
INTRODUCTION
Cardiovascular disease (CVD), which refers a class of diseases that involve the heart or blood vessels, is the leading cause of death globally, and a major determinant of global health [1, 2]. It was estimated that CVD accounted for an estimated 17. 3 million (95% UI, 16.5–18.1 million) of 54 million total deaths, or 31.5% (95% UI, 30.3%–32.9%) of all global deaths [3]. While, the burden of atherosclerosis is heritable and associated with elevated risk of developing CVDs [4–8]. Up to 90% of atherosclerosis may be preventable with a proper screening program, while biomarkers identified from genetic association studies, including genome-wide association studies (GWAS), have provided us an efficacious approach for screening of atherosclerosis [9–16].
Adiponectin (ADIPOQ), an adipokine with anti-inflammatory, antioxidant, antiatherogenic, pro-angiogenic, vasoprotective and insulin-sensitizing properties, has been identified to be inversely associated with higher risk of atherosclerosis and could be used as a predictor [17–19]. This is because ADIPOQ may protected the aorta from atherosclerosis injury by reducing the oxidative stress, as well as reducing the lesion formation size in the aortic root and reducing TC, TG, and LDL-C in serum [20]. Recently, the UK10K project identified that a low-frequency intronic variant in ADIPOQ was associated with decreased ADIPOQ levels (rs74577862-A, effect allele frequency (EAF) = 2.6%, P value = 3.04 × 10-64) in participants of European ancestry [21]. However, whether ADIPOQ variants were associated with risk of atherosclerosis, especially in a non- European population, is still unknown. Here, we aim to evaluate the association of the genetic variants of ADIPOQ gene with risk of atherosclerosis among a large Chinese population with a case-control study design. Besides, we also selected tagSNPs of the ADIPOQ gene using the RegulomeDB score system and SNAP [22, 23], thus, we got rs74577862 and rs62292784 genotyped and included in our analyses. Furthermore, we also conducted functional study of ADIPOQ rs74577862 for its role in the development of atherosclerosis.
RESULTS
Characteristics of study participants
The characteristics of the study participants were summarized in Table 1. No significant differences were found between cases and controls for age group, gender, smoking status, and drinking status. For the atherosclerosis subtypes, we included 400 carotid atherosclerosis cases (44.4%) and 500 coronary atherosclerosis cases (55.6%) in this case-control study.
Table 1: Clinical and demographic characteristics of atherosclerosis cases and controls
Variables |
Cases (n=900) |
Controls (n=900) |
P value |
|---|---|---|---|
Age |
|||
≥60 |
424 (47.1%) |
411 (45.7%) |
0.539 |
<60 |
476 (52.9%) |
489 (54.3%) |
|
Gender |
|||
Male |
650 (72.2%) |
634 (70.4%) |
0.404 |
female |
250 (27.8%) |
266 (29.6%) |
|
Smoking status |
|||
Smokers |
280 (31.1%) |
253 (28.1%) |
0.055 |
Non-Smokers |
620 (68.9%) |
657 (71.9%) |
|
Alcohol status |
|||
drinkers |
292 (32.4%) |
277 (30.8%) |
0.447 |
Non-drinkers |
608 (67.6%) |
623 (69.2%) |
|
Subtypes |
|||
Carotid atherosclerosis |
400 (44.4%) |
||
Coronary atherosclerosis |
500 (55.6%) |
Association analysis between genetic variants of ADIPOQ gene with risk of atherosclerosis
The distribution of ADIPOQ rs74577862 and rs62292784 in atherosclerosis patient and control groups are presented in Table 2. The minor allele frequencies (MAF) were consistent with those in CHB of 1000 genomes data. Both of the two SNPs were in Hardy–Weinberg equilibrium in control group (P > 0.05). We found rs74577862 was significantly associated with risk of atherosclerosis (OR=2.08; 95%CI=1.48-2.91; P=2.2×10-5). Using QUANTO [32], we have a 99.2% power for rs74577862 in current analysis. Compared with carriers of genotype GG, those with genotype AG (OR=1.94; 95%CI=1.34-2.80; P=4.0×10-4) and AA (OR=4.38; 95%CI=1.08-17.7; P=0.038) have significantly increased risk of atherosclerosis. In dominant model, rs74577862 was also associated with increased risk of atherosclerosis (OR=2.03; 95%CI=1.43-2.90; P=8.5×10-5). However, we didn’t find any significant associations for rs62292784.
Table 2: Associations of genetic variants of ADIPOQ with atherosclerosis risk
atherosclerosis cases |
Controls |
OR (95% CIs)* |
P value |
|
|---|---|---|---|---|
rs74577862 |
||||
GG |
807 (89.7%) |
850 (94.4%) |
1.00 (Reference) |
|
AG |
85 (9.4%) |
48 (5.3%) |
1.94 (1.34-2.80) |
4.0×10-4 |
AA |
8 (0.9%) |
2 (0.2%) |
4.38 (1.08-17.7) |
0.038 |
AA+AG |
93 (10.3%) |
50 (5.5%) |
2.03 (1.43-2.90) |
8.5×10-5 |
A vs G |
2.08 (1.48-2.91) |
2.2×10-5 |
||
MAF |
0.056 |
0.029 |
||
MAF in CHB of 1000 genomes |
0.024 |
|||
rs62292784 |
||||
CC |
338 (37.6%) |
370 (41.1%) |
1.00 (Reference) |
|
CT |
452 (50.2%) |
429 (47.6%) |
1.20 (0.94-1.53) |
0.138 |
TT |
110 (12.2%) |
101 (11.2%) |
1.24 (0.87-1.77) |
0.240 |
T vs C |
1.15 (0.96-1.38) |
0.136 |
||
MAF |
0.373 |
0.351 |
||
MAF in CHB of 1000 genomes |
0.354 |
|||
* Adjusted for age, gender, smoking status, and drinking status.
MAF=minor allele frequency.
Multiple testing were conducted using Bonferroni correction, and 0.025 was used as the p value threshold for the two variants.
Stratified analyses between ADIPOQ rs74577862 with risk of atherosclerosis
To find the potential population stratification, we analyzed the associations between ADIPOQ rs74577862 with risk of atherosclerosis stratified by atherosclerosis site. As shown in Table 3, we found rs74577862 was associated with increased risk of either carotid atherosclerosis (OR=2.03; 95%CI=1.35-3.06; P=6.3×10-4) or coronary atherosclerosis (OR=2.11; 95%CI=1.44-3.09; P=1.1×10-4).
Table 3: Associations of rs74577862 with atherosclerosis risk
atherosclerosis cases |
Controls |
OR (95% CIs) * |
P value |
|
|---|---|---|---|---|
Carotid atherosclerosis |
||||
GG |
359 (89.8%) |
850 (94.4%) |
1.00 (Reference) |
|
AG |
38 (9.5%) |
48 (5.3%) |
1.95 (1.25-3.03) |
3.1×10-3 |
AA |
3 (0.7%) |
2 (0.2%) |
3.69 (0.71-19.3) |
0.121 |
AA+AG |
41 (10.3%) |
50 (5.5%) |
2.02 (1.31-3.10) |
1.3×10-3 |
A vs G |
2.03 (1.35-3.06) |
6.3×10-4 |
||
Coronary atherosclerosis |
||||
GG |
448 (89.6%) |
850 (94.4%) |
1.00 (Reference) |
|
AG |
47 (9.4%) |
48 (5.3%) |
1.93 (1.27-2.94) |
2.0×10-3 |
AA |
5 (1.0%) |
2 (0.2%) |
4.93 (1.15-21.2) |
0.032 |
AA+AG |
52 (10.4%) |
50 (5.5%) |
2.05 (1.37-3.07) |
4.6×10-4 |
A vs G |
2.11 (1.44-3.09) |
1.1×10-4 |
||
* Adjusted for age, gender, smoking status, and drinking status.
Multiple testing were conducted using Bonferroni correction, and 0.025 was used as the p value threshold for the two variants.
Site-directed mutagenesis and dual-luciferase reporter assay
To evaluated the potential functions of ADIPOQ rs74577862, we conducted the Site-Directed Mutagenesis and dual-luciferase reporter assay. As shown in Figure 1, we found that a significant decrease in luciferase expression for the reconstructed plasmid with rs74577862 A allele in comparison to the one with G allele in HAECs cell lines (P<0.001). This means allele A was associated with lower level ADIPOQ, then increased risk of atherosclerosis.
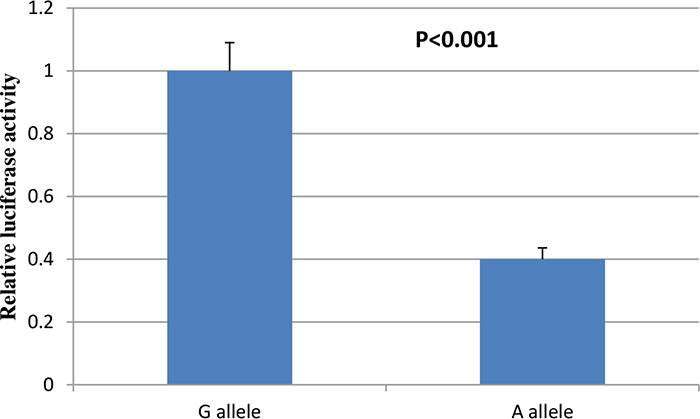
Figure 1: Dual-luciferase reporter assay results of ADIPOQ rs74577862.
Quantification of gene expression using real-time PCR
We then assessed the influence of ADIPOQ rs74577862 on the expression of ADIPOQ gene in the plaque tissues of 50 individuals was confirmed by real time PCR. As shown in Figure 2, the atherosclerosis risk allele of rs74577862 correlated with decreased expression level of ADIPOQ gene (P<0.001).
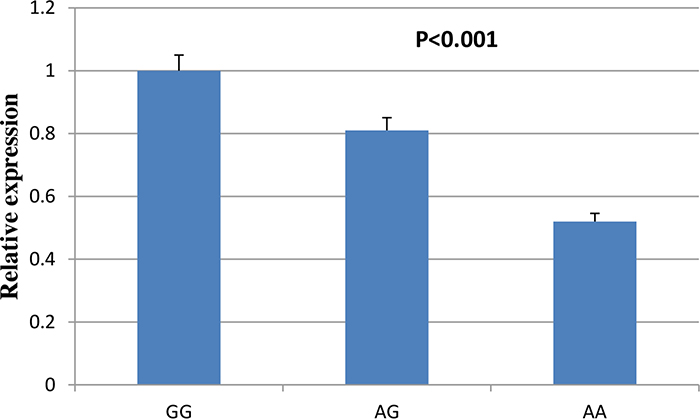
Figure 2: Comparison of ADIPOQ gene expressions between rs74577862 genotypes.
DISCUSSION
The current study explored association between genetic variants of ADIPOQ gene (rs74577862 and rs62292784) with risk of atherosclerosis among a large Chinese population. Significantly association with risk of atherosclerosis was detected for ADIPOQ rs74577862. Even stratified by atherosclerosis site, rs74577862 was still associated with increased risk of either carotid or coronary atherosclerosis. Then, we also conducted dual-luciferase reporter assay and real-time PCR of ADIPOQ rs74577862 for its role in the development of atherosclerosis.
It has been demonstrated that ADIPOQ worked as a novel modulator for endothelial adhesion molecules, and plasma ADIPOQ concentrations were significantly lower in patients with coronary artery disease early in 1999 [24]. ADIPOQ, which accumulated in the injured artery from the plasma and suppressed endothelial inflammatory response and vascular smooth muscle cell proliferation, could also suppress the development of atherosclerosis in vivo [25]. Epidemiological study also suggested that low level of plasma ADIPOQ was associated with higher risk of atherosclerosis, diabetes, insulin resistance, obesity, and cancers [26–29]. Inamura et al [30] reported that Low-level plasma adiponectin was associated with KRAS-mutant colorectal cancer risk.
SNP rs74577862 is located at 3q27.3, the intron region of ADIPOQ. We found that a significant decrease in luciferase expression for the reconstructed plasmid with rs74577862 A allele in comparison to the one with G allele, which was mutually confirmed with the previous finding that A allele of rs74577862 was associated with decreased ADIPOQ levels [21]. Using HaploReg v4.1 [31], we found rs74577862 could cause the change of motifs NF-kappaB and TATA. NF-κB signaling has been linked with lipid metabolism and atherosclerosis, and inhibition of NF-κB signaling has been shown to protect against atherosclerosis [32].
Our study had its own advantages. First, our large sample size warranted the liability of the results. Although as a low frequency variant, we still have a 99.2% power for rs74577862 in current study using QUANTO [33]. Second, we characterized the function of SNP rs74577862, making the association of this SNP with the risk of atherosclerosis biological plausible. Despite of these strengths mentioned above, some limitations should be noted. Firstly, lack of evaluation of gene–environment interactions; second, an independent replication. However, our results still provided us an important clue for the prevention of atherosclerosis. Future studies should address the mechanisms of ADIPOQ with regard to the risk of atherosclerosis.
In summary, the current study investigated the association between genetic variants of ADIPOQ gene and risk of atherosclerosis in a Chinese population. We identified ADIPOQ rs74577862 minor allele associated with a higher atherosclerotic burden. This polymorphism was also shown to be associated with increased risk of either carotid or coronary atherosclerosis, suggesting that rs74577862 has the similar involvements in the pathophysiology of carotid and coronary atherosclerosis. These findings provide further evidence for an important causal role of rs74577862 in atherosclerosis development.
MATERIALS AND METHODS
Study subjects
Totally included in current study were 900 atherosclerosis and 900 matched healthy controls. Clinical diagnosis of 500 coronary atherosclerosis cases was evaluated by percutaneous coronary angiography (a stenosis degree greater than or equal to 50% in at least one artery), confirmed by two experienced cardiologists. While 400 carotid atherosclerosis cases were defined as patients with evidence of carotid plaques (CPs) presence in the internal carotid artery (ICA) or the common carotid artery (CCA) who were consecutively admitted for carotid endarterectomy (greater than or equal to 70% NASCET stenosis). A complete medical history together with demographic characteristics was compiled for each individual enrolled by a face to face interview in the study. The exclusion criteria for all patients were those with systemic diseases such as inflammation, tumors, chronic inflammatory disease, rheumatic autoimmune disease, or thyroid dysfunction (current hypo- or hyperthyroidism), liver and kidney diseases. Five milliliter peripheral blood was collected using EDTA-anticoagulant tubes from all the participants. The study was approved by the ethics committees of all the involved hospitals and each subject gave written informed consent to participate in the study.
DNA extraction, SNP selection and genotyping
Genomic DNA was extracted from whole blood samples collected with EDTA using a standardized BloodPrep DNA Chemistry isolation kit (Applied Biosystems, Forester City, CA, USA). All DNA samples were assessed for quality and quantity using a Nanodrop 2000, and DNA electrophoresis prior to genotyping. Except for rs74577862, we also selected the potential functional TagSNPs using the RegulomeDB score system ranging from categories 1-4, together with SNAP. Finally, we got SNP rs74577862 and rs62292784 in our analyses. Genotyping was performed using the high resolution melting (HRM) analysis. For quality control, Additionally, 10 % of samples were randomly selected for genotyping in duplicates and the results demonstrated a 100% degree of concordance among the duplicate pairs.
Site-directed mutagenesis and dual-luciferase reporter assay
Site-Directed Mutagenesis were conducted using the Phusion Site-Directed Mutagenesis Kit (Thermo Fisher) according to the instructions of the manufacturer. The site mutagenesis was proved through sequencing. Then these two target sequences were cloned into pGL3-Basic vector (Promega, Madison, WI, USA), respectively. Negative control pGL3-Basic and reconstructed plasmids containing rs74577862 wild type or mutation type were respectively co-transfected into HAECs cell with pRL-SV40 vector, which expressed renilla luciferase as the transfection control, using Lipofectamine 3000 Reagent (Invitrogen, Waltham, MA, USA) after planting in 24-well plates for 24 h. luciferase activity was measured using the Dual-Luciferase Reporter Assay System (Promega) according to the manufacturer’s protocol, and all experiments were performed three times in triplicate.
Quantification of gene expression using real-time PCR
Expression of the ADIPOQ gene in the plaque tissues of 50 individuals was confirmed by real time PCR. Assays were performed using TaqMan gene expression probes and reagents (Life Technologies) and run on a 7900HT Real Time PCR System (Applied Biosystems). GAPDH was used as the reference gene.
Statistical analysis
Pearson’s χ2-test, or t-test was adopted to examine the differences in demographic variables and distributions of genotypes between cases and controls, when appropriate. Significant departure of genotype frequencies from Hardy-Weinberg expectation and test of differences in allele frequencies between cases and controls were determined by the chi-square test. Multivariate logistic regression analyses were used and expressed in terms of adjusted odds ratio (OR) and 95% confidence interval (CI) with adjustment for age, gender, smoking status, and drinking status. Multiple testing were conducted using Bonferroni correction, and 0.025 was used as the p value threshold for the two variants. Statistical analyses were undertaken using STATA (version 13.1, StataCorp LP, TX, USA).
ACKNOWLEDGEMENTS
This work was supported by the National Natural Science Fund of China (Grants 81270265, 30872541), and the Applied Basic Research Programs of Wuhan (No.2014060101010031).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
1. Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, et al, and American Heart Association Statistics Committee and Stroke Statistics Subcommittee-2017 Update: A Report From the American Heart Association. Circulation. 2017; 135:e146-e603.
2. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, et al, and Writing Group Members, and American Heart Association Statistics Committee, and Stroke Statistics Subcommittee-2016 Update: A Report From the American Heart Association. Circulation. 2016; 133:e38-360.
3. Roth GA, Huffman MD, Moran AE, Feigin V, Mensah GA, Naghavi M, Murray CJ. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation. 2015; 132:1667-1678.
4. Shendre A, Wiener H, Irvin MR, Zhi D, Limdi NA, Overton ET, Wassel CL, Divers J, Rotter JI, Post WS, Shrestha S. Admixture Mapping of Subclinical Atherosclerosis and Subsequent Clinical Events Among African Americans in 2 Large Cohort Studies. Circ Cardiovasc Genet. 2017; 10.
5. Oliveira-Santos M, Castelo-Branco M, Silva R, Gomes A, Chichorro N, Abrunhosa A, Donato P, Pedroso de Lima J, Pego M, Goncalves L, Ferreira MJ. Atherosclerotic plaque metabolism in high cardiovascular risk subjects - A subclinical atherosclerosis imaging study with 18F-NaF PET-CT. Atherosclerosis. 2017; 260:41-46.
6. Lopez-Mejias R, Corrales A, Vicente E, Robustillo-Villarino M, Gonzalez-Juanatey C, Llorca J, Genre F, Remuzgo-Martinez S, Dierssen-Sotos T, Miranda-Filloy JA, Huaranga MA, Pina T, Blanco R, et al. Influence of coronary artery disease and subclinical atherosclerosis related polymorphisms on the risk of atherosclerosis in rheumatoid arthritis. Sci Rep. 2017; 7:40303.
7. Hisamatsu T, Miura K, Arima H, Kadota A, Kadowaki S, Torii S, Suzuki S, Miyagawa N, Sato A, Yamazoe M, Fujiyoshi A, Ohkubo T, Yamamoto T, et al, and Shiga Epidemiological Study of Subclinical Atherosclerosis (SESSA) Research Group. Smoking, Smoking Cessation, and Measures of Subclinical Atherosclerosis in Multiple Vascular Beds in Japanese Men. J Am Heart Assoc. 2016; 5:5.
8. Fernandez-Alvira JM, Fuster V, Dorado B, Soberon N, Flores I, Gallardo M, Pocock S, Blasco MA, Andres V. Short Telomere Load, Telomere Length, and Subclinical Atherosclerosis: The PESA Study. J Am Coll Cardiol. 2016; 67:2467-2476.
9. Andreassi MG, Piccaluga E, Gargani L, Sabatino L, Borghini A, Faita F, Bruno RM, Padovani R, Guagliumi G, Picano E. Subclinical carotid atherosclerosis and early vascular aging from long-term low-dose ionizing radiation exposure: a genetic, telomere, and vascular ultrasound study in cardiac catheterization laboratory staff. JJACC Cardiovasc Interv. 2015; 8:616-627.
10. Dauriz M, Porneala BC, Guo X, Bielak LF, Peyser PA, Durant NH, Carnethon MR, Bonadonna RC, Bonora E, Bowden DW, Florez JC, Fornage M, Hivert MF, et al. Association of a 62 Variants Type 2 Diabetes Genetic Risk Score With Markers of Subclinical Atherosclerosis: A Transethnic, Multicenter Study. Circ Cardiovasc Genet. 2015; 8:507-515.
11. Gebreab SY, Riestra P, Khan RJ, Xu R, Musani SK, Tekola-Ayele F, Correa A, Wilson JG, Rotimi CN, Davis SK. Genetic ancestry is associated with measures of subclinical atherosclerosis in African Americans: the Jackson Heart Study. Arterioscler Thromb Vasc Biol. 2015; 35:1271-1278.
12. Sabater-Lleal M, Malarstig A, Folkersen L, Soler Artigas M, Baldassarre D, Kavousi M, Almgren P, Veglia F, Brusselle G, Hofman A, Engstrom G, Franco OH, Melander O, et al. Common genetic determinants of lung function, subclinical atherosclerosis and risk of coronary artery disease. PLoS One. 2014; 9:e104082.
13. Zhang L, Buzkova P, Wassel CL, Roman MJ, North KE, Crawford DC, Boston J, Brown-Gentry KD, Cole SA, Deelman E, Goodloe R, Wilson S, Heiss G, et al. Lack of associations of ten candidate coronary heart disease risk genetic variants and subclinical atherosclerosis in four US populations: the Population Architecture using Genomics and Epidemiology (PAGE) study. Atherosclerosis. 2013; 228:390-399.
14. Cassidy-Bushrow AE, Bielak LF, Sheedy PF 2nd, Turner ST, Chu JS, Peyser PA. Shared genetic architecture in the relationship between adult stature and subclinical coronary artery atherosclerosis. Atherosclerosis. 2011; 219:679-683.
15. Wassel CL, Pankow JS, Peralta CA, Choudhry S, Seldin MF, Arnett DK. Genetic ancestry is associated with subclinical cardiovascular disease in African-Americans and Hispanics from the multi-ethnic study of atherosclerosis. Circ Cardiovasc Genet. 2009; 2:629-636.
16. Tsai MY, Johnson C, Kao WH, Sharrett AR, Arends VL, Kronmal R, Jenny NS, Jacobs DR Jr, Arnett D, O'Leary D, Post W. Cholesteryl ester transfer protein genetic polymorphisms, HDL cholesterol, and subclinical cardiovascular disease in the Multi-Ethnic Study of Atherosclerosis. Atherosclerosis. 2008; 200:359-367.
17. Juarez-Rojas JG, Posadas-Sanchez R, Martinez-Alvarado MDR, Torres-Tamayo M, Jorge-Galarza E, Mancilla-Valenzuela EY, Posadas-Romero C, Cardoso-Saldana GC, Gonzalez-Salazar MDC, Vargas-Alarcon G, Medina-Urrutia AX. Association of Adiponectin with Subclinical Atherosclerosis in a Mexican-Mestizo Population. Arch Med Res. 2017; 48:73-78.
18. Katsiki N, Mantzoros C, Mikhailidis DP. Adiponectin, lipids and atherosclerosis. Curr Opin Lipidol. 2017.
19. Omelchenko E, Gavish D, Shargorodsky M. Adiponectin is better predictor of subclinical atherosclerosis than liver function tests in patients with nonalcoholic fatty liver disease. Journal of the American Society of Hypertension : J Am Soc Hypertens. 2014; 8:376-380.
20. Wang X, Pu H, Ma C, Jiang T, Wei Q, Zhang C, Duan M, Shou X, Su L, Zhang J, Yang Y. Adiponectin abates atherosclerosis by reducing oxidative stress. Med Sci Monit. 2014; 20:1792-1800.
21. Walter K, Min JL, Huang J, Crooks L, Memari Y, McCarthy S, Perry JR, Xu C, Futema M, Lawson D, Iotchkova V, Schiffels S, Hendricks AE, et al, and UK10K Consortium. Nature. 2015; 526:82-90.
22. Boyle AP, Hong EL, Hariharan M, Cheng Y, Schaub MA, Kasowski M, Karczewski KJ, Park J, Hitz BC, Weng S, Cherry JM, Snyder M. Annotation of functional variation in personal genomes using RegulomeDB. Genome Res. 2012; 22:1790-1797.
23. Johnson AD, Handsaker RE, Pulit SL, Nizzari MM, O'Donnell CJ, de Bakker PI. SNAP: a web-based tool for identification and annotation of proxy SNPs using HapMap. Bioinformatics. 2008; 24:2938-2939.
24. Ouchi N, Kihara S, Arita Y, Maeda K, Kuriyama H, Okamoto Y, Hotta K, Nishida M, Takahashi M, Nakamura T, Yamashita S, Funahashi T, Matsuzawa Y. Novel modulator for endothelial adhesion molecules: adipocyte-derived plasma protein adiponectin. Circulation. 1999; 100:2473-2476.
25. Okamoto Y, Kihara S, Ouchi N, Nishida M, Arita Y, Kumada M, Ohashi K, Sakai N, Shimomura I, Kobayashi H, Terasaka N, Inaba T, Funahashi T, et al. Adiponectin reduces atherosclerosis in apolipoprotein E-deficient mice. Circulation. 2002; 106:2767-2770.
26. Dunajska K, Milewicz A, Jedrzejuk D, Szymczak J, Kuliczkowski W, Salomon P, Bialy D, Poczatek K, Nowicki P. Plasma adiponectin concentration in relation to severity of coronary atherosclerosis and cardiovascular risk factors in middle-aged men. Endocrine. 2004; 25:215-221.
27. Higashiura K, Ura N, Ohata J, Togashi N, Takagi S, Saitoh S, Murakami H, Takagawa Y, Shimamoto K. Correlations of adiponectin level with insulin resistance and atherosclerosis in Japanese male populations. Clin Endocrinol (Oxf). 2004; 61:753-759.
28. Duncan BB, Schmidt MI, Pankow JS, Bang H, Couper D, Ballantyne CM, Hoogeveen RC, Heiss G. Adiponectin and the development of type 2 diabetes: the atherosclerosis risk in communities study. Diabetes. 2004; 53:2473-2478.
29. Matsuda M, Tamura R, Kishida N, Segawa T, Kanno K, Nishimoto O, Nakamoto K, Nishiyama H, Kawamoto T. Predictive value of adiponectin in patients with multivessel coronary atherosclerosis detected on computed tomography angiography. J Atheroscler Thromb. 2013; 20:767-776.
30. Inamura K, Song M, Jung S, Nishihara R, Yamauchi M, Lochhead P, Qian ZR, Kim SA, Mima K, Sukawa Y, Masuda A, Imamura Y, Zhang X, et al. Prediagnosis Plasma Adiponectin in Relation to Colorectal Cancer Risk According to KRAS Mutation Status. J Natl Cancer Inst. 2016; 108.
31. Ward LD, Kellis M. HaploReg v4: systematic mining of putative causal variants, cell types, regulators and target genes for human complex traits and disease. Nucleic Acids Res. 2016; 44:D877-881.
32. Yu XH, Zheng XL, Tang CK. Nuclear Factor-kappaB Activation as a Pathological Mechanism of Lipid Metabolism and Atherosclerosis. Adv Clin Chem. 2015; 70:1-30.
33. Gauderman W, Morrison J. QUANTO 1.1: A computer program for power and sample size calculations for genetic-epidemiology studies. http://hydrauscedu/gxe/. 2006.