
INTRODUCTION
The curative treatment modalities for hepatocellular carcinoma (HCC) include liver transplantation, surgical resection (SR), and radiofrequency ablation (RFA). Although liver transplantation is the best treatment option for patients with HCC, SR and RFA are most commonly considered first-line treatments because of the graft shortage. Numerous studies suggest both SR and RFA are comparable in terms of long-term survival for patients with early stage HCC. The 5-year survival rates are 42%–56% for SR and 42%–70% for RFA [1–6]. However, even in patients who underwent liver transplantation, tumor recurrence is not uncommon with a 10%–15% risk of recurrence [7]. The 5-year recurrence rate after SR is 42%–52% [8–11], which is higher up to 42%–70% after RFA [12, 13]. Therefore, how to manage recurrent HCC is important in improving the survival and merits further evaluation. Of all the recurrence patterns, intrahepatic recurrence is the most common and the size of the recurring HCC is usually smaller than that of the initial HCC because the surveillance interval is shorter [14]. Accordingly, the treatment options do not particularly differ between recurrent HCC after SR and primary tumor. Liver transplantation is still recognized as the better choice for recurrent HCC [15], but its wide application has been limited by the shortage of donors. Repeated SR for recurrent HCC has been reported to be an effective treatment option with a comparable survival rate to that of primary SR [16–18], but its feasibility is limited by small liver remnants, poor liver function reserve, or technical difficulties owing to expected postoperative adhesion [19–21]. RFA, as a nonsurgical, less invasive, and repeatable therapeutic approach, is safer and causes less damage in treating recurrent HCC following primary resection [22–24]. As to the choice of repeated SR and RFA, although several studies have compared the clinical outcome of RFA vs. SR for recurrent HCC, no clear recommendation has yet been established. Many of the studies were limited by small case numbers or large tumor size [25–31] and there remain many controversies regarding the choice of repeated SR and RFA in treating recurrent tumor after primary resection. This study aimed to compare the efficacy, safety, and long-term survival of repeated SR and RFA for recurrent HCCs.
MATERIALS AND METHODS
This study was conducted as a retrospective chart review and analysis of a prospective database from the cancer center in our hospital. Our study was approved by the institutional review board of our hospital and informed consent was waived.
Patients
From January 2002 to September 2014, a total of 530 consecutive patients with early and intermediate stage HCC underwent hepatic resection at the Division of General Surgery, Department of Surgery, Kaohsiung Veteran General Hospital. At the time of the data collection and analysis, 271 patients were free of tumor recurrence, 235 patients had intrahepatic recurrence, and 24 patients had extrahepatic recurrence. For matching comparison between repeated surgical resection and RFA, patients with fewer or equal to 3 recurrent tumors and each tumor size less than or equal to 3cm were enrolled. The detailed inclusion and exclusion of patients were shown in Figure 1. Among the 235 patients with intrahepatic recurrence, 100 patients with fewer or equal to 3 recurrent tumors and each tumor size ≦ 3cm received either repeated SR or RFA as the secondary treatment, and these patients were enrolled in our study The data of patient characteristics, clinicopathologic features, and survival outcomes were reviewed.
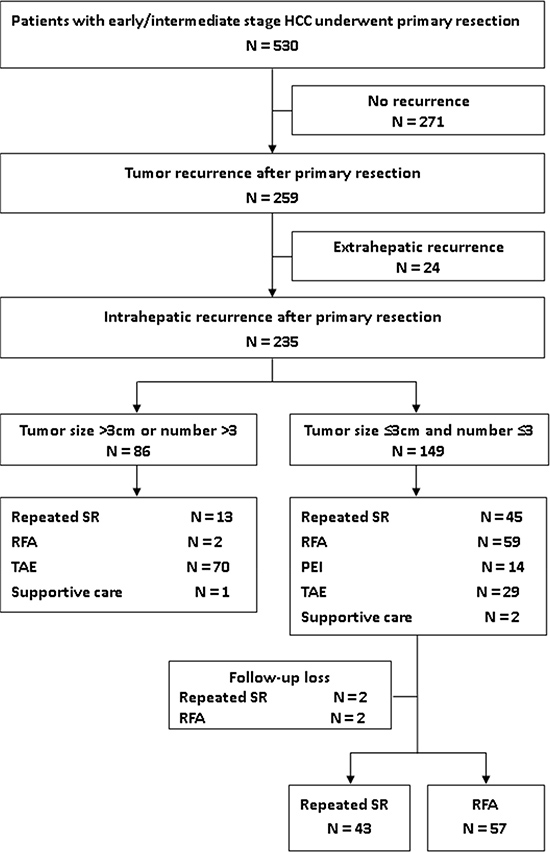
Figure 1: Flowchart summarizes patient inclusion. PEI = percutaneous ethanol injection, RFA = radiofrequency ablation, SR = surgical resection, TAE = transcatheter arterial embolization.
Surveillance and diagnosis for recurrent HCC
In our hospital, all patients received computed tomography (CT) or magnetic resonance imaging (MRI) of the liver within one to two months after primary hepatectomy of the HCC to confirm complete tumor clearance. Thereafter, surveillance for recurrent HCC consisted of measurements of serum alpha-fetoprotein (AFP), liver biochemistry, and ultrasonography, CT scan, or MRI scans of the liver every three months. Intrahepatic recurrence was defined as a new lesion with arterial contrast enhancement and portal venous washout. If there was a new lesion less than 1cm and without typical HCC imaging pattern on contrast-enhanced CT or MRI scans, we arranged image studies every three months. If there was a new lesion more than 1cm and without a typical HCC imaging pattern on contrast-enhanced CT or MRI scans, we would arrange a needle biopsy for histological confirmation.
Treatment strategy selection for recurrent HCC
Neither SR and RFA were adopted for recurrent HCC treatment if a patient had any symptoms and signs of irreversible liver decompensation and severe portal hypertension such as jaundice, ascites, encephalopathy, PTINR >1.5x, the presence of severe varix, and thrombocytopenia with a platelet count < 50 x× 109/Cumm. Repeated hepatic resection was considered if a patient had a single tumor or tumors within a monosegment of liver with good liver function reserve. Repeated hepatic resection was generally avoided if patients had gross ascites, an indocyanine green (ICG) retention rate of more than 20% at 15 minutes and/or a serum total bilirubin level of more than 1.5 mg/dL, or the presence of moderate esophageal varix. RFA was generally selected in patients with Child-Pugh class A or B disease, prothrombin time ratio of more than 50%, and platelet count of more than 50 000/mm3 (50 × 109/L). RFA also was considered if the indocyanine green (ICG) retention rate was more than 20% at 15 minutes or recurrent tumors in a deep-seated intraparenchymal location where anatomical resection would remove more than one segment of liver, resulting in insufficient liver reservation. CT guided RFA was more preferred than sono-guided RFA if the tumor size was small and invisible by sonogram, difficult to approach due to altered anatomy, and tumors in high-risk locations, which was defined as tumors less than 5 mm adjacent to the hollow viscera, big bile duct, gallbladder, diaphragm, liver capsule, liver hilum, heart, major portal or hepatic vein.
Statistical analysis
Continuous variables were expressed as medians and interquartile ranges and were compared using the Mann–Whitney U-test. Categorical variables were compared with the χ2 test or Fisher’s exact test when appropriate. Overall survival, disease-free survival, and cumulative incidence of second recurrence of the two study groups were estimated by the Kaplan-Meier method. Comparison of survival between groups was performed with the log-rank test. Disease-free survival following treatment of the first recurrence of HCC was defined as the period from the date of treatment of the first recurrence of HCC to the date of the second tumor recurrence or death. Overall survival after treatment of the first recurrence of HCC was defined as the period from the date of treatment of the first recurrence to the date of death related to any cause. Univariate and multivariate analyses of prognostic factors with the overall survival were evaluated by step wise forwards Cox’s regression analysis. A p value ≤ 0.05 was considered significant. Statistical analysis was performed using the SPSS 19.0 computer software program.
RESULTS
Baseline profile of primary HCC
Table 1 shows the patient and tumor characteristics of the initial HCC. The age, gender ratio, incidence of comorbidity, and positive rates of viral hepatitis, and laboratory data were comparable in both groups. In the repeated SR group, 35 (81.4%) patients had Child-Pugh class A cirrhosis and 1 (2.3%) had Child-Pugh class B cirrhosis, whereas 50 (87.7%) patients in the RFA group had Child-Pugh class A cirrhosis (p = 0.41). In each group, 7 patients did not have cirrhosis, which was based on radiological finding and Ishak score of non-tumor part in the surgical pathology. The two groups had similar clinico-pathological features of initial HCC in terms of tumor size, tumor number, distribution of tumor location, proportion of tumor BCLC staging, histological grade of tumor cell differentiation, and presence of microvascular invasion. Most patients had laparotomy segmentectomy or wedge resection for treatment of the initial HCC, and only four (7%) patients in the RFA group received a lobectomy.
Table 1: Patient and tumor characteristics of initial HCC
Repeat SR (n = 43) |
RFA (n = 57) |
P |
|
|---|---|---|---|
Age (years) |
60 (35–76) |
63 (27–81) |
0.28 |
Gender M/F |
34 (79%)/9 (21%) |
38 (67%)/19 (33%) |
0.19 |
Comorbidity (DM, CHF, COPD, CKD) |
14 (33%) |
19 (33%) |
1.00 |
Risk factor of HCC |
|||
viral hepatitis B |
21 (49%) |
32 (56%) |
0.55 |
viral hepatitis C |
20 (47%) |
23 (40%) |
0.55 |
alcohol |
2 (5%) |
4 (7%) |
0.62 |
Cirrhosis severity |
|||
Child-Pugh class A |
35 (81%) |
50 (88%) |
0.41 |
Child-Pugh class B |
1 (2%) |
0 (0%) |
0.25 |
Laboratory data |
|||
serum bilirubin (mg/dL) |
0.7 (0.3–1.4) |
0.7 (0.2–2.3) |
0.26 |
serum alanine transaminase (U/L) |
92 (1–1808) |
58 (1–221) |
0.42 |
serum aspartate transaminase (U/L) |
106 (1–1724) |
72 (17–284) |
0.40 |
serum albumin (g/dL) |
3.9 (2.7–4.7) |
3.9 (2.7–4.9) |
0.60 |
platelet count (x103/Cumm) |
169 (62–362) |
177 (60–502) |
0.62 |
PTINR |
1.10 (0.97–1.83) |
1.05 (0.91–1.31) |
0.06 |
serum creatinine (mg/dL) |
1.6 (0.7–12.1) |
1.5 (0.6–12.8) |
0.92 |
serum a-fetoprotein (ng/mL) |
602 (1–11681) |
1090 (3–29141) |
0.54 |
ICG (%) |
12.3 (2.6–28.0) |
14.4 (0.8–48) |
0.26 |
Primary tumor stage |
|||
BCLC stage 0 |
5 (12%) |
8 (14%) |
0.77 |
BCLC stage A |
29 (67%) |
34 (60%) |
0.42 |
BCLC stage B |
9 (21%) |
15 (26%) |
0.53 |
Initial tumor size (cm) |
3.9 (1.0–16.0) |
3.9 (1.3–15.0) |
0.94 |
Initial tumor number |
1.1 (1–4) |
1.2 (1–3) |
0.60 |
Initial tumor number 1/> 1 |
36 (84%)/7 (16%) |
48 (84%)/9 (16%) |
0.58 |
Initial tumor location |
|||
monosegment/disegment |
41 (95%)/2 (5%) |
55 (96%)/2 (4%) |
0.77 |
Surgery method |
|||
laparotomy/laparoscopy |
39 (91%)/4 (9%) |
55 (97%)/2 (3%) |
0.23 |
lobectomy/segmentectomy/wedge resection |
0(0%)/42 (98%)/1 (2%) |
4(7%)/40 (70%)/13 (23%) |
0.11 |
Histologic grade of initial tumor |
|||
grade I |
0 (0%) |
2 (4%) |
0.22 |
grade II |
23 (54%) |
30 (53%) |
0.55 |
grade III |
19 (44%) |
24 (42%) |
0.84 |
grade IV |
1 (2%) |
1 (1%) |
0.84 |
Microvascular invasion |
8 (19%) |
7 (12%) |
0.41 |
Baseline profile of recurrent HCC
With the regards to the recurrent HCC (Table 2), the median time from initial resection to first recurrence was longer in the repeated SR group, but the there was no statistically significant difference (26 vs. 14 months, p = 0.06). The clinical characteristics of patients and the recurrent tumor were not significantly different in the two groups including laboratory data, tumor size, tumor number, and tumor staging. In the repeated SR group, 41 (90.7%) patients underwent segmentectomy and four (9.3%) wedge resections. In the RFA group, most (81%) procedures were performed via a CT guided approach, and 46 (81%) patients received one session of RFA, whereas 11 (19%) needed two sessions of RFA for complete treatment of recurrent tumors.
Table 2: Patient and tumor characteristics of first recurrent HCC
Repeat SR (n = 43) |
RFA (n = 57) |
P |
|
|---|---|---|---|
Median time from initial resection to 1st recurrence (m) |
26 (4–126) |
14 (1–86) |
0.06 |
Age (years) |
63 (37–84) |
65 (31–84) |
0.51 |
Cirrhosis severity |
|||
Child-Pugh class A |
35 (81%) |
50 (88%) |
0.41 |
Child-Pugh class B |
1 (2%) |
0 (0%) |
0.25 |
Laboratory data |
|||
serum bilirubin (mg/dL) |
0.6 (0.1–1.3) |
0.7 (0.3–1.8) |
0.09 |
serum alanine transaminase (U/L) |
39 (1–131) |
49 (1–205) |
0.06 |
serum aspartate transaminase (U/L) |
48 (1–162) |
51 (1–206) |
0.62 |
serum albumin (g/dL) |
3.9 (2.7–4.6) |
3.9 (3.0–4.8) |
0.85 |
platelet count (x103/Cumm) |
165 (90–321) |
149 (78–305) |
0.12 |
PTINR |
1.03 (0.91–1.21) |
1.08 (0.89–2.12) |
0.13 |
serum creatinine (mg/dL) |
1.9 (0.7–13.1) |
1.5 (0.1–10.4) |
0.37 |
serum a-fetoprotein (ng/mL) |
23 (3–290) |
67 (2–817) |
0.19 |
ICG (%) |
14.0 (4.0–34.0) |
22.0 (19.0–25.0) |
0.17 |
Recurrent tumor stage |
|||
BCLC stage 0 |
17 (40%) |
32 (56%) |
0.11 |
BCLC stage A |
26 (60%) |
25 (44%) |
0.11 |
Recurrent tumor size (cm) |
1.9 (0.8–3.0) |
1.8 (1.0–3.0) |
0.17 |
Recurrent tumor number |
1.2 (1–3) |
1.1 (1–2) |
0.14 |
Recurrent tumor number 1/> 1 |
41 (95%)/2 (5%) |
55 (96%)/2 (4%) |
0.77 |
Recurrent tumor location |
|||
monosegment/disegment |
41 (95%)/2 (5%) |
55 (96%)/2 (4%) |
0.77 |
Repeat surgery method |
|||
lobectomy/segmentectomy/wedge resection |
0 (0%)/39 (91%)/4 (9%) |
- |
- |
Radiofrequency ablation |
|||
CT/ultrasound guided method |
- |
46 (81%)/11(19%) |
- |
Total RFA session |
- |
1.1 (1–2) |
- |
RFA session 1/2 |
- |
53 (93%)/4 (7%) |
- |
Clinical outcome after treatment of recurrent HCC
Table 3 showed the postoperative and long term outcomes of patients receiving repeated SR and RFA for the treatment of the first recurrence of HCC. Seven (16%) patients developed a total of 10 operation related complications in the repeated SR group, and one (2%) patient experienced a major complication: death due to bile duct injury with bile leakage and septic shock. In the RFA group, four (7%) patients developed a total of six procedure related complications, and there was no complication related mortality. The incidences of treatment related morbidity (p = 0.14) and mortality (p = 0.25) did not differ in the two groups. The total hospital day was longer in the repeated SR group (13 vs. 5 days, p < 0.05). The overall treatment response rates were similar (repeated SR 100% vs. RFA 98%, p = 0.67). At the time of analysis, 30.2% of patients over the median follow up time of 53 months in the repeated SR group and 28.1% patients over the median follow up time of 54 months in the RFA group remained free of a second recurrence. The median time from the treatment of recurrent HCC to developing a second recurrence was 11 months in the repeated SR group and 10 months in the RFA group (p = 0.74). Intrahepatic recurrence was the most common recurrence pattern in both groups. For the treatment of the second recurrence of HCC, 55% of patients received curative treatment in the repeated SR group, whereas 67% of patients received curative treatment in the RFA group.
Table 3: Postoperative and long term outcomes after treatment of first recurrent HCC
Repeat SR (n = 43) |
RFA (n = 57) |
P |
|
|---|---|---|---|
Operation related complications |
7 (16%) |
4 (7%) |
0.14 |
Pleural effusion |
1 |
2 |
0.73 |
Pneumothorax |
0 |
1 |
0.38 |
Wound infection |
1 |
0 |
0.25 |
Intraabdominal hemorrhage |
0 |
0 |
1.00 |
Sepsis |
5 |
2 |
0.12 |
Bile duct injury/Bile leakage |
3 |
1 |
0.19 |
Hospital mortality |
1 (2%) |
0 (0%) |
0.25 |
Total hospital day (day) |
13 (5–27) |
5 (2–17) |
< 0.05 |
Overall treatment response |
100% |
98% |
0.67 |
Complete response |
42 |
55 |
|
Partial response |
1 |
1 |
|
Stable disease |
0 |
1 |
|
Progressive disease |
0 |
0 |
|
Median time from 1st recurrence to 2nd recurrence (m) |
11 (4–82) |
10 (0–87) |
0.74 |
2nd recurrence pattern |
|||
No recurrence |
13 (30%) |
16 (28%) |
|
Intrahepatic recurrence |
29 (67%) |
39 (68%) |
|
Extrahepatic recurrence |
1 (3%) |
2 (4%) |
|
Management of second intrahepatic recurrence |
|||
OP |
8 (27%) |
3 (8%) |
|
PEI |
2 (7%) |
7 (18%) |
|
RFA |
6 (21%) |
16 (41%) |
|
TACE |
13 (45%) |
13 (33%) |
|
Others (HAIC, Sorafenib, R/T, palliation) |
0 (0%) |
0 (0%) |
Comparison of survival results between the groups
The 1-, 3-, 5-year overall survival rates after treatment of the first recurrence of HCC were 97.6%, 82.7%, 56.4% in the repeated SR group and 98.2%, 77.2%, 52.6% in the RFA group (P = 0.69) (Figure 2). The 1-, 3-, 5-year disease-free survival rates were 57.0%, 32.1%, 28.6% in the repeated SR group and 60.8%, 26.6%, 16.6% in the RFA group (P = 0.89) (Figure 3). The 1-, 3-, 5-year cumulative incidences of the second recurrence after treatment of the first recurrence of HCC were 41.7%, 67.1%, 70.8% in the repeated SR and 28.1%, 72.9%, 79.7% in the RFA group (P = 0.94) (Figure 4). In the Cox’s regression analysis, with regard to overall survival, the histologic grade of the initial tumor (I vs non-I), AFP level at the time of tumor recurrence, time from initial resection to 1st recurrence, and time from treatment of 1st recurrent HCC to 2nd recurrence were significant prognostic factors at univariate analysis; HBsAg positive, age at the time of tumor recurrence, the histologic grade of the initial tumor (I vs non-I), AFP level at the time of tumor recurrence, time from initial resection to 1st recurrence, and time from treatment of 1st recurrent HCC to 2nd recurrence were significant prognostic factors at multivariate analysis (Table 4).
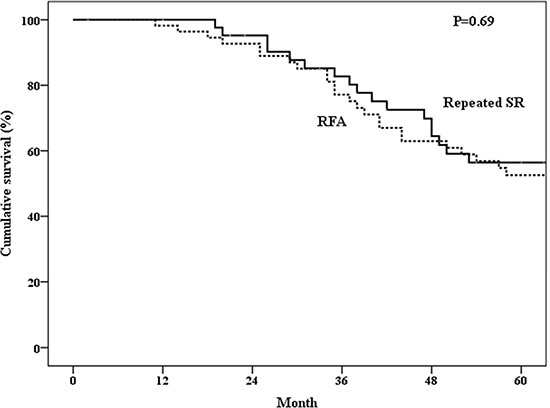
Figure 2: Overall survival of patients who underwent repeated surgical resection (SR) or radiofrequency ablation (RFA).
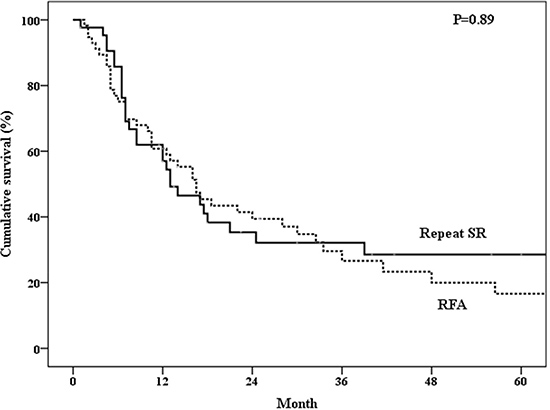
Figure 3: DDisease free survival of patients who underwent repeated surgical resection (SR) or radiofrequency ablation (RFA).
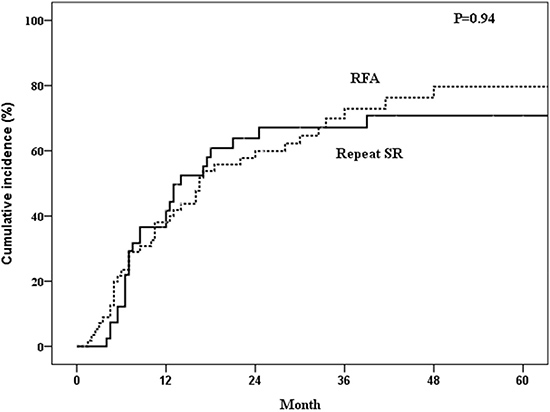
Figure 4: Incidence of second recurrence of patients who underwent repeated surgical resection (SR) or radiofrequency ablation (RFA).
Table 4: Univariate and multivariate analyses of prognostic factors for overall survival
Univariate Analysis |
Multivariate Analysis |
|||||
|---|---|---|---|---|---|---|
HR |
95% CI |
P |
HR |
95% CI |
P |
|
RFA & Repeated SR |
1.136 |
0.610–2.116 |
0.687 |
1.058 |
0.375–2.988 |
0.915 |
Gender |
1.868 |
0.997–3.501 |
0.051 |
0.405 |
0.088–1.872 |
0.247 |
HBsAg positive |
0.860 |
0.464–1.594 |
0.631 |
0.136 |
0.026–0.720 |
0.019 |
Anti-HCV-Ab positive |
0.916 |
0.496–1.689 |
0.778 |
0.498 |
0.109–2.275 |
0.368 |
Liver cirrhosis |
1.171 |
0.559–2.453 |
0.676 |
6.172 |
0.940–40.50 |
0.058 |
Histologic grade of initial tumor (I vs non-I) |
10.04 |
2.209–45.64 |
0.003 |
242.4 |
10.12–5800.7 |
0.001 |
Microvascular invasion of initial tumor |
0.842 |
0.353–2.005 |
0.697 |
1.572 |
0.399–6.193 |
0.518 |
Age at the time of tumor recurrence |
1.011 |
0.982–1.041 |
0.465 |
1.075 |
1.012–1.143 |
0.019 |
Recurrent tumor size |
1.002 |
0.604–1.662 |
0.994 |
2.532 |
0.932–6.875 |
0.068 |
Recurrent tumor number |
1.423 |
0.741–2.733 |
0.290 |
0.700 |
0.172–2.856 |
0.620 |
AFP level at the time of tumor recurrence |
1.004 |
1.001–1.007 |
0.007 |
1.005 |
1.001–1.009 |
0.014 |
Time from initial resection to 1st recurrence |
0.974 |
0.957–0.991 |
0.003 |
0.965 |
0.940–0.991 |
0.009 |
Time from treatment of 1st recurrent HCC to 2nd recurrence |
0.973 |
0.954–0.993 |
0.008 |
0.949 |
0.911 – 0.989 |
0.013 |
DISCUSSION
Our study suggested RFA achieves long-term survival outcomes similar to repeated SR in small recurring HCCs less than 3cm after primary resection. Previous studies comparing the efficacy of repeated RFA vs. resection after recurrence of HCCs usually also enrolled recurring tumors of more than 3cm in size (25, 28, 30, 31). Actually, following surgical resection of the primary tumors, intensive screening was usually applied and the recurring tumors were usually smaller than 3cm and the recurrent HCCs in our study were relatively small: 46% were smaller than 2cm, which was more like the real situation in the recurrence of tumors. A recent meta-analysis [32] reported RFA was associated with lower disease-free survival rates, however, our study we found both SR and RFA achieved a similar outcome for recurrent HCCs.. This might be explained by the inclusion criteria whereby the recurrent HCCs in our study were relatively small. As expected, a smaller tumor size is closely related to a higher rate of complete tumor elimination after RFA and a greater safety margin with fewer non-tumorous liver parenchyma resections in repeated SR, so the outcomes will be better. Besides, most RFA were performed under sonogram guidance in previous reports, but most (81%) patients received RFA under CT guidance in our study because the tumor size was usually small and some were not visible by sonogram. Altered anatomy after resection also contributed to difficulty with US guided RFA. Some experts suggested CT-guided RFA provides better detection of RFA lesions, margin discrimination, immediate ablation zone evaluation, and few artifacts [33], which may achieve better complete tumor ablation and better outcomes. Indeed, the RFA treated group in our study had a better 5-year overall survival rate and disease free survival rates than several previous studies [25–28]. Although in a recent study, Lee et al. found that either US or CT guided RFA was comparable for treatment naïve HCC [34], there was no study that compared the efficacy and safety of US or CT in the guidance of RFA for recurrent HCC after primary resection. This interesting problem merits further investigation in the future.
Previous studies found that patients with a tumor size ≦ 3cm and tumor numbers ≦ 3 benefited most from RFA treatment, so this is the reason we included only patients with tumor size ≦ 3cm and tumor numbers ≦ 3.
In our study, both repeated SR and RFA completely eliminated recurrent HCC and achieved near 100% response rates. However, a second recurrence of HCC is not uncommon. Chan et al [28] showed 72.4% of patients in the repeated SR group and 84.4% of patients in the RFA group developed a second recurrence with a similar median time from treatment of the first recurrence to second recurrence (6.3 vs. 9.5 months, p = 0.25). Our study showed 79.8% of patients in the repeated SR group and 71.9% of patients in the RFA group developed a second recurrence with a similar median time from treatment of the first recurrence to second recurrence (11 vs. 10 months, p = 0.74).
The improvement in liver function evaluation, surgical technique and perioperative care and decrease in postoperative morbidity and mortality make it possible for more patients to receive surgical resection [16, 35, 36]. However, surgical resection of recurrent HCC is still challenging due to small liver remnants, poor liver function reserve, intra-abdominal adhesion from previous surgery, and the tumor location being adjacent to major vascular or biliary structures. Although the latest literatures suggest repeated SR is considered a favorable and important curative treatment for recurrent HCC, postoperative complications, and in particular hepatic failure, are not uncommon and can not be overlooked [37]. A meta-analysis study showed repeated SR for recurrent HCC was associated with a higher procedure related morbidity rate compared with RFA [32]. Our study showed the procedure-related complication rates were higher in the repeated SR group than that in the RFA group (16% vs. 7% p = 0.14). One patient with repeated SR had major complications and died of bile duct injury with bile leakage and septic shock. RFA is a minimally invasive procedure and can be performed percutaneously either by ultrasound or CT guided approach. Compared with repeated SR via the open or laparoscopic approach, RFA is a highly target-selective thermal treatment technique to conserve non-tumorous liver parenchyma and minimize the degree of surgical insult to the limited liver reserve. Apart from surgery, RFA can be performed under conscious sedation and has a shorter hospital day, making it more cost-effective than surgical resection [2, 38]. In our study, median total hospital stay for patients who underwent RFA was significantly shorter than for those who underwent repeated SR (5 vs. 13 days, p < 0.05). Further, the characteristics and benefits of less invasiveness and highly-targeted tumor treatment improved the feasibility of patients and repeatability of RFA for recurrent HCC. Our study showed more than one third of patients in both groups underwent loco-regional treatment for a second recurrence of HCC, whereas 8% of patients in the RFA group and 27% of patients in the repeated SR group were amenable to surgical resection of a second recurrence of HCC. The aforementioned beneficial factors of RFA make it more safe and feasible in treating recurrent HCC after hepatectomy.
Previous studies reported the serum albumin level, serum alpha fetoprotein level, recurrent tumor size, time interval from primary hepatectomy to first recurrence, and time interval from treatment of recurrent HCC to second recurrence were significant prognostic factors to overall survival [23, 25, 28]. A shorter time interval from treatment to recurrence, is associated with poor prognosis. The finding of our study is consistent with the result of previous report by Albert C.Y. Chan, et al in 2012 [39]. The univariate and multivariate analyses in our study also showed similar findings, except recurrent tumor size was not related to overall survival. Our finding can be explained by the relatively small recurrent tumor size in our study and complete elimination rate of recurrent tumor increase with a decreased possibility of the presence of satellite nodules which decrease early recurrence and improve overall survival. Moreover, the presence of HBV infection and younger age at the time of tumor recurrence were significant factors of better overall survival at univariate analysis. Although an acceptable long term survival is reachable in carefully selected elderly patients [40, 41], patient age is theoretically related to the post-treatment complication and disease morbidity and is always more relevant for the prognosis than many tumor and treatment factors. However, the reason why the presence of HBV infection was also a favorable factor was unknown. It was probably because all HBV patients with indication (45.3%) in our study had anti-viral agent treatment, which had been proved to reduce HBV related long-term complications and lead to better prognosis [42].
The limitation of our study included non-randomization. Although this was not a randomized study, the baseline characteristics including the ICG retention rate at 15 minutes at initial diagnosis of HCC and at recurrence of HCC after surgical resection between the two groups of patients were similar. A prospective randomized controlled trial to compare the efficacy or repeated RFA and surgical resection for recurrent HCCs after surgical resection is required.
CONCLUSIONS
In small recurrent HCCs after SR, RFA achieved similar overall survival and disease-free survival than those with repeated SR and also had a shorter hospital stay.
CONFLICTS OF INTEREST
The authors have no conflicts of interests.
GRANT SUPPORT
This study was supported by Kaohsiung Veterans General Hospital (VGHKS-104–049).
REFERENCES
1. Cho YK, Kim JK, Kim WT, Chung JW. Hepatic resection versus radiofrequency ablation for very early stage hepatocellular carcinoma: a Markov model analysis. Hepatology. 2010; 51:1284–90.
2. Cucchetti A, Piscaglia F, Cescon M, Colecchia A, Ercolani G, Bolondi L, Pinna AD. Cost-effectiveness of hepatic resection versus percutaneous radiofrequency ablation for early hepatocellular carcinoma. J Hepatol. 2013; 59:300–07.
3. Li L, Zhang J, Liu X, Li X, Jiao B, Kang T. Clinical outcomes of radiofrequency ablation and surgical resection for small hepatocellular carcinoma: a meta-analysis. J Gastroenterol Hepatol. 2012; 27:51–58.
4. Molinari M, Helton S. Hepatic resection versus radiofrequency ablation for hepatocellular carcinoma in cirrhotic individuals not candidates for liver transplantation: a Markov model decision analysis. Am J Surg. 2009; 198:396–406.
5. Ueno S, Sakoda M, Kubo F, Hiwatashi K, Tateno T, Baba Y, Hasegawa S, Tsubouchi H, and Kagoshima Liver Cancer Study Group. Surgical resection versus radiofrequency ablation for small hepatocellular carcinomas within the Milan criteria. J Hepatobiliary Pancreat Surg. 2009; 16:359–66.
6. Wang JH, Wang CC, Hung CH, Chen CL, Lu SN. Survival comparison between surgical resection and radiofrequency ablation for patients in BCLC very early/early stage hepatocellular carcinoma. J Hepatol. 2012; 56:412–18.
7. Welker MW, Bechstein WO, Zeuzem S, Trojan J. Recurrent hepatocellular carcinoma after liver transplantation - an emerging clinical challenge. Transpl Int. 2013; 26:109–18.
8. Cheung TT, Poon RT, Yuen WK, Chok KS, Jenkins CR, Chan SC, Fan ST, Lo CM. Long-term survival analysis of pure laparoscopic versus open hepatectomy for hepatocellular carcinoma in patients with cirrhosis: a single-center experience. Ann Surg. 2013; 257:506–11.
9. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012; 379:1245–55.
10. Roayaie S, Obeidat K, Sposito C, Mariani L, Bhoori S, Pellegrinelli A, Labow D, Llovet JM, Schwartz M, Mazzaferro V. Resection of hepatocellular cancer ≤2 cm: results from two Western centers. Hepatology. 2013; 57:1426–35.
11. Shrager B, Jibara G, Schwartz M, Roayaie S. Resection of hepatocellular carcinoma without cirrhosis. Ann Surg. 2012; 255:1135–43.
12. Lencioni R, Cioni D, Crocetti L, Franchini C, Pina CD, Lera J, Bartolozzi C. Early-stage hepatocellular carcinoma in patients with cirrhosis: long-term results of percutaneous image-guided radiofrequency ablation. Radiology. 2005; 234:961–67.
13. N’Kontchou G, Mahamoudi A, Aout M, Ganne-Carrié N, Grando V, Coderc E, Vicaut E, Trinchet JC, Sellier N, Beaugrand M, Seror O. Radiofrequency ablation of hepatocellular carcinoma: long-term results and prognostic factors in 235 Western patients with cirrhosis. Hepatology. 2009; 50:1475–83.
14. Neumann U. Outcome after partial hepatectomy for hepatocellular cancer within the Milan criteria (Br J Surg 2011; 98:1292-1300). Br J Surg. 2011; 98:1300–01.
15. Ng KK, Lo CM, Liu CL, Poon RT, Chan SC, Fan ST. Survival analysis of patients with transplantable recurrent hepatocellular carcinoma: implications for salvage liver transplant. Arch Surg. 2008; 143:68–68-74; discussion 74.
16. Fan ST, Mau Lo C, Poon RT, Yeung C, Leung Liu C, Yuen WK, Ming Lam C, Ng KK, Ching Chan S. Continuous improvement of survival outcomes of resection of hepatocellular carcinoma: a 20-year experience. Ann Surg. 2011; 253:745–58.
17. Nagasue N, Yukaya H, Ogawa Y, Sasaki Y, Chang YC, Niimi K. Second hepatic resection for recurrent hepatocellular carcinoma. Br J Surg. 1986; 73:434–38.
18. Tralhao JG, Dagher I, Lino T, Roudie J, Franco D. Treatment of tumour recurrence after resection of hepatocellular carcinoma. Analysis of 97 consecutive patients. Eur J Surg Oncol. 2007; 33:746–51.
19. Itamoto T, Nakahara H, Amano H, Kohashi T, Ohdan H, Tashiro H, Asahara T. Repeat hepatectomy for recurrent hepatocellular carcinoma. Surgery. 2007; 141:589–97.
20. Kakazu T, Makuuchi M, Kawasaki S, Miyagawa S, Hashikura Y, Kosuge T, Takayama T, Yamamoto J. Repeat hepatic resection for recurrent hepatocellular carcinoma. Hepatogastroenterology. 1993; 40:337–41.
21. Suenaga M, Sugiura H, Kokuba Y, Uehara S, Kurumiya T. Repeated hepatic resection for recurrent hepatocellular carcinoma in eighteen cases. Surgery. 1994; 115:452–57.
22. Choi D, Lim HK, Kim MJ, Lee SH, Kim SH, Lee WJ, Lim JH, Joh JW, Kim YI. Recurrent hepatocellular carcinoma: percutaneous radiofrequency ablation after hepatectomy. Radiology. 2004; 230:135–41.
23. Choi D, Lim HK, Rhim H, Kim YS, Yoo BC, Paik SW, Joh JW, Park CK. Percutaneous radiofrequency ablation for recurrent hepatocellular carcinoma after hepatectomy: long-term results and prognostic factors. Ann Surg Oncol. 2007; 14:2319–29.
24. Rhim H, Lim HK, Choi D. Current status of radiofrequency ablation of hepatocellular carcinoma. World J Gastrointest Surg. 2010; 2:128–36.
25. Liang HH, Chen MS, Peng ZW, Zhang YJ, Zhang YQ, Li JQ, Lau WY. Percutaneous radiofrequency ablation versus repeat hepatectomy for recurrent hepatocellular carcinoma: a retrospective study. Ann Surg Oncol. 2008; 15:3484–93.
26. Ren ZG, Gan YH, Fan J, Chen Y, Wu ZQ, Qin LX, Ge NL, Zhou J, Xia JL, Wang YH, Ye QH, Wang L, Ye SL. Treatment of postoperative recurrence of hepatocellular carcinoma with radiofrequency ablation comparing with repeated surgical resection. [Article in Chinese] Zhonghua Wai Ke Za Zhi. 2008; 46:1614-6.
27. Umeda Y, Matsuda H, Sadamori H, Matsukawa H, Yagi T, Fujiwara T. A prognostic model and treatment strategy for intrahepatic recurrence of hepatocellular carcinoma after curative resection. World J Surg. 2011; 35:170–77.
28. Chan AC, Poon RT, Cheung TT, Chok KS, Chan SC, Fan ST, Lo CM. Survival analysis of re-resection versus radiofrequency ablation for intrahepatic recurrence after hepatectomy for hepatocellular carcinoma. World J Surg. 2012; 36:151–56.
29. Eisele RM, Chopra SS, Lock JF, Glanemann M. Treatment of recurrent hepatocellular carcinoma confined to the liver with repeated resection and radiofrequency ablation: a single center experience. Technol Health Care. 2013; 21:9–18
30. Shen Q, Xue HZ, Jiang QF. Comparison of the effects of percutaneous radiofrequency ablation and surgical reresectionon postoperative recurrence of hepatocellular carcinoma. Chin J Clin Oncol. 2008; 35:1088.
31. Ho CM, Lee PH, Shau WY, Ho MC, Wu YM, Hu RH. Survival in patients with recurrent hepatocellular carcinoma after primary hepatectomy: comparative effectiveness of treatment modalities. Surgery. 2012; 151:700–09.
32. Chen X, Chen Y, Li Q, Ma D, Shen B, Peng C. Radiofrequency ablation versus surgical resection for intrahepatic hepatocellular carcinoma recurrence: a meta-analysis. J Surg Res. 2015; 195:166–74.
33. Cha CH, Lee FT Jr, Gurney JM, Markhardt BK, Warner TF, Kelcz F, Mahvi DM. CT versus sonography for monitoring radiofrequency ablation in a porcine liver. AJR Am J Roentgenol. 2000; 175:705–11.
34. Lee LH, Hwang JI, Cheng YC, Wu CY, Lee SW, Yang SS, Yeh HZ, Chang CS, Lee TY. Comparable Outcomes of Ultrasound versus Computed Tomography in the Guidance of Radiofrequency Ablation for Hepatocellular Carcinoma. PLoS One. 2017; 12:e0169655.
35. Duffy JP, Hiatt JR, Busuttil RW. Surgical resection of hepatocellular carcinoma. Cancer J. 2008; 14:100–10.
36. Fan ST. Liver functional reserve estimation: state of the art and relevance for local treatments: the Eastern perspective. J Hepatobiliary Pancreat Sci. 2010; 17:380–84.
37. Dai WC, Cheung TT. Strategic overview on the best treatment option for intrahepaitc hepatocellular carcinoma recurrence. Expert Rev Anticancer Ther. 2016; 16:1063–72.
38. Guo WX, Sun JX, Cheng YQ, Shi J, Li N, Xue J, Wu MC, Chen Y, Cheng SQ. Percutaneous radiofrequency ablation versus partial hepatectomy for small centrally located hepatocellular carcinoma. World J Surg. 2013; 37:602–07.
39. Chan AC, Poon RT, Cheung TT, Chok KS, Chan SC, Fan ST, Lo CM. Survival analysis of re-resection versus radiofrequency ablation for intrahepatic recurrence after hepatectomy for hepatocellular carcinoma. World J Surg. 2012; 36:151–56.
40. El-Fattah MA, Aboelmagd M, Elhamouly M. Prognostic factors of hepatocellular carcinoma survival after radiofrequency ablation: A US population-based study. United European Gastroenterol J. 2017; 5:227–35.
41. Faber W, Stockmann M, Schirmer C, Möllerarnd A, Denecke T, Bahra M, Klein F, Schott E, Neuhaus P, Seehofer D. Significant impact of patient age on outcome after liver resection for HCC in cirrhosis. Eur J Surg Oncol. 2014; 40:208–13.
42. Liaw YF. Impact of therapy on the outcome of chronic hepatitis B. Liver Int. 2013 (Suppl 1); 33:111–15.