
INTRODUCTION
Coffee is among the most consumed beverages worldwide: in Europe, the geographic area showing the highest coffee consumer in the world, people are reported to drink 725 million cups of coffee every day [1]. In light of its wide consumption, it is an important public health goal to assess whether coffee has protective or detrimental effects against cancer risk.
Current evidence from epidemiological and experimental studies suggests that coffee consumption may exert beneficial effects towards non-communicable diseases [2]. In particular, coffee consumption has been associated with decreased risk of cardio-metabolic conditions, including metabolic syndrome [3], diabetes [4] and cardiovascular disease [5]. Research on cancer risk showed more controversial findings: a summary of evidence reported that coffee could have a protective role against the development of various cancers, including liver, colorectal, endometrial, oral, melanoma, and prostate cancer among others [6–12]. However, other revision of existing literature reported contrasting results [13, 14]: this conclusion was based on a dose-response meta-analysis of 10 cohort studies, and the relative risk (RR) for an increment of 1 cup/day appeared to be not significantly associated with risk of overall cancers [15]. Numerous confounders and effect modifiers can have a role in assessing the relationship between coffee consumption and health outcomes: for instance, recent meta-analyses on coffee consumption and various health outcomes pointed out that the ambiguous results on cancer mortality and hypertension were due to the modifying effect of smoking [16, 17].
Ovarian cancer has a major epidemiological and social burden for women worldwide: in 2012, women with a diagnosis of ovarian cancer occurred in the last 5 years were over 587,000 and 157,000 worldwide and in Europe, respectively [18, 19]. In 2013, deaths accounted for ovarian cancer were about 158,000 worldwide, together with over 4 million disability adjusted life years (DALYs); such figure significantly increased from 1990 (2.7 million DALYs) and poses ovarian cancer as the worldwide 12th contributor of death and disability among cancers [20].
The evidence on the association between coffee drinking and the risk of ovarian cancer is quite limited and inconsistent. Results of a meta-analysis of prospective cohort studies revealed a non-significant positive association between coffee drinking and risk of ovarian cancer [21]. However, more recent data has been published and comprehensive summary of evidence is lacking. Thus, the aim of this study is to update current evidence on the association between dietary coffee consumption and risk of ovarian cancer testing also the dose-response relation.
METHODS
We performed a meta-analysis of prospective cohort studies following Meta-Analysis of Observational Studies in Epidemiology (MOOSE) protocols throughout design, execution, analysis and reporting stages (Supplementary Table 1).
Search strategy
To collect and critically review the evidence, we performed a comprehensive literature search in PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) and EMBASE (http://www.embase.com/) databases, from the earliest available online indexing year to March 2017. The search was limited to studies published in English. Search terms included the following: (coffee OR caffeine OR beverages) AND (ovarian) AND (cancer OR carcinoma OR neoplasm) (Supplementary Table 2). Titles and abstracts of all identified studies were screened by two members of the team. Studies were eligible for inclusion in the meta-analysis if they met the following inclusion criteria: 1) the study had a prospective design; 2) the exposure of interest was coffee consumption; 3) the outcome was ovarian cancer incidence; 4) the investigators reported relative risks with 95% confidence intervals for 3 or more quantitative categories of coffee consumption. When discrepancies over inclusion arose, inclusion criteria were assessed to reach a consensus. Reference lists of included manuscripts were also screened for any additional study not previously identified. When duplicate reports on the same cohort were identified, we included the one that provided the largest number of cases (or entire cohort) or with the longest follow-up for each endpoint of interest.
Data extraction
Data were abstracted from all identified studies using a standardized extraction form. Information was extracted from each study and consisted of: 1) first author name; 2) year of publication; 3) study cohort name; 4) country; 5) number of participants; 6) gender of participants; 7) age range of the study population at baseline; 8) categories of consumption; 9) coffee type; 10) follow-up period; 11) endpoints and cases; 12) distributions of cases and person-years, HRs, and 95% CIs for all categories of exposure; 13) covariates used in adjustments. Extraction of data was performed independently by two authors. Discrepancies were discussed and resolved by consensus. The quality of included studies was assessed according to the Newcastle-Ottawa Quality Assessment Scale [22].
Statistical analysis
Highest versus lowest and dose-response meta-analyses were performed to determine the relationship between coffee intake and ovarian cancer risk. The most fully adjusted RRs/HRs with 95% CI for all categories of exposure were extracted. Random-effects models were used to calculate pooled effects, wherein HRs were deemed as equivalent to relative risks (RRs) [23]. Heterogeneity was assessed through the I2 statistic, which estimates the fraction of variance that is due to heterogeneity and by Q test. The level of significance for the Q test was defined as P < 0.10. The values of I2 statistic ≤25%, 25–50%, 50–75%, and >75% indicated no, small, moderate, and significant heterogeneity, respectively. The stability of the results and potential sources of heterogeneity were examined in a sensitivity analysis excluding one study at a time and in subgroup analysis according to menopausal status and geographical area. Included studies did not provide datasets of stratified analysis to test for potential confounders/effect modifiers, such as smoking or BMI. Therefore, subgroup analyses were only performed according to adjustment for smoking status, BMI, education level and alcohol consumption. Publication bias was evaluated by a visual investigation of funnel plots for potential asymmetry.
To examine linear and non-linear relationship between coffee intake and risk of ovarian cancer, random-effects dose-response meta-analysis was used. We extracted data on the amount of coffee intake, distributions of cases and person-years (when available), and RRs/HRs with 95% CIs for ≥3 exposure categories. In each study across categories of consumption, the mean or median intake of coffee was assigned to the corresponding RR/HR with the 95% CI. When originally in article the range of coffee intake was reported , the midpoint of the range was selected . When the highest category was open ended, we assumed the width of the category to be the same as the adjacent category. When the lowest category was open ended, we set the lower boundary to zero. Random-effects dose-response meta-analysis was performed in two-stages. In the first stage the method reported by Greenland and Orsini (that is, GLS) was used to calculate study-specific slopes (generalized least-squares, GLS) on the basis of results across categories of coffee intake taking into account the correlation within each set of retrieved HRs [24, 25]. Model of restricted cubic splines with 3 knots at fixed percentiles (25%, 50%, and 75%) of the distribution was applied in non-linear dose-response. [26]. We combined the coefficients that had been calculated within each study by performing random-effects meta-analysis with DerSimonian and Laird estimator of between study variance (in linear dose-response meta-analysis) or estimator received by using the method of moments (in non-linear dose-response meta-analysis). We calculated an overall P-value by testing that the 2 regression coefficients were simultaneously equal to zero. We then calculated a P-value for non-linearity by testing that the coefficient of the second spline was equal to zero. All analyses were performed with R software version 3.0.3 and we mainly used dosresmeta package (Development Core Team, Vienna, Austria).
RESULTS
Study characteristics
We identified a total of 1,340 studies, of which 1,223 were excluded after review of title, and 104 on the basis of abstract (Figure 1). Of the remained thirteen publications, four were not included for the following reasons: 1) the article did not provide relative risks (or similar risk measures) and corresponding confidence intervals; 2) the study provided less than three exposures of coffee consumption; 3) the article reported on gene polymorphism. For the analysis on the association between coffee consumption and ovarian cancer risk, nine studies were eligible [13, 27–34], of which one was a multi-center study [27]. Studies included in the analysis comprised 787,076 participants and 3,541 ovarian cancer cases. Five studies were conducted in Europe [27, 28, 30, 31, 33] and four in USA [13, 29, 32, 34]. Three studies provided risk estimates for postmenopausal status [13, 29, 33], and three for caffeinated and decaffeinated coffee consumption (27, 29, 34). The follow-up in prospective studies ranged from about 11 to 24 years, and the age range at study baseline was 25-76 years. Characteristics of the studies included in the meta-analysis are provided in Table 1.
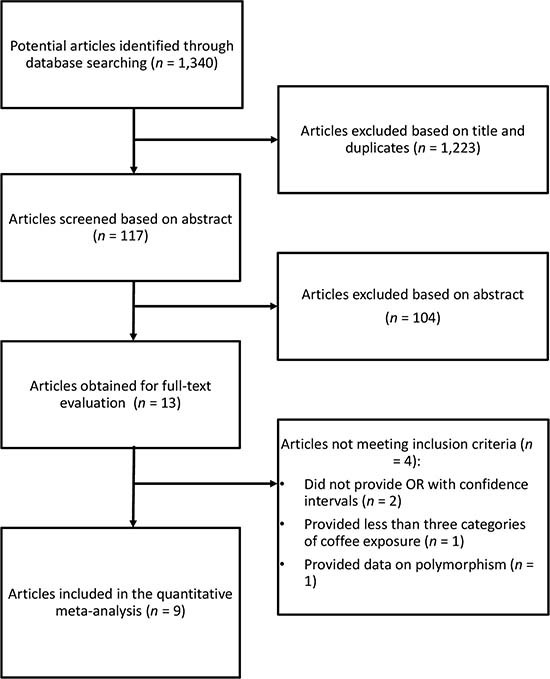
Figure 1: Flow chart and process selection of relevant studies exploring the association between coffee consumption and ovarian cancer risk.
Table 1: Characteristics of the cohort studies included in the meta-analysis
Author, year |
Cohort name, country |
Years of study, follow-up |
Cases; total population |
Age range |
Adjustments |
|---|---|---|---|---|---|
Larsson 2005 |
SMC, Sweden |
1987–2004, 15.1y (mean) |
301; 61,057 |
40–76y |
Age in months, BMI, education, parity, oral contraceptive use, and intakes of total energy, fruit, vegetables, milk, and tea. |
Silvera 2007 |
NBSS, Canada |
1980–2000, 16.4y (mean) |
264; 48,776 |
40–59y |
Age, smoking history, pack-years of smoking, alcohol intake, education, BMI, parity, participation in vigorous physical activity, menopausal status, oral contraceptive use, energy intake, lactose intake, study center, and randomization group. |
Steevens 2007 |
NLCS, Netherlands |
1986–1999, 13.3y |
280; 62,573 |
55–69y |
Age, use of oral contraceptives, parity, cigarette smoking, tea. |
Lueth 2008 |
IWHS, USA |
1986–2004, 18y (maximum) |
266; 29,060 |
55–69y |
Age, smoking, BMI, age at menopause, parity, oral contraceptive use, education level, physical activity, and total energy intake. |
Tworoger 2008 |
NHS, USA |
1980–2004, 24y (maximum) |
507; 80,253 |
30–55y |
Age, parity, oral contraceptive use, postmenopausal hormone use, tubal ligation, smoking status, and BMI. |
Nilsson 2010 |
VIP, Sweden |
1985–2007, 15y (maximum) |
71; 32,178 |
30–60y |
Age, sex, BMI, smoking, education, recreational physical activity. |
Braem 2012 |
EPIC, Europe |
1992–NA; 11.7y (median) |
1,244; 330,849 |
25–70y |
Center, age, parity, oral contraceptive use, BMI, smoking status, alcohol consumption, total energy intake, duration of breastfeeding, menopausal status, height, educational level. |
Hashibe 2015 |
PLCO, USA |
1992–2011; 13y (maximum) |
162; 50,563 |
55–74y |
Age, sex, race, education, smoking status, smoking frequency, smoking duration, time since stopping smoking for past smokers, and drinking frequency. |
Lukic 2016 |
NOWAC, Norway |
1991–2013; 13.1y (average) |
446; 91,767 |
30–70y |
Menopausal status at baseline, smoking status, age at smoking initiation, number of pack-years smoked, duration of education, BMI, physical activity level, use of oral contraceptives, alcohol consumption, number of children, use of hormone replacement therapy, and maternal history of breast cancer. |
Summary relative risk for highest versus lowest category of coffee consumption
The summary risk of ovarian cancer for highest versus lowest category of coffee consumption was RR = 1.06, 95% CI: 0.89, 1.26, with no evidence of heterogeneity I2 = 25%, P = 0.24 (Figure 2). No publication bias was found after visual inspection of funnel plot (Supplementary Figure 1) Two cohorts, NOWAC and VIP were excluded from the main analysis, as part of their cases are included in the multicentre study EPIC. However, an alternative analysis was performed by including this cohorts and excluding EPIC study; the relative risk was RR = 1.05, 95% CI: 0.88, 1.26; I2 = 20%, P = 0.27. Similarly, when taking into account menopausal status, no association between coffee consumption and ovarian cancer risk was found, and RR = 1.15, 95% CI: 0.92, 1.45; I2 = 0%, P = 0.87 (Table 2). Finally, no significant differences were found for coffee type or adjustment for potential confounders (Table 2).
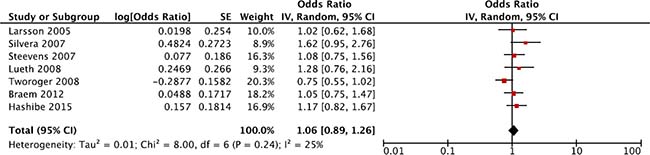
Figure 2: Forest plot of summary relative risks (RRs) of ovarian cancer for the highest versus lowest (reference) category of coffee consumption.
Table 2: Subgroup analyses of studies reporting risk of ovarian cancer for the highest versus lowest (reference) category coffee consumption
Subgroup |
No. of datasets |
RR (95% CI) |
I2 |
Pheterogeneity |
|---|---|---|---|---|
Total |
7 |
1.06 (0.89, 1.26) |
25% |
0.24 |
Geographical area |
||||
North America |
4 |
1.11 (0.79, 1.56) |
62% |
0.05 |
Europe |
3 |
1.05 (0.85, 1.32) |
0% |
0.98 |
Menopausal status |
||||
Postmenopausal |
3 |
1.15 (0.92, 1.45) |
0% |
0.87 |
Premenopausal |
0 |
NA |
NA |
NA |
Coffee type |
||||
Caffeinated |
3 |
1.09 (0.70, 1.68) |
78% |
0.01 |
Decaffeinated |
3 |
0.89 (0.66, 1.20) |
0% |
0.99 |
Adjusted for smoking |
||||
No |
1 |
1.02 (0.62, 1.69) |
NA |
NA |
Yes |
6 |
1.07 (0.88, 1.31) |
37% |
0.16 |
Adjusted for BMI |
||||
No |
2 |
1.13 (0.87, 1.45) |
0% |
0.76 |
Yes |
5 |
1.05 (0.81, 1.36) |
46% |
0.12 |
Adjusted for education |
||||
No |
2 |
0.89 (0.62, 1.27) |
55% |
0.14 |
Yes |
5 |
1.17 (0.97, 1.41) |
0% |
0.69 |
Adjusted for alcohol intake |
||||
No |
4 |
0.96 (0.76, 1.22) |
26% |
0.26 |
Yes |
3 |
1.18 (0.95, 1.47) |
0% |
0.40 |
Dose-response meta-analysis
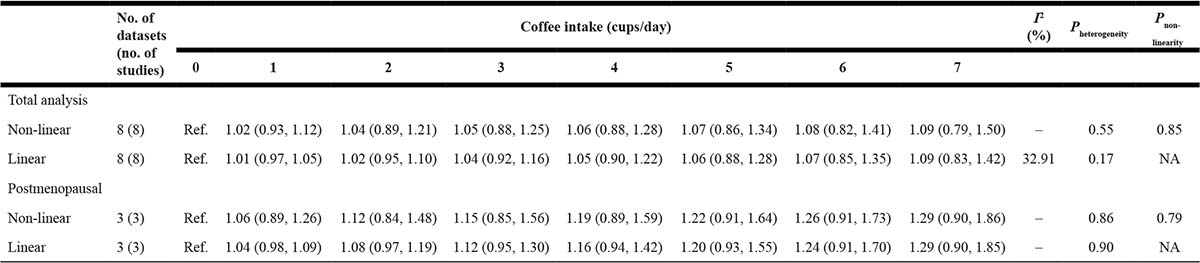
Eight studies [13, 28–34] were included in dose-response meta-analysis of prospective studies on coffee consumption and ovarian cancer risk, three of which provided risk estimates for postmenopausal individuals [13, 29, 33].
We found no evidence of association between coffee consumption and ovarian cancer risk in both analysis on total group of women (Figure 3, Table 3) and when considering only postmenopausal individuals.
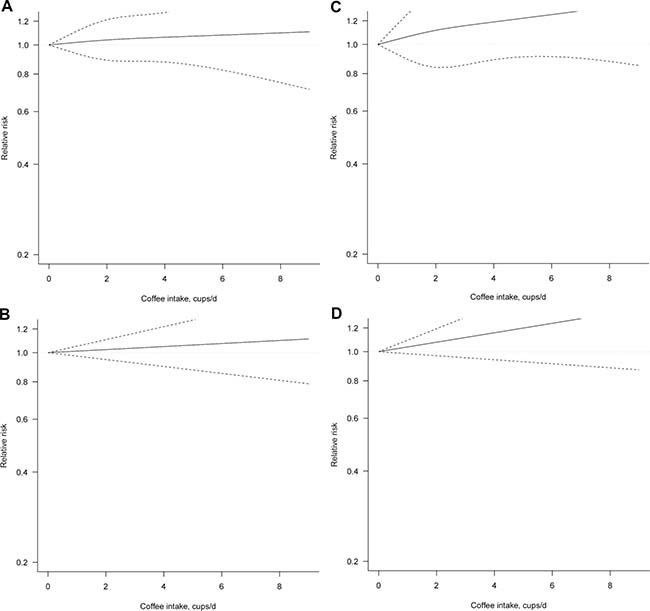
Figure 3: Dose-response association between coffee consumption and ovarian cancer risk (A) non-linear, total analysis; (B) linear, total analysis (C) non-linear, postmenopausal; (D) linear, postmenopausal.
Table 3: Dose-response meta-analysis of prospective cohort studies on coffee consumption and ovarian cancer risk
DISCUSSION
In this large meta-analysis of prospective cohort studies, we did not find any association of consumption of total, caffeinated, and decaffeinated coffee with risk of ovarian cancer. Despite a large number of studies suggested that an inverse relationship of coffee consumption and cancer risks may be mediated by various mechanisms, such as reduction of oxidative stress and DNA damages, detoxification of carcinogens, inhibition of carcinogenesis, and induction of apoptosis [35–38], a clear association with ovarian cancer risk could not be assessed. Coffee contains thousands of bioactive components including polyphenols, caffeine, diterpens and melanoidins, which have been shown to reduce oxidative stress and exert anti-cancerogenic properties [39, 40]. Dietary polyphenol intake has been associated lower risk of certain cancers and mortality in meta-analysis on prospective cohort studies [41, 42]. A protective effect of polyphenols could be exerted through an indirect action and through triggering defence mechanisms, carcinogenic detoxification, and activation or suppression of onco-suppressors and proto-oncogenes, respectively [43–45]. Additionally, it has been demonstrated that coffee intake improves metabolic features, both in women and men, which in turn could affect the association between cardio-metabolic conditions and certain cancers related to impaired metabolism and hormonal homeostasis [3, 46–49]. However, the results of the present meta-analysis showed that it is not likely a direct association between coffee consumption and ovarian cancer. A possible reason related to lack of effects of its polyphenol content may depend on their bioavailability [50]; in fact, it is still questionable which are the polyphenol metabolites reaching the target tissues, what is their amount, and whether they can actually exert any protective effects specifically on the ovarian cells [51].
Another reason for lack of association retrieved is potential confounding effect of other foods. Coffee consumption might be associated with unhealthy habits (i.e., higher alcohol intake. smoking), which in turn could be related to higher risk of cancers due to a synergistic effect of many functional components rather than an individual food or beverage [52]. Moreover, it has been suggested that polyphenols (including those contained in coffee) may be effective against multiple targets in cancer development and progression especially whether in combination with other polyphenols or micronutrients, such as antioxidant vitamins [53, 54]. In turn, the potential beneficial effects of coffee might be enhanced or counteracted by other dietary components, resulting in an overall null association depending on the overall diet rather than coffee alone. However, this hypothesis on the confounding effect of other foods on coffee should result in null results also for the association with other cancers, which in fact is not supported by other meta-analyses showing a decreased risk of certain cancers associated with higher coffee consumption: thus, either the confounding factors are strictly related to ovarian cancer risk or other explanation should be further investigated.
A major strength of our meta-analysis was the inclusion of cohort studies carried out with a prospective design, which implies detailed exposure and covariate assessment before the diagnosis of the outcome of interest (that is, ovarian cancer). Moreover, we performed a dose-response meta-analysis, which scientific value is higher than meta-analyses with exposure classified as high versus low, as it aims to investigate a possible dose-response relationship. However, the results of this study should be considered in light of some limitation. First, no stratified analysis was performed due to lack of available datasets, which prevented us from an in-depth analysis of potential confounders and effect modifiers, such as smoking status or body weight; despite our adjustment for smoking status, BMI index, education level and alcohol exposure, there is still a chance of unmeasured or residual confounding (e.g. menopausal status, that has not been considered in our analysis). Another limitation lies in the exposure assessment phase: the categories of low and high consumption varied across different studies, therefore overall estimates of high consumption might not be perfectly comparable; moreover, we don’t have data on coffee brewing methods, preparation, cup size, and duration of consumption. Such differences, if properly addressed, could yield to significant results in specific exposure subgroups (for instance, when analysing the relationship between tea consumption and ovarian cancer risk, a positive association has been detected for all tea and for black tea, but not for green tea) [55]. Similarly, histological information on cancer-subtype, to differentiate among epithelial cancer histotypes (“high grade serous” versus “endometrioid” versus “clear cell”), included through a stratified analysis, could highlight different pathological pathways and diversified exposure-disease relationships.
In conclusion, the present study provided a robust assessment of the relationship between coffee consumption and ovarian cancer, which, coherently with previously published literature, appears null. Additional prospective cohort studies specifying also subgroup analyses by key variables (i.e., smoking status, type of coffee, etc.) are needed to further improve current knowledge on such topic.
Abbreviations
EPIC: European Prospective Investigation into Cancer and Nutrition; IWHS: Iowa Women’s Health Study; NBSS: National Breast Screening Study; NHS: The Nurses’ Health Study; NLCS: The Netherlands Cohort Study; NOWAC: The Norwegian Women and Cancer study; PLCO: Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial; SMC: The Swedish Mammography Cohort; VIP: Västerbotten intervention project cohort.
CONFLICTS OF INTEREST
The authors have no conflicts of interest.
REFERENCES
1. European Coffee Federation. Coffee consumption in Europe [Available from: http://www.ecf-coffee.org/about-coffee/coffee-consumption-in-europe].
2. Grosso G, Godos J, Galvano F, Giovannucci EL. Coffee, Caffeine, and Health Outcomes: An Umbrella Review. Annu Rev Nutr. 2017; 37:131–156.
3. Marventano S, Salomone F, Godos J, Pluchinotta F, Del Rio D, Mistretta A, Grosso G. Coffee and tea consumption in relation with non-alcoholic fatty liver and metabolic syndrome: A systematic review and meta-analysis of observational studies. Clin Nutr. 2016; 35:1269–81.
4. Ding M, Bhupathiraju SN, Chen M, van Dam RM, Hu FB. Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: a systematic review and a dose-response meta-analysis. Diabetes Care. 2014; 37:569–86.
5. Ding M, Bhupathiraju SN, Satija A, van Dam RM, Hu FB. Long-term coffee consumption and risk of cardiovascular disease: a systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation. 2014; 129:643–59.
6. Zhou Q, Luo ML, Li H, Li M, Zhou JG. Coffee consumption and risk of endometrial cancer: a dose-response meta-analysis of prospective cohort studies. Sci Rep. 2015; 5:13410.
7. Bravi F, Tavani A, Bosetti C, Boffetta P, La Vecchia C. Coffee and the risk of hepatocellular carcinoma and chronic liver disease: a systematic review and meta-analysis of prospective studies. Eur J Cancer Prev. 2016.
8. Li YM, Peng J, Li LZ. Coffee consumption associated with reduced risk of oral cancer: a meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016; 121:381–389.e1.
9. Peisch SF, Van Blarigan EL, Chan JM, Stampfer MJ, Kenfield SA. Prostate cancer progression and mortality: a review of diet and lifestyle factors. World J Urol. 2016.
10. Wang A, Wang S, Zhu C, Huang H, Wu L, Wan X, Yang X, Zhang H, Miao R, He L, Sang X, Zhao H. Coffee and cancer risk: A meta-analysis of prospective observational studies. Sci Rep. 2016; 6:33711.
11. Godos J, Micek A, Marranzano M, Salomone F, Rio DD, Ray S. Coffee Consumption and Risk of Biliary Tract Cancers and Liver Cancer: A Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutrients. 2017; 9:E950.
12. Micek A, Godos J, Lafranconi A, Marranzano M, Pajak A. Caffeinated and decaffeinated coffee consumption and melanoma risk: a dose-response meta-analysis of prospective cohort studies. Int J Food Sci Nutr. 2017; 11:1–10.
13. Hashibe M, Galeone C, Buys SS, Gren L, Boffetta P, Zhang ZF, La Vecchia C. Coffee, tea, caffeine intake, and the risk of cancer in the PLCO cohort. Br J Cancer. 2015; 113:809–16.
14. Alicandro G, Tavani A, La Vecchia C. Coffee and cancer risk: a summary overview. Eur J Cancer Prev. 2017; 26:424–32.
15. Malerba S, Turati F, Galeone C, Pelucchi C, Verga F, La Vecchia C, Tavani A. A meta-analysis of prospective studies of coffee consumption and mortality for all causes, cancers and cardiovascular diseases. Eur J Epidemiol. 2013; 28:527–39.
16. Grosso G, Micek A, Godos J, Sciacca S, Pajak A, Martínez-González MA, Giovannucci EL, Galvano F. Coffee consumption and risk of all-cause, cardiovascular, and cancer mortality in smokers and non-smokers: a dose-response meta-analysis. Eur J Epidemiol. 2016; 31:1191–205.
17. Grosso G, Micek A, Godos J, Pajak A, Sciacca S, Bes-Rastrollo M, Galvano F, Martinez-Gonzalez MA. Long-Term Coffee Consumption Is Associated with Decreased Incidence of New-Onset Hypertension: A Dose-Response Meta-Analysis. Nutrients. 2017; 9:E890.
18. Friberg E, Orsini N, Mantzoros CS, Wolk A. Coffee drinking and risk of endometrial cancer—a population-based cohort study. Int J Cancer. 2009; 125:2413–17.
19. WHO. http://globocan.iarc.fr/Default.aspx [Available from: http://globocan.iarc.fr/Default.aspx.]
20. Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M, MacIntyre MF, Allen C, Hansen G, Woodbrook R, Wolfe C, Hamadeh RR, Moore A, Werdecker A, et al, and Global Burden of Disease Cancer Collaboration. The Global Burden of Cancer 2013. JAMA Oncol. 2015; 1:505–27.
21. Yu X, Bao Z, Zou J, Dong J. Coffee consumption and risk of cancers: a meta-analysis of cohort studies. BMC Cancer. 2011; 11:96.
22. Wells GA, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P, editors. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa, Canada: Ottawa Health Research Institute; 1999.
23. Greenland S. Quantitative methods in the review of epidemiologic literature. Epidemiol Rev. 1987; 9:1–30.
24. Greenland S, Longnecker MP. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am J Epidemiol. 1992; 135:1301–09.
25. Orsini NB, Greenland S. Generalized least squares for trend estimation of summarized dose-response data. Stata J. 2006; 6:40–57.
26. Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D. Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software. Am J Epidemiol. 2012; 175:66–73.
27. Braem MG, Onland-Moret NC, Schouten LJ, Tjønneland A, Hansen L, Dahm CC, Overvad K, Lukanova A, Dossus L, Floegel A, Boeing H, Clavel-Chapelon F, Chabbert-Buffet N, et al. Coffee and tea consumption and the risk of ovarian cancer: a prospective cohort study and updated meta-analysis. Am J Clin Nutr. 2012; 95:1172–81.
28. Larsson SC, Wolk A. Coffee consumption is not associated with ovarian cancer incidence. Cancer Epidemiol Biomarkers Prev. 2005; 14:2273–74.
29. Lueth NA, Anderson KE, Harnack LJ, Fulkerson JA, Robien K. Coffee and caffeine intake and the risk of ovarian cancer: the Iowa Women’s Health Study. Cancer Causes Control. 2008; 19:1365–72.
30. Lukic M, Licaj I, Lund E, Skeie G, Weiderpass E, Braaten T. Coffee consumption and the risk of cancer in the Norwegian Women and Cancer (NOWAC) Study. Eur J Epidemiol. 2016; 31:905–16.
31. Nilsson LM, Johansson I, Lenner P, Lindahl B, Van Guelpen B. Consumption of filtered and boiled coffee and the risk of incident cancer: a prospective cohort study. Cancer Causes Control. 2010; 21:1533–44.
32. Silvera SA, Jain M, Howe GR, Miller AB, Rohan TE. Intake of coffee and tea and risk of ovarian cancer: a prospective cohort study. Nutr Cancer. 2007; 58:22–27.
33. Steevens J, Schouten LJ, Verhage BA, Goldbohm RA, van den Brandt PA. Tea and coffee drinking and ovarian cancer risk: results from the Netherlands Cohort Study and a meta-analysis. Br J Cancer. 2007; 97:1291–94.
34. Tworoger SS, Gertig DM, Gates MA, Hecht JL, Hankinson SE. Caffeine, alcohol, smoking, and the risk of incident epithelial ovarian cancer. Cancer. 2008; 112:1169–77.
35. Lee WJ, Zhu BT. Inhibition of DNA methylation by caffeic acid and chlorogenic acid, two common catechol-containing coffee polyphenols. Carcinogenesis. 2006; 27:269–77.
36. Lee KJ, Jeong HG. Protective effects of kahweol and cafestol against hydrogen peroxide-induced oxidative stress and DNA damage. Toxicol Lett. 2007; 173:80–87.
37. Kalthoff S, Landerer S, Reich J, Strassburg CP. Protective effects of coffee against oxidative stress induced by the tobacco carcinogen benzo[α]pyrene. Free Radic Biol Med. 2017; 108:66–76.
38. Park GH, Song HM, Jeong JB. Kahweol from Coffee Induces Apoptosis by Upregulating Activating Transcription Factor 3 in Human Colorectal Cancer Cells. Biomol Ther (Seoul). 2017; 25:337–43.
39. Liang N, Kitts DD. Antioxidant property of coffee components: assessment of methods that define mechanisms of action. Molecules. 2014; 19:19180–208.
40. Hogervorst JG, Schouten LJ, Konings EJ, Goldbohm RA, van den Brandt PA. A prospective study of dietary acrylamide intake and the risk of endometrial, ovarian, and breast cancer. Cancer Epidemiol Biomarkers Prev. 2007; 16:2304–13.
41. Grosso G, Godos J, Lamuela-Raventos R, Ray S, Micek A, Pajak A, Sciacca S, D’Orazio N, Del Rio D, Galvano F. A comprehensive meta-analysis on dietary flavonoid and lignan intake and cancer risk: level of evidence and limitations. Mol Nutr Food Res. 2017; 61:1600930.
42. Grosso G, Micek A, Godos J, Pajak A, Sciacca S, Galvano F, Giovannucci EL. Dietary Flavonoid and Lignan Intake and Mortality in Prospective Cohort Studies: Systematic Review and Dose-Response Meta-Analysis. Am J Epidemiol. 2017; 185:1304–16.
43. Milenkovic D, Jude B, Morand C. miRNA as molecular target of polyphenols underlying their biological effects. Free Radic Biol Med. 2013; 64:40–51.
44. Wierzejska R. Coffee consumption vs. cancer risk - a review of scientific data. Rocz Panstw Zakl Hig. 2015; 66:293–98.
45. Cavin C, Holzhaeuser D, Scharf G, Constable A, Huber WW, Schilter B. Cafestol and kahweol, two coffee specific diterpenes with anticarcinogenic activity. Food Chem Toxicol. 2002; 40:1155–63.
46. Kim K, Kim K, Park SM. Association between the Prevalence of Metabolic Syndrome and the Level of Coffee Consumption among Korean Women. PLoS One. 2016; 11:e0167007.
47. Grosso G, Stepaniak U, Micek A, Topor-Mądry R, Pikhart H, Szafraniec K, Pająk A. Association of daily coffee and tea consumption and metabolic syndrome: results from the Polish arm of the HAPIEE study. Eur J Nutr. 2015; 54:1129–37.
48. Micek A, Grosso G, Polak M, Kozakiewicz K, Tykarski A, Puch Walczak A, Drygas W, Kwasniewska M, Pajak A. Association between tea and coffee consumption and prevalence of metabolic syndrome in Poland - results from the WOBASZ II study (2013-2014). Int J Food Sci Nutr. 2017; 69:358-368.
49. Takami H, Nakamoto M, Uemura H, Katsuura S, Yamaguchi M, Hiyoshi M, Sawachika F, Juta T, Arisawa K. Inverse correlation between coffee consumption and prevalence of metabolic syndrome: baseline survey of the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study in Tokushima, Japan. J Epidemiol. 2013; 23:12–20.
50. Martini D, Del Bo’ C, Tassotti M, Riso P, Del Rio D, Brighenti F, Porrini M. Coffee Consumption and Oxidative Stress: A Review of Human Intervention Studies. Molecules. 2016; 21:E979.
51. Koehnlein EA, Koehnlein EM, Corrêa RC, Nishida VS, Correa VG, Bracht A, Peralta RM. Analysis of a whole diet in terms of phenolic content and antioxidant capacity: effects of a simulated gastrointestinal digestion. Int J Food Sci Nutr. 2016; 67:614–23.
52. Grosso G, Bella F, Godos J, Sciacca S, Del Rio D, Ray S, Galvano F, Giovannucci EL. Possible role of diet in cancer: systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr Rev. 2017; 75:405–19.
53. Niedzwiecki A, Roomi MW, Kalinovsky T, Rath M. Anticancer Efficacy of Polyphenols and Their Combinations. Nutrients. 2016; 8:E552.
54. Stedile N, Canuto R, Col CD, Sene JS, Stolfo A, Wisintainer GN, Henriques JA, Salvador M. Dietary total antioxidant capacity is associated with plasmatic antioxidant capacity, nutrient intake and lipid and DNA damage in healthy women. Int J Food Sci Nutr. 2016; 67:479–88.
55. Leung AC, Cook LS, Swenerton K, Gilks B, Gallagher RP, Magliocco A, Steed H, Köbel M, Nation J, Brooks-Wilson A, Le ND. Tea, coffee, and caffeinated beverage consumption and risk of epithelial ovarian cancers. Cancer Epidemiol. 2016; 45:119–25.