express hormone receptors (HR). Endocrine therapy, also known as hormone therapy, is the standard treatment for these HR-positive breast cancer subtypes, significantly reducing the relapse rate after receiving treatment in an early stage [2]. However, most patients have different resistance reactions to current endocrine therapy, which requires the development of alternative endocrine therapies [3–6].
Deregulation of cell cycle is one of the cancer hallmarks. In this regard, several genetic mutations in key proteins of cell cycle regulatory have been described to be responsible for breast cancer [7, 8]. The cyclin-dependent kinases (CDKs), a large family of serine threonine kinases, play an important role in regulating cell cycle progression. CDK4 and CDK6, activated by cyclin D, facilitate the hyperphosphorylation of retinoblastoma (Rb) protein, which can lead to the cell cycle transition from G1 phase to S phase. Importantly, this critical Rb check point has been demonstrated to be associated with endocrine resistance in breast cancer. At this point, the inhibition of this pathway including cyclin D, CDK4/6 and pRb can be considered as an effective treatment for HR-positive advanced breast cancer, not only as a first-line therapy [9–11], but also for patients with disease progress after receiving endocrine therapy [12, 13].
Recently, a large number of CDK4/6 inhibitors, especially palbociclib, ribociclib, and abemaciclib, have been tested in clinical trials. In all, 165 postmenopausal women with HR-positive/HER2-negative advanced breast cancer were randomly selected in a phase-II trial (PALOMA-1) to receive letrozole with or without palbociclib. Median progression-free survival (PFS) with combination therapy was 20.2 months, whereas in the control group (letrozole only) was 10.2 months (hazard ratio (HR) = 0.49; 95% confidence interval (CI) = 0.319–0.748; P = 0.0004) [9]. Similar result was found in other three phase-III trials, supporting the conclusion that the combination therapy would contribute to a longer survival. Based on this research finding, the U.S. Food and Drug Administration (FDA) eventually approved palbociclib and letrozole as the treatment for postmenopausal patients with HR-positive/HER2-negative advanced breast cancer in 2015.
Besides palbociclib, ribociclib and abemaciclib have also been considered as the target inhibitors of CDK4/6 in several clinical trials. Here, we performed a meta-analysis to assess the safety and efficacy of these CDK4/6 inhibitors for treating HR-positive/HER2-negative advanced breast cancer.
METHODS
Study protocol
At the beginning of this project, a research protocol was drafted following the Cochrane Collaboration format.
Eligibility criteria
Eligibility criteria were designed as follows: (a) research type: randomized controlled trial (RCT); (b) language restriction: English only; (c) participants: patients with HR-positive/HER2-negative advanced breast cancer; (d) intervention: CDK4/6 inhibitors; (e) outcomes: progression-free survival, response and adverse events.
On the contrary, eligibility criteria did not include the conditions as follows: (a) control: positive control; (b) withdraw rate >20 %.
Search strategy and information sources
MEDLINE, EMBASE, and Cochrane Library were used for information search by two independent authors (W.D. and Z.L.). They collected all available researches published up to June 2017. The search strategy for the MEDLINE was mainly the combination of variable key words: “cyclin dependent kinase 4 and 6 inhibitors” or “palbociclib” or “abemaciclib” or “ribociclib” AND “breast cancer”. A limited number of clinical trials were found from MEDLINE, which then would be double-checked by the correlation between titles and abstracts. The search strategy for EMBASE and Cochrane Library was similar to the one for MEDLINE. Besides the electronical databases, articles from RCT reference lists and systematic reviews were checked after a manually screening, in order to ensure that all the relevant researches had been included in this systematic review. As for unpublished or ongoing trials, we searched the website of ClinicalTrials.gov and contacted authors for the relevant data.
Study selection and data collection
All records from this systematic review in electronical databases, reference lists of RCTs and systematic reviews were independently evaluated by two authors (W.D. and Z.L.), in accordance with the eligibility criteria as mentioned above. After strict selection and evaluation, the data were extracted from these RCT records with the basic information including clinical trials, criteria, study design, patient demographic characteristics, as well as outcome assessments.
After data collection, we performed a meta-analysis and obtained two outcomes. The primary outcome was PFS. And the secondary outcome included objective response (complete response or partial response) and clinical benefit response (complete response + partial response + stable disease for ≥ 24weeks).
Risk of bias and quality assessment
In this review, W.D. and C.W. independently assessed the risk of bias in individual studies using Review Manager 5.3 software. For evaluating the risk of bias of RCTs, we applied uniform criteria recommended by the Cochrane Collaboration, which included six items: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other potential bias as previously used in our meta-analysis.
Summary measures and synthesis of results
Review Manager 5.3 from the Cochrane Collaboration was used to assess the risk of bias in individual studies. After that subgroup analyses were performed to detect the influence of stratification factors and other baseline characteristics. Sensitivity analysis was used to detect the stability of the consolidated results except the only phase-II clinical trial. Statistical heterogeneity was estimated by the I2 statistic as follows: I2 < 30% means “low heterogeneity”; I2 between 30–50% denotes “moderate heterogeneity”; I2 < 50% represents “substantial heterogeneity”. Dichotomous outcomes were analyzed as hazard ratio (95% CI) by using the Mantel–Haenszel test. A fixed effects model was used if the heterogeneity was low or moderate. Otherwise, the random effect model was reported after exploring the cause of heterogeneity. All tests mentioned were two-tailed and a P-value of less than 0.05 was considered to be statistically significant for all analyses.
RESULTS
According to the search strategy established by us,1182 records were retrieved totally from MEDLINE, EMBASE, Cochrane Library. After removing the duplicates and irrelevant records, 16 full-text articles were eligible for the meta-analysis. Furthermore, 11 records were excluded due to the following reasons: 8 conference abstracts, 2 meta-analyses, and 1 note. Ultimately, 5 RCT records containing 2689 patients were included in qualitative synthesis (Figure 1). The main characteristics of these included studies are listed in Table 1.
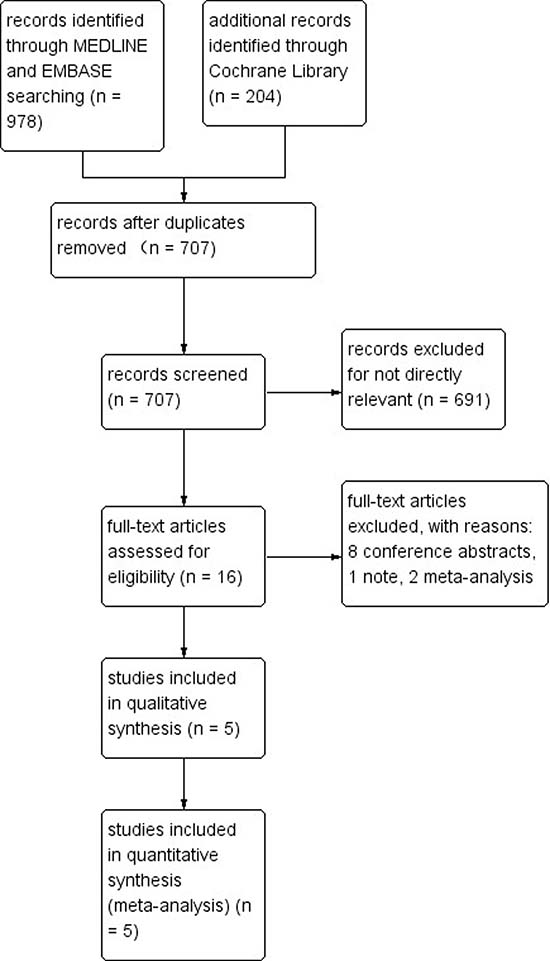
Figure 1: The flowchart of data search, collection and selection. Ultimately, five RCTs containing 2689 patients were selected to undergo meta-analysis.
Table 1: Characteristics of included studies and outcome events
Trials |
Finn 2014 |
Finn 2016 |
Cristofanilli 2016 |
Hortobagyi 2016 |
Sledge 2017 |
|---|---|---|---|---|---|
Information of the included trials |
|||||
Regions |
50 sites in 12 countries |
186 sites in 17 countries |
144 sites in 17 countries |
223 sites in 29 countries |
142 sites in 19 countries |
Phases |
II |
III |
III |
III |
III |
Accrual dates |
December 22, 2009, and May 12, 2012 |
February 2013 and July 2014 |
October 7, 2013, and August 26, 2014 |
January 24, 2014, and March 24, 2015 |
August7, 2014, and December 29, 2015 |
Inclusion criteria and study design |
|||||
Inclusion criteria |
Postmenopausal;HR+,HER2- ABC; first-line |
Postmenopausal; HR+,HER2- ABC; first-line |
any menopausalstatus; HR+,HER2- ABC; second-line |
Postmenopausal; HR+,HER2- ABC; first-line |
Any menopausalstatus, HR+,HER2- ABC; first-line |
study design |
Palbociclib (125 mg daily for 21 days every 28 days)+letrozole (2.5 mg daily) vs. placebo+ letrozole (2.5mg daily) |
Palbociclib (125 mg daily for 21 days every 28 days)+letrozole (2.5 mg daily) vs. placebo+ letrozole (2.5mg daily) |
Palbociclib (125 mg daily for 21 days every 28 days)+fulvestrant (500 mg every 28 days) vs. placebo+ fulvestrant (500 mg every 28 days) |
Ribociclib (600mg daily for 21 days every 28 days)+letrozole (2.5 mg daily) vs. placebo+ letrozole (2.5mg daily) |
Abemaciclib (150 mg twice daily every 28 days)+fulvestrant (500 mg every 28 days) vs. placebo+ fulvestrant (500mg every 28 days) |
Patient demographic characteristic |
|||||
Age, year |
T: 63 (54–71) |
T: 62 (30–89) |
T: 57 (30–88) |
T: 62 (23–91) |
T: 59 (32-91) |
No. of Patients |
T: 84 |
T: 444 |
T: 347 |
T: 334 |
T: 446 |
Outcomes assessment |
|||||
primary end point |
progression-free survival |
progression-free survival |
progression-free survival |
progression-free survival |
progression-free survival |
Secondary end point |
OR, CBR |
OR, CBR |
OR, CBR |
OR, CBR |
OR, CBR |
Abbreviations: HR+: hormone receptor positive; HER2-: human epidermal growth factor receptor 2 negative; ABC: advanced breast cancer; OR: objective response; CBR: clinical benefit response T: treatment group (also known as CDK4/6 inhibitor group); C: control group.
Primary outcome analysis
All five RCTs enrolling 2689 patients were available for the analysis of PFS at the end of the observation period. The fixed effects model was used because there were no heterogeneities (I2 = 0%, p = 0.53) between these data. The pooled data showed that the CDK4/6 inhibitor group had a longer PFS than the control group (HR = 0.51; 95% CI = 0.46–0.57, p < 0.00001; Figure 2).
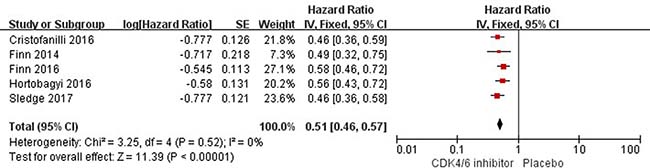
Figure 2: Forest plot of comparison: progression-free survival.
Secondary outcome analysis
For the analysis of Overall Response among 2689 patients enrolled from five RCTs, 2025 patients can be evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 [14].
Objective response
Because the heterogeneity of these data was apparent (I2 = 66%, p = 0.02), the random effects model was used. All the patients who were treated with CDK4/6 inhibitors (palbociclib, ribociclib or abemaciclib) had a trend to get an increasing probability of objective response (complete response or partial response), compared with the non-treated patients (risk rate (RR) = 1.56; 95% CI = 1.23–1.97, p = 0.0002; Figure 3). For another subgroup whose patient disease could be evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, there were also apparent heterogeneities (I2 = 71%, p = 0.008). And the CDK4/6 inhibitor group had a higher rate of objective response compared with the control group (RR = 1.60; 95% CI = 1.26–2.03, p = 0.0001; Figure 3). Thus, the results showed that CDK4/6 inhibitors could significantly increase the rate of objective response.
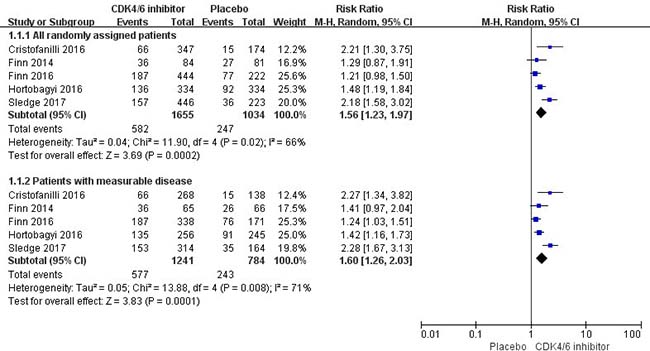
Figure 3: Forest plot of comparison: Objective response.
Clinical benefit response
Because the data heterogeneity of clinical benefit response (complete response + partial response + stable disease for ≥24 weeks) was apparent (I2 =80%, p = 0.0005), the random effects model was used. And the results of meta-analysis showed that the CDK4/6 inhibitor group had a higher rate of clinical benefit response compared with the control group (RR = 1.29; 95% CI = 1.13–1.47, p = 0.0001; Figure 4). Moreover, in patients with measurable disease, the data of clinical benefit response also presented an apparent heterogeneity (I2 = 71%, p = 0.008). And the CDK4/6 inhibitor group had a higher rate of clinical benefit response compared with the control group (RR = 1.22; 95% CI = 1.09–1.36, p = 0.0004; Figure 4). Thus, the results showed that CDK4/6 inhibitors could significantly increase the rate of clinical benefit response.
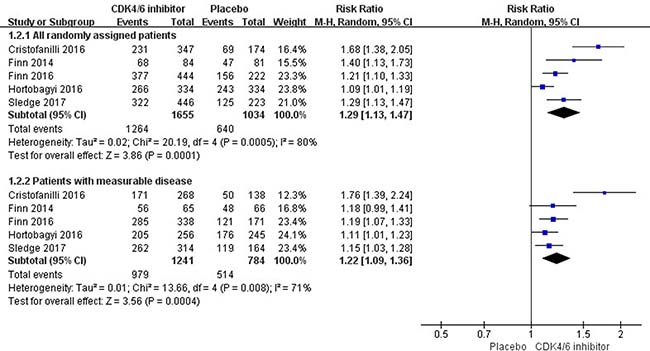
Figure 4: Forest plot of comparison: Clinical benefit response.
Subgroup analysis and sensitivity analysis
Subgroup analyses of PFS, according to stratification factors and other baseline characteristics, confirmed a consistent conclusion across all subgroups that CDK4/6 inhibitors could decrease the incidence of disease progression or death. (Table 2). For patients with age <65 years, the CDK4/6 inhibitor group had a significant decrease in the incidence of disease progression or death (HR = 0.50; 95% CI = 0.43–0.58); similar result was observed in patients with age ≥65 years (HR = 0.56; 95% CI = 0.46–0.68). For patients with visceral disease, the CDK4/6 inhibitor group had a significant decrease in the incidence of disease progression or death (HR = 0.53; 95% CI = 0.46–0.61); patients with non-visceral disease had a similar result (HR = 0.52; 95% CI = 0.43–0.62). For patients with bone-only disease at baseline, the CDK4/6 inhibitor group had a significant decrease in the incidence of disease progression or death (HR = 0.45; 95% CI = 0.31–0.64); patients with other sites of metastasis had a similar result (HR = 0.58; 95% CI = 0.49–0.69). For race, not only Asian but also non-Asian patients had a significant decrease in the incidence of disease progression or death with the treatment of CDK4/6 inhibitors (HR = 0.51; 95% CI = 0.39–0.67 vs. HR = 0.55; 95% CI = 0.48–0.63). In addition, with respect to disease-free interval, the risk of disease progression or death in the CDK4/6 inhibitor group was also lower than that in the control group, where all the patients had a disease-free interval of 12 months or less (HR = 0.51; 95% CI = 0.38–0.68) or had a disease-free interval of more than 12 months (HR = 0.48; 95% CI = 0.37–0.61). In the subgroup of patients with newly metastatic disease, patients in the CDK4/6 inhibitor group also had a significantly lower risk of disease progression or death than those in the control group (HR = 0.58; 95% CI = 0.43–0.79). Besides, for patients who had received prior hormonal therapy, the incidence of disease progression or death was significantly decreased in the CDK4/6 inhibitor group (HR = 0.48; 95% CI = 0.40–0.56); similar result was shown in the patients who had not received prior hormonal therapy (HR = 0.56; 95% CI = 0.48–0.66). Therefore, receive previous chemotherapy did not reduce the therapeutic effect of CDK4/6 inhibitors for advanced breast cancer patients (HR = 0.51; 95% CI = 0.43–0.61 vs. HR = 0.51; 95% CI = 0.41–0.62). Furthermore, Eastern Cooperative Oncology Group (ECOG) performance status also did not weaken the therapeutic effect of CDK4/6 inhibitors, which was verified by the data that the risk of disease progression or death was lower in the CDK4/6 inhibitor group than that in the control group, among patients who had ECOG performance status of 0 (HR = 0.55; 95% CI = 0.45–0.65) and among those who had ECOG performance status of 1 or 2 (HR = 0.55; 95% CI = 0.46–0.67). The status of PR would not weaken the curative effect of CDK4/6 inhibitors. The CDK4/6 inhibitors could reduce the risk of disease progression or death in patients with PR-positive (HR = 0.55; 95% CI = 0.45–0.67), and the similar result was presented in the patients with PR-negative (HR = 0.48; 95% CI = 0.36–0.64). In addition, different kind of CDK4/6 inhibitors (palbociclib or ribociclib or abemacicli) had a similar effect which could decrease the incidence of disease progression or death (HR = 0.51; 95% CI = 0.43–0.60 vs. HR = 0.52; 95% CI = 0.46–0.60 vs. HR = 0.46; 95%CI = 0.36–0.58). And no matter whether the patients received previous systemic therapy for advanced disease or not, CDK4/6 inhibitors could decrease the incidence of disease progression or death (first-line therapy vs. second-line therapy: HR = 0.53; 95% CI = 0.46–0.60 vs. HR = 0.46; 95% CI = 0.36–0.59). Sensitivity analysis showed that all outcomes were stable except Finn 2014 [9] (Table 2).
Table 2: Subgroup sensitivity and analysis for progression-free survival
HR (95 % CI) |
P value |
I2 , % |
|
|---|---|---|---|
Subgroup analysis |
|||
Age |
|||
<65 years |
0.50 (0.43, 0.58) |
<0.00001 |
11% |
≥65 years |
0.56 (0.46, 0.68) |
<0.00001 |
0% |
Visceral metastasis |
|||
yes |
0.53 (0.46, 0.61) |
<0.00001 |
0% |
no |
0.52 (0.43, 0.62) |
<0.00001 |
23% |
Bone-only metastasis |
|||
yes |
0.45 (0.31, 0.64) |
<0.0001 |
39% |
no |
0.58 (0.49, 0.69) |
<0.00001 |
0% |
Race |
|||
Asian |
0.51 (0.39, 0.67) |
<0.00001 |
0% |
non-Asian |
0.55 (0.48, 0.63) |
<0.00001 |
38% |
Disease-free interval |
|||
<12 months |
0.51 (0.38, 0.68) |
<0.00001 |
20% |
≥12 months |
0.48 (0.37, 0.61) |
<0.00001 |
0% |
Newly metastatic disease |
|||
yes |
0.58 (0.43, 0.79) |
0.0005 |
33% |
no |
0.55 (0.45, 0.67) |
<0.00001 |
0% |
Previous hormonal therapy |
|||
yes |
0.48 (0.40, 0.56) |
<0.00001 |
0% |
no |
0.56 (0.48,0.66) |
<0.00001 |
0% |
Previous chemotherapy |
|||
yes |
0.51 (0.43, 0.61) |
<0.00001 |
0% |
no |
0.51 (0.41, 0.62) |
<0.00001 |
47% |
ECOG performance status |
|||
0 |
0.55 (0.45, 0.65) |
<0.00001 |
0% |
1 or 2 |
0.55 (0.46,0.67) |
<0.00001 |
0% |
Hormone-receptor status |
|||
ER and PR-positive |
0.55 (0.45, 0.67) |
<0.0001 |
0% |
Other |
0.48 (0.36, 0.64) |
<0.00001 |
0% |
Palbociclib vs. Ribociclib |
|||
Palbociclib |
0.51 (0.43, 0.60) |
<0.00001 |
37% |
Ribociclib |
0.56 (0.43, 0.72) |
<0.00001 |
- |
Abemaciclib |
0.46 (0.36,0.58) |
<0.00001 |
- |
First-line vs. Second-line |
|||
First-line |
0.53 (0.46, 0.60) |
<0.00001 |
0% |
Second-line |
0.46 (0.36, 0.59) |
<0.00001 |
- |
Sensitivity analysis |
|||
Excluding Finn 2014 trial |
0.51 (0.46, 0.58) |
<0.00001 |
3% |
Abbreviations: HR: hazard ratio; CI: confidence interval; ECOG: Eastern Cooperative Oncology Group; ER: estrogen receptor; PR: progesterone receptor.
Adverse events
As for neutropenia, all grades of it were substantially more frequent in the CDK4/6 inhibitor group (70%), compared with the control group (5%). Interestingly, grade 3 or 4 neutropenia was found among 47% of patients in the CDK4/6 inhibitor group and among 1% of patients in the control group.
Meanwhile, leucopenia with all grades also appeared much more common in the CDK4/6 inhibitor group than in the control group (37% and 3% respectively), especially grade 3 or 4 leucopenia. Furthermore, infection, fatigue, nausea, anemia, thrombocytopenia, alopecia, nausea, rash, constipation, vomiting and stomatitis were also more common in the CDK4/6 inhibitor group. Serious adverse events from any cause were occurred among 308 (19%) persons of 1647 patients in the CDK4/6 inhibitor group, and among 121 people (12%) of 1024 patients in the control group (Table 3).
Table 3: Adverse events from any cause that occurred in at least 10% of the patients in either study group
Adverse event |
CDK4/6 inhibitor group |
Control group |
||
|---|---|---|---|---|
All Grades % (n) |
Grade 3 or 4% (n) |
All Grades % (n) |
Grade 3 or 4% (n) |
|
Any adverse event |
89 (1461) |
77 (1274) |
57 (579) |
37 (384) |
Neutropenia |
70 (1145) |
47 (778) |
5 (51) |
1 (12) |
Leucopenia |
37 (615) |
20 (330) |
3 (33) |
0 (4) |
Fatigue |
39 (635) |
2 (40) |
28 (298) |
1 (8) |
Anaemia |
26 (422) |
5 (75) |
7 (70) |
1 (14) |
Alopecia |
24 (402) |
0 (0) |
10 (103) |
0 (0) |
Thrombocytopenia |
14 (225) |
2 (32) |
18 (182) |
0 (1) |
Vomiting |
21 (351) |
1 (19) |
14 (139) |
1 (12) |
Nausea |
4 (660) |
1 (23) |
25 (261) |
1 (10) |
Diarrhoea |
43 (705) |
4 (72) |
23 (232) |
1 (8) |
Constipation |
19 (305) |
1 (9) |
16 (161) |
0 (2) |
Arthralgia |
22 (358) |
1 (9) |
24 (241) |
1 (7) |
Hot flush |
17 (279) |
0 (1) |
20 (206) |
0 (1) |
Back pain |
16 (267) |
1 (21) |
17 (175) |
1 (7) |
Cough |
18 (296) |
0 (0) |
15 (156) |
0 (0) |
Decreased appetite |
19 (310) |
1 (17) |
12 (118) |
0 (3) |
Headache |
21 (350) |
0 (7) |
19 (196) |
0 (6) |
Pain in extremity |
14 (119) |
0 (1) |
14 (66) |
1 (6) |
Upper respiratory tract infection |
11 (144) |
0 (3) |
8 (56) |
0 (2) |
Stomatitis |
14 (188) |
0 (5) |
6 (42) |
0 (0) |
Nasopharyngitis |
14 (75) |
0 (0) |
10 (30) |
0 (0) |
Dizziness |
13 (112) |
1 (6) |
11 (52) |
0 (0) |
Asthenia |
16 (86) |
2 (12) |
10 (29) |
0 (0) |
Dyspnoea |
13 (167) |
2 (20) |
11 (75) |
1 (9) |
Rash |
15 (237) |
1 (13) |
7 (71) |
0 (1) |
Increased ALT |
12 (130) |
5 (55) |
4 (31) |
1 (8) |
Infections |
46 (312) |
3 (21) |
39 (197) |
3 (13) |
Abdominal pain |
19 (233) |
1 (17) |
9 (57) |
0 (3) |
Insomnia |
13 (99) |
0 (1) |
10 (38) |
0 (0) |
Pyrexia |
11 (141) |
0 (4) |
7 (41) |
0 (1) |
Abbreviations: CDK: cyclin-dependent kinase; ALT: alanine transaminase.
Risk of bias in included RCT studies
Full details about the risk of bias of RCT studies are shown in Figure 5. For allocation concealment, the risk of bias was unclear in three RCTs with an allocation scheme which was not mentioned in the trials. For random sequence generation, the risk of bias was unclear in two RCT studies. For the performance bias and detection bias, the risk was high in one study and unclear in another one. Except these three outliers, no high or unclear risk of bias was observed in any other studies.
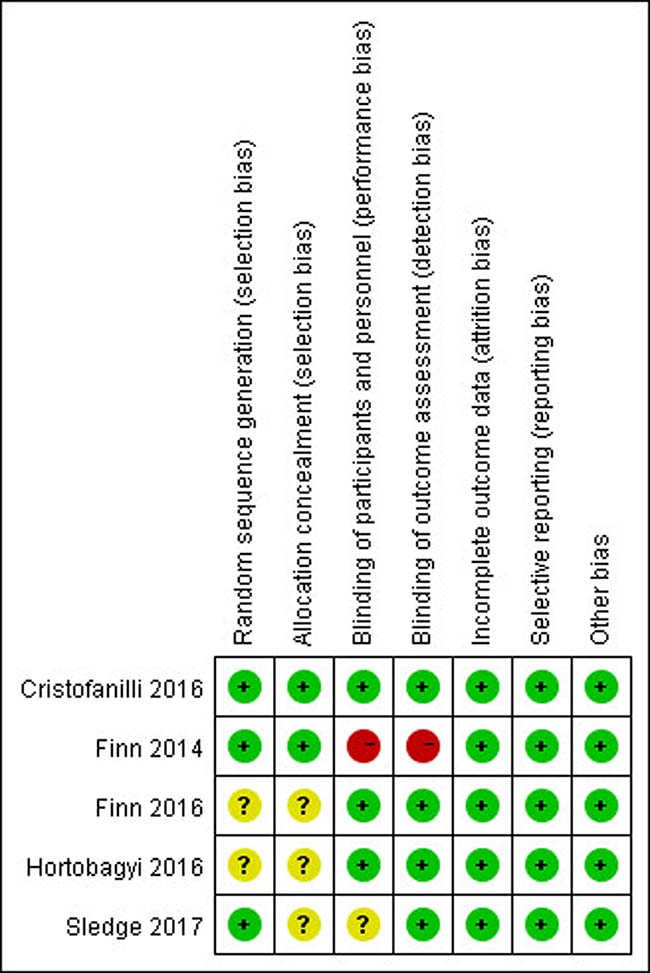
Figure 5: Risk of bias: a summary table for each risk of bias item for each study.
DISCUSSION
As we mentioned above, HR-positive breast cancer is the most common subtype of breast cancer, with the fact that about 80% of breast cancer patients express hormone receptors. And endocrine therapy is a preferred approach for patients with advanced or metastatic disease due to its treatment effectiveness and preferable toxicity profile. To date, improvements have been made in clinical outcomes with both new endocrine agents and new endocrine combinations. Recently, several clinical trial data have suggested that the orally highly selective inhibitors of CDK4/6, such as palbociclib, ribociclib and abemaciclib, would significantly improve the clinical outcomes when combined with letrozole or fulvestrant.
The current meta-analysis we performed which data were collected from five published RCTs presented a higher testing efficiency, and the results showed that the highly selective inhibitors of CDK4/6 were associated with the significant improvement in objective response, clinical benefit, and PFS in patients with HR-positive advanced breast cancer. Furthermore, these results were not influenced by age, race, performance status, disease site, prior chemotherapy, prior endocrine therapy, disease-free interval after adjuvant treatment, the kind of CDK4/6 inhibitors, or biomarkers that affect sensitivity to endocrine therapy, such as the expression level of estrogen and progesterone receptors (Table 2).
In the patients who received the combination treatment with CDK4/6 inhibitors, a higher incidence of hematologic adverse events would occur. The most common hematologic adverse events with grade 3 or 4 were neutropenia (47.2%% vs. 1.1%), leucopenia (20.0% vs. 0.4%), anemia (4.5% vs. 1.4%), and thrombocytopenia (2.4% vs. 0.1%). Although the incidence of neutropenia with any grade in the CDK4/6 inhibitor group was 70% in the current meta-analysis, it did not go along with the significantly increasing rate of febrile neutropenia; the incidence of febrile neutropenia was1.3% (16 of 1206).
Given the increasing risk of toxicity, how to identify the patients who might preferentially benefit from CDK4/6 inhibitors is important. Many predictive biomarkers have been evaluated for this purpose, such as the changed levels of protein RB, cyclin D1 amplification, or p16 loss [15]. Recently, a number of researches have focused on the loss of Rb function, the over expression/amplification of cyclin E, and CDK6 amplification, trying to figure out the possible resistance mechanisms [16–18]. But most of these results remained speculative and have not been validated in clinical specimens. Therefore, these putative biomarkers, however, have not yet been demonstrated to be clinically useful because of the lack of their sufficiently predictive ability or reproducibility.
However, the main reason for permanent treatment discontinuation in both subgroups of meta-analysis was disease progression [9, 10]. The rate of discontinuation due to adverse events was lower than other therapies applied for this population. Majority of adverse events with grade 1 or 2, and grade 3 or 4 were reversible and controlled by dose interruptions and reductions, which allowed most patients to go on with the treatment with light adverse events.
Palbociclib is an orally available pyridopyrimidine compound, which can inhibit CDK 4 and CDK 6. Previous researches have demonstrated that palbociclib have the ability to inhibit pRb phosphorylation as well and cause growth inhibition of tumors, in particularly for the ER-positive subtype of breast cancer [16]. PALOMA-1 [9] and PALOMA-2 [10] trials were designed to assess the safety and efficacy of the combination of palbociclib and letrozole as a first-line therapy for postmenopausal women with HR-positive/HER2-negative advanced breast cancer. The result showed that the patients in the palbociclib–letrozole group (i.e. CDK4/6 inhibitor group) had a longer median PFS (more than 10 months) than those in the letrozole group (i.e. control group). And PALOMA-3 [13] studied the combination of palbociclib and fulvestrant as a second-line treatment for premenopausal and postmenopausal patients with HR-positive/HER2-negative metastatic breast cancer and progression after prior endocrine therapy. Adding palbociclib to endocrine therapy with fulvestrant clinically led to a significant improvement in median PFS from 3.8 months (95% CI = 3.5–5.5) to 9.2 months (95% CI = 7.5 to not estimable). The difference in PFS rates between PALOMA-2 and PALOMA-3 might be caused of the fact that different studies recruited different patient populations (endocrine-sensitive disease vs. endocrine-resistant disease, first-line therapy vs. second-line therapy). Besides, the PARSIFAL phase-II trial compared the efficacy of palbociclib-fulvestrant to palbociclib-letrozole as a first-line treatment [19]. The trail enrolled patients with HR-positive/HER2-negative advanced breast cancer, and the primary endpoint was 1-year PFS. To date, this trial, started from August 2015, has still been in progress and planned to end in July 2017. Subgroup analyses revealed that the PFS was similar in both pre/perimenopausal and postmenopausal patients. And the overall global quality of life scores of palbociclib-treated patients was significantly higher than that in the control group (66.1, 95% CI = 64.5–67.7 vs. 63.0, 95% CI = 60.6–65.3; p = 0.0313) [20].
In addition to palbociclib, two other highly selective inhibitors of CDK4/6, ribociclib and abemaciclib, have currently been in early clinical development. Ribociclib, a oral molecule CDK4/6 inhibitor molecule, has been tested as a first-line therapy in the MONALEESA-2 [11] trial and an initial therapy with letrozole in patients with HR-positive/HER2-negative advanced breast cancer. And this large RCT also supported the results found in our meta-analysis, that adding ribociclib could prolong the duration of PFS and improve the rate of overall response and clinical benefit. Besides ribociclib, abemaciclib is another highly specific oral CDK4/6 inhibitor molecule. Preclinical data verified that abemaciclib can effectively inhibit tumor growth and prolong survival time of patients [21]. MONARCH-1 is a phase-II single-arm study designed to evaluate safety and efficacy of abemaciclib monotherapy in women with HR-positive/HER2-negative advanced breast cancer whose disease progressed on or after endocrine therapy and chemotherapy [22]. In MONARCH-2, patients with similar conditions were given abemaciclib and fulvestrant. The result showed that the rate of objective response was 35.2% (95% CI = 30.8%–39.6%), the clinical benefit rate was 72.2% (95% CI = 68.0%–76.4%), and median PFS was 16.4 months, which significantly improved PFS and ORR compared with placebo plus fulvestrant [23].
The CDK4/6 inhibitors are efficacious and low toxic when applied in combination with various hormonal compounds in the treatment for HR-positive/HER2-negative advanced breast cancer. However, how to combine it with chemotherapy or other targeted drugs is still a significantly clinical problem to be solved. Clinical data showed that CDK4/6 inhibitors could suppress the proliferation of breast cancer cells, which would not only be a great benefit to patients with advanced breast cancer, but also to patients with early breast cancer [24]. Besides, related preclinical researches have shown that HER2+ breast cancer cell lines remain to be sensitive to CDK4/6 inhibitors, indicating that HER2+ breast cancer patients may also benefit from the treatment of CDK4/6 inhibitors [25]. In contrast to ER-positive and HER2-positive disease, one preclinical research has revealed that there was no relevant effect of CDK 4/6 inhibitors on triple-negative subtype of breast cancer [16]. In addition, animal experiments showed that CDK 4/6 inhibitors may have the ability to cross the blood–brain barrier, which can be the potential target for treating brain metastases in patients with breast cancer [26]. Based on this data, a phase-II trial, designed to investigate the potential role of abemaciclib in patients with newly diagnosed brain metastases or brain metastases progressing after prior local therapy who had original HR-positive or HER2-positive breast cancer, has been currently under way (NCT02308020). Nevertheless, there is still doubt whether the CDK4/6 inhibitors have the ability to antagonize the anti-tumor effects of cytotoxic chemotherapy and targeted therapy that have the function of killing cancer cells in cell cycle [27].
This meta-analysis improved the result credibility that CDK 4/6 inhibitors could prolong the PFS, compared with the placebo-treated group from five RCTs. Importantly, several limitations should be noted in our analysis. First, the present meta-analysis only included five published RCTs with 2689 patients, which might cause publication bias. The Finn 2014 trial was a rater-blinded RCT. Although the randomization codes were only released at the time of interim and final analyses without any crossover, and the sensitivity analysis showed that all the outcomes were stable after excluding the Finn 2014 trial, it should still be cautious when applying these results to the clinical practice. Second, overall survival results are not mature and available today. Thus, the finding that this prolonged PFS can result in longer overall survival will not be proved until the further follow-up is completed. However, this result of clinically relevant potential PFS prolongation can already be used in the individual patients to delay the time of cytotoxic chemotherapy, and reduce the associated toxicity, side effects and psychological pressure.
CONCLUSIONS
CDK 4/6 inhibitors can significantly prolong the PFS and improve the objective response or clinical benefit response, which was confirmed in every subgroup of the meta-analysis we performed. Adverse events are reversible, and the rate of discontinuation due to adverse events is low. Further studies should focus on whether treating with CDK4/6 inhibitors can significantly prolong the overall survival of patients with advanced breast cancer.
Abbreviations
HR-positive: hormone receptor positive; ER; estrogen receptor; PR; progesterone receptor; HER2; human epidermal growth factor receptor 2; TNBC: triple-negative breast cancer; CDK4/6: Cyclin-dependent kinases 4/6; Rb: retinoblastoma; pRb: retinoblastoma protein; PFS: progression-free survival; HR: hazard ratio; CI: confidence interval; RR: risk rate; FDA: Food and Drug Administration; ECOG: Eastern Cooperative Oncology Group; RECIST: Evaluation Criteria in Solid Tumors; ALT: alanine transaminase; RCT: randomized controlled trial.
Data availability
All data generated or analyzed during this project are presented in this article (and its Supplementary Information files).
Author contributions
C.J. Tu designedthestudyanddevelopedtheanalysisplan. W Ding and Z.A. Li collectedthedata and performed the meta-analysis. C.Y. Wang and W Ding assessed the risk of bias. W Ding was responsible forwriting of the article. G.D. Ruan and L.P Chen revised the manuscript with helpful comments.
ACKNOWLEDGMENTS
We’d like to thank LiGen Shi and Zhenwei Li for their support and guidance throughout the project.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interests.
REFERENCES
1. Perou CM, Sørlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA, Fluge O, Pergamenschikov A, Williams C, et al. Molecular portraits of human breast tumours. Nature. 2000; 406:747–752.
2. Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005; 365:1687–1717.
3. Di Leo A, Jerusalem G, Petruzelka L, Torres R, Bondarenko IN, Khasanov R, Verhoeven D, Pedrini JL, Smirnova I, Lichinitser MR, Pendergrass K, Garnett S, Lindemann JP, et al. Results of the CONFIRM phase III trial comparing fulvestrant 250 mg with fulvestrant 500 mg in postmenopausal women with estrogen receptor-positive advanced breast cancer. J Clin Oncol. 2010; 28:4594–4600.
4. Chia S, Gradishar W, Mauriac L, Bines J, Amant F, Federico M, Fein L, Romieu G, Buzdar A, Robertson JF, Brufsky A, Possinger K, Rennie P, et al. Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECT. J Clin Oncol. 2008; 26:1664–1670.
5. Osborne CK, Schiff R. Mechanisms of endocrine resistance in breast cancer. Annu Rev Med. 2011; 62:233–247.
6. Higgins MJ, Baselga J. Targeted therapies for breast cancer. J Clin Invest. 2011; 121:3797–3803.
7. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011; 144:646–674.
8. Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012; 490:61–70.
9. Finn RS, Crown JP, Lang I, Boer K, Bondarenko IM, Kulyk SO, Ettl J, Patel R, Pinter T, Schmidt M, Sh paryk Y, Thummala AR, Voytko NL, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015; 16:25–35.
10. Finn RS, Martin M, Rugo HS, Jones S, Im SA, Gelmon K, Harbeck N, Lipatov ON, Walshe JM, Moulder S, Gauthier E, Lu DR, Randolph S, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016; 375:1925–1936.
11. Hortobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, Campone M, Blackwell KL, André F, Winer EP, Janni W, Verma S, Conte P, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016; 375:1738–1748.
12. Turner NC, Ro J, André F, Loi S, Verma S, Iwata H, Harbeck N, Loibl S, Huang Bartlett C, Zhang K, Giorgetti C, Randolph S, Koehler M, et al. Palbociclib in hormone receptor-positive advanced breast cancer. N Engl J Med. 2015; 373:209–219.
13. Cristofanilli M, Turner NC, Bondarenko I, Ro J, Im SA, Masuda N, Colleoni M, DeMichele A, Loi S, Verma S, Iwata H, Harbeck N, Zhang K, et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016; 17:425–439.
14. Watanabe H, Okada M, Kaji Y, Satouchi M, Sato Y, Yamabe Y, Onaya H, Endo M, Sone M, Arai Y. [New response evaluation criteria in solid tumours-revised RECIST guideline (version 1.1)]. [Article in Japanese]. Gan To Kagaku Ryoho. 2009; 36:2495–2501.
15. Dickson MA. Molecular pathways: CDK4 inhibitors for cancer therapy. Clin Cancer Res. 2014; 20:3379–3383.
16. Finn RS, Dering J, Conklin D, Kalous O, Cohen DJ, Desai AJ, Ginther C, Atefi M, Chen I, Fowst C, Los G, Slamon DJ. PD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitro. Breast Cancer Res. 2009; 11:R77.
17. Herrera-Abreu MT, Palafox M, Asghar U, Rivas MA, Cutts RJ, Garcia-Murillas I, Pearson A, Guzman M, Rodriguez O, Grueso J, Bellet M, Cortés J, Elliott R, et al. Early adaptation and acquired resistance to CDK4/6 inhibition in estrogen receptor-positive breast cancer. Cancer Res. 2016; 76:2301–2313.
18. Yang C, Li Z, Bhatt T, Dickler M, Giri D, Scaltriti M, Baselga J, Rosen N, Chandarlapaty S. Acquired CDK6 amplification promotes breast cancer resistance to CDK4/6 inhibitors and loss of ER signaling and dependence. Oncogene. 2016; 36:2255–2264.
19. Llombart-Cussac A, Bellet M, Zamora P, Ruiz M, Gligorov J, Di Cosimo S. A randomized, multicenter, open-label, phase II trial to evaluate the efficacy and safety of palbociclib in combination with fulvestrant or letrozole in patients with ER+/HER2- metastatic breast cancer (MBC). J Clin Oncol. 2016; 34:TPS625.
20. Harbeck N, Iyer S, Turner N, Cristofanilli M, Ro J, André F, Loi S, Verma S, Iwata H, Bhattacharyya H, Puyana Theall K, Bartlett CH, Loibl S. Quality of life with palbociclib plus fulvestrant in previously treated hormone receptor-positive, HER2-negative metastatic breast cancer: patient-reported outcomes from the PALOMA-3 trial. Ann Oncol. 2016; 27:1047–1054.
21. Tolaney SM, Rosen LS, Beeram M, Goldman JW, Gandhi L, Tolcher AW, Papadopoulos KP, Rasco DW, Myrand S, Kulanthaivel P, Andrews JM, Frenzel M, Cronier DM, et al. Clinical activity of abemaciclib, an oral cell cycle inhibitor, in metastatic breast cancer. Cancer Res. 2015; 75:P5–19–13.
22. Dickler MN, Tolaney SM, Rugo HS, Cortés J, Diéras V, Patt D, Wildiers H, Hudis CA, O'Shaughnessy J, Zamora E, Yardley DA, Frenzel M, Koustenis A, Baselga J. MONARCH1: results from a phase II study of abemaciclib, a CDK4 and CDK6 inhibitor, as monotherapy, in patients with HR+/ HER2- breast cancer, after chemotherapy for advanced disease. J Clin Oncol. 2016; 34:510.
23. Sledge GW Jr, Toi M, Neven P, Sohn J, Inoue K, Pivot X, Burdaeva O, Okera M, Masuda N, Kaufman PA, Koh H, Grischke EM, Frenzel M, et al. MONARCH 2: Abemaciclib in Combination With Fulvestrant in Women With HR+/HER2- Advanced Breast Cancer Who Had Progressed While Receiving Endocrine Therapy. J Clin Oncol. 2017; 35:2875–2884.
24. Curigliano G, Gómez Pardo P, Meric-Bernstam F, Conte P, Lolkema MP, Beck JT, Bardia A, Martínez García M, Penault-Llorca F, Dhuria S, Tang Z, Solovieff N, Miller M, et al. Ribociclib plus letrozole in early breast cancer: a presurgical, window-of-opportunity study. Breast. 2016; 28:191–198.
25. Goel S, Wang Q, Watt AC, Tolaney SM, Dillon DA, Li W, Ramm S, Palmer AC, Yuzugullu H, Varadan V, Tuck D, Harris LN, Wong KK, et al. Overcoming therapeutic resistance in HER2-positive breast cancers with CDK4/6 inhibitors. Cancer Cell. 2016; 29:255–269.
26. Berghoff A, Bago-Horvath Z, De Vries C, Dubsky P, Pluschnig U, Rudas M, Rottenfusser A, Knauer M, Eiter H, Fitzal F, Dieckmann K, Mader RM, Gnant M, et al. Brain metastases free survival differs between breast cancer subtypes. Br J Cancer. 2012; 106:440–446.
27. Xu H, Yu S, Liu Q, Yuan X, Mani S, Pestell RG, Wu K. Recent advances of highly selective CDK4/6 inhibitors in breast cancer. J Hematol Oncol. 2017; 10:97.