
INTRODUCTION
Abdominal pain is an important clinical manifestation of Crohn’s disease (CD). Such pain occurs not only in approximately 50% to 70% of patients during acute inflammation [1] but also in a significant proportion of patients during clinical and/or endoscopic remission [2]. Abdominal pain in patients with CD in remission has been associated with emotional suffering, disability, and high medical costs. Limited treatment options are currently available for this pain [3], and understanding the neurophysiological underpinnings of pain is fundamental to the development of an effective treatment.
The pathophysiology of abdominal pain in patients with CD in clinical remission is multifaceted. In these patients, pain is related to a dysfunction in brain-gut interactions [4], low-grade intestinal inflammation [5], visceral hypersensitivity [6], and other related mechanisms. The sensitization of the central nervous system (CNS) and reorganization of brain areas might play a role in visceral pain processing in CD [3, 7]. Magnetic resonance imaging (MRI) has been used to assess the structural plasticity and reorganization of the brain under different pathological conditions. Previous MRI studies have demonstrated pain-related cortical changes in patients with chronic conditions, such as irritable bowel syndrome [8, 9], chronic pancreatitis [10], and trigeminal neuropathic pain [11]. To date, several studies [12–14] have demonstrated structural changes in gray matter (GM) in patients with CD. The GM volume [12], sub-cortical volume [13], cortical thickness [12–14], surface area [13, 14]and folding [14] of multiple brain regions were significant changed. In our previous study [12], we found that, compare with healthy controls (HCs), patients with CD showed significant changes in GM volumes of multiple brain regions involved in pain, emotion, and homeostasis, and specific altered profiles of GM volume correlated with disease duration. Although these studies revealed changes in the GM structures in various brain regions, and pain has been associated with GM loss in numerous studies, the specific patterns of altered GM in patients with CD with or without abdominal pain have yet to be delineated.
In this study, we hypothesized that the structural changes in GM vary between patients with and without abdominal pain and that sustained abdominal pain is associated with changes in brain GM in areas involved in visceral pain processing. Specifically, the aims of the study were (1) to determine the changes in GM volume in patients with and without abdominal pain and (2) to potentially correlate the GM structural changes in specific brain regions with pain severity.
RESULTS
HCs vs. patients with CD with or without abdominal pain
Clinical variables
Among the 47 quiescent patients, 21 (44.7%) experienced abdominal pain. The average pain score ranged from 1 to 5.4, with a mean ± standard deviation of 2.68 ± 1.18.
There were no significant differences among the three groups in gender, age, height or weight. No differences existed between the pain and pain-free CD groups in disease duration, Montreal classification, or concomitant medication. The anxiety and depression scores of Hospital Anxiety and Depression Scale (HADS; including HADS-A and HADS-D subscales) in the pain, pain-free and HC groups were significantly different (P < 0.01). The patients in the pain group had higher HADS-A and HADS-D scores than did the subjects in the HC group (P < 0.01). The patients in the pain-free group had higher HADS-A scores than those in the HC group (P < 0.05). No significant difference was observed between the pain group and the pain-free group. The patients with abdominal pain exhibited higher CD activity index (CDAI) scores and lower Inflammatory Bowel Disease Questionnaire (IBDQ) scores than those of the patients without abdominal pain (P < 0.01).
The platelet (PLT) level and erythrocyte sedimentation rate (ESR) were not significantly different between the pain group and the pain-free group, while the C-reactive protein (CRP) level was significantly different between these two groups (P < 0.01). The Crohn’s disease endoscopic index of severity (CDEIS) scores of all the patients were below 3, with a mean (min~max) value of 1.24 (0~2.6) for the pain group and 0.89 (0~2.0) for the pain-free group. No significant difference was observed between the two groups (Table 1).
Table 1: Clinical demographics of the CD with pain, pain-free CD, and HC groups
CD with Pain (n = 21) |
Pain-free CD (n = 26) |
HC (n = 30) |
P value |
||
|---|---|---|---|---|---|
Gender (male/female) |
12/9 |
20/6 |
20/10 |
0.352 |
|
Age (years) |
30.86 ± 6.99 |
29.77 ± 7.23 |
30.47 ± 5.93 |
0.850 |
|
Height (cm) |
169.33 ± 8.71 |
170.69 ± 5.96 |
169.60 ± 7.68 |
0.794 |
|
Weight (kg) |
55.88 ± 9.66 |
57.62 ± 9.37 |
59.10 ± 6.47 |
0.410 |
|
HADS-A |
6.52 ± 3.75** |
5.27 ± 2.66* |
3.40 ± 2.01 |
0.001 |
|
HADS-D |
5.90 ± 3.99** |
3.65 ± 2.87 |
3.00 ± 1.72 |
0.002 |
|
Disease duration (months) |
88.29 ± 52.76 |
68.77 ± 45.04 |
— |
0.178 |
|
CDAI |
93.86 ± 36.00### |
44.52 ± 30.74 |
— |
0.000 |
|
IBDQ |
162.95 ± 29.74## |
187.77 ± 18.76 |
— |
0.003 |
|
PLT |
229.81 ± 33.00 |
209.00 ± 49.63 |
— |
0.106 |
|
ESR |
12.37 ± 5.10 |
9.85 ± 5.70 |
— |
0.123 |
|
CRP |
5.46 ± 2.35## |
2.92 ± 2.72 |
— |
0.002 |
|
CDEIS |
1.24 ± 0.76 |
0.89 ± 0.50 |
— |
0.068 |
|
Montreal classificationΔ |
|||||
Age at diagnosis |
A1 |
0 |
4 |
— |
0.074 |
A2 |
20 |
22 |
— |
||
A3 |
1 |
0 |
— |
||
Location |
L1 |
3 |
7 |
— |
0.606 |
L2 |
4 |
5 |
— |
||
L3 |
14 |
14 |
— |
||
L4 |
0 |
0 |
— |
||
Behavior |
B1 |
7 |
9 |
— |
0.385 |
B2 |
1 |
2 |
— |
||
B3 |
6 |
7 |
— |
||
B1P |
0 |
4 |
— |
||
B2P |
1 |
0 |
— |
||
B3P |
6 |
4 |
— |
||
Concomitant medication |
15 |
15 |
— |
0.240 |
|
5-Aminosalicylate |
9 |
7 |
— |
||
Azathioprine |
3 |
7 |
— |
||
5-Aminosalicylate & azathioprine |
3 |
1 |
— |
||
*P < 0.05 and **P < 0.01 compared with the HC group; ##P < 0.01 and ###P < 0.001, compared with the pain-free group; Δ Montreal classification: A1, below 16 years; A2, between 17-40 years; A3, above 40 years; L1, ileal; L2, colonic; L3, ileocolonic; L4, isolated upper disease; B1, non-stricturing, non-penetrating; B2, structuring; B3, penetrating; P, perianal disease modifier. CD, Crohn’s disease; CDAI, Crohn’s Disease Activity Index; CDEIS, Crohn’s disease endoscopic index of severity; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HADS-A, Hospital Anxiety and Depression Scale anxiety score; HADS-D, Hospital Anxiety and Depression Scale depression score; HCs, healthy controls; IBDQ, Inflammatory Bowel Disease Questionnaire; PLT, platelet. Values are presented as the mean values (standard deviations).
The CDAI scores of all the patients were correlated with the CDEIS scores (r = 0.445, P < 0.01), CRP levels (r = 0.361, P < 0.05), PLT levels (r = 0.407, P < 0.01), and ESR levels (r = 0.431, P < 0.01).
Differences in GM volume
A one-way ANOVA revealed that the GM volumes of 4 brain regions, including the left insula, hippocampal and parahippocampal cortex (HIPP/paraHIPP) and putamen, and right anterior cingulate cortex (ACC) (Table 2, Figure 1A), were significantly different among the pain, pain-free, and HC groups.
Table 2: Brain regions with significant differences in GM volume among the CD with pain, pain-free CD, and HC groups
Regions |
Hem |
BA |
MNI |
F value |
Voxels |
||
|---|---|---|---|---|---|---|---|
X |
Y |
Z |
|||||
ACC |
R |
32 |
3 |
51 |
15 |
7.98 |
151 |
Insula |
L |
47 |
39 |
21 |
3 |
9.61 |
137 |
HIPP/paraHIPP |
L |
28 |
-18 |
–6 |
-24 |
10.09 |
178 |
Putamen |
L |
11 |
-24 |
15 |
-3 |
17.56 |
417 |
The results were based on the total GM volume, age, gender, weight, anxiety and depression as covariates. The statistical threshold was set at P < 0.05, and the false discovery rate was corrected for multiple comparisons. ACC, anterior cingulate cortex; CD, Crohn’s disease; HC, healthy controls; HIPP/paraHIPP, hippocampal and parahippocampal cortex; L, left hemisphere; R, right hemisphere.
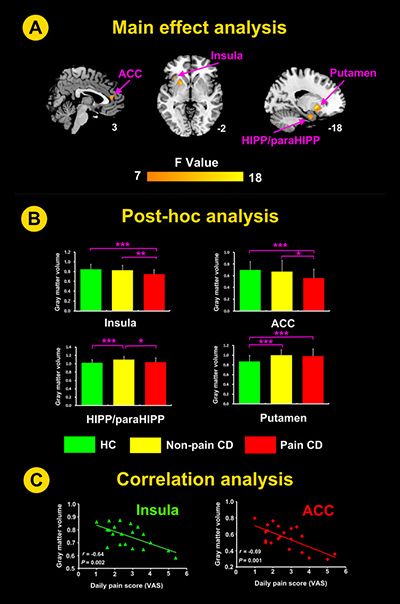
Figure 1: Significant differences in GM volumes in patients with CD-related pain, CD without pain, and HC groups with total GM volume, age, gender, weight, anxiety and depression as covariates. (A) GM volumes of the putamen, HIPP/paraHIPP, insula and ACC differed significantly among the 3 groups. (B) Post-hoc analysis showed that the GM volumes of the insula and ACC in the CD with pain group were lower than the GM volumes in the remaining two groups. The GM volumes of the HIPP/paraHIPP in the pain-free group were higher than the GM volumes in the remaining two groups. The GM volumes of the putamen in the HC group were lower than the GM volumes in the remaining two groups, but the CD with pain and pain-free CD groups were not significantly different. (C) Correlation analysis between the GM volumes of the ROIs in the CD with pain group and the pain scores. ACC, anterior cingulate cortex; CD, Crohn’s disease; HC, healthy controls; HIPP/paraHIPP, hippocampal and parahippocampal cortex; L, left hemisphere; r, correlation coefficient; ROI, region of interest; VAS, visual analogue scale; *P < 0.05, **P < 0.01, ***P < 0.005.
The post-hoc analysis showed that the GM volumes of the insula and ACC in the pain group were lower than those in the pain-free and the HC groups. The GM volumes of the HIPP/paraHIPP in the pain-free group were higher than those in the pain and HC groups. The GM volumes of the putamen in the pain and pain-free CD groups were higher than those in the HC group; however, the difference between the two patient groups was not significant (Table 3, Figure 1B).
Table 3: The post-hoc analysis of the GM volume in the brain regions with significant differences among the CD with pain, pain-free CD, and HC groups
Regions |
CD with pain (n =21) |
Pain-free CD (n =26) |
HC (n= 30) |
Pain vs. pain-free |
Pain vs. HC |
Pain-free vs. HC |
|||
|---|---|---|---|---|---|---|---|---|---|
Effect size |
P value |
Effect size |
P value |
Effect size |
P value |
||||
ACC_R |
0.56±0.15 |
0.67 ± 0.19 |
0.70 ± 0.14 |
0.64 |
0.02 |
0.96 |
0.002 |
0.18 |
0.432 |
Insula_L |
0.75 ± 0.09 |
0.83 ± 0.10 |
0.85 ± 0.10 |
0.84 |
0.009 |
1.05 |
0.001 |
0.20 |
0.417 |
HIPP/paraHIPP_L |
1.04 ± 0.10 |
1.10 ± 0.10 |
1.02 ± 0.08 |
0.70 |
0.018 |
0.22 |
0.295 |
1.06 |
0.000 |
Putamen_L |
0.98 ± 0.15 |
1.00 ± 0.11 |
0.87± 0.12 |
0.15 |
0.619 |
0.81 |
0.003 |
1.13 |
0.000 |
Data are present as mean ± SD. ACC, anterior cingulate cortex; CD, Crohn’s disease; HC, healthy controls; HIPP/paraHIPP, hippocampal and parahippocampal cortex; L, left hemisphere; R, right hemisphere.
These results suggested that the patients with CD-related abdominal pain yielded the lowest GM volumes in the insula and ACC whereas the CD patients without abdominal pain exhibited the highest GM volumes in the HIPP/paraHIPP.
Correlation between GM volumes and the severity of abdominal pain
The GM volumes of the insula and ACC were significantly negatively correlated with the daily pain scores in the patients with abdominal pain (r = -0.64, P = 0.002; r = -0.69, P = 0.001, respectively; Figure 1C). The GM volumes in the HIPP/paraHIPP of the CD patients with abdominal pain were not significantly correlated with the daily pain scores (r = -0.30, P = 0.18).
For the whole-brain analysis, the daily pain scores negatively correlated with the GM volumes of the right ACC, left OFC and bilateral insula (Table 4, Figure 2).
Table 4: Whole-brain correlation analysis between the GM volumes and daily pain scores in CD patients with abdominal pain
Regions |
Hem |
BA |
MNI |
T Value |
Voxels |
||
|---|---|---|---|---|---|---|---|
X |
Y |
Z |
|||||
ACC |
R |
11 |
3 |
36 |
–3 |
–4.37 |
127 |
Insula |
R |
47 |
41 |
24 |
0 |
–4.86 |
134 |
Insula |
L |
47 |
–38 |
21 |
0 |
–5.56 |
120 |
OFC |
L |
11 |
–3 |
58 |
–9 |
–5.33 |
123 |
The results employed age, gender, weight, anxiety and depression as covariates. The statistical threshold was set at P < 0.005 (uncorrected) and cluster P < 0.05 (false discovery rate corrected). ACC, anterior cingulated cortex; BA, Brodmann area; Hem, hemisphere; L, left; OFC, orbitofrontal cortex; R, right.
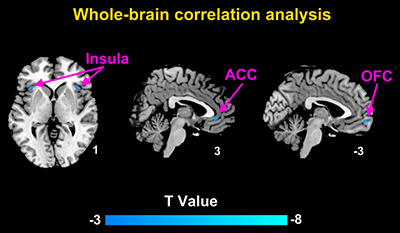
Figure 2: Brain regions with significant correlation between the GM volumes and daily pain scores in CD patients with abdominal pain using whole-brain correlation analysis. The daily pain scores correlated negatively with the GM volumes of the right ACC, left OFC, and bilateral insula.
DISCUSSION
In the present study, we found the lowest GM volumes in the insula and ACC in remissive CD patients with abdominal pain. The reduced GM volumes in the insula and ACC were correlated with the daily pain scores of the patients. The patients without abdominal pain exhibited the highest GM volumes in the HIPP/paraHIPP. These findings suggested that the structural reorganization of the brain varied between CD patients with abdominal pain and those without pain, which may indicate a relationship between changes in specific brain structures and the existence of visceral pain in patients with intestinal inflammatory disease.
Similar to the observations in the patients with CD-related abdominal pain, abnormal changes in GM structures in the insula and ACC occur in patients afflicted with other chronic diseases such as lower back pain [15], irritable bowel syndrome [9] and fibromyalgia [16] and also similar to functional activity changes in these CD patients reported in our previous study [17]. These brain areas are important components of pain networks [18, 19]. The ACC and insula are the key components of the medial pain system, which might be primarily involved in processing affective-motivational aspects of pain. Studies [20, 21] have shown that the ACC is not only involved in the transmission of pain sensations but also plays a role in processing pain-related emotion. The ACC might respond to pain and participate in pain control [20]. The insula participates in the integration of visceral sensation and motor function and is responsible for transmitting pain signals to the frontal cortex [10].
The visceral pain (abdominal pain) signals may be transmitted to the "visceral and cortical pain matrix" via the brain - gut axis in CD patients [3]. Specifically, pain fibers carrying visceral nociceptive signals from the periphery synapse traverse through unmyelinated C fibers on both sides of the spinal cord to the dorsal root ganglia of spinal afferent nerves and synapse onto dorsal horn neurons and then ascend to the higher order brain processing areas in the thalamic nuclei and reticular formation [3]. The thalamic nuclei project to the primary and secondary somatosensory cortex where the sensory-discriminative aspects of pain is processed, and the reticular formation projects to the limbic system and frontal cortex, where the affective-motivational aspects of pain is processed [3, 20]. In this way, visceral pain signals in CD patients may be mainly transmitted to ACC and insula of the limbic system via the reticular formation.
We found that the GM volumes in the insula and ACC were negatively correlated with the daily pain scores in the patients with abdominal pain. The whole-brain analysis further confirmed the correlation and increased the reliability of the study. Structural GM abnormalities in the insula and ACC have been observed in nearly all pain-related diseases [22]. Similar negative correlations between GM volume and pain severity have also been observed in other imaging studies on GM plasticity, such as post-herpetic neuralgia, chronic back pain, and osteoarthritis [23]. The pain in CD patients in clinical remission is chronic, involves multiple factors. CD patients with abdominal pain yielded higher disease condition indices (CDAI scores and CRP levels) and significantly lower quality of life (QOL) than patients without abdominal pain, suggesting that the pain may not only be involved in the afferent processing of visceral pain signals, but may also be related to the stimulation of low inflammation in peripheral circulation.
In general, the mechanism underlying GM changes may be attributed to frequent and chronic nociceptive input and the subsequent functional reorganization and plasticity of the brain. The lower GM volumes could be related to a decrease in the size of neuronal somata, cell atrophy, or a decrease in intra-cortical axonal architecture (i.e., synaptic loss) [24]. In addition to the afferent processing of visceral pain signals, circulating inflammatory cytokines/mediators can reach the brain through circumventricular organs and active transport [25, 26], which may promote GM changes by inducing the apoptosis of neural or glial cells, including astrocytes and oligodendrocytes [27, 28], and activating endothelial cells, microglial cells, and macrophages. Furthermore, inflammatory cytokines/mediators may propagate signals within the brain by suppressing neurogenesis and exerting cytotoxic effects via increased glutamatergic activation and increased oxidative stress [28]. Thus, interactions among chronic nociceptive input, inflammation-induced neuronal changes, and brain reorganization may contribute to the reduced GM volumes in brain regions that are observed during pain processing and perception.
The patients without CD-related pain exhibited the highest GM volumes in the HIPP/paraHIPP, while the patients with CD-related pain exhibited lower GM volumes in this region. These findings suggest a role for specific brain structures in the control of abdominal pain in this disease: patients with the highest GM volumes exhibited better intrinsic pain relief (CD without pain) than patients with a lesser GM volumes increase (CD with pain). The HIPP/paraHIPP is associated with limbic and non-limbic system structures; the HIPP/paraHIPP regulates immune responses via the hypothalamic-pituitary-adrenal axis and neurohumoral pathways and plays an important role in neural immune regulation [29]. Studies have shown that experimental colitis and intestinal dysbiosis are associated with aberrant mRNA or protein expression of brain-derived neurotrophic factor in the HIPP/paraHIPP and the abnormal development of anxiety-like behavior [30]. The HIPP/paraHIPP may also interact with the vagus nerve, which is involved in the neural modulation of intestinal inflammation by releasing acetylcholine to regulate the functions of immune cells in the intestinal wall. In addition, an abnormal blood oxygen level-dependent (BOLD) signal has been found in the HIPP/paraHIPP in inflammatory bowel disease patients relative to control subjects [31]. Furthermore, given the critical role of the HIPP/paraHIPP in pain processing and modulation [32] and the finding that the highest GM volumes were present in the patients without abdominal pain may suggest an enhanced compensation by this region.
The present study has two limitations. First, this study was a cross-sectional study, which prevented the confirmation of a relationship between the abnormal GM changes in the CD patients in remission with the disease onset or the disease per se. In addition, neurotransmitter modulation and receptor binding in the associated brain areas and the correlation of these parameters with the GM structural changes must be elucidated. Future studies should observe longitudinal brain GM changes, together with the levels of related neurotransmitters in target brain regions, and to elucidate the neuroimaging biomarkers of CD.
In summary, our study represents the first investigation to demonstrate differences in brain GM volumes between CD patients in remission with and without abdominal pain. The reduced GM volumes in the insula and ACC in patients with CD with abdominal pain suggest a potential role in visceral pain processing and correlate with the presence and severity of abdominal pain. The findings may expand our understanding of the pathogenesis of CD, particularly the pathophysiology underlying pain in patients with CD.
MATERIALS AND METHODS
Subjects
All participants provided written informed consent. The study protocol was approved by the Institutional Review Board of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine at Shanghai University of Traditional Chinese Medicine.
This study evaluated 21 patients with CD-related abdominal pain, 26 CD patients without abdominal pain, and 30 HCs. All the patients underwent a systemic and gastrointestinal examination, including a colonoscopy and pathological tissue biopsy. Laboratory tests and the colonoscopy were performed at 2 weeks and 1 month before the MRI scan, respectively. The CRP level, ESR, and PLT level were measured in all the patients. For the endoscopic examination, the CDEIS scores [33] were scored by an experienced endoscopist who was blinded to other details of the patients with CD.
The HCs were recruited via advertisements from Shanghai University of Traditional Chinese Medicine. These subjects were not treated with any medications, had no gastrointestinal symptoms or pain-related diseases, nor had negative findings in colonoscopic examinations.
Eligibility criteria
The inclusion criteria were as follows: aged between 18 and 50 years, ≥ 6 years of education, right-handed, a CDAI of < 150, a CDEIS score of < 3 and in disease remission for > 12 months. Patients were excluded from the study if they met any of the following conditions: elevated biological disease activity indices (CRP > 10 mg/L, ESR > 20 mm/h, PLT > 300×109/L); a history of CD-related abdominal surgery; treatment with corticosteroids, biological agents, psychotropic or opioid drugs in the previous 3 months; pregnant or lactating; a current or past history of psychiatric or neurological disorders, head trauma or loss of consciousness; claustrophobic; or had metal implants.
Furthermore, CD patients with chronic abdominal pain (i.e., dull periumbilical pain and/or pain in the right/left lower quadrant, etc. for ≥ 3 days per week for at least 12 months) were included in the pain group. Patients without abdominal pain for at least 12 months were included in the pain-free group.
Symptoms and psychological assessment
The intensity of abdominal pain in the CD patients was evaluated using a 0-10 visual analog scale (VAS) [34]. The average pain score was calculated by dividing the total pain score by the number of days of pain during the week prior to the MRI scan. The CDAI [35] and the IBDQ [36] were used to evaluate the patients’ disease conditions and QOL, respectively.
The HADS [37] was used to assess the psychological status, including anxiety and depression, of all the subjects. The HADS included 14 questionnaire items and 7 items for each of the two sub-scales (anxiety and depression). Each item had a 4-point Likert scale (0-3 points) and a sub-scale of more than 8 points indicating anxiety or depression.
Image acquisition
The MRI data were acquired in an interleaved multi-slice mode using a Siemens TRIO 3T clinical scanner (Magnetom Verio, Siemens, Erlangen, Germany). A high-resolution T1-weighted sagittal 3-dimensional magnetization-prepared rapid gradient-echo sequence was acquired for each participant with the following parameters: TR = 2300 ms; TE = 2.98 ms; field of view = 256 × 256 mm; matrix size = 256 × 256; in-plane resolution = 1 mm × 1 mm; slice thickness = 1.0 mm; flip angle = 9°; and slices = 176.
Image analysis
Voxel-based morphometry (VBM) preprocessing
Structural image processing and analysis were performed using optimized VBM8 toolbox (C. Gaser, Department of Psychiatry, University of Jena, Germany; http://dbm.neuro.uni-jena.de/vbm8) in the Statistical Parametric Mapping software, version 12 (SPM12; Wellcome Trust Centre for Neuroimaging, University College London, England; http://www.fil.ion.ucl.ac.uk/spm), which was operated in a MATLAB (Mathworks, Natick, MA, USA) environment. All the structural images were transformed into a Montreal Neurological Institute (MNI) 152 standard space using linear transformations re-sampled to 1.5 × 1.5 × 1.5 mm3. The images were subsequently segmented into GM, white matter (WM), and cerebrospinal fluid (CSF). A modulation step was added to incorporate volume changes during spatial normalization [38]. This step involved multiplying each spatially normalized GM image by the relative volume of the image before and after normalization. The resulting GM images were smoothed with an 8-mm full-width-at-half-maximum (FWHM) isotropic Gaussian kernel.
Statistical analysis
At the secondary level of analysis, we determined the differences in the GM volumes among the HCs and the patients with or without pain. A one-way analysis of variance (ANOVA) was performed at each voxel to assess the main effect, with a statistical threshold was set at P < 0.005 (uncorrected) and cluster P < 0.05 [false discovery rate (FDR) corrected]. The total GM volume, age, gender, weight, anxiety and depression were used as covariates.
For post hoc tests, regions of interest (ROIs) were selected from the sets of voxels within 6-mm spheres, with the centers at the peaks of the clusters with significant differences based on the ANOVA results of the VBM between the patients and the HCs. A 2-step correlation analysis was conducted in CD patients with abdominal pain: first, a Pearson’s correlation analysis was used to examine the relationship between the mean GM volume in each ROI and the pain score for the CD patients, with the total GM volume, age, gender, weight, anxiety and depression as covariates. The significance level was set at P < 0.05 with Bonferroni’s correction. Second, whole-brain correlation analysis was applied to determine potential correlations between the brain regions and pain condition. The significance level was set at P < 0.005 (uncorrected), and the FDR was corrected with the cluster size at P < 0.05.
The imaging results were overlaid on MRIcroN (http://www.sph.s.c.edu/comd/rorden/mricro.html) for presentation. The behavioral data were presented as the means ± standard deviations. The Statistical Package for the Social Sciences (SPSS) software package (SPSS Inc., Chicago, IL, USA), version 16.0, was used for the statistical analysis.
Author contributions
CHB, PL, HRL, and HGW were responsible for the study protocol and design; CHB, HRL, LYW, XQZ, JYZ and YS contributed to data acquisition; PL and DW assisted with data analysis and interpretation; CHB and PL drafted of the manuscript; XMJ and YS provided critical revision of the manuscript.
ACKNOWLEDGMENTS AND FUNDING
Many thanks to Chen Zhao, Hui Feng, Yuan Lu, Yifang Zhu, and Chunbin Song for their assistance in the recruitment of subjects, Lili Ma for her assistance in the endoscopic examination and data acquisition and to Xiaoming Liu for his technical assistance with the data analysis. This work was supported by the National Key Basic Research Program of China (973 program), No. 2009CB522900, 2015CB554501; the Program for Outstanding Medical Academic Leader, No.80; the Program of Shanghai Academic Research Leader, No.17XD1403400 and the National Natural Science Foundation of China, No.81471738 and 81771918.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Wagtmans MJ, Verspaget HW, Lamers CB, van Hogezand RA. Crohn's disease in the elderly: a comparison with young adults. J Clin Gastroenterol. 1998; 27:129–133.
2. Bielefeldt K, Davis B, Binion DG. Pain and inflammatory bowel disease. Inflamm Bowel Dis. 2009; 15:778–788.
3. Srinath A, Young E, Szigethy E. Pain management in patients with inflammatory bowel disease: translational approaches from bench to bedside. Inflamm Bowel Dis. 2014; 20:2433–2449.
4. Bonaz BL, Bernstein CN. Brain-Gut Interactions in Inflammatory Bowel Disease. Gastroenterology. 2013; 144:36–49.
5. Vivinus-Nebot M, Frin-Mathy G, Bzioueche H, Dainese R, Bernard G, Anty R, Filippi J, Saint-Paul MC, Tulic MK, Verhasselt V, Hebuterne X, Piche T. Functional bowel symptoms in quiescent inflammatory bowel diseases: role of epithelial barrier disruption and low-grade inflammation. Gut. 2014; 63:744–752.
6. Makharia GK. Understanding and treating abdominal pain and spasms in organic gastrointestinal diseases: inflammatory bowel disease and biliary diseases. J Clin Gastroenterol. 2011; 45:S89.
7. Vermeulen W, De Man JG, Pelckmans PA, De Winter BY. Neuroanatomy of lower gastrointestinal pain disorders. World J Gastroenterol. 2014; 20:1005–1020.
8. Blankstein U, Chen J, Diamant NE, Davis KD. Altered brain structure in irritable bowel syndrome: potential contributions of pre-existing and disease-driven factors. Gastroenterology. 2010; 138:1783–1789.
9. Seminowicz DA, Labus JS, Bueller JA, Tillisch K, Naliboff BD, Bushnell MC, Mayer EA. Regional gray matter density changes in brains of patients with irritable bowel syndrome. Gastroenterology. 2010; 139:48.
10. Frøkjær JB, Bouwense SA, Olesen SS, Lundager FH, Eskildsen SF, Van GH, Wilder-Smith OH, Drewes AM. Reduced cortical thickness of brain areas involved in pain processing in patients with chronic pancreatitis. Clin Gastroenterol Hepatol. 2012; 10:434.
11. Obermann M, Rodriguez-Raecke R, Naegel S, Holle D, Mueller D, Yoon MS, Theysohn N, Blex S, Diener HC, Katsarava Z. Gray matter volume reduction reflects chronic pain in trigeminal neuralgia. Neuroimage. 2013; 74:352–358.
12. Bao CH, Liu P, Liu HR, Wu LY, Shi Y, Chen WF, Qin W, Lu Y, Zhang JY, Jin XM, Wang XM, Zhao JM, Liu XM, et al. Alterations in Brain Grey Matter Structures in Patients With Crohn’s Disease and Their Correlation With Psychological Distress. J Crohns Colitis. 2015; 20151–9.
13. Nair VA, Beniwalpatel P, Mbah I, Young BM, Prabhakaran V, Saha S. Structural Imaging Changes and Behavioral Correlates in Patients with Crohn’s Disease in Remission. Front Hum Neurosci. 2016; 10:460.
14. Thomann AK, Thomann PA, Wolf RC, Dusan H, Christian S, Ebert MP, Kristina S, Wolfgang R, Martin G. Altered Markers of Brain Development in Crohn’s Disease with Extraintestinal Manifestations – A Pilot Study. Plos One. 2016; 11:e0163202.
15. Seminowicz DA, Wideman TH, Naso L, Hatamikhoroushahi Z, Fallatah S, Ware MA, Jarzem P, Bushnell MC, Shir Y, Ouellet JA. Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function. J Neurosci. 2011; 31:7540–7550.
16. Puri BK, Agour M, Gunatilake KD, Fernando KA, Gurusinghe AI, Treasaden IH. Reduction in left supplementary motor area grey matter in adult female fibromyalgia sufferers with marked fatigue and without affective disorder: a pilot controlled 3-T magnetic resonance imaging voxel-based morphometry study. J Int Med Res. 2010; 38:1468–1472.
17. Bao CH, Liu P, Liu HR, Wu LY, Jin XM, Wang SY, Shi Y, Zhang JY, Zeng XQ, Ma LL, Qin W, Zhao JM, Calhoun VD, et al. Differences in regional homogeneity between patients with Crohn's disease with and without abdominal pain revealed by resting-state functional magnetic resonance imaging. Pain. 2016; 157:1037.
18. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. European journal of pain. 2005; 9:463–484.
19. May A. Structural brain imaging: a window into chronic pain. Neuroscientist. 2011; 17:209–220.
20. Xie YF, Huo FQ, Tang JS. Cerebral cortex modulation of pain. Acta Pharmacol Sin. 2009; 30:31–41.
21. Ma LQ, Ning L, Wang Z, Wang YW. Visual and noxious electrical stimulus-evoked membrane-potential responses in anterior cingulate cortical neurons. Mol Brain. 2016; 1;9:82.
22. Oudenhove LV, Coen SJ, Aziz Q. Functional brain imaging of gastrointestinal sensation in health and disease. World J Gastroenterol. 2007; 13:3438–3445.
23. Apkarian AV, Baliki MN, Geha PY. Towards a theory of chronic pain. Prog Neurobiol. 2009; 87:81–97.
24. May A. Chronic pain may change the structure of the brain. Pain. 2008; 137:7–15.
25. Konsman JP, Kelley K, Dantzer R. Temporal and spatial relationships between lipopolysaccharide-induced expression of Fos, interleukin-1beta and inducible nitric oxide synthase in rat brain. Neuroscience. 1999; 89:535.
26. Quan N, Banks WA. Brain-immune communication pathways. Brain Behav Immun. 2007; 21:727.
27. Buntinx M, Moreels M, Vandenabeele F, Lambrichts I, Raus J, Steels P, Stinissen P, Ameloot M. Cytokine-induced cell death in human oligodendroglial cell lines: I. Synergistic effects of IFN-γ and TNF-α on apoptosis. J Neurosci Res. 2004; 76:834.
28. Miller AH, Maletic V, Raison CL. Inflammation and Its Discontents: The Role of Cytokines in the Pathophysiology of Major Depression. Biological Psychiatry. 2009; 65:732–741.
29. Lathe R. Hormones and the hippocampus. J Endocrinol. 2001; 169:205.
30. Hassan AM, Jain P, Reichmann F, Mayerhofer R, Farzi A, Schuligoi R, Holzer P. Repeated predictable stress causes resilience against colitis-induced behavioral changes in mice. Front Behav Neurosci. 2014; 8:386.
31. Agostini A, Filippini N, Benuzzi F, Bertani A, Scarcelli A, Leoni C, Farinelli V, Riso D, Tambasco R, Calabrese C. Functional magnetic resonance imaging study reveals differences in the habituation to psychological stress in patients with Crohn's disease versus healthy controls. J Behav Med. 2013; 36:477–487.
32. Wang H. Role of the hippocampus on learning and memory functioning and pain modulation. Neural Regen Res. 2008; 3:569–572.
33. Mary JY, Modigliani R. Development and validation of an endoscopic index of the severity for Crohn ' s disease : a prospective multicentre study. Gut. 1989; 30:983–989.
34. Akbar A, Yiangou Y, Facer P, Brydon WG, Walters JR, Anand P, Ghosh S. Expression of the TRPV1 receptor differs in quiescent inflammatory bowel disease with or without abdominal pain. Gut. 2010; 59:767.
35. Best WR, Becktel JM, Singleton JW. Rederived values of the eight coefficients of the Crohn's Disease Activity Index (CDAI). Gastroenterology. 1979; 77:843.
36. Irvine EJ, Feagan B, Rochon J, Archambault A, Fedorak RN, Groll A, Kinnear D, Saibil F, Mcdonald JW. Quality of life: a valid and reliable measure of therapeutic efficacy in the treatment of inflammatory bowel disease. Canadian Crohn's Relapse Prevention Trial Study Group. Gastroenterology. 1994; 106:287–296.
37. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983; 67:361.
38. Good CD, Johnsrude IS, Ashburner J, Henson RN, Friston KJ, Frackowiak RS. A Voxel-Based Morphometric Study of Ageing in 465 Normal Adult Human Brains. Neuroimage. 2001; 14:21.