
INTRODUCTION
Neonatal diabetes mellitus (NDM) is rare and estimated incidence is about 1 in 90,000–260,000 live births [1–3]. NDM defined as the occurrence of diabetes in the first 6 months of life [4]. It can be divided into two clinical subtypes: permanent neonatal diabetes mellitus (PNDM) that requires continuous treatment since diagnosis, and transient neonatal diabetes mellitus (TNDM) that typically resolves after a few weeks to months, but relapsing around puberty after a period of remission [5].
For a long period, the cause of NDM was unknown. Insulin treatment is generally acutely required in most infants with newly diagnosed diabetes mellitus to treat or prevent ketoacidosis and dehydration [6]. However, insulin therapy presents a particular challenge in these very young children with respect to compliance, and precise dosage.
Recently, activating mutations in the Kir6.2 and sulfonylurea receptor 1 (SUR1) subunits of the pancreatic ATP sensitive KATP channel, coded for by the genes KCNJ11 and ABCC8, have been identified major causes of NDM [7, 8]. Based on this key breakthrough, sulfonylurea which is widely used to treat type 2 diabetes, is becoming a new treatment option for NDM.
Sulfonylurea binds specifically to the SUR1 subunit, closing the KATP channel via an ATP-independent mechanism and therefore increasing the insulin secretion from the β cells [9]. However, sulfonylureas are not approved for use in infants in most countries. All guidelines and recommendations have also not mentioned the sulfonylureas for NDM.
Though the studies about sulfonylureas for activating mutations NDM have increased rapidly in the last few years [10, 11], due to small sample sizes, these studies were not adequately powered to detect the effect of sulfonylureas in NDM.
Therefore, we performed this systematic review and meta-analysis to investigate the effect of sulfonylurea for NDM. Furthermore, we provide the latest and most convincing evidence for developing clinical practice guidelines of NDM by this meta-analysis.
RESULTS
Study identification and selection
Initially, 941 records were retrieved from the database search and 12 additional records identified through other sources. After removing duplicate articles, 432 records were eligible. Based on the inclusion and exclusion criteria, 404 articles were excluded after a simple reading of the titles and abstracts of the articles. The remaining 28 full-text articles were assessed for eligibility. Then, no sulfonylurea treatment, review, no available data, written in other language were excluded. Finally, a total of 10 studies were included in the meta-analysis. The selection process is shown in Figure 1.
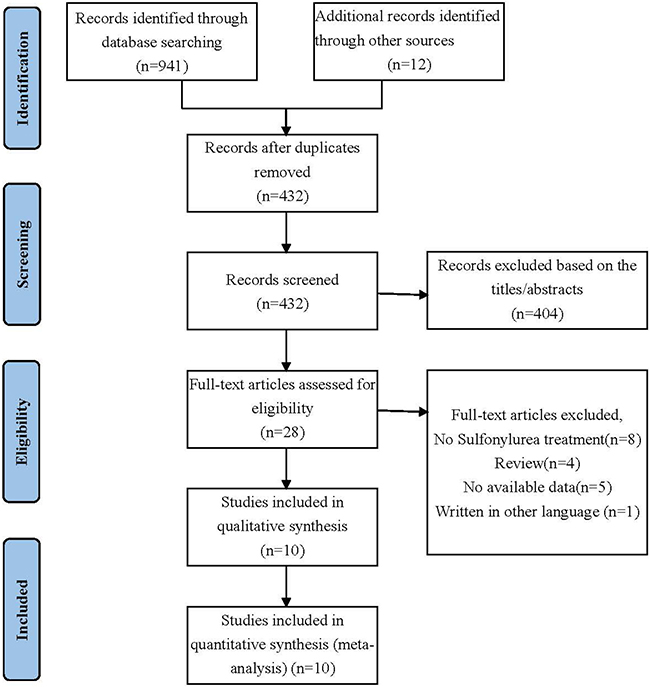
Figure 1: Selection process for the studies included in the meta-analysis.
Study characteristics
The main characteristics of the included studies are summarized in Table 1, and the outcome data of each included study are shown in Table 2. These studies were published from 2006 to 2016. The number of participants in the studies involving 285 participants ranged from 5 to 73. Six of 10 were cohort studies [9, 12–16], and 4 of 10 were cross-sectional studies [17–20].
Table 1: Search strategy
Source: PubMed; Searched on: Jan 5, 2017 |
||
|---|---|---|
Search |
Query |
Items found |
#11 |
Search #10 AND #3 |
395 |
#10 |
Search #6 AND #9 |
14766 |
#9 |
Search #7 OR #8 |
520111 |
#8 |
Search Diabetes [Title/Abstract] |
411384 |
#7 |
Search “Diabetes Mellitus” [Mesh] |
353111 |
#6 |
Search #4 OR #5 |
667779 |
#5 |
Search (neonatal [Title/Abstract]) OR Newborn [Title/Abstract] |
273607 |
#4 |
Search “Infant, Newborn” [Mesh] |
539228 |
#3 |
Search #1 OR #2 |
22050 |
#2 |
Search (((((((((glimepiride [Title/Abstract]) OR Acetohexamide [Title/Abstract]) OR Carbutamide [Title/Abstract]) OR Chlorpropamide [Title/Abstract]) OR Gliclazide[Title/Abstract]) OR Glipizide [Title/Abstract]) OR Glyburide [Title/Abstract]) OR Tolazamide [Title/Abstract]) OR Tolbutamide [Title/Abstract]) OR Sulfonylurea [Title/Abstract] |
13505 |
#1 |
Search “Sulfonylurea Compounds” [Mesh] |
17797 |
Source: Embase; Searched on: Jan 5, 2017 |
||
Search |
Query |
Items found |
#10 |
#3 AND #6 AND #9 |
556 |
#9 |
#7 OR #8 |
849821 |
#8 |
diabetes:ab,ti |
586257 |
#7 |
‘diabetes mellitus’/exp |
761547 |
#6 |
#4 OR #5 |
661321 |
#5 |
neonatal:ab,ti OR newborn:ab,ti |
322871 |
#4 |
‘newborn’/exp |
518403 |
#3 |
#1 OR #2 |
26280 |
#2 |
sulfonylurea:ab, ti OR glyburide:ab,ti OR glipizide:ab, ti OR gliclazide:ab, ti OR glimepiride:ab, ti OR acetohexamide:ab, ti OR carbutamide:ab, ti ORchlorpropamide:ab, ti OR tolazamide:ab, ti OR tolbutamide:ab, ti |
17822 |
#1 |
‘sulfonylurea’/exp |
11821 |
Table 2: Characteristics of included studies
Study |
Country |
Study design |
Participants (KCNJ11/ABCC8 mutant) |
Transfer sulfonylurea therapy |
Successful treatment |
Treatment regimen |
Treatment time |
Outcome indicators |
|---|---|---|---|---|---|---|---|---|
Ewan R. Pearson 2006 [17] |
UK |
cohort study |
49 |
49 |
44 |
glibenclamide |
12 weeks |
HbA1c |
Juraj Stanik 2007 [24] |
Slovakia |
cross-sectional study |
5 |
5 |
4 |
glibenclamide |
1 month; 6 months |
HbA1c, CGMS, C-peptide |
Meena Rafiq 2008 [18] |
UK |
cohort study |
27 |
27 |
23 |
glibenclamide |
HbA1c |
|
Jahnavi S 2013 [23] |
India |
cross-sectional study |
10 |
5 |
5 |
glibenclamide |
HbA1c, glucose tolerant |
|
David Carmody 2014 [21] |
USA |
cross-sectional study |
73 |
73 |
69 |
glibenclamide |
||
Brian W. Thurber 2015 [20] |
USA |
cohort study |
58 |
58 |
58 |
glibenclamide |
HbA1c |
|
Jacques Beltrand 2015 [16] |
France |
cohort study |
18 |
18 |
18 |
glibenclamide |
HbA1c, C-peptide |
|
Evgenia Globa 2015 [22] |
Ukraine |
cross-sectional study |
12 |
12 |
11 |
glibenclamide |
3 months; 1 year |
HbA1c |
Patricia Taberner 2016 [19] |
Argentina |
Wcohort study |
8 |
5 |
4 |
glibenclamide |
3 months |
HbA1c, C-peptide |
Yukiko Hashimoto 2016 [9] |
Japan |
cohort study |
25 |
17 |
14 |
glibenclamide |
HbA1c, C-peptide |
Risk of bias assessment
Risk of bias assessment of the included studies is summarized in Tables 3 and 4. Based on the Newcastle-Ottawa Scale (NOS) to assess the risk of bias of the cohort studies, 5 studies [9, 12, 13, 15, 16] were rated as a total score of 9 and one study [14] scored 8, indicating a low risk of bias. According to the Agency for Healthcare Research and Quality (AHRQ) items to assess the cross-sectional studies, all four studies [17–20] are categorized moderate quality.
Table 3: Outcome data of included studies
Study |
HbA1c |
Basal C-peptide, ng/mL |
||
|---|---|---|---|---|
Before treatment |
After treatment |
Before treatment |
After treatment |
|
Ewan R. Pearson 2006 [17] |
8.1 (7.7–8.6) |
6.4 (6.2–6.6) |
– |
– |
Juraj Stanik 2007 [24] |
10.0 ± 0.73 |
6.2 ± 0.37 |
0.04 ± 0.04 |
0.73 ± 0.07 |
Meena Rafiq 2008 [18] |
7.2 (6.6–8.2) |
5.5 (5.3–6.2) |
– |
– |
Jahnavi S 2013 [23] |
10.18 ± 2.6 |
6.84 ± 0.46 |
– |
– |
David Carmody 2014 [21] |
– |
– |
– |
– |
Brian W. Thurber 2015 [20] |
8.5 ± 1.8 |
6.2 ± 1.0 |
– |
– |
Jacques Beltrand 2015 [16] |
7.75 (5.5–12.8) |
6.4 (5.4–10) |
0.07 (0.02–0.51) |
0.28 (0.12–0.82) |
Evgenia Globa 2015 [22] |
7.4 (6.6–9.6) |
5.6 (5.4–5.9) |
– |
– |
Patricia Taberner 2016 [19] |
8.56 ± 0.56 |
5.80 ± 1.07 |
0.15 ± 0.10 |
1.29 ± 0.97 |
Yukiko Hashimoto 2016 [9] |
– |
6.4(4.9–8.5) |
– |
– |
Table 4: NOS quality assessment of included cohort studies
Items |
Study |
Ewan R. Pearson 2006 |
Meena Rafiq 2008 |
Brian W. Thurber 2015 |
Jacques Beltrand 2015 |
Patricia Taberner 2016 |
Yukiko Hashimoto 2016 |
|---|---|---|---|---|---|---|---|
Selection |
Representativeness of the exposed cohort |
★ |
★ |
★ |
★ |
★ |
★ |
Selection of the non-exposed cohort |
★ |
★ |
★ |
★ |
★ |
★ |
|
Ascertainment of exposure |
★ |
★ |
★ |
★ |
★ |
★ |
|
Demonstration that outcome of interest was not present at start of study |
★ |
★ |
★ |
★ |
★ |
★ |
|
Comparability |
Comparability of cohorts on the basis of the design or analysis |
★★ |
★★ |
★★ |
★★ |
★★ |
★★ |
Outcome |
Assessment of outcome |
★ |
★ |
★ |
★ |
★ |
★ |
Was follow-up long enough for outcomes to occur |
★ |
– |
★ |
★ |
★ |
★ |
|
Adequacy of follow up of cohorts |
★ |
★ |
★ |
★ |
★ |
★ |
|
Quality Scores |
9 |
8 |
9 |
9 |
9 |
9 |
|
Treatment success rate
In all studies, treatment success rate was varying from 80% to 100%. Low heterogeneity (I2=0.00, P = 0.362) was present among studies. The pooled estimated success rate by the random-effects model was 90.1% (95% CI: 85.1% –93.5%; Figure 2). It’s necessary to conduct subgroup analyses, due to different types of studies were eligible in this meta-analysis. For cohort studies, six studies enrolled 173 participants, and pooled estimated success rate by the random-effects model was 89.3% (95% CI: 81.3% –94.2%; Figure 3). In cross-sectional studies, four studies totaling 95 patients were included. Based on our analysis, the pooled estimate of success rate was 90.4%, and the 95% CI was 85.5% to 93.7%.
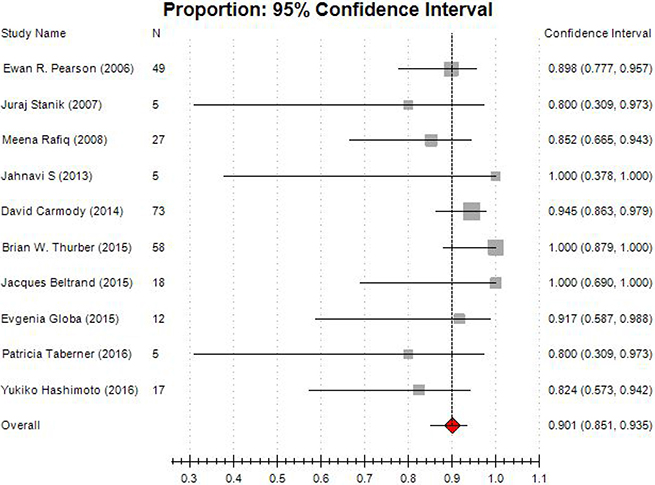
Figure 2: Forest plot of meta-analysis on treatment success rate.
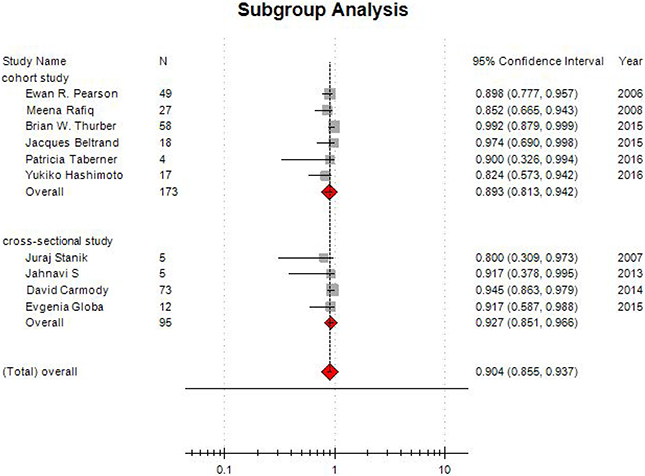
Figure 3: Funnel plot of subgroup analysis on treatment success rate.
HbA1c level
As a marker of chronic hyperglycemia, glycated hemoglobin (HbA1c) has now been used to diagnosis of diabetes and monitor glycemic control. The American Diabetes Association (ADA) and other major diabetes organizations also incorporated HbA1c into clinical practice guidelines, setting an HbA1c level of ≥ 6.5% (48 mmol/mol) as the cutoff value for the diabetes control [21, 22].
In this systematic review, nine studies involving 268 participants provided data on HbA1c level. Compared with before treatment, HbA1c level was obviously decreased when sulfonylurea was administrated for the subjects. The test for heterogeneity of 9 studies demonstrated no heterogeneity (P = 0.00; I2 = 8.21%), and the random-effects model was performed. The pooled estimate of mean deviation, (MD) was –2.289, and the 95% CI was –2.790 to –1.789 (P < 0.001) (Figure 4).
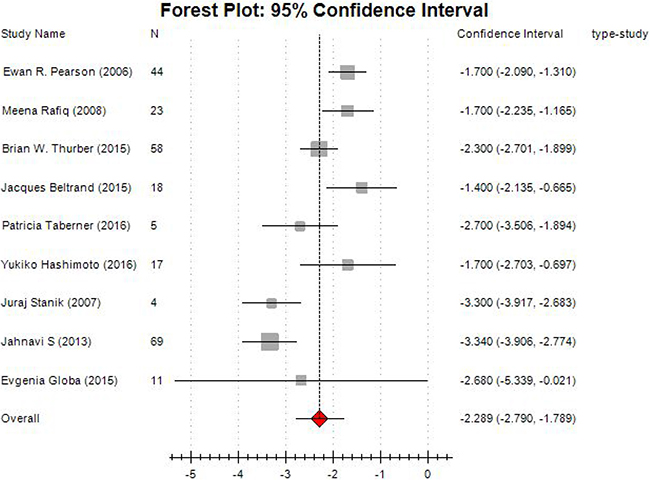
Figure 4: Forest plot of meta-analysis on changes of HbA1c level.
The results of subgroup analysis showed the combined MD in cohort studies was –1.919 (95% CI: –2.273~–1.565). For cross-sectional studies, the combined effect size was –3.306 (95% CI: –3.719 ~–2.894; Figure 5).
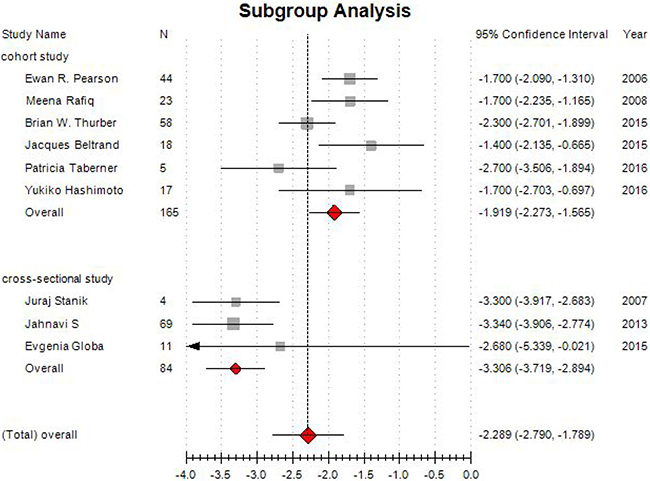
Figure 5: Forest plot of subgroup analysis on changes of HbA1c level.
The results suggested that sulfonylurea are effective when used in NDM with KATP-channel mutations.
C-peptide levels
C-peptide in plasma may be a better measure of portal insulin secretion than insulin itself. In this systematic review, only three studies [12, 15, 20] mentioned to this indicator. It is elevated significantly after sulfonylurea treatment in these studies.
Side effects
Two cohort studies [13, 14] and one cross-sectional study [20] reported adverse events. The most common side effect of sulfonylurea was the gastrointestinal reaction. In total, six patients had diarrhea, two associated with abdominal pain and one mild loss of appetite caused transitory weight loss. In addition, one patient had morning nausea, and one severe hypoglycemic episode was reported in a patient. All these side effects are transitory and resolved without discontinuing treatment.
Publication bias
For the meta-analysis of sulfonylurea on treatment success rate and changes of HbA1c level, there were no evidence of significant publication bias by inspection of the funnel plot (Figure 6 and Figure 7).
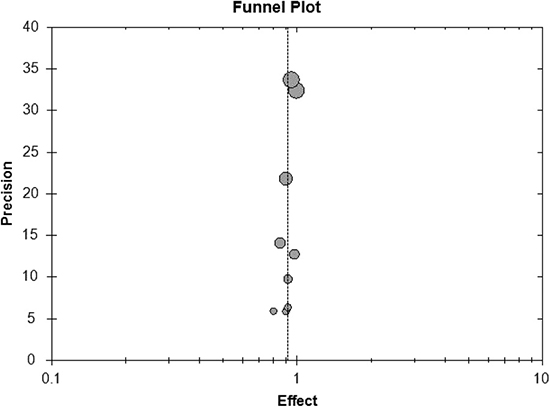
Figure 6: Funnel plot of meta-analysis on treatment success rate.
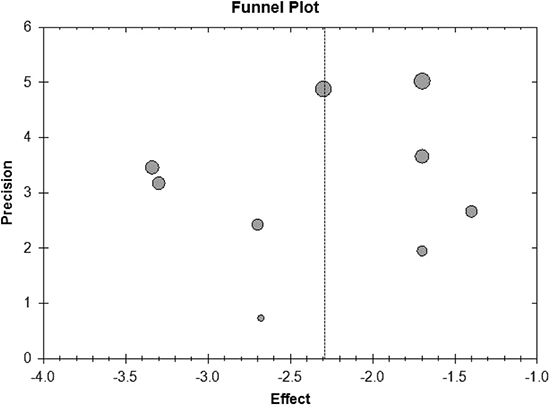
Figure 7: Funnel plot of meta-analysis on changes of HbA1c level.
DISCUSSION
Main findings
This systematic review and meta-analysis identified 6 cohort studies and 4 cross-sectional studies investigating the effect of sulfonylurea for the treatment of neonatal diabetes owing to KATP-channel mutations. The meta-analysis revealed that sulfonylurea has a highly successful rate for treatment NDM due to heterozygous mutations of the genes KCNJ11 andABCC8 encoding the two subunits (Kir6.2 and SUR1) of KATP channel. Moreover, the finding was consistent in subgroup analyses for both in cohort studies and in cross-sectional studies. Furthermore, in some studies, sulfonylurea therapy is also safe and successful in neonatal diabetes patients before genetic testing results [23]. It is might be KATP-channel mutations accounting for larger proportions of NDM. This implies that sulfonylurea might be used in all new diagnosed NDM; however, larger numbers of cases must be studied.
Blood glucose monitoring and adjustment of the treatment regimen is critically important in the management of diabetes. The way of conventional blood sugar monitoring is susceptible to short-term changes in diet, the presence of stress as well as other confounding factors [24]. In addition, determination of fasting plasma glucose has the poor compliance due to overnight fast. HbA1c could reflect average glycaemia over the past two to three months, owing to the lifespan of red blood cells is approximately 120 days [25]. Furthermore, advantages of HbA1c include the lack of participant preparation; high within-person reliability; and excellent standardization of the assay in most countries [26]. Besides, HbA1c is more reflective of macro-and microvascular complications than glucose [27]. Thus, HbA1c has become the gold standard for monitoring glycemic control in diabetes mellitus with the endorsement of influential diabetes societies and the World Health Organization.
In this systematic review, HbA1c had a significantly lower compared with before treatment. The pooled estimate of MD was –2.289, and the 95% CI was –2.790 to –1.789 (P < 0.001). The subgroup analysis showed a similar result for cohort studies and in cross-sectional studies.
In new diagnosed diabetic patients, it is vital to evaluate insulin secretion function of β cell. Also, residual insulin secretion has been proposed as a mean of classifying diabetes. However, insulin has a short half-life of a few minutes [28]. In addition, in patients with type I diabetes need to receive exogenous insulin, it also be difficult to estimate own insulin secretion by measuring insulin in serum.
Connecting peptide (C-peptide) is known for several decades. As a 31 amino acid segment, it is released in equimolar amounts together with insulin from the pancreatic beta cells [28]. Thus, C-peptide will reflect insulin secretion. Furthermore, C-peptide passes liver, has a longer half-life of half an hour, and is finally catabolized by the kidneys, and some is secreted in the urine [29]. Therefore, determination of C-peptide has been a common way of trying to standardize the evaluation of beta cell function. In this study, C-peptide level is obviously increased after sulfonylurea treatment in the three studies.
The common side effects are gastrointestinal reaction when sulfonylurea were used for NDM. In addition, nausea and hypoglycemic episode were also reported in a very small size of patient. As previously reported [30], all these side effects are transitory and resolved without discontinuing treatment. No other fatal side effects were reported.
These results indicated that sulfonylurea is a better choice for NDM with KATP-channel mutations.
Comparison with other studies
To the best of our knowledge, this meta-analysis is a first systematically and quantitatively evaluates the roles of sulfonylurea for NDM. However, all the included studies in this systematic review are observational study. Until now, there is no RCT studies to support its use. Further well-conducted trials that examine long-term outcomes are required.
Implications for clinical practice
Though sulfonylurea for treatment neonatal diabetes is supported by some researchers and clinicians, insulin treatment is still acutely required in most infants with newly diagnosed diabetes mellitus to treat or prevent ketoacidosis and dehydration. In addition, sulfonylureas are not approved for use in infants in most countries. All these explanations limit the use of sulfonylureas for NDM especially for KATP-channel mutations patients. Based on the results of our meta-analysis, sulfonylurea has a highly successful rate for treatment NDM and it also fulfill an evident glycemic control with HbA1c level significantly lower. Therefore, this meta-analysis provides the latest and most convincing references for developing clinical practice guidelines of NDM.
Strengths and limitations
There are several strengths for our meta-analysis. Firstly, this meta-analysis was in compliance with the PRISMA guidelines and the recommendations of the Cochrane Collaboration. Secondly, we conducted this meta-analysis by exhaustive search without any restrictions. In addition, we performed several subgroup analyses to explore the potential sources of heterogeneity and increase the robustness of this meta-analysis.
Several limitations should be taken into consideration when interpreting the present results. First of all, all the included studies in our meta-analysis were observational studies. Observational studies are highly subject to selection bias and confounding which can contribute to underestimates or overestimates of the actual effect of an intervention [31]. Second, other factors such as spontaneous recovery tendency, time factor, environmental change were also the potential bias resulting from all the comparisons are self-control. It is reported that younger age at the time of initiation of sulfonylureas therapy is correlated with lower required doses of sulfonylureas therapy, shorter transition time and decreased likelihood of requiring additional diabetes medications [16]. In this meta-analysis, we did not
Besides, the sample sizes in this meta-analysis were not large and unpublished studies were not included in the analysis.
CONCLUSIONS
The present systematic review and meta-analysis suggested that sulfonylurea had a highly successful rate for treatment NDM due to KATP channel mutations. Furthermore, sulfonylurea significantly decreased HbA1c level when compared with before treatment. In addition, sulfonylurea displayed sound safety except the mild gastrointestinal reaction.
MATERIALS AND METHODS
Selection criteria
Studies meeting the following criteria were included: (1) population: neonatal diabetes receiving sulfonylurea; (2) intervention: sulfonylurea with or without concurrent insulin; (3) comparison: insulin, before and latter intervention or non-intervention; (4) outcome: success rates of treatment, change of HbA1c and C-peptide; (5) design: all types of clinical studies (i.e., RCTs, cohort studies, case control studies, case series studies and case reports) which involved sulfonylurea for treatment neonatal diabetes were included.
Search strategy
Pubmed, Embase and the Cochrane Library, were searched for studies reporting the sulfonylurea on the treatment of neonatal diabetes. All the data were searched from inception of the database to Jan. 2017. Search terms included those related to neonatal diabetes, sulfonylurea, glibenclamide and their variants. The search strategy for Pubmed and Embase were shown in Table 5. No language restriction was imposed. The reference lists of all retrieved articles were also reviewed to identify additional articles missed by using these search terms. In addition, we also manually checked the bibliographies of previous reviews and included trials to identify other potentially eligible trials.
Table 5: AHRQ quality assessment of included cross-sectional studies
Study |
Juraj Stanik 2007 |
Jahnavi S 2013 |
David Carmody 2014 |
Evgenia Globa 2015 |
|
|---|---|---|---|---|---|
Items |
1 |
YES |
YES |
YES |
YES |
2 |
YES |
YES |
YES |
YES |
|
3 |
YES |
UNCLEAR |
UNCLEAR |
YES |
|
4 |
YES |
YES |
YES |
YES |
|
5 |
UNCLEAR |
UNCLEAR |
UNCLEAR |
UNCLEAR |
|
6 |
YES |
YES |
YES |
YES |
|
7 |
YES |
NO |
UNCLEAR |
UNCLEAR |
|
8 |
UNCLEAR |
UNCLEAR |
UNCLEAR |
UNCLEAR |
|
9 |
UNCLEAR |
UNCLEAR |
UNCLEAR |
UNCLEAR |
|
10 |
UNCLEAR |
YES |
YES |
YES |
|
11 |
YES |
NO |
UNCLEAR |
UNCLEAR |
|
Quality Scores |
7 |
5 |
5 |
6 |
|
Selection of studies and data extraction
Two authors (Zhang and Huang) independently carried out the initial search, deleted duplicate records, screened the titles and abstracts of every record. Full-text articles were obtained when information given in the title or abstracts either conformed to the selection criteria, or could not be ascertained owing to limited information. To include studies, data were extracted independently by the two authors (Zhang and Huang) and entered into a standardized Excel form. The following information was extracted from each study: first author, year of publication, country, study design, patient characteristics, number of patients enrolled, intervention, and outcome data. Any discrepancy was resolved by discussion and consensus.
Risk of bias assessment
Two reviewers (Huang and Zhong) independently evaluated the methodological quality of identified studies. Newcastle-Ottawa Scale (NOS) was used for cohort studies and case control studies [32]. The NOS is a nine-star rating system designed for non-randomized studies, especially case-control and cohort studies. It contains 3 domains and 8 items. A maximum of 2 stars can be allotted in the item of comparability. The other items get a single star if appropriate methods have been reported.
The methodological quality of the cross-sectional studies was assessed using an 11-item checklist which was recommended by Agency for Healthcare Research and Quality (AHRQ) [33]. An item would be scored ‘0’ if it was answered ‘NO’ or ‘UNCLEAR’; if it was answered ‘YES’, then the item scored ‘1’. Article quality was assessed as follows: low quality = 0–3; moderate quality = 4–7; high quality = 8–11.
Statistical method
Data were analyzed using the Open Meta-Analyst Beta 3.13 software (Tufts Medical Center, Boston, MA, USA). The indicators of rates such as success rate of treatment were analyzed by applying MetaAnalyst with the random-effects mode. For continuous outcome measurements, such as mean reduction value of HbA1c level and C-peptide, mean and standard deviation values (SD) were calculated and transformed if not given directly in the paper.
Heterogeneity among the included studies was evaluated by the I² test. A value greater than 50% to indicate substantial heterogeneity and sought the potential sources of heterogeneity (clinical heterogeneity and methodological heterogeneity) [34]. If the results of the studies could not combine using meta-analysis (due to significant clinical heterogeneity and unconventional methods used in the analysis of studies), they were just only presented individually.
Finally, publication bias was evaluated by using funnel plots.
Author contributions
Yue Qiu and Taotao Liu contributed to the study concept and design, data acquisition and interpretation, and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Hongliang Zhang and Chun Huang had full access to all of the data in the study and drafting and final approval of the manuscript.
Zhenguang Huang and XiaoBin Zhong contributed to the data acquisition, data analysis and interpretation, and revision and final approval of the manuscript.
ACKNOWLEDGMENTS AND FUNDING
This project was financially supported by Guangxi Zhuang Autonomous Region Health Department of Traditional Chinese Medicine Science and Technology projects, Guangxi Province, China (No. GZZJ13-17); the project of improving the basic ability of young teachers in colleges and universities in Guangxi (KY2016YB098) and Innovation Project of Guangxi Graduate Education (YCBZ2017043)
Dr. Hongliang Zhang is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
CONFLICTS OF INTEREST
The authors have reported no potential conflicts of interest exist with any companies/organizations whose products or services may be discussed in this article.
REFERENCES
1. Iafusco D, Massa O, Pasquino B, Colombo C, Iughetti L, Bizzarri C, Mammi C, Lo Presti D, Suprani T, Schiaffini R, Nichols CG, Russo L, Grasso V, et al. Minimal incidence of neonatal/infancy onset diabetes in Italy is 1:90,000 live births. Acta Diabetol. 2012; 49:405–8. https://doi.org/10.1007/s00592-011-0331-8.
2. Greeley SA, Tucker SE, Naylor RN, Bell GI, Philipson LH. Neonatal diabetes mellitus: a model for personalized medicine. Trends Endocrinol Metab. 2010; 21:464–72. https://doi.org/10.1016/j.tem.2010.03.004.
3. Slingerland AS, Shields BM, Flanagan SE, Bruining GJ, Noordam K, Gach A, Mlynarski W, Malecki MT, Hattersley AT, Ellard S. Referral rates for diagnostic testing support an incidence of permanent neonatal diabetes in three European countries of at least 1 in 260,000 live births. Diabetologia. 2009; 52:1683–5. https://doi.org/10.1007/s00125-009-1416-6.
4. Greeley SA, Tucker SE, Worrell HI, Skowron KB, Bell GI, Philipson LH. Update in neonatal diabetes. Curr Opin Endocrinol Diabetes Obes. 2010; 17:13–9. https://doi.org/10.1097/MED.0b013e328334f158.
5. Steck AK, Winter WE. Review on monogenic diabetes. Curr Opin Endocrinol Diabetes Obes. 2011; 18:252–8. https://doi.org/10.1097/MED.0b013e3283488275.
6. Rubio-Cabezas O, Ellard S. Diabetes mellitus in neonates and infants: genetic heterogeneity, clinical approach to diagnosis, and therapeutic options. Horm Res Paediatr. 2013; 80:137–46. https://doi.org/10.1159/000354219.
7. Babenko AP, Polak M, Cave H, Busiah K, Czernichow P, Scharfmann R, Bryan J, Aguilar-Bryan L, Vaxillaire M, Froguel P. Activating mutations in the ABCC8 gene in neonatal diabetes mellitus. N Engl J Med. 2006; 355:456–66. https://doi.org/10.1056/NEJMoa055068.
8. Gloyn AL, Pearson ER, Antcliff JF, Proks P, Bruining GJ, Slingerland AS, Howard N, Srinivasan S, Silva JM, Molnes J, Edghill EL, Frayling TM, Temple IK, et al. Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med. 2004; 350:1838–49. https://doi.org/10.1056/NEJMoa032922.
9. Hashimoto Y, Dateki S, Hirose M, Satomura K, Sawada H, Mizuno H, Sugihara S, Maruyama K, Urakami T, Sugawara H, Shirai K, Yorifuji T. Molecular and clinical features of KATP -channel neonatal diabetes mellitus in Japan. Pediatr Diabetes. 2016. https://doi.org/10.1111/pedi.12447.
10. Koster JC, Remedi MS, Dao C, Nichols CG. ATP and sulfonylurea sensitivity of mutant ATP-sensitive K+ channels in neonatal diabetes: implications for pharmacogenomic therapy. Diabetes. 2005; 54:2645–54.
11. Karges B, Schnur D, Ellard S, Kentrup H, Karges W. Effective treatment of diabetes caused by activating ABCC8/SUR1 mutation with glimepiride. Diabet Med. 2012; 29:692–3. https://doi.org/10.1111/j.1464-5491.2011.03487.x.
12. Beltrand J, Elie C, Busiah K, Fournier E, Boddaert N, Bahi-Buisson N, Vera M, Bui-Quoc E, Ingster-Moati I, Berdugo M, Simon A, Gozalo C, Djerada Z, et al. Sulfonylurea Therapy Benefits Neurological and Psychomotor Functions in Patients With Neonatal Diabetes Owing to Potassium Channel Mutations. Diabetes Care. 2015; 38:2033–41. https://doi.org/10.2337/dc15-0837.
13. Pearson ER, Flechtner I, Njolstad PR, Malecki MT, Flanagan SE, Larkin B, Ashcroft FM, Klimes I, Codner E, Iotova V, Slingerland AS, Shield J, Robert JJ, et al. Switching from insulin to oral sulfonylureas in patients with diabetes due to Kir6.2 mutations. N Engl J Med. 2006; 355:467–77. https://doi.org/10.1056/NEJMoa061759.
14. Rafiq M, Flanagan SE, Patch AM, Shields BM, Ellard S, Hattersley AT, Neonatal Diabetes International Collaborative G. Effective treatment with oral sulfonylureas in patients with diabetes due to sulfonylurea receptor 1 (SUR1) mutations. Diabetes Care. 2008; 31:204–9. https://doi.org/10.2337/dc07-1785.
15. Taberner P, Flanagan SE, Mackay DJ, Ellard S, Taverna MJ, Ferraro M. Clinical and genetic features of Argentinian children with diabetes-onset before 12months of age: Successful transfer from insulin to oral sulfonylurea. Diabetes Res Clin Pract. 2016; 117:104–10. https://doi.org/10.1016/j.diabres.2016.04.005.
16. Thurber BW, Carmody D, Tadie EC, Pastore AN, Dickens JT, Wroblewski KE, Naylor RN, Philipson LH, Greeley SA. Age at the time of sulfonylurea initiation influences treatment outcomes in KCNJ11-related neonatal diabetes. Diabetologia. 2015; 58:1430–5.
17. Carmody D, Bell CD, Hwang JL, Dickens JT, Sima DI, Felipe DL, Zimmer CA, Davis AO, Kotlyarevska K, Naylor RN. Sulfonylurea treatment before genetic testing in neonatal diabetes: pros and cons. J Clin Endocrinol Metab. 2014; 99:2709–14.
18. Globa E, Zelinska N, Mackay DJ, Temple KI, Houghton JA, Hattersley AT, Flanagan SE, Ellard S. Neonatal diabetes in Ukraine: incidence, genetics, clinical phenotype and treatment. J Pediatr Endocrinol Metab. 2015; 28:1279–86. https://doi.org/10.1515/jpem-2015-0170.
19. Jahnavi S, Poovazhagi V, Mohan V, Bodhini D, Raghupathy P, Amutha A, Suresh Kumar P, Adhikari P, Shriraam M, Kaur T, Das AK, Molnes J, Njolstad PR, et al. Clinical and molecular characterization of neonatal diabetes and monogenic syndromic diabetes in Asian Indian children. Clin Genet. 2013; 83:439–45. https://doi.org/10.1111/j.1399-0004.2012.01939.x.
20. Stanik J, Gasperikova D, Paskova M, Barak L, Javorkova J, Jancova E, Ciljakova M, Hlava P, Michalek J, Flanagan SE, Pearson E, Hattersley AT, Ellard S, et al. Prevalence of permanent neonatal diabetes in Slovakia and successful replacement of insulin with sulfonylurea therapy in KCNJ11 and ABCC8 mutation carriers. J Clin Endocrinol Metab. 2007; 92:1276–82. https://doi.org/10.1210/jc.2006-2490.
21. American Diabetes A. Standards of medical care in diabetes--2010. Diabetes Care. 2010; 33 Suppl 1: S11-61. https://doi.org/10.2337/dc10-S011.
22. Jia W. Standardising HbA1c-based diabetes diagnosis: opportunities and challenges. Expert Rev Mol Diagn. 2016; 16:343–55. https://doi.org/10.1586/14737159.2016.1133299.
23. Khurana D, Contreras M, Malhotra N, Bargman R. The diagnosis of neonatal diabetes in a mother at 25 years of age. Diabetes Care. 2012; 35: e59. https://doi.org/10.2337/dc11-2439.
24. Higgins T. HbA1c for screening and diagnosis of diabetes mellitus. Endocrine. 2013; 43:266–73. https://doi.org/10.1007/s12020-012-9768-y.
25. Phillips PJ. HbA1c and monitoring glycaemia. Aust Fam Physician. 2012; 41:37–40.
26. Parrinello CM, Selvin E. Beyond HbA1c and glucose: the role of nontraditional glycemic markers in diabetes diagnosis, prognosis, and management. Curr Diab Rep. 2014; 14: 548. https://doi.org/10.1007/s11892-014-0548-3.
27. Bejan-Angoulvant T, Cornu C, Archambault P, Tudrej B, Audier P, Brabant Y, Gueyffier F, Boussageon R. Is HbA1c a valid surrogate for macrovascular and microvascular complications in type 2 diabetes? Diabetes Metab. 2015; 41:195–201. https://doi.org/10.1016/j.diabet.2015.04.001.
28. Ludvigsson J. C-peptide in diabetes diagnosis and therapy. Front Biosci (Elite Ed). 2013; 5:214–23.
29. Zhu S, Larkin D, Lu S, Inouye C, Haataja L, Anjum A, Kennedy R, Castle D, Arvan P. Monitoring C-Peptide Storage and Secretion in Islet beta-Cells In Vitro and In Vivo. Diabetes. 2016; 65:699–709. https://doi.org/10.2337/db15-1264.
30. Codner E, Flanagan S, Ellard S, García H, Hattersley AT. High-dose glibenclamide can replace insulin therapy despite transitory diarrhea in early-onset diabetes caused by a novel R201L Kir6.2 mutation. Diabetes Care. 2005; 28: 758.
31. Starks H, Diehr P, Curtis JR. The challenge of selection bias and confounding in palliative care research. J Palliat Med. 2009; 12:181–7. https://doi.org/10.1089/jpm.2009.9672.
32. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
33. Hu J, Dong Y, Chen X, Liu Y, Ma D, Liu X, Zheng R, Mao X, Chen T, He W. Prevalence of suicide attempts among Chinese adolescents: A meta-analysis of cross-sectional studies. Compr Psychiatry. 2015; 61:78–89.
34. Zhang H, Huang Z, Zou X, Liu T. Bevacizumab and wound-healing complications: a systematic review and meta-analysis of randomized controlled trials. Oncotarget. 2016; 7:82473–81. https://doi.org/10.18632/oncotarget.12666.