
INTRODUCTION
Haemophilus parasuis (HPS) is a Gram-negative bacterium belongs to of the Pasteurella genus. The HPS bacterium is a common inhabitant of the upper respiratory tract in pigs, and infection is characterised by arthritis, meningitis and polyserositis [1, 2]. HPS can invade the body and cause a systemic infection, and is associated with the transportation, weaning and impaired maternal immunity. According to previous reports More than 15 kinds of HPS serovars had been described. Serovars 1, 5, 10, 12, 13 and 14 have been reported to be highly pathogenic, causing the death or morbidity. Serovars 4 and 5 are the most epidemic among isolates in China [3], and this pathogen has caused a massive worldwide economic losses in the pigs industry in recent decades.
Tildipirosin is a semi-synthetic tylosin analog, characterised as a novel 16-membered ring macrolide antimicrobial, depicted in Figure 1. Tildipirosin acts as a bacteriostatic against HPS and Actinobacillus pleuropneumoniae [4]. As a class, macrolides are characterised by extensive partitioning into tissues, where they can be found in a multi-fold higher concentration compared to the concentration in plasma [5–7]. Compared with other macrolides, tildipirosin has a long half-life and maintains a high concentration in lung tissue [8, 9].
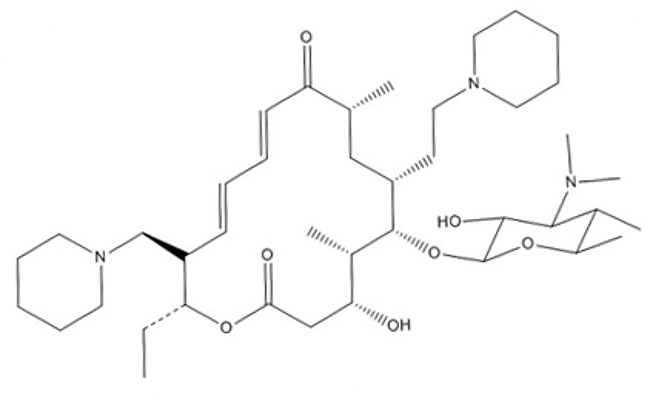
Figure 1: Structure of tildipirosin.
According to the guidelines that encourage the rational use of antibiotics, the susceptibility of bacteria to antimicrobial agents should be determined prior to treatment. Presently, microbiological breakpoints (epidemiological cutoff values) and clinical breakpoints are used. Epidemiological cut-off values, in bimodal distributions of minimum inhibitory concentrations (MIC), are used to separate susceptible subpopulations from resistant subpopulations. However, microbiological breakpoints do not consider the pharmacological effects of antimicrobial agents in vivo. The concentration of antimicrobial agents, which can be determined at the site of infection under the recommended dosage, is an important parameter for breakpoint determination [10, 11]. The breakpoints of tildipirosin against HPS have not yet been established. Therefore it has a great importance to establish the susceptibility breakpoint of tildipirosin for both the susceptibility testing and monitoring of resistance. A multistage approach is used to develop a susceptibility breakpoints, which generally includes four steps, as follows: (1) MIC distribution is determined for a group of bacteria; (2) bacteriostatic activities are examined by time-kill experiments with selected strains; (3) available pharmacodynamic (PD) and target animal pharmacokinetic (PK) data obtained in vitro, in addition to efficacy data, are analysed by Monte Carlo simulation; and (4) statistical analyses of susceptibility data to determine breakpoints [12]. In previous studies, clinical data regarding antimicrobial agents have been difficult to obtain. In the absence of clinical breakpoints, epidemiological cutoff values (ECVs) can be used to help separate susceptible from resistant isolates [13, 14]. However, the susceptibility breakpoint determined from ECVs alone cannot be used to calculate the clinical breakpoint, although the PK/PD cutoff values are associated with clinical efficacy [15].
Macrolides have an extraordinary capability to accumulate in different lung tissue compartments, showing rapid and extensive distribution, in addition to persistence in pulmonary epithelial lining fluid (PELF) [7, 16]. The concentration of macrolides in PELF has been used previously to establish an intrapulmonary PK model reported by Conte [17]. However, it had been widely accepted that lung tissue was not act as the bio-phase for lung infected by pathogens [18–21]. HPS similar to pasteurella multocida was strictly extracellular pathogens, and the PELF was its main location for these extracellular pathogens. Although the drug concentration in PELF exceeded many times than that in plasma, it could be unable to maintain an effective local extracellular concentration in PLEF because of its extremely slow dynamic and release of drug in vivo. It had been reported in the previously described study by Kiem [22, 23], that high PELF drug concentration was caused by the lyses of cells (including high drug concentrations) during the bronchoalveolar lavage procedure when it was required to collect PELF. Thus, the high drug concentrations in PELF were not authentic, and it could not be the final target tissue for PK/PD analysis [20]. Furthermore, it was recommended to select PK data in plasma to study the PK/PD cutoff (COPD) for macrolides.
For the evaluation of antimicrobial drugs, it is essential to optimise the dose schedule to attain the clinical cures and reduce the emergence of antimicrobial drug resistance [24]. The pharmacokinetics-pharmacodynamics (PK/PD) integration model can reveal the relationship between antibiotics and bacterium in the specific animals, and quantify the potency and efficacy of antibiotics against bacterium. Moreover, the PK/PD integration model can also prevent resistance development and provide optimal dosage strategies [25, 26]. As an effective tool for assessing the optimal dosage regimens, PK/PD analysis has been recommended in the development of new antimicrobial compounds by the Food and Drug Administration (FDA) and European Medicines Agency (EMA) [27].
The purpose of the current study was to establish the ECV and COPD of tildipirosin against HPS based on wild-type MIC distributions and PK/PD data in vitro and ex vivo, respectively, and also compare the pharmacokinetics in plasma and PELF. Moreover, the rational dosage regimen of tildipirosin against HPS was also established for veterinary clinical guidance based on PK-PD integration modeling.
RESULTS
Minimum inhibitory concentration distributions and wild-type cutoff values
The MIC distribution of tildipirosin against HPS, shown in Figure 2, was determined to be bimodal by visual inspection. The MICs of tildipirosin were distributed in the range of 0.032 to 256 μg/ml, with two peak values observed at 0.0625 and 0.5 μg/ml. The distribution ratios of each MIC (0.032, 0.0625, 0.125, 0.25, 0.5, 1, 2, 4, 8, 16 and 256 μg/ml) for the 164 isolates were as follows: “2.44% for 0.032 μg/ml, 12.20% for 0.0625 μg/ml…” and so on. The MIC50 and MIC90 were 0.25 and 2 μg/ml, respectively. All of the 164 HPS isolates were able to be identified by PCR. The MIC for chloromycetin against Escherichia coli (ATCC25922) was found to be 8 μg/ml, which is within and suitable for the acceptable quality control (QC) range according to the CLSI (M31-A3).
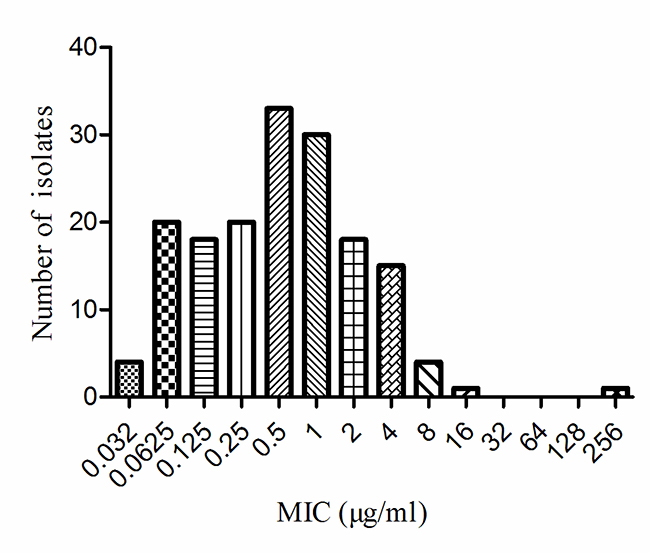
Figure 2: MIC distributions of tildipirosin against 164 HPS.
Epidemiological cutoff values
The cumulative counts for MIC data, with the exception of one resistant strain with an MIC of 256 μg/ml, were performed to match a suitably shaped normal distribution (normality test, P > 0.200) using SigmaStat and GraphPad Prism software (Figure 3). Furthermore, the strain whose MIC was 256 μg/ml had been proved as resistant one, with a resistant HAPS_RS04930 reported by Zhixin Lei [49, 50]. The optimum MIC range from 0.002 to 32 μg/ml was obtained from non-linear regression (Table 1), and the range was further corrected to 0.032 to 32 μg/ml according to the optimum distribution determined using the NORMINV function in Microsoft Excel. The probability of an MIC at 8 μg/ml was 97.9%, which encompassed 95% of the WT isolates, defined as the ECV using the NORMDIST function in Microsoft Excel (Table 2).
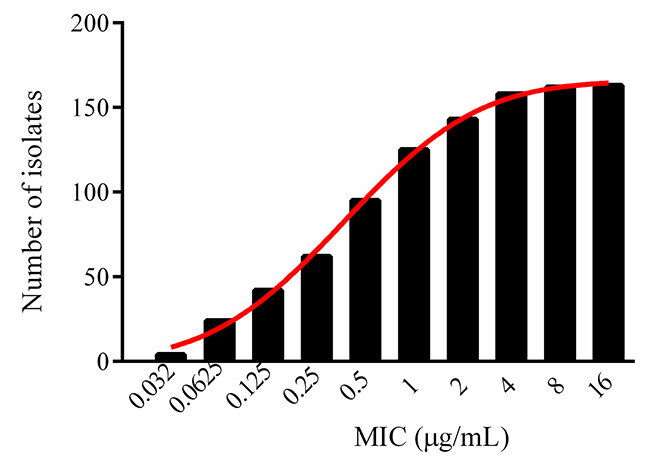
Figure 3: Cumulative MICs distribution of tildipirosin against HPS after non-linear regression.
Table 1: The values of optimum non-linear least squares regression fitting
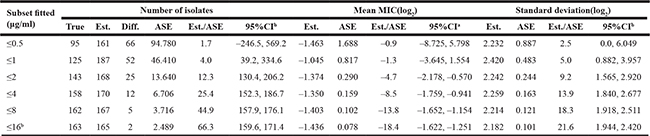
Note: Est., represent the value of non-linear regression estimation; Diff., represent the value of estimation of N minus true N; ASE, represent the value of asymptotic standard error; Est./ASE, represent the value of estimation divided by asymptotic standard error; CI, represent the value of confidence intervals; a, represent the value of 95%CI of estimation; b, represent the value of the smallest difference between the estimation and the true number of isolates.
Table 2: The probability estimation of ECV with NORMDIST function in microsoft excel
Optimum MIC |
Log2 Mean MIC |
Mean MIC |
Log2 SD |
High cut-off (μg/ml) |
Probability of a higher value |
|---|---|---|---|---|---|
≤32 |
–1.436 |
0.370 |
2.182 |
32 |
99.8% |
≤16 |
–1.436 |
0.370 |
2.182 |
16 |
99.3% |
≤8* |
–1.436 |
0.370 |
2.182 |
8 |
97.9% |
≤4 |
–1.436 |
0.370 |
2.182 |
4 |
94.2% |
≤2 |
–1.436 |
0.370 |
2.182 |
2 |
86.8% |
Note: *the epidemiologic cut-off value.
Growth and time-killing curves and MIC of SH0165 in vitro and ex vivo
The logarithmic growth phase was determined to occur between 6 and 12 hours, as evaluated at OD630nm, shown in Figure 4. Compared with other bacteria like E. coli, Streptococcus and Pasteurella multocida, HPS required a longer time to reach its logarithmic growth phase. The time-killing curve of tildipirosin against SH0165 (Figure 5A) demonstrated that lower concentrations (≤ 2MIC) showed similar antimicrobial activity for HPS. The bacteriostatic efficiency gradually strengthened with increasing tildipirosin concentrations, when tildipirosin concentrations were higher than 2MIC. According to the characteristics of the killing-curve in vitro (Figure 5A), the activity of tildipirosin against HPS was identified as being concentration-dependent.
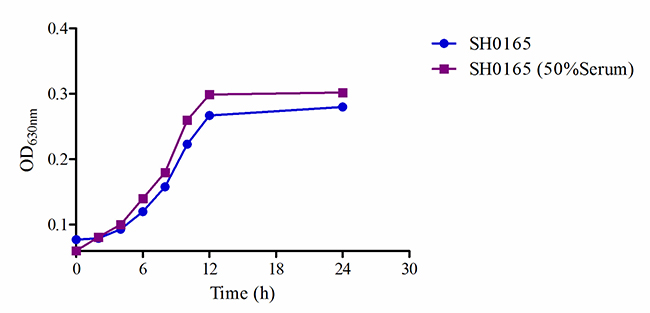
Figure 4: The growth-time curve of SH0165 in vitro and ex vivo.
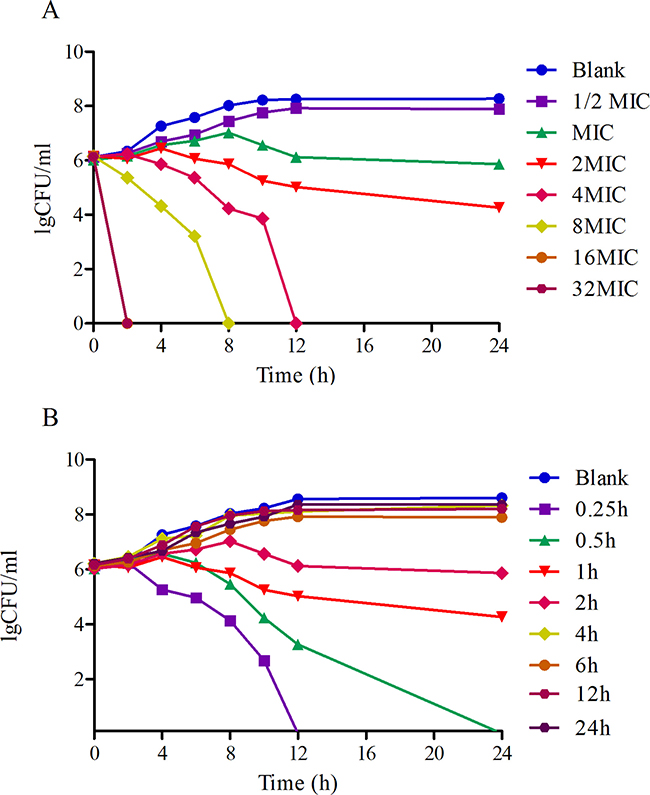
Figure 5: The Killing-time curves of tildipirosin against SH0165 in vitro (A) and ex vivo (B).
For ex vivo growth and time-kill curve, the 50% serum added into TSB was the highest limit for culturing HPS (SH0165). The serum drug concentration at 0.25 and 0.5 h (1.29 and 0.89 μg/ml) could eradicate bacterium completely (Figure 5B). This result was similar to the time-killing curve in vitro, and these results revealed that tildipirosin was a typically concentration-dependent drug both in vitro and ex vivo.
Validation of the high-performance liquid chromatography method
The calibration curves showed a high degree of linearity for tildipirosin in the range of 0.05–10 μg/ml for both the plasma and bronchoaveolar lavage (BAL) samples. The correlation coefficients (R2) for tildipirosin were determined to be 0.9989 and 0.9996 in the plasma and BAL samples, respectively. The lower limit of quantification (LLOQ) value of tildipirosin was 0.05 μg/ml in the plasma and BAL samples, which appeared to be obtained with sufficient precision and accuracy. The typical chromatograms of blank samples, samples at LLOQ and samples after i.m. administration are presented in Figure 6, in which good separation of tildipirosin could be observed. The accuracy and precision were within the tolerated limits for the (QCs), ranging from 0.05 to 10 μg/ml. The inter-day variation was determined to be in the range of 0.52–1.03% and 0.25–0.68% for the BAL and plasma samples, respectively. The recovery ratios were in the range of 86 ± 1.05% to 104 ± 0.92% in BAL and 84 ± 1.02% to 102 ± 0.53% in plasma, respectively. These results suggest that the accuracy, precision, recovery and stability tests met the requirements for quantitative determination in biological samples.
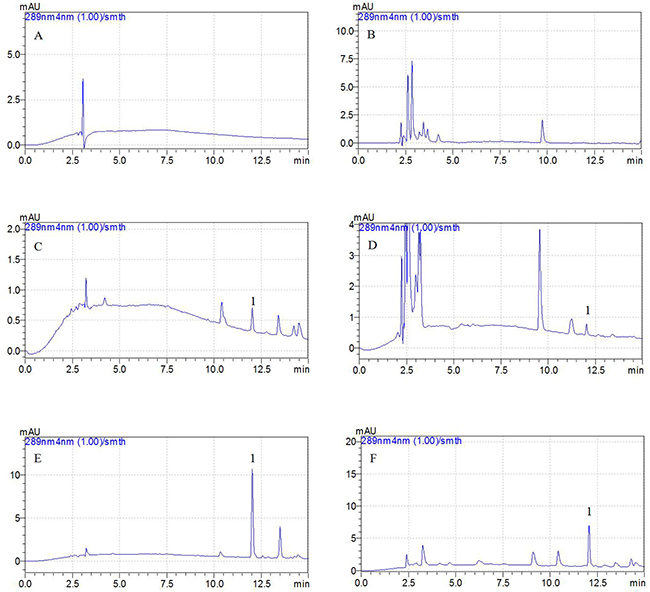
Figure 6: Representative HPLC chromatograms: A, blank plasma sample; B, blank BAL sample; C, plasma sample at the LLOQ of 0.01 μg/ml (5X concentration); D, BAL sample at the LLOQ of 0.05 μg/ml; E, plasma sample after i.m. administration of tildipirosin at the point of 15 min; F, BAL sample after i.m. administration of tildipirosin at the point of 1 h; 1, tildipirosin at the peak time of 12.2 min.
Comparison of pharmacokinetic characteristics of tildipirosin in plasma and pulmonary epithelial lining fluid samples
The mean PK parameters in plasma and PELF after i.m. administration of tildipirosin (4 mg/kg body weight) were summarised in Table 3, including the mean and SD for tildipirosin concentrations in plasma and PELF over time. The tildipirosin concentrations were plotted on a semi-logarithmic graph, presented in Figure 7A and B. No serious adverse effects were observed in pigs after i.m. administration of tildipirosin. While plasma concentrations were eliminated below the LLOQ after 48 hours, tildipirosin concentrations in PELF reached its peak at 5.33 hours, and remained at a high concentration until 408 hours, with a low elimination rate. The ratios of urea in BAL to serum (UreaBAL/UreaSerum) were determined between five and eight times with an automatic dry-type biochemical analyser. A non-compartment model and absorbing two – compartment open model were selected to analyse the drug concentration characteristics for plasma and PELF samples. The PK parameters of tildipirosin in plasma and PELF were calculated using WinNolin software. The results for the area under the curve within 24 h (AUC24h), the area under the curve (AUC), the time to peak concentration (Tmax), terminal half-life (T1/2) of tildipirosin, peak concentration (Cmax), relative total systemic clearance (CLb)and the mean residence time (MRT) in the plasma and PELF were shown in Table 3.
Table 3: Comparison pharmacokinetic parameters in plasma and PELF
Parameters |
Plasma |
PELF |
Ratio of PELF/Plasma |
|---|---|---|---|
AUC24h (μg*h/ml) |
4.25 ± 0.60 |
83.13 ± 11.26** |
19.56 |
AUC |
14.16 ± 2.12 |
855.46 ± 76.25** |
60.41 |
Tmax (h) |
- |
5.33 ± 2.37 |
- |
T1/2 (h) |
73.39 ± 6.62 |
170.91 ± 18.41** |
2.32 |
Cmax (μg/ml) |
1.01 ± 0.18 |
4.06 ± 0.65** |
4.02 |
CLb (L/h) |
0.283 ± 0.109 |
0.005 ± 0.001** |
56.6 |
MRTlast (h) |
93.24± 12.11 |
245.19 ± 28.61** |
2.63 |
Note: *represent statistical significance (p ≤ 0.05), **represent extreme significance (p ≤ 0.01). AUC24h, area under the curve within 24 h, AUC, the area under the curve, Tmax, the time to peak concentration, T1/2, the eliminate half-life, Cmax, the peak concentration, CLb, relative total systemic clearance, MRT, the mean residence time
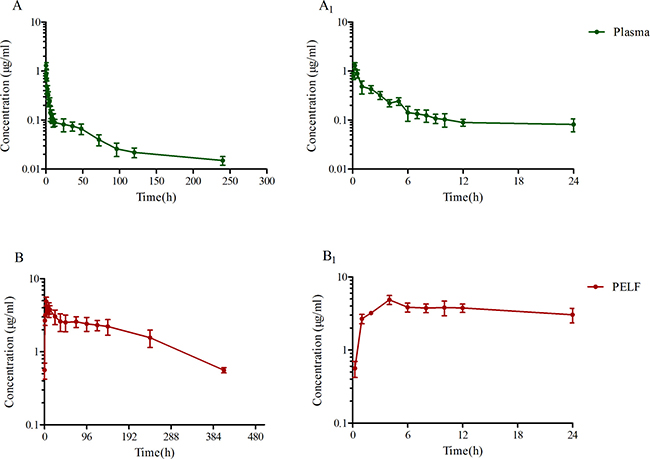
Figure 7: Tildipirosin concentration in porcine plasma (A), PELF (B) after i.m. administration at a dose of 4 mg/kg body weight.
The Cmax of tildipirosin in plasma and PELF were 1.01 and 4.06 μg/ml, respectively, with the Cmax for PELF determined to be four-fold higher than that in plasma. The T1/2 of tildipirosin in plasma (73.39 h) was much shorter than in PELF (170.91 h). However, the CLb in plasma (0.283 L/h) was much higher than that in PELF (0.005 L/h), suggesting that tildipirosin was released and eliminated slowly and remained high concentration in PELF. The AUC24h of PELF was 83.13 μg*h/ml, which was 19.56 folds higher than that in plasma (4.25 μg*h/ml). Significant differences in MRT, Clb, Cmax, AUC, AUC24h and T1/2 (p ≤ 0.01) were observed in plasma and PELF. Both pharmacokinetic parameters in PELF were higher than those in plasma apparently (Table 3).
PK/PD integration analysis
As a concentration-dependent antibiotic, the selected PK/PD parameters achieved from PK data in vivo combined with ex vivo MIC were showed in Table 3. The ratios of Cmax/MIC and AUC24h/MIC were 4.06 and 17.12 h, respectively, based on PK/PD data in plasma (Table 3). Ex vivo antibacterial activity of tildipirosin against HPS (SH0165) was determined in ileum content samples collected before and at 0, 0.5, 1, 2, 4, 6, 12, 24 h after i.m. administration. The relationship between antimicrobial efficacy and the ex vivo PK/PD parameter of AUC24h/MIC ratios were simulated by using the inhibitory sigmoid Emax model. The model parameters of the Hill coefficient N, E0, Emax and AUC24h/MIC values were shown for three levels of growth inhibition in the Table 4 and Figure 8. The values of AUC24h/MIC ratio needed for bacteriostatic activity (E = 0), bactericidal activity (E = –3), and bacterial elimination (E = –4) were 26.35, 52.27 and 73.29 h shown in Table 4. Thus, the PK/PD targets (AUC24h/MIC) for COPD analysis was 52.27h when it appeared bactericidal activity (E = –3).
Table 4: The main ex vivo parameters of PK/PD modeling of tildipirosin in plasma
Parameters |
Unites |
Mean ± SD |
|---|---|---|
AUC24h/MIC |
h |
17.12 ± 1.27 |
Cmax/MIC |
- |
4.06 ± 0.68 |
Emax |
LgCFU/ml |
2.48 ± 0.27 |
E0 |
LgCFU/ml |
-5.99 ± 0.34 |
Emax-E0 |
LgCFU/ml |
8.47 ± 0.98 |
EC50 |
h |
61.92 ± 6.12 |
N |
- |
1.96 ± 0.92 |
AUC24h/MIC for bacteriostatic (E = 0) |
h |
26.35 ± 2.32 |
AUC24h/MIC for bactericidal (E = –3) |
h |
52.27 ± 5.15 |
AUC24h/MIC for eradication (E = –4) |
h |
73.29 ± 6.45 |
Note: Emax, presented the Lg change in bacterial counts of blank sample, E0, presented the maximal antibacterial effect, EC50, presented the value to achieve 50% maximal antibacterial effect, N, presented the hill coefficient.
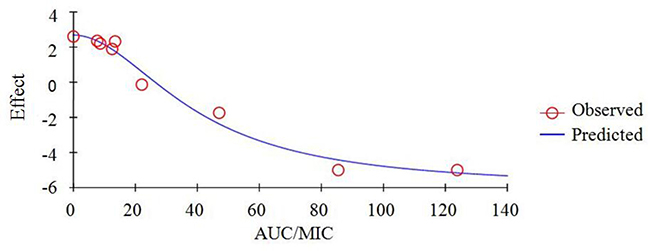
Figure 8: Plots of ex vivo AUC/MIC ratios versus the amount difference of tildipirosin against SH0165 within 24 h.
Estimation of doses
The predicted once daily doses were shown in Table 5 according to the AUC24h/MIC ratios and CLb for these three levels of antibacterial activity calculated from the PK/PD integrating model and the distribution of ex vivo MIC using Monte Carlo Simulations in Oracle Crystal Ball. The distribution of predicted population dose (AUC24h/MIC) values of tildipirosin curing HPS for 50% and 90% targets could be observed, respectively, in Figure 9. In this study, based on the dose equations, the predicted doses for bacteriostatic, bactericidal and elimination activity of tildipirosin against HPS over 24 h were 1.85, 3.67 and 5.16 mg/kg.bw for 50% target, respectively, and 2.07, 4.17 and 5.78 mg/kg.bw for 90% target, respectively in (Table 5).
Table 5: The predicted daily doses of tildipirosin curing HPS
Predicted doses (mg/kg.bw) |
Target ratios |
|
|---|---|---|
50% |
90% |
|
Bacteriostatic (E = 0) |
1.85 |
2.07 |
Bactericidal (E = –3) |
3.67 |
4.17 |
Eradication (E = –4) |
5.16 |
5.78 |
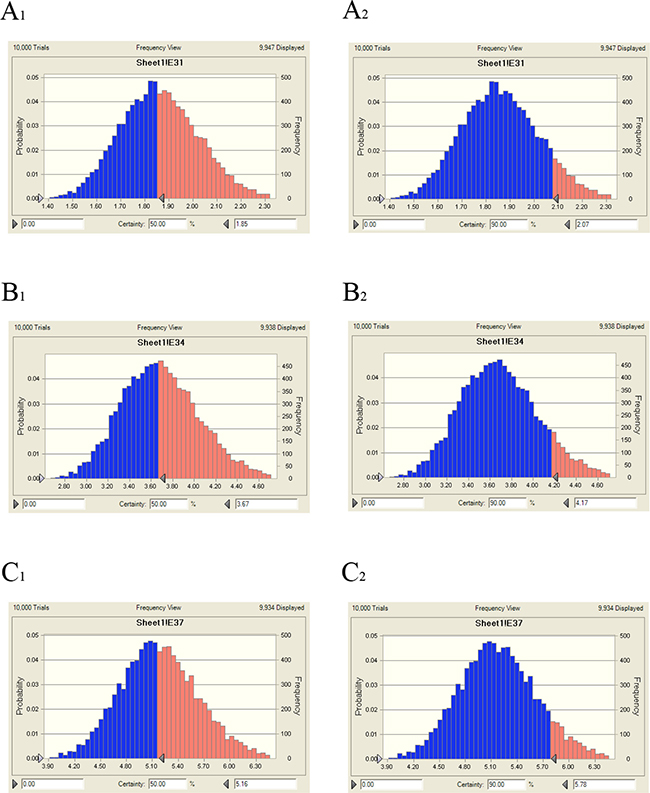
Figure 9: Distribution of predicted population doses (AUC24h/MIC) of tildipirosin against HPS (SH0165). (A1) presented the predicted population dose for bacteriostatic at 50% target, (A2) presented the predicted population dose for bacteriostatic at 90% target, (B1) presented the predicted population dose for bactericidal at 50% target, (B2) presented the predicted population dose for bactericidal at 90% target, (C1) presented the predicted population dose for elimination at 50% target, (C2) presented the predicted population dose for elimination at 90% target.
Monte Carlo simulation and pharmacodynamic cut-off
Using the ex vivo PD and PK data determined from plasma, 10,000 Monte Carlo simulations were run using Crystal Ball software. The cumulative PTA was determined for target “52.27h” (AUC24h/MIC) at different WT MICs in 50% serum of pigs, as presented in Table 6. The PTA was only 0.12% at an value of 0.125 μg/ml, but reached 96.54% when the MIC value was 0.0625 μg/ml. Consequently, a PTA ≥ 90% could be obtained for isolates with MIC ≤ 0.0625 μg/ml in pig serum (50%) after i.m. administration at a dose of 4 mg/kg body weight. Based on the predicted doses of tildipirosin against HPS for bactericidal (E = –3) and elimination activity (E = –4), the PTA were calculated to be 48.23% at the MIC value of 0.25 μg/ml but 100% at the MIC value of 0.125 μg/ml, and 0.07% at the MIC value of 0.5 μg/ml but 99.79% at the MIC value of 0.25 μg/ml (Table 6). Therefore, the COPD for tildipirosin against HPS would be 0.125 and 0.25 μg/ml (ex vivo) after i.m. administration at a dose of 4.17 and 5.78 mg/kg body weight. However, the predicted doses required to be verified in the clinical practice, and the detail PK data also needed to obtain in the pigs. Therefore, the COPD for tildipirosin against HPS (0.0625) μg/ml at the 50% serum of pigs (ex vivo) was finally selected to use after i.m. administration at a dose of 4 mg/kg. According to the ratio of MIC in vitro to ex vivo (8 times), the COPD for tildipirosin against HPS was 0.5 μg/ml determined in vitro (TSB).
Table 6: The AUC24/MIC values calculated with Monte Carlo simulation at the predicted doses (E = –3, and E = –4)
Doses (mg/kg) |
Effect |
MIC (μg/ml) |
|||||
|---|---|---|---|---|---|---|---|
0.03125 |
0.0625 |
0.125 |
0.25 |
0.5 |
1 |
||
4 |
- |
100% |
96.54%* |
0.12% |
0% |
0% |
0% |
4.17 |
Bactericidal (E = –3) |
100% |
100% |
100%* |
48.23% |
0% |
0% |
5.78 |
Elimination (E = –4) |
100% |
100% |
100% |
99.79%* |
0.07% |
0% |
Note: *represent the value of COPD breakpoint
DISCUSSION
In current study, the MICs of 164 HPS isolates were tested according to the recommendations of CLSI. The WT distribution of MICs of tildipirosin against HPS ranged from 0.032 to 16 μg/ml, however, one isolate had a MIC of 256 μg/ml, which had a wider scope than previously measured [9, 51]. The MIC90 (2 μg/ml) measured in this study was higher than that of determined by Zuprevo for certain strains (1 μg/ml), as detailed in the CVMP assessment report [4, 52, 51]. Wild-type isolates should not have acquired any resistance mechanisms, and therefore, this isolate should be removed [53, 54]. The high MIC value (256 μg/ml) may be explained by cross-resistance of macrolides, exposure to precursors of tildipirosin (tylosin and tilmicosin) or misuse of tildipirosin. The resistance mechanism of HPS to tildipirosin or other macrolides may be associated with the pathways of amino acid ATP-binding cassette (ABC) transporter system (HAPS_2069, HAPS_RS03630) and the metabolite transporter superfamily (HAPS_2067 and HAPS_2068, HAPS_RS08950) [49, 50, 55, 56], which will be a focus of future studies. Hence, all HPS isolates (163) except one (256 μg/ml) tested in this study could be considered as a WT isolates for ECV. The measured MIC in TSB or serum and the ratio of serum to TSB were compared. The MIC in serum (50%) and TSB of SH0165 were 0.25 and 2 μg/ml, and the ratio of serum to TSB (1:2) was the limit condition for HPS which was a fastidious bacteria. The MIC in TSB was 8 times higher than that in serum. This revealed a very strong serum effect on the potency of tildipirosin, as also had been found in the previously reported by Toutain and Godinho [20, 57, 58]. It was detected broth : serum MIC ratio (up to 16) in the presence of 40% bovine serum reported by Godinho [57], and a lower ratio (50) but in the 100% serum reported by Toutain [19, 20]. Thus, the selection for MIC measure in TSB or serum was important, and the serum effect should be also considered in science study.
The bacteriostatic characteristic of tildipirosin against HPS revealed a concentration dependence, which is similar to that of reported on tilmicosin, according to data obtained from a time-kill curve obtained in vitro, which is different from most other macrolides that can exhibit time dependence [3, 59]. Moreover, The MIC values and growth curves of SH0165 in TSB and serum showed no significant difference (Figure 4), and the time-killing curves in vitro and ex vivo showed that tildipirosin was bactericidal against HPS, with a concentration-dependent type (Figure 5). The 4MIC concentration of tildipirosin could completely eliminate HPS after 12 h. All of these results demonstrated that tildipirosin have a strong antibacterial activity against HPS in vitro and in the serum. The parameter (Tmax > MIC) is used to assess PK/PD for time-dependent antibacterial agents, but parameters AUC24/MIC and Cmax/MIC are used for concentration-dependent antibacterial agents. As a concentration-dependent antibacterial, this has been used as a clinical medication in pigs; AUC24h/MIC and Cmax/MIC are used to assess the relationship of PK/PD for tildipirosin in pigs.
The combination of HPLC with a tandem mass spectrometry has been previously used for the detection of tildipirosin. However, methods of extraction for tildipirosin from plasma and bronchial fluid with automated solid-phase extraction coupled are complex, inconvenience, inefficient and uneconomical [9, 51]. The current study reports a simplified HPLC method and extraction procedure. In this method, not many chemicals (acetonitrile, ammonium formate, methanoic acid, ethereal and dipotassium hydrogen phosphate solution) are required for the detection and extraction procedures. When developing the HPLC method for tildipirosin, we tested a different mobile phases, and found an efficient and easily accessible method with a simple composition 0.3% formic acid and acetonitrile) for HPLC analysis, with 200 μl dipotassium hydrogen phosphate solution (0.1 M) and 5 ml diethyl ether used for efficient extraction.
Similar to other macrolides (tulathromycin and tilmicosin), the concentration of tildipirosin in plasma was far below the MIC90 and ECV of WT isolates [60, 61]. As pathogens that target the respiratory system, HPS can attach to the bronchial epithelial cells, maintaining a high concentration in the extracellular fluid. Tildipirosin was found to be rapidly absorbed and extensively distributed to the site of infection. In general, macrolides are characterised by their rapid and extensive distribution, as well as their persistence in the PELF [7, 51]. In bronchial fluids (BF) obtained at post-mortem, the numbers of time points for the collected BF were equal to the numbers of animals required. [9] regarding to the previous reports it had been suggested that macrolides and ketolides accumulate in the inflammatory cells located in a region where the target pathogen causes infection. It is best to assess the clinical efficacy of macrolides at the site of infection [7]. According to previous studies, intrapulmonary pharmacokinetic examination had been performed by collecting the BAL from larger mammals using a sterilised catheter [7, 38, 43, 62]. However, the target tissue should be plasma but not PELF for the calculation of COPD for macrolides. Lung tissue was not the bio-phase for lung infected pathogens, and it had been accepted widely [21, 53, 54, 63]. HPS similar to pasteurella multocida was strictly extracellular pathogens, and the PELF was its main location for these extracellular pathogens. Although the drug concentration in PELF exceeded many times than that in plasma, it could be unable to maintain an effective local extracellular concentration in PLEF because of its extremely slow dynamic and release of drug in vivo. Moreover, the clinical relevance of PELF (the total tildipirosin concentrations) was only well understood by those working in a marketing department of a drug company but not by physio-pathologists [22]. At the same time, the high PELF drug concentration was caused by the lyses of cells (including high drug concentrations) during the broncho-alveolar lavage procedure when it was required to collect PELF. In this study, The Cmax of tildipirosin in plasma and PELF were 1.01 and 4.06 μg/ml, respectively, with the Cmax for PELF determined to be four-fold higher than that in plasma. The T1/2 of tildipirosin in plasma (73.39 h) was much shorter than in PELF (170.91 h). The CLb in plasma (0.283 L/h) was much higher than that in PELF (0.005 L/h), suggesting that tildipirosin was released and eliminated slowly and remained high concentration in PELF. These result revealed that the drug concentration in PELF released very slowly and had a feebly dynamic. And it could be unable to reflect a real and effective local extracellular concentration, as had been previously reported by others. Therefore, it was recommended to select PK data in plasma to study the PK/PD cutoff (COPD) for macrolides.
The mean plasma tildipirosin concentrations were above the MIC90 (0.25 μg/ml) in serum and COPD (0.0625 μg/ml in serum, 0.5 μg/ml in TSB) for HPS over a period of 4 h, predicted to remain high for a long period of time. The Cmax of the mean plasma concentration (1.01 μg/ml) in this study was similar to that (0.90 μg/ml) in previously reported by Rose [9]. A lower mean PELF concentration (4.912 μg/ml) than those in BF (6.47 μg/ml) was measured in this study, which were comparatively higher than values previously reported in lung tissue (4.253 μg/ml) [9]. In addition, T1/2 (170.91 h) in this study was higher than that (106 h) reported by Rose. These differences may be explained by the abrasion of epithelial cells, as tildipirosin in lung tissue is passed into the BF during BF collection at postmortem with mechanical separation, leading to substantially higher concentrations and overestimation of the BF concentrations and longer elimination half-life [9, 41]. The higher elimination half-life was also caused by the lyses of cells (including high drug concentrations) during the broncho-alveolar lavage procedure. The tildipirosin concentrations in the current study were determined from the PELF obtained from the live animals with no cell injury, and therefore, concentrations could be lower than that previously reported in the BF. However, our results provide a more precise and representative drug concentration response in the PELF.
As a kind of concentration-dependent action for tildipirosin, the parameters AUC24h/MIC was regarded as a threshold for the successful therapeutic outcome of a few marcolides [27, 49, 64]. However, these thresholds may be different for different marcolides. There were differences in the immune status of target animals and pathogens. The published AUC24h/MIC was 30 h for bactericidal action in PK/PD study of tilmicosin against HPS [3]. Therefore, it was of great importance to study the PK/PD indices of tildipirosin individually. In this study, the PD data were obtained from a serum to predict the dosage regimens since it was more clinically relevant than those from broth. The ratios of ex vivo AUC24h/MIC and Cmax/MIC were 17.12 h and 4.06, respectively (Table 4). The inhibitory sigmoidal Emax model was used for PK/PD integration model and dosage prediction, and it showed a favourable correlation (0.992) between the observed and predicted antibacterial efficacy of tildipirosin against HPS (Figure 8). The ex vivo AUC24h/MIC ratios of tildipirosin requiring bactericidal action and eradication of the SH0165 were 52.27 and 73.29 h, which was higher than in vivo AUC24h/MIC (17.12 h) achieved after intramuscular injection administration (4 mg/kg). These result suggest that the recommended dosage of 4 mg/kg could not guarantee clinical efficacy against infections associated with HPS with an MIC90 of 2 μg/ml. Based on the Monte Carlo simulations, the predicted daily dose for 50 and 90% targets to achieve bactericidal effect were 3.67 and 4.17 mg/kg, respectively. The Monte Carlo simulation to predict the dosage for a clinical use had the advantage of taking into account the PK/PD parameters based on bacteriological outcome, and it could set target percentage such as 90 and 50% for simulation models for all data in relation to incidence in pigs [49, 65, 66]. However, due to the animals’ immune system also being an important factor contributing to bacterial eradication, the bacterial endpoint in vivo conditions may differ from the predicted dosages ex vivo [67].
CONCLUSIONS
In order to summarize, tildipirosin demonstrated the fast absorption, rapid and extensive distribution in PELF, where respiratory tract pathogens are known to multiply and cause damage. The PK in PELF and plasma were compared in this study. According to the PK/PD evaluation in vivo and ex vivo, an observed COPD were calculated as 0.0625 μg/ml in serum and 0.5 μg/ml in TSB, and ECV was 8 μg/ml, respectively. The COPD suggested for breakpoint could be used to provide a better guidance and a greater clinical significance than ECV in the absence of clinical cut-off value. The combination of COPD with the PK/PD data obtained in vivo and ex vivo which o provide more significant results. According to the PK/PD parameters ex vivo, the single doses required to reach bacteriostatic, bactericidal, and eradication activity for 90% target were 2.07, 4.17 and 5.78 mg/kg, respectively. These result offers an alternative optimal dosage regimen (4.17 mg/kg for bactericidal and 5.78 mg/kg for eradication) and avoided the emergence of resistance for clinical veterinary use. However, further research is essential to achieve a more comprehensive insight into the PK/PD relationships of tildipirosin and these values are of great significance for the effective treatment of HPS infections, but it could also deserve to be validated in a clinical practice for evaluating the treatment effect of infected pigs in the future research.
MATERIALS AND METHODS
Bacterial isolates
A total of 164 HPS isolates were collected from Huazhong Agricultural University, specifically the National Reference Laboratory of Veterinary Drug Residues and State Key Laboratory of Agricultural Microbiology. These isolates had been isolated from pigs lung tissue samples obtained between 2014 and 2016 from 10 Chinese provinces, including Hubei, Anhui, Shandong and Henan, among others. The species of isolates was identified by polymerase chain reaction (PCR) with 16sRNA of HPS. Prior to testing the MIC, each isolate was subcultured at least three times in tryptic soy broth (TSB) and tryptic soy agar (TSA; Qingdao Hai Bo Biological Technology Co., Ltd., Shangdong, China) containing 5% newborn calf serum (Zhejiang Tianhang Biotechnology Co., Ltd., Zhejiang, China) and 10 μg/ml nicotinamide adenine dinucleotide (NAD; Qingdao Hope Bio-Technology Co., Ltd.). Tildipirosin was donated from Hubei Huisheng Biological Technology Company (Hubei, China).
Animals
Fourteen healthy crossbred (Doroc × Large White × Landrace) pigs, about 25–30 kg body weight, were purchased from the pig breeding farm of Huazhong Agricultural University. Two out of fourteen pigs were used in a preliminary experiment to establish the PK and high-performance liquid chromatography (HPLC) methods. The other pigs were used for the formal PK studies. Pigs were allowed to acclimatise for 7 days prior to the experiment. All animal studies were conducted in compliance with the guidelines for the Care and Use of Laboratory Animals of Hubei Provincial Laboratory Animal Public Service Center (permit number SYXK 2013-0044), and the protocol was approved by the Ethics Committee of Huazhong Agricultural University.
Antimicrobial susceptibility testing
Susceptibility determination of tildipirosin against HPS was performed using the agar dilution method in accordance with the CLSI recommendations in a previously described report [3]. Strains of HPS (2–4 μl, about 108 CFU/ml) were inoculated onto TSA agar plates containing newborn calf serum and nicotinamide adenine dinucleotide, with two-fold serial dilutions of tildipirosin (0.0625–32 μg/ml). The resistance of strains over 32 μg/ml were screened to expand the range of two-fold dilutions of tildipirosin. Plates of strains were incubated in the presence of CO2 for 48 hours at 37ºC. MICs were determined as the lowest drug concentrations that caused complete growth inhibition (100%). Escherichia coli (ATCC 25922) was used as the quality control (QC) strain to verify the results of the susceptibility testing.
Determination of wild-type or epidemiological cutoff values
The wild-type (WT) cutoff (COWT) value was defined for microorganisms that had not acquired resistance mechanisms against the target drug. The ECV was the population separate to drug-resistant isolates that had acquired or mutated resistant isolates [13, 28, 29]. The ECV were defined as the highest MIC for WT comprised at least 95% of each MIC distribution, according to the CLSI guidelines described in previous reports by Turnidge and Espinel-ingroff [28, 30–33]. The ECV was based on fit to a normal distribution at the lower end of the MIC range for obtaining reasonable MICs distribution, which was determined using Sigma-Stat software (version 3.5) (Systat Software Inc). The mean and standard deviation of the normal distribution was calculated for optimum non-linear least squares regression fitting of MICs, performed using GraphPad Prism (version 5.01) (GraphPad Software Inc, USA). The NORMINV and NORDIST functions in Microsoft Excel were performed to set the WT distribution cutoffs which were used to determine the MIC that captured at least 95% of that distribution [13, 34–36].
In vitro and ex vivo growth, time-kill curves and MIC of tildipirosin against SH0165
The SH0165 isolate was chosen to determine the growth curve, using the method of plates count in 10–1 to 10–5 dilution ratio, in the range of 30–300 bacteria. According to the MIC of tildipirosin against SH0165 in the WT population (2 μg/ml), TSA plates were prepared with different tildipirosin concentrations ranging from 1/4 to 32 MIC (2 μg/ml) described in the previous report by Pengzhang. From the bacteria-containing fluid, 100 μl was diluted with normal sterile saline (10–1 to 10–5 dilution ratio), then aliquots of the last four diluted samples were dropped onto the TSA plates at 0, 2, 4, 6, 8, 10, 12 and 24 hours of culture, which was incubated in an atmosphere containing CO2 for 48 hours at 37ºC.
TSB including 50% serum obtained from pigs was prepared as culture medium for ex vivo growth, time-kill curve and MIC. The methods of determination were similar to those in vitro described above using TSB (50% serum) instead of TSB. The bacteria (106 CFU/ml) were co-incubated with ileum content samples obtained from pigs at different point (0, 0.25, 1, 2, 4, 6, 12 and 24 h) after treated with 4 mg/kg tildipirosin by i.m administration. The ex vivo time-killing curve in vitro was fitted to a PD model with the hypothesis of a decrease in tildipirosin concentration based on incubation time with inhibitory sigmoid Emax model.
High-performance liquid chromatography to determine tildipirosin concentration
Quantitative analyses of tildipirosin by HPLC were performed for the first time in BAL and plasma. A C18 reverse-phase column (250 × 4.6 mm, i.d., 5 μm, Agilent, USA) was used for HPLC, which was performed with a 289 nm detection wavelength at 30ºC. The mobile phase consisted of 0.3% formic acid (phase A) and acetonitrile (phase B). Plasma (0.5 ml) and BAL (0.5 ml) samples were mixed with 200 μl dipotassium hydrogen phosphate solution (0.1 mol/L), then extracted twice with 5 ml diethyl ether. The supernatants were achieved by centrifugation, then evaporated to dryness under nitrogen at 45ºC, followed by resuspension in the mobile phase at concentrated 5 times volume (0.1 ml).
PK study design and bronchoaveolar lavage collection
For the formal test, 12 pigs were randomly divided into two groups. Another two pigs were used to provide BAL and plasma for the HPLC analysis. Prior to the experiment, blank BAL and plasma samples were collected from every pig. Tildipirosin was intramuscularly administrated to the six pigs in each group at a recommended single dose of 4 mg/kg [9]. In group A, 30–50 ml samples of BAL were collected at 0, 5 and 15 minutes, then 1, 2, 4, 6, 8, 10, 12, 24, 36, 48, 144, 244, and 408 hours after administration. In group B, 3 ml blood samples were obtained at 15 and 30 minutes, then 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 12, 24 hour, 1.5, 2, 4, 6, 8 and 10 days after administration. The dose administered was the recommended dosage for PK of animals in vivo [9].
The BAL was performed using a previously described method using an electronic fiber-optic bronchoscope (Kangmei GU-180VET, Shanghai Kang Medical Equipment Co., Ltd. China) inserted into the right middle lung lobe, in order to determine the concentration of tildipirosin [37–40]. Atropine (0.05 mg/kg), ketamine (5 mg/kg) and propofol (3 mg/kg) were administrated intramuscularly and intravenously 30 minutes before drug administration. At each time point, 50 ml of sterile saline was infused into the lobe then aspirated into a 50 ml centrifugal tube. The plasma and BAL samples were stored on ice, then centrifuged at approximately 3000 g for 10 minutes before storing at –80ºC until further analysis.
All animal studies were conducted in compliance with the guidelines for the Care and Use of Laboratory Animals of Hubei Provincial Laboratory Animal Public Service Center (permit number SYXK 2013-0044), and the protocol was approved by the Ethics Committee of Huazhong Agricultural University.
Determination of tildipirosin concentrations in pulmonary epithelial lining fluid
The urea dilution method was used to estimate the volume of PELF in the BAL fluid, as previously described method [17, 41–43]. The concentration of urea in plasma and BAL were determined by the urea glutamate dehydrogenase enzymatic method, measured using an automatic dry-type biochemical analyser (DRI-CHEM NX500iVC, FUJIFILM (China) Investment Co., Ltd.) at the National Reference Laboratory of Veterinary Drug Residues (Wuhan, China). The volume of PELF (VPELF) in BAL fluid was derived according to equation 1, and the concentration of tildipirosin in PELF (TDPELF) was derived according to equation 2:


VBAL is the volume of recovered BAL fluid, and TDBAL is the concentration of tildipirosin in the BAL fluid.
PK/PD integration analysis
The PK data were analysed using WinNonlin software (version 5.2.1)(Certara USA). Plasma and PELF concentration data was analysed using a non-compartment model and absorbing two-compartment open model with lower Akaike’s Information Criterion (AIC) values of 2.26 and 1.764, respectively.
Due to tildipirosin was concentration-dependent drug, the PK/PD indexes were AUC24h/MIC and Cmax/MIC. The AUC24h/MIC and Cmax/MIC were selected as the combined PK/PD parameters which were calculated in each dose of the time-killing curve. Inhibitory sigmoid Emax model was used to analyze the integration of AUC24h/MIC ratio in vitro and bacteria count change (CFU/ml) in ileum contents during 24 h incubation with WinNonlin software [44–46]. The model equation was described as follows equation 1.
E, presented effect of antimicrobial agent measured as log10 difference of bacterial number before and after 24 h incubation in vitro, E0 and Emax presented the changes in log10 difference between 0 to 24 h in the control samples and containing tildipirosin samples, EC50, the AUC24h/MIC value reached 50% of the Emax, C, presented the AUC24h/MIC ratio, N, presented the Hill coefficient.
Monte Carlo analysis and determination of pharmacodynamic cutoff value
A Monte Carlo simulation (MCS) with 10,000 iterations was conducted using Crystal Ball software (version 7.2.2) (Oracl USA) based on PK parameters and calculated PK/PD targets (AUC24h/MIC) when it appeared bactericidal action (E = –3) [3, 47, 48]. The area under the curve at 24 hours (AUC24h) was assumed to be log-normally distributed for the mean values and confidence intervals (CI). The COPD was defined as the MIC at which the probability of target attainment (PTA) reached up to 90%, according to the CLSI guidelines described in previous reports by Pengzhang and Turnidge J [3, 28].
Doses estimation
The following formula was used to estimate dosages in different magnitudes of efficiency (E = 0, no change in bacterial count, E = –1, 99.9% reduction in count, E = –3, 99.99% reduction) to deduce an optimal regimen.

AUC/MIC indicates the targeted end-point for optimal efficacy, MIC denotes the minimum inhibitory concentration, CL shows clearance per day, fu indicates the free fraction of the drug in plasma, ignoring minimal binding, and F denotes the bioavailability.
The daily dose was calculated by Monte Carlo Simulations in Oracle Ball (Oracle Corporation, Redwood Shores, CA, USA).
Statistical analysis
MIC90 was calculated by using SPSS software, and statistical analysis was performed with Student’s t-test and Bonferroni revision for comparing the parameters of each group. The p < 0.05 and p ≤ 0.01 was considered to indicate statistically significant and extremely significant. *p ≤ 0.05 and **p ≤ 0.01.
Abbreviations
HPS: Haemophilus parasuis; MIC: minimum inhibitory concentration; PD: pharmacodynamic; PK: pharmacokinetic; COPD: PK/PD cutoff; PELF: pulmonary epithelial lining fluid; ECVs: epidemiological cutoff values; PK/PD: pharmacokinetics-pharmacodynamics; TSB: tryptic soy broth; TSA: tryptic soy agar; HPLC: high-performance liquid chromatography; AUC24h: area under the curve at 24 hours; BAL: bronchoaveolar lavage; AUC: the area under the curve; Tmax: the time to peak concentration; T1/2: terminal half-life; Cmax: peak concentration: CLb: relative total systemic clearance; MRT: the mean residence time; PTA: the probability of target attainment; CFU: colony forming unit.
Author contributions
Experiment designation: Z.L., Q.H. and J.C. Experiment carry out: Z.L., Q.L. and B.Y. Manuscript writing: Z.L. Manuscript review and modification: J.C., S.A. and Q.H.
ACKNOWLEDGMENTS
This work was supported by the China Agricultural Research System (CARS-36).
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
1. Sun J, Xiao X, Huang RJ, Yang T, Chen Y, Fang X, Huang T, Zhou YF, Liu YH. In vitro Dynamic Pharmacokinetic/Pharmacodynamic (PK/PD) study and COPD of Marbofloxacin against Haemophilus parasuis. BMC veterinary research. 2015; 11:293.
2. Xiao X, Sun J, Chen Y, Huang RJ, Huang T, Qiao GG, Zhou YF, Liu YH. In vitro dynamic pharmacokinetic/pharmacodynamic(PK/PD) modeling and PK/PD cutoff of cefquinome against Haemophilus parasuis. BMC veterinary research. 2015; 11:33.
3. Zhang P, Hao H, Li J, Ahmad I, Cheng G, Chen D, Tao Y, Huang L, Wang Y, Dai M, Liu Z, Yuan Z. The Epidemiologic and Pharmacodynamic Cutoff Values of Tilmicosin against Haemophilus parasuis. Frontiers in microbiology. 2016; 7:385.
4. The summary of Zuprevo. https://www.drugs.com/vet/zuprevo-18.html.
5. Nightingale CH. Pharmacokinetics and pharmacodynamics of newer macrolides. The Pediatric infectious disease journal. 1997; 16:438–443.
6. Anadon A, Reeve-johnson L. Macrolide antibiotics, drug interactions and microsomal enzymes: implications for veterinary medicine. Research in veterinary science. 1999; 66:197–203.
7. Villarino N, Martin-Jimenez T. Pharmacokinetics of macrolides in foals. Journal of veterinary pharmacology and therapeutics. 2013; 36:1–13.
8. Menge M, Rose M, Bohland C, Zschiesche E, Kilp S, Metz W, Allan M, Ropke R, Nurnberger M. Pharmacokinetics of tildipirosin in bovine plasma, lung tissue, and bronchial fluid (from live, nonanesthetized cattle). Journal of veterinary pharmacology and therapeutics. 2012; 35:550–559.
9. Rose M, Menge M, Bohland C, Zschiesche E, Wilhelm C, Kilp S, Metz W, Allan M, Ropke R, Nurnberger M. Pharmacokinetics of tildipirosin in porcine plasma, lung tissue, and bronchial fluid and effects of test conditions on in vitro activity against reference strains and field isolates of Actinobacillus pleuropneumoniae. Journal of veterinary pharmacology and therapeutics. 2013; 36:140–153.
10. Bywater R, Silley P, Simjee S. Antimicrobial breakpoints-definitions and conflicting requirements. Veterinary microbiology. 2006; 118:158–159.
11. Schwarz S, Bottner A, Goossens L, Hafez HM, Hartmann K, Kaske M, Kehrenberg C, Kietzmann M, Klarmann D, Klein G, Krabisch P, Luhofer G, Richter A, et al. A proposal of clinical breakpoints for amoxicillin applicable to porcine respiratory tract pathogens. Veterinary microbiology. 2008; 126:178–188.
12. Maaland MG, Papich MG, Turnidge J, Guardabassi L. Pharmacodynamics of doxycycline and tetracycline against Staphylococcus pseudintermedius: proposal of canine-specific breakpoints for doxycycline. Journal of clinical microbiology. 2013; 51:3547–3554.
13. Espinel-Ingroff A, Diekema DJ, Fothergill A, Johnson E, Pelaez T, Pfaller MA, Rinaldi MG, Canton E, Turnidge J. Wild-type MIC distributions and epidemiological cutoff values for the triazoles and six Aspergillus spp. for the CLSI broth microdilution method (M38-A2 document). Journal of clinical microbiology. 2010; 48:3251–3257.
14. Espinel-Ingroff A, Canton E, Peman J, Martin-Mazuelo E. Comparison of anidulafungin MICs determined by the clinical and laboratory standards institute broth microdilution method (M27-A3 document) and Etest for Candida species isolates. Antimicrobial agents and chemotherapy. 2010; 54:1347–1350.
15. Barbour A, Scaglione F, Derendorf H. Class-dependent relevance of tissue distribution in the interpretation of anti-infective pharmacokinetic/pharmacodynamic indices. International journal of antimicrobial agents. 2010; 35:431–438.
16. Villarino N, Lesman S, Fielder A, Garcia-Tapia D, Cox S, Lucas M, Robinson J, Brown SA, Martin-Jimenez T. Pulmonary pharmacokinetics of tulathromycin in swine. Part I: Lung homogenate in healthy pigs and pigs challenged intratracheally with lipopolysaccharide of Escherichia coli. Journal of veterinary pharmacology and therapeutics. 2013; 36:329–339.
17. Conte JE Jr, Golden JA, McQuitty M, Kipps J, Lin ET, Zurlinden E. Effects of AIDS and gender on steady-state plasma and intrapulmonary ethionamide concentrations. Antimicrobial agents and chemotherapy. 2000; 44:1337–1341.
18. Mouton JW, Theuretzbacher U, Craig WA, Tulkens PM, Derendorf H, Cars O. Tissue concentrations: do we ever learn? Journal of Antimicrobial Chemotherapy. 2008; 61:235–237.
19. Toutain PL, Pelligand L, Potter T, Lacroix M, Illambas J, Lees P. Demonstration of applicability of PK/PD concepts to determine a dosage regimen for tulathromycin in the calf. Journal of Veterinary Pharmacology & Therapeutics. 2015; 38:13–14.
20. Toutain PL, Potter T, Pelligand L, Lacroix M, Illambas J, Lees P. Standard PK/PD concepts can be applied to determine a dosage regimen for a macrolide: the case of tulathromycin in the calf. Journal of Veterinary Pharmacology & Therapeutics. 2016; 40:16–27.
21. Villarino N, Garcia-Tapia D, Lesman S, Lucas M, Robinson J, Brown SA, Martin-Jimenez T. An acute reversible experimental model of pneumonia in pigs: time-related histological and clinical signs changes. Journal of Veterinary Pharmacology & Therapeutics. 2013; 36:241–247.
22. Kiem S, Schentag JJ. Interpretation of antibiotic concentration ratios measured in epithelial lining fluid. Antimicrobial Agents & Chemotherapy. 2008; 52:24–36.
23. Sungmin K, Schentag JJ. Interpretation of epithelial lining fluid concentrations of antibiotics against methicillin resistant Staphylococcus aureus. Infection & Chemotherapy. 2014; 46:219.
24. Burgess DS. Pharmacodynamic principles of antimicrobial therapy in the prevention of resistance. Chest. 1999; 115:19S–23S.
25. Drusano GL. Pharmacokinetics and Pharmacodynamics of Antimicrobials. Clinical Infectious Diseases An Official Publication of the Infectious Diseases Society of America. 2007; 45:S89.
26. Nielsen EI, Friberg LE. Pharmacokinetic-pharmacodynamic modeling of antibacterial drugs. Pharmacological Reviews. 2013; 65:1053–1090.
27. Yan L, Xie S, Chen D, Pan Y, Tao Y, Qu W, Liu Z, Yuan Z, Huang L. Pharmacokinetic and pharmacodynamic modeling of cyadox against Clostridium perfringens in swine. 2017; 7:4064.
28. Turnidge J, Paterson DL. Setting and revising antibacterial susceptibility breakpoints. Clinical microbiology reviews. 2007; 20:391–408. table of contents.
29. Pfaller MA, Andes D, Diekema DJ, Espinel-Ingroff A, Sheehan D, CLSI Subcommittee for Antifungal Susceptibility Testing. Wild-type MIC distributions, epidemiological cutoff values and species-specific clinical breakpoints for fluconazole and Candida: time for harmonization of CLSI and EUCAST broth microdilution methods. Drug resistance updates : reviews and commentaries in antimicrobial and anticancer chemotherapy. 2010; 13:180–195.
30. Pfaller MA, Diekema DJ, Ghannoum MA, Rex JH, Alexander BD, Andes D, Brown SD, Chaturvedi V, Espinel-Ingroff A, Fowler CL, Johnson EM, Knapp CC, Motyl MR, et al. Wild-type MIC distribution and epidemiological cutoff values for Aspergillus fumigatus and three triazoles as determined by the Clinical and Laboratory Standards Institute broth microdilution methods. Journal of clinical microbiology. 2009; 47:3142–3146.
31. Pfaller MA, Boyken L, Hollis RJ, Kroeger J, Messer SA, Tendolkar S, Jones RN, Turnidge J, Diekema DJ. Wild-type MIC distributions and epidemiological cutoff values for the echinocandins and Candida spp. Journal of clinical microbiology. 2010; 48:52–56.
32. Pfaller MA, Boyken L, Hollis RJ, Kroeger J, Messer SA, Tendolkar S, Diekema DJ. Wild-type minimum effective concentration distributions and epidemiologic cutoff values for caspofungin and Aspergillus spp. as determined by Clinical and Laboratory Standards Institute broth microdilution methods. Diagnostic microbiology and infectious disease. 2010; 67:56–60.
33. Pfaller MA, Andes D, Arendrup MC, Diekema DJ, Espinel-Ingroff A, Alexander BD, Brown SD, Chaturvedi V, Fowler CL, Ghannoum MA, Johnson EM, Knapp CC, Motyl MR, et al. Clinical breakpoints for voriconazole and Candida spp. revisited: review of microbiologic, molecular, pharmacodynamic, and clinical data as they pertain to the development of species-specific interpretive criteria. Diagnostic microbiology and infectious disease. 2011; 70:330–343.
34. Espinel-Ingroff A, Colombo AL, Cordoba S, Dufresne PJ, Fuller J, Ghannoum M, Gonzalez GM, Guarro J, Kidd SE, Meis JF, Melhem TM, Pelaez T, Pfaller MA, et al. International Evaluation of MIC Distributions and Epidemiological Cutoff Value (ECV) Definitions for Fusarium Species Identified by Molecular Methods for the CLSI Broth Microdilution Method. Antimicrobial agents and chemotherapy. 2016; 60:1079–1084.
35. Turnidge JD, Nimmo GR, Pearson J, Gottlieb T, Collignon PJ, Australian Group on Antimicrobial R. Epidemiology and outcomes for Staphylococcus aureus bacteraemia in Australian hospitals, 2005-06: report from the Australian Group on Antimicrobial Resistance. Communicable diseases intelligence quarterly report. 2007; 31:398–403.
36. Turnidge J, Bordash G. Statistical methods for establishing quality control ranges for antibacterial agents in Clinical and Laboratory Standards Institute susceptibility testing. Antimicrobial agents and chemotherapy. 2007; 51:2483–2488.
37. Yamazaki K, Ogura S, Ishizaka A, Oh-hara T, Nishimura M. Bronchoscopic microsampling method for measuring drug concentration in epithelial lining fluid. American journal of respiratory and critical care medicine. 2003; 168:1304–1307.
38. Poulsen KP, McGuirk SM. Respiratory disease of the bovine neonate. The Veterinary clinics of North America Food animal practice. 2009; 25:121–137.
39. Choi SH, Hong SB, Ko GB, Lee Y, Park HJ, Park SY, Moon SM, Cho OH, Park KH, Chong YP, Kim SH, Huh JW, Sung H, et al. Viral infection in patients with severe pneumonia requiring intensive care unit admission. American journal of respiratory and critical care medicine. 2012; 186:325–332.
40. Lee JY, Park HJ, Kim YK, Yu S, Chong YP, Kim SH, Sung H, Lee SO, Kim MN, Lim CM, Kim YS, Koh Y, Woo JH, Choi SH. Cellular profiles of bronchoalveolar lavage fluid and their prognostic significance for non-HIV-infected patients with Pneumocystis jirovecii pneumonia. Journal of clinical microbiology. 2015; 53:1310–1316.
41. Lei Z, Liu Q, Yang B, Khaliq H, Cao J, He Q. PK-PD Analysis of Marbofloxacin against Streptococcus suis in Pigs. Front Pharmacol. 2017; 8:856.
42. Giguere S, Huang R, Malinski TJ, Dorr PM, Tessman RK, Somerville BA. Disposition of gamithromycin in plasma, pulmonary epithelial lining fluid, bronchoalveolar cells, and lung tissue in cattle. American journal of veterinary research. 2011; 72:326–330.
43. Mzyk DA, Baynes RE, Messenger KM, Martinez M, Smith GW. Pharmacokinetics and distribution in interstitial and pulmonary epithelial lining fluid of danofloxacin in ruminant and preruminant calves. Journal of veterinary pharmacology and therapeutics. 2016; 40:179–191.
44. Aliabadi FS, Ali BH, Landoni MF, Lees P. Pharmacokinetics and PK-PD modelling of danofloxacin in camel serum and tissue cage fluids. Veterinary Journal. 2003; 165:104–118.
45. Aliabadi FS, Lees P. Pharmacokinetics and pharmacodynamics of danofloxacin in serum and tissue fluids of goats following intravenous and intramuscular administration. American journal of veterinary research. 2001; 62:1979.
46. Aliabadi FS, Lees P. Pharmacokinetics and pharmacokinetic/pharmacodynamic integration of marbofloxacin in calf serum, exudate and transudate. Journal of Veterinary Pharmacology & Therapeutics. 2002; 25:161–174.
47. Andes D, Anon J, Jacobs MR, Craig WA. Application of pharmacokinetics and pharmacodynamics to antimicrobial therapy of respiratory tract infections. Clinics in laboratory medicine. 2004; 24:477–502.
48. Andes D, Marchillo K, Conklin R, Krishna G, Ezzet F, Cacciapuoti A, Loebenberg D. Pharmacodynamics of a new triazole, posaconazole, in a murine model of disseminated candidiasis. Antimicrobial agents and chemotherapy. 2004; 48:137–142.
49. Lei Z, Liu Q, Yang B, Xiong J, Li K, Ahmed S, Hong L, Chen P, He Q, Cao J. Clinical Efficacy and Residue Depletion of 10% Enrofloxacin Enteric-Coated Granules in Pigs. Frontiers in pharmacology. 2017; 8:294.
50. Lei Z, Fu S, Yang B, Liu Q, Ahmed S, Xu L, Xiong J, Cao J, Qiu Y. Comparative transcriptional profiling of tildipirosin-resistant and sensitive Haemophilus parasuis. Sci Rep. 2017; 7:7517.
51. Torres F, Santamaria R, Jimenez M, Menjon R, Ibanez A, Collell M, Azlor O, Fraile L. Pharmacokinetics of tildipirosin in pig tonsils. Journal of veterinary pharmacology and therapeutics. 2016; 39:199–201.
52. The summary reports of Tildipirosin. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/veterinary/002009/WC500106579.pdf
53. Meletiadis J, Al-Saigh R, Velegraki A, Walsh TJ, Roilides E, Zerva L. Pharmacodynamic effects of simulated standard doses of antifungal drugs against Aspergillus species in a new in vitro pharmacokinetic/pharmacodynamic model. Antimicrobial agents and chemotherapy. 2012; 56:403–410.
54. Meletiadis J, Mavridou E, Melchers WJ, Mouton JW, Verweij PE. Epidemiological cutoff values for azoles and Aspergillus fumigatus based on a novel mathematical approach incorporating cyp51A sequence analysis. Antimicrobial agents and chemotherapy. 2012; 56:2524–2529.
55. Wang C, Chen F, Hu H, Li W, Wang Y, Chen P, Liu Y, Ku X, He Q, Chen H, Xue F. Gene expression profiling of Cecropin B-resistant Haemophilus parasuis. Journal of molecular microbiology and biotechnology. 2014; 24:120–129.
56. Liu Y, Chen P, Wang Y, Li W, Cheng S, Wang C, Zhang A, He Q. Transcriptional profiling of Haemophilus parasuis SH0165 response to tilmicosin. Microbial drug resistance. 2012; 18:604–615.
57. Godinho KS, Keane SG, Nanjiani IA, Benchaoui HA, Sunderland SJ, Jones MA, Weatherley AJ, Gootz TD, Rowan TG. Minimum inhibitory concentrations of tulathromycin against respiratory bacterial pathogens isolated from clinical cases in European cattle and swine and variability arising from changes in in vitro methodology. Veterinary Therapeutics Research in Applied Veterinary Medicine. 2005; 6:113.
58. Thomas V, Jong AD, Butty P, Felmingham D, Godinho K, Klein U. Antimicrobial susceptibility of respiratory tract pathogens isolated from diseased cattle and swine across Europe. 2009; 172:202–15.
59. Owens RC Jr, Ambrose PG. Antimicrobial stewardship and the role of pharmacokinetics-pharmacodynamics in the modern antibiotic era. Diagnostic microbiology and infectious disease. 2007; 57:77S–83S.
60. Benchaoui HA, Nowakowski M, Sherington J, Rowan TG, Sunderland SJ. Pharmacokinetics and lung tissue concentrations of tulathromycin in swine. Journal of veterinary pharmacology and therapeutics. 2004; 27:203–210.
61. Godinho KS. Susceptibility testing of tulathromycin: interpretative breakpoints and susceptibility of field isolates. Veterinary microbiology. 2008; 129:426–432.
62. Womble A, Giguere S, Lee EA. Pharmacokinetics of oral doxycycline and concentrations in body fluids and bronchoalveolar cells of foals. Journal of veterinary pharmacology and therapeutics. 2007; 30:187–193.
63. Villarino N, Lesman S, Fielder A, Garcíatapia D, Cox S, Lucas M, Robinson J, Brown SA, Martínjiménez T. Pulmonary pharmacokinetics of tulathromycin in swine. Part 2: Intra-airways compartments. Journal of Veterinary Pharmacology & Therapeutics. 2013; 36:340–349.
64. Lei Z, Cao J, He Q. Pharmacokinetic and Pharmacodynamic Evaluation of Marbofloxacin and PK/PD Modelling against E scherichia coli in Pigs. 2017; 8:542.
65. Dorey L, Pelligand L, Cheng Z, Lees P. Pharmacokinetic/pharmacodynamic integration and modelling of florfenicol for the pig pneumonia pathogens Actinobacillus pleuropneumoniae and Pasteurella multocida. Journal of Veterinary Pharmacology & Therapeutics. 2017; 12:e0177568.
66. Lei Z, Liu Q, Yang B, Ahmed S, Xiong J, Song T, Chen P, Cao J, He Q. Evaluation of Bioequivalence of Two Long-Acting 20% Oxytetracycline Formulations in Pigs. Front Vet Sci. 2017; 4:61.
67. Garrison KE, Pasas SA, Cooper JD, Davies MI. A review of membrane sampling from biological tissues with applications in pharmacokinetics, metabolism and pharmacodynamics. European Journal of Pharmaceutical Sciences Official Journal of the European Federation for Pharmaceutical Sciences. 2002; 17:1.