
INTRODUCTION
By 2012, cancer holds the first place of morbidity and mortality in the worldwide, with 14 million new cases and 8 million deaths, which means the age-standardized incidence and mortality were 182 and 102 per 100 000, respectively [1]. According to the International Cancer Research Center, the latest data shows that lung cancer still accounts first for the world’s cancer incidence and death in 2012 [2], but also the first cause of incidence and death of malignant tumors in China [3]. Particularly, lung cancer for men had the highest incidence (34.2 per 100 000) and mortality (30.0 per 100 000) and for women had the fourth highest incidence (13.6 per 100 000) and the second highest mortality (11.1 per 100 000) [1].
Besides dietary factors and tobacco smoke, infectious diseases represent the third leading cause of cancer in the entire world and the proportion of cancers associated with pathogenic microorganism was estimated to be 16.1% [4]. As well known, infection with HPVs is the risk factor of almost all cervical cancer [5], most of the anus - genital cancer and more than a quarter of oropharyngeal cancer [6]. In fact, it appears that the chronic infections with HPV should be responsible for approximately the 5% of all human cancers [7]. A dozen of HPV types, including types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59, have been allocated by International Agency for Research on Cancer in Group 1, as their carcinogenicity to humans has been sufficiently demonstrated. Other HPV types are categorized either in Group 2A (probably carcinogenic), Group 2B (possibly carcinogenic) or Group 3 (inadequate evidence of carcinogenicity to humans).
HPV belongs to the papillomaviridae, a large family of epitheliotropic DNA viruses. HPV gene expression and the viral life cycle are tightly controlled by epithelial cell differentiation. It is assumed that scratching of the epithelial tissue allows the virus to infect undifferentiated cells in the basal layers of stratified squamous epithelium [8]. According to the character of HPV, which has a high degree of affinity to the squamous epithelium and the feature of bronchus and lung, whose main tissue type was epithelial tissue, so it is postulated that HPV is probably related with lung neoplasms.
It has been 38 years since Syrjänen who first suggested that HPV could possibly be involved in bronchial squamous cell carcinoma [9]. But in the follow-up studies, the results were not consistent. In worldwide, HPV infection rate was 0–78.3% in lung cancer [10]. There is an enormous difference of infectious rate of HPV in different regions. At the meantime, differences in sensitivity and specificity of HPV genotyping methods and diagnostic criteria, in addition to the limited spectrum of HPV types analyzed may all contribute to the inconsistent result. The current epidemiological study of the relationship between HPV infection and lung cancer is controversial, and the associated meta-analysis is mainly limited to a single study type or the rate of HPV infection in patients with lung cancer. Herein, this systematic review and formal meta-analysis aimed at conducting a quantitative evaluation for the strength of the association between the lung neoplasms and HPV infection, by searching published analytic epidemiologic studies at home and abroad.
RESULTS
Eligible studies characteristics
According to the established search strategy and inclusion criteria, after screening and detailed examination, a total of 37 eligible articles were selected (Figure 1). 36 of them were case-control studies (24 allogeneic case-control studies [11–34], 8 self-matched case-control studies [35–42], 3 nested case-control studies [43–45] and 1 nested and allogeneic case-control study [46]), including 6,980 cases of lung cancer and 7,474 controls. One population-based cohort study from China was also included. In that study, the incidence of lung cancer in 24,162 HPV-infected patients was compared to 1,026,986 uninfected individuals. After adjusting for age, sex, income, residence and concomitant diseases, there was a significant increase in the risk of lung cancer among women who were exposed to HPV infection (RR = 1.263, 95% CI: 1.015–1.571, P = 0.0367), while no significant association was found among men (RR = 1.169, 95% CI: 0.984–1.390, P = 0.0754). However, this cohort-study lacked information on individual lifestyle, smoking, diagnostic criteria for HPV infection, and detailed HPV types.
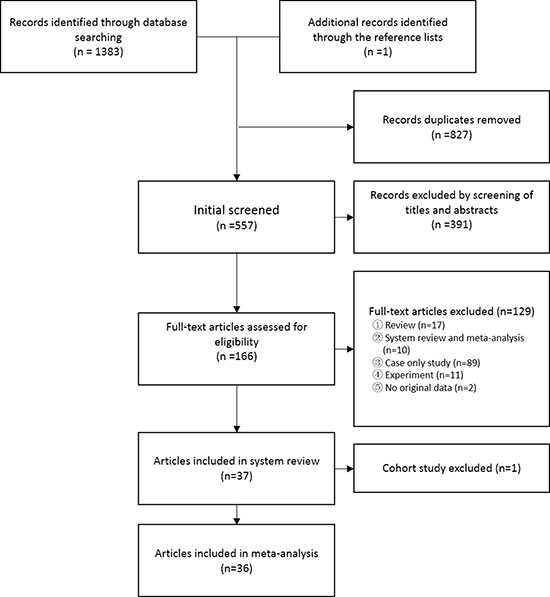
Figure 1: Flow diagram of systematic literature search.
36 case-control studies were conducted further meta-analysis. The majority of cases in the pooled dataset were from Europe (61.2%, 4,274 cases) and Asia (33.2%, 2,315 cases). North American studies represented 4.1% of all cases in the pooled dataset (n = 287) and Oceania studies represented 1.5% of all cases in the pooled dataset (n = 104). The size of studies in the pooled dataset varied from 30 to 1,634 cases. The full list of the included case-control publications was shown in Table 1.
Table 1: The basic information of the selected literature
Author_year |
Country |
Method |
HPV types |
Sample type |
Case (n/N) |
Control (n/N) |
|---|---|---|---|---|---|---|
Béjui-Thivolet_1990 |
French |
ISH |
6, 11, 16, 18 |
tissue |
6/33 |
0/10 |
Li_1995 |
China |
PCR, DB |
16, 18 |
tissue |
16/50 |
0/22 |
Fong_1995 |
Australia |
PCR |
6, 11, 16, 18, 31, 33, 52b, 58 |
tissue |
2/104 |
0/104 |
Yang_1998 |
China |
PCR |
6/11, 16, 31/33 |
tissue |
13/50 |
3/30 |
Niyaz_2000 |
China |
PCR |
16, 18 |
tissue |
44/110 |
1/40 |
Cheng_2001 |
China |
PCR, ISH |
16, 18 |
tissue |
77/141 |
16/60 |
Chiou_2003 |
China |
PCR |
16, 18 |
blood |
71/149 |
22/174 |
Cheng_2004 |
China |
PCR, ISH |
6, 11 |
tissue |
40/141 |
1/60 |
Jain_2005 |
India |
PCR |
16, 18 |
tissue(case) blood(control) |
2/40 |
0/40 |
Ciotti_2006 |
Italy |
PCR, sequencing |
16, 18, 31 |
tissue |
8/38 |
0/38 |
Fei_2006 |
China |
ISH |
16, 18 |
tissue |
23/73 |
2/34 |
Giuliani_2007 |
Italy |
PCR, reverse blot hybridization, sequencing |
- |
tissue |
10/78 |
0/78 |
Nadji_2007 |
Iran |
PCR, sequencing |
- |
tissue |
33/129 |
8/89 |
Buyru_2008 |
Turkey |
PCR, SB |
16, 18 |
blood |
1/65 |
0/87 |
Wang_2008 |
China |
PCR, ISH, IHC |
16, 18 |
tissue |
138/313 |
4/96 |
Yu_2009 |
China |
PCR |
25 types |
tissue |
43/109 |
16/71 |
Xu_2009 |
China |
ISH |
16/18 |
tissue |
32/44 |
0/15 |
Krikelis_2010 |
Greece |
PCR |
16 |
tissue, BW |
36/58 |
11/16 |
Wang_2010 |
China |
PCR |
16, 18 |
tissue |
18/45 |
0/16 |
Joh_2010 |
USA |
PCR, sequencing |
- |
tissue |
5/30 |
0/21 |
Carpagnano_2011 |
Italy |
PCR, sequencing, INFINITI HPV-QUAD assay |
16, 18, 30, 31, 33, 45, 35/68, 39/56, 58/52, 59/51, 6/11 |
tissue, BW, EBC |
12/89 |
0/68 |
Galvan_2012 |
Italy, UK |
PCR,DB |
35 types |
tissue |
0/100 |
0/100 |
Gatta_2012 |
Italy |
PCR |
16, 18, 33, 35, 52, 58 |
tissue |
2/50 |
1/23 |
Yu_2013 |
China |
PCR, reverse blot hybridization, SB |
25 types |
tissue |
75/170 |
21/91 |
Anantharaman_2014 |
7 European countries |
BMSM |
6, 11, 16, 18, 31 |
blood |
791/1634 |
991/2729 |
Sagerup_2014 |
Norway |
PCR |
15 types |
tissue |
13/334 |
0/13 |
Sarchianaki_2014 |
Greece |
PCR, genotyping |
37 types |
tissue |
19/100 |
0/16 |
Yu_2015 |
China |
PCR |
L1, 16, 18 |
tissue |
100/180 |
8/110 |
Fan_2016 |
China |
ICC |
16 |
PE |
42/95 |
1/55 |
Gupta_2016 |
India |
PCR |
16, 18, 31, 33, 45 |
FNAC, tissue |
5/73 |
0/75 |
Lu_2016 |
China |
PCR |
16, 18 |
tissue |
33/72 |
2/54 |
Robinson_2016 |
USA |
microarray, oncovirus panel, genotyping PCR |
28 types |
tissue |
15/57 |
1/10 |
Xiong_2016 |
China |
PCR, reverse blot hybridization |
21 types |
tissue |
7/83 |
6/83 |
Simen_2010 |
Finland |
ELISA |
16, 18 |
serum |
67/311 |
220/930 |
Anantharaman_2014 |
10 European countries |
BMSM |
6, 11, 16, 18, 31 |
blood |
604/1449 |
601/1599 |
Colombara_2015 |
USA |
LBMA |
6, 11, 16, 18, 31, 33, 52, 58 |
serum |
4/200 |
15/200 |
Colombara_2016 |
China |
LBMA |
6, 11, 16, 18, 31, 33, 52, 58 |
serum |
8/183 |
8/217 |
Abbreviations: Author_year, name of first author_year of publication; Case(n/N), Case (number of HPV positive cases/number of cases); Control (n/N), Control (number of HPV positive controls/number of controls); ISH, In situ hybridization; PCR, Polymerase chain reaction; DB, Dot blot; SB, Southern blot; IHC, Immunohistochemistry; BMSM, Bead-based multiplex serology method; ICC, Immunocytochemistry; ELISA, Enzyme-linked immunosorbent assay; LBMA, Multiplex liquid bead microarray antibody assay; BW, bronchial washing; EBC, exhaled breath condensate; PE, pleural effusion; FNAC, fine-needle aspiration cytology.
HPV infection and lung neoplasms pooled risk
The heterogeneity test results of case group and control group were χ2 = 212.51, P < 0.001, I2 = 83.5%. Due to P < 0.1, I2 > 50%, we used a random effects model meta-analysis and pooled OR and 95% CI: 3.64 (2.60–5.08), P < 0.001, estimate of between-study variance Tau2 = 0.47 (Figure 2).
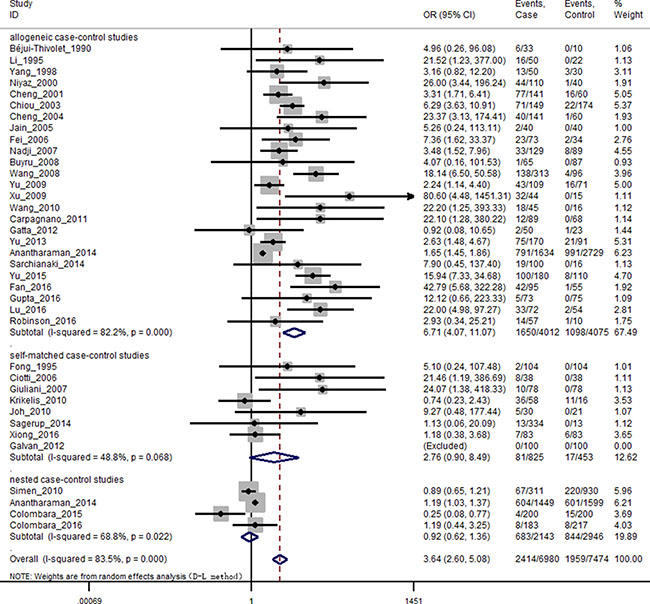
Figure 2: Forest plot of random effects model stratified by study design. Individual study OR (squares) and ORsub (diamonds) values are plotted with 95% confidence intervals (LCL, lower confidence limit; UCL, upper confidence limit) for each study design. Symbol sizes reflect relative weight of the studies.
The results of subgroup analysis were shown as follows: By the study design, using random effects model for allogeneic case-control studies P < 0.001, I2 = 82.2%, pooled OR as 6.71 and 95% CI: 4.07–11.07; using fixed effects model for self-matched case-control studies P = 0.07, I2 = 48.8%, pooled OR as 2.59 and 95% CI: 1.43–4.69; using random effects model for nested case-control studies P = 0.02, I2 = 68.8%, pooled OR as 0.92 and 95% CI: 0.63–1.36 (Figure 2).
In different regions: HPV infection in lung cancer patients were significantly higher compared to controls only among the Asian subjects (OR = 6.24, 95% CI: 3.88–10.04, P < 0.001). Significantly higher HPV infection rates were found in lung cancer patients, compared to controls, in both male (OR = 3.31, 95% CI: 2.02–5.42, P < 0.001) and female (OR = 3.29, 95% CI: 1.01–10.74, P = 0.049). And a significant difference in pooled OR between male and female was not found in HPV infection and lung cancer (P > 0.05). However, significantly higher HPV infection rates were found in lung cancer patients, compared to controls, in non-smokers (OR = 6.51, 95% CI: 3.78–11.21, P < 0.001), but not in smoker subgroup (P > 0.05). Stratified by HPV detection method, significantly higher HPV infection rates were found in polymerase chain reaction (PCR), in situ hybridization (ISH), southern blot/dot blot (SB/DB), sequencing and bead-based multiplex serology method (BMSM), but not in multiplex liquid bead microarray antibody assay (LBMA). Stratified by HPV type, significantly higher HPV infection rates were found in lung cancer, compared to controls, in both HPV 16 (OR = 3.14, 95% CI: 2.07–4.76, P < 0.001), HPV 18 (OR = 2.25, 95% CI: 1.49–3.40, P < 0.001) and HPV 11 (OR = 1.30, 95% CI: 1.12–1.52, P = 0.001), but not in HPV 6 and HPV 31 (P > 0.05). There was a significant difference in pooled OR between tissue and blood (P < 0.05). Using tissues as detection materials, we found that HPV infection was a risk factor of lung cancer. While using blood, a significant association was not found between HPV infection and lung cancer. We also pooled HPV DNA positive rates in lung cancer patients and controls by sample type (Supplementary Figure 1). There is no significant difference in pooled OR between blood (OR = 6.43, 95% CI: 3.74–11.05, P < 0.001) and tissue (OR = 6.29, 95% CI: 4.01–9.88, P < 0.001). Stratified by histological type, significantly higher HPV infection rates were found in lung cancer, compared to controls, in both adenocarcinoma (OR = 5.39, 95% CI: 2.89–10.06, P < 0.001), squamous cell carcinoma (OR = 5.66, 95% CI: 4.38–7.33, P < 0.001) and small cell carcinoma (OR = 6.74, 95% CI: 3.41–13.35, P < 0.001), but not in adenosquamous carcinoma and large cell carcinoma (P > 0.05). Regardless of the clinical stage and differentiated grade, HPV infection was a risk factor of lung cancer. Subgroup analysis results of continent, gender, smoking, detection method, HPV type, material, histological type, clinical stage and differentiated grade for the relationships between HPV infection and lung cancer were shown in Table 2.
Table 2: Subgroup analysis for the relationships between HPV infection and lung cancer
subgroup |
No. of studies |
Case (n/N) |
Control (n/N) |
I2,% |
model |
OR (95%CI) |
P |
|---|---|---|---|---|---|---|---|
Continent |
|||||||
Europe |
12 |
1568/4274 |
1824/5620 |
70.7 |
random |
1.37 (0.99–1.90) |
0.058 |
Asia |
21 |
821/2315 |
119/1519 |
69.3 |
random |
6.24 (3.88–10.04) |
< 0.001 |
America |
3 |
23/287 |
16/231 |
74.7 |
random |
1.44 (0.14–14.31) |
0.757 |
Gender |
|||||||
male |
9 |
108/675 |
19/350 |
0.0 |
fixed |
3.31 (2.02–5.42) |
< 0.001 |
female |
10 |
143/711 |
225/1104 |
68.8 |
random |
3.29 (1.01–10.74) |
0.049 |
smoking |
|||||||
non-smoker |
9 |
103/256 |
17/203 |
7.7 |
fixed |
6.51 (3.78–11.21) |
< 0.001 |
smoker |
11 |
117/1048 |
38/533 |
57.1 |
random |
1.97 (0.86–4.52) |
0.108 |
detection method |
|||||||
PCR |
28 |
837/2958 |
121/1685 |
59.6 |
random |
5.30 (3.44–8.17) |
< 0.001 |
ISH |
3 |
61/150 |
2/59 |
17.9 |
fixed |
12.40 (3.86–39.83) |
< 0.001 |
SB/DB |
6 |
109/546 |
27/461 |
41.9 |
fixed |
3.12 (1.95–4.98) |
< 0.001 |
sequencing |
4 |
60/326 |
8/256 |
12.6 |
fixed |
5.94 (2.91–12.15) |
< 0.001 |
BMSM |
2 |
1395/3083 |
1592/4328 |
91.1 |
random |
1.40 (1.02–1.93) |
0.039 |
LBMA |
2 |
12/383 |
23/417 |
76.0 |
random |
0.56 (0.12–2.59) |
0.458 |
HPV type |
|||||||
16 |
27 |
1030/5908 |
799/6915 |
80.8 |
random |
3.14 (2.07–4.76) |
< 0.001 |
18 |
26 |
732/5828 |
687/6937 |
73.7 |
random |
2.25 (1.49–3.40) |
< 0.001 |
6 |
17 |
938/4929 |
964/5549 |
70.2 |
random |
1.14 (0.81–1.60) |
0.461 |
11 |
13 |
357/4526 |
348/5226 |
0.0 |
fixed |
1.30 (1.12–1.52) |
0.001 |
31 |
14 |
209/4541 |
296/5347 |
12.4 |
fixed |
0.96 (0.80–1.16) |
0.680 |
33 |
6 |
19/972 |
23/604 |
0.0 |
fixed |
0.45 (0.22–0.91) |
0.025 |
material |
|||||||
frozen tissue |
12 |
310/1373 |
38/666 |
50.4 |
random |
5.68 (2.60–12.42) |
< 0.001 |
FFPE tissue |
15 |
479/1325 |
63/727 |
64.9 |
random |
6.89 (3.73–12.72) |
< 0.001 |
fresh tissue |
2 |
23/118 |
0/91 |
0.0 |
fixed |
17.05 (2.22–131.01) |
0.006 |
blood |
7 |
1546/3991 |
1857/5936 |
89.6 |
random |
1.41 (0.95–2.10) |
0.088 |
histological type |
|||||||
AC |
23 |
277/1191 |
96/1451 |
68.8 |
random |
5.39 (2.89–10.06) |
< 0.001 |
SCC |
25 |
348/1156 |
100/1503 |
42.7 |
fixed |
5.66 (4.38–7.33) |
< 0.001 |
SmCC |
8 |
24/101 |
22/587 |
26.5 |
fixed |
6.74 (3.41–13.35) |
< 0.001 |
ASC |
3 |
1/21 |
6/203 |
1.3 |
fixed |
3.04 (0.48–19.47) |
0.240 |
LCC |
7 |
1/18 |
14/505 |
0.0 |
fixed |
3.68 (0.53–25.31) |
0.186 |
clinical stage |
|||||||
I-II |
12 |
226/984 |
84/874 |
48.0 |
fixed |
3.53 (2.58–4.84) |
< 0.001 |
III-IV |
11 |
167/536 |
84/836 |
26.3 |
fixed |
4.97 (3.60–6.86) |
< 0.001 |
differentiated grade |
|||||||
well |
5 |
18/95 |
10/272 |
0.0 |
fixed |
4.66 (1.93–11.24) |
0.001 |
moderate & low |
4 |
134/369 |
10/262 |
0.0 |
fixed |
15.46 (7.90–30.27) |
< 0.001 |
Abbreviations: Case(n/N), Case (number of HPV positive cases/number of cases); Control (n/N), Control (number of HPV positive controls/number of controls); PCR, Polymerase chain reaction; ISH, In situ hybridization; SB, Southern blot; DB, Dot blot; BMSM, Bead-based multiplex serology method; LBMA, Multiplex liquid bead microarray antibody assay; FFPE tissue, Formalin fixed and paraffin embedded tissue; AC, Adenocarcinoma; SCC, Squamous cell carcinoma; SmCC, Small cell carcinoma; ASC, Adenosquamous carcinoma; LCC, Large cell carcinoma. Fixed model used Mantel-Haenszel method, random model used DerSimonian-Laird method.
Meta regression
In single covariate meta-regression, study design, continent, HPV detection method, material, histological type were significant study-level covariates. However, in multi-covariates meta-regression, all the covariates were not significant study-level covariates (data not shown).
Sensitivity analysis and publication bias
Sensitivity analysis using fixed effects model revealed that there was no significant difference between the studies, and that the effect of a single study removed on the combined results was not significantly changed. When the pooled effect size was compared between fixed effects model (pooled OR 95% CI: 1.82 (1.69–1.97), P < 0.001) and random effects model (pooled OR 95% CI: 3.64 (2.60–5.08), P < 0.001), we found the results of the two models were different, indicating that the small sample studies had an effect on combined effect. Therefore, after we excluded the studies with sample size of case group or control group less than 100, the pooled effect size of fixed effects model (pooled OR 95% CI: 1.49 (1.37–1.63), P < 0.001) was similar with random effects model (pooled OR 95% CI: 1.87 (1.19–2.95), P = 0.007). We used iterative methods to estimate the number of missing studies, and 15 studies were trimmed and filled with recalculating of pooled OR and 95% CI (Figure 3). The recalculating pooled effect size of fixed effects model (pooled OR 95% CI: 1.49 (1.37–1.62), P < 0.001) and that of random effects model (pooled OR 95% CI: 1.71 (1.22–2.39), P = 0.002) did not occur significantly reversed which meant the results of the meta-analysis were robust. It was less likely that the results would change with new studies reported in the future.
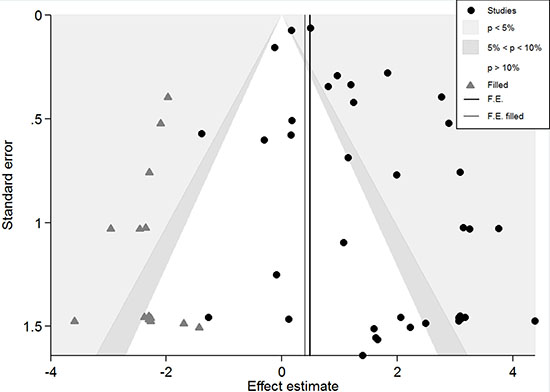
Figure 3: Contour-enhanced meta-analysis funnel plots. The vertical black line shows the pooled log odds ratio on the original meta-analysis, while the vertical grey line shows the pooled estimate including the filled studies.
Although some asymmetry occurred in the contour-enhanced funnel plots (Figure 3), Beggs’ rank correlation test suggested no significant publication bias existed (Pcontinuity corrected = 0.796). However, the result of Harbord’s modified linear regression test (P = 0.001) and Peters’ regression test (P = 0.011) were significant. Furthermore, the limited number of studies (n = 36) indicated a potential publication bias. In Figure 3, trim and fill estimated that 15 studies were missing, all of which indicated those infected HPV were at a reduced risk of lung cancer and eight of which were in the region of P > 0.10. Hence, it was plausible that publication bias was a part of the cause of the observed asymmetry in this funnel plot. However, seven of 15 studies were in the region of P < 0.05, then confounding factors that cause systematic differences in the results of large and small studies was a likely cause of the funnel asymmetry. Nfs0.05 = 2326, which was much larger than the number of eligible studies. Even if there was a publication bias, the results were still relatively stable.
DISCUSSION
HPV is a non-coated double-stranded epitheliotropic DNA virus [47]. There are more than 150 types of HPV transmitted through the skin and / or sexual contact [48]. There are three hypotheses regarding the pathogenesis of HPV infection in thoracic visceral lungs (Figure 4): (1) transmission through the cervical lesion to the lung, (2) high-risk sexual behavior from the infected reproductive system to the mouth and then through the throat into the lungs, (3) through the air to the respiratory system and the lungs. Iwamasa et al. reports that approximately 80% of HPV-infected women with lung cancer have cervical intraepithelial neoplasia [49]. The same HPV 16/18 DNA sequence can be detected in cervical smears, peripheral blood lymphocytes, and lung cancer [19], suggesting that HPV is likely to be transported from the cervix to the lung tissue. The lung is rich with endothelium, which can capture the virus and lead to lung cancer [50]. HPV can also be transmitted mouth to mouth or mouth to genitalia. A survey study of 222 men and their female partners finds that the male oral HPV infection rate is 7.2%, and the majority of the female partners of HPV-infected males have either oral or genital HPV infection [51]. Thus, HPV in oral cavity foci may transmit through the throat into the lungs. Carpagnano et al. [26] are the first to report the presence of HPV DNA in exhaled breath condensate samples obtained from patients with lung cancer, suggesting that HPV reaches the lungs through respiratory gas flow. Thus, HPV infection may be transmitted through inhalation.
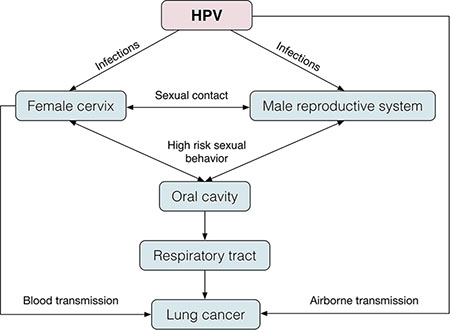
Figure 4: The pathogenesis of HPV infection in thoracic visceral lungs. (1) Transmission through the cervical lesion to the lung, (2) high-risk sexual behavior from the infected reproductive system to the mouth and then through the throat into the lungs, (3) through the air to the respiratory system and the lungs.
The molecular mechanism of HPV infection leading to lung cancer has in recent years been an active research field, and a number of reviews have described the pathogenesis in detail [52–56]. HPV E6 and E7 oncogene proteins can regulate the expression of multiple target genes and proteins such as p53, pRb, HIF-1α, VEGF, IL-6, IL-10, Mcl-1, Bcl-2, cIAP-2, EGFR, FHIT, hTERT, HER-2, ALK, ROS1 and AhR to promote lung cell proliferation, angiogenesis and cell immortalization through various signaling pathways [56–60] (Figure 5). Therefore, in HPV-associated lung cancers, these target genes and proteins may be potential therapeutic targets.
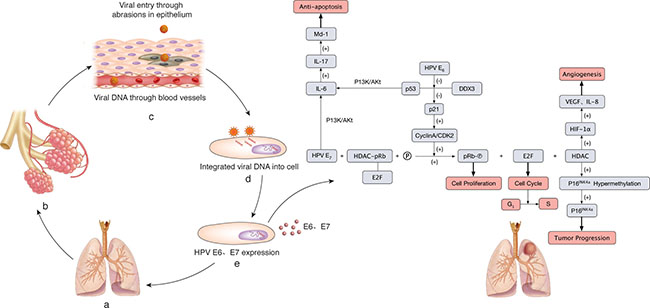
Figure 5: The molecular mechanism of HPV infection leading to lung cancer. (A–B) Normal structure of lung and alveoli. (C) HPV DNA enters the lung epithelial cells through blood vessels and pulmonary lumina. (D) HPVs are recognized by membrane receptors, and viral DNA is integrated into the host cells. (E) The expression of HPV E6 and E7 oncogene proteins plays an important role in carcinogenesis. HPV E6 inhibits p53 interaction with DDX3, following p21 inactivation. Thus, the complex cyclin A/CDK2 is free to phosphorylate pRb, which promotes cell proliferation, and the E2F transcription factor is released and determines the cell cycle and G1/S transition. E7 HPV resolves the HDAC/pRb/E2F complex by interacting with pRb. Hence, HDAC is released to hypermethylate p16INK4 and inhibits the expression of p16INK4, which leads to tumor progression. HDAC can also cause angiogenesis induced by VEGF and IL-8 through HIF-1α. HPV E7 and inactivated p53 by HPV E6 can up-regulate Mcl-1 through the PI3K/Akt-(IL-6)-(IL-17) pathway, resulting in anti-apoptosis.
Growing evidence supports the link between HPV infection and lung cancer, but the relationship is still debatable. To date, seven independent systematic reviews and meta-analyses [10, 61–66] have evaluated and incorporated existing research evidence that HPV may be a risk factor for lung cancer. However, the studies above do not include the results of longitudinal studies (such as nested case-control and cohort studies) with high causal inference, and it is not clear that HPV infection had a causal link with lung cancer. In this paper, we present the prospective nested case-control studies and cohort studies of HPV infection and lung cancer for the first time to provide meta-analysis. The result suggests that HPV infection increase the risk of lung cancer, pooled OR and 95% CI: 3.64 (2.60–5.08). Zhai et al. [66] analyze the case-control studies of HPV infection and lung cancer and find that the combined OR is 5.67 (95% CI: 3.09–10.40, P < 0.001). Moreover, an international pooled analysis about HPV-associated lung cancers shows that pooled OR is 3.86 (95% CI: 2.87–5.19) [64]. However, allogeneic case-control studies and self-matched case-control studies are difficult to determine the time sequence. Individuals suffering from lung cancer with lower immunity are more susceptible to HPV, which may lead to false causal association. The pooled OR of this study is smaller, which is possibly due to the inclusion of nested case-control studies leading to weak correlations. The pooled OR of allogeneic case-control studies is significantly higher than that of nested case-control studies, and HPV infection do not increase the risk of primary lung cancer in nested case-control studies. The lack of association between HPV antibody positivity and increased risk of lung cancer can be explained as a high level of serum HPV antibodies reflecting a strong host immune response that prevents the recurrence or reactivation of HPV infection and thereby hinders the development of HPV-associated lung cancer [44]. This hypothesis should be explored and verified.
At present, the conclusion of HPV infection and lung cancer is still inconsistent. The possible influencing factors are: research population, test samples, sample processing methods and detection methods [42]. Therefore, the effect of HPV infection on lung cancer is discussed from the aspects of research area, gender, smoking status, detection method, HPV subtype, material, histological type, clinical stage and histological differentiation. The results of subgroup analyses suggest that research area, gender, smoking status, HPV subtype, histological type, clinical stage and histological differentiation may be the sources of total heterogeneity. The prevalence of HPV infection in lung cancer patients is quite different in published studies which may be due to geographical differences. A meta-analysis shows that the average HPV infection rate of lung cancer in the world is 26.5%, the lowest in North America (12.5%), the highest in China (including Taiwan) (37.7%), followed by other Asian regions (17.2%), and the result of meta regression suggests that there may be a high incidence area of HPV infection in lung cancer (P = 0.02) [62]. According to our subgroup analysis of the continent, the pooled OR of Asian is higher than European and American. It is closely related to the higher positive rate of HPV in lung cancer tissues in Asia (28.1[63]-35.7%[61]) than in other continents. HPV is a well-known carcinogen in a particularly virulent form of head and neck cancer in never smokers. We find that HPV-infected non-smokers (OR = 6.51, 95% CI: 3.78–11.21) have a higher risk of lung cancer than smokers. A meta-analysis of four case-control studies shows pooled OR in never-smokers is 4.78 (95% CI: 2.25–10.15) [65], which is similar to our results. Reported prevalence of HPV infection among non-smoking lung cancer patients in Asia [67] and Europe [63] is significantly higher than that among smoking lung cancer patients, but some studies find that there is no statistically significant difference of HPV infection rate in smokers and non-smokers [46, 63]. Whether HPV infection has synergistic effect with smoking on carcinogenesis remains controversial. The combined ORs of tissue detection methods (PCR, ISH, SB/DB and sequencing) are generally higher than those of serological detection methods (LBMA and BMSM), possibly due to the low amount of HPV in the blood circulation and the low sensitivity and specificity of serological detection methods. The sensitivity and false positive rate of PCR are higher than other methods [64, 68]. However, we do not find the pooled OR of PCR is higher than other methods, resulting from the selection of primers and the small sample sizes of other detection methods. In this study, HPV 16, HPV 18 and HPV 11 infection significantly increase the risk of lung cancer, while HPV 6 and HPV 31 infection are not significantly associated with lung cancer. A meta-analysis suggests that the average infection rates of HPV 16 and HPV 18 in lung cancer patients are 19.80% and 18.59%, compared with non-cancer controls, the combined ORs are 5.84 (95% CI: 3.14–10.86) and 4.29 (95% CI: 2.34–7.86) [66]. There is no significant difference of carcinogenic risk between HPV 16 and HPV 18 in lung cancer [66]. It is generally believed that low-risk types of HPV lead to benign lesions without the potential for malignance [69]. However, the role of HPV 11 and HPV 31 in lung cancer remains unclear, and the association between HPV subtype and lung cancer is worthy of further study. HPV replicates when infected keratinocytes are differentiated and does not release virus particles into the blood [70]. Therefore, we find that the combined OR of tissue is significantly higher than that of blood. The point estimated OR of lung squamous cell carcinoma (5.66) is slightly higher than that of lung adenocarcinoma (5.39). Because of the affinity to squamous cell, HPV infection rate of squamous cell carcinoma is higher than that of adenocarcinoma. The result is consistent with the results of Syrjänen [62] and Zhai [66]. In addition to traditional squamous cell carcinoma, we also find that HPV infection may be associated with adenocarcinoma and small cell carcinoma. Limited to the number of studies, the association with adenosquamous carcinoma and large cell carcinoma has not been found. The association between HPV and other histopathological types of lung cancer needs further study.
In this article, we ensure the high recall ratio through multi-databases and multi- approaches, and improve the precision ratio with the strict inclusion and exclusion criteria. Eligible studies are selected by two people who paid attention to control the quality as much as possible to reduce the search bias. Subgroup and sensitivity analyses show that the result of meta-analysis is stable and the conclusion is reliable. However, in the process of meta-analysis, there are still some limitations: (1) Potential bias cannot be completely ruled out, because HPV infection depends largely on the sensitivity, specificity and HPV subtype of detection methods. Subgroup analysis can explain partial bias, but there are still unknown bias. (2) There is a slight publication bias. According to the funnel plot, there is still a lack of small samples and no statistically significance unpublished articles. (3) There may be multiple publication bias, because it is difficult to distinguish whether a study published repeatedly.
In summary, our meta-analysis indicates that HPV infection, especially HPV 16 and 18, increases lung cancer risk, particularly in squamous cell carcinoma and small cell carcinoma. The development of international standard laboratory contributes to the favorable combination of multi-center experimental results and increases the reliability of causal inference. Case-control studies are difficult to determine the time sequence, so well-designed cohort study or randomized controlled trial urgent need to clarify the relationship between HPV and lung cancer. Although HPV vaccines can theoretically prevent the development of lung cancer, future research needs to focus attention toward whether an HPV vaccine can effectively reduce the incidence of lung cancer.
MATERIALS AND METHODS
Search strategy
We identified eligible studies either in English or Chinese published up to Feb 28, 2017 by searching the MEDLINE (PubMed), Embase (OVID) and Web of Science. Search terms were “human papillomavirus”, “HPV”, “lung carcinoma”, “lung neoplasm” and “lung lesions”. The search was limited to studies that had been conducted on human subjects. Meeting abstracts were excluded because of limited data they offered. Reference lists of the retrieved articles, reviews and editorials were also screened to find all additional eligible studies. This meta-analysis was performed in accordance with PRISMA guidelines.
Study selection and inclusion criteria
The studies selected had to meet the following criteria: (1) case–control or cohort studies compared HPV infection among lung neoplasms patients and non-cancer controls; (2) histological diagnosis of cases and controls were established; (3) sufficient information was provided to calculate OR or RR with 95% CI; (4) there were no restrictions based on patients’ nationality, ethnicity or gender; (5) when an overlap of patients was found in several studies, only the study with the largest sample size and detailed information or the study that met the above criteria was included.
Literature evaluation and data extraction
An initial screening of the title and abstract was performed in the first step, followed by a further screening based on a full text review. Information was independently extracted from all eligible publications by two investigators (Wei-min Xiong and Fei He), and discrepancies were resolved through discussion or via a third researcher. Literatures quality evaluation were evaluated using the Newcastle-Ottawascale (NOS) scale [71]. For studies meeting our inclusion criteria, the following data were collected: first author, publication year, country of study, specimen type, histological type, HPV detection method, HPV types, basic situation of case / exposure group and control / non-exposure group and numbers of HPV positive and negative subjects in tumors and control groups.
Statistical analysis
When sufficient data were available, a meta-analysis was performed and ORs or RRs with corresponding 95% CIs were calculated. If there are no events in either the case or control arms of the trial, the trial should be discarded from the meta-analysis [72]. Heterogeneity among studies was examined using the Cochran’s Q test by calculating the P value and I2 value[73]. If I2 is less than or equal to 50%, that suggested that it was homogeneity and the fixed effects model (Mantel-Haenszel method [74]) of meta-analysis was performed; if I2 > 50%, which means there is a statistical heterogeneity between the study results and the random effects model (DerSimonian-Laird method [75]) should be chosen [66].
Moreover, we did pre-specified exploratory meta-regression and subgroup analyses to investigate the effect of selected study and participant characteristics on the results, including study design, research area, gender, smoking status, detection methods, HPV subtypes, material, histological type, clinical stage and tissue differentiation. Sensitivity analysis by sequential omission of individual studies and trim and fill method [76] with recalculating of pooled OR/RRs and 95% CIs was conducted to test the meta-analysis results of stability. Using Contour-enhanced funnel plots (confunnel with filled studies from metatrim) [77], Beggs’ rank correlation test [78], Harbord’s modified linear regression test [79] and Peters’ regression test [80] to detect funnel plot asymmetry and analyze potential publication bias. Rosenthal fail-safe number (Nfs) was also calculated to estimate the degree of publication bias and the meta-analysis results of stability [81]. Nfs0.05 = (Σz/1.64)2 - K, where z is the z value of each independent study and K is the number of studies. When Nfs > 5K + 10, it is judged that there is no publication bias [82].
All statistical tests were performed with the Stata 13.0 (Stata Corporation, College Station, TX, USA). All above analyses were two-sided test and the significance level was 0.05.
Abbreviations
HPV, human papillomavirus; CI, confidence intervals; PCR, polymerase chain reaction; ISH, in situ hybridization; SB/DB, southern blot/dot blot; BMSM, bead-based multiplex serology method; LBMA, multiplex liquid bead microarray antibody assay; Nfs, Rosenthal fail-safe number.
Author contributions
All authors have made substantial contributions to the conception and design of the study. WX performed the protocol design, search, data extraction, quality assessment, data analysis and drafted the manuscript. FH contributed to protocol design, search, data extraction and quality assessment. WX and QX have made substantial contributions to charts making and have revised the manuscript critically. XL and RX performed the search and data collection. FH and LC conceived the project, guided the work, and wrote the manuscript. All authors read and approved the final manuscript.
ACKNOWLEDGMENTS
None.
CONFLICTS OF INTEREST
The authors disclose no conflicts of interest.
FUNDING
This study was supported by the National Natural Science Foundation of China [grant number 81402738], the Ph.D. Fund Project of Fujian Medical University [grant number 2014MP006], Fujian Provincial Health and Family Planning Commission Youth Research Project [grant number 2014-1-37], Fujian Provincial Natural Science Foundation Project [grant number 2016J01355].
REFERENCES
1. Stewart BW, Wild C, International Agency for Research on Cancer and World Health Organization. (2014). World cancer report. 2014.
2. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87–108.
3. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66:115–132.
4. de Martel C, Ferlay J, Franceschi S, Vignat J, Bray F, Forman D, Plummer M. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lance Oncol. 2012; 13:607–615.
5. Crosbie EJ, Einstein MH, Franceschi S, Kitchener HC. Human papillomavirus and cervical cancer. Lancet. 2013; 382:889–899.
6. Grulich AE, Jin F, Conway EL, Stein AN, Hocking J. Cancers attributable to human papillomavirus infection. Sexual Health. 2010; 7:244–252.
7. De Flora S, La Maestra S. Epidemiology of cancers of infectious origin and prevention strategies. J Prevent Med Hyg. 2015; 56:E15–20.
8. Tommasino M. The human papillomavirus family and its role in carcinogenesis. Sem Cancer Biol. 2014; 26:13–21.
9. Syrjanen KJ. Condylomatous changes in neoplastic bronchial epithelium: report of a case. Respiration. 1979; 38:299–304.
10. Srinivasan M, Taioli E, Ragin CC. Human papillomavirus type 16 and 18 in primary lung cancers--a meta-analysis. Carcinogenesis. 2009; 30:1722–1728.
11. Bejui-Thivolet F, Liagre N, Chignol MC, Chardonnet Y, Patricot LM. Detection of human papillomavirus DNA in squamous bronchial metaplasia and squamous cell carcinomas of the lung by in situ hybridization using biotinylated probes in paraffin-embedded specimens. Hum Pathol. 1990; 21:111–116.
12. Li Q, Hu K, Pan X, Cao Z, Yang J, Hu S. Detection of human papillomavirus types 16, 18 DNA related sequences in bronchogenic carcinoma by polymerase chain reaction. Chin Med J. 1995; 108:610–614.
13. Yang Y, Dong D, Peng L, Ling J, Xiao Y, Zhuang H. [A study on the relationship between HPV infection and the oncogenesis of primary squamous carcinoma of the lung.] [Article in Chinese]. Zhongguo fei ai za zhi. 1998; 1:35–36.
14. Niyaz H, Zhao C, Li Y. [Detection and significance of HPV16, 18 infection, P53 overexpression and telomerase activity in patients with lung cancer]. [Article in Chinese]. Zhonghua jie he he hu xi za zhi. 2000; 23:679–682.
15. Cheng YW, Chiou HL, Sheu GT, Hsieh LL, Chen JT, Chen CY, Su JM, Lee H. The association of human papillomavirus 16/18 infection with lung cancer among nonsmoking Taiwanese women. Cancer Res. 2001; 61:2799–2803.
16. Chiou HL, Wu MF, Liaw YC, Cheng YW, Wong RH, Chen CY, Lee H. The presence of human papillomavirus type 16/18 DNA in blood circulation may act as a risk marker of lung cancer in Taiwan. Cancer. 2003; 97:1558–1563.
17. Cheng YW, Chiou HL, Chen JT, Chou MC, Lin TS, Lai WW, Chen CY, Tsai YY, Lee H. Gender difference in human papillomarvirus infection for non-small cell lung cancer in Taiwan. Lung Cancer. 2004; 46:165–170.
18. Jain N, Singh V, Hedau S, Kumar S, Daga MK, Dewan R, Murthy NS, Husain SA, Das BC. Infection of human papillomavirus type 18 and p53 codon 72 polymorphism in lung cancer patients from India. Chest. 2005; 128:3999–4007.
19. Fei Y, Yang J, Hsieh WC, Wu JY, Wu TC, Goan YG, Lee H, Cheng YW. Different human papillomavirus 16/18 infection in Chinese non-small cell lung cancer patients living in Wuhan, China. Jpn J Clin Oncol. 2006; 36:274–279.
20. Nadji SA, Mokhtari-Azad T, Mahmoodi M, Yahyapour Y, Naghshvar F, Torabizadeh J, Ziaee AA, Nategh R. Relationship between lung cancer and human papillomavirus in north of Iran, Mazandaran province. Cancer Lett. 2007; 248:41–46.
21. Buyru N, Altinisik J, Isin M, Dalay N. p53 codon 72 polymorphism and HPV status in lung cancer. Med Sci Mon. 2008; 14:Cr493–497.
22. Wang Y, Wang A, Jiang R, Pan H, Huang B, Lu Y, Wu C. Human papillomavirus type 16 and 18 infection is associated with lung cancer patients from the central part of China. Oncol Rep. 2008; 20:333–339.
23. Xu Y, Cheng B, Pan H, Wu A, Zhang L. [The Relationship between the Status of Human Papillomavirus 16/18 Infection and the Expression of Bcl-2 and Bax in Squamous Cell Carcinomas of the Lung.] [Article in Chinese]. Zhongguo fei ai za zhi. 2009; 12:849–852.
24. Yu Y, Yang A, Hu S, Yan H. Correlation of HPV-16/18 infection of human papillomavirus with lung squamous cell carcinomas in Western China. Oncol Rep. 2009; 21:1627–1632.
25. Wang YH, Chen DJ, Yi TN, Liu XH. The relationship among human papilloma virus infection, survivin, and p53 gene in lung squamous carcinoma tissue. Saudi Med J. 2010; 31:1331–1336.
26. Carpagnano GE, Koutelou A, Natalicchio MI, Martinelli D, Ruggieri C, Di Taranto A, Antonetti R, Carpagnano F, Foschino-Barbaro MP. HPV in exhaled breath condensate of lung cancer patients. Br J Cancer. 2011; 105:1183–1190.
27. Gatta LB, Balzarini P, Tironi A, Berenzi A, Benetti A, Angiero F, Grigolato P, Dessy E. Human papillomavirus DNA and p16 gene in squamous cell lung carcinoma. Anticancer Res. 2012; 32:3085–3089.
28. Yu Y, Yang A, Hu S, Zhang J, Yan H. Significance of human papillomavirus 16/18 infection in association with p53 mutation in lung carcinomas. Clin Respir J. 2013; 7:27–33.
29. Sarchianaki E, Derdas SP, Ntaoukakis M, Vakonaki E, Lagoudaki ED, Lasithiotaki I, Sarchianaki A, Koutsopoulos A, Symvoulakis EK, Spandidos DA, Antoniou KM, Sourvinos G. Detection and genotype analysis of human papillomavirus in non-small cell lung cancer patients. Tumour Biol. 2014; 35:3203–3209.
30. Yu Y, Liu X, Yang Y, Zhao X, Xue J, Zhang W, Yang A. Effect of FHIT loss and p53 mutation on HPV-infected lung carcinoma development. Epidemiol Health. 2015; 10:392–398.
31. Fan R, Hou WJ, Zhao YJ, Liu SL, Qiu XS, Wang EH, Wu GP. Overexpression of HPV16 E6/E7 mediated HIF-1alpha upregulation of GLUT1 expression in lung cancer cells. Tumour Biol. 2016; 37:4655–4663.
32. Gupta P, Haldar D, Naru J, Dey P, Aggarwal AN, Minz RW, Aggarwal R. Prevalence of human papillomavirus, Epstein-Barr virus, and cytomegalovirus in fine needle aspirates from lung carcinoma: A case-control study with review of literature. Diagnost Cytopathol. 2016.
33. Lu Y, Yu LQ, Zhu L, Zhao N, Zhou XJ, Lu X. Expression of HIF-1alpha and P-gp in non-small cell lung cancer and the relationship with HPV infection. Oncol Lett. 2016; 12:1455–1459.
34. Robinson LA, Jaing CJ, Pierce Campbell C, Magliocco A, Xiong Y, Magliocco G, Thissen JB, Antonia S. Molecular evidence of viral DNA in non-small cell lung cancer and non-neoplastic lung. Br J Cancer. 2016; 115:497–504.
35. Fong KM, Schonrock J, Frazer IM, Zimmerman PV, Smith PJ. Human papillomavirus not found in squamous and large cell lung carcinomas by polymerase chain reaction. Cancer. 1995; 75:2400–2401.
36. Ciotti M, Giuliani L, Ambrogi V, Ronci C, Benedetto A, Mineo TC, Syrjanen K, Favalli C. Detection and expression of human papillomavirus oncogenes in non-small cell lung cancer. Oncol Rep. 2006; 16:183–189.
37. Giuliani L, Jaxmar T, Casadio C, Gariglio M, Manna A, D’Antonio D, Syrjanen K, Favalli C, Ciotti M. Detection of oncogenic viruses SV40, BKV, JCV, HCMV, HPV and p53 codon 72 polymorphism in lung carcinoma. Lung Cancer. 2007; 57:273–281.
38. Joh J, Jenson AB, Moore GD, Rezazedeh A, Slone SP, Ghim SJ, Kloecker GH. Human papillomavirus (HPV) and Merkel cell polyomavirus (MCPyV) in non small cell lung cancer. Exp Mol Pathol. 2010; 89:222–226.
39. Krikelis D, Tzimagiorgis G, Georgiou E, Destouni C, Agorastos T, Haitoglou C, Kouidou S. Frequent presence of incomplete HPV16 E7 ORFs in lung carcinomas: memories of viral infection. J Clin Virol. 2010; 49:169–174.
40. Galvan A, Noci S, Taverna F, Lombardo C, Franceschi S, Pastorino U, Dragani TA. Testing of human papillomavirus in lung cancer and non-tumor lung tissue. BMC Cancer. 2012; 12:512.
41. Sagerup CM, Nymoen DA, Halvorsen AR, Lund-Iversen M, Helland A, Brustugun OT. Human papilloma virus detection and typing in 334 lung cancer patients. Acta Oncol. 2014; 53:952–957.
42. Xiong WM, He F, Xiao RD, Yu TT, Zhang X, Liu ZQ, Xu QP, Cai L. [Association between human papillomavirus infection and lung cancer]. [Article in Chinese]. Zhonghua liu xing bing xue za zhi. 2016; 37:1658–1661.
43. Simen-Kapeu A, Surcel HM, Koskela P, Pukkala E, Lehtinen M. Lack of association between human papillomavirus type 16 and 18 infections and female lung cancer. Cancer Epidemiol Biomark Prevent. 2010; 19:1879–1881.
44. Colombara DV, Manhart LE, Carter JJ, Hawes SE, Weiss NS, Hughes JP, Barnett MJ, Goodman GE, Smith JS, Qiao YL, Galloway DA. Prior human polyomavirus and papillomavirus infection and incident lung cancer: a nested case-control study. Cancer Cause Con. 2015; 26:1835–1844.
45. Colombara DV, Manhart LE, Carter JJ, Hawes SE, Weiss NS, Hughes JP, Qiao YL, Taylor PR, Smith JS, Galloway DA. Absence of an association of human polyomavirus and papillomavirus infection with lung cancer in China: a nested case-control study. BMC Cancer. 2016; 16:342.
46. Anantharaman D, Gheit T, Waterboer T, Halec G, Carreira C, Abedi-Ardekani B, McKay-Chopin S, Zaridze D, Mukeria A, Szeszenia-Dabrowska N, Lissowska J, Mates D, Janout V, et al. No causal association identified for human papillomavirus infections in lung cancer. Cancer Res. 2014; 74:3525–3534.
47. Psyrri A, Boutati E, Karageorgopoulou S. Human papillomavirus in head and neck cancers: biology, prognosis, hope of treatment, and vaccines. Anti-Cancer Drugs. 2011; 22:586–590.
48. Bernard HU, Burk RD, Chen Z, van Doorslaer K, zur Hausen H, de Villiers EM. Classification of papillomaviruses (PVs) based on 189 PV types and proposal of taxonomic amendments. Virology. 2010; 401:70–79.
49. Iwamasa T, Miyagi J, Tsuhako K, Kinjo T, Kamada Y, Hirayasu T, Genka K. Prognostic implication of human papillomavirus infection in squamous cell carcinoma of the lung. Pathol Res Prac. 2000; 196:209–218.
50. Lin FC, Huang JY, Tsai SC, Nfor ON, Chou MC, Wu MF, Lee CT, Jan CF, Liaw YP. The association between human papillomavirus infection and female lung cancer: A population-based cohort study. Medicine. 2016; 95:e3856.
51. Dahlstrom KR, Burchell AN, Ramanakumar AV, Rodrigues A, Tellier PP, Hanley J, Coutlee F, Franco EL. Sexual transmission of oral human papillomavirus infection among men. Cancer Epidemiol Bio Prevent. 2014; 23:2959–2964.
52. Rezazadeh A, Laber DA, Ghim SJ, Jenson AB, Kloecker G. The role of human papilloma virus in lung cancer: a review of the evidence. Am J Med Sci. 2009; 338:64–67.
53. Prabhu PR, Jayalekshmi D, Pillai MR. Lung Cancer and Human Papilloma Viruses (HPVs): Examining the Molecular Evidence. J Oncol. 2012; 2012:750270.
54. Zhang EY, Tang XD. Human papillomavirus type 16/18 oncoproteins: potential therapeutic targets in non-smoking associated lung cancer. Asian Pac J Cancer Prevent. 2012; 13:5363–5369.
55. Pallis AG, Syrigos KN. Lung cancer in never smokers: disease characteristics and risk factors. Crit Rev Oncol Hematol. 2013; 88:494–503.
56. de Freitas AC, Gurgel AP, de Lima EG, de Franca Sao Marcos B, do Amaral CM. Human papillomavirus and lung cancinogenesis: an overview. J Cancer Res Clin Oncol. 2016.
57. Li G, He L, Zhang E, Shi J, Zhang Q, Le AD, Zhou K, Tang X. Overexpression of human papillomavirus (HPV) type 16 oncoproteins promotes angiogenesis via enhancing HIF-1alpha and VEGF expression in non-small cell lung cancer cells. Cancer Lett. 2011; 311:160–170.
58. Zhang E, Feng X, Liu F, Zhang P, Liang J, Tang X. Roles of PI3K/Akt and c-Jun signaling pathways in human papillomavirus type 16 oncoprotein-induced HIF-1alpha, VEGF, and IL-8 expression and in vitro angiogenesis in non-small cell lung cancer cells. PLoS One. 2014; 9:e103440.
59. Liu F, Lin B, Liu X, Zhang W, Zhang E, Hu L, Ma Y, Li X, Tang X. ERK Signaling Pathway Is Involved in HPV-16 E6 but not E7 Oncoprotein-Induced HIF-1alpha Protein Accumulation in NSCLC Cells. Oncol Res. 2016; 23:109–118.
60. Willey JC, Broussoud A, Sleemi A, Bennett WP, Cerutti P, Harris CC. Immortalization of normal human bronchial epithelial cells by human papillomaviruses 16 or 18. Cancer Res. 1991; 51:5370–5377.
61. Klein F, Amin Kotb WF, Petersen I. Incidence of human papilloma virus in lung cancer. Lung Cancer. 2009; 65:13–18.
62. Syrjanen K. Detection of human papillomavirus in lung cancer: systematic review and meta-analysis. Anticancer Res. 2012; 32:3235–3250.
63. Hasegawa Y, Ando M, Kubo A, Isa S, Yamamoto S, Tsujino K, Kurata T, Ou SH, Takada M, Kawaguchi T. Human papilloma virus in non-small cell lung cancer in never smokers: a systematic review of the literature. Lung Cancer. 2014; 83:8–13.
64. Ragin C, Obikoya-Malomo M, Kim S, Chen Z, Flores-Obando R, Gibbs D, Koriyama C, Aguayo F, Koshiol J, Caporaso NE, Carpagnano GE, Ciotti M, Dosaka-Akita H, et al. HPV-associated lung cancers: an international pooled analysis. Carcinogenesis. 2014; 35:1267–1275.
65. Bae JM, Kim EH. Human papillomavirus infection and risk of lung cancer in never-smokers and women: an ‘adaptive’ meta-analysis. Epidemiol Health. 2015; 37:e2015052.
66. Zhai K, Ding J, Shi HZ. HPV and lung cancer risk: a meta-analysis. J Clin Virol. 2015; 63:84–90.
67. Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011; 32:605–644.
68. Kimple AJ, Torres AD, Yang RZ, Kimple RJ. HPV-associated head and neck cancer: molecular and nano-scale markers for prognosis and therapeutic stratification. Sensors. 2012; 12:5159–5169.
69. zur Hausen H. Papillomaviruses in the causation of human cancers - a brief historical account. Virology. 2009; 384:260–265.
70. Read SA, Douglas MW. Virus induced inflammation and cancer development. Cancer Lett. 2014; 345:174–181.
71. Wells GA, Shea BJ, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Appl Engineer Agri. 2000; 18:págs. 727–734.
72. Sterne JA, Bradburn MJ, Egger M. Meta–Analysis in Stata™: BMJ. 2001.
73. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21:1539–1558.
74. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Nat Cancer Inst. 1959; 22:719–748.
75. DerSimonian R, Laird N. Meta-analysis in clinical trials. Contr Clin Trials. 1986; 7:177–188.
76. Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56:455–463.
77. Palmer TM, Peters JL, Sutton AJ, Moreno SG. Contour-enhanced funnel plots for meta-analysis. Stata Journal. 2009; 8:242–254.
78. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994; 50:1088–1101.
79. Harbord RM, Egger M, Sterne JA. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med. 2006; 25:3443–3457.
80. Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Comparison of two methods to detect publication bias in meta-analysis. JAMA. 2006; 295:676–680.
81. Rosenthal R. The file drawer problem and tolerance for null results. Psychol Bull. 1979; 86:638–641.
82. Hoeve M, Stams GJ, van der Put CE, Dubas JS, van der Laan PH, Gerris JR. A meta-analysis of attachment to parents and delinquency. J Abnorm Child Psychol. 2012; 40:771–785.