
INTRODUCTION
Apparent diffusion coefficient (ADC) is a quantitative parameter of water diffusion in tissues [1]. Previously, numerous studies investigated associations between ADC and several histopathological features in different tumors [2–5]. Some reports indicated that ADC can predict proliferation activity and, therefore, behavior of several malignancies [2, 3, 5]. As already mentioned, ADC can be divided into three sub-parameters: ADC minimum or ADCmin, mean ADC or ADCmean and ADC maximum or ADCmax [5]. As shown in the part 1 of this meta-analysis, several tumors showed different inverse correlations between ADCmean and KI 67 [6]. Overall, the calculated correlation coefficients ranged from –0.22 in breast cancer to –0.62 in ovarian cancer [6].
There were studies, which showed that ADCmin had stronger correlations with KI 67, and can better reflect proliferation potential of malignant lesions [7, 8]. However, the reported data were based on small number of investigated tumors/patients.
The purpose of this part of the meta-analysis was to provide evident data regarding associations between minimum ADC (ADCmin), and KI 67 in different tumors.
RESULTS
Overall, the identified 22 studies [7–28] contained data about associations between ADCmin and KI 67 for 944 patients (Table 1).
Table 1: Tumor types involved into the meta-analysis
Diagnosis |
n |
% |
|---|---|---|
Different breast tumors |
200 |
34.33 |
Glioma |
144 |
15.25 |
Cervical cancer |
117 |
12.39 |
Lung cancer |
93 |
9.85 |
Meningioma |
72 |
7.63 |
Pituary adenoma |
50 |
5.30 |
Cerebral lymphoma |
49 |
5.19 |
Prostatic cancer |
29 |
3.07 |
Neuroendocrine tumor |
22 |
2.33 |
Thyroid cancer |
14 |
1.48 |
Head and neck cancer |
11 |
1.17 |
Ganglioglioma |
10 |
1.06 |
Neurocytoma |
9 |
0.95 |
Total |
944 |
100 |
The pooled correlation coefficient for all patients (Figure 1) was –0.47 (95 % CI = [–0.58; –0.35]), heterogeneity Tau2 = 0.06, Chi2 = 193.62, df = 22 (P < 0.00001), I2 = 89 %, and test for overall effect Z = 7.76 (P < 0.00001).
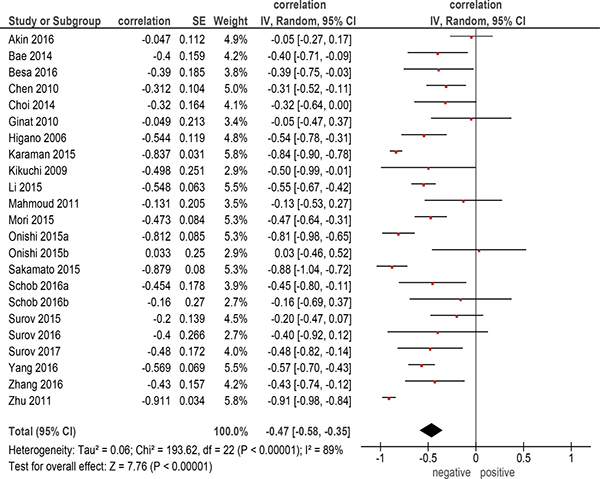
Figure 1: Forest plots of correlation coefficients between ADCmin and KI 67 in all included studies (n = 22).
On the next step correlation analysis for every identified entity was performed. Thereby, only primary tumors with more than two reports were included into the analysis. There were 6 entities with 632 patients (Table 2). The calculated correlation coefficients were as follows (Figure 2): -cerebral lymphoma: ρ = –0.61 (95% CI = [–0.82; –0.41]); -cervical cancer: ρ = –0.56 (95% CI = [–0.68;–0.43]); -pituitary adenoma:ρ = –0.55 (95% CI = [–1.31; 0.22]); -glioma: ρ = –0.40 (95% CI = [–0.55; –0.24]); - breast cancer: ρ = –0.37 (95% CI = [–0.74; –0.01]); -meningioma, ρ = –0.15 (95% CI = [–0.38; 0.07]).
Table 2: Tumor entities included into the subgroup analysis
Diagnosis |
n |
|---|---|
Breast cancer |
200 |
Glioma |
144 |
Cervical carcinoma |
117 |
Meningioma |
72 |
Pituary adenoma |
50 |
Cerebral lymphoma |
49 |
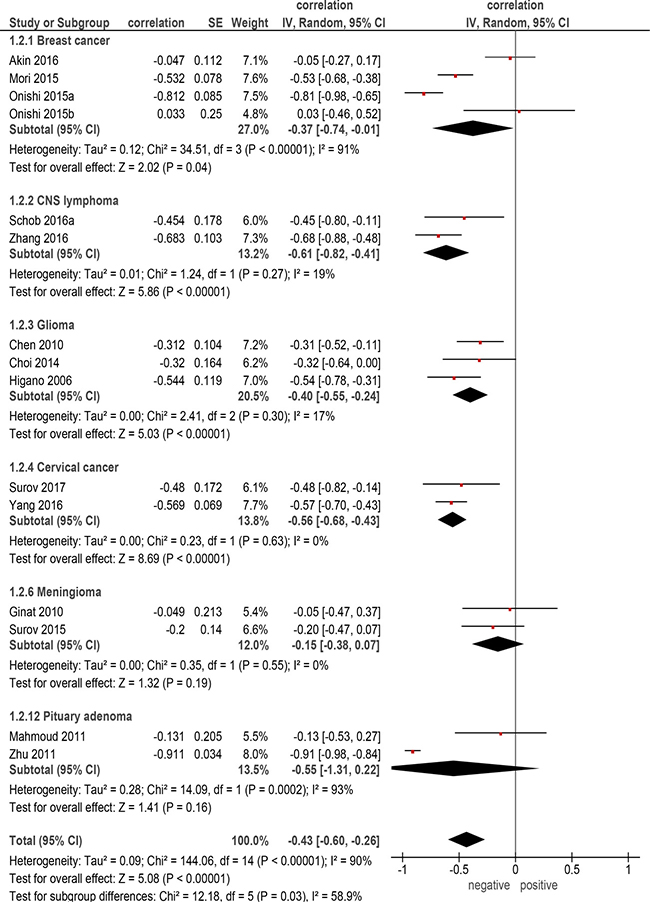
Figure 2: Forest plots of correlation coefficients between ADCmin and KI 67 in different primary tumors.
DISCUSSION
The present meta-analysis summarizes data about associations between ADCmin and KI 67 in different tumors
Previously, some investigations focused on relationships between ADC and histopathology, such as cell count and/or proliferation potential, in several tumors [2, 5]. However, the reported data were inconsistent: while some authors mentioned that ADC fractions can be associated with cellularity and KI 67, others did not confirm this finding [5, 7, 8]. Our previous meta-analysis regarding correlation between ADCmean and tumor cellularity showed that several tumors have different associations between the investigated parameters [29]. In detail, the calculated correlation coefficients ranged significantly and were as follows: ρ = –0.25 in lymphoma, ρ = –0.45 in meningioma, ρ = –0.48 in breast cancer, ρ = –0.53 in renal cell carcinoma, ρ = –0.53 in head and neck squamous cell carcinoma, ρ = –0.56 in prostatic cancer, ρ = –0.57 in uterine cervical cancer, ρ = –0.63 in lung cancer, ρ = –0.64 in ovarian cancer, and ρ = –0.66 in glioma [29]. Almost similar results were also identified for associations between ADCmean and KI 67 in the part 1 of the present work [6]. Because of these findings it can be postulated that ADCmean does not reflect cellularity and proliferation potential in all tumors and tumor-like lesions as assumed previously.
According to some authors, another ADC parameter, namely ADCmin has been reported to be more sensitive in prediction of cell count and proliferation activity than ADCmean [2, 7, 8]. However, a recent meta-analysis showed that ADCmin did not better correlate with tumor cellularity than ADCmean [30].
There were also inconsistent data about correlation between ADCmin and proliferation activity
As seen, in the present analysis, ADCmin correlated moderately with KI 67 expression in overall sample. The calculated correlation coefficient (ρ = –0.47) was almost similar to those reported for ADCmean (ρ = –0.44). However, for the identified tumor entities, it was different in comparison with the coefficients for ADCmean. So, in breast cancer, ADCmin correlated stronger with KI 67 (ρ = –0.37) than ADCmean (ρ = –0.22) [6], although the identified associations were slightly. Also in pituitary adenoma, and cerebral lymphoma, ADCmin tended to be better in comparison to ADCmean: ρ = –0.56 vs ρ = –0.44 [6], and ρ = –0.61 vs ρ = –0.55, respectively [6]. On the other hand, in glioma and meningioma, ADCmin did not better correlate with KI 67 expression than ADCmean: ρ = –0.40 vs ρ = –0.51 [6], and ρ = –0.15 vs ρ = –0.43 [6], respectively.
The exact cause of our findings is unclear. They supported previous suggestions that different ADC fractions reflect different histopathological features [2]. Obviously, there is no general rule regarding ADC parameters and tumor proliferation, i.e. for some tumors ADCmin and for other ADCmean predicts better proliferation potential.
Also for this part of the meta-analysis, already the mentioned limitations [6] do apply: only 6 named above tumor entities were involved into the work. For other malignancies and tumor-like lesions no data could be provided. In addition, the number of patients in the groups of pituitary adenoma, cerebral lymphoma, and meningioma was very small that questions the validity of the estimated correlation coefficients.
In conclusion, there are different inverse correlations between ADCmin and KI 67 in several tumors. In comparison with ADCmean, ADCmin seems to correlate better with proliferation activity in breast cancer, cerebral lymphoma, and pituitary adenoma.
In meningioma and glioma, however, ADCmean reflects better tumor proliferation than ADCmin.
MATERIALS AND METHODS
Data acquisition and proving
The search strategy and data acquisition are described precisely in the part 1 of the meta-analysis [6]. For this part, only data regarding associations between ADCmin derived from diffusion weighted imaging (DWI) and expression of KI 67 in different tumors and tumor-like lesions were collected. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) was used for the research [31].
Overall, 22 studies were included into the present analysis [7–28]. The following data were extracted from the literature: authors, year of publication, number of patients, tumor type, and correlation coefficients.
Meta-analysis
The methodological quality of the 23 studies was independently checked by two observers (A.S. and H.J.M.) using the Quality Assessment of Diagnostic Studies (QUADAS) instrument according to previous descriptions [32, 33]. The results of QUADAS proving is given in Table 3.
Table 3: Methodological quality of the involved 23 studies according to the QUADAS criteria
QUADAS criteria |
Yes (%) |
No (%) |
Unclear (%) |
|---|---|---|---|
Patient spectrum |
23 (100) |
||
Selection criteria |
20 (86.96) |
3 (13.04) |
|
Reference standard |
23 (100) |
||
Disease progression bias |
23 (100) |
||
Partial vertification bias |
23 (100) |
||
Differential vertification bias |
23 (100) |
||
Incorporation bias |
23 (100) |
||
Text details |
23 (100) |
||
Reference standard details |
23 (100) |
||
Text review details |
12 (52.18) |
3 (13.04) |
8 (34.78) |
Diagnostic review bias |
15 (65.22) |
3 (13.04) |
5 (21.74) |
Clinical review bias |
23 (100) |
||
Uninterpretable results |
23 (100) |
||
Withdrawls explained |
23 (100) |
Associations between ADCmin and KI 67 were analyzed by Spearman’s correlation coefficient. The reported Pearson correlation coefficients in some studies were converted into Spearman correlation coefficients as described previously [34].
The meta-analysis was undertaken by using RevMan 5.3 (Computer program, version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Heterogeneity was calculated by means of the inconsistency index I² [35, 36]. In a subgroup analysis, studies were stratified by tumor type. Furthermore, DerSimonian and Laird random-effects models with inverse-variance weights were used without any further correction [37].
CONFLICTS OF INTEREST
There are no conflicts of interest.
FUNDING
None.
REFERENCES
1. Fornasa F. Diffusion-weighted Magnetic Resonance Imaging: What Makes Water Run Fast or Slow? J Clin Imaging Sci. 2011; 1:27.
2. Bollineni VR, Kramer G, Liu Y, Melidis C, deSouza NM. A literature review of the association between diffusion-weighted MRI derived apparent diffusion coefficient and tumour aggressiveness in pelvic cancer. Cancer Treat Rev. 2015; 41:496–502.
3. Surov A, Meyer HJ, Höhn AK, Behrmann C, Wienke A, Spielmann RP, Garnov N. Correlations between intravoxel incoherent motion (IVIM) parameters and histological findings in rectal cancer: preliminary results. Oncotarget. 2017; 8:21974–21983. https://doi.org/10.18632/oncotarget.15753.
4. Sinkus R, Van Beers BE, Vilgrain V, DeSouza N, Waterton JC. Apparent diffusion coefficient from magnetic resonance imaging as a biomarker in oncology drug development. Eur J Cancer. 2012; 48:425–31.
5. Surov A, Caysa H, Wienke A, Spielmann RP, Fiedler E. Correlation between different ADC fractions, cell count, Ki-67, total nucleic areas and average nucleic areas in meningothelial meningiomas. Anticancer Res. 2015; 35:6841–6.
6. Surov A, Meyer HJ, Wienke A. Associations between apparent diffusion coefficient (ADC) and KI 67 in different tumors: A Meta-Analysis. Part 1: ADCmean. Oncotarget. 2017; 8:75434–75444. https://doi.org/10.18632/oncotarget.20406.
7. Surov A, Meyer HJ, Schob S, Höhn AK, Bremicker K, Exner M, Stumpp P, Purz S. Parameters of simultaneous 18F-FDG-PET/MRI predict tumor stage and several histopathological features in uterine cervical cancer. Oncotarget. 2017; 8:28285–28296. https://doi.org/10.18632/oncotarget.16043.
8. Zhang Y, Zhang Q, Wang XX, Deng XF, Zhu YZ. Value of pretherapeutic DWI in evaluating prognosis and therapeutic effect in immunocompetent patients with primary central nervous system lymphoma given high-dose methotrexate-based chemotherapy: ADC-based assessment. Clin Radiol. 2016; 71:1018–1029.
9. Akın Y, Uğurlu MÜ, Kaya H, Arıbal E. Diagnostic value of diffusion-weighted Imaging and apparent diffusion coefficient values in the differentiation of breast lesions, histpathologic subgroups and correlatıon with prognostıc factors using 3.0 Tesla MR. J Breast Health. 2016; 12:123–132.
10. Bae H, Yoshida S, Matsuoka Y, Nakajima H, Ito E, Tanaka H, Oya M, Nakayama T, Takeshita H, Kijima T, Ishioka J, Numao N, Koga F, et al. Apparent diffusion coefficient value as a biomarker reflecting morphological and biological features of prostate cancer. Int Urol Nephrol. 2014; 46:555–561.
11. Besa C, Ward S, Cui Y, Jajamovich G, Kim M, Taouli B. Neuroendocrine liver metastases: Value of apparent diffusion coefficient and enhancement ratios for characterization of histopathologic grade. J Magn Reson Imaging. 2016; 44:1432–1441.
12. Chen Z, Ma L, Lou X, Zhou Z. Diagnostic value of minimum apparent diffusion coefficient values in prediction of neuroepithelial tumor grading. J Magn Reson Imaging. 2010; 31:1331–1338.
13. Choi H, Paeng JC, Cheon GJ, Park CK, Choi SH, Min HS, Kang KW, Chung JK, Kim EE, Lee DS. Correlation of 11C-methionine PET and diffusion-weighted MRI: is there a complementary diagnostic role for gliomas? Nucl Med Commun. 2014; 35:720–726.
14. Ginat DT, Mangla R, Yeaney G, Wang HZ. Correlation of diffusion and perfusion MRI with Ki-67 in high-grade meningiomas. AJR Am J Roentgenol. 2010; 195:1391–1395.
15. Higano S, Yun X, Kumabe T, Watanabe M, Mugikura S, Umetsu A, Sato A, Yamada T, Takahashi S. Malignant astrocytic tumors: clinical importance of apparent diffusion coefficient in prediction of grade and prognosis. Radiology. 2006; 241:839–846.
16. Karaman A, Durur-Subasi I, Alper F, Araz O, Subasi M, Demirci E, Albayrak M, Polat G, Akgun M, Karabulut N. Correlation of diffusion MRI with the Ki-67 index in non-small cell lung cancer. Radiol Oncol. 2015; 49:250–255.
17. Kikuchi T, Kumabe T, Higano S, Watanabe M, Tominaga T. Minimum apparent diffusion coefficient for the differential diagnosis of ganglioglioma. Neurol Res. 2009; 31:1102–1107.
18. Li L, Wang K, Sun X, Wang K, Sun Y, Zhang G, Shen B. Parameters of dynamic contrast-enhanced MRI as imaging markers for angiogenesis and proliferation in human breast cancer. Med Sci Monit. 2015; 21:376–382.
19. Mahmoud OM, Tominaga A, Amatya VJ, Ohtaki M, Sugiyama K, Sakoguchi T, Kinoshita Y, Takeshima Y, Abe N, Akiyama Y, El-Ghoriany AI, Abd Alla AK, El-Sharkawy MA, et al. Role of PROPELLER diffusion-weighted imaging and apparent diffusion coefficient in the evaluation of pituitary adenomas. Eur J Radiol. 2011; 80:412–417.
20. Mori N, Ota H, Mugikura S, Takasawa C, Ishida T, Watanabe G, Tada H, Watanabe M, Takase K, Takahashi S. Luminal-type breast cancer: correlation of apparent diffusion coefficients with the Ki-67 labeling index. Radiology. 2015; 274:66–73.
21. Onishi N, Kanao S, Kataoka M, Iima M, Sakaguchi R, Kawai M, Kataoka TR, Mikami Y, Toi M, Togashi K. Apparent diffusion coefficient as a potential surrogate markerfor Ki-67 index in mucinous breastcarcinoma. J Magn Reson Imaging. 2015; 41:610–615.
22. Sakamoto R, Okada T, Kanagaki M, Yamamoto A, Fushimi Y, Kakigi T, Arakawa Y, Takahashi JC, Mikami Y, Togashi K. Estimation of proliferative potentiality of central neurocytoma: correlation alanalysis of minimum ADC and maximum SUV with MIB-1 labeling index. Acta Radiol. 2015; 56:114–120.
23. Schob S, Meyer J, Gawlitza M, Frydrychowicz C, Müller W, Preuss M, Bure L, Quäschling U, Hoffmann KT, Surov A. Diffusion-Weighted MRI reflects proliferative activity in primary CNS lymphoma. PLoS One. 2016; 11:e0161386.
24. Schob S, Voigt P, Bure L, Meyer HJ, Wickenhauser C, Behrmann C, Höhn A, Kachel P, Dralle H, Hoffmann KT, Surov A. Diffusion-Weighted imaging using a readout-segmented, multishot EPI sequence at 3 T distinguishes between morphologically differentiated and undifferentiated subtypes of thyroid carcinoma- a preliminary study. Transl Oncol. 2016; 9:403–410.
25. Surov A, Stumpp P, Meyer HJ, Gawlitza M, Höhn AK, Boehm A, Sabri O, Kahn T, Purz S. Simultaneous (18)F-FDG-PET/MRI: Associations between diffusion, glucose metabolism and histopathological parameters in patients with head and neck squamous cell carcinoma. Oral Oncol. 2016; 58:14–20.
26. Surov A, Gottschling S, Mawrin C, Prell J, Spielmann RP, Wienke A, Fiedler E. Diffusion-weighted imaging in meningioma: Prediction of tumor grade and association with histopathological parameters. Transl Oncol. 2015; 8:517–523.
27. Yang W, Qiang JW, Tian HP, Chen B, Wang AJ, Zhao JG. Minimum apparent diffusion coefficient for predicting lymphovascular invasion in invasive cervical cancer. J Magn Reson Imaging. 2017; 45:1771–1779.
28. Zhu L, Ren G, Li K, Liang ZH, Tang WJ, Ji YM, Li YX, Cheng HX, Geng DY. Pineal parenchymal tumours: minimum apparent diffusion coefficient in prediction of tumour grading. J Int Med Res. 2011; 39:1456–1463.
29. Surov A, Meyer HJ, Wienke A. Correlation between apparent diffusion coefficient (ADC) and cellularity is different in several tumors: A Meta-Analysis. Oncotarget. 2017; 8:59492–59499. https://doi.org/10.18632/oncotarget.17752.
30. Surov A, Meyer HJ, Wienke A. Correlation between minimum apparent diffusion coefficient (ADCmin) and tumor cellularity: A meta-analysis. Anticancer Res. 2017; 37:3807–3810.
31. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6:e1000097.
32. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol. 2003; 3:25.
33. Whiting PF, Weswood ME, Rutjes AW, Reitsma JB, Bossuyt PN, Kleijnen J. Evaluation of QUADAS, a tool for the quality assessment of diagnostic accuracy studies.BMC Med Res Methodol. 2006; 6:9.
34. Chalkidou A, Landau DB, Odell EW, Cornelius VR, O’Doherty MJ, Marsden PK. Correlation between Ki-67 immunohistochemistry and 18F-fluorothymidine uptake in patients with cancer: A systematic review and meta-analysis. Eur J Cancer. 2012; 48:3499–513.
35. Leeflang MM, Deeks JJ, Gatsonis C, Bossuyt PM. Systematic reviews of diagnostic test accuracy. Ann Intern Med. 2008; 149:889–97.
36. Zamora J, Abraira V, Muriel A, Khan K, Coomarasamy A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Medical Research Methodology. 2006; 6:31.
37. DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clinical Trials. 1986; 7:177–88.