
INTRODUCTION
Exact diagnosis and staging of primary prostate cancer is crucial for optimal treatment decisions. The differentiation between an indolent low-grade tumor (GS 6, 7a) which may allow conservative management such as active surveillance and an aggressive high-grade tumor (GS≥7b) [1–3] leading to prostatectomy, radio-/chemotherapy or androgen-deprivation is essential for the patient’s quality of life and prognosis. Epstein and Montironi showed that GS 7 is misleading, as GS7b tumors have a much worse prognosis than GS7a tumors and should be considered differently for treatment and prognostic purposes [2].
Morphological imaging techniques, e.g. transrectal ultrasound, computed tomography and magnetic resonance imaging, have limited accuracy in the diagnosis of primary prostate cancer [4, 5]. Imaging is the preferred base for sampling biopsies to minimize undetected lesions leading to under treatment [6–9], and over diagnosis resulting in overtreatment of low risk lesions [10].
Molecular imaging with specific tracers should improve diagnostic accuracy. Some studies report a high sensitivity of PET/CT with radioactive labeled choline derivatives for the detection of primary prostate cancer lesions by focally increased choline uptake [11–14]. But although choline PET/CT is widely used, other studies report low sensitivity and specificity, particularly at low PSA levels and high GS [15–19]. The major factors which compromise the diagnostic accuracy of choline PET/CT for primary prostate cancer are the tumor configuration, especially the detection of small carcinoma, and the differentiation of prostatitis, benign prostatic hyperplasia or high-grade intraepithelial neoplasia [4, 5, 13, 20, 21].
Prostate-specific membrane antigen (PSMA) is a transmembrane protein which is significantly overexpressed in prostate carcinoma cells, and its expression increases with tumor aggressiveness [4, 5, 13, 20, 21], metastatic disease and recurrence while normal prostatic tissue expresses PSMA sparsely [22–24]. PSMA PET/CT and multiparametric magnetic resonance imaging (mpMRI) correlated well with regard to tumor allocation in patients with a high pretest probability for large tumors [25]. Preliminary results of 37 patients with recurrent prostate cancer and rising PSA levels (background ratio between 18.8 and 28.3) indicated that the labeling of PSMA ligand with 68Ga could detect relapses and metastases of prostate carcinoma with high contrast compared to normal tissue [23].
Afshar-Oromieh et al. (2014) used an 68Ga-labeled HBED-CC conjugate of the PSMA-specific pharmacophore Glu-NH-CO-NH-Lys (“68Ga-PSMA-11”), and detected at least one lesion characteristic for prostate cancer in 86.5% of patients, but only in 26 of 37 (70.3%) patients with 18FEC PET/CT. In patients with PSA values ≤2.82 ng/ml at least one lesion characteristic of prostate cancer was identified in 68.8% of patients with 68Ga-PSMA-11 PET/CT, but only in 43.8% of patients with 18FEC PET/CT. All lesions detected by 18FEC PET/CT were also seen in 68Ga-PSMA-11 PET/CT [19].
Despite positive results for recurrent prostate cancer the availability of data for the primary diagnosis is poor. Therefore, the aim of this study was the evaluation of the diagnostic performance of68Ga-PSMA-11 PET/CT for detection of primary prostate cancer in patients with increased PSA levels and comparison of the results to 18FEC PET/CT. The intent of this study is to improve the diagnostic precision of prostate cancer detection in patients with increased PSA by use of 68Ga-PSMA-11 PET/CT with subsequent imaging guided biopsy. Furthermore, we have demonstrated that this approach may be able to predict the histological aggressiveness of the underlying tumor.
RESULTS
68Ga-PSMA-11 PET/CT was conducted in 25 patients with a mean age of 67.0 ± 8.1 years and a basic PSA of 20.4 ± 33.50 ng/ml. Another 40 patients, who underwent 18FEC PET/CT, were aged 69.4 ± 7.7 years and had a mean basic PSA of 55.0 ± 56.9 ng/ml (Table 1).
Table 1: Characteristics of patients with suspected prostate cancer
Test |
68Ga-PSMA-11 PET/CT |
18FEC PET/CT |
||
|---|---|---|---|---|
n |
(mean ± SD) |
n |
(mean ± SD) |
|
Age (years) |
25 |
67.0 ± 8.1 |
40 |
69.4 ± 7.7 |
PSA (ng/ml) |
25 |
20.4 ± 33.5 |
40 |
55.0 ± 56.9 |
SUVmax prostate |
25 |
12.1 ± 13.9 |
40 |
6.3 ± 6.4 |
Patients with metastases |
7 |
|
15 |
|
Patients without metastases |
18 |
|
25 |
|
SUVmax positive lymph nodes |
4 |
16.9 ± 12.5 |
13 |
11.0 ± 11.5 |
SUVmax bone metastases |
4 |
24.8 ± 25.9 |
8 |
7.7 ± 7.7 |
SUVmax lung metastases |
1 |
2.9 |
1 |
- |
Perineural invasion |
8 |
|
10 |
|
SD, standard deviation.
The 68Ga-PSMA PET/CT scans showed prostatic lesions with accumulation of the radiotracer above SUVmax 2.5 in 21/25 patients (84%), which related to lesions with GS≥6 (low-grade and high-grade carcinoma). The mean prostatic SUVmax was 12.1 ± 13.9 (1.5-56.0) in the whole group and 12.1 ± 14.7 (1.5-38.7) in 18 patients without metastases. In the group of 18FEC PET/CT scans such lesions (SUVmax >2.5, GS≥6) were seen in 38/40 patients (95%) and the mean prostatic SUVmax accounted for 6.3 ± 6.4 in the whole group and 5.8 ± 2.8 (2.4-14.5) in 25 patients without metastases. In 68Ga-PSMA PET/CT, but not in 18FEC PET/CT, there was a tendency towards increasing SUVmax with rising PSA as shown in Figure 1 for patients without metastases (68Ga-PSMA PET/CT: R 0.42, p = 0.082; 18FEC PET/CT: R 0.033; p = 0.875).
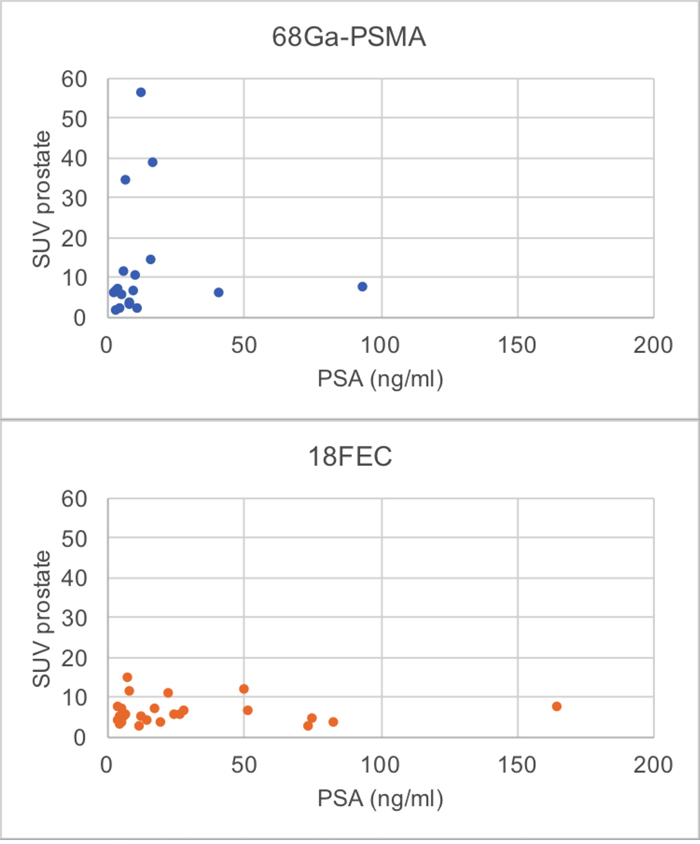
Figure 1: Relation between PSA and prostatic SUVmax of 68Ga-PSMA-11 PET/CT and 18FEC PET/CT in patients without metastases (68Ga-PSMA PET/CT: R 0.42, p= 0.082; 18FEC PET/CT: R 0.033; p = 0.875).
After histopathologic examination of biopsies and application of the GS, 8% of patients in the 68Ga-PSMA PET/CT group had non-malignancy-relevant (GS<6), 16% low-grade (GS 6, 7a) and 76% high-grade (GS≥7b) lesions. The corresponding distribution in the 18FEC PET/CT-group was 10%, 20%, and 70%, respectively (Table 2). Rising SUVmax values were associated with rising GS categories in both 68Ga-PSMA PET/CT (R 0.642, p = 0.005) and 18FEC PET/CT (R 0.404, p = 0.009).
Table 2: Distribution of GS in two groups of patients with 68Ga-PSMA PET/CT or 18FEC PET/CT using different SUVmax cut off-levels
68Ga-PSMA (n = 25) |
Gleason Score |
|||||
|---|---|---|---|---|---|---|
|
<6 |
6 |
7a |
7b |
8 |
9 |
|
Non- malignancy- relevant |
Low-grade carcinoma |
High-grade carcinoma |
|||
SUV ≤2.5 |
2 |
1 |
1 |
0 |
0 |
0 |
SUV >2.5 |
0 |
1 |
1 |
9 |
4 |
6 |
Total |
2 |
2 |
2 |
9 |
4 |
6 |
SUV ≤5.4 |
2 |
2 |
2 |
2 |
1 |
0 |
SUV >5.4 |
0 |
0 |
0 |
7 |
3 |
6 |
Total |
2 |
2 |
2 |
9 |
4 |
6 |
18FEC (n = 40) |
Gleason Score |
|||||
|---|---|---|---|---|---|---|
|
<6 |
6 |
7a |
7b |
8 |
9 |
|
Non- malignancy- relevant |
Low-grade carcinoma |
High-grade carcinoma |
|||
SUV ≤2.5 |
1 |
0 |
0 |
0 |
1 |
0 |
SUV >2.5 |
3 |
3 |
5 |
7 |
6 |
14 |
Total |
4 |
3 |
5 |
7 |
7 |
14 |
SUV ≤6.5 |
4 |
2 |
5 |
2 |
4 |
5 |
SUV >6.5 |
0 |
1 |
0 |
5 |
3 |
9 |
Total |
4 |
3 |
5 |
7 |
7 |
14 |
As shown in Figure 2 the two histopathologic non-malignancy-relevant lesions (GS<6) in the 68Ga-PSMA PET/CT group had SUVmax≤2.5 and the SUVmax means of all histopathologic high-grade categories (GS≥7b) continuously increased starting from SUVmax values above 12.0, whereas in the 18FEC PET/CT group the SUVmax means remained stable across all GS categories.
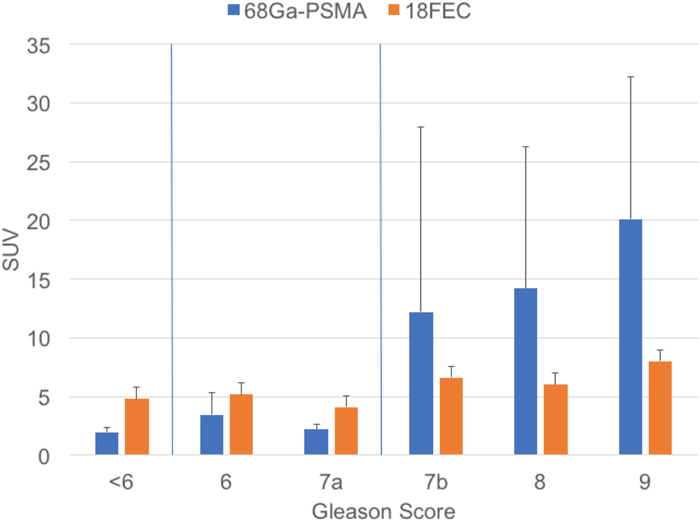
Figure 2: Distribution between GS and SUVmaxin 68Ga-PSMA PET/CT scans and 18FEC PET/CT scans for prostate cancer.
Using an SUVmax of 2.5 as the cut off-level between not-malignancy-relevant and malignant lesions (GS<6 vs. GS≥6) 68Ga-PSMA PET/CT revealed no false malignant and 2/23 false non-malignancy-relevant (8.7%) results indicating a sensitivity of 91%, a specificity of 100% and a NPV of 50%. With regard to the distinction between low-grade (GS≤7a) and high-grade carcinoma (GS≥7b) the sensitivity was 100%, the specificity 67% and the NPV 100%.
Using ROC analysis SUVmax 5.4 was found to be an optimal cut off-level to distinguish between low- and high-grade carcinoma by means of 68Ga-PSMA PET/CT (AUC = 0.9692; 95% CI 0.9086; 1.0000; SD(AUC) = 0.0309) (Figure 3). Applying this split-point analysis the specificity increased to 100% while the sensitivity was 84%, which resulted in an efficiency (= sum of all correct diagnoses) of 88% and a NPV of 67% (p<0.001) (Table 3).
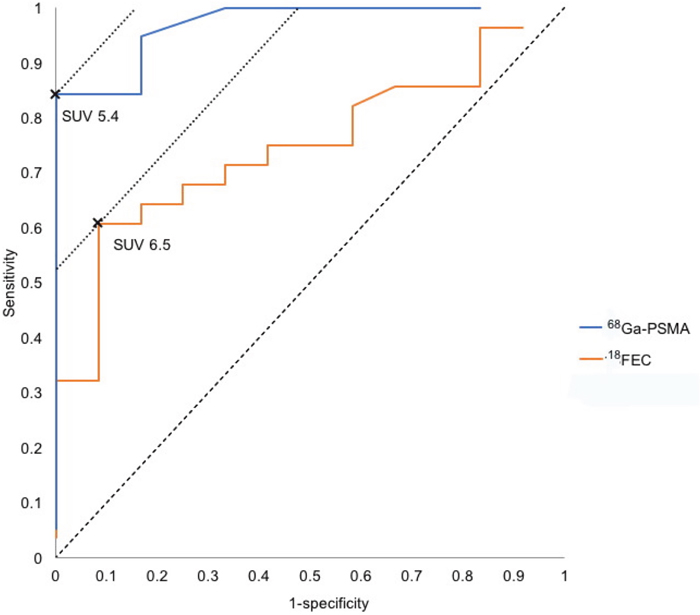
Figure 3: ROC curve according to the SUVmax values of our patients.
Table 3: Test parameters for 68Ga-PSMA PET/CT and 18FEC PET/CT
|
GS<6 vs. ≥6 |
GS≤7a vs. ≥7b |
GS≤7a vs. ≥7b |
|||
|---|---|---|---|---|---|---|
68Ga-PSMA |
18FEC |
68Ga-PSMA |
18FEC |
68Ga-PSMA |
18FEC |
|
Sensitivity |
91% |
97% |
100% |
96% |
84% |
61% |
Specificity |
100% |
25% |
67% |
8% |
100% |
92% |
NPV |
50% |
50% |
100% |
50% |
67% |
50% |
PPV |
100% |
92% |
90% |
71% |
100% |
94% |
Efficiency |
92% |
90% |
92% |
70% |
88% |
70% |
*68Ga-PSMA PET/CT SUVmax 5.4, 18FEC PET/CT SUVmax 6.5.
In comparison, at a chosen split-point of SUVmax 2.5 the sensitivity and specificity of 18FEC PET/CT was 97% and 25% for all malignant lesions (GS≥6) and 96% and 8% for the separation between GS≤7a vs. ≥7b. The ROC analysis revealed a SUVmax 6.5 as an optimal cut off-level (AUC = 0.7470; 95% CI 0.5919; 0.9020; SD(AUC) = 0.07910) (Figure 3) with a sensitivity of 61% and a specificity of 92%; but the efficiency was only 70% and the NPV 50% (p=0.01) (Table 3).
In 7 patients 68Ga-PSMA PET/CT showed metastases in lymph nodes (n = 4), bones (n = 4) and/or lung (n = 1). Also biopsy results demonstrated perineural invasion in 8 of 25 patients, which was associated with PET-positive nodal metastases in 2 patients, but with no metastases in 6 patients.
The 18FEC scans showed metastases in 15 patients, mainly in the lymph nodes (n = 13) and bones (n = 8). A lung metastasis was found in one patient. In 10 patients the biopsy results revealed perineural invasion, which was associated with nodal metastases in five cases. Another 5 patients had a perineural invasion without metastases.
DISCUSSION
In this study, we present the results from two groups of patients with increased PSA plasma levels undergoing 68Ga-PSMA-11 PET/CT (n = 25) or 18FEC PET/CT (n = 40) and imaging guided biopsy to detect significant cancer of the prostate.
18FEC PET/CT has been in widespread use for the diagnosis of prostate carcinoma [19], but in many malignant lesions the choline metabolism is not increased while most prostate carcinomas overexpress PSMA [19]. By labeling of PSMA ligands with 68Ga, relapses and metastases of prostate carcinoma with high contrast compared to normal tissues can be detected [23]. Therefore, 68Ga-PSMA PET/CT might also be superior to 18FEC PET/CT in the detection of primary prostate cancer.
In two groups of patients with elevated PSA levels, scheduled for biopsy, we analyzed 68Ga-PSMA-11 PET/CT-scans of 25 patients with an increased PSA and compared the results to 18FEC PET/CT scans of another 40 patients. Prostatic lesions with radiotracer uptake above SUVmax 2.5 were seen in 21/25 patients (84%) with 68Ga-PSMA-11 PET/CT scans and in 38/40 patients (95%) with 18FEC PET/CT. In the patient group with and without metastases both 68Ga-PSMA-11 PET/CT scans and 18FEC PET/CT scans showed no tendency towards increasing SUVmax with rising PSA. However in the patient group without metastases 68Ga-PSMA PET/CT, but not 18FEC PET/CT, showed a tendency towards increasing SUVmax with rising PSA (68Ga-PSMA PET/CT: R 0.42, p = 0.082; 18FEC PET/CT: R 0.033; p = 0.875).
Choosing an SUVmax of 2.5 as cut off-level between histologically confirmed non-malignancy-relevant and malignant lesions (GS<6/≥6), 68Ga-PSMA-11 PET/CT detected 2/2 cases (100%) as correct benign, but 18FEC PET/CT only 1/4 (25%). False negative 68Ga-PSMA-11 PET/CT scans (not used in our study) may occur if a prostate tumor is poorly differentiated and displays neuroendocrine aberrations [23, 26]. The specificity of 100% for 68Ga-PSMA-11 PET/CT and of 25% for 18FEC PET/CT for differentiating between non-malignancy-relevant and malignancy-relevant lesions (GS<6/≥6) observed here, has to be interpreted with caution because of the low rate of benign results in both groups. Our study was conducted in patients with a high probability of malignancy due to an increased PSA which is regarded as a marker for progressive disease because there is a strong association between PSA-level and positive68Ga-PSMA-11 PET/CT scans [27] but not with 18FEC PET/CT [12]. Studies including a higher proportion of patients with benign prostate alterations are needed to verify the results.
In contrast, the calculation of sensitivity and other prognostic parameters did not show major differences between both radio tracer methods using a cut off-level of 2.5. 68Ga-PSMA-11 PET/CT detected 21/23 cases (91%) and 18FEC PET/CT 35/36 (97%) correctly identified malignancy (GS≥6) (Table 3). However, for discrimination between high-grade and low-grade carcinoma (GS≤7a/GS≥7b), 68Ga-PSMA-11 PET/CT was superior to 18FEC PET/CT.
In our study we distinguished between non-malignancy-relevant (GS<6) and malignant (GS≥6) and between low-grade carcinoma (GS≤7a) and high-grade carcinoma (GS≥7b). The latter for the reason, that several studies showed significantly worse prognosis with regard to prostate cancer with GS≥7b [27].
With regard to prognosis and the choice of treatment individual risk stratification is of great importance. Afshar-Oromieh et al. (2015) found no correlation between 68Ga-PSMA PET/CT-results and GS [27] in spite of such correlation having been described in the literature [28–31]. They explained this by their low number of patients with a GS 5–6 which might have caused substantial variability in the statistical analysis. In our study we observed a possible correlation between GS and the SUVmax values measured by 68Ga-PSMA PET/CT: The two histopathologic non-malignancy-relevant lesions (GS<6) had PSMA-SUVmax ≤2.5 and all histopathologic high-grade lesions (GS≥7b) showed PSMA-SUVmax >2.5. Starting from GS 7b the mean SUVmax increased with rising GS category, while the SUVmax means of 18FEC PET/CT scans did not vary between different GS categories. Statistical analysis revealed a correlation between SUVmax and GS for both methods (68Ga-PSMA PET/CT R 0.642, p = 0.005; 18FEC PET/CT R 0.404, p = 0.009). However the sensitivity for distinction between GS≤7a/≥7b by means of 68Ga-PSMA-11 PET/CT vs. 18FEC PET/CT at a cut off-level of SUVmax 2.5 was 100% vs. 96%, the specificity 67% vs. 8%, NPV 100% vs. 50% and PPV 90% vs. 71%. This means that only 68Ga-PSMA-11 PET/CT was able to correctly predict an aggressive prostate cancer.
Assuming that a greater amount of prostate tissue is altered in higher GS categories this difference might be due to a higher specificity of the radiolabeled 68Ga-PSMA for cancer cells than 18FEC. Because of the high affinity of PSMA to prostate cancer cells every lesion with an accumulation of PSMA should be regarded as prostate cancer or prostate cancer metastasis until proven otherwise [27]. This means that a significant focal increase of PSMA metabolism might be predictive for a high GS, i.e. an aggressive cancer.
Our data showed that ROC analysis indicated an optimal cut off-level of SUVmax 5.4 for 68Ga-PSMA-11 PET/CT, which increased the specificity and PPV for separating GS≤7a/≥7b up to 100% but slightly decreased sensitivity to 84% and NPV to 67%. Using the calculated optimal cut off-level of SUVmax 6.5 for 18FEC PET/CT all prognostic parameters were less favorable than for 68Ga-PSMA-11 PET/CT.
Fendler et al. (2016) evaluated the accuracy of 68Ga-PSMA-11 PET/CT to localize cancer in the prostate and surrounding tissue. They found a statistically higher SUVmax in histopathologically positive segments (11.8 ± 7.6) compared to negative segments (4.9 ± 2.9; p<0.001). ROC revealed an optimal SUVmax cut off-value of 6.5 for discrimination between positive/negative segments [32], i.e. the results were concordant with our data. Fendler et al. concluded that 68Ga-PSMA-11 PET/CT accurately detects location and extent of primary prostate cancer and might be a promising tool for noninvasive tumor characterization and biopsy guidance [32]. Koerber et al. observed a significantly higher mean SUVmax in tumors with higher d’Amico risk classification and GS from biopsy (p<0.001 for grouped analyses) [33]. Giesel et al. published that based on the eight-segment resolution of biopsy, mpMRI and PSMA PET/CT presented identical tumor allocations [25]. MpMRI combined with ultrasound fusion guided biopsy of the prostate is a widely accepted method for T-Staging. However, no statistical significance could be shown regarding the differentiation between high- and low-grade carcinomas in a recently published study by our group [34].
High PSA values, T2b-T3 stage, poor tumor differentiation and perineural invasion are associated with high risk of nodal metastases [35, 36]. Measurement of PSA alone is not helpful in predicting lymph node metastases [37]. With regard to the therapeutic strategy, T-staging determines local surgery and radiotherapy while the pretreatment nodal status defines the extent of pelvic lymph node dissection or radiotherapy [38, 39]. PSMA PET/CT may provide valuable information in planning for focal radiation to the dominant lesions [40], because of its ability to detect even small lymph metastases, primarily due to a high radiotracer uptake [19].
In our study 68Ga-PSMA-11 PET/CT revealed metastases in 7/25 patients (28%) and 18FEC PET/CT in 15/40 patients (37.5%), mainly in lymph nodes and bone. In 4 patients positive lymph nodes, in 4 patients bone metastases and in 1 patient a lung metastasis were demonstrated by 68Ga-PSMA-11 PET/CT. Whereas by 18FEC PET/CT, 13 patients showed positive lymph nodes, 8 patients bone metastases and 1 patient a lung metastasis. A perineural invasion was seen in 8 patients (biopsy results according to 68Ga-PSMA-11 PET/CT) and in 10 patients (biopsy results according to 18FEC PET/CT), respectively. But a perineural invasion was associated with nodal metastases in only 2 of 8 (68Ga-PSMA-11 PET/CT) and 5 of 10 patients (18FEC PET/CT).
It is assumed that 68Ga-PSMA-11 PET/CT reveals the highest contrast in lymph node metastases, followed by bone metastases, local relapses and soft tissue metastases [27]. 68Ga-PSMA-11 PET/CT allows the detection of bone and organ metastases – due to low background signal [19] – which may lead to systemic therapy, but if excluded may lead to curative therapy [41]. 18F-PSMA agents are an attractive alternative to 68Ga-PSMA compounds. 18F-PSMA can be produced in larger amounts per batch in PET radiopharmaceuticals with an on-site cyclotron. Additionally, the average lower positron range of 18F reduces blurring effects leading to a higher spatial resolution and the longer half-life of 18F (110 min.) in comparison to 68Ga (67 min.) optimizes the production and distribution of 18F [42].
MATERIALS AND METHODS
Patients
In this retrospective study we included 61 consecutive patients from the Central Military Hospital Koblenz and 4 consecutive patients from the Practice of Radiology and Nuclear Medicine Cologne Triangle with suspected prostate carcinoma due to an elevated PSA (≥4.0, depending on age). Patients with a history of specific cancer pretreatment, surgical intervention, or inconspicuous PSA plasma levels were excluded. In 25 patients we conducted a 68Ga-PSMA-11 PET/CT (7/2015 – 08/2016) and in another 40 patients an 18FEC PET/CT (2/2010 – 7/2015). In all patients, prostate cancer was verified histologically with transrectal ultrasound (TRUS)-guided biopsy, and the GS results of TRUS biopsy served as reference for the PET findings. Detailed information on patient characteristics is shown in Table 1. Biopsy specimens were histopathologically evaluated based on the Gleason System on ISUP criteria 2014 and stratified by categorization into low-grade (GS≤3+4 = 7a) and high-grade malignancies (GS≥4+3 = 7b), respectively [43].
Our study was in accordance with the Helsinki Declaration and with our national legislation (German Medicinal Products Act, AMG § 13 Abs. 2b), and all patients gave their written informed consent. The retrospective study was approved by the ethics committee (Landesärztekammer Rheinland-Pfalz).
PET/CT imaging protocols
PET/CT acquisition was performed on a Biograph 64 TruePoint (True V HD) PET/CT scanner (Siemens, Erlangen, Germany) for the Koblenz patient group and on a Gemini GXL 16 (Philips, Eindhoven, NL) for the Cologne patient group.
68Ga-PSMA-11 PET/CT was performed about 60 min. (whole body) after intravenous injection of 68Ga-PSMA-11 (median 176 MBq, range 157-268 MBq). 68Ga-PSMA-11 was obtained from the Department of Nuclear Medicine of the University of Mainz and from Advanced Accelerator Applications Bonn.
18FEC PET/CT was performed about 60 min. (whole body) after intravenous injection of 18FEC (IASON, Linz, Austria; median 230 MBq, range 175-291 MBq).
A contrast-enhanced diagnostic CT scan (140 keV, 100-400 mAs, dose modulation) or a low-dose CT scan (120 keV, 55 mAs) was performed for attenuation correction at the time of the PET scan. Contrast media could not be used in the following cases: renal insufficiency, contrast media allergy, hyperthyreosis, and oral administration of the pharmaceutical Metformin. PET was acquired in 3D (matrix: 168x168/Koblenz;144x144/Cologne). Each bed position (axial field of view of 21.8 cm/Koblenz;19 cm/Cologne) was acquired for 3 min.. Random, scatter and decay correction were applied to the emission data. An ordered-subsets expectation maximization (OSEM) algorithm was used for reconstruction (two iterations, fourteen subsets, Gaussian filtering, 4.2 mm/Koblenz;5.3 mm Cologne transaxial resolution, full-width at half-maximum). CT data were obtained for attenuation correction.
The uptake of 68Ga-PSMA-11 and 18FEC, i.e. the tracer concentration of the hypermetabolic cancer region detected in the image, was quantified in terms of SUVmax.
SUVmax values above 2.5 were related to clear and reproducible visual detection of PET positivity and therefore a cut off of SUVmax 2.5 was used to discriminate PET positivity from PET negativity for both tracers [27].
Statistical analysis
The PET/CT results were related to the GS obtained by histopathologic analysis of biopsies. Additionally, we analyzed correlations between PSA, SUVmax, GS and detection of metastases.
The data analysis was performed using descriptive statistics (relative and absolute frequencies, arithmetic means, standard deviation).
Spearman rank correlation coefficients were calculated to specify the relationship between two variables. The SUVmax values were related to the GS obtained by histopathologic analysis of biopsies. Additionally, we analyzed correlations between PSA, SUVmax, GS and detection of metastases.
By means of ROC analysis we tested the ability of the method to distinguish between high- and low-grade cancer (significant/not significant) by plotting the true positive cases (sensitivity) against the false positive cases (1-specificity) for various SUVmax cut off-levels. Area under the ROC curve (AUC) together with 95%-confidence interval (CI) and standard deviation (SD) were calculated to characterize the quality of the discrimination between the two groups.
All tests were carried out using the software BiAS; p-values of less than 0.05 were stated as significant.
CONCLUSION
Our results show that 68Ga-PSMA-11 PET/CT and 18FEC PET/CT are both suitable for the detection of primary prostate cancer. An advantage for 68Ga-PSMA-11 PET/CT is its excellent imaging quality, its high specificity and a correlation of positive scans with GS which may allow a differentiation between low- and high-grade carcinoma. Our results support the view that 68Ga-PSMA-11 PET/CT promotes higher detection rates of significant malignancies requiring intervention as does the diagnostic procedure using 18FEC PET/CT.
Therefore 68Ga-PSMA-11 PET/CT is intended to increase diagnostic precision (avoiding false-negative results and understaging) to guide prostate biopsy and might help to reduce overtreatment of low-grade malignant disease as well as detect the foci of the highest Gleason pattern.
68Ga-PSMA-11 PET/CT is already clinically accepted in detecting metastases in patients with biochemical recurrence [31], but it may play an important role also in initial tumor staging similar to and in conjunction with mpMRI-supported biopsy [33, 42].
Abbreviations
ADT: androgen deprivation therapy; 18FEC: 18F-fluoroethylcholine; 68Ga: 68Gallium; GS: Gleason Score; mpMRI: multiparametric magnetic resonance imaging; NPV: negative predictive value; PPV: positive predictive value; PSA: prostate-specific antigen; PSMA: prostate-specific membrane antigen; SUVmax: maximum standardized uptake value.
Author contributions
M.A. Hoffmann: Protocol development, Project development, Data collection, Data management, Data analysis, Manuscript writing, Manuscript editing.
M. Miederer: Protocol development, Project development, Data management, Data analysis, Manuscript writing.
H.J. Wieler: Protocol development, Project development, Data analysis, Manuscript editing.
C. Ruf: Data management, Data analysis, Manuscript writing, Manuscript editing.
F.M. Jakobs: Data analysis, Manuscript writing, Manuscript editing.
M. Schreckenberger: Protocol development, Project development, Data management, Data analysis, Manuscript editing.
ACKNOWLEDGMENTS
The authors thank Ed Michaelson, MD, Fort Lauderdale, Florida, for language revision.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest. They reveal to the Editors any relationships that they believe could be construed as resulting in an actual, potential, or perceived conflict of interest with regard to the manuscript submitted for review.
FUNDING
The authors declare having no financial support.
Editorial note
This paper has been accepted based in part on peer-review conducted by another journal and the authors’ response and revisions as well as expedited peer-review in Oncotarget.
REFERENCES
1. Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA, Grading C. The 2014 International Society of Urological Pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol. 2016; 40:244-252.
2. Epstein JI, Montironi R. Grading of prostate cancer in the 21st century. Urologia. 2016; 83:1-3.
3. Recabal P, Assel M, Sjoberg DD, Lee D, Laudone VP, Touijer K, Eastham JA, Vargas HA, Coleman J, Ehdaie B. The efficacy of multiparametric magnetic resonance imaging and magnetic resonance imaging targeted biopsy in risk classification for patients with prostate cancer on active surveillance. J Urol. 2016; 196:374-381.
4. Giovacchini G, Picchio M, Coradeschi E, Scattoni V, Bettinardi V, Cozzarini C, Freschi M, Fazio F, Messa C. [(11)C]choline uptake with PET/CT for the initial diagnosis of prostate cancer: relation to PSA levels, tumour stage and anti-androgenic therapy. Eur J Nucl Med Mol Imaging. 2008; 35:1065-1073.
5. Schwarzenbock S, Souvatzoglou M, Krause BJ. Choline PET and PET/CT in primary diagnosis and staging of prostate cancer. Theranostics. 2012; 2:318-330.
6. Heidegger I, Skradski V, Steiner E, Klocker H, Pichler R, Pircher A, Horninger W, Bektic J. High risk of under-grading and-staging in prostate cancer patients eligible for active surveillance. PLoS One. 2015; 10:e0115537.
7. Oliveira IS, Pontes-Junior J, Abe DK, Crippa A, Dall’oglio MF, Nesralah AJ, Leite KR, Reis ST, Srougi M. Undergrading and understaging in patients with clinically insignificant prostate cancer who underwent radical prostatectomy. Int Braz J Urol. 2010; 36:292-299.
8. Rapiti E, Schaffar R, Iselin C, Miralbell R, Pelte MF, Weber D, Zanetti R, Neyroud-Caspar I, Bouchardy C. Importance and determinants of Gleason score undergrading on biopsy sample of prostate cancer in a population-based study. BMC Urol. 2013; 13:19.
9. Shapiro RH, Johnstone PA. Risk of Gleason grade inaccuracies in prostate cancer patients eligible for active surveillance. Urology. 2012; 80:661-666.
10. Haffner J, Lemaitre L, Puech P, Haber GP, Leroy X, Jones JS, Villers A. Role of magnetic resonance imaging before initial biopsy: comparison of magnetic resonance imaging-targeted and systematic biopsy for significant prostate cancer detection. BJU Int. 2011; 108:E171-178.
11. Kwee SA, Coel MN, Lim J, Ko JP. Prostate cancer localization with 18fluorine fluorocholine positron emission tomography. J Urol. 2005; 173:252-255.
12. Reske SN, Blumstein NM, Neumaier B, Gottfried HW, Finsterbusch F, Kocot D, Moller P, Glatting G, Perner S. Imaging prostate cancer with 11C-choline PET/CT. J Nucl Med. 2006; 47:1249-1254.
13. Sutinen E, Nurmi M, Roivainen A, Varpula M, Tolvanen T, Lehikoinen P, Minn H. Kinetics of [(11)C]choline uptake in prostate cancer: a PET study. Eur J Nucl Med Mol Imaging. 2004; 31:317-324.
14. de Jong IJ, Pruim J, Elsinga PH, Vaalburg W, Mensink HJ. Visualization of prostate cancer with 11C-choline positron emission tomography. Eur Urol. 2002; 42:18-23.
15. Husarik DB, Miralbell R, Dubs M, John H, Giger OT, Gelet A, Cservenyak T, Hany TF. Evaluation of [(18)F]-choline PET/CT for staging and restaging of prostate cancer. Eur J Nucl Med Mol Imaging. 2008; 35:253-263.
16. Cimitan M, Bortolus R, Morassut S, Canzonieri V, Garbeglio A, Baresic T, Borsatti E, Drigo A, Trovo MG. [18F]fluorocholine PET/CT imaging for the detection of recurrent prostate cancer at PSA relapse: experience in 100 consecutive patients. Eur J Nucl Med Mol Imaging. 2006; 33:1387-1398.
17. Heinisch M, Dirisamer A, Loidl W, Stoiber F, Gruy B, Haim S, Langsteger W. Positron emission tomography/computed tomography with F-18-fluorocholine for restaging of prostate cancer patients: meaningful at PSA < 5 ng/ml? Mol Imaging Biol. 2006; 8:43-48.
18. Kwee SA, DeGrado T. Prostate biopsy guided by 18F-fluorocholine PET in men with persistently elevated PSA levels. Eur J Nucl Med Mol Imaging. 2008; 35:1567-1569.
19. Afshar-Oromieh A, Zechmann CM, Malcher A, Eder M, Eisenhut M, Linhart HG, Holland-Letz T, Hadaschik BA, Giesel FL, Debus J, Haberkorn U. Comparison of PET imaging with a (68)Ga-labelled PSMA ligand and (18)F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2014; 41:11-20.
20. Souvatzoglou M, Weirich G, Schwarzenboeck S, Maurer T, Schuster T, Bundschuh RA, Eiber M, Herrmann K, Kuebler H, Wester HJ, Hoefler H, Gschwend J, Schwaiger M, et al. The sensitivity of [11C]choline PET/CT to localize prostate cancer depends on the tumor configuration. Clin Cancer Res. 2011; 17:3751-3759.
21. Martorana G, Schiavina R, Corti B, Farsad M, Salizzoni E, Brunocilla E, Bertaccini A, Manferrari F, Castellucci P, Fanti S, Canini R, Grigioni WF, D’Errico Grigioni A. 11C-choline positron emission tomography/computerized tomography for tumor localization of primary prostate cancer in comparison with 12-core biopsy. J Urol. 2006; 176:954-960; discussion 960.
22. Wright GL Jr, Haley C, Beckett ML, Schellhammer PF. Expression of prostate-specific membrane antigen in normal, benign, and malignant prostate tissues. Urol Oncol. 1995; 1:18-28.
23. Afshar-Oromieh A, Malcher A, Eder M, Eisenhut M, Linhart HG, Hadaschik BA, Holland-Letz T, Giesel FL, Kratochwil C, Haufe S, Haberkorn U, Zechmann CM. PET imaging with a [68Ga]gallium-labelled PSMA ligand for the diagnosis of prostate cancer: biodistribution in humans and first evaluation of tumour lesions. Eur J Nucl Med Mol Imaging. 2013; 40:486-495.
24. Krohn T, Verburg FA, Pufe T, Neuhuber W, Vogg A, Heinzel A, Mottaghy FM, Behrendt FF. [(68)Ga]PSMA-HBED uptake mimicking lymph node metastasis in coeliac ganglia: an important pitfall in clinical practice. Eur J Nucl Med Mol Imaging. 2015; 42:210-214.
25. Giesel FL, Sterzing F, Schlemmer HP, Holland-Letz T, Mier W, Rius M, Afshar-Oromieh A, Kopka K, Debus J, Haberkorn U, Kratochwil C. Intra-individual comparison of (68)Ga-PSMA-11-PET/CT and multi-parametric MR for imaging of primary prostate cancer. Eur J Nucl Med Mol Imaging. 2016; 43:1400-1406.
26. Chakraborty PS, Tripathi M, Agarwal KK, Kumar R, Vijay MK, Bal C. Metastatic poorly differentiated prostatic carcinoma with neuroendocrine differentiation: negative on 68Ga-PSMA PET/CT. Clin Nucl Med. 2015; 40:e163-166.
27. Afshar-Oromieh A, Avtzi E, Giesel FL, Holland-Letz T, Linhart HG, Eder M, Eisenhut M, Boxler S, Hadaschik BA, Kratochwil C, Weichert W, Kopka K, Debus J, Haberkorn U. The diagnostic value of PET/CT imaging with the (68)Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2015; 42:197-209.
28. Kasperzyk JL, Finn SP, Flavin R, Fiorentino M, Lis R, Hendrickson WK, Clinton SK, Sesso HD, Giovannucci EL, Stampfer MJ, Loda M, Mucci LA. Prostate-specific membrane antigen protein expression in tumor tissue and risk of lethal prostate cancer. Cancer Epidemiol Biomarkers Prev. 2013; 22:2354-2363.
29. Marchal C, Redondo M, Padilla M, Caballero J, Rodrigo I, Garcia J, Quian J, Boswick DG. Expression of prostate specific membrane antigen (PSMA) in prostatic adenocarcinoma and prostatic intraepithelial neoplasia. Histol Histopathol. 2004; 19:715-718.
30. Minner S, Wittmer C, Graefen M, Salomon G, Steuber T, Haese A, Huland H, Bokemeyer C, Yekebas E, Dierlamm J, Balabanov S, Kilic E, Wilczak W, et al. High level PSMA expression is associated with early PSA recurrence in surgically treated prostate cancer. Prostate. 2011; 71:281-288.
31. Eiber M, Maurer T, Souvatzoglou M, Beer AJ, Ruffani A, Haller B, Graner FP, Kubler H, Haberhorn U, Eisenhut M, Wester HJ, Gschwend JE, Schwaiger M. Evaluation of hybrid (6)(8)Ga-PSMA ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J Nucl Med. 2015; 56:668-674.
32. Fendler WP, Schmidt DF, Wenter V, Thierfelder KM, Zach C, Stief C, Bartenstein P, Kirchner T, Gildehaus FJ, Gratzke C, Faber C. 68Ga-PSMA PET/CT detects the location and extent of primary prostate cancer. J Nucl Med. 2016; 57:1720-1725.
33. Koerber SA, Utzinger MT, Kratochwil C, Kesch C, Haefner M, Katayama S, Mier W, Iagaru AH, Herfarth K, Haberkorn U, Debus J, Giesel FL. 68Ga-PSMA11-PET/CT in newly diagnosed carcinoma of the prostate: correlation of intraprostatic PSMA uptake with several clinical parameters. J Nucl Med. 2017. https://doi.org/10.2967/jnumed.117.190314.
34. Hoffmann MA, Wieler HJ, Jakobs FM, Taymoorian K, Gerhards A, Miederer M, Schreckenberger M. [Diagnostic significance of multiparametric MRI combined with US-fusion guided biopsy of the prostate in patients with increased PSA levels and negative standard biopsy results to detect significant prostate cancer - Correlation with the Gleason score.]. [Article in German]. Nuklearmedizin. 2017; 56:147-155. https://doi.org/10.3413/Nukmed-0871-16-12.
35. Eifler JB, Feng Z, Lin BM, Partin MT, Humphreys EB, Han M, Epstein JI, Walsh PC, Trock BJ, Partin AW. An updated prostate cancer staging nomogram (Partin tables) based on cases from 2006 to 2011. BJU Int. 2013; 111:22-29.
36. Stone NN, Stock RG, Parikh D, Yeghiayan P, Unger P. Perineural invasion and seminal vesicle involvement predict pelvic lymph node metastasis in men with localized carcinoma of the prostate. J Urol. 1998; 160:1722-1726.
37. Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, Fossati N, Gross T, Henry AM, Joniau S, Lam TB, Mason MD, Matveev VB, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2016.
38. Briganti A, Larcher A, Abdollah F, Capitanio U, Gallina A, Suardi N, Bianchi M, Sun M, Freschi M, Salonia A, Karakiewicz PI, Rigatti P, Montorsi F. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: the essential importance of percentage of positive cores. Eur Urol. 2012; 61:480-487.
39. Briganti A, Suardi N, Capogrosso P, Passoni N, Freschi M, di Trapani E, Gallina A, Capitanio U, Abdollah F, Tutolo M, Bianchi M, Salonia A, Da Pozzo LF, et al. Lymphatic spread of nodal metastases in high-risk prostate cancer: the ascending pathway from the pelvis to the retroperitoneum. Prostate. 2012; 72:186-192.
40. Zamboglou C, Wieser G, Hennies S, Rempel I, Kirste S, Soschynski M, Rischke HC, Fechter T, Jilg CA, Langer M, Meyer PT, Bock M, Grosu AL. MRI versus (6)(8)Ga-PSMA PET/CT for gross tumour volume delineation in radiation treatment planning of primary prostate cancer. Eur J Nucl Med Mol Imaging. 2016; 43:889-897.
41. Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T, Zattoni F, Mottet N, European Association of U. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol. 2014; 65:124-137.
42. Eiber M, Fendler WP, Rowe SP, Calais J, Hofman MS, Maurer T, Schwarzenboeck SM, Kratowchil C, Herrmann K, Giesel FL. Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy. J Nucl Med. 2017; 58:67S-76S.
43. Junker D, Quentin M, Nagele U, Edlinger M, Richenberg J, Schaefer G, Ladurner M, Jaschke W, Horninger W, Aigner F. Evaluation of the PI-RADS scoring system for mpMRI of the prostate: a whole-mount step-section analysis. World J Urol. 2015; 33:1023-1030.