
INTRODUCTION
Lung cancer is the main cause of cancer-related mortality in men and second to breast cancer in women. The majority of patients is diagnosed at an advanced stage with 5-year survival rates with conventional chemotherapy regimens of about 5%. The most common type is non-small cell lung cancer (NSCLC) with adenocarcinoma (AC) as the main subtype with rising incidence. A subgroup of NSCLC harbors an oncogenic driver, in particular activating EGFR mutations, ALK- or ROS1 translocations, or BRAF mutations. These oncogenic drivers are almost exclusively present in AC. In 2004, it was reported that activating mutations in EGFR predict response to specific EGFR-tyrosine kinase inhibitors (TKIs) in NSCLC patients [1, 2]. In the following, these EGFR-TKI sensitizing mutations are referred to as “EGFR-positive”.
Unlike conventional chemotherapy reagents, TKI are mainly cytostatic compounds that interfere with a specific mechanism driving tumor growth. Several trials confirmed the superiority of the reversible 1st generation EGFR-TKIs gefitinib and erlotinib, and the irreversible 2nd generation EGFR-TKI afatinib over cytotoxic chemotherapy in terms of response and progression-free survival (PFS) both in pretreated and untreated EGFR-positive NSCLC [3, 4, 5, 6]. In ALK-rearranged NSCLC, the ALK-TKIs crizotinib, ceritinib, and more recently alectinib have shown superior response and PFS compared to chemotherapy irrespective of treatment line [7, 8, 9, 10]. Furthermore, uncontrolled studies showed high response rates to crizotinib and ceritinib in ROS1-rearranged NSCLC [11, 12], and to dabrafenib and vemurafenib (more recently combined with a MEK-inhibitor, e. g. trametinib) in BRAF-mutated (V600E) NSCLC [13, 14, 15]. Thus, the presence of a driver mutation predicts response to specific TKIs. Moreover, EGFR-positive NSCLC and probably ROS1-rearranged NSCLC are associated with improved prognosis [16, 17], whereas this is appears not to be the case for ALK- or BRAF-positive NSCLC [18, 19].
Mainly due to crossover, a benefit of EGFR-TKI therapy in EGFR-positive NSCLC on overall survival (OS) is hard to demonstrate in the context of prospective randomized trials [20, 21, 22, 23]. Thus, prospective clinical trials are of limited value for the assessment of the effect of TKI-therapy on OS [24]. However, retrospective analyses of OS of patients with advanced inoperable EGFR-positive NSCLC on EGFR-TKI-therapy reported a median OS of 25-31 months and a 5-year survival of 15-20% [25, 26, 27]. These reports together with historic comparisons of survival of EGFR-mutation positive patients before and after availability of EGFR-TKI therapy [28, 29], post-hoc pooled survival analysis of patients with EGFR-TKI sensitive NSCLC (del exon 19 only) [20], and prospective non-randomized data from the Lung Cancer Mutation Consortium [30] have strengthened the general assumption that EGFR-TKI-therapy also improves OS. However, a controversy remains as to whether 1st line EGFR-TKI therapy confers an OS advantage compared to 2nd line EGFR-TKI therapy [31]. A survival advantage was reported for 1st line EGFR-TKI therapy in a Chinese retrospective analysis [32]. This contrasts with findings from the nationwide French survival data recently presented pointing to an OS benefit of EGFR-mutation positive patients treated with EGFR-TKI 2nd line [33] and with recent clinical evidence of poorer efficacy of chemotherapy after EGFR-TKI [34]. The only study directly comparing a second generation EGFR-TKI (afatinib) with a first generation EGFR-TKI (gefitinib) as first-line therapy did not reveal a difference in OS [35]. Despite good response to TKI therapy in driver-mutation positive NSCLC, resistance develops after generally less than one year. In the case of EGFR-positive NSCLC, resistance is due to the de novo mutation T790M in EGFR exon 20 in more than 50% of cases [36]. The 3rd generation EGFR-TKI osimertinib has recently been shown to be active in T790M-mutated NSCLC [37].
Most studies on driver-mutation positive NSCLC are based on Eastern Asian populations because of a higher incidence [38]. ‘Real world data’ from routine clinical practice on driver mutations, treatment, and long-term survival in Caucasian lung cancer patients are still scarce. Such data are, however, important to assess performance of precision medicine approaches in daily clinical practice and to guide testing as well as clinical management and therapy of NSCLC patients. To bridge this gap, we here report prevalence and distribution of driver mutations, treatment modalities, and analysis of resistance mechanisms in a current predominantly Caucasian patient population and performed a retrospective case-control analysis of OS.
RESULTS
Baseline characteristics
Eight-hundred twenty-four patients were diagnosed with NSCLC from 2006-2015. A detailed analysis of the full patient cohort is in preparation and will be reported elsewhere. An EGFR-mutation test result was available for 322 patients (39%). In none of the 57 non-AC patients with EGFR-test results, an activating EGFR mutation was detected. The following analysis focuses on 265 patients with AC histology or adenosquamous histology for whom EGFR-test results were available (59.8% of all AC patients). Of these patients, 188 (70.9%) had died at databank lock. Of the 77 living patients, 71 (92.2%) had attended the last scheduled follow-up examination (at least once a year until five years after diagnosis). Thus, follow-up was complete for 259 patients (97.7%). Median follow-up of living patients was 36.6 months.
Baseline clinical characteristics and results of molecular testing are given in Table 1. The EGFR-tested population had a better performance status and included a higher proportion of women (51% of tested patients, 46% of all AC patients) and of never-smokers (29% of tested patients, 21% of all AC patients) than the unselected AC population. 84% of never-smokers had an EGFR-test result compared to 60% of the unselected AC population. Histological grading of the tumor influenced the likelihood of being tested for EGFR-mutational status (Table 2). Whereas 76% of well differentiated G1 tumors had a test result available, this was the case for only 55-59 % of less well differentiated tumors or tumors for which no grading was reported.
Table 1: Clinical characteristics of unselected AC patients, AC patients with driver-mutation test result, and case-control patients for analysis of driver-mutation status and survival
Oncogenic driver mutation |
Adenocarcinoma (AC) |
Unselected population with EGFR-test result |
Case-control patients |
|||
|---|---|---|---|---|---|---|
All patients |
EGFR-tested patients |
Driver-mutation positive |
Driver-mutation negative |
Driver-mutation positive |
Driver-mutation negative |
|
n |
443 |
265 |
55 |
210 |
49 |
|
Age (mean, range) |
67.3 (38.8-94.7) |
67.1 (38.8-88.2) |
68.7 (38.8-87.0) |
66.7 (44.6-88.2) |
68.2 (38.8-84.3) |
67.6 (45.0-86.2) |
Deceased |
316 (71%) |
188 (71%) |
35 (64%) |
153 (73%) |
30 (64%) |
34 (72%) |
Gender |
||||||
Male |
240 (54%) |
129 (49%) |
18 (33%) |
111 (53%) |
16 (33%) |
|
Female |
203 (46%) |
136 (51%) |
37 (67%) |
99 (47%) |
33 (67%) |
|
Stage (UICC 7th ed.) |
||||||
IA/B |
49/41 (20%) |
17/18 (13%) |
3/5 (15%) |
13/13 (13%) |
3/4 (14%) |
|
IIA/B |
22/19 (9%) |
12/13 (9%) |
2/3 (9%) |
10/9 (9%) |
1/3 (8%) |
|
IIIA/B |
41/28 (16%) |
23/16 (15%) |
5/3 (15%) |
18/13 (15%) |
4/3 (14%) |
|
IV M1a/M1b |
87/156 (55%) |
61/105 (63%) |
11/23 (62%) |
49/82 (63%) |
12/19 (63%) |
|
Performance status |
n. a. 1 |
|||||
ECOG 0 |
128 (29%) |
90 (34%) |
24 (44%) |
66 (31%) |
21 (43%) |
|
ECOG 1 |
219 (50%) |
133 (50%) |
24 (44%) |
109 (52%) |
24 (49%) |
|
ECOG 2 |
72 (16%) |
36 (14%) |
6 (11%) |
30 (14%) |
4 (8%) |
|
ECOG 3 |
19 (4%) |
6 (2%) |
1 (2%) |
5 (2%) |
0 |
|
ECOG 4 |
4 (1%) |
0 |
0 |
0 |
0 |
|
Smoking status |
n. a. 16 |
n. a. 2 |
n. a. 2 |
|||
Never-smoker |
91 (21%) |
76 (29%) |
39 (71%) |
37 (18%) |
34 (69%) |
|
Long-term ex-smoker |
156 (37%) |
101 (39%) |
10 (18%) |
91 (44%) |
10 (20%) |
|
Quitter |
92 (22%) |
58 (22%) |
6 (11%) |
52 (25%) |
5 (10%) |
|
Smoker |
88 (21%) |
28 (11%) |
0 |
28 (13%) |
0 |
|
EGFR mutation |
||||||
EGFR status known |
265 |
265 |
55 |
210 |
49 |
|
EGFR positive |
44 (17%) |
44 (17%) |
44 |
0 |
39 (80%)a |
0 |
Del Exon19 |
27b |
27c |
27 |
- |
25 |
- |
Exon21 L858R |
12 |
12 |
12 |
- |
9 |
- |
Exon18 |
5 |
5 |
5 |
- |
5 |
- |
ALK translocation |
||||||
ALK status known |
111 |
111 |
17 |
94 |
13 |
22 |
ALK positive |
8 (7%) |
8 (7%) |
8 |
0 |
7 (14%)b |
0 |
BRAF |
||||||
BRAF status known |
39 |
39 |
6 |
33 |
5 |
7 |
BRAF pos. (V600E)d |
3 (8%) |
3 (8%) |
3 |
0 |
3 (6%)b |
0 |
n. a.: not assessed.
a Percentage of driver-positive case-control population.
b Including one patient with dupExon19 mutation.
c Including one patient with dupExon19 mutation.
d excluding one EGFR-mutation positive patient with BRAF mutation detected after EGFR-TKI treatment as a resistance mutation.
Patients were matched for gender, performance status, clinical stage, smoking status, and age. All patients for oncogenic-driver analysis had AC histology since no driver mutations were detected in other histologies. Matched parameters are given as a single column.
Table 2: Histopathological grading, EGFR-testing and EGFR-positivity in patients with AC
Grade |
All AC patients (n=443) |
EGFR tested (n=265) |
EGFR-positive (n=44) |
|---|---|---|---|
G1 |
38 (8.6%) |
29 (10.9%) |
9 (20.5%) |
G2 |
97 (21.9%) |
55 (20.8%) |
15 (34.1%) |
G3 |
248 (56.0%) |
146 (55.1%) |
12 (27.3%) |
No grade given |
50 (11.3%) |
28 (10.6%) |
4 (9.1 %) |
Adenosquamous |
10 (2.3%) |
7 (2.6%) |
4 (9.1%) |
Oncogenic driver mutations: distribution
Driver mutations were detected in 55 patients of 265 tested AC patients (20.8%). The distribution and frequency of the 55 patients with an oncogenic driver mutation are shown in Figure 1A. Sensitizing EGFR-mutations were most prevalent (79%), followed by ALK-translocations (15%) and the BRAF mutation V600E (6%).

Figure 1: Oncogenic-driver mutation: distribution. (A) Distribution of oncogenic driver mutations in AC patients with EGFR-test result. (B) Distribution of EGFR mutations.
EGFR: Forty-eight EGFR mutations were detected. Forty-four were mutations known to be sensitizing [39, 40, 41, 42]. Four mutations were rare point mutations:
• Transition exon 19 c.2203G>A; p.G735S in a female ex-smoker with AC G3 stage IV (M1b). This mutation has been described twice in lung cancer (COSMIC databank accessed 31.10.2016) with no data on response to EGFR-TKI therapy given in the literature [43, 44]. The patient showed progressive disease on 2nd line EGFR-TKI therapy with gefitinib.
• Transition exon 19 c.2258T>C; p.P753L in a female smoker with SCC stage IIIA. This mutation has not been described previously in lung cancer (COSMIC databank search 31.10.2016). Upon recurrence after resection, the patient was treated 1st-line with erlotinib with early progression after 14 weeks of disease stabilization.
• Transition exon 21 c.2543C>T; p.P848L in a male ex-smoker with AC G1 stage IV (M1b). This patient showed stable disease on erlotinib with a relatively short PFS of 4.6 months. This mutation has been previously described in nine lung samples (COSMIC databank, accessed 31.10.16) and was shown to be non-activating [45].
• Transition exon 21 c.2527G>A; p.V843I mutation in an ex-smoker with NSCLC (NOS) who did not receive targeted EGFR-TKI therapy. This mutation has been reported twice in lung cancer (COSMIC databank, accessed 31.10.16) and is activating from a biological point of view but does not confer sensitivity to EGFR-TKIs [46, 47].
Such point mutations are typically smoking-induced [48]. Since these four mutations do not confer EGFR-TKI sensitivity, they were counted as EGFR-negative for the survival analysis of EGFR-tested patients. Thus, the prevalence of EGFR-positive patients was 16.6% in the tested population. The majority had a del-exon 19 mutations followed by exon 21 point mutation and exon 18 mutations (Figure 1B, Table 3). While 22.8% of tested women were EGFR-positive, only 10.1% of men had an EGFR-positive NSCLC. EGFR-positive patients were older than EGFR-negative patients (70.2 vs. 66.5 years, p=0.038). 31% of tested G1 tumors and 28% of G2 tumors were EGFR-positive, compared to only 8% of G3 tumors (Table 2). In line with a previous report [49], the few patients with adenosquamous carcinoma and an EGFR-test result (n=7) had a high likelihood of a positive result (57%). Based on conventional staining, two of the patients with adenosquamous histology had been initially classified as squamous-cell carcinoma (SCC). However, re-evaluation of these cases including TTF1 immunohistochemistry revealed areas with AC differentiation. None of 36 current smokers tested for EGFR-mutation was EGFR-positive.
Table 3: Patient characteristics and type of EGFR mutation, and EGFR-TKI treatment of EGFR-positive patients
Exon 19 |
Exon 21 |
Exon 18 |
||||
|---|---|---|---|---|---|---|
|
del Exon19 |
dup Exon19 |
Exon19 point mutations (G735S; P753L), non-activating |
L858R |
V843I, activating but not sensitizing; P848L, non-activating |
G719A: 1 |
|
n |
26 |
1 |
2 |
12 |
2 |
5 |
age (mean) |
70.1 |
65.7 |
60.9 |
70.7 |
56.8 |
70.5 |
female/male |
18/8 |
0/1 |
2/0 |
10/2 |
1/1 |
3/2 |
smoking status1 |
0: 18; |
0: 1 |
1: 1 |
0: 8 |
1: 2 |
0: 4 |
histology |
AC 26 |
AC 1 |
AC 1, SCC 1 |
AC 12 |
AC 1, NOS 1 |
AC 5 |
TKI treated |
232 |
1 |
2 |
83 |
1 |
5 |
ECOG4 |
0: 9 |
1: 1 |
1: 2 |
0: 2 |
0: 1 |
0: 3 |
Stage |
I-III: 55 |
IV M1b: 1 |
IV M1a: 1 |
IV M1a: 2 |
IV M1a: 1 |
IV M1a: 3 |
BRA6 |
6 |
1 |
0 |
4 |
1 |
0 |
OSS7 |
13 |
1 |
0 |
4 |
0 |
2 |
other M1b site |
4 |
1 |
1 |
0 |
0 |
0 |
line TKI |
1st: 15 |
1st:1 |
2nd: 2 |
1st: 6 |
1st:1 |
1st: 3 |
1st TKI8 |
A 1 |
E 1 |
E 1 |
A 1 |
E 1 |
A 1 |
response9 to 1st TKI |
CR 1 |
SD 1 |
SD 1 |
PR 8 |
SD 1 |
PR 4 |
progression |
0: 8 |
1: 1 |
1: 2 |
0: 2 |
1: 1 |
0: 1 |
brain as site of 1st progression |
3 |
1 |
0 |
2 |
0 |
1 |
local therapy at progression11 |
RT 5 |
RT 1 |
0 |
RT 2 |
RT 1 |
RT 1 |
1st chemotherapy (carboplatinum-gemcitabine)12 |
7 |
1 |
1 |
4 |
1 |
1 |
response to first chemotherapy6 |
PR 3 |
PD 1 |
PR 1 |
PR 2 |
PR 1 |
PD 1 |
subsequent chemotherapies13 |
Pem 5 |
0 |
0 |
Pem 2 |
Pem, Doce |
Pem 4 |
response to subsequent chemotherapies6 |
PR 2 |
- |
- |
PR 1 |
PD 1, SD 1 |
PR 2 |
switch TKI14 |
A 4 |
A 1 |
E 1 |
A 2 |
- |
- |
response to |
PD 6 |
PR 1 |
PD 1 |
PD 3 |
- |
- |
T790M positive at progression15 |
7 (n=8) |
n. a. |
n. a. |
n. a. |
n. a. |
1 (n=3) |
3rd gen TKI |
7 |
- |
- |
- |
- |
1 |
1 0: never smoker, 1: ex-smoker, 2: smoker.
2 Performance status at start of TKI.
3 BRA: Brain metastases present at start of TKI-therapy.
4 OSS: Bone metastases present at start of TKI-therapy.
5 A: afatinib; E: erlotinib; G: gefitinib.
6 Number of patients with complete remission (CR), partial remission (PR), stable disease (SD), or progressive disease (PD).
7 0: no progression; 1: progression at last observation.
8 RT: radiotherapy (number of patients).
9 EGFR-TKI holiday during platinum doublett chemotherapy.
10 No EGFR-TKI holiday during subsequent mono-chemotherapies. Pem: pemetrexed; Gem: gemcitabine; Doce: docetaxel; Pac: paclitaxel.
11 Number of patients receiving another 1st/2nd generation EGFR-TKI after progression on TKI.
12 Number of patients with positive test result (n: number of patients tested).
13 Three localized stage operable patients (IB, IIB, IIIA) did not have a recurrence and did not receive EGFR-TKI therapy.
14 Five functionally inoperable localized stage patients (IB (3), IIIA, IIIB) received palliative EGFR-TKI therapy.
15 One localized stage operable patient (IIIA) did not have a recurrence and did not receive EGFR-TKI therapy. Four stage IV patients did not receive EGFR-TKI therapy because of poor performance state.
ALK/ROS1/BRAF: 111 patients (97% EGFR negative) were tested for an ALK translocation with 8 positive results (7%). Five of 56 men (8.9%), and 3 of 54 women (5.6%) had a positive ALK-FISH test. In line with the literature [50], patients with an ALK-translocation tended to be younger than the ALK-negative patients (60.7 vs. 65.7 years, p=0.17). In keeping with the concept of mutual exclusiveness of classic mutated driver genes, none of the four EGFR-positive patients who also underwent ALK-testing had an ALK-translocated tumor [51]. Among 35 patients (all EGFR- and ALK-negative) tested for ROS1 translocation, none was detected. Among 39 patients tested for BRAF mutations, the classic V600E mutation was detected in three patients (8%). All of the three BRAF-positive patients were women (n=16, 19% positive), whereas none of 22 men tested had a BRAF mutation.
Oncogenic driver mutations: OS by stage and mutation
The unselected driver-mutation positive population had a significantly longer OS of 33.6 months compared to 18.9 months in driver-mutation negative patients (Hazard ratio [HR] 0.60, CI 0.45 - 0.86, p=0.0045 [Figure 2A]). The case-control analysis confirmed a significantly superior OS in the driver-mutation positive population of 39.6 months compared to 19.4 months in driver-mutation negative patients (HR 0.51, CI 0.29 - 0.79, p=0.021 [Figure 2B]). Case-control analysis by stage revealed no difference in OS in stage I-III patients but a highly significant benefit in OS in the stage IV driver-positive population (HR 0.39, CI 0.18 - 0.61, p=0.0015 [Figure 2C, 2D]). In this population, 5-year survival of driver-positive patients was 34.3% compared to 3.9% of driver-negative patients. Median OS of the case-control subpopulations compared to the corresponding driver-negative controls was 39 vs. 20 months for EGFR-positive patients (HR 0.55, CI 0.30 – 0.92, p=0.016, n=37), 48 vs. 15 months for ALK-positive patients (HR 0.39, CI 0.09 - 1.21, p=0.11, n=7), and 37 vs. 18 months for BRAF-positive patients (HR 0.33, CI 0.014 – 1.30, p=0.166, n=3) (Figure 3A-3C).
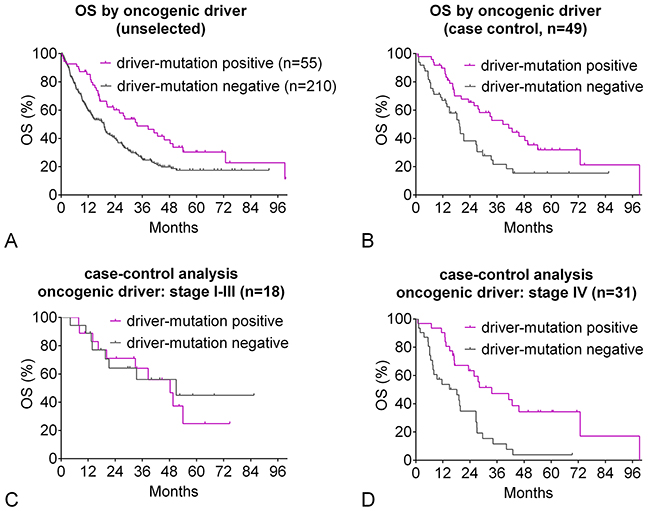
Figure 2: Oncogenic-driver mutation: overall survival. (A) Unselected patients: Kaplan-Meier curves for OS of driver-mutation positive patients compared to patients with no driver mutation detected. Clinical characteristics are given in Table 1. (B-D) Case-control analysis: Patients were matched for gender, clinical stage, performance status, smoking status, and age. Clinical characteristics are given in Table 1. (B) Kaplan-Meier curves for OS of driver-mutation positive patients compared to patients with no driver mutation detected. (C) Kaplan-Meier curves for OS of driver-mutation positive patients stage I-III compared to patients with no driver mutation detected. (D) Kaplan-Meier curves for OS of driver-mutation positive patients stage IV compared to patients with no driver mutation detected.
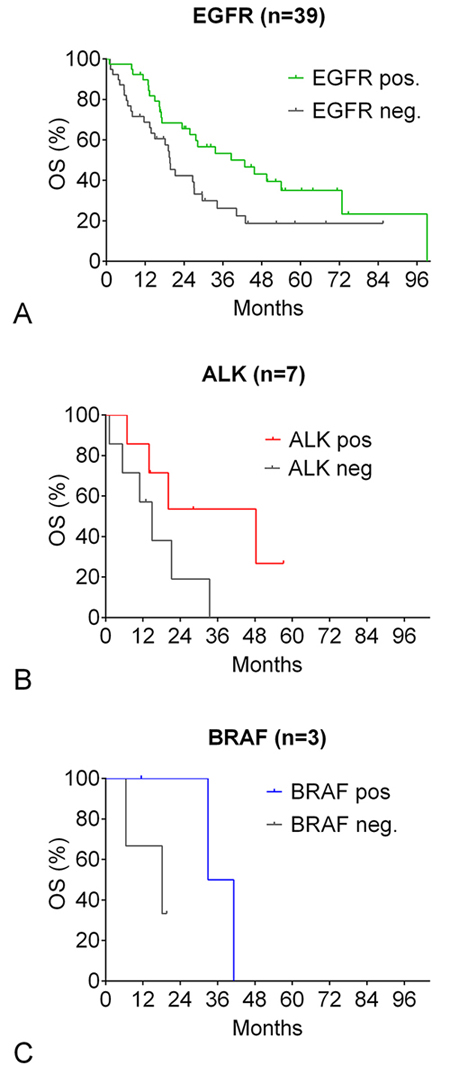
Figure 3: Oncogenic-driver mutation: overall survival by specific mutation. (A-C) Kaplan-Meier curves for OS of driver-mutation positive patients compared to patients with no driver mutation detected (case-control analysis). Patients were matched for gender, clinical stage, performance status, smoking status, and age. (A) EGFR-positive patients. (B) ALK-positive patients. (C) BRAF-positive patients.
Oncogenic driver mutations: treatment
Forty-seven of 55 patients with a sensitizing driver mutation received targeted therapy. Their treatment course is shown in the swimmer plot (Figure 4). Eight driver-positive patients did not receive targeted therapy either because they had localized disease and received curative treatment without recurrence (n=4) or because of poor performance state (n=4). The swimmer plot shows that in line with the outlined treatment principles, most patients received both targeted therapy and chemotherapy. The patient surviving longest (99.2 months) was a male patient with stage IV disease at diagnosis and a complex EGFR exon18 mutation (E709A and G719S). Because of the small numbers of ALK- and BRAF-positive patients, the survival analysis focuses on EGFR-positive patients.
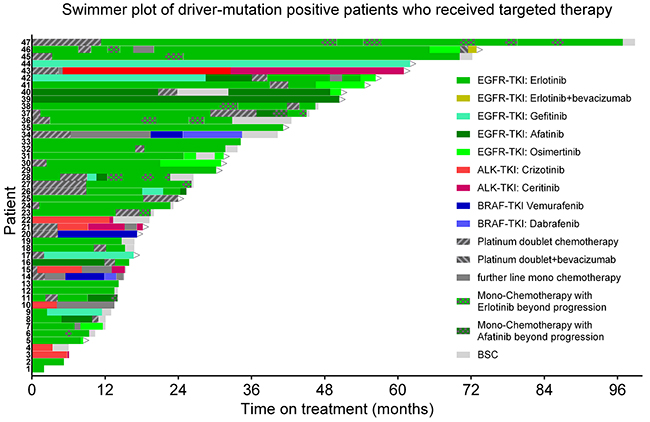
Figure 4: Oncogenic driver mutation-positive patients: treatment course. Swimmer plot showing the sequence of treatment lines in patients who received at least one line of targeted therapy. Bars start from begin of palliative treatment. Arrows signify ongoing therapy. Green: EGFR TKIs. Red: ALK TKIs. Blue: BRAF TKIs. Dark gray: Chemotherapy.
Thirty-seven of the 44 EGFR-positive patients received EGFR-TKI therapy (Figure 4, Table 3). PFS of unselected EGFR-positive patients on first or second generation EGFR-TKI (gefitinib, erlotinib, or afatinib) was 16.9 months with no difference between 1st line TKI therapy (16.9 months) and 2nd line therapy (18.5 months). The total time on TKI therapy was longer (26.2 months), reflecting EGFR-TKI therapy beyond progression. OS of TKI-treated EGFR-positive patients was 38.6 months.
EGFR-mutation: OS by subpopulation
Case-control analysis of subpopulations shows that the OS advantage of EGFR-positive patients was independent of type of EGFR-mutation, gender and age (Forest plot Figure 5). Comparing the different EGFR mutations, there was a trend in favor of exon 19 mutations (HR 0.49) compared to exon 21 mutations (HR 0.61). The few patients with exon 18 mutations had a very good survival compared to controls (HR 0.46). Similarly, there were minor trends in favor of female patients and older patients. With respect to stage, an improved OS was seen in metastasized disease, but not in localized disease. In the EGFR case-control population with stage I-III (n=13), 11 patients were resected in both groups. Despite adequate adjuvant therapy, the recurrence rate after resection was higher in EGFR-positive patients than in matched controls (7/11 [64%] vs. 5/11 [45%]). All EGFR-positive case-control patients initially diagnosed at stage I-III who had a recurrence received EGFR-TKI therapy. None of the comparisons between subpopulations reached statistical significance.
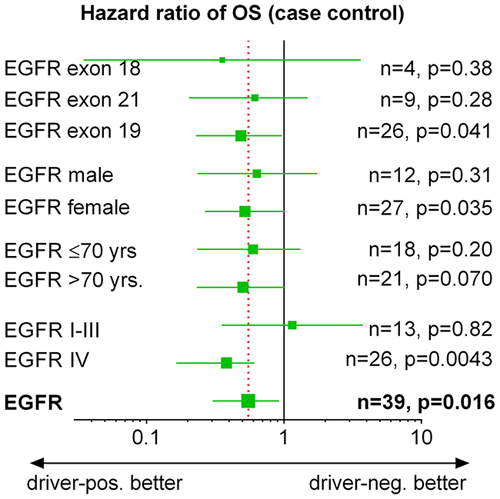
Figure 5: EGFR-positive patients: subgroup analysis of overall survival. Forrest plot showing HR and CI of subgroups of the case-control population in Figure 3A. I-III: UICC stage I-III, IV: UICC stage IV. p-values are given for comparison with matched EGFR-negative controls.
EGFR-mutation: OS by TKI-treatment
A case-control analysis of EGFR-TKI treated EGFR-positive patients compared to negative patients is given in Figure 6. OS of EGFR-positive patients treated with EGFR-TKI either 1st or 2nd line was 38.6 months compared to 19.4 months of EGFR-negative controls (HR 0.47, CI 0.23-0.80, p=0.010, Figure 6A). 5-year survival was 31.9% compared to 10.9% of EGFR-negative controls. The survival benefit was more pronounced for patients treated with EGFR-TKI as 2nd-therapy (HR 0.39, CI 0.10-0.84, p=0.031, Figure 6D) than for patients treated with EGFR-TKI 1st line (HR 0.56, CI 0.24-1.19, p=0.13, Figure 6C). In the few EGFR-positive patients not treated with EGFR-TKI, there was no difference in the OS compared to EGFR-negative controls (HR 0.80, CI 0.14-4.66, Figure 6B).
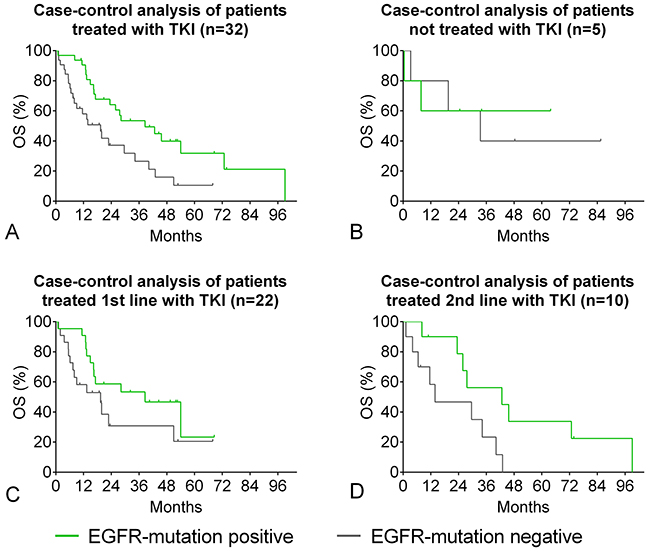
Figure 6: EGFR-positive patients: overall survival by TKI-therapy. Case-control analysis of EGFR-positive and negative patients matched for gender, clinical stage, performance status, smoking status, and age. For patient characteristics and type of EGFR mutation cp. Table 3. (A) EGFR-mutation positive patients who received EGFR-TKI therapy. (B) EGFR-positive patients who did not receive EGFR-TKI therapy. (C) EGFR-positive patients who received 1st line EGFR-TKI therapy. (D) EGFR-positive patients who received 2nd line EGFR-TKI therapy.
EGFR-positive patients: resistance to TKI-treatment
Of eleven patients with acquired resistance to 1st/2nd generation EGFR-TKI therapy, ten had an accessible progressive lesion and were re-biopsied. In the remaining case, liquid biopsy was used. In eight patients (73%), a T790M-resistance mutation was detected. Seven of 8 patients with del exon 19 mutation and one of three patients with exon 18 mutation had the T790M resistance mutation. In one patient, the initial re-biopsy was negative for T790M. However, a second re-biopsy taken after chemotherapy followed by erlotinib beyond progression revealed a T790M-mutant clone. In a patient with an activating EGFR-exon 18 mutation (c.2155G>T; p.G719C), NGS at progression on erlotinib revealed three mutations: the activating exon-18 mutation, a new T790M mutation, and a V600E mutation of the BRAF gene which had been undetectable by pyrosequencing in the initial biopsy. The patient responded to the third generation EGFR-TKI osimertinib and did not receive targeted therapy against the BRAF mutation. Another patient with extensively metastasized del exon 19-positive AC was treated 1st-line with erlotinib with partial remission including response of brain metastases. At progression (including progressive brain metastases and a new liver metastasis) after 7 months on erlotinib, a re-biopsy revealed a T790M resistance mutation. Whilst awaiting the result of molecular testing, the patient received one cycle of carboplatin and pemetrexed and whole-brain irradiation. After report of the T790M mutation, therapy with osimertinib was started resulting in partial remission. After four months on osimertinib, the liver metastasis was stable but primary tumor and mediastinal lymphadenopathy were rapidly progressive. Re-biopsy revealed small-cell lung cancer as the underlying cause (Figure 7). Molecular workup using NGS confirmed the continued presence of the initial EGFR exon 19 deletion in the SCLC biopsy with high allele frequency of 92%. However, the T790M TKI resistance mutation had become undetectable. Additionally, the tumor now carried a highly penetrant TP53 inactivating mutation (p.R248W; 92% allele frequency) which represents a common genetic variant in small-cell lung cancer [52]. One patient with adenosquamous carcinoma and a low level EGFR exon 18 G719C mutation (2%) responded to first-line erlotinib with stable disease for 18 months. At progression of the primary tumor, a re-biopsy revealed squamous-cell carcinoma. The EGFR mutation and the AC component were not detectable any more.
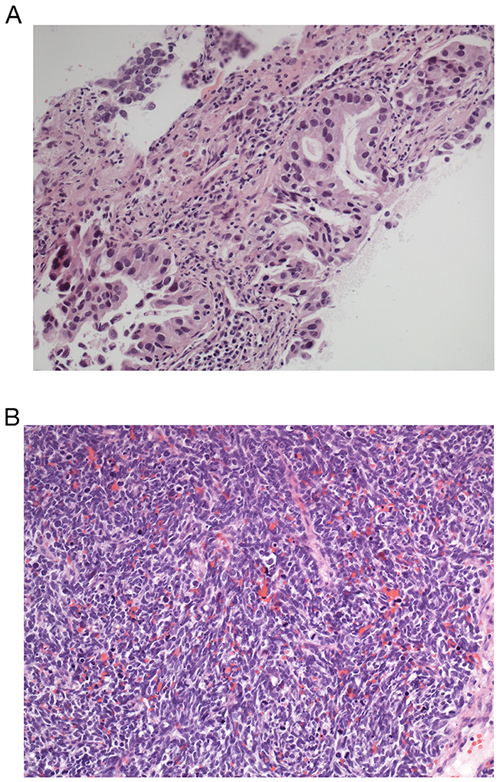
Figure 7: HE stains of endobronchial biopsies of patient 7 (Figure 4). (A) EGFR-positive adenocarcinoma. (B) Transformation into small-cell lung cancer. Magnification 400 fold.
All patients with a T790M mutation were treated with osimertinib (n=8). There were six partial remissions and one stable disease on osimertinib, one patient had not been assessed at data bank lock. Two patients progressed after 4 and 5 months on osimertinib. After a median follow-up of 5.5 months (0.5-9.2 months), median PFS and OS have not been reached.
DISCUSSION
The increased proportion of never-smokers and women among the EGFR-tested NSCLC population underlines the usefulness clinical selection criteria (i. e. predictors of the presence of a sensitizing EGFR mutation) leading to an enrichment of positive cases [50, 53]. Hence, the prevalence of oncogenic driver mutations in our study was higher than expected for a Caucasian patient population [33, 54, 55, 56]. For ALK and BRAF, further enrichment can be achieved by exclusion of patients tested already positive for EGFR and, in case of BRAF, for ALK. Our data are in line with results from the Lung Cancer Mutation Consortium [30] who found an activating EGFR mutation in 17%, an ALK translocation in 8% and a BRAF mutation in 2% in a similarly enriched predominantly Caucasian population with a high proportion of females (60%) and never-smokers (34%). The finding that about 8% of EGFR mutations were non-activating point mutations in exon 19 and 21 of the EGFR gene or activating EFGR mutations not conferring EGFR-TKI sensitivity underlines the necessity to check each mutation for its clinical relevance before starting EGFR-TKI treatment.
The patient selection for EGFR-mutation testing resulted in a population with good prognostic parameters: The stage IV AC population tested at least for EGFR mutation status (n=165) had a median OS of 19.8 months compared to only 9.8 months in unselected stage IV AC patients. This is not explained by differences in age (tested population: 67.2, unselected population: 67.7). However, performance status of the tested stage IV population was better than that of the unselected population (ECOG 0: 22% vs. 17%, ECOG 1: 56% vs. 52%, ECOG 2: 18% vs. 22%). Also the proportion of never-smokers or ex-smokers (72% vs. 63%) was higher among the tested population. Finally, due to enrichment, the proportion of driver-positive patients is expected to be higher in the tested population. Good performance state, non-smoker status, and presence of a driver mutation are associated with an improved prognosis and account for the improved survival of the EGFR-tested population.
Both in the unselected and in the case-control population, driver-positive patients had a longer OS than driver-negative patients with a HR of about 0.60. The survival advantage was confined to stage IV patients who are most likely to receive targeted therapy. An advantage in OS was seen EGFR-positive patients as well as in ALK- and BRAF-positive patients. This emphasizes the need to test all patients with advanced NSCLC and AC histology for drugable driver mutations. In the near future, this will be facilitated by increased availability of multiplex-testing in routine clinical practice. These techniques using next-generation sequencing test with higher sensitivity than previous methods that were based on e. g. Sanger sequencing or FISH and work particularly well with small biopsies and low tumor cellularity [46, 57, 58]. Moreover, they can also be applied for testing of liquid biopsies.
The subgroup analysis of the EGFR case-control population revealed an improved OS irrespective of the type of EGFR mutation, gender or age. In line with previous reports, EGFR-positive patients with exon 19 mutations had a trend to longer OS (39 months) than those with an exon 21 mutation (34 months) [5, 20]. The five patients with rare exon 18 mutations showed an even better survival, but due to small numbers, no final conclusions can be drawn [59]. Time on TKI-treatment included a median of 14 months on TKI beyond progression which prolongs disease control [60] and may, by preventing early switch to chemotherapy, positively influence patients’ quality of life [31].
In localized stages, EGFR-positive patients did not have an advantage in OS, although EGFR-positive patients received EGFR-TKI at recurrence. A potential benefit of targeted therapy may have been balanced by the higher proportion of recurrences after definitive therapy in the EGFR-positive group. From our data, we cannot decide whether this is a chance finding or reflects a higher risk of recurrence in driver-positive NSCLC. However, although the finding of a higher recurrence rate in EGFR-positive stage I-III patients is based on a small number of patients, it is tempting to speculate that cytotoxic (adjuvant or neo-adjuvant) chemotherapy might be less effective in EGFR-positive tumors in a curative-intent setting.
The median OS of 38.6 months found in our EGFR-positive population on EGFR-TKI is longer than that reported in phase IIb/III studies (19-28 months) [5, 21, 35]. Newer retrospective data show a slightly longer median OS of up to 31 months [25, 26]. TKI-treatment beyond progression which may be used more frequently in routine clinical practice than in a more rigid clinical study setting may have contributed to the increased survival [47, 48]. Moreover, in our study, the control patients (mainly stage IV NSCLC) showed a relatively long survival as well indicating good prognostic parameters in the EGFR-TKI-treated case-control population. The HR for OS of EGFR-positive patients compared to EGFR-negative controls was 0.47 if the EGFR-positive patients received EGFR-TKI therapy compared to 0.80 for those who did not receive EGFR-TKI-therapy. In accordance with the literature, this points to a contribution of EGFR-TKI therapy to the improved OS of EGFR-positive patients.
Our observation that patients receiving EGFR-TKI as 2nd line therapy tend to have a longer OS than patients on 1st line EGFR-TKI is in line with the French registry data but contrasts with the Chinese retrospective experience [32, 33]. However, neither study reports the clinical reason why some patients received 1st-line chemotherapy and other 1st line chemotherapy possibly resulting in systematic imbalances between the characteristics of patients treated with EGFR-TKI 1st or 2nd line. This question can only be answered by a randomized clinical trial systematically comparing the treatment sequence of EGFR-TKI and chemotherapy. With current evidence of an OS advantage for patients sequentially receiving both EGFR-TKI and chemotherapy compared to either TKI or chemotherapy alone [21], it is important in clinical practice to use both EGFR-TKI and chemotherapy.
Our early experience with re-biopsy at progression on EGFR-TKI shows that re-biopsy is feasible in clinical practice and affects further treatment with detection of a treatable T790M-resistance mutation in a high proportion of cases. In the near future, increased availability of liquid biopsy and NGS will allow all EGFR-mutation positive patients who progress on EGFR-TKI to be tested for resistance mutations. Two other possible mechanisms of resistance were detected in our population: transformation into small-cell lung cancer, and a BRAF mutation. The clinical relevance of the BRAF mutation is unknown since it was detected in addition to a T790M mutation, and the patient so far did not receive targeted treatment against BRAF. The knowledge both on drugable activating mutations and on resistance mutations - not only in EGFR-positive NSCLC [36], but also in ALK-rearranged NSCLC [61] - is rapidly increasing. It is therefore of paramount importance for first-line and further-line therapies to perform a complete mutation screening in each eligible patient. In this context, traditional technology and sequential testing are of limited value since they require large tumor biopsies and possibly repeat biopsies in case of low tumor cellularity. The availability of new sensitive multiplex detection methods will make precision-medicine approaches available to most eligible patients and improve their quality of life and prognosis. Liquid biopsies will complement these approaches further. Moreover, the case showing transformation into SCLC strongly argues for concomitant histologic evaluation. Although some genetic events have been described recently, genetic analysis alone will most likely miss this resistance mechanism that has direct therapeutic implications. [62]
Limitations: Data are retrospective and non-randomized with a limited sample size. However, due to the large control group, exact matching of most driver mutation-positive patients was possible demonstrating significant clinical results. Only testing for EGFR was complete, thus the control group may include some ALK-, BRAF- or ROS1-positive patients. Moreover, Sanger sequencing may have missed some activating mutations which might have been found with more sensitive techniques (e. g. NGS) evolving during the study period.
Strengths: Our study provides data on diagnostic strategies, treatment patterns and OS in a current typical predominantly Caucasian lung cancer population with long-term follow-up data of up to 100 months. Since our study is a case-control analysis, we provide data from routine clinical practice on the effect of driver mutations and treatment on OS beyond anecdotal evidence of single positive cases.
In conclusion, testing for driver mutations is feasible in routine clinical practice, profoundly affects treatment and identifies patients with a good prognosis. Driver mutation-positive patients on TKI therapy in clinical routine have an OS at least as favorable as that reported in clinical studies. Our study supports current data that improved OS can be attributed to targeted therapies, and shows controlled long-term survival rates for driver-positive NSCLC that well exceed reported trial data.
MATERIALS AND METHODS
Patients
We recorded results of genetic testing (EGFR, ALK, ROS1, BRAF), treatment, and survival in patients diagnosed with NSCLC at our institution (lung cancer center certified by the German Cancer Society [DKG]) from January 2006 until December 2015. The databank was locked on December 31st, 2016. Overall survival (OS) was analyzed retrospectively in unselected patients and in case-control analyses of pairs of driver-positive and driver-negative patients individually matched for gender, smoking status, performance state, stage, and age. To avoid bias, matching was performed using only these parameters (i.e. blinded to patient number, treatment, and survival). Staging was performed according to UICC 7th edition [63]. Stage matching included substage (A vs. B for stage I-III) and M-status (M1a vs. M1b for stage IV). Smoking status was self-reported. The study was approved by the local ethics committee (Landesärztekammer Baden-Württemberg F-2017-004).
Molecular pathology
Pathological diagnosis and grading were carried out in accordance with the respective relevant WHO-guidelines [64, 65, 66]. In accordance with ESMO guidelines [67], molecular testing was performed in patients with predominant AC histology and a palliative situation (no surgical curative option, no definitive radio-chemotherapy), if TKI-therapy was considered a treatment option. Furthermore, patients with NSCLC of any histological subtype and stage were tested when our center participated in the REASON study [68] which allowed testing of patients with NSCLC irrespective of stage or histology. All molecular tests were performed by two quality controlled centers of pathology (Institute of Pathology Esslingen (certified by the national accreditation body of the Federal Republic of Germany (DAKKS), and Institute of Pathology Heidelberg, Heidelberg (accredited by the national accreditation body of the Federal Republic of Germany (DAKKS)).
EGFR-mutation testing has been performed since June 2009. EGFR testing was done from tumor biopsies with at least 20% tumor-cell content using micro-dissection of tumor cells, PCR, and Sanger sequencing of exons 18, 19, and 21 of the EGFR gene. Since January 2015, also exon 20 has been tested. With the availability of the third-generation EGFR-TKI osimertinib, patients with EGFR-TKI sensitive NSCLC and acquired resistance to 1st/2nd generation EGFR-TKI therapy with an accessible progressive lesion were re-biopsied for molecular pathological workup with a focus on detection of the T790M-resistance mutation in exon 20. In one case, liquid biopsy was used for molecular pathological workup [69].
Testing for ALK translocation status became available in October 2012. ALK translocation testing was performed using FISH. On an individual patient basis, testing for ROS1 translocation (FISH) and BRAF mutation (pyrosequencing) was performed. Following the concept of mutual exclusiveness of oncogenic driver mutations, tests for ALK, ROS1, and BRAF were only performed in AC with a negative EGFR-test result. Since 2016, next generation sequencing (NGS) testing both for mutations (EGFR incl. T790M, BRAF) and translocations (ALK, ROS1) has been used for some patients [70].
Principles of TKI treatment in the study population
For EGFR-, ALK-, or BRAF-positive patients, the following principles based on experience with patients with EGFR-positive NSCLC were applied:
• Use of TKI beyond radiological progression until clinically relevant progression [29, 71, 72, 73].
• Dose adjustments to avoid intolerable side effects [74].
• Sequential use of different generation TKIs, e. g. 3rd generation EGFR-TKI osimertinib (after demonstration of a T790M resistance mutation in a re-biopsy) following 1st or 2nd generation EGFR-TKIs gefitinib, erlotinib, or afatinib for EGFR-positive patients, or 2nd generation ALK-TKI ceritinib following 1st generation ALK-TKI crizotinib for ALK positive patients.
• Addition of local therapy, in particular radiotherapy, as clinically needed.
• Use of systemic chemotherapy in case of clinically relevant systemic progression if switch to a higher generation TKI was not possible or local therapy was insufficient to control disease.
○ If platinum-doublet chemotherapy was used, EGFR-TKI was paused following the concept of “TKI drug holiday” by Becker and colleagues [47].
○ During most of the study period, single-agent chemotherapy was combined with EGFR-TKI beyond progression to prevent disease flare described after discontinuation of EGFR-TKI [48, 75].
Statistical methods
Kaplan-Meier plots were generated using GraphPad Prism6. Hazard ratios and significances were calculated using the log-rank test (Mantel-Cox). For age comparisons, an unpaired t-test was used (GraphPad Prism6).
CONFLICTS OF INTEREST
None of the authors has declared a conflict of interest.
FUNDING
There was no external funding.
REFERENCES
1. Paez JG, Jänne PA, Lee JC, Tracy S, Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, Naoki K, Sasaki H, Fujii Y, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304:1497-500. https://doi.org/10.1126/science.1099314.
2. Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, Louis DN, Christiani DC, Settleman J, Haber DA. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129-39. https://doi.org/10.1056/NEJMoa040938.
3. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, Nishiwaki Y, Ohe Y, Yang JJ, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947-57. https://doi.org/10.1056/NEJMoa0810699.
4. Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I, Fujita Y, Okinaga S, Hirano H, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380-8. https://doi.org/10.1056/NEJMoa0909530.
5. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, Porta R, Cobo M, Garrido P, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomized phase 3 trial. Lancet Oncol. 2012;13:239-46. https://doi.org/10.1016/S1470-2045 (11)70393-X.
6. Wu YL, Zhou C, Hu CP, Feng J, Lu S, Huang Y, Li W, Hou M, Shi JH, Lee KY, Xu CR, Massey D, Kim M, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomized phase 3 trial. Lancet Oncol. 2014;15:213-22. https://doi.org/10.1016/S1470-2045 (13)70604-1.
7. Shaw AT, Kim DW, Nakagawa K, Seto T, Crinó L, Ahn MJ, De Pas T, Besse B, Solomon BJ, Blackhall F, Wu YL, Thomas M, O’Byrne KJ, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013;368:2385-94. https://doi.org/10.1056/NEJMoa1214886.
8. Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T, Felip E, Cappuzzo F, Paolini J, Usari T, Iyer S, Reisman A, Wilner KD, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371:2167-77. https://doi.org/10.1056/NEJMoa1408440.
9. Shaw AT, Kim DW, Mehra R, Tan DS, Felip E, Chow LQ, Camidge DR, Vansteenkiste J, Sharma S, De Pas T, Riely GJ, Solomon BJ, Wolf J, et al. Ceritinib in ALK-rearranged non-small-cell lung cancer. N Engl J Med. 2014;370:1189-97. https://doi.org/10.1056/NEJMoa1311107.
10. Shaw AT, Gandhi L, Gadgeel S, Riely GJ, Cetnar J, West H, Camidge DR, Socinski MA, Chiappori A, Mekhail T, Chao BH, Borghaei H, Gold KA, et al. Alectinib in ALK-positive, crizotinib-resistant, non-small-cell lung cancer: a single-group, multicentre, phase 2 trial. Lancet Oncol. 2016;17:234-42. https://doi.org/10.1016/S1470-2045 (15)00488-X.
11. Shaw AT, Ou SH, Bang YJ, Camidge DR, Solomon BJ, Salgia R, Riely GJ, Varella-Garcia M, Shapiro GI, Costa DB, Doebele RC, Le LP, Zheng Z, et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N Engl J Med. 2014;371:1963-71. https://doi.org/10.1056/NEJMoa1406766.
12. Subbiah V, Hong DS, Meric-Bernstam F. Clinical activity of ceritinib in ROS1-rearranged non-small cell lung cancer: bench to bedside report. Proc Natl Acad Sci U S A. 2016;113:E1419-20. https://doi.org/10.1073/pnas.1522052113.
13. Planchard D, Kim TM, Mazieres J, Quoix E, Riely G, Barlesi F, Souquet PJ, Smit EF, Groen HJ, Kelly RJ, Cho BC, Socinski MA, Pandite L, et al. Dabrafenib in patients with BRAF (V600E)-positive advanced non-small-cell lung cancer: a single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016;17:642-50. https://doi.org/10.1016/S1470-2045 (16)00077-2.
14. Hyman DM, Puzanov I, Subbiah V, Faris JE, Chau I, Blay JY, Wolf J, Raje NS, Diamond EL, Hollebecque A, Gervais R, Elez-Fernandez ME, Italiano A, et al. Vemurafenib in multiple nonmelanoma cancers with BRAF V600 mutations. N Engl J Med. 2015;373:726-36. https://doi.org/10.1056/NEJMoa1502309.
15. Planchard D, Besse B, Groen HJ, Souquet PJ, Quoix E, Baik CS, Barlesi F, Kim TM, Mazieres J, Novello S, Rigas JR, Upalawanna A, D’Amelio AM Jr, et al. Dabrafenib plus trametinib in patients with previously treated BRAF (V600E)-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Lancet Oncol. 2016;17:984-93. https://doi.org/10.1016/S1470-2045 (16)30146-2.
16. Liu YT, Hao XZ, Li JL, Hu XS, Wang Y, Wang ZP, Wang HY, Wang B, Han XH, Zhang XR, Shi YK. Survival of patients with advanced lung AC before and after approved use of gefitinib in China. Thorac Cancer. 2015;6:636-42. https://doi.org/10.1111/1759-7714.12267.
17. Scheffler M, Schultheis A, Teixido C, Michels S, Morales-Espinosa D, Viteri S, Hartmann W, Merkelbach-Bruse S, Fischer R, Schildhaus HU, Fassunke J, Sebastian M, Serke M, et al. ROS1 rearrangements in lung adenocarcinoma: prognostic impact, therapeutic options and genetic variability. Oncotarget. 2015 30;6:10577-85. https://doi.org/10.18632/oncotarget.3387.
18. Takeda M, Okamoto I, Sakai K, Kawakami H, Nishio K, Nakagawa K. Clinical outcome for EML4-ALK-positive patients with advanced non-small-cell lung cancer treated with first-line platinum-based chemotherapy. Ann Oncol. 2012;23:2931-6. https://doi.org/10.1093/annonc/mds124.
19. Tissot C, Couraud S, Tanguy R, Bringuier PP, Girard N, Souquet PJ. Clinical characteristics and outcome of patients with lung cancer harboring BRAF mutations. Lung Cancer. 2016;91:23-8. https://doi.org/10.1016/j.lungcan.2015.11.006.
20. Yang JC, Wu YL, Schuler M, Sebastian M, Popat S, Yamamoto N, Zhou C, Hu CP, O’Byrne K, Feng J, Lu S, Huang Y, Geater SL, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomized, phase 3 trials. Lancet Oncol. 2015;16:141-51. https://doi.org/10.1016/S1470-2045 (14)71173-8.
21. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, Zhang S, Wang J, Zhou S, Ren S, Lu S, Zhang L, Hu C, et al. Final overall survival results from a randomized, phase III study of erlotinib versus chemotherapy as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer (OPTIMAL, CTONG-0802). Ann Oncol. 2015;26:1877-83. https://doi.org/10.1093/annonc/mdv276.
22. Greenhalgh J, Dwan K, Boland A, Bates V, Vecchio F, Dundar Y, Jain P, Green JA. First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer. Cochrane Database Syst Rev. 2016:CD010383. https://doi.org/10.1002/14651858.CD010383.pub2.
23. Guetz GD, Landre T, Uzzan B, Chouahnia K, Nicolas P, Morere JF. Is there a survival benefit of first-line epidermal growth factor receptor tyrosine-kinase inhibitor monotherapy versus chemotherapy in patients with advanced non-small-cell lung cancer? A meta-analysis. Target Oncol. 2016;11:41-7. https://doi.org/10.1007/s11523-015-0373-x.
24. Del Rivero J, Enewold L, Thomas A. Metastatic lung cancer in the age of targeted therapy: improving long-term survival. Transl Lung Cancer Res. 2016;5:727-30. https://doi.org/10.21037/tlcr.2016.11.08.
25. Inoue A, Yoshida K, Morita S, Imamura F, Seto T, Okamoto I, Nakagawa K, Yamamoto N, Muto S, Fukuoka M. Characteristics and overall survival of EGFR mutation-positive non-small cell lung cancer treated with EGFR tyrosine kinase inhibitors: a retrospective analysis for 1660 Japanese patients. Jpn J Clin Oncol. 2016;46:462-7. https://doi.org/10.1093/jjco/hyw014.
26. Lin JJ, Cardarella S, Lydon CA, Dahlberg SE, Jackman DM, Jänne PA, Johnson BE. Five-year survival in EGFR-mutant metastatic lung adenocarcinoma treated with EGFR-TKIs. J Thorac Oncol. 2016;11:556-65. https://doi.org/10.1016/j.jtho.2015.12.103.
27. Zhao D, Chen X, Qin N, Su D, Zhou L, Zhang Q, Li X, Zhang X, Jin M, Wang J. The prognostic role of EGFR-TKIs for patients with advanced non-small cell lung cancer. Sci Rep. 2017;7:40374. https://doi.org/10.1038/srep40374.
28. Takano T, Fukui T, Ohe Y, Tsuta K, Yamamoto S, Nokihara H, Yamamoto N, Sekine I, Kunitoh H, Furuta K, Tamura T. EGFR mutations predict survival benefit from gefitinib in patients with advanced lung adenocarcinoma: a historical comparison of patients treated before and after gefitinib approval in Japan. J Clin Oncol. 2008;26:5589-95. https://doi.org/10.1200/JCO.2008.16.7254.
29. Ohashi K, Maruvka YE, Michor F, Pao W. Epidermal growth factor receptor tyrosine kinase inhibitor-resistant disease. J Clin Oncol. 2013;31:1070-80. https://doi.org/10.1200/JCO.2012.43.3912.
30. Kris MG, Johnson BE, Berry LD, Kwiatkowski DJ, Iafrate AJ, Wistuba II, Varella-Garcia M, Franklin WA, Aronson SL, Su PF, Shyr Y, Camidge DR, Sequist LV, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311:1998-2006. https://doi.org/10.1001/jama.2014.3741.
31. Mok T, Yang JJ, Lam KJ. Treating patients with EGFR-sensitizing mutations: first line or second line - is there a difference? J Clin Oncol. 2013;31:1081-8. https://doi.org/10.1200/JCO.2012.43.0652.
32. Xu J, Zhang X, Yang H, Ding G, Jin B, Lou Y, Zhang Y, Wang H, Han B. Comparison of outcomes of tyrosine kinase inhibitor in first- or second-line therapy for advanced non-small-cell lung cancer patients with sensitive EGFR mutations. Oncotarget. 2016;7:68442-8. https://doi.org/10.18632/oncotarget.12035.
33. Leduc C, Blons H, Besse B, Merlio JP, Debieuvre D, Lemoine A, Monnet I, Pouessel D, Bringuier M, Poudenx PP, Rouquette I, Vaylet F, Morin F, et al. Clinical and biological characteristics of non-small cell lung cancer (NSCLC) harbouring EGFR mutation: Results of the nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Ann Oncol. 2016;27:12020.
34. Zeng Z, Yan HH, Zhang XC, Zhong WZ, He YY, Guan JL, Niu FY, Xie Z, Huang YS, Xu CR, Dong S, Wu YL. Reduced chemotherapy sensitivity in EGFR-mutant lung cancer patient with frontline EGFR tyrosine kinase inhibitor. Lung Cancer. 2014;86:219-24. https://doi.org/10.1016/j.lungcan.2014.09.008.
35. Paz-Ares L, Tan EH, O’Byrne K, Zhang L, Hirsh V, Boyer M, Yang JC, Mok T, Lee KH, Lu S, Shi Y, Lee DH, Laskin J, et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: overall survival data from the phase IIb LUX-Lung 7 trial. Ann Oncol. 2017;28:270-7. https://doi.org/10.1093/annonc/mdw611.
36. Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, Kris MG, Miller VA, Ladanyi M, Riely GJ. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19:2240-7. https://doi.org/10.1158/1078-0432.CCR-12-2246.
37. Mok TS, Wu YL, Ahn MJ, Garassino MC, Kim HR, Ramalingam SS, Shepherd FA, He Y, Akamatsu H, Theelen WS, Lee CK, Sebastian M, Templeton A, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. 2017;376:629-40. https://doi.org/10.1056/NEJMoa1612674.
38. Sun Y, Ren Y, Fang Z, Li C, Fang R, Gao B, Han X, Tian W, Pao W, Chen H, Ji H. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J Clin Oncol. 2010;28:4616-20. https://doi.org/10.1200/JCO.2010.29.6038.
39. Sequist LV, Bell DW, Lynch TJ, Haber DA. Molecular predictors of response to epidermal growth factor receptor antagonists in non-small-cell lung cancer. J Clin Oncol. 2007;25:587-95. https://doi.org/10.1200/JCO.2006.07.3585.
40. Sharma SV, Bell DW, Settleman J, Haber DA. Epidermal growth factor receptor mutations in lung cancer. Nat Rev Cancer. 2007;7:169-81. https://doi.org/10.1038/nrc2088.
41. Kobayashi Y, Mitsudomi T. Not all epidermal growth factor receptor mutations in lung cancer are created equal: perspectives for individualized treatment strategy. Cancer Sci. 2016;107:1179-86. https://doi.org/10.1111/cas.12996.
42. Beau-Faller M, Prim N, Ruppert AM, Nanni-Metéllus I, Lacave R, Lacroix L, Escande F, Lizard S, Pretet JL, Rouquette I, de Crémoux P, Solassol J, de Fraipont F, et al. Rare EGFR exon 18 and exon 20 mutations in non-small-cell lung cancer on 10 117 patients: a multicentre observational study by the French ERMETIC-IFCT network. Ann Oncol. 2014;25:126-31. https://doi.org/10.1093/annonc/mdt418.
43. Nakamura H, Kawasaki N, Taguchi M, Kato H. Epidermal growth factor receptor gene mutations in early pulmonary adenocarcinomas. Ann Thorac Cardiovasc Surg. 2007;13:87-92.
44. Tsao MS, Sakurada A, Cutz JC, Zhu CQ, Kamel-Reid S, Squire J, Lorimer I, Zhang T, Liu N, Daneshmand M, Marrano P, da Cunha Santos G, Lagarde A, et al. Erlotinib in lung cancer - molecular and clinical predictors of outcome. N Engl J Med. 2005;353:133-44. https://doi.org/10.1056/NEJMoa050736.
45. Han B, Zhou X, Zhang RX, Zang WF, Chen ZY, Song HD, Wan HY, Zheng CX. Mutations of the epidermal growth factor receptor gene in NSCLC patients. Oncol Lett. 2011;2:1233-7. https://doi.org/10.3892/ol.2011.366.
46. Matsushima S, Ohtsuka K, Ohnishi H, Fujiwara M, Nakamura H, Morii T, Kishino T, Goto H, Watanabe T. V843I, a lung cancer predisposing EGFR mutation, is responsible for resistance to EGFR tyrosine kinase inhibitors. J Thorac Oncol. 2014;9:1377-84. https://doi.org/10.1097/JTO.0000000000000241.
47. Demierre N, Zoete V, Michielin O, Stauffer E, Zimmermann DR, Betticher DC, Peters S. A dramatic lung cancer course in a patient with a rare EGFR germline mutation exon 21 V843I: is EGFR TKI resistance predictable? Lung Cancer. 2013;80:81-4. https://doi.org/10.1016/j.lungcan.2012.11.013.
48. Halvorsen AR, Silwal-Pandit L, Meza-Zepeda LA, Vodak D, Vu P, Sagerup C, Hovig E, Myklebost O, Børresen-Dale AL, Brustugun OT, Helland Å. TP53 mutation spectrum in smokers and never smoking lung cancer patients. Front Genet. 2016;7:85. https://doi.org/10.3389/fgene.2016.00085.
49. Vassella E, Langsch S, Dettmer MS, Schlup C, Neuenschwander M, Frattini M, Gugger M, Schäfer SC. Molecular profiling of lung adenosquamous carcinoma: hybrid or genuine type? Oncotarget. 2015;6:23905-16. https://doi.org/10.18632/oncotarget.4163.
50. Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, Ou SH, Dezube BJ, Jänne PA, Costa DB, Varella-Garcia M, Kim WH, Lynch TJ, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363:1693-703. https://doi.org/10.1056/NEJMoa1006448.
51. Gainor JF, Varghese AM, Ou SH, Kabraji S, Awad MM, Katayama R, Pawlak A, Mino-Kenudson M, Yeap BY, Riely GJ, Iafrate AJ, Arcila ME, Ladanyi M, et al. ALK rearrangements are mutually exclusive with mutations in EGFR or KRAS: an analysis of 1,683 patients with non-small cell lung cancer. Clin Cancer Res. 2013;19:4273-81. https://doi.org/10.1158/1078-0432.CCR-13-0318.
52. George J, Lim JS, Jang SJ, Cun Y, Ozretić L, Kong G, Leenders F, Lu X, Fernández-Cuesta L, Bosco G, Müller C, Dahmen I, Jahchan NS, et al. Comprehensive genomic profiles of small cell lung cancer. Nature. 2015;524:47-53. https://doi.org/10.1038/nature14664.
53. Jänne PA, Johnson BE. Effect of epidermal growth factor receptor tyrosine kinase domain mutations on the outcome of patients with non-small cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors. Clin Cancer Res. 2006;12:4416s-20s. https://doi.org/10.1158/1078-0432.CCR-06-0555.
54. Tapia C, Savic S, Bihl M, Rufle A, Zlobec I, Terracciano L, Bubendorf L. EGFR mutation analysis in non-small-cell lung cancer: experience from routine diagnostics. Pathologe. 2009;30:384-92. https://doi.org/10.1007/s00292-009-1141-4.
55. Esteban E, Majem M, Martinez Aguillo M, Martinez Banaclocha N, Dómine M, Gómez Aldaravi L, Juan O, Cajal R, Gonzalez Arenas MC, Provencio M. Prevalence of EGFR mutations in newly diagnosed locally advanced or metastatic non-small cell lung cancer Spanish patients and its association with histological subtypes and clinical features: the Spanish REASON study. Cancer Epidemiol. 2015;39:291-7. https://doi.org/10.1016/j.canep.2015.02.003.
56. Barlesi F, Mazieres J, Merlio JP, Debieuvre D, Mosser J, Lena H, Ouafik L, Besse B, Rouquette I, Westeel V, Escande F, Monnet I, Lemoine A, et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet. 2016;387:1415-26. https://doi.org/10.1016/S0140-6736 (16)00004-0.
57. Endris V, Penzel R, Warth A, Muckenhuber A, Schirmacher P, Stenzinger A, Weichert W. Molecular diagnostic profiling of lung cancer specimens with a semiconductor-based massive parallel sequencing approach: feasibility, costs, and performance compared with conventional sequencing. J Mol Diagn. 2013;15:765-75. https://doi.org/10.1016/j.jmoldx.2013.06.002.
58. Volckmar AL, Endris V, Bozorgmehr F, Lier C, Porcel C, Kirchner M, Leichsenring J, Penzel R, Thomas M, Schirmacher P, Warth A, Stenzinger A. Next-generation sequencing facilitates detection of the classic E13-A20 EML4-ALK fusion in an ALK-FISH/IHC inconclusive biopsy of a stage IV lung cancer patient: a case report. Diagn Pathol. 2016;11:133. https://doi.org/10.1186/s13000-016-0581-4.
59. Kuiper JL, Hashemi SM, Thunnissen E, Snijders PJ, Grünberg K, Bloemena E, Sie D, Postmus PE, Heideman DA, Smit EF. Non-classic EGFR mutations in a cohort of Dutch EGFR-mutated NSCLC patients and outcomes following EGFR-TKI treatment. Br J Cancer. 2016;115:1504-12. https://doi.org/10.1038/bjc.2016.372.
60. Chen Q, Quan Q, Ding L, Hong X, Zhou N, Liang Y, Wu H. Continuation of epidermal growth factor receptor tyrosine kinase inhibitor treatment prolongs disease control in non-small-cell lung cancers with acquired resistance to EGFR tyrosine kinase inhibitors. Oncotarget. 2015;6:24904-11. https://doi.org/10.18632/oncotarget.4570.
61. Gainor JF, Dardaei L, Yoda S, Friboulet L, Leshchiner I, Katayama R, Dagogo-Jack I, Gadgeel S, Schultz K, Singh M, Chin E, Parks M, Lee D, et al. Molecular mechanisms of resistance to first- and second-generation ALK inhibitors in ALK-rearranged lung cancer. Cancer Discov. 2016;6:1118-33.
62. Oser MG, Niederst MJ, Sequist LV, Engelman JA. Transformation from non-small-cell lung cancer to small-cell lung cancer: molecular drivers and cells of origin. Lancet Oncol. 2015;16:e165-72. https://doi.org/10.1016/S1470-2045 (14)71180-5.
63. Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V, Sobin L; International Association for the Study of Lung Cancer International Staging Committee; Participating Institutions. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706-14. https://doi.org/10.1097/JTO.0b013e31812f3c1a.
64. Travis WD, Brambilla E, Müller-Hermelink HK, Harris CC (Ed.). Pathology and Genetics of Tumors of the Lung, Pleura, Thymus and Heart. WHO/IARC Classification of Tumors, 3rd Edition, Volume 10 (2004).
65. Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG (Ed.). WHO Classification of Tumors of the Lung, Pleura, Thymus and Heart. WHO/IARC Classification of Tumors, 4th Edition, Volume 7 (2015).
66. Petersen I, Warth A. Lung cancer: developments, concepts, and specific aspects of the new WHO classification. J Cancer Res Clin Oncol. 2016;142:895-904. https://doi.org/10.1007/s00432-015-2004-4.
67. Kerr KM, Bubendorf L, Edelman MJ, Marchetti A, Mok T, Novello S, O’Byrne K, Stahel R, Peters S, Felip E; Panel Members. Second ESMO consensus conference on lung cancer: pathology and molecular biomarkers for non-small-cell lung cancer. Ann Oncol. 2014;25:1681-90. https://doi.org/10.1093/annonc/mdu123.
68. Schuette W, Schirmacher P, Eberhardt WE, Fischer JR, von der Schulenburg JM, Mezger J, Schumann C, Serke M, Zaun S, Dietel M, Thomas M. EGFR mutation status and first-line treatment in patients with stage III/IV non-small cell lung cancer in Germany: an observational study. Cancer Epidemiol Biomarkers Prev. 2015;24:1254-61. https://doi.org/10.1158/1055-9965.EPI-14-1149.
69. Rachiglio AM, Esposito Abate R, Sacco A, Pasquale R, Fenizia F, Lambiase M, Morabito A, Montanino A, Rocco G, Romano C, Nappi A, Iaffaioli RV, et al. Limits and potential of targeted sequencing analysis of liquid biopsy in patients with lung and colon carcinoma. Oncotarget. 2016;7:66595-605. https://doi.org/10.18632/oncotarget.10704.
70. Pfarr N, Stenzinger A, Penzel R, Warth A, Dienemann H, Schirmacher P, Weichert W, Endris V. High-throughput diagnostic profiling of clinically actionable gene fusions in lung cancer. Genes Chromosomes Cancer. 2016;55:30-44. https://doi.org/10.1002/gcc.22297.
71. Becker A, Crombag L, Heideman DA, Thunnissen FB, van Wijk AW, Postmus PE, Smit EF. Retreatment with erlotinib: regain of TKI sensitivity following a drug holiday for patients with NSCLC who initially responded to EGFR-TKI treatment. Eur J Cancer. 2011;47:2603-6. https://doi.org/10.1016/j.ejca.2011.06.046.
72. Faehling M, Eckert R, Kamp T, Kuom S, Griese U, Sträter J, Ott G, Spengler W. EGFR-tyrosine kinase inhibitor treatment beyond progression in long-term Caucasian responders to erlotinib in advanced non-small cell lung cancer: a case-control study of overall survival. Lung Cancer. 2013;80:306-12. https://doi.org/10.1016/j.lungcan.2013.02.010.
73. Yap TA, Macklin-Doherty A, Popat S. Continuing EGFR inhibition beyond progression in advanced non-small cell lung cancer. Eur J Cancer. 2016;70:12-21. https://doi.org/10.1016/j.ejca.2016.10.014.
74. Faehling M, Eckert R, Kuom S, Kamp T, Stoiber KM, Schumann C. Benefit of erlotinib in patients with non-small-cell lung cancer is related to smoking status, gender, skin rash and radiological response but not to histology and treatment line. Oncology. 2010;78:249-58. https://doi.org/10.1159/000315731.
75. Chaft JE, Oxnard GR, Sima CS, Kris MG, Miller VA, Riely GJ. Disease flare after tyrosine kinase inhibitor discontinuation in patients with EGFR-mutant lung cancer and acquired resistance to erlotinib or gefitinib: implications for clinical trial design. Clin Cancer Res. 2011;17:6298-303. https://doi.org/10.1158/1078-0432.CCR-11-1468.