
INTRODUCTION
Breast cancer can present in many different ways with regards to stage, phenotype, location, and heterogeneity of the disease. Many treatment options are available, and their efficacy is highly dependent on the disease characteristics. Treatment of non-rapidly progressive metastatic breast cancer (MBC) is stratified on the basis of the tumor expression of receptors that are targets for pharmacological intervention. Human epidermal growth factor receptor 2 (HER2-) and hormone receptor (HR–estrogen receptor (ER) and progesterone receptor (PR)) targeted and hormonal therapies are recommended for patients with tumors that express these receptors [1, 2]. Patients with negative receptor status (HER2- and HR-negative) of the metastatic disease do not respond to targeted therapy in general, therefore, chemotherapy remains as a treatment option [3, 4]. Targeted therapy for MBC can potentially prolong the survival of MBC patients [5], but can also be costly and may bring adverse effects. New targeted therapies regularly become available (e.g. palbociclib, pertuzumab) and a prior selection of patients is crucial to optimize outcomes of targeted therapy at acceptable costs. Moreover, this may also improve progression-free and overall survival [5], and further minimize adverse effects and avoid unnecessary harms and associated costs for those who do not respond.
Targeted treatment for MBC patients is currently selected and administered according to pathology results of tumor receptor status, often obtained from the primary tumor. However, pathology can often be inconclusive or insufficient regarding receptor expression [6], and receptor expression in the primary tumor or in a single metastatic lesion is not necessarily identical or reflects the receptor status of all metastases [7–11]. As an alternative positron emission tomography and computed tomography (PET/CT) imaging with the tracers 16α-[18F]fluoro-17β-estradiol (FES) and zirconium-89-(89Zr)-trastuzumab has been proposed to evaluate the tumor ER and HER2 expression in MBC and thus guide the selection of patients who might benefit from targeted treatment [12–15].
Since molecular imaging with PET/CT is perceived as expensive and there is still uncertainty regarding its sensitivity and specificity, prior evaluation of its potential cost-effectiveness when applied to select first-line targeted treatment in MBC patients is warranted. Previous economic evaluations of PET/CT in MBC are limited to diagnosis of the disease [16, 17]. As a result, the potential cost-effectiveness of the application of molecular PET/CT imaging to select targeted treatment in MBC patients is unclear. Therefore, the aim of this study was to evaluate the potential cost-effectiveness of PET/CT with FES and 89Zr-trastuzumab tracers compared to pathology testing to select first-line targeted treatment in MBC patients with non-rapidly progressive disease. We worked on a model including a “biopsy versus imaging” strategy for receptor status evaluation because we wanted to test the potential cost-effectiveness of PET/CT with FES and 89Zr-trastuzumab as a one-stop shop for treatment selection in MBC. We limited our analysis to a few important treatment options to demonstrate proof of concept of potential cost-effectiveness of imaging, instead of working on a model including all new targeted therapies.
RESULTS
For baseline scenario 1 we assumed that the sensitivity of FES-PET/CT and 89Zr-trastuzumab PET/CT was set at 77.1% and the specificity was set at 80%, as this was the minimum at which PET/CT could demonstrate potential cost-effectiveness. For baseline scenario 2 we assumed that the sensitivity of FES-PET/CT and 89Zr-trastuzumab PET/CT was set at 80% and the specificity was set at 76.7%, as this was the minimum at which PET/CT could demonstrate potential cost-effectiveness. The results from the decision analytical model are presented in Table 1.
Table 1: Simulation results for the care as usual and the intervention pathways for a hypothetical cohort of 1,000 women
Care as usual |
Intervention |
Care as usual |
Intervention |
|
|---|---|---|---|---|
Baseline scenario 1 |
Baseline scenario 2 |
|||
Diagnosed MBCs |
||||
Bone |
228 |
234 |
228 |
235 |
Lung |
199 |
203 |
199 |
204 |
Brain |
65 |
66 |
65 |
66 |
Liver |
159 |
163 |
159 |
163 |
Cost of receptor status evaluation (in k€) |
695 |
3,500 |
695 |
3,500 |
Cost of therapies (in k€) |
||||
Chemotherapy |
1,700 |
1,700 |
1,700 |
1,800 |
Trastuzumab monotherapy |
360 |
370 |
360 |
366 |
Trastuzumab with paclitaxel or vinorelbine) |
1,700 |
1,740 |
1,700 |
1,740 |
Anastrozole |
790 |
815 |
790 |
811 |
Letrozole |
990 |
1,020 |
990 |
1,014 |
Trastuzumab + hormonal therapy |
4,300 |
4,500 |
4,300 |
4,170 |
Total costs (in k€) |
7,800*/9,400** |
10,900*/12,500** |
7,800*/9,400** |
10,700*/12,200** |
Total LYG |
1,500*/1,700** |
1,600*/1,700** |
1,500*/1,700** |
1,600*/1,700** |
ICER |
n/a |
71,000*/77,000** |
n/a |
74,000*/80,000** |
*If ER+/HER2– patients were treated with Anastrozole and ER-/HER2+ patients were treated with Trastuzumab monotherapy;
**If ER+/HER2- patients were treated with Letrozole and ER-/HER2+ patients were treated with Trastuzumab combination therapy (trastuzumab and paclitaxel).
n/a – not applicable.
Health effects and costs
More MBC lesions were detected in the intervention pathway than in the care as usual pathway. The diagnostic costs to evaluate the receptor status and the treatment costs were also higher in the intervention strategy, as were total costs and total life years gained (LYG). The treatment with anastrozole and trastuzumab monotherapy was cheaper than the use of letrozole and trastuzumab combination therapy (trastuzumab and paclitaxel) (Table 1).
Cost-effectiveness
The incremental cost-effectiveness ratio (ICER) for replacing biopsies with PET/CT imaging with FES and 89Zr-trastuzumab for receptor status evaluation and treatment selection in MBC patients (assuming sensitivity of 77.1% and specificity of 80%) ranged from to €71,000 to €77,000 per LYG if patients were treated with letrozole and trastuzumab combination therapy (trastuzumab and paclitaxel), or with anastrozole and trastuzumab monotherapy, respectively (baseline scenario 1, Table 1).
The ICER for replacing biopsies with PET/CT imaging with FES and 89Zr-trastuzumab for receptor status evaluation and treatment selection in MBC patients (assuming sensitivity of 80% and specificity of 76.7%) ranged from to €74,000 to €80,000 per LYG if patients were treated with letrozole and trastuzumab combination therapy (trastuzumab and paclitaxel), or with anastrozole and trastuzumab monotherapy, respectively (baseline scenario 2, Table 1).
Sensitivity analyses
When the probabilities of inconclusive and unobtainable biopsies were set at their minimum values (i.e. 10%), the minimum sensitivity and specificity of FES-PET/CT and 89Zr-trastuzumab PET/CT, at which the intervention strategy was likely to be cost-effective were 90% and 90.6%, respectively. For values of PET/CT sensitivity and specificity below 90% and 90.6%, respectively, the intervention strategy was dominated, because it was costlier and less effective than the care as usual. For even lower values of PET/CT sensitivity and specificity, below 70% and 80%, respectively, effectiveness was logically even less. This lack of effectiveness resulted in cost savings from avoided treatment costs as compared to care as usual (Supplementary Appendix A, Supplementary Tables A1 and A2).
When the probabilities of inconclusive and unobtainable biopsies were set at 15%, the minimum sensitivity and specificity of FES-PET/CT and 89Zr-trastuzumab PET/CT, at which the intervention strategy was likely to be cost-effective were 83% and 86%, respectively. Below these values for PET/CT sensitivity and specificity the intervention strategy was less effective than the care as usual (Supplementary Appendix A, Supplementary Tables A1 and A2).
When the probabilities of inconclusive and unobtainable biopsies were set at 20%, for values of PET/CT sensitivity and specificity below 77% and 80%, respectively, the intervention strategy was less effective than the care as usual (Supplementary Appendix A, Supplementary Tables A1 and A2).
When the probabilities of inconclusive and unobtainable biopsies were set at their maximum values (i.e. 30%), the minimum sensitivity, at which the intervention strategy was likely to be cost-effective was 59.6% and the corresponding specificity was 70%. Alternatively, the lowest specificity value for which the intervention strategy was still cost-effective than care as usual was 58.5 %, at a sensitivity of 70%. For values of PET/CT sensitivity and specificity below these, the intervention strategy was less effective than the care as usual (Supplementary Appendix A, Supplementary Tables A1 and A2).
DISCUSSION
The aim of this study was to assess the potential cost-effectiveness of applying PET/CT with FES and 89Zr-trastuzumab as compared to pathology testing to select first-line treatment in MBC patients with non-rapidly progressive disease. A previously published and validated computer model on metastatic breast cancer simulation was extended and applied in this analysis. The intervention pathway yielded higher costs to evaluate receptor status of the MBC disease and select treatment as compared to the care as usual pathway. The number of LYG was also higher in the intervention pathway, provided sensitivity and specificity were sufficiently high. The application of PET/CT with FES and 89Zr-trastuzumab tracers for selecting the first-line therapy in MBC had the potential to be cost-effective when the sensitivity and the specificity of the PET/CT were at least 77.1% and 80% (aiming at the lowest sensitivity), or – starting with low values of specificity: 80% and 76.7%, respectively. The results of this analysis reflected the expected LYG, costs and cost-effectiveness in MBC patients based on the receptor status of their disease (either ER or HER2, or both).
The clinical value of PET/CT has thus far only been established with the FDG tracer for detection, staging, re-staging and therapy monitoring in various neoplastic processes, including breast cancer [18–21]. FDG-PET was included in some guidelines for breast cancer work-up, but the value of FDG-PET in metastatic breast cancer has been debated. FDG-PET could aid the staging of the disease (i.e. detect lesions), but it does not provide information about the status of the drug targets in the lesions [18–21]. PET/CT with the FES and the 89Zr-trastuzumab tracers could provide a whole-body visualization of metastatic recurrence after breast cancer and its ER- and HER2-status. Therefore, it has implications for therapy selection, personalized treatment and follow-up which may result in increase of survival [12–15, 22]. Furthermore, PET/CT with FES and 89Zr-trastuzumab could be a valuable alternative in situations where biopsy is not feasible. Biopsy could only give information about several drug targets in a small part of a single lesion. In contrast, PET/CT imaging could give information about a few targets in all lesions in the body. It is known that discrepancy in target expression between lesions in a single patient is observed in a high percentage of the patients (10 – 30%) [8–12].
We varied the sensitivity and the specificity of PET/CT with FES and 89Zr-trastuzumab from 0 to 100% to evaluate different combinations of these at which the intervention pathway was likely to be cost-effective. The values for sensitivity and specificity in our analysis are theoretical and suggest a precision which is not reached in daily practice. Previous studies showed a high sensitivity of FES-PET (overall 84%), but with considerable variability between studies (range 69–100 %) [14]. This variability was probably due to differences in inclusion criteria and the location of lesions. FES-PET/CT demonstrated high sensitivity in patients with bone and lung lesions, and relatively poor sensitivity in patients with liver and brain lesions. The specificity of FES-PET/CT in ER-positive lesions is generally very high in all studies (overall 98%) [14]. For 89Zr-trastuzumab PET, no sensitivity and specificity data are available yet. Our analysis demonstrated that even small increase in the sensitivity and the specificity of PET/CT could have a large impact on its potential cost-effectiveness. Whether the impact of FES-PET/CT and 89Zr-trastuzumab-PET/CT on treatment selection in MBC would actually result in prolonged progression-free and overall survival and maintained quality of life is yet to be determined [23].
There are currently few economic evaluations of PET/CT which are mainly aimed at assessing its cost-effectiveness in diagnosing and staging of different types of cancers [16, 17, 19–21]. PET/CT with FDG tracer was found to be cost-effective in pre-operative staging of colorectal cancer, non-small cell lung cancer and solitary pulmonary nodes [19–21]. FDG-PET/CT was also found beneficial in evaluating the treatment response in the follow-up of non-small cell lung cancer [20, 21]. Previously, we have demonstrated that FES-PET/CT can diminish the number of both false positive and false negative results when applied as a first choice diagnostic to ER-positive MBC patients. In addition, it could decrease the number of imaging and pathology tests required to diagnose distant relapse [16]. Other studies have demonstrated that PET/CT could generate more quality-adjusted life years (QALYs) in comparison to the standard work-up for diagnosing MBC at an incremental cost of ₤29,700 (~ €36,000) per QALY [17]. The limited economic evaluations of PET/CT resulted from lack of clinical data from randomized controlled trials (RCTs) or observational studies which explore the potential of PET/CT for treatment selection and response monitoring.
This study evaluated the potential cost-effectiveness of the application of molecular imaging with PET/CT for selecting the first-line treatment in MBC. Although our findings clearly demonstrated the potential of PET/CT with FES- and 89Zr-trastuzumab tracers to be cost-effective when selecting the first-line treatment in MBC patients we must be aware of the limitations of this analysis.
We simplified our approach and limited it to a “biopsy versus imaging” for receptor status evaluation and a few important treatment options to demonstrate proof of concept. It should be noted here, that combinations of biopsy and imaging, and other treatment options can be substituted into the model, if necessary. This study is a starting point for further research on more specific situations using a more sophisticated model.
The data regarding the inconclusive and unobtainable rate of biopsies to detect MBC and reveal receptor status were obtained from literature and not from a dedicated RCT or cohort study aimed at evaluating these parameters.
The possible treatment combinations were limited to those listed in NICE guidance documents, irrespective of the recommendation status, and therefore did not necessarily reflect therapeutic advances and variety in management of MBC patients. Costs of therapies were obtained from the NICE guidelines, converted to euros according to the 2016 exchange rate and corrected for the difference in per capita expenses between the United Kingdom and the Netherlands using World data bank estimates, that is costs of all therapies were valued in 2016 euros and used a fixed PPP (Purchasing Power Parity) conversion rate, not a fluctuating exchange rate. Thus, they were normalized for inflation and exchange rate fluctuations.
Another limitation of the current analysis is that the data on survival periods were obtained from reviews and meta-analyses of RCTs examining the progression-free and overall survival after a specified type of treatment. These survival periods did not necessarily reflect the survival of MBC patients according to the location of the distant spread and the breast cancer subtype (luminal A, luminal B, luminal/ HER2, HER2-enriched, basal-like, and triple negative nonbasal). As it is known that every cancer subtype demonstrates a distinct pattern of metastatic relapse and the location of the metastatic spread is associated with notable differences in survival, including these probabilities in the model alongside the probability of different survival according to the type of treatment would allow for a more precise estimation of the expected incremental cost-effectiveness. This would have implications not only for the improved survival rate but for costs as well as MBC patients who survive longer would incur additional substantial costs for their end of life care and treatment.
Furthermore, we assumed a single number for the sensitivity and the specificity of PET/CT for both FES and 89Zr-trastuzumab, but it is known that sensitivity and specificity are highly dependent on, amongst others, the expression levels of the target, the instrumentation and the characteristics of the tracer used. Another limitation was that a significant fraction of the patients has a heterogeneous receptor status between lesions (i.e. some lesions are positive, while others are negative). Pathology cannot provide information about this heterogeneity. On the other hand, little is known about the impact of heterogeneity on treatment selection.
We did not take into consideration the complications resulting from obtaining invasive pathology tests, which could also affect the costs and the quality of life of MBC patients.
Non-responsiveness to selected therapy and adverse effects resulting from assigned therapies were also not evaluated and these could affect costs and survival, and thus cost-effectiveness estimates.
We only considered first-line treatment selection in our analysis, therefore, second-line therapies and the potential application of molecular imaging for treatment selection in second-line and beyond metastatic setting was outside the scope of this study.
The uncertainty and the limitations in our study were mainly due to the lack of clinical data from RCTs and observational studies investigating the role of PET/CT for treatment selection in MBC patients. Initial data from other studies regarding the sensitivity and the specificity of Zr-trastuzumab PET demonstrated multiple false positives in presumed HER2-negative patients but the sample size was small [24]. Part or all of these uncertainties and limitations in data availability could be solved when a recent RCT aimed at patient-tailored cancer treatment supported by molecular imaging is concluded [23]. This would allow to explore other premises in which PET/CT would not replace pathology in all patients but would be added in specific cases.
The application of PET/CT with FES and 89Zr-trastuzumab as a replacement for care as usual in first-line treatment selection in MBC patients comes at additional costs but has the potential to be a cost-effective intervention. The minimum sensitivity and specificity at which PET/CT imaging with FES and 89Zr-trastuzumab tracers would be cost-effective were estimated at 77.1% and 80%, or 80% and 76.7%, respectively. PET/CT imaging with FES and 89Zr-trastuzumab tracers could be a promising advancement in the treatment selection in MBC [22–24]. Our analysis, however, demonstrated that even a small increase in the sensitivity and the specificity of PET/CT can have a large impact on its potential cost-effectiveness. As the current analysis has uncertainties and limitations resulting from the lack of RCTs’ or cohort study clinical data, additional prospective research (in terms of more and larger clinical studies) is required to validate the role of PET/CT in treatment selection and assess the generalizability of the reported benefits, particularly given the associated costs of the modality.
MATERIALS AND METHODS
A published and validated computer model on metastatic breast cancer simulation (MBCSIM) served as a basis for this analysis [16]. The MBCSIM model was designed to simulate the follow-up of women after initial breast cancer and diagnose MBC in women who exhibited symptoms suggestive of distant relapse from the Dutch health care perspective. Detailed description of the MBCSIM model and its parameters could be found in a previous publication [16].
Structure of the model
For this application, we designed a decision tree which extended the MBCSIM model by incorporating targeted treatment selection components after diagnosing the distant relapse. The structure of the current model and its parameters are presented in Figure 1 and Table 2. The presence of distant relapse was based on the probability of developing MBC and distributed over four locations (bone, lung, liver, brain). When MBC was diagnosed, the patient followed either a care as usual pathway or an intervention pathway involving targeted therapy.
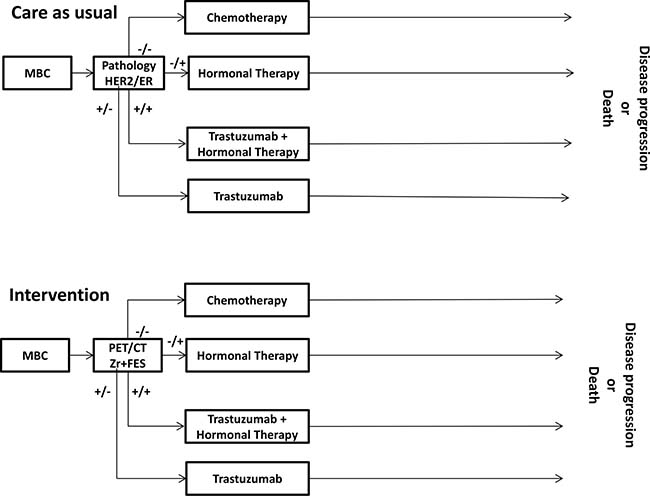
Figure 1: Flow chart of the decision analytical model.
Table 2: Parameters of the decision analytical model
Baseline estimate (%) |
Minimum estimate (%) |
Maximum estimate (%) |
Reference |
|
|---|---|---|---|---|
Distribution of location of MBC |
||||
Bone |
46 |
25 |
61 |
25 |
Lung |
40 |
26 |
60 |
|
Brain |
13 |
7 |
28 |
|
Liver |
32 |
24 |
49 |
|
Probability of MBC being ER+ |
62 |
45 |
70 |
7 |
Probability of MBC being ER– |
26 |
23 |
30 |
7 |
Probability of MBC being HER2+ |
18 |
14 |
20 |
8 |
Probability of MBC being HER2– |
76 |
72 |
80 |
8 |
Probability of inconclusive pathology |
20 |
10 |
30 |
16 |
Probability of unobtainable pathology |
20 |
10 |
30 |
9–11 |
Survival periods (in months) |
||||
after chemotherapy |
22.7 |
20.3 |
31.9 |
5, 26–30 |
after trastuzumab therapy |
32.2 |
25.4 |
40.8 |
|
after hormonal therapy |
28.6*/33.2** |
17.4*/32.3** |
39.2*/34** |
|
after trastuzumab and hormonal therapy |
34.1 |
n/a |
n/a |
|
*anastrozole, **letrozole, n/a – not available.
Simulated patient population
We used two hypothetical cohorts of 1000 women each to perform the simulations for the care as usual and the intervention pathways. The women in each cohort were diagnosed and treated for primary breast cancer. Within the 5-year period after primary diagnosis these women developed distant relapse. The presence of metastatic disease was simulated on the basis of the risk to develop distant relapse over time and distributed over the four most common locations, bone, lung, liver, and brain. The receptor status of the primary tumor as well as the probability of receptor change in the metastatic disease was based on literature. In the simulation, each cohort was assigned to either the care as usual or the intervention pathway irrespective of the receptor status of the primary breast cancer.
Strategies for treatment selection in MBC
Two pathways for selecting targeted treatment in MBC patients were compared.
Care as usual pathway
In the care as usual pathway after being diagnosed with MBC, patients were assumed to undergo pathology testing to determine the ER- and HER2-expression of the biopsied lesions. Then patients were assigned to therapy based on the receptor status of their disease as determined by the pathology results. Patients with metastatic lesions which expressed positive ER and positive HER2 status received first-line trastuzumab and hormonal therapy (anastrozole). Patients with metastatic lesions which expressed positive ER and negative HER2-status were assigned to first-line hormonal therapy alone (either anastrozole or letrozole). Patients with metastatic lesions who tested negative on the ER and positive on the HER2-status received first-line trastuzumab (mono or combination (trastuzumab and paclitaxel) therapy). Patients with metastatic lesions which had negative ER and HER2-expression received first-line chemotherapy.
Intervention pathway
In the intervention pathway two PET/CT scans with different tracers, FES and 89Zr-trastuzumab, replaced pathology testing to establish receptor status of the MBC disease, and the relevant therapy was assigned on the basis of the PET imaging results.
Parameters of the decision analytical model
The parameters of the model and their baseline, minimum and maximum estimates were derived from literature (Table 2). The distribution of the locations of MBC was obtained from a cohort of patients diagnosed with primary disease and subsequently developed MBC within a 5-year follow-up [25]. The overall survival estimates were based on meta-analyses and RCTs of receptor positive MBC patients treated with targeted, hormonal and chemo- therapies [5, 26–30]. The inconclusive rate of pathology and the rate of unobtainable pathology samples were based on previous publications [9–11, 16]. As studies reporting on the sensitivity and specificity of PET/CT with different tracers were either limited [14, 15, 24] or still in progress [23], we chose to vary these parameters independently of age and of the location of the MBC to analyze cost-effectiveness.
Outcomes
The outcomes evaluated were life years gained (LYG), costs (diagnosis and treatment related), and cost-effectiveness (incremental cost-effectiveness ratio – ICER).
Health effects
Life years gained were modeled by assigning survival periods to the different health states. These survival periods were obtained from meta-analyses and RCTs which estimated overall survival of MBC patients treated with targeted, hormonal and chemo- therapies [5, 26–30].
Costs
Only direct costs of imaging tests and treatment regimens were included, valued in euros. The costs of the imaging and pathology tests were obtained from the tariffs level for 2016 (Table 3) [31]. Only Food and Drug Agency and European Medicines Agency approved hormonal, targeted and chemotherapies were considered for costing. The costs of the approved therapies were obtained from the National Institute for Health and Care Excellence (NICE) guidance reports [32–38], and corrected for the difference in per capita expenses between the United Kingdom and the Netherlands using World data bank estimates from 2015 [39].
Table 3: Costs of imaging and pathology tests, and treatment
Cost in € |
Reference |
|
|---|---|---|
Imaging test |
||
PET whole body |
1,144 |
31 |
CT bone |
175 |
31 |
CT lung |
194 |
31 |
CT brain |
145 |
31 |
CT liver |
207 |
31 |
Pathology test |
||
Liver |
137 |
31 |
Bone/lung/brain |
657 |
31 |
Treatment options |
||
Trastuzumab monotherapy |
9,730 |
33, 34, 37–39 |
Trastuzumab combination therapy (trastuzumab and paclitaxel) |
46,080 |
|
Trastuzumab + anastrozole |
48,512 |
33, 34, 36–39 |
Docetaxel |
11,015 |
35, 37–39 |
Anastrozole |
2,141 |
36, 37–39 |
Letrozole |
2,676 |
36, 37–39 |
The treatment costs represent cost per patients for the whole duration of treatment.
Table 3 presents the costs per treatment for the whole duration of treatment and the average duration of treatment is provided in Appendix B. Detailed description of costs and cost calculations is available in Supplementary Appendix B. Costs of pathology complications, treatment of adverse events or palliative care, and second and third line treatment were not taken into account. Discounting was not applied due to the relatively short-time horizon (less than 5 years) of the analysis.
Cost-effectiveness analyses
A health payer perspective was adopted. The total costs of each pathway was calculated by summing the costs of all performed tests and the selected treatments. The ICER was calculated by dividing the incremental cost by the number of incremental LYG. Potential cost-effectiveness was established by varying the sensitivity and the specificity of the PET/CT and assessing the impact of these variations on the ICERs.
In the Netherlands, an informal ceiling ratio of € 80,000 per LYG was established by the Dutch Council for Public Health and Health Care [40]. This is considered a maximum ceiling ratio applicable when there is a high burden of disease, as is the case of MBC.
Sensitivity analyses
A univariate sensitivity analysis was performed for practical reasons. Since the model has demonstrated to be predominantly sensitive to the input parameters related to the sensitivity and the specificity of the PET/CT and the pathology failure, it was considered that a probabilistic sensitivity analysis where all the input parameters were changed at the same time would not provide essentially different information. Therefore, univariate sensitivity analyses with minimum and maximum values of the 95% CI for the input parameters listed in Table 2 for the entire cohort of 1,000 women were performed to evaluate the effects of parameter uncertainty in each pathway.
Since sensitivity and specificity show a certain trade-off, we evaluated different combinations of these, setting in turn sensitivity or specificity at a pre-specified value and then varying the remaining parameter. We analyzed the values at which the intervention was just cost-effective (at €80,000 per LYG), effective (had positive LYG) and some fixed values below and above these values, to gain insight into the changes in incremental cost-effectiveness of the intervention as compared to the care as usual, for three different values of biopsy failure probability. We used values of 77.4% for sensitivity and 80% for specificity in the baseline scenario 1 and 80% and 76.7%, respectively, for baseline 2 to calculate the point estimate for the cost-effectiveness. The sensitivity of FES-PET/CT ranges between 69% and 100% and the specificity varies between 80% and 100% [14]. For the sensitivity analyses we applied a fixed sensitivity and varying specificity of PET/CT (Supplementary Table A1) as well as a fixed specificity and varying sensitivity (Supplementary Table A2) to estimate the sensitivity of the ICER resulting from the error margins in the PET/CT sensitivity and specificity.
Author contributions
GHdB, MJWG and RKK designed the study. GHdB, MJWG, RKK and EFJdV provided study materials. RKK and KMV collected and assembled the data. GHdB, MJWG, TLF and RKK analyzed the data and all authors were involved in the interpretation of the results. All authors participated in manuscript writing. All authors read and approved the final manuscript.
Note
Callout for reference [41] is included into Supplementary File.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
1. NCCN Guidelines Version 2 Available at http://www.NCCN.com, accessed on 15.06.2016. 2016.
2. Cardoso F, Costa A, Norton L, Senkus E, Aapro M, André F, Barrios CH, Bergh J, Biganzoli L, Blackwell KL, Cardo so MJ, Cufer T, El Saghir N, et al. ESO-ESMO 2nd international consensus guidelines for advanced breast cancer (ABC2). Ann Oncol. 2014; 25:1871–88. https://doi.org/10.1093/annonc/mdu385.
3. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, Fleming T, Eiermann W, Wolter J, Pegram M, Baselga J, Norton L. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001; 344:783–92. https://doi.org/10.1056/NEJM200103153441101.
4. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, Goldhirsch A, Untch M, Smith I, Gianni L, Baselga J, Bell R, Jackisch C, Cameron D, Dowsett M, Barrios CH, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005; 353:1659–72. https://doi.org/10.1056/NEJMoa052306.
5. Koleva-Kolarova RG, Oktora MP, Robijn AL, Greuter MJ, Reyners AK, Buskens E, de Bock GH. Increased life expectancy as a result of non-hormonal targeted therapies for HER2 or hormone receptor positive metastatic breast cancer: a systematic review and meta-analysis. Cancer Treat Rev. 2017; 55:16–25. https://doi.org/10.1016/j.ctrv.2017.01.001.
6. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, Fitzgibbons PL, Francis G, Goldstein NS, Hayes M, Hicks DG, Lester S, Love R, et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010; 28:2784–2795. https://doi.org/10.1200/JCO.2009.25.6529.
7. Amir E, Ooi WS, Simmons C, Kahn H, Christakis M, Popovic S, Kalina M, Chesney A, Singh G, Clemons M. Discordance between receptor status in primary and metastatic breast cancer: an exploratory study of bone and bone marrow biopsies. Clin Oncol (R Coll Radiol). 2008; 20:763–768. https://doi.org/10.1016/j.clon.2008.08.005.
8. Lower E, Glass E, Blau R, Harman S. HER-2/neu expression in primary and metastatic breast cancer. Breast Cancer Res Treat. 2009; 113:301–306. https://doi.org/10.1007/s10549-008-9931-6.
9. Amir E, Miller N, Geddie W, Freedman O, Kassam F, Simmons C, Oldfield M, Dranitsaris G, Tomlinson G, Laupacis A, Tannock IF, Clemons M. Prospective study evaluating the impact of tissue confirmation of metastatic disease in patients with breast cancer. J Clin Oncol. 2012; 30:587–592. https://doi.org/10.1200/JCO.2010.33.5232.
10. André F, Bachelot T, Commo F, Campone M, Arnedos M, Dieras V, Lacroix-Triki M, Lacroix L, Cohen P, Gentien D, Adélaide J, Dalenc F, Goncalves A, et al. Comparative genomic hybridisation array and DNA sequencing to direct treatment of metastatic breast cancer: a multicentre, prospective trial (SAFIR01/UNICANCER). Lancet Oncol. 2014; 15:267–74. https://doi.org/10.1016/S1470-2045(13)70611-9.
11. Thompson AM, Jordan LB, Quinlan P, Anderson E, Skene A, Dewar JA, Purdie CA; Breast Recurrence in Tissues Study Group. Prospective comparison of switches in biomarker status between primary and recurrent breast cancer: the Breast Recurrence In Tissues Study (BRITS). Breast Cancer Res. 2010; 12:R92. https://doi.org/10.1186/bcr2771.
12. Peterson LM, Mankoff DA, Lawton T, Yagle K, Schubert EK, Stekhova S, Gown A, Link JM, Tewson T, Krohn KA. Quantitative imaging of estrogen receptor expression in breast cancer with PET and 18F-fluoroestradiol. J Nucl Med. 2008; 49:367–374. https://doi.org/10.2967/jnumed.107.047506.
13. Peterson LM, Kurland BF, Schubert EK, Link JM, Gadi VK, Specht JM, Eary JF, Porter P, Shankar LK, Mankoff DA, Linden HM. A Phase 2 Study of 16α-[18F]-fluoro-17β-estradiol positron emission tomography (FES-PET) as a marker of hormone sensitivity in metastatic breast cancer (MBC). Mol Imaging Biol. 2014; 16:431–440. https://doi.org/10.1007/s11307-013-0699-7.
14. Van Kruchten M, Glaudemans AW, De Vries EF, Beets-Tan RG, Schröder CP, Dierckx RA, de Vries EG, Hospers GA. PET imaging of oestrogen receptors in patients with breast cancer. Lancet Oncol. 2013; 14:e465–75. https://doi.org/10.1016/S1470-2045(13)70292-4.
15. Gaykema SB, Schröder CP, Vitfell-Rasmussen J, Chua S, Oude Munnink TH, Brouwers AH, Bongaerts AH, Akimov M, Fernandez-Ibarra C, Lub-de Hooge MN, de Vries EG, Swanton C, Banerji U. 89Zrtrastuzumab and 89Zr-bevacizumab PET to evaluate the effect of the HSP90 inhibitor NVP-AUY922 in metastatic breast cancer patients. Clin Cancer Res. 2014; 20:3945–3954. https://doi.org/10.1158/1078-0432.CCR-14-0491.
16. Koleva-Kolarova RG, Greuter MJ, van Kruchten M, Vermeulen KM, Feenstra T, Buskens E, Glaudemans AW, de Vries EF, de Vries EG, Hospers GA, de Bock GH. The value of PET/CT with FES or FDG tracers in metastatic breast cancer: a computer simulation study in ER-positive patients. Br J Cancer. 2015; 112:1617–1625. https://doi.org/10.1038/bjc.2015.138.
17. Auguste P, Barton P, Hyde C, Roberts TE. An economic evaluation of positron emission tomography (PET) and positron emission tomography/computed tomography (PET/CT) for the diagnosis of breast cancer recurrence. Health Technol Assess. 2011; 15:1–54. https://doi.org/10.3310/hta15180.
18. Dirisamer A, Halpernb BS, Flöryc D, Wolf F, Beheshti M, Mayerhoefer ME, Langsteger W. Integrated contrast-enhanced diagnostic whole-body PET/CT as a first-line restaging modality in patients with suspected metastatic recurrence of breast cancer. Eur J Radiol. 2010; 73:294–9. https://doi.org/10.1016/j.ejrad.2008.10.031.
19. Brush J, Boyd K, Chappell F, Crawford F, Dozier M, Fenwick E, Glanville J, McIntosh H, Renehan A, Weller D, Dunlop M. The value of FDG positron emission tomography/computerised tomography (PET/CT) in pre-operative staging of colorectal cancer: a systematic review and economic evaluation. Health Technol Assess. 2011; 15:1–210. https://doi.org/10.3310/hta15350.
20. Cao JQ, Rodrigues GB, Louie AV, Zaric GS. Systematic review of the cost-effectiveness of positron-emission tomography in staging of non–small-cell lung cancer and management of solitary pulmonary nodules. Clin Lung Cancer. 2012; 13:161–70. https://doi.org/10.1016/j.cllc.2011.09.002.
21. Van Loon J, Grutters JP, Wanders R, Boersma L, Dingemans AM, Bootsma G, Geraedts W, Pitz C, Simons J, Brans B, Snoep G, Hochstenbag M, Lambin P, et al. 18FDG-PET-CT in the follow-up of non-small cell lung cancer patients after radical radiotherapy with or without chemotherapy: An economic evaluation. Eur J Cancer. 2010; 46:110–119. https://doi.org/10.1016/j.ejca.2009.10.028.
22. Liao GJ, Clark AS, Schubert EK, Mankoff DA. 18F-Fluoroestradiol PET: Current status and potential future clinical applications. J Nucl Med. 2016; 57:1269–75. https://doi.org/10.2967/jnumed.116.175596.
23. IMaging PAtients for Cancer Drug selecTion – Metastatic Breast Cancer (IMPACT-MBC). Study protocol. ClinicalTrials.gov Identifier: NCT01957332. Available from https://clinicaltrials.gov/ct2/show/record/NCT01957332, accessed on 13 July 2016.
24. Ulaner GA, Hyman DM, Ross DS, Corben A, Chandarlapaty S, Goldfarb S, McArthur H, Erinjeri JP, Solomon SB, Kolb H, Lyashchenko SK, Lewis JS, Carrasquillo JA. Detection of HER2-positive metastases in patients with HER2-negative primary breast cancer using 89Zr-trastuzumab PET/CT. J Nucl Med. 2016; 57:1523–1528.
25. Lord SJ, Marinovich ML, Patterson JA, Wilcken N, Kiely BE, Gebski V, Crossing S, Roder DM, Gattellari M, Houssami N. Incidence of metastatic breast cancer in an Australian population-based cohort of women with non-metastatic breast cancer at diagnosis. Med J Aust. 2012; 196:688–692. https://doi.org/10.5694/mja12.10026.
26. Mauri D, Pavlidis N, Pozylos NP, Ioannidis JP. Survival with aromatase inhibitors and inactivators versus standard hormonal therapy in advanced breast cancer: meta-analysis. J Natl Cancer Inst. 2006; 98:1285–91. https://doi.org/10.1093/jnci/djj357.
27. Andersson M, Lidbrink E, Bjerre K, Wist E, Enevoldsen K, Jensen AB, Karlsson P, Tange UB, Sørensen PG, Møller S, Bergh J, Langkjer ST. Phase III randomized study comparing docetaxel plus trastuzumab with vinorelbine plus trastuzumab as first-line therapy of metastatic or locally advanced human epidermal growth factor receptor 2-positive breast cancer: The HERNATA Study. J Clin Oncol. 2011; 29:264–71. https://doi.org/10.1200/JCO.2010.30.8213.
28. Baselga J, Manikhas A, Cortés J, Llombart A, Roman L, Semiglazov VF, Byakhov M, Lokanatha D, Forenza S, Goldfarb RH, Matera J, Azarnia N, Hudis CA, et al. Phase III trial of nonpegylated liposomal doxorubicin in combination with trastuzumab and paclitaxel in HER2-positive metastatic breast cancer. Ann Oncol. 2014; 25:592–8. https://doi.org/10.1093/annonc/mdt543.
29. Robert N, Leyland-Jones B, Asmar L, Belt R, Ilegbodu D, Loesch D, Raju R, Valentine E, Sayre R, Cobleigh M, Albain K, McCullough C, Fuchs L, et al. Randomized phase III study of trastuzumab, paclitaxel, and carboplatin compared with trastuzumab and paclitaxel in women with HER-2-overexpressing metastatic breast cancer. J Clin Oncol. 2006; 24:2786–92. https://doi.org/10.1200/JCO.2005.04.1764.
30. Valero V, Forbes J, Pegram MD, Pienkowski T, Eiermann W, von Minckwitz G, Roche H, Martin M, Crown J, Mackey JR, Fumoleau P, Rolski J, Mrsic-Krmpotic Z, et al. Multicenter phase III randomized trial comparing docetaxel and trastuzumab with docetaxel, carboplatin, and trastuzumab as first-line chemotherapy for patients with HER2-gene-amplified metastatic breast cancer (BCIRG 007 Study): two highly active therapeutic regimens. J Clin Oncol. 2011; 29:149–56. https://doi.org/10.1200/JCO.2010.28.6450.
31. NZA. Available at http://www.nza.nl, 2016.
32. Excellence NIfHaC. Advanced breast cancer: diagnosis and treatment, Clinical guideline (CG81), Available from: https://www.nice.org.uk/guidance/cg81. 2014.
33. Excellence NIfHaC. Guidance on the use of trastuzumab for the treatment of advanced breast cancer (TA34), Available from: https://www.nice.org.uk/guidance/ta34, 2002.
34. Excellence NIfHaC. Lapatinib or trastuzumab in combination with an aromatase inhibitor for the first-line treatment of metastatic hormone-receptor-positive breast cancer that overexpresses HER2 (TA257), Available from: https://www.nice.org.uk/guidance/ta257. 2012.
35. Excellence NIfHaC. Docetaxel for the adjuvant treatment of early node-positive breast cancer (TA 109), Available from: https://www.nice.org.uk/guidance/ta109, 2006.
36. Excellence NIfHaC. Hormonal therapies for the adjuvant treatment of early oestrogen-receptor-positive breast cancer (TA112), Available from: https://www.nice.org.uk/guidance/ta112, 2006.
37. British National Formularly, available from https://www.medicinescomplete.com/mc, 2016.
38. Exchange rate, available from https://www.ecb.europa.eu/stats/policy_and_exchange_rates/euro_reference_exchange_rates/html/eurofxref-graph-gbp.en.html.
39. World data bank, available from http://data.worldbank.org.
40. Dutch Council for Public Health and Health Care 2006, available from https://www.raadrvs.nl/en.
41. Care Institute – The Netherlands (ZIN), available at https://www.zorginstituutnederland.nl/.