
INTRODUCTION
Cancer is a leading cause of mortality worldwide according to the latest statistics from the American Cancer Society. In 2016, there were approximately 1.7 million new cancer cases and 0.6 million cancer-related deaths in the United States [1]. Many solid tumors lack specific tumor biomarkers and effective treatment options. Novel therapeutic approaches and tumor biomarkers with high specificity and sensitivity are necessary for the diagnosis and outcome evaluation of cancer patients.
Chemokines are a group of small molecular proteins that bind to corresponding cell-surface receptors and participate in various immunological, physiological, and pathological processes. There are nearly 50 human genes that encode chemokine ligands, and more than 20 corresponding chemokine receptors. Chemokines are further divided into four classes according to structural differences: CXC, CC, CX3C, and C [2]. Emerging evidence indicates that CXC chemokines and their receptors contribute to tumor-related processes including tumor cell proliferation, invasion, metastasis, and angiogenesis [3]. CXC chemokines are further divided into ELR+ and ELR- subtypes according to the presence or absence of an ELR (Glu-Leu-Arg) tripeptide motif at the NH2 terminus.
Multiple receptors have been identified as CXCR1-CXCR7 [4]. CXC chemokine receptor-2 (CXCR2) is a primary receptor of the CXC superfamily and has a high affinity for chemokines [5]. This seven-transmembrane G protein-coupled receptor is expressed on cell membranes of leukocytes, endothelial cells, and tumor cells. Chemokine-receptor binding can promote tumor cell proliferation and invasion as well as tumor tissue angiogenesis, regulate the association between tumor cell and extracellular matrix, and mediate immune cell infiltration and drug resistance [4, 6–10]. CXCR2 has been associated with to the biological behavior of tumors in colon cancer [11], oral squamous cell carcinoma [12], pancreatic cancer [13], and hepatocellular carcinoma [14].
Several studies have shown that CXCR2 overexpression was associated with poor survival in gastric cancer [15], hepatocellular cancer [16], and renal cell cancer [17]. Other studies revealed had no obvious association of CXCR2 with the outcomes of esophageal cancer [18], pancreatic ductal cancer [19], or ovarian cancer [7]. We conducted a systematic review and meta-analysis to clarify the prognostic effect of elevated CXCR2 levels in solid tumors.
RESULTS
Study characteristics
According to the described searching strategy, 3534 records were initially collected. After initial screening of titles, abstracts, and full text of each publication to exclude non-conforming articles, 135 records were obtained. Then 114 full-text articles were further excluded due to lack of survival data, CXCR2 detected in a non-tissue sample, or investigation of the same patient. Finally, 21 articles were enrolled in this meta-analysis. Figure 1 describes the detailed study selection process.
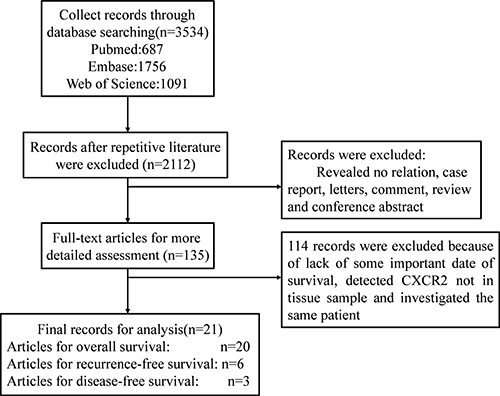
Figure 1: Scheme of the study selection process.
Primary information of the included studies is shown in Table 1. A total of 4012 patients from USA, China, Japan, Iran, and Greece were diagnosed with hepatocellular carcinoma, esophageal cancer, gastric cancer, non-small cell lung cancer, laryngeal squamous cell carcinoma, ovarian cancer, renal cell carcinoma, pancreatic ductal adenocarcinoma, colorectal cancer, or astrocytic tumors. Among these studies, 3894 patients from 20 studies were evaluated by overall survival (OS), 1450 patients from 6 studies were evaluated by recurrence-free survival (RFS), and 377 patients from 3 studies were evaluated by disease-free survival (DFS). The 2411 patients from 13 studies were diagnosed with cancers of the digestive system. All studies were published in 2010 or later and assessed CXCR2 expression in tumor tissue by immunohistochemistry. All tumor tissues were derived from surgical specimens. Asian subjects comprised 15 studies, and 6 studies were on Caucasians. Hazard ratios (HRs) and 95% confidence intervals (95% CIs) were reported directly in 13 studies and estimated indirectly from the other 8 studies. The co-variables of the studies controlled for by multivariable Cox regression are shown in Table 2 and the cut-off values in these studies varied.
Table 1: Characteristics of studies included in the meta-analysis
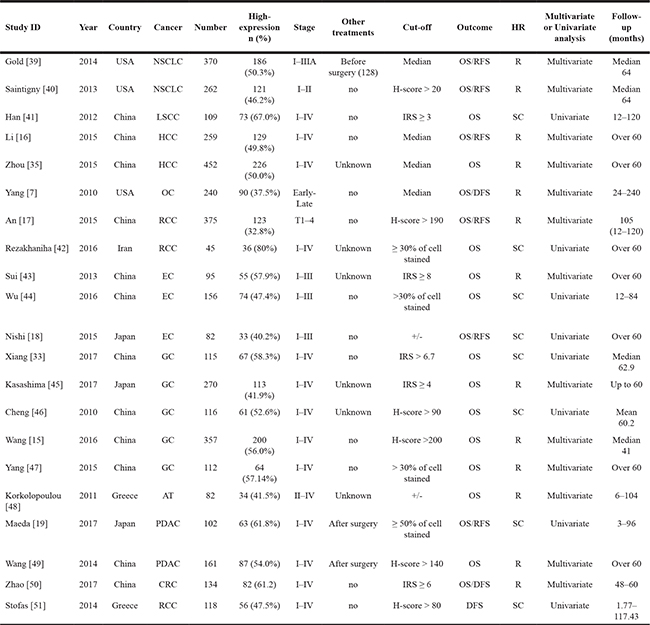
NSCLC: non-small cell lung cancer; LSCC: laryngeal squamous cell carcinoma; HCC: hepatocellular carcinoma; OC: Ovarian Cancer; RCC: renal cell carcinoma; EC: esophageal cancer; GC: gastric cancer; AT: Astrocytic Tumors; PDAC: Pancreatic Ductal Adenocarcinoma; CRC: Colorectal cancer IHC: immunohistochemistry; OS: overall survival; DFS: disease-free survival; RFS: recurrence-free survival; R: report; SC: survival curve; IRS: immunoreactivity score.
Table 2: Co-variables controlled for by studies using multivariable Cox regression
Study ID |
Outcome |
Co-variables |
|---|---|---|
Gold [39] |
OS |
Age, Stage, c-pAMPK, c-pmTOR, c-EPCAM, n-FEN1 |
RFS |
Age, Stage, c-pAMPK, c-pmTOR, c-EPCAM, c-IGF-1R, m-Insulin receptor, m-CASK |
|
Saintigny [40] |
OS |
Age, Gender, Stage |
RFS |
Age,, Stage |
|
Li [16] |
OS/RFS |
Age, Gender, HBsAg, Cirrhosis, ALT, AST, AFP, Tumor size, Tumor differentiation, Vascular invasion, Tumor multiplicity, TNM stage, BCLC stage |
Zhou [35] |
OS |
AFP, GGT, Liver cirrhosis, Tumor size, Microvascular invasion, Tumor encapsulation, Tumor differentiation |
Yang [7] |
OS/DFS |
Age, Stage, Family history, Subtype, Clinical response, Ascities |
An [17] |
OS/RFS |
Tumor size, Stage, Fuhrman grade, Necrosis, ECOG-PS |
Sui [43] |
OS |
Age, Gender, TNM stage, Lymph node metastasis, Tumor dimension |
Kasashima [45] |
OS |
CXCL1, CXCL1 and CXCR2 both, Macroscopic type, Histological type, T invasion, Lymph node metastasis, Lymphatic invasion, Venous invasion, Hepatic metastasis, Peritoneal metastasis, Peritoneal cytology |
Wang [15] |
OS |
T stage, Lymph node metastasis, Distant metastasis, Lauren classification |
Yang [47] |
OS |
Age, IL-22BP expression, TNM stage, Depth of invasion, Lymph node metastasis |
Korkolopoulou [48] |
OS |
Surgery, Radiotherapy, Histological grade |
Wang [49] |
OS |
Age, Gender, TNM stage, Lymph node metastasis, Tumor size, Tumor differentiation, Vascular invasion, Tumor location, Perineural invasion, Surrounding tissue invasion |
Zhao [50] |
OS/DFS |
Dukes stage |
c: cytoplasmic, m: membrane, n: nuclear, AFP alpha-fetoprotein, ALT alanine aminotransferase, AST aspartate aminotransferase, BCLC Barcelona Clinic Liver Cancer, HBsAg hepatitis B surface antigen, TNM tumor-nodes-metastasis, GGT, gamma glutamyl transferase, ECOG-PS, Eastern Cooperative Oncology Group performance status, IL-22BP, interleukin-22 receptor 2.
Quality assessment
We used the Quality in Prognostic Studies (QUIPS) tool to assess the quality of the 21 eligible studies included in our meta-analysis [20] (Supplementary Table 1). A moderate risk of bias for domain 1 (Study Participation) was shown in 4 original studies and was primarily due to small participation cohorts. Moderate bias in domain 2 (Study Attrition) was indicated for 1 original study due to missing data from participants without a follow-up. Moderate bias in domain 3 (Prognostic Factor Measurement) was shown in 6 original studies due to a lack of definite cutoff values. All original studies provided clear outcome definitions and had a low risk of bias for domain 4 (Outcome Measurement). Moderate bias in domain 5 (Study Confounding) was shown in 6 original studies that lacked detailed descriptions of treatment beyond surgery. Moreover, 8 original studies conducted only univariate Cox analysis and had a moderate risk of bias for domain 6 (Statistical Analysis and Reporting).
CXCR2 and OS
The 20 studies including 3894 patients provided correlative data for OS analysis. We used the fixed-effects model to calculate the pooled HR and its 95% CI due to no obvious heterogeneity (P = 0.724, I2 = 0.0%). The pooled HR was 1.82 (95% CI = 1.63–2.03, P < 0.001), and indicated that increased CXCR2 expression might predict poor OS in solid tumor patients (Figure 2).
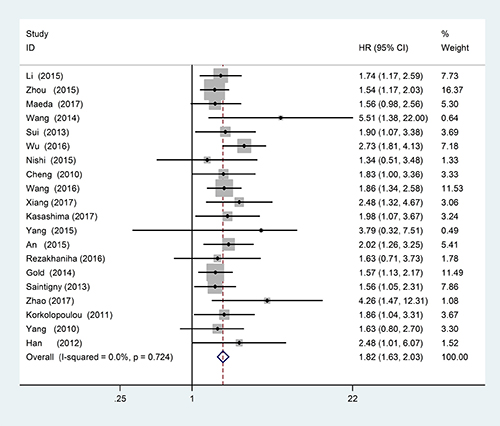
Figure 2: Forest plots of studies evaluating hazard ratios of high CXCR2 expression in solid tumors for overall survival (OS).
Subgroup analyses were carried out according to tumor type, tumor source, analysis type, and ethnicity. Heterogeneity was found in the pancreatic ductal adenocarcinoma group (P = 0.091, I2=65%), so we used a random-effect model to calculate the pooled HR and its 95% CI. The CXCR2 expression had no significant association with OS in pancreatic ductal adenocarcinoma (pooled HR = 2.47; 95% CI = 0.75–8.10; P = 0.137). There was no obvious heterogeneity in other subgroups, so we used the fixed-effects model to calculate the pooled HR and its 95% CI. These results are shown in Table 3. According to tumor type, CXCR2 overexpression predicted poor OS for patients with hepatocellular carcinoma (HR = 1.60; 95% CI = 1.28–2.01; P < 0.001), esophageal cancer (HR = 2.26; 95% CI = 1.65–3.11; P < 0.001), gastric cancer (HR = 1.98; 95% CI = 1.56–2.51; P < 0.001), renal cell carcinoma (HR = 1.92; 95% CI = 1.27–2.90; P = 0.002), non-small cell lung cancer (HR = 1.56; 95% CI = 1.22–2.01; P < 0.001) and others tumor type (HR = 2.04; 95% CI = 1.43–2.92; P < 0.001) (Figure 3).
Table 3: Pooled OS HRs according to subgroup analyses
Subgroup |
Study |
No. of patients |
Fixed-effects model |
Heterogeneity |
||
|---|---|---|---|---|---|---|
HR (95%CI) |
P value |
I2 (%) |
P |
|||
Overall survival |
3894 |
1.82 (1.63–2.03) |
< 0.001 |
0 |
0.724 |
|
Tumor type |
||||||
HCC |
711 |
1.60 (1.28–2.01) |
< 0.001 |
0 |
0.632 |
|
EC |
333 |
2.26 (1.65–3.11) |
< 0.001 |
12.8 |
0.318 |
|
GC |
970 |
1.98 (1.56–2.51) |
< 0.001 |
0 |
0.854 |
|
RCC |
420 |
1.92 (1.27–2.90) |
0.002 |
0 |
0.658 |
|
NLCC |
632 |
1.56 (1.22–2.01) |
< 0.001 |
0 |
0.982 |
|
Others |
565 |
2.04 (1.43–2.92) |
< 0.001 |
0 |
0.449 |
|
Tumor source |
||||||
DSN |
2411 |
1.88 (1.64–2.16) |
< 0.001 |
3.9 |
0.407 |
|
Others |
1483 |
1.70 (1.41–2.05) |
< 0.001 |
0 |
0.942 |
|
Analysis type |
||||||
multivariate |
3169 |
1.75 (1.54–1.99) |
< 0.001 |
0 |
0.732 |
|
univariate |
725 |
2.06 (1.64–2.59) |
< 0.001 |
0 |
0.570 |
|
Ethnicity |
||||||
Asian |
2895 |
1.91 (1.67–2.17) |
< 0.001 |
0 |
0.534 |
|
Caucasian |
999 |
1.61 (1.31–1.99) |
< 0.001 |
0 |
0.990 |
|
HR: hazard ratio; CI: confidence interval; DSN: digestive system neoplasms; HCC: hepatocellular carcinoma; EC: esophageal cancer; GC: gastric cancer; RCC: renal cell carcinoma, NSCLC: non-small cell lung cancer.
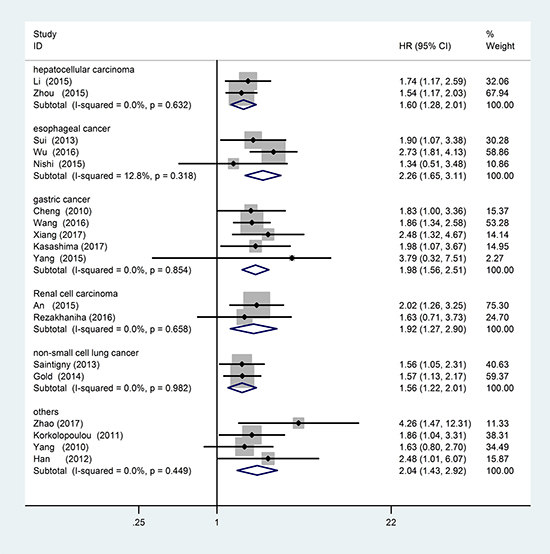
Figure 3: Forest plot of tumor type subgroup analysis.
Funnel plots, Egger’s, and Begg’s tests were used to evaluate the publication bias of all included studies. There was obvious publication bias because of the P-value of the Egger’s regression intercept was 0.012 (Figure 4). We used the “Trim and Fill” method to adjust for publication bias under the fixed-effects model, and the corrected multivariable-adjusted pooled HR for OS was 1.78 (95% CI = 1.60–2.00).
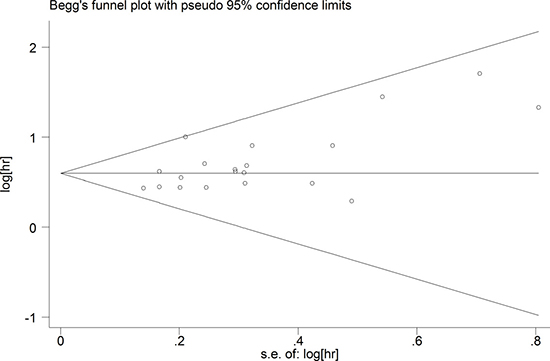
Figure 4: Funnel plots of publication biases of association between CXCR2 expression and overall survival (OS) in solid cancer patients.
CXCR2 and RFS
In this meta-analysis, 6 studies with a total of 1450 patients provided suitable data for RFS analysis. No obvious statistical heterogeneity (I2 = 0.0%; P = 0.490) was found, so we used a fixed-effects model to pool the HR. High CXCR2 expression was significantly associated with poor RFS (pooled HR = 1.40; 95% CI = 1.21–1.62; P < 0.001) (Figure 5). The subgroup analyses results are shown in Table 4.
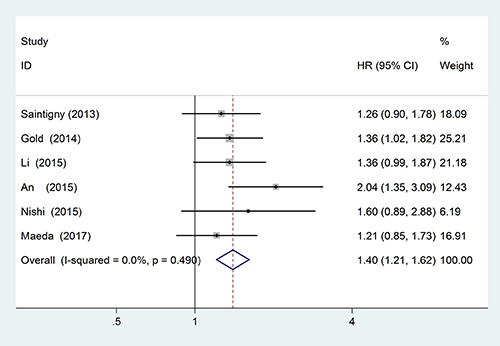
Figure 5: Forest plots of studies evaluating hazard ratios (HR) of high CXCR2 expression in solid tumors for recurrence-free survival analysis (RFS).
Table 4: Pooled RFS HR according to subgroup analyses
Subgroup |
Study |
No. of patients |
Fixed-effects model |
Heterogeneity |
||
|---|---|---|---|---|---|---|
HR(95% CI) |
P value |
I2 (%) |
P |
|||
RFS |
1450 |
1.40 (1.21–1.62) |
< 0.001 |
0.0% |
0.490 |
|
Ethnicity |
||||||
Asian |
818 |
1.46 (1.20–1.77) |
< 0.001 |
22.3% |
0.277 |
|
Caucasian |
632 |
1.32 (1.06–1.65) |
0.015 |
0.0% |
0.747 |
|
Tumor source |
||||||
DSN |
443 |
1.33 (1.07–1.66) |
0.011 |
0.0% |
0.716 |
|
Others |
1007 |
1.45 (1.19–1.77) |
< 0.001 |
41.3% |
0.182 |
|
Analysis type |
||||||
multivariate |
1266 |
1.43 (1.21–1.68) |
< 0.001 |
15.1% |
0.317 |
|
univariate |
184 |
1.30 (0.96–1.77) |
0.087 |
0.0% |
0.425 |
|
RFS: recurrence-free survival; HR: hazard ratio; CI: confidence interval; DSN: digestive system neoplasms.
CXCR2 and DFS
Correlative data for DFS analysis was provided in 3 studies including 377 patients. The studies that evaluated DFS had statistical heterogeneity (I2 = 57.8%, P = 0.093), so we used a random-effects model to pool the HR. High CXCR2 expression was significantly associated with poor DFS (pooled HR = 1.89; 95% CI = 1.05–3.40; P = 0.033) (Figure 6).
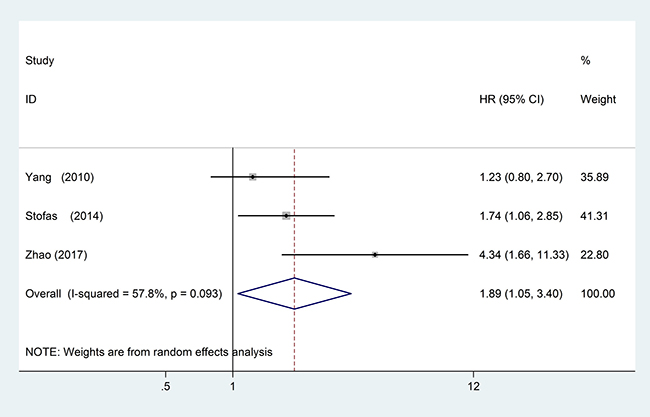
Figure 6: Forest plots of studies evaluating hazard ratios (HR) of high CXCR2 expression in solid tumors for disease-free survival analysis (DFS).
DISCUSSION
CXC chemokines are a group of small molecule proteins with similar structure and function that are secreted by various cells in vivo. They primarily induce leukocyte accumulation in lesions and sites of inflammation [21]. Most ELR+ CXC chemokines, including CXCL1–3 and CXCL5–8, increase the tumor tissue penetration of immunosuppressive cells, reduce apoptosis, and promote angiogenesis as well as tumor cell proliferation, migration, and invasion by activating the CXCR2 receptor [6–10, 22]. Therefore, CXCR2 might play a critical role in cancer progression.
Tumor progression depends on adequate blood supply, and there is evidence that CXCR2 is essential for tumor angiogenesis. Previous reports have demonstrated that the blockade of CXCR2 can significantly inhibit the formation of microvessels in tumor tissue [23–25] The activation of CXCR2 promotes tumor angiogenesis through the following mechanisms: (1) increase the migration and tube formation of human umbilical vein endothelial cells (HUVECs) [26]; (2) promote vasculogenic mimicry (VM) in tumors [27], which is a non-classical mechanism whereby cancer cells, rather than endothelial cells, form blood vessels; (3) increase the expression of vascular endothelial growth factor (VEGF) in tumor tissues [28]; (4) regulate migratory and angiogenic activities of endothelial progenitor cells (EPCs) and induce tumor tissue angiogenesis [29]; (5) induce tumor-infiltrating myeloid cells of tumor tissues, which are known to support blood vessel development in solid tumor growth [30].
Blockade of the CXCR2 signaling pathway can significantly enhance the effect of chemotherapy in colon cancer patients [31] and inhibit the proliferation and invasion of chemotherapy-resistant breast cancer cells [32]. The activation of this signaling pathway can also promote the invasion and metastasis of gastric cancer cells [33] as well as the progression of bladder cancer by inducing the penetration of myeloid-derived inhibitory cells [34]. Activation of CXCR2 mainly induced the PI3K/Akt/GSK-3β/Snail signaling pathway and the subsequent epithelial- mesenchymal transition (EMT) to promote tumor cell invasion and metastasis [35]. CXCR2 also promoted tumor cell proliferation by modulating cell cycle regulatory proteins and inhibited cellular apoptosis by suppressing phosphorylated p53 and PUMA [7]. Moreover, CXCR2 can induce the accumulation of inflammatory cells to promote a local inflammatory response [36], which is closely related to the development of tumors [37]. Therefore, CXCR2 overexpression in tumor microenvironment could be associated with poor prognosis of cancer patients.
We provided strong evidence that CXCR2 overexpression in tumor tissue was an independent predictor of poor OS, RFS, and DFS in most cancers regardless of the ethnic background of patients in this meta-analysis. The subgroup analyses revealed that high CXCR2 expression was associated with poor prognosis of most digestive system cancers, including hepatocellular carcinoma, gastric cancer, and esophageal cancer. The results tended to be inversely related to the prognosis of patients with pancreatic ductal adenocarcinoma but were not statistically significant. However, there was distinct heterogeneity in the pancreatic ductal adenocarcinoma subgroup, and the corresponding sample size was small. Therefore, larger samples are needed to further evaluate the association between CXCR2 expression and the prognosis of patients with pancreatic cancer.
This was the first meta-analysis to demonstrate that high CXCR2 expression was significantly associated with poor prognosis of most solid tumors. There were limitations to our analysis. This study included 20 related studies. The cut-off value of each study was different so there was a lack of uniform cut-off values when CXCR2 was used as a predictive biomarker of cancer prognosis. A unified cut-off value should be further defined. Some HRs were indirectly calculated from data extracted from the survival curves, which could result in small statistical errors. The different analysis modes, tumor types, follow-up times, and sample sources may have also lead to a statistical bias and affected our results.
Our results were the first to suggest that CXCR2 overexpression was associated with poor survival of patients with most cancer types. However, there was no clear evidence that CXCR2 was associated with the prognosis of pancreatic cancer patients. We demonstrated that CXCR2 might be a prognostic biomarker of some cancers. In addition, the blockade of CXCR2 receptors might contribute to novel cancer treatments. However, there were limitations in our study, and the relevant results require further investigation. Additional high-quality clinical research data and larger sample sizes are needed to characterize the role of CXCR2 expression in cancer further.
MATERIALS AND METHODS
The meta-analysis was reported according to the Systematic Reviews and Meta-Analyses (PRISMA) statement [38] (Supplementary Table 2 ).
Search strategy
Literature published before July 31, 2017, was searched in the PubMed, Embase, and Web of Science databases. The search keywords were “CXCR2 or CXC chemokine receptor-2” (all fields) AND “cancer or carcinoma or tumor or neoplasm” (all fields). There were no other limitations when searching the databases. The reference lists of relative articles were screened manually to avoid deviations in the search process. Two investigators (Y. Yong and L. Baoyang) independently conducted the study selection.
Inclusion and exclusion criteria
The literature included in this meta-analysis met the following criteria: (1) study subjects were patients with any type of solid tumor; (2) CXCR2 expression was measured in cancer tissue; (3) the association between survival outcome and CXCR2 expression was investigated; (4) the HR and 95% CI was provided directly or was extracted from the survival curves. Articles were excluded according to the following criteria: (1) studies of cell lines, animals, or non-solid tumors; (2) reviews, letters and case reports; (3) articles without original data or the prognostic data beyond CXCR2 alone; (4) lack of survival outcome or related data for the estimation of HR and 95% CI.
Data extraction and quality assessment
The relevant information was collected by two independent searches of all incorporated studies and included: first author, publication year, country, tumor type, sample number, tumor stage, detection method, cut-off value, follow-up period, and HR as well as the corresponding 95% CI for OS, RFS or DFS. We preferentially used the multivariate analysis result if the study reported included both univariate and multivariate analysis. The QUIPS tool [20] was used to assess the bias risk of each study. Risk of bias was graded as high, moderate, or low.
Statistical analysis
High and low expression of CXCR2 was defined according to the cut-off values specified in the studies. We calculated the pooled data by using the HRs and their 95% CIs from each study. P < 0.05 indicated that CXCR2 expression was related to the prognosis of cancer patients. We evaluated the heterogeneity by the Q test and I2 statistic. We used a random-effect model when the data were heterogeneous (P ≤ 0.05 or I2 ≥ 50%). The fixed-effect model was used when the data indicated no obvious heterogeneity (P > 0.05 or I2 < 50%). The source of heterogeneity was identified through sensitivity and subgroup analyses. Meta-regression was also used to determine the factors contributing to the heterogeneities of some results. The Funnel plot and Egger test were used to analyze publication bias. All analyses were performed with Stata 12.0 software (Stata Corporation, College Station, TX, USA)
ACKNOWLEDGMENTS
Yong Yang and Baoyang Luo contributed equally to this work. Yong Yang, Baoyang Luo, Yong An, and Donglin Sun designed the study. Yong Yang and Baoyang Luo wrote the manuscript. Han Sun and Huihua Cai collected the relevant papers and data. Yong Yang, Baoyang Luo, Han Sun, and Huihua Cai analyzed the data. All authors reviewed the manuscript.
CONFLICTS OF INTEREST
The authors declared no conflicts of interest.
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016; 66:7–30.
2. Balkwill FR. The chemokine system and cancer. The Journal of pathology. 2012; 226:148–157.
3. Zhu Q, Han X, Peng J, Qin H, Wang Y. The role of CXC chemokines and their receptors in the progression and treatment of tumors. Journal of molecular histology. 2012; 43:699–713.
4. Vandercappellen J, Van Damme J, Struyf S. The role of CXC chemokines and their receptors in cancer. Cancer Lett. 2008; 267:226–244.
5. Addison CL, Daniel TO, Burdick MD, Liu H, Ehlert JE, Xue YY, Buechi L, Walz A, Richmond A, Strieter RM. The CXC chemokine receptor 2, CXCR2, is the putative receptor for ELR+ CXC chemokine-induced angiogenic activity. Journal of immunology (Baltimore, Md : 1950). 2000; 165:5269–5277.
6. Murphy C, McGurk M, Pettigrew J, Santinelli A, Mazzucchelli R, Johnston PG, Montironi R, Waugh DJ. Nonapical and cytoplasmic expression of interleukin-8, CXCR1, and CXCR2 correlates with cell proliferation and microvessel density in prostate cancer. Clin Cancer Res. 2005; 11:4117–4127.
7. Yang G, Rosen DG, Liu G, Yang F, Guo X, Xiao X, Xue F, Mercado-Uribe I, Huang J, Lin SH, Mills GB, Liu J. CXCR2 promotes ovarian cancer growth through dysregulated cell cycle, diminished apoptosis, and enhanced angiogenesis. Clin Cancer Res. 2010; 16:3875–3886.
8. Gabellini C, Trisciuoglio D, Desideri M, Candiloro A, Ragazzoni Y, Orlandi A, Zupi G, Del Bufalo D. Functional activity of CXCL8 receptors, CXCR1 and CXCR2, on human malignant melanoma progression. Eur J Cancer. 2009; 45:2618–2627.
9. Lee YS, Choi I, Ning Y, Kim NY, Khatchadourian V, Yang D, Chung HK, Choi D, LaBonte MJ, Ladner RD, Nagulapalli Venkata KC, Rosenberg DO, Petasis NA, et al. Interleukin-8 and its receptor CXCR2 in the tumour microenvironment promote colon cancer growth, progression and metastasis. British journal of cancer. 2012; 106:1833–1841.
10. Katoh H, Wang D, Daikoku T, Sun H, Dey SK, Dubois RN. CXCR2-expressing myeloid-derived suppressor cells are essential to promote colitis-associated tumorigenesis. Cancer cell. 2013; 24:631–644.
11. Desurmont T, Skrypek N, Duhamel A, Jonckheere N, Millet G, Leteurtre E, Gosset P, Duchene B, Ramdane N, Hebbar M, Van Seuningen I, Pruvot FR, Huet G, et al. Overexpression of chemokine receptor CXCR2 and ligand CXCL7 in liver metastases from colon cancer is correlated to shorter disease-free and overall survival. Cancer Sci. 2015; 106:262–269.
12. Khurram SA, Bingle L, McCabe BM, Farthing PM, Whawell SA. The chemokine receptors CXCR1 and CXCR2 regulate oral cancer cell behaviour. J Oral Pathol Med. 2014; 43:667–674.
13. Hertzer KM, Donald GW, Hines OJ. CXCR2: a target for pancreatic cancer treatment? Expert Opin Ther Targets. 2013; 17:667–680.
14. Liu Z, Yang L, Xu J, Zhang X, Wang B. Enhanced expression and clinical significance of chemokine receptor CXCR2 in hepatocellular carcinoma. The Journal of surgical research. 2011; 166:241–246.
15. Wang Z, Liu H, Shen Z, Wang X, Zhang H, Qin J, Xu J, Sun Y, Qin X. The prognostic value of CXC-chemokine receptor 2 (CXCR2) in gastric cancer patients. BMC Cancer. 2015; 15:766.
16. Li L, Xu L, Yan J, Zhen ZJ, Ji Y, Liu CQ, Lau WY, Zheng L, Xu J. CXCR2-CXCL1 axis is correlated with neutrophil infiltration and predicts a poor prognosis in hepatocellular carcinoma. J Exp Clin Cancer Res. 2015; 34:129.
17. An H, Xu L, Chang Y, Zhu Y, Yang Y, Chen L, Lin Z, Xu J. CXC chemokine receptor 2 is associated with postoperative recurrence and survival of patients with non-metastatic clear-cell renal cell carcinoma. Eur J Cancer. 2015; 51:1953–1961.
18. Nishi T, Takeuchi H, Matsuda S, Ogura M, Kawakubo H, Fukuda K, Nakamura R, Takahashi T, Wada N, Saikawa Y, Omori T, Kitagawa Y. CXCR2 expression and postoperative complications affect long-term survival in patients with esophageal cancer. World J Surg Oncol. 2015; 13:232.
19. Maeda S, Kuboki S, Nojima H, Shimizu H, Yoshitomi H, Furukawa K, Miyazaki M, Ohtsuka M. Duffy antigen receptor for chemokines (DARC) expressing in cancer cells inhibits tumor progression by suppressing CXCR2 signaling in human pancreatic ductal adenocarcinoma. Cytokine. 2017; 95:12–21.
20. Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C. Assessing bias in studies of prognostic factors. Annals of internal medicine. 2013; 158:280–286.
21. Raman D, Sobolik-Delmaire T, Richmond A. Chemokines in health and disease. Experimental cell research. 2011; 317:575–589.
22. Balkwill F. Cancer and the chemokine network. Nature reviews Cancer. 2004; 4:540–550.
23. Keane MP, Belperio JA, Xue YY, Burdick MD, Strieter RM. Depletion of CXCR2 inhibits tumor growth and angiogenesis in a murine model of lung cancer. Journal of immunology (Baltimore, Md : 1950). 2004; 172:2853–2860.
24. Mestas J, Burdick MD, Reckamp K, Pantuck A, Figlin RA, Strieter RM. The role of CXCR2/CXCR2 ligand biological axis in renal cell carcinoma. Journal of immunology (Baltimore, Md : 1950). 2005; 175:5351–5357.
25. Wang B, Hendricks DT, Wamunyokoli F, Parker MI. A growth-related oncogene/CXC chemokine receptor 2 autocrine loop contributes to cellular proliferation in esophageal cancer. Cancer research. 2006; 66:3071–3077.
26. Wang Y, Liu J, Jiang Q, Deng J, Xu F, Chen X, Cheng F, Zhang Y, Yao Y, Xia Z, Xu X, Su X, Huang M, et al. Human Adipose-Derived Mesenchymal Stem Cell-Secreted CXCL1 and CXCL8 Facilitate Breast Tumor Growth by Promoting Angiogenesis. Stem cells (Dayton, Ohio). 2017; 35:2060–2070.
27. Aikins AR, Kim M, Raymundo B, Kim CW. Downregulation of transgelin blocks interleukin-8 utilization and suppresses vasculogenic mimicry in breast cancer cells. Experimental biology and medicine (Maywood, NJ). 2017; 242:573–583.
28. Wei ZW, Xia GK, Wu Y, Chen W, Xiang Z, Schwarz RE, Brekken RA, Awasthi N, He YL, Zhang CH. CXCL1 promotes tumor growth through VEGF pathway activation and is associated with inferior survival in gastric cancer. Cancer Lett. 2015; 359:335–343.
29. Hou Y, Wu Y, Farooq SM, Guan X, Wang S, Liu Y, Oblak JJ, Holcomb J, Jiang Y, Strieter RM, Lasley RD, Arbab AS, Sun F, et al. A critical role of CXCR2 PDZ-mediated interactions in endothelial progenitor cell homing and angiogenesis. Stem cell research. 2015; 14:133–143.
30. Jablonska J, Wu CF, Andzinski L, Leschner S, Weiss S. CXCR2-mediated tumor-associated neutrophil recruitment is regulated by IFN-beta. International journal of cancer. 2014; 134:1346–1358.
31. Lee YS, Choi D, Kim NY, Yang S, Jung E, Hong M, Yang D, Lenz HJ, Hong YK. CXCR2 inhibition enhances sulindac-mediated suppression of colon cancer development. International journal of cancer. 2014; 135:232–237.
32. Sharma B, Varney ML, Saxena S, Wu L, Singh RK. Induction of CXCR2 ligands, stem cell-like phenotype, and metastasis in chemotherapy-resistant breast cancer cells. Cancer Lett. 2016; 372:192–200.
33. Xiang Z, Zhou ZJ, Xia GK, Zhang XH, Wei ZW, Zhu JT, Yu J, Chen W, He Y, Schwarz RE, Brekken RA, Awasthi N, Zhang CH. A positive crosstalk between CXCR4 and CXCR2 promotes gastric cancer metastasis. Oncogene. 2017; 36:5122–5133.
34. Zhang H, Ye YL, Li MX, Ye SB, Huang WR, Cai TT, He J, Peng JY, Duan TH, Cui J, Zhang XS, Zhou FJ, Wang RF, et al. CXCL2/MIF-CXCR2 signaling promotes the recruitment of myeloid-derived suppressor cells and is correlated with prognosis in bladder cancer. Oncogene. 2017; 36:2095–2104.
35. Zhou SL, Zhou ZJ, Hu ZQ, Li X, Huang XW, Wang Z, Fan J, Dai Z, Zhou J. CXCR2/CXCL5 axis contributes to epithelial-mesenchymal transition of HCC cells through activating PI3K/Akt/GSK-3beta/Snail signaling. Cancer Lett. 2015; 358:124–135.
36. Jamieson T, Clarke M, Steele CW, Samuel MS, Neumann J, Jung A, Huels D, Olson MF, Das S, Nibbs RJ, Sansom OJ. Inhibition of CXCR2 profoundly suppresses inflammation-driven and spontaneous tumorigenesis. The Journal of clinical investigation. 2012; 122:3127–3144.
37. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008; 454:436–444.
38. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS medicine. 2009; 6:e1000100.
39. Gold KA, Kim ES, Liu DD, Yuan P, Behrens C, Solis LM, Kadara H, Rice DC, Wistuba II, Swisher SG, Hofstetter WL, Lee JJ, Hong WK. Prediction of survival in resected non-small cell lung cancer using a protein expression-based risk model: implications for personalized chemoprevention and therapy. Clin Cancer Res. 2014; 20:1946–1954.
40. Saintigny P, Massarelli E, Lin S, Ahn YH, Chen Y, Goswami S, Erez B, O’Reilly MS, Liu D, Lee JJ, Zhang L, Ping Y, Behrens C, et al. CXCR2 expression in tumor cells is a poor prognostic factor and promotes invasion and metastasis in lung adenocarcinoma. Cancer research. 2013; 73:571–582.
41. Han L, Jiang B, Wu H, Wang X, Tang X, Huang J, Zhu J. High expression of CXCR2 is associated with tumorigenesis, progression, and prognosis of laryngeal squamous cell carcinoma. Med Oncol. 2012; 29:2466–2472.
42. Rezakhaniha B, Dormanesh B, Pirasteh H, Yahaghi E, Masoumi B, Ziari K, Rahmani O. Immunohistochemical distinction of metastases of renal cell carcinoma with molecular analysis of overexpression of the chemokines CXCR2 and CXCR3 as independent positive prognostic factors for the tumorigenesis. IUBMB life. 2016; 68:629–633.
43. Sui P, Hu P, Zhang T, Zhang X, Liu Q, Du J. High expression of CXCR-2 correlates with lymph node metastasis and predicts unfavorable prognosis in resected esophageal carcinoma. Med Oncol. 2014; 31:809.
44. Wu K, Cui L, Yang Y, Zhao J, Zhu D, Liu D, Zhang C, Qi Y, Li X, Li W, Zhao S. Silencing of CXCR2 and CXCR7 protects against esophageal cancer. American journal of translational research. 2016; 8:3398–3408.
45. Kasashima H, Yashiro M, Nakamae H, Masuda G, Kinoshita H, Morisaki T, Fukuoka T, Hasegawa T, Nakane T, Hino M, Hirakawa K, Ohira M. Clinicopathologic significance of the CXCL1-CXCR2 axis in the tumor microenvironment of gastric carcinoma. PloS one. 2017; 12:e0178635.
46. Cheng WL, Wang CS, Huang YH, Tsai MM, Liang Y, Lin KH. Overexpression of CXCL1 and its receptor CXCR2 promote tumor invasion in gastric cancer. Annals of oncology. 2011; 22:2267–2276.
47. Yang SB, Han F, Wu JH, Zhao Z, Zhan W. Association between CXCR2 and IL-22BP expression indicate a poor outcome for gastric adenocarcinoma progression. Oncology letters. 2016; 12:1477–1484.
48. Korkolopoulou P, Levidou G, El-Habr EA, Adamopoulos C, Samaras V, Zisakis A, Kavantzas N, Boviatsis E, Fragkou P, Papavassiliou AG, Patsouris E, Piperi C. Expression of interleukin-8 receptor CXCR2 and suppressor of cytokine signaling-3 in astrocytic tumors. Molecular medicine (Cambridge, Mass). 2012; 18:379–388.
49. Wang Q, Zheng J, Ni Q, Zhu H, Lu Y, Qian H, Zhu J. Prognostic significance of CXCR2 expression in pancreatic ductal carcinoma. [Article in Chinese]. Zhonghua yi xue za zhi. 2014; 94:3805–3808.
50. Zhao J, Ou B, Feng H, Wang P, Yin S, Zhu C, Wang S, Chen C, Zheng M, Zong Y, Sun J, Lu A. Overexpression of CXCR2 predicts poor prognosis in patients with colorectal cancer. Oncotarget. 2017; 8:28442–28454. https://doi.org/10.18632/oncotarget.16086.
51. Stofas A, Levidou G, Piperi C, Adamopoulos C, Dalagiorgou G, Bamias A, Karadimou A, Lainakis GA, Papadoukakis S, Stravodimos K, Dimopoulos MA, Patsouris E, Gakiopoulou H, et al. The role of CXC-chemokine receptor CXCR2 and suppressor of cytokine signaling-3 (SOCS-3) in renal cell carcinoma. BMC Cancer. 2014; 14:149.