
INTRODUCTION
Prostate cancer (Pca) is the most frequent malignancy and the second leading cause of cancer-related death for males in the United States. Historically, the incidence of prostate cancer in China was lower than in America, however current data indicates that the occurrence of Pca is increasing [1]. A prostate-specific antigen (PSA) blood test is used to screen for Pca and the condition is then diagnosed with a prostate biopsy. Although PSA is considered the most powerful biomarker for the detection and risk classification of prostate cancer, it has noteworthy limitations [2]. In Pca patients with Gleason grade 8 – 10 disease, a proportion of tumor cells are so poorly differentiated that they produce relatively little PSA [3, 4]. Therefore, more precise indicators of disease severity are critical for optimizing the treatment of Pca patients [2] and may offer predictive and prognostic clinical information [5, 6].
In our present study, we found that Aminopeptidase P2 (XPNPEP2) was highly expressed in prostate tissues. XPNPEP2 is an aminoacylproline hydrolase that specifically removes the N-terminal amino acid from peptides with a penultimate prolyl residue. A large number of biologically active polypeptides, including hormones, growth factors, neurotransmitters, coagulating proteins, toxins, and cytokines, are potential substrates of XPNPEP2 [7]. Importantly, XPNPEP2 acts synergistically with kallikrein during bradykinin production [8]. PSA, i.e., human kallikrein 3 (hK3), is also a serine protease in the kallikrein family of proteases [9] and is able to produce kinins via its kininogenase activity. Both a variant XPNPEP2 and an abnormality in the kallikrein-kinin system are associated with bradykinin-mediated angioedema [10]. A correlation between polymorphisms and haplotype mutations of XPNPEP2 and ACEI-induced angioedema has been reported [11].
However, there is little information regarding the physiological roles and clinical significance of XPNPEP2 in prostate diseases. In this study, we investigated the expression of XPNPEP2 in normal and cancerous prostate tissue. Meanwhile, the serum levels of XPNPEP2 in Pca patients were measured to evaluate the association between serum XPNPEP2 levels and patient clinical and pathologic characteristics, including the PSA value, pathologic Gleason score, extracapsular extension, seminal vesicle invasion, and lymph node metastasis.
RESULTS
Clinical characteristics
In the present study, we collected samples from 128 prostate cancer patients with localized Pca or with local invasion and LN metastasis. two Pca patients lacked complete lymph node dissections. The median age of the Pca patients was 67 years (ranging from 51-82 years). In the BPH group, the median age was 72 years. Clinical details were listed in Table 1.
Table 1: Relationship between serum protein levels (XPNPEP2 and PSA) and clinicopathological variables
|
No(%) |
XPNPEP2(ng/mL) |
P Value |
PSA(ng/mL) |
P Value |
|---|---|---|---|---|---|
Age, yr |
|
|
|
|
|
≤65 |
42(32.5) |
87.06±13.85 |
|
47.34±9.08 |
|
>65 |
86(67.5) |
71.88±10.23 |
P=0.58 |
242.5±36.10 |
P<0.01* |
Biopsy Gleason Score |
|
|
|
|
|
≤7 |
53(42) |
78.54±13.48 |
|
125.3±39.07 |
|
>7 |
73(58) |
62.10±8.55 |
P=0.49 |
176.9±48.86 |
P=0.53 |
lymph node metastasis |
|
|
|
|
|
No |
87(70) |
61.63±5.50 |
|
78.12±14.59 |
|
Yes |
39(30) |
142.7±14.40 |
P<0.01 |
250.8±55.08 |
P<0.01 |
Local invasion |
|
|
|
|
|
No |
62(49) |
77.58±9.80 |
|
71.62±19.90 |
|
Yes |
64(51) |
95.91±9.70 |
P=0.19 |
198.0±36.74 |
P<0.01 |
Expression of XPNPEP2 in normal tissues
In this study, the expression of XPNPEP2 in all organs was detected by IHC using the normal tissue microarray (MC5003a), which includes kidney, lung, liver, colon, testis, breast prostate and other organs. We demonstrated that XPNPEP2 was preferentially expressed in the renal proximal tubule. Importantly, we observed that the glandular cells in the prostate had moderately high levels of XPNPEP2 protein. The pancreatic islet cells, brush border membranes of intestinal epithelial cells and liver cells were weakly positive, and tissues of the cervix, ovary, breast and lung were negative. Representative immunohistochemically stained sections were shown in Supplementary Figure 1.
Expression of XPNPEP2 in Pca patients
For primary evaluation of XPNPEP2 in Pca patients, a prostate cancer tissue microarray and 30 BPH tissue samples collected at Tongji hospital were used. XPNPEP2 expression was lower in prostate samples from Pca patients including localized and lymph node metastasis than in samples from normal or BPH patients. (Figure 1A and 1B)
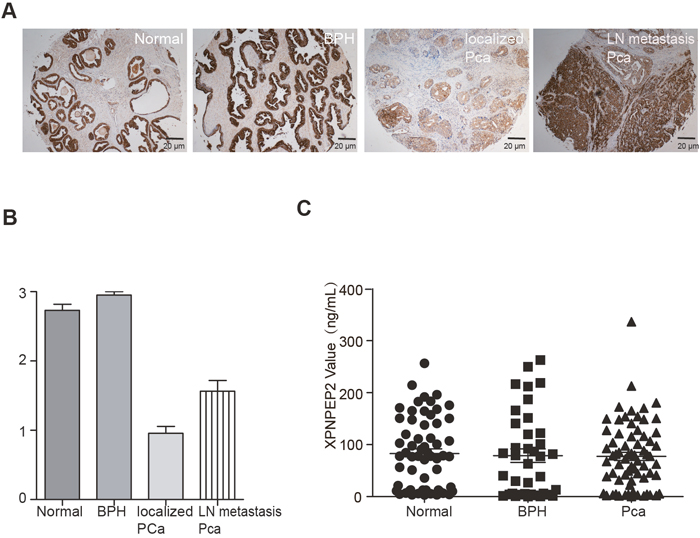
Figure 1: The profile of XPNPEP2 protein levels in tissues and serum from normal, BPH and Pca patients. A prostate cancer tissue microarray and 30 BPH tissues were used for detecting XPNPEP2 expression. A representative figure was shown in panel (A) and the statistical analysis was presented in (B). The serum levels of XPNPEP2 were not significantly different among normal, BPH and Pca patients (C).
XPNPEP2 expression in patients with localized, locally invasive and LN-metastatic Pca
Comparing XPNPEP2 expression, we found it to be higher in locally invasive and LN-metastatic Pca than in localized Pca (p<0.01) (Figure 2A and 2B). A schematic diagram of immunoreactivity scoring (IRS) was presented in Figure 2A. In the meantime, we also observed that XPNPEP2 expression in occult metastases was higher than in large foci (Figure 2B).
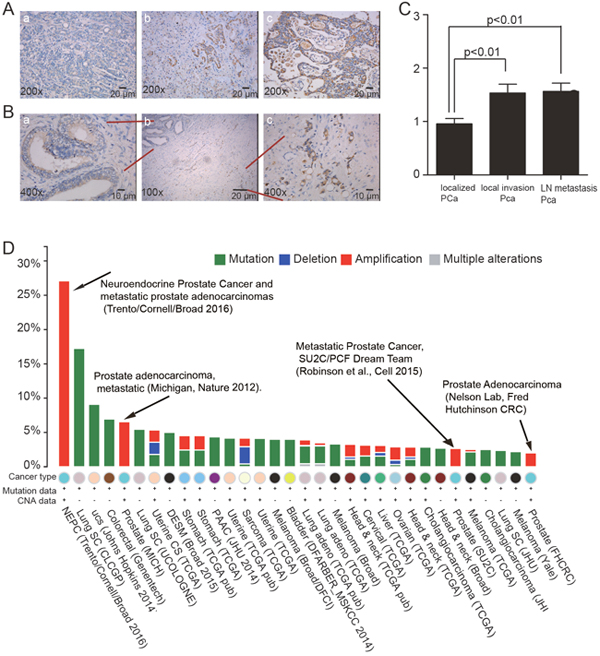
Figure 2: Comparison of XPNPEP2 expression among localized, locally invasive and LN-metastatic Pca. The schematic diagram of immunoreactivity scoring (IRS) was presented in (A), and the statistical analysis shown in (C). In the same FFPE section, the XPNPEP2 expression in the occult metastases was significantly higher than that in large foci (B). XPNPEP2 gene mutations using data extracted from the cBioPortal online analysis tool (the cBioPortal for Cancer Genomics). The cross-cancer XPNPEP2 mutation analysis showed that metastatic prostate cancer had the highest frequency of XPNPEP2 gene amplification (D).
To confirm that XPNPEP2 plays a role in human prostate cancer, we analyzed XPNPEP2 gene alterations using data extracted from the cBioPortal online tool (the cBioPortal for Cancer Genomics)[12, 13]. Cross-cancer XPNPEP2 alteration analysis demonstrated that XPNPEP2 is frequently altered in different types of cancers (Figure 2D). Interestingly, among the 36 examined cancer types or subtypes, prostate cancer had the highest frequency of XPNPEP2 gene amplifications. Moreover, all studies of Pca patients were associated with metastatic prostate cancer.
Serum XPNPEP2 protein levels in Pca patients
In contrast to its expression in tissues from Pca patients, serum XPNPEP2 levels were not significantly different when comparing Pca patients (77.35 ± 7.72 ng/mL), to normal (85.82 ± 8.16 ng/mL) and BPH patients (76.94 ±12.86 ng/mL) (Figure 1C). For further analysis, we compared Pca subtypes and found that the serum XPNPEP2 levels in patients with locally invasive Pca (95.91±9.70 ng/mL) were higher than the levels in Pca patients without local invasion (77.58±9.80 ng/mL) (P =0.19) (Figure 3C). Serum XPNPEP2 levels in Pca patients with LN metastasis (198.0±36.74 ng/mL) were also significantly higher than levels in Pca patients without LN metastasis (71.62±19.90 ng/mL) (P <0.01) (Figure 3D). The corresponding serum PSA levels of Pca patients were analyzed and also found to be associated with LN metastasis (Figure 3B). We also observed a few Pca patients with outlier levels of PSA. When these outliers were excluded, the serum PSA levels from patients with local invasion were still significantly higher than levels in patients without local invasion (Figure 4A), but serum PSA levels did not correlate with LN metastasis (Figure 4B). However, when the PSA outliers were excluded, the serum XPNPEP2 levels in Pca patients with LN metastasis were higher than levels in Pca patients without LN metastasis (Figure 4C and 4D).
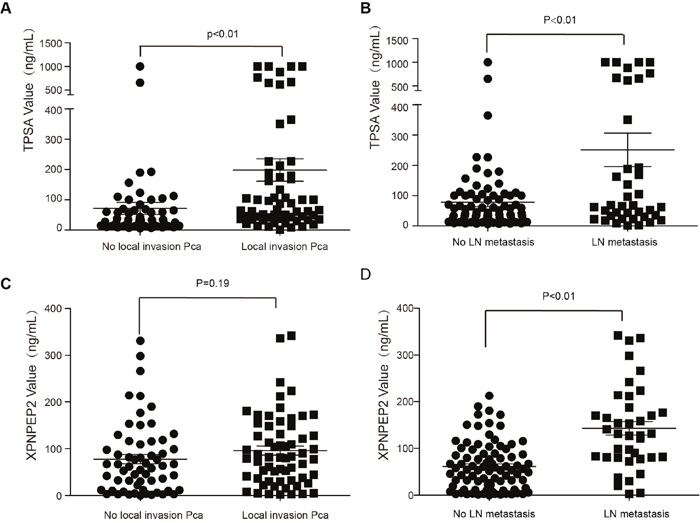
Figure 3: Serum levels of XPNPEP2 and corresponding serum levels of PSA in Pca patients with different clincopathologies. PSA levels (A) were significantly higher than in Pca patients with local invasion than without local invasion (p<0.01), But serum XPNPEP2 levels was not (C). Serum XPNPEP2 levels (D) and PSA levels (B) were significantly different in Pca patients with LN metastasis and Pca patients without LN metastasis.
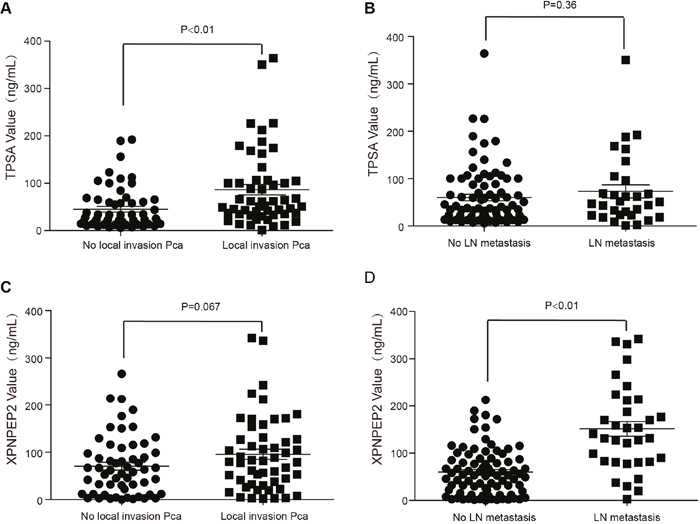
Figure 4: XPNPEP2 and the corresponding PSA serum levels in Pca patient with different clinicopathologies. When PSA outliers were excluded, the serum PSA levels in patients with local invasion were higher than levels in patients without local invasion (A) (p<0.01). However, serum PSA levels were not associated with LN metastasis (B). Serum XPNPEP2 levels of Pca patients with LN metastasis were obviously higher than levels of Pca patients without LN metastasis (D) (p<0.01), but showed no significant difference when compared to levels from Pca patients with local invasion (C).
ROC analysis of XPNPEP2 and PSA levels in Pca patients with LN metastasis
To validate the potential usefulness of serum XPNPEP2 as a noninvasive biomarker for predicting the risk of lymph node involvement in Pca patients, an ROC curve analysis was performed using serumXPNPEP2 levels alone or in combination with PSA. a comparison was made between Pca with LN metastasis and Pca without metastasis yielding AUC value of 0.620, 0.795 and 0.845 for XPNPEP2, PSA and their combination, respectively (Figure 5A). Therefore, combined application of serumXPNPEP2 levels and PSA levels might improve diagnostic accuracy for Pca with LN metastasis.
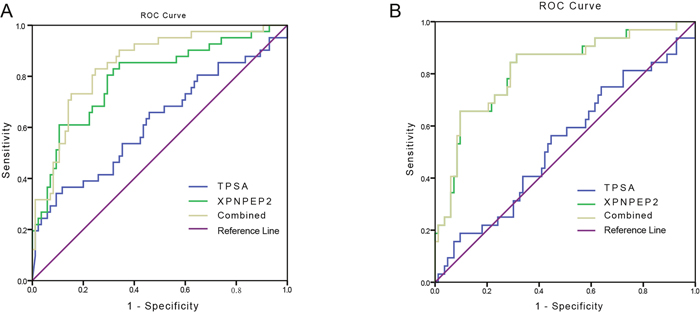
Figure 5: ROC curve tests of serum XPNPEP2 and PSA. ROC curves of XPNPEP2, PSA and both for patients with LN metastasis versus patients without (A). Outliers of PSA were excluded and ROC curves were generated for XPNPEP2, PSA and both for all patients with LN metastasis versus patients without (B).
When the PSA outliers were excluded from the Pca patients with lymph node metastasis, the AUC for serum XPNPEP2 was 0.818, while the AUC for PSA decreased to 0.529 (Figure 5B).
Correlation analysis
To explore whether there is an association between serum XPNPEP2 levels and PSA levels in Pca patients, a correlation analysis was performed demonstrating that serum XPNPEP2 levels were independent of serum PSA levels (Figure 6A). The protein expression in Pca tissue as detected by IHC also revealed no relationship between PSA and XPNPEP2. As shown in Figure 6B, patient 1 had strong PSA but weak XPNPEP2 expression, but patient 2 had weak and focal PSA but strong XPNPEP2 expression.
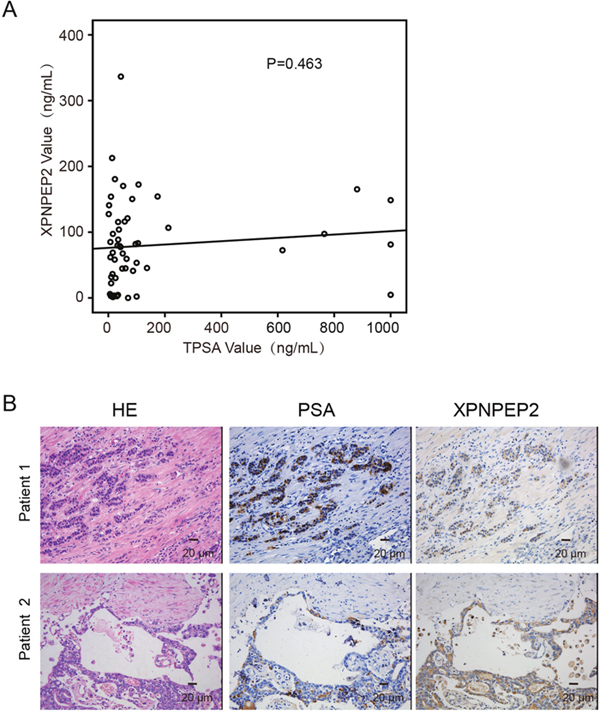
Figure 6: The correlation between PSA and XPNPEP2. A correlation analysis between serum XPNPEP2 and PSA levels was performed (A). Expression of XPNPEP2 in Pca tissues did not accord with the PSA expression (B).
DISCUSSION
Aminopeptidase P (APP or XPNPEP2) is an aminoacylproline hydrolase widely distributed in prokaryotes and eukaryotes that specifically removes the N-terminal amino acid from peptides with a penultimate prolyl residue [7]. Several studies have demonstrated the correlation between polymorphisms and haplotype mutations of XPNPEP2 and ACEI-induced angioedema. There are fewer studies investigating the role of XPNPEP2 in cancer [11, 14].
We confirmed that the expression of XPNPEP2 was significantly lower in prostate cancer tissues than normal prostate tissues. However, there was a discrepancy between the plasma and tissue levels of XPNPEP2 in Pca patients. Our study demonstrated that Serum XPNPEP2 levels correlate with lymph node metastasis in Pca patients. In addition, we analyzed XPNPEP2 gene alterations using data extracted from the cBioPortal online analysis tool and found that metastatic prostate cancer has the highest frequency of XPNPEP2 gene amplification [12, 13]. Using a gene prioritization method (GP-MIDAS-VXEF) to compare prostate cancer and lymph node metastasis, Carlos Roberto Arias et al. demonstrated that XPNPEP2 is a metastatic gene candidate [15]. Cheng et al. showed XPNPEP2 facilitated cervical cancer cell invasion and migration by inducing epithelial–mesenchymal transition [16]. Bioinformatic methods also verified that serum XPNPEP2 could be a potential biomarker for lymph node metastasis.
Lymph node metastasis is a powerful prognostic factor in guiding clinical decision-making in terms of surgery, follow-up scheduling and adjuvant therapies. Several previous studies created a nomogram to predict the risk of lymph node involvement (LNI)[17–19]. The three-variable nomogram includes basic grade clinical variables (pretreatment PSA, clinical stage, and biopsy Gleason grade). In this study, we also verified that PSA levels correlated with Pca aggressiveness and tumor volume. However, approximately 5 – 10% of prostatic adenocarcinomas produce little PSA, and some patients with low PSA levels have higher rates of adverse pathologic features [3]. Especially for patients with low PSA levels, the XPNPEP2 test may be useful for predicting lymph node metastasis when combined with the PSA test. The expression of PSA is mainly induced by androgens. And Christian Drouet et al. revealed that Patients with HAE receiving androgen prophylaxis showed a significantly higher plasma APP activity. Androgen can regulate the PSA expression and XPNPEP2 activity, but mechanisms are different, PSA expression was mainly regulated by the androgen receptor (AR) at the transcriptional level. The author hypothesized that the effect that androgens have on the circulating APP activity results from a potentiating effect on a glycosylphosphatidyli-nositol hydrolase activity. This includes metalloprotease and phospholipase mechanisms, with subsequent release of glycosylphosphatidylinositol–anchored proteins, which are responsible for the shedding of APP from the endothelial membrane. May be that is why BPH tissues have higher XPNPEP2 expression than PCa tissues which are not advanced [20].
The major limitation of this study is the relatively small serum sample pool from Pca patients with lymph node metastasis. We believe that larger studies are required to confirm our findings. In addition, this was a single institution study, and a large scale multicenter and multiracial study will be needed to evaluate the value of XPNPEP2 as a lymph node metastatic biomarker for Pca.
In summary, we demonstrated that serum XPNPEP2 levels were associated with lymph node metastasis and local invasion. Combining PSA and XPNPEP2 can increase the efficiency of predicting LN metastasis compared to the efficiency of using PSA or XPNPEP2 alone. Especially for Pca patients with low serum PSA levels, XPNPEP2 was a powerful marker for predicting LN metastasis.
MATERIALS AND METHODS
Serum collection
Between December 2014 and March 2017, 128 serum samples from prostate cancer patients, 70 samples from healthy males and 40 samples from patients with prostate hyperplasia were obtained from the clinical laboratory of Tongji hospital (Wuhan, China). All serum samples were collected prior to radical prostatectomy and chemotherapy. Patient clinical data were recorded, including their age, Gleason score, histopathological findings, PSA levels, positive lymph nodes and medication history. Ethical approval was obtained from the ethical management committees of Tongji hospital. All participants provided written informed consent before being sampled for our study.
Tissue microarrays and prostate cancer tissue
High-density multiple organ tumor tissue array(MC5003a, US Biomax, Inc.) was used for the initial screen of XPNPEP2 expression. This 500 core tissue microarray includes the 20- most common types of cancer (25 cases/type) and normal controls (5 cases/type) with TNM classifications and pathological grades of the tumors. Based on this initial screen, XPNPEP2 expression was further analyzed in individual organs using the prostate cancer tissue microarray PR1921 which contains adjacent normal prostate tissues and normal tissues as controls. This array includes the TNM, clinical stage and pathological grades and the level of IHC markers (PSA) from 96 cases arrayed in duplicate to yield 192 cores. To analyze XPNPEP2 expression associated with invasion and metastasis, 90 formalin-fixed paraffin-embedded (FFPE) prostate cancer tissue samples, including 30 from patients with localized Pca, 30 from patients with local invasion, and 30 from patients with lymph node metastasis, and corresponding adjacent normal prostate tissues were collected from the pathology department of Tongji hospital (Wuhan, China). The pathologic features were determined by urological pathologists using standardized protocols. The characteristics of all study subjects were summarized in Table 1.
XPNPEP2 expression by immunohistochemistry
The above tissue microarrays and prostate cancer tissue samples were subjected to immunohistochemistry with rabbit anti-XPNPEP2 (1:250, GTX109995, GeneTex, USA) and anti-PSA antibodies (1:250, ab76113, Abcam, USA). Briefly, FFPE sections were deparaffinized in xylene and then rehydrated with descending concentrations of alcohol. Antigen retrieval was performed by microwave heating in citric acid buffer (pH 6.0) for 12 min at 100°C followed by cooling at room temperature. Endogenous peroxidase was blocked by 3% hydrogen peroxide for 30 min at 37°C. Then, the samples were incubated with a primary antibody overnight at 4°C. The immunohistocemistry procedure was continued using the standard protocol from a goat anti-rabbit IHC kit (SP-9001; ZSGB-BIO). Chromogen was developed with a DAB chromogenic substrate kit (GoodBio, Wuhan). Then, sections were counterstained with hematoxylin. Immunostaining was evaluated and a blind score assigned by two experienced pathologists with no prior knowledge of the pathological parameters. The immunoreactivity scoring (IRS) system was based on the staining intensity on a scale of 0 to 3 (0 = negative; 1 = weakly positive; 2 = moderately positive; 3 = strongly positive).
ELISA
Serum levels of XPNPEP2 were measured by using a human XPNPEP2 ELISA pair set (cat: SEK11903, Sino Biological, Beijing). The ELISA assay was performed as follows. A 96-well microplate was coated with 100μL monoclonal antibody specific for XPNPEP2 (2 μg/mL) overnight at 4°C. The wells were then washed three times and blocked, and 100μL of standards or samples (diluted 1:200) were added to individual wells. Each well was aspirated and washed three times with at least 300μl of buffer per wash. Subsequently, 100μL of HRP-conjugated anti-XPNPEP2 monoclonal antibody (0.5μg/mL) was added. The aspiration and wash cycle was repeated, and then 100μL of TMB substrate solution was loaded. 50μL of stop solution was added and the absorbance of each well at 450 nm was measured. XPNPEP2 concentrations were calculated based on the curve generated from the standards.
Statistical analysis
Between-group differences for continuous variables with a normal distribution were tested with Student’s t test. The Mann-Whitney U test was employed to compare continuous variables that did not have a normal distribution. Receiver operating characteristic (ROC) curves were constructed to determine the diagnostic performance of serum XPNPEP2 levels and PSA levels in distinguishing prostate cancer patients with localized invasion or lymph node metastasis from patients with low-grade prostate cancer. The area under the ROC curve (AUC) was used to assess the predictive power. Analyses were performed using Prism 5 software (GraphPad) and SPSS 13.0. Two-sided P values of < 0.05 were considered statistically significant.
Abbreviations
Pca: prostate cancer; XPNPEP2: aminopeptidase P2; PSA: prostate-specific antigen; BPH: benign prostate hyperplasia; ROC: receiver operating characteristic; AUC: area under the curve; FFPE: Formalin-fixed paraffin-embedded; LN: lymph nodes; IHC: immunohistochemistry; ELISA: enzyme-linked immunosorbent assay; TCGA: the cancer genome atlas
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING
This work was supported by the National Natural Science Foundation of China (81172468; 81302249; 81202061, 86271600). Fei Li and Mengqin Lv contributed equally to this manuscript.
REFERENCES
1. Yang X, Monn MF, Liu L, Liu Y, Su J, Lyu T, Gong Y, Wang L, Davidson DD, Cheng L. Incidental prostate cancer in Asian men: high prevalence of incidental prostatic adenocarcinoma in Chinese patients undergoing radical cystoprostatectomy for treatment of bladder cancer and selection of candidates for prostate-sparing cystectomy. Prostate. 2015; 75:845-854.
2. Morlacco A, Karnes RJ. High-risk prostate cancer: the role of surgical management. Crit Rev Oncol Hematol. 2016; 102:135-143.
3. McGuire BB, Helfand BT, Loeb S, Hu Q, O’Brien D, Cooper P, Yang X, Catalona WJ. Outcomes in patients with Gleason score 8-10 prostate cancer: relation to preoperative PSA level. BJU Int. 2012; 109:1764-1769.
4. Izumi K, Ikeda H, Maolake A, Machioka K, Nohara T, Narimoto K, Ueno S, Kadono Y, Kitagawa Y, Konaka H, Mizokami A, Namiki M. The relationship between prostate-specific antigen and TNM classification or Gleason score in prostate cancer patients with low prostate-specific antigen levels. Prostate. 2015; 75:1034-1042.
5. Leapman MS, Nguyen HG, Cooperberg MR. Clinical utility of biomarkers in localized prostate cancer. Curr Oncol Rep. 2016; 18:30.
6. Izumi K, Mizokami A, Lin HP, Ho HM, Iwamoto H, Maolake A, Natsagdorj A, Kitagawa Y, Kadono Y, Miyamoto H, Huang CK, Namiki M, Lin WJ. Serum chemokine (CC motif) ligand 2 level as a diagnostic, predictive, and prognostic biomarker for prostate cancer. Oncotarget. 2016; 7:8389-8398. https://doi.org/10.18632/oncotarget.6690.
7. Ersahin C, Szpaderska AM, Orawski AT, Simmons WH. Aminopeptidase P isozyme expression in human tissues and peripheral blood mononuclear cell fractions. Arch Biochem Biophys. 2005; 435:303-310.
8. Craig TJ, Bernstein JA, Farkas H, Bouillet L, Boccon-Gibod I. Diagnosis and treatment of bradykinin-mediated angioedema: outcomes from an angioedema expert consensus meeting. Int Arch Allergy Immunol. 2014; 165:119-127.
9. Bryant RJ, Sjoberg DD, Vickers AJ, Robinson MC, Kumar R, Marsden L, Davis M, Scardino PT, Donovan J, Neal DE, Lilja H, Hamdy FC. Predicting high-grade cancer at ten-core prostate biopsy using four kallikrein markers measured in blood in the ProtecT study. J Natl Cancer Inst. 2015; 107:djv095.
10. Defendi F, Charignon D, Ghannam A, Ponard D, Drouet C. [Biological investigation of kinin-mediated angioedema]. [Article in French]. Ann Dermatol Venereol. 2015; 142:163-169.
11. Cilia La Corte AL, Carter AM, Rice GI, Duan QL, Rouleau GA, Adam A, Grant PJ, Hooper NM. A functional XPNPEP2 promoter haplotype leads to reduced plasma aminopeptidase P and increased risk of ACE inhibitor-induced angioedema. Hum Mutat. 2011; 32:1326-1331.
12. Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, Jacobsen A, Byrne CJ, Heuer ML, Larsson E, Antipin Y, Reva B, Goldberg AP, et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012; 2:401-404.
13. Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, Sun Y, Jacobsen A, Sinha R, Larsson E, Cerami E, Sander C, Schultz N. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci Signal. 2013; 6:pl1.
14. Duan QL, Nikpoor B, Dube MP, Molinaro G, Meijer IA, Dion P, Rochefort D, Saint-Onge J, Flury L, Brown NJ, Gainer JV, Rouleau JL, Agostoni A, et al. A variant in XPNPEP2 is associated with angioedema induced by angiotensin I-converting enzyme inhibitors. Am J Hum Genet. 2005; 77:617-626.
15. Arias CR, Yeh HY, Soo VW. Biomarker identification for prostate cancer and lymph node metastasis from microarray data and protein interaction network using gene prioritization method. ScientificWorldJournal. 2012; 2012:842727.
16. Cheng T, Wei R, Jiang G, Zhou Y, Lv M, Dai Y, Yuan Y, Luo D, Ma D, Li F, Xi L. XPNPEP2 is overexpressed in cervical cancer and promotes cervical cancer metastasis. Tumour Biol. 2017; 39:1010428317717122.
17. Godoy G, Chong KT, Cronin A, Vickers A, Laudone V, Touijer K, Guillonneau B, Eastham JA, Scardino PT, Coleman JA. Extent of pelvic lymph node dissection and the impact of standard template dissection on nomogram prediction of lymph node involvement. Eur Urol. 2011; 60:195-201.
18. Abdollah F, Karnes RJ, Suardi N, Cozzarini C, Gandaglia G, Fossati N, Bianchi M, Boorjian SA, Sun M, Karakiewicz PI, Montorsi F, Briganti A. Predicting survival of patients with node-positive prostate cancer following multimodal treatment. Eur Urol. 2014; 65:554-562.
19. Kluth LA, Abdollah F, Xylinas E, Rieken M, Fajkovic H, Seitz C, Sun M, Karakiewicz PI, Schramek P, Herman MP, Becker A, Hansen J, Ehdaie B, et al. Clinical nodal staging scores for prostate cancer: a proposal for preoperative risk assessment. Br J Cancer. 2014; 111:213-219.
20. Drouet C, Desormeaux A, Robillard J, Ponard D, Bouillet L, Martin L, Kanny G, Moneret-Vautrin DA, Bosson JL, Quesada JL, Lopez-Trascasa M, Adam A. Metallopeptidase activities in hereditary angioedema: effect of androgen prophylaxis on plasma aminopeptidase P. J Allergy Clin Immunol. 2008; 121:429-433.