
INTRODUCTION
Breast cancer is the second leading cause of cancer-related deaths in women and is the most common cancer in females, accounting for 23% of all cancer cases [1, 2]. Triple-negative breast cancer (TNBC) is a subtype characterized by the lack of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER-2) expression, as confirmed by immunohistochemistry or fluorescent in situ hybridization. TNBC is associated with a poor prognosis due to its more aggressive behavior, higher recurrence, generation of more metastases, and fewer treatment options compared with other breast cancer subtypes [3]. Cytotoxic chemotherapy remains the mainstay of treatment for TNBC, and metastatic organ sites and disease-free interval (DFI) are thought to be prognostic factors of advanced disease [4].
Serum lactate dehydrogenase (LDH) converts pyruvate to lactate in the cytoplasm during glycolysis and is thought to be a marker of tissue injury, inflammation, hemolysis, and myocardial damage [5–7]. In addition, abnormally high serum levels of LDH are predictive of prognosis in various malignancies [8] and are associated with breast cancer patient survival [4, 9–10]. Nevertheless, the association between advanced TNBC and serum LDH is not well understood; thus, we conducted an explorative study to determine the potential relationship.
RESULTS
All patients received a platinum-based or taxane-based regimen as first-line treatment (Table 1). In our daily practice, the previously used drugs will not be reapplied in those patients experiencing relapse within 3 months after completing neo-adjuvant or adjuvant chemotherapies. Table 2 shows the association between baseline serum LDH levels and clinical characteristics. Age (> 40 y vs. ≤ 40 y, odds ratio [OR]: 0.383, 95% confidence interval [CI]: 0.160–0.918, P = 0.031) and number of metastatic sites (2 vs. 1, OR: 4.619, 95% CI: 1.558–13.694, P = 0.006; ≥ 3 vs. 1, OR: 4.727, 95% CI: 1.777–12.570, P = 0.002) independently associated with abnormally high baseline serum LDH levels above normal. Univariate analyses revealed that DFI, number of metastatic sites, chemotherapeutic response, and LDH changes were potential prognostic factors for PFS (Table 3), and DFI, number of metastatic sites, liver, skeletal and lymph node metastases, chemotherapeutic response, and baseline serum LDH and LDH changes were potential prognosis factors for OS (Table 4). PFS and OS of different groups are shown in Figures 1 and 2. Patients with abnormally high baseline serum LDH levels above normal had significantly shorter OS (unadjusted HR: 2.192, 95% CI: 1.504–3.194, P < 0.001) but no difference in PFS (unadjusted HR: 1.237, 95% CI: 0.837–1.828, P = 0.284) compared to those with normal baseline serum LDH levels (Figure 1).
Table 1: Baseline clinical characteristics
Characteristics |
No. of patients (%) |
|
|---|---|---|
Age |
≤ 40 years |
31 (23.7) |
> 40 years |
100 (76.3) |
|
Menopausal status |
Pre-menopause |
75 (57.3) |
Post-menopause |
56 (42.7) |
|
Number of metastatic sites |
1 |
40 (30.5) |
2 |
32 (24.4) |
|
≥ 3 |
59 (45.1) |
|
Liver metastases |
Absent |
94 (71.8) |
Present |
37 (28.2) |
|
Lung metastases |
Absent |
69 (51.8) |
Present |
63 (48.1) |
|
Skeletal metastases |
Absent |
83 (63.4) |
Present |
48 (36.6) |
|
Lymph node metastases |
Absent |
39 (29.8) |
Present |
92 (70.2) |
|
Disease-free survival |
DFI > 12 months |
70 (53.4) |
DFI ≤ 12 months |
51 (38.9) |
|
Primary metastases |
10 (7.6) |
|
Chemotherapy response |
Yes |
77 (58.8) |
No |
54 (41.2) |
|
Baseline serum LDH |
Normal |
77 (58.8) |
Abnormal |
54 (41.2) |
|
LDH level Changes |
Group 1: Abnormal and higher than baseline |
25 (19.1) |
Group 2: Did not return to normal |
16 (12.2) |
|
Group 3: Decreased to normal |
28 (21.4) |
|
Group 4: Both normal |
62 (47.3) |
Table 2: The difference in baseline serum LDH status (normal vs abnormal) according to various baseline characteristics
Variables |
Baseline serum LDH status |
Logistic regression model |
|||
|---|---|---|---|---|---|
Normal |
Abnormal |
P* |
OR (95%CI) |
P** |
|
Age |
0.009 |
||||
≤ 40 years |
12 (38.7%) |
19 (61.3%) |
Ref. |
||
> 40 years |
65 (65.0%) |
35 (35.0%) |
0.383 (0.160–0.918) |
0.031 |
|
Menopausal status |
0.068 |
||||
Pre-menopause |
39 (52.0%) |
36 (48.0%) |
|||
Post-menopause |
38 (67.9%) |
18 (32.1%) |
|||
Number of metastatic sites |
0.001 |
||||
1 |
33 (82.5%) |
7 (17.5%) |
Ref. |
||
2 |
16 (50.0%) |
23 (50.0%) |
4.619 (1.558–13.694) |
0.006 |
|
≥ 3 |
28 (47.5%) |
31 (52.5%) |
4.727 (1.777–12.570) |
0.002 |
|
Liver metastases |
0.139 |
||||
Absent |
59 (62.8%) |
35 (37.2%) |
|||
Present |
18 (48.6%) |
19 (51.4%) |
|||
Lung metastases |
0.714 |
||||
Absent |
41 (60.3%) |
27 (39.7%) |
|||
Present |
36 (57.1%) |
27 (42.9%) |
|||
Skeletal metastases |
0.008 |
0.137 |
|||
Absent |
56 (67.5%) |
27 (32.5%) |
|||
Present |
21 (43.8%) |
27 (56.3%) |
|||
Lymph node metastases |
0.027 |
0.563 |
|||
Absent |
29 (74.4%) |
10 (25.6%) |
|||
Present |
48 (52.2%) |
44 (47.8%) |
|||
Disease-free survival |
0.365 |
||||
> 12 months |
44 (62.9%) |
26 (37.1%) |
|||
≤ 12 months |
29 (56.9%) |
22 (43.1%) |
|||
Primary metastatic |
4 (40.0%) |
6 (60.0%) |
|||
*chi-squared test; **Logistic regression model with multiple variables (age, menopausal status, number of metastatic sites, liver metastases, lung metastases, skeletal metastases, lymph node metastases, and disease-free survival)
Table 3: Univariate and multivariate analysis of prognostic factors in PFS of advanced TNBC patients
Variables |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
Median PFS(months) |
P* |
HR(95%CI) |
P** |
|
Disease-free survival |
0.023 |
|||
> 12 months |
11.3 |
Ref. |
||
≤ 12 months |
7.5 |
1.976 (1.300–3.003) |
0.001 |
|
Primary metastatic |
7.50 |
1.867 (0.831–4.194) |
0.130 |
|
Number of metastatic sites |
0.012 |
|||
1 |
12.2 |
|||
2 |
8.7 |
|||
≥ 3 |
7.8 |
|||
Chemotherapy response |
< 0.001 |
|||
Yes |
11.6 |
Ref. |
||
No |
6.7 |
2.684 (1.787–4.032) |
< 0.001 |
|
LDH level Changes |
0.004 |
|||
Group 1 |
6.0 |
Ref. |
||
Group 2 |
7.1 |
0.815 (0.412–1.612) |
0.557 |
|
Group 3 |
9.4 |
0.517 (0.278–0.963) |
0.038 |
|
Group 4 |
11.4 |
0.346 (0.204–0.587) |
< 0.001 |
|
* Log-rank test; **Cox regression model with multiple variables(disease-free survival, number of metastatic sites, chemotherapy response and LDH level Changes)
Table 4: Univariate and multivariate analysis of prognostic factors in OS of advanced TNBC patients
Variables |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
Median OS(months) |
P* |
HR(95%CI) |
P** |
|
Disease-free survival |
0.002 |
|||
> 12 months |
23.2 |
Ref. |
||
≤ 12 months |
14.7 |
1.888 (1.252–2.848) |
0.002 |
|
Primary metastatic |
13.6 |
1.571 (0.788–3.132) |
0.119 |
|
Number of metastatic sites |
< 0.001 |
|||
1 |
27.7 |
Ref. |
||
2 |
18.9 |
1.839 (1.805–3.118) |
0.024 |
|
≥ 3 |
13.1 |
2.449 (1.548–3.874) |
< 0.001 |
|
Liver metastases |
0.005 |
|||
Absent |
21.0 |
|||
Present |
13.6 |
|||
Skeletal metastases |
0.004 |
|||
Absent |
21.5 |
|||
Present |
14.3 |
|||
Lymph nodes metastases |
0.001 |
|||
Absent |
26.3 |
|||
Present |
15.7 |
|||
Chemotherapy response |
0.019 |
|||
Yes |
21.3 |
Ref. |
||
No |
15.4 |
1.754 (1.203–2.559) |
0.004 |
|
Baseline LDH level |
< 0.001 |
|||
Normal |
22.8 |
Ref. |
||
Abnormal |
13.4 |
2.073 (1.397–3.074) |
< 0.001 |
|
LDH level Changes |
< 0.001 |
|||
Group 1 |
13.9 |
|||
Group 2 |
11.8 |
|||
Group 3 |
14.2 |
|||
Group 4 |
24.9 |
|||
*Log-rank test; **Cox regression model with multiple variables(disease-free survival, number of metastatic sites, liver metastases, lung metastases, skeletal metastases, lymph node metastases, chemotherapy response, baseline LDH level and LDH level Changes).
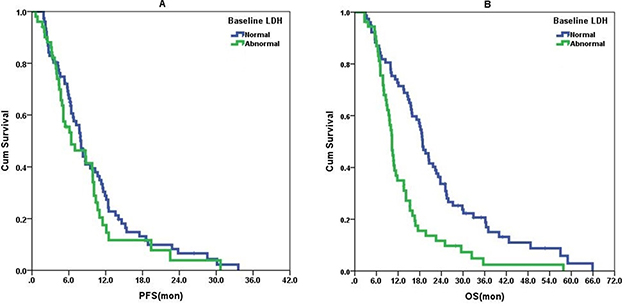
Figure 1: Baseline serum LDH level as a prognostic indicator of survival. There was no difference in PFS between advanced TNBC patients with abnormal baseline serum LDH levels (n = 54) and those with normal baseline serum LDH levels (n = 77) in (A) (unadjusted HR: 1.237, 95% CI: 0.837–1.828, P = 0.284). Advanced TNBC patients with abnormal baseline serum LDH levels (n = 54) had significantly poorer OS than those with normal baseline levels (n = 77) in (B) (unadjusted HR: 2.192, 95% CI: 1.504–3.194, P < 0.001).
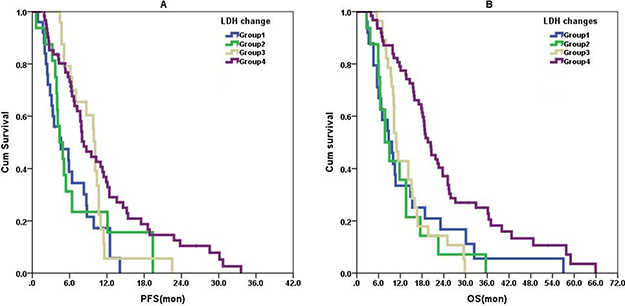
Figure 2: Serum LDH level changes as the prognostic variable in survival curves. There was a significant difference in PFS among the four groups defined by the changes of serum LDH in (A) (P = 0.004) even if adjusted with other variables. However, the difference in OS among the four groups in (B) (P < 0.001) disappears when adjusted. Group 1: Abnormal and higher than baseline; Group 2: Did not return to normal; Group 3: Decreased to normal; Group 4: Both normal.
Using the Cox regression model, we found that the independent prognostic factors of PFS for advanced TNBC patients were DFI (≤ 12 mon vs. > 12 mon, HR: 1.976, 95% CI: 1.300–3.003, P = 0.001), chemotherapeutic response (no vs. yes, HR: 2.684, 95% CI: 1.787–4.032, P < 0.001), and LDH changes (Group 3 vs. Group 1, HR: 0.517, 95% CI: 0.278–0.963, P = 0.038; Group 4 vs. Group1, HR: 0.346, 95% CI: 0.204–0.587, P < 0.001). The difference in OS among the four groups defined by LDH changes in Figure 2 disappeared when adjusted with other variables identified by univariate analysis with P < 0.1 (DFI, number of metastatic sites, liver metastases, skeletal metastases, lymph nodes metastases, chemotherapy response, and baseline LDH level). Actually, only DFI (≤ 12 mon vs. > 12 mon, HR = 1.888, 95% CI: 1.252–2.848, P = 0.002), number of metastatic sites (2 vs. 1, 95% CI: 1.805–3.118, P = 0.024; ≥ 3 vs. 1, HR: 2.449, 95% CI: 1.548–3.874, P < 0.001), chemotherapeutic response (no vs. yes, HR: 1.754, 95% CI: 1.203–2.559, P = 0.004) and baseline LDH (high vs. normal, HR: 2.073, 95% CI: 1.397–3.074, P < 0.001) were independent prognostic factors of OS for advanced TNBC patients.
Associations between clinical characteristics and chemotherapeutic responses are summarized in Table 5. No response to chemotherapy (SD or PD) was significantly associated with the presence of liver metastases (present vs. absent, OR: 4.267, 95% CI: 1.703–10.692, P = 0.002) and LDH changes (Group 3 vs. Group 1, OR: 0.074, 95% CI: 0.018–0.311, P < 0.001) according to logistic regression. Patients with post-treatment serum LDH that decreased to normal had the greatest ORR. With regard to ORR, Group 1 patients did not show inferiority compared to groups 2 and 4. Liver metastases and post-treatment LDH that decreased to normal were independently associated with ORR according to logistic regression.
Table 5: The difference in clinical response (CR or PR vs SD or PD) according to various clinical characteristics
Variables |
Clinical response |
Logistic regression model |
|||
|---|---|---|---|---|---|
CR or PR n (%) |
SD or PD n (%) |
P* |
OR (95%CI) |
P** |
|
Age |
0.745 |
||||
≤ 40 years |
19 (61.3%) |
12 (38.7%) |
|||
> 40 years |
58 (58.0%) |
42 (42.0%) |
|||
Menopausal status |
0.976 |
||||
Pre-menopause |
44 (58.7%) |
31 (41.3%) |
|||
Post-menopause |
33 (58.9%) |
23 (41.1%) |
|||
Number of metastatic sites |
0.413 |
||||
1 |
26 (65.0%) |
14 (35.0%) |
|||
2 |
20 (62.5%) |
12 (37.5%) |
|||
≥ 3 |
31 (52.5%) |
28 (47.5%) |
|||
Liver metastases |
0.008 |
||||
Absent |
62 (66.0%) |
32 (34.0%) |
Ref. |
||
Present |
15 (40.5%) |
22 (59.5%) |
4.267 (1.703–10.692) |
0.002 |
|
Lung metastases |
0.077 |
||||
Absent |
35 (51.5%) |
33 (48.5%) |
|||
Present |
42 (66.7%) |
21 (33.3%) |
|||
Skeletal metastases |
0.415 |
||||
Absent |
51 (61.4%) |
32 (38.6%) |
|||
Present |
26 (54.2%) |
27 (45.8%) |
|||
Lymph node metastases |
0.420 |
||||
Absent |
25 (64.1%) |
14 (35.9%) |
|||
Present |
52 (56.5%) |
40 (43.5%) |
|||
Disease-free survival |
0.365 |
||||
> 12 months |
26 (51.0%) |
25 (49.0%) |
|||
≤ 12 months |
44 (62.9%) |
26 (37.1%) |
|||
Primary metastatic |
7 (70.0%) |
3 (30.0%) |
|||
Baseline serum LDH |
0.415 |
||||
Normal |
43 (55.8%) |
34 (44.2%) |
|||
Abnormal |
34 (63.0%) |
20 (37.0%) |
|||
LDH level Changes |
0.005 |
||||
Group 1 |
10 (40.0%) |
15 (60.0%) |
Ref. |
||
Group 2 |
8 (50.0%) |
8 (50.0%) |
0.555 (0.145–2.121) |
0.390 |
|
Group 3 |
24 (85.7%) |
4 (14.3%) |
0.074 (0.018–0.311) |
< 0.001 |
|
Group 4 |
35 (56.5%) |
27 (43.5%) |
0.537 (0.201–1.437) |
0.216 |
|
*chi-squared test; **Logistic regression model with multiple variables (age, menopausal status, number of metastatic sites, liver metastases, lung metastases, skeletal metastases, lymph node metastases, disease-free survival, baseline serum LDH and LDH level Changes).
DISCUSSION
Advanced TNBC is highly aggressive, with a median PFS of 3–7.7 months and a median OS of about 1 year [11–15]. Similarly, the PFS and OS in this study population were 7.9 months (95% CI: 6.3–9.5 months) and 15.1 months (95% CI: 13.2–17.0 months), respectively.
LDH is required for aerobic glycolysis and can reversibly catalyze conversion of pyruvate to lactate. Recently, serum LDH has been reported to be important in numerous malignances and is documented to be 1 of 5 risk factors in the International Prognostic Index for the diffuse large B-cell lymphoma [16]. Baseline serum LDH has also been included in TNM staging system of melanoma [17]. Furthermore, high serum LDH levels are associated with adverse outcomes in lung cancer [18], esophageal squamous cell carcinoma [19], gastric [20] and pancreatic cancer [21] and renal cell carcinoma [22]. A recent systematic review and meta-analysis identified 76 studies of various solid tumors in which higher LDH was associated with shorter OS (HR = 1.7, P < 0.00001) and shorter PFS (HR = 1.75, P < 0.00001) [23]. In addition, LDH is reported to be a promising predictor of effectiveness of targeted agents such as bevacizumab, vatalanib, and sorafenib [24–26].
Although multiple studies have demonstrated the prognostic value of LDH in various malignances, the underlying pathophysiological mechanism remains unclear. LDH is possibly translationally controlled by HIF-1 and myc, and thus is regulated by the key oncogenic processes such as the phosphatidylinositol 3-kinase/AKt/TORC1/HIF pathway or by myc overexpression [27–29]. There is a positive feedback loop between HIF and LDH, and each can stimulate the activation of the other [30]. Moreover, HIF overexpression can activate vascular endothelial growth factor-A [31], thereby linking glycolysis and LDH to angiogenesis and cancer progression [32].
Here, we exploratively studied the association between serum LDH and prognosis of advanced TNBC patients, and found that abnormal serum LDH levels were significantly associated with metastatic sites and younger age of cancer onset. Greater metastatic sites reflect heavier tumor burden and younger patients tend to have poorer prognosis as compared to older patients [33, 34], and our data indicated that LDH might negatively influence the progression of advanced TNBC. However, menopausal status, liver, lung, skeleton, lymph node metastases and DFI were shown to have no effect on baseline serum LDH. Few studies describe the prognostic value of serum LDH in breast cancer. Yamamoto’s group[4] reported that abnormal serum LDH was associated with poorer survival among metastatic breast cancer subjects and Brown’s group[10] confirmed that LDH was strongly correlated with survival in breast cancer patients with bone metastases. Moreover, Liu and colleague [9] reported that greater LDH predicted worse 5-year OS in non-metastatic stage II and III breast cancers. We also found significant associations between serum LDH level and prognosis of advanced TNBC patients. However, an independent prognostic value was only found with LDH changes between baseline and post-treatment for PFS and baseline LDH for OS. Patients with post-treatment serum LDH level that decreased to normal and patients who had both normal baseline and post-treatment serum LDH had significantly longer PFS than patients whose post-treatment serum LDH were abnormal and higher than baseline. In addition, patients with normal baseline serum LDH had significantly longer OS than patients with abnormal baseline serum LDH. As mentioned earlier, abnormal serum LDH might have a negative effect on the progression of advanced TNBC, and this may partially explain why patients with normal post-treatment serum LDH level had better survival outcomes.
Decreases in LDH may reflect cessation of tumor growth, while increases are associated with tumor progression [35]. In this study, most of the 28 patients with post-treatment LDH that decreased to normal after chemotherapy, had a good response to chemotherapy (PR or CR), and ORR was significantly higher than that in patients with abnormal post-treatment serum LDH higher than baseline. This suggested that LDH changes after chemotherapy reflect tumor regression. However, no significant advantages were found for patients with post-treatment LDH that did not decline to normal and patients with both normal baseline and post-treatment LDH. Likely tumor regression occurred with the rapid and dramatic fall in LDH and this might explain why patients whose post-treatment LDH decreased to normal had longer PFS.
Therefore, serum LDH may be a useful biomarker to predict survival and chemotherapeutic response in advanced TNBC patients. More research is needed to confirm these findings and to understand the mechanism underlying LDH and tumor progression.
MATERIALS AND METHODS
A retrospective review was undertaken with female patients with advanced TNBC (n = 131) who received first-line chemotherapy at Fudan University Shanghai Cancer Center between 2005 and 2013. Patients were included if they had pathological confirmation of TNBC, biopsy or radiological confirmation of tumor recurrence or distant metastasis, good ECOG performance status, and available data on baseline and post-treatment serum LDH levels (see patient characteristics in Table 1). Patients were excluded if they had complications from other types of malignancies, no evidence of tumor recurrence or distant metastasis, acute heart failure, or severe renal or liver dysfunction.
Patients’ medical charts were reviewed to obtain data about clinical features, treatment information, and serum LDH levels. Menopause status was defined according to the National Comprehensive Cancer Network (NCCN) Guidelines (NCCN Clinical practice guidelines in oncology. Breast Cancer V1 2017 [36]). Serum LDH levels were measured using the Roche Cobas 8000 system (Roche, Indianapolis, IN, USA). All patients were told to fast after midnight on the day of the blood test. Baseline serum LDH levels were measured within 2 weeks before administering first-line chemotherapy. If multiple measurements were taken, the average of the measurements was used. Patients were stratified to normal baseline LDH (≤ 250 IU/L) and abnormal baseline LDH (>250 IU/L) groups. Post-treatment serum LDH measurements were conducted after two cycles of first-line chemotherapy. According to changes between baseline and post-treatment LDH values, patients were divided into four groups: Group 1 included patients with abnormal post-treatment serum LDH levels higher than baseline; Group 2 included patients with post-treatment serum LDH levels that decreased but did not return to normal; Group 3 included patients with post-treatment serum LDH levels that decreased to normal; and Group 4 included patients with normal baseline and post-treatment LDH levels. Tumor responses to chemotherapy (chemotherapeutic response) were assessed and graded as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD) according to the revised RECIST guideline (version 1.1) [37]. Clinical response was defined as either CR or PR. Survival information was collected from medical records or telephone interviews. The disease-free interval (DFI) was defined as the period between surgical resection and diagnosis of tumor recurrence or distant metastasis. Progression-free survival (PFS) was defined as the period between the start of chemotherapy and the first time of documented PD. Overall survival (OS) was defined as the period between diagnosis of local recurrence or distant metastasis and death or last follow-up. Objective response rate (ORR) was defined as the percent of patients with CR and PR.
We used SPSS 21.0 statistical software to analyze data, and a two-tailed p value < 0.05 was considered statistically significant. A multiple comparisons analysis was not mandatory because the goal of this exploratory analysis was to identify hypotheses that could be subject to more rigorous future examinations. A chi-squared test was used to investigate the association between baseline serum LDH levels and clinical features, as well as the association between various risk factors and chemotherapy response. Logistic regression was used to analyze the association between serum LDH levels and potentially relevant factors, as well as the association between the chemotherapeutic response and potential relevant factors. PFS and OS were determined according to the Kaplan–Meier method, and intergroup comparison according to the variables in Table 1 was performed by the log-rank test. Subsequently, the relevant variables identified by univariate analysis with a significant association with PFS and OS (P < 0.1) and two clinically potentially important variables (age and type of first-line treatment) were analyzed using the Cox regression model to determine the independent prognostic factors for PFS and OS.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.
FUNDING
This research was supported by a grant from Shanghai Municipal Commission of Health and Family Planning (No. 201640069) and the Shanghai Natural Science Foundation (No. 17ZR1405700).
REFERENCES
1. Boyle P. The globalisation of cancer. Lancet. 2006; 368:629–30.
2. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69–90.
3. Carey L, Winer E, Viale G, Cameron D, Gianni L. Triple-negative breast cancer: disease entity or title of convenience? Nat Rev Clin Oncol. 2010; 7:683–692.
4. Yamamoto N, Watanabe T, Katsumata N, Omuro Y, Ando M, Fukuda H, Takue Y, Narabayashi M, Adachi I, Takashima S. Construction and validation of a practical prognostic index for patients with metastatic breast cancer. J Clin Oncol. 1998; 16:2401–2408.
5. Kemp M, Donovan J, Higham H, Hooper J. Biochemical markers of myocardial injury. Br J Anaesth. 2004; 93:63–73.
6. Drent M, Cobben NA, Henderson RF, Wouters EF, van Dieijen-Visser M. Usefulness of lactate dehydrogenase and its isoenzymes as indicators of lung damage or inflammation. Eur Respir J. 1996; 9:1736–1742.
7. Kato GJ, McGowan V, Machado RF, Little JA, Taylor J 6th, Morris CR, Nichols JS, Wang X, Poljakovic M, Morris SM Jr, Gladwin MT. Lactate dehydrogenase as a biomarker of hemolysis-associated nitric oxide resistance, priapism, leg ulceration, pulmonary hypertension, and death in patients with sickle cell disease. Blood. 2006; 107:2279–2285.
8. Wulaningsih W, Holmberg L, Garmo H, Malmstrom H, Lambe M, Hammar N, Walldius G, Jungner I, Ng T, Van Hemelrijck M. Serum lactate dehydrogenase and survival following cancer diagnosis. Br J Cancer. 2015; 113:1389–1396.
9. Liu X, Meng QH, Ye Y, Hildebrandt MA, Gu J, Wu X. Prognostic significance of pretreatment serum levels of albumin, LDH and total bilirubin in patients with non-metastatic breast cancer. Carcinogenesis. 2015; 36:243–248.
10. Brown JE, Cook RJ, Lipton A, Coleman RE. Serum lactate dehydrogenase is prognostic for survival in patients with bone metastases from breast cancer: a retrospective analysis in bisphosphonate-treated patients. Clin Cancer Res. 2012; 18:6348–55.
11. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P, Narod SA. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007; 13:4429–4434.
12. Kassam F, Enright K, Dent R, Dranitsaris G, Myers J, Flynn C, Fralick M, Kumar R, Clemons M. Survival outcomes for patients with metastatic triple-negative breast cancer: implications for clinical practice and trial design. Clin Breast Cancer. 2009; 9:29–33.
13. Hu XC, Zhang J, Xu BH, Cai L, Ragaz J, Wang ZH, Wang BY, Teng YE, Tong ZS, Pan YY, Yin YM, Wu CP, Jiang ZF, et al. Cisplatin plus gemcitabine versus paclitaxel plus gemcitabine as first-line therapy for metastatic triple-negative breast cancer (CBCSG006): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2015; 16:436–46.
14. Tutt A, Ellis P, Kilburn L, Gilett C, Pinder S, Abraham J, Barrett S, Barrett-Lee P, Chan S, Cheang M, Fox L, Grigoriadis A, Harper-Wynne C, et al. The TNT trial: a randomized phase III trial of carboplatin (C) compared with docetaxel (D) for patients with metastatic or recurrent locally advanced triple negative or BRCA1/2 breast cancer (CRUK/07/012). Cancer Res. 2015; 75:S3–01.
15. O’Shaughnessy J, Schwartzberg L, Danso MA, Miller KD, Rugo HS, Neubauer M, Robert N, Hellerstedt B, Saleh M, Richards P, Specht JM, Yardley DA, Carlson RW, et al. Phase III Study of Iniparib Plus Gemcitabine and Carboplatin Versus Gemcitabine and Carboplatin in Patients With Metastatic Triple-Negative Breast Cancer. J Clin Oncol. 2014; 32:3840–3847.
16. Nagle SJ, Woo K, Schuster SJ, Nasta SD, Stadtmauer E, Mick R, Svoboda J. Outcomes of patients with relapsed/refractory diffuse large B-cell lymphoma with progression of lymphoma after autologous stem cell transplantation in the rituximab era. Am J Hematol. 2013; 88:890–4.
17. Garbe C, Peris K, Hauschild A, Saiag P, Middleton M, Spatz A, Grob JJ, Malvehy J, Newton-Bishop J, Stratigos A, Pehamberger H, Eggermont AM. Diagnosis and treatment of melanoma. European consensus-based interdisciplinary guideline--Update 2012. Eur J Cancer. 2012; 48:2375–2390.
18. Lee DS, Park KR, Kim SJ, Chung MJ, Lee YH, Chang JH, Kang JH, Hong SH, Kim MS, Kim YS. Serum lactate dehydrogenase levels at presentation in stage IV non-small cell lung cancer: predictive value of metastases and relation to survival outcomes. Tumour Biol. 2016; 37:619–25.
19. Zhang P, Xi M, Li QQ, He LR, Liu SL, Zhao L, Shen JX, Liu MZ. The modified glasgow prognostic score is an independent prognostic factor in patients with inoperable thoracic esophageal squamous cell carcinoma undergoing chemoradiotherapy. J Cancer. 2014; 5:689–695.
20. Zhao Z, Han F, Yang S, Hua L, Wu J, Zhan W. The Clinicopathologic Importance of Serum Lactic Dehydrogenase in Patients with Gastric Cancer. Dis Markers. 2014; 2014.
21. Tas F, Karabulut S, Ciftci R, Sen F, Sakar B, Disci R, Duranyildiz D. Serum levels of LDH, CEA, and CA19–9 have prognostic roles on survival in patients with metastatic pancreatic cancer receiving gemcitabine-based chemotherapy. Cancer Chemother Pharmacol. 2014; 73:1163–1171.
22. Cetin B, Afsar B, Deger SM, Gonul II, Gumusay O, Ozet A, Benekli M, Coskun U, Buyukberber S. Association between hemoglobin, calcium, and lactate dehydrogenase variability and mortality among metastatic renal cell carcinoma. Int Urol Nephrol. 2014; 46:1081–1087.
23. Petrelli F, Cabiddu M, Coinu A, Borgonovo K, Ghilardi M, Lonati V, Barni S. Prognostic role of lactate dehydrogenase in solid tumors: a systematic review and meta-analysis of 76 studies. Acta Oncol. 2015; 54:961–970.
24. Faloppi L, Scartozzi M, Bianconi M, Svegliati Baroni G, Toniutto P, Giampieri R, Del Prete M, De Minicis S, Bitetto D, Loretelli C, D’Anzeo M, Benedetti A, Cascinu S. The role of LDH serum levels in predicting global outcome in HCC patients treated with sorafenib: implications for clinical management. BMC Cancer. 2014; 14:110.
25. Scartozzi M, Giampieri R, Maccaroni E, Del Prete M, Faloppi L, Bianconi M, Galizia E, Loretelli C, Belvederesi L, Bittoni A, Cascinu S. Pre-treatment lactate dehydrogenase levels as predictor of efficacy of first-line bevacizumab-based therapy in metastatic colorectal cancer patients. Br J Cancer. 2012; 106:799–804.
26. Koukourakis MI, Giatromanolaki A, Sivridis E, Gatter KC, Trarbach T, Folprecht G, Shi MM, Lebwohl D, Jalava T, Laurent D, Meinhardt G, Harris AL. Prognostic and predictive role of lactate dehydrogenase 5 expression in colorectal cancer patients treated with PTK787/ZK 222584 (vatalanib) antiangiogenic therapy. Clin Cancer Res. 2011; 17:4892–4900.
27. Majumder PK, Febbo PG, Bikoff R, Berger R, Xue Q, McMahon LM, Manola J, Brugarolas J, McDonnell TJ, Golub TR, Loda M, Lane HA, Sellers WR. mTOR inhibition reverses Akt-dependent prostate intraepithelial neoplasia through regulation of apoptotic and HIF-1-dependent pathways. Nat Med. 2004; 10:594–601.
28. Zha X, Wang F, Wang Y, He S, Jing Y, Wu X, Zhang H. Lactate dehydrogenase B is critical for hyperactive mTOR-mediated tumorigenesis. Cancer Res. 2011; 71:13–18.
29. Youssef RF, Cost NG, Darwish OM, Margulis V. Prognostic markers in renal cell carcinoma: A focus on the ’mammalian target of rapamycin’ pathway. Arab J Urol. 2012; 10:110–117.
30. McFate T, Mohyeldin A, Lu H, Thakar J, Henriques J, Halim ND, Wu H, Schell MJ, Tsang TM, Teahan O, Zhou S, Califano JA, Jeoung NH, et al. Pyruvate dehydrogenase complex activity controls metabolic and malignant phenotype in cancer cells. J Biol Chem. 2008; 283:22700–22708.
31. Pouysségur J, Dayan F, Mazure NM. Hypoxia signalling in cancer and approaches to enforce tumour regression. Nature. 2006; 441:437–443.
32. Parks SK, Chiche J, Pouysségur J. Disrupting proton dynamics and energy metabolism for cancer therapy. Nat Rev Cancer. 2013; 13:611–623.
33. Lee DS, Park KR, Kim SJ, Chung MJ, Lee YH, Chang JH, Kang JH, Hong SH, Kim MS, Kim YS. Serum lactate dehydrogenase levels at presentation in stage IV non-small cell lung cancer: predictive value of metastases and relation to survival outcomes. Tumour Biol. 2016; 37:619–625.
34. Radecka B, Litwiniuk M. Breast cancer in young women. Ginekol Pol. 2016; 87:659–63.
35. Brindley CO, Francis FL. Serum lactic dehydrogenase and glutamic-oxaloacetic transminase correlations with measurements of tumor masses during therapy. Cancer Res. 1963; 23:112–117.
36. NCCN Clinical practice guidelines in oncology. Breast Cancer,Version 1. 2017.
37. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009; 45:228–247.