
INTRODUCTION
Breast cancer (BC) is one of the most commonly diagnosed cancer among women in most countries, representing a quarter of all cancers diagnosed in women [1]. It is also the primary cause of cancer-related deaths among women [2]. Approximately three-quarters of BC patients are diagnosed at an early stage or are operable [3]. For these patients, it is essential to administer adjuvant chemotherapy to reduce the risk of recurrence [4–5]. Recent studies and meta-analyses have shown that the taxane-based (neo)adjuvant regimen reduce recurrence rates and improve survival in high-risk EBC patients [6–9].
Capecitabine is an oral prodrug of fluorouracil, it is metabolized in the liver and in cancerous tissue after absorption. Capecitabine is converted into 5-fluorouracil (5-FU) by sequential enzyme activity. The final process of capecitabine is converted to 5-FU through the enzymatic activity of thymidine phosphorylase (TP), which is known to be over expressed in tumor cells [10]. Capecitabine has been considered one of the most active drugs available for metastatic BC (MBC), and it has a favorable safety profile that is characterized by minimal alopecia and myelosuppression [11]. Previous phase III metastatic breast cancer trials had demonstrated that patients have a better survival benefit with capecitabine plus docetaxel versus docetaxel alone [12–13].
An athracycline-taxane based regimen is most frequently used for breast cancer (neo)adjuvant treatment. The efficacy and adverse effects of capecitabine in addition to this regimen in patients with EBC which were reported in previous trials remained inconsistent. The US Oncology Group trial revealed that the addition of capecitabine to an anthracycline-taxane regimen significantly improved the OS (HR = 0.68, 95% CI 0.51–0.92, p = 0.011) compared to the anthracycline-taxane regimen, but there was no significant difference in DFS (HR = 0.84, 95% CI 0.67–1.05, p = 0.125) between the two regimens [14]. At a 2016 American Society of Clinical Oncology (ASCO) conference, Shao Z. reported that the addition capecitabine to the adjuvant treatment of triple-negative patients could significantly improve RFS (HR = 0.57, 95% CI 0.33–1.0, p = 0.049). Whereas, no significant difference in DFS was found between adjuvant therapies with and without capecitabine (HR = 0.73, 95% CI 0.44–1.23, p = 0.2344) [15]. Contrary to these reports, other studies suggested that the addition of capecitabine to an anthracycline-taxane based regimen would not improve DFS and OS [16–19].
To determine whether EBC patients would benefit from capecitabine combined with an anthracycline-taxane based (neo)adjuvant regimen. We here report the results of a meta-analysis of seven prospective randomized controlled trials (RCTs), examining the efficacy and safety of (neo)adjuvant therapies with and without capecitabine for the treatment of early breast cancer patients.
RESULTS
Eligibility studies
A total of seven trials (included ten articles) were identified from potential relevant studies (Figure 1). All the studies were randomized prospective cohort studies which included 7,416 early breast cancer patients; 3,725 received an anthracycline-taxane-capecitabine containing regimen and 3,691 received an anthracycline-taxane based regimen. Four trials focused on neoadjuvant chemotherapy and the other three were adjuvant chemotherapy trials. One trial was only published as an abstract and it only recruited triple negative early breast cancer patients. The remaining six trials were published as full articles. For the NSABP B-40 and GeparQuattro study, data were reported for three groups: Patients receiving gemcitabine in the NSABP B-40 trial and patients receiving docetaxel followed by capecitabine (T-X) in the GeparQuattro study were excluded from the meta-analysis based on the exclusion criteria. Of the seven trials, only six reported the survival data, four trials reported the endpoint pathologic complete response (pCR), and six trials reported adverse events. The characteristics of the seven RCTs included in this meta-analysis are shown in Table 1. The baseline demographics of patients of each eligible study are shown in Table 2.
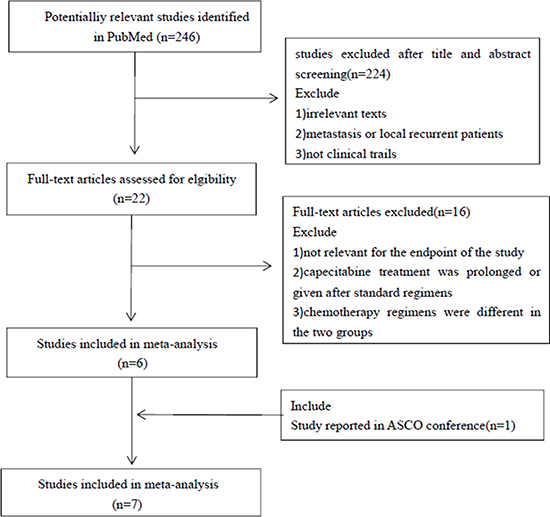
Figure 1: Process of studies selection.
Table 1: The characteristic of randomized clinical trials
Study |
Aouthors |
Year |
Regimens |
ITT |
Dose of X |
Dose of T |
Follow-up |
|---|---|---|---|---|---|---|---|
FinXX |
Joensuu H |
2012 |
TX-CEX |
751 |
900 mg/m2 bid |
60 mg/m2 |
5 |
T-CEF |
745 |
80 mg/m2 |
|||||
US Oncology Group |
O’Shaughnessy J |
2015 |
AC-TX |
1307 |
825 mg/m2 bid |
75 mg/m2 |
5 |
AC-T |
1304 |
100 mg/m2 |
|||||
Shao Z |
Shao Z |
2016 |
TX-CEX |
288 |
1000 mg/m2 bid |
N/A |
2.5 |
T-CEF |
273 |
N/A |
|||||
Ohno S |
Ohno S |
2013 |
CEF-TX |
239 |
825 mg/m2 bid |
75 mg/m2 |
4.5 |
CEF-T |
238 |
75 mg/m2 |
|||||
GeparQuattro |
von Minckwitz G |
2014 |
EC-TX |
471 |
900 mg/m2 bid |
75 mg/m2 |
5.4 |
EC-T |
471 |
100 mg/m2 |
|||||
NSABP B-40 |
Bear HD |
2015 |
TX-AC |
400 |
825 mg/m2 bid |
75 mg/m2 |
4.7 |
T-AC |
394 |
100 mg/m2 |
|||||
ABCSG-24 |
Steger GG |
2013 |
EDX |
270 |
1000 mg/m2 bid |
75 mg/m2 |
N/A |
ED |
266 |
75 mg/m2 |
ITT = intent-to-treat; X = capecitabine; T = docetaxel; C = cyclophosphamide; E = epeirubicin; A = doxorubicin; F = fl uorouracil; D = docetaxel. N/A = Not available.
Table 2: Baseline demographics of patients of each eligible study
Study |
Comparison |
Mean Age, Years |
HR positive, % |
HR negative, % |
HER-2 positive, % |
HER-2 negative, % |
TNBC, % |
|---|---|---|---|---|---|---|---|
FinXX (2012) |
TX-CEX vs T-CEF |
52 vs 53 |
77 vs 75 |
23 vs 25 |
19 vs 19 |
81 vs 81 |
N/A |
US Oncology Group (2015) |
AC-TX vs AC-T |
50 vs 51 |
64 vs 64 |
36 vs 36 |
12 vs 13 |
87 vs 86 |
30 vs 29 |
Shao Z (2016) |
TX-CEX vs T-CEF |
N/A |
N/A |
N/A |
N/A |
N/A |
100 vs 100 |
Ohno S(2013) |
CEF-TX vs CEF-T |
49 vs 49 |
66 vs 66 |
32 vs 31 |
20 vs 19 |
75 vs 77 |
N/A |
GeparQuattro (2014) |
EC-TX vs EC-T |
51 vs 49 |
64 vs 65 |
36 vs 35 |
31 vs 31 |
69 vs 69 |
23 vs 24 |
NSABP B-40 (2015) |
TX-AC vs T-AC |
N/A |
59 vs 60 |
41 vs 40 |
0 vs 0 |
100 vs 100 |
N/A |
ABCSG-24 (2013) |
EDX vs ED |
49 vs 49 |
67 vs 67 |
33 vs 33 |
74 vs 75 |
24 vs 23 |
N/A |
X = capecitabine; T = docetaxel; C = cyclophosphamide; E = epeirubicin; A = doxorubicin; F = fluorouracil; D = docetaxel. N/A = Not available: HR = hormone receptor: TNBC = triple negative breast cancer.
Total effect of capecitabine
Data for DFS were reported in six trials. The pooled estimate suggested that capecitabine could significantly improve DFS (HR = 0.87, 95% CI 0.77–0.97, heterogeneity I2 = 0.0% , p = 0.833) compared with the controls (Figure 2). The OS data were reported in five trials. The pooled estimate showed that capecitabine could significantly improved OS (HR = 0.78, 95% CI 0.66–0.91, heterogeneity I2 = 0.0%, p = 0.449) compared with the no capecitabine arm (Figure 3).
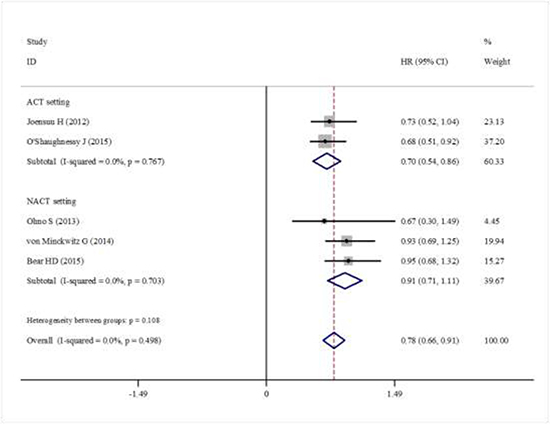
Figure 2: Forest plot showing the difference of total DFS in using capecitabine or not.
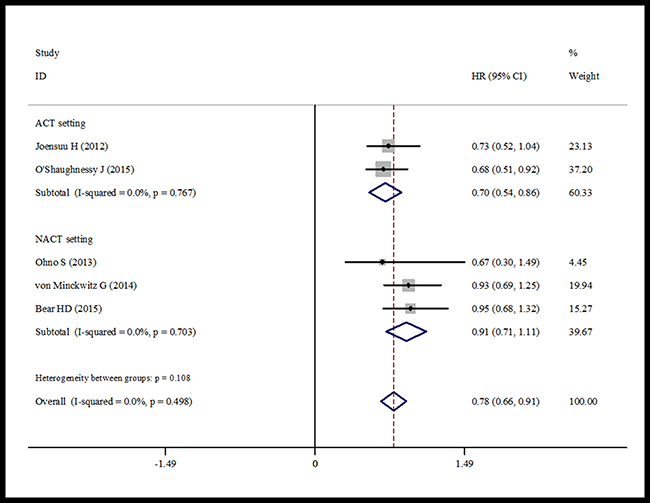
Figure 3: Forest plot showing the difference of total OS in using capecitabine or not.
Data about RFS were reported in three trials. We found that capecitabine significantly improved the RFS (HR = 0.79, 95% CI 0.64–0.93, heterogeneity I2 = 16.6%, p = 0.302) (Figure 4). Four trials reported the pCR rate [19, 20–22]. The pooled analysis showed no significant increase in the pCR rate in the capecitabine group (HR = 0.94, 95% CI 0.81–1.07, heterogeneity I2 = 31.8%, p = 0.222) compared with the control group (Figure 5).
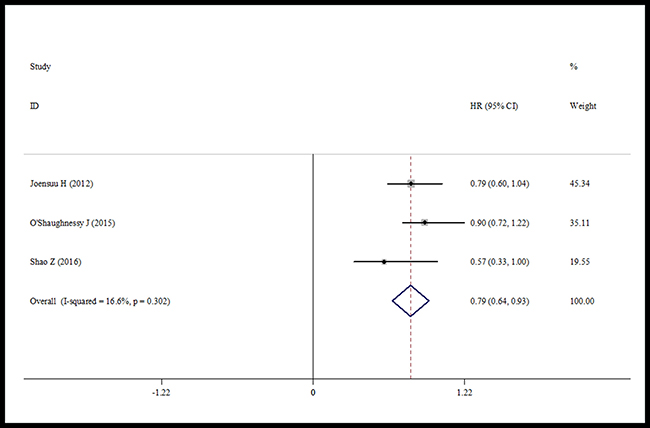
Figure 4: Forest plot of RFS in using capecitabine or not.
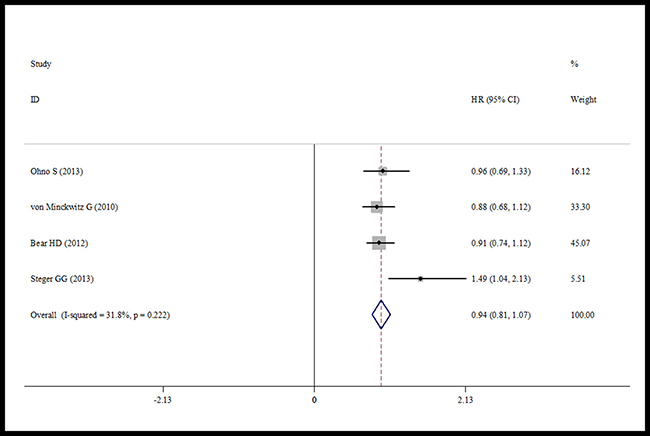
Figure 5: Forest plot of the pCR for the addition of capecitabine or not.
Subgroup analysis
Because of the lack of some patient information in trials, subgroup analysis was conducted only according to hormone receptor (HR) status, HER2 status, triple negative status, and for DFS, distant-DFS and breast cancer specific survival. The treatment effect according to HR status was only reported in two trials. The pooled estimate showed that there was no significant difference in the DFS in the HR positive subset between the capecitabine treated group and patients not treated with capecitabine (HR = 0.90, 95% CI 0.69–1.11, heterogeneity I2 = 0.0%, p = 0.963) (Figure 6). But for the HR negative subset, capecitabine significantly improved DFS (HR = 0.72, 95% CI 0.53–0.92, heterogeneity I2 = 0.0%, p = 0.655) (Figure 6).
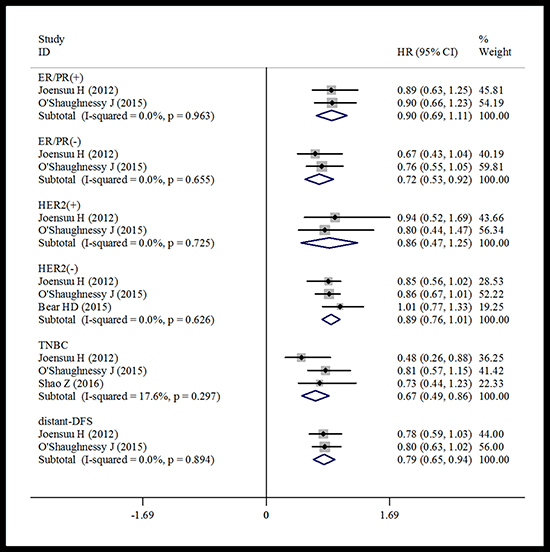
Figure 6: Forest plot of the subgroup DFS for the addition of capecitabine or not.
The pooled data based on two trials suggested that there was no significant difference in DFS for HER2 positive patients who were treated with and without capecitabine (HR = 0.86, 95% CI 0.47–1.25, heterogeneity I2 = 0.0%, p = 0.725) (Figure 6). Similarly, the pooled analysis including three trials showed that capecitabine did not make a significant improvement in DFS in the HER2 negative subset compared with the control group (HR = 0.89, 95% CI 0.76–1.01, heterogeneity I2 = 0.0%, p = 0.626) (Figure 6).
Data for TNBC were reported in three trials. A pooled estimate suggested that the capecitabine group had significantly improved DFS (HR = 0.67, 95% CI 0.49–0.86, heterogeneity I2 = 17.6%, p = 0.297) compared with the no capecitabine group (Figure 6).
Subgroup analysis based on two trials showed that adding capecitabine would significantly improve both distant-DFS and breast cancer specific survival compared with the controls. The pooled estimates were (HR = 0.79, 95% CI 0.65–0.94, heterogeneity I2 = 0.0%, p = 0.894) for distant-DFS (Figure 6) and (HR = 0.65, 95% CI 0.48–0.81, heterogeneity I2 = 0.0%, p = 0.953) for breast cancer specific survival (Figure 7), respectively.
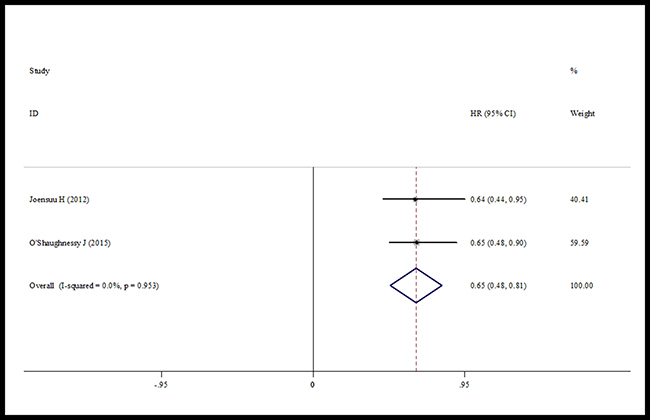
Figure 7: Forest plot of the breast cancer specific survival for the addition of capecitabine or not.
Safety
Adverse events were reported in six studies [14–15, 19, 21–23]. The pooled data showed a statistically significant increase in side effects in the capecitabine treated patients (≥ grade 3) among participants with early breast cancer: for hand-foot syndrome (HR = 4.91, 95% CI 3.78–6.03, heterogeneity I2 = 0.0%, p = 0.772), stomatitis (HR = 2.02, 95% CI 1.52–2.51, heterogeneity I2 = 0.0%, p = 0.889), diarrhea (HR = 1.87, 95% CI 1.36–2.38, heterogeneity I2 = 0.0%, p = 0.630). However, heterogeneity among trials was found in these analyses, possibly due to the use of different dosage of docetaxel and capecitabine (Figure 8).
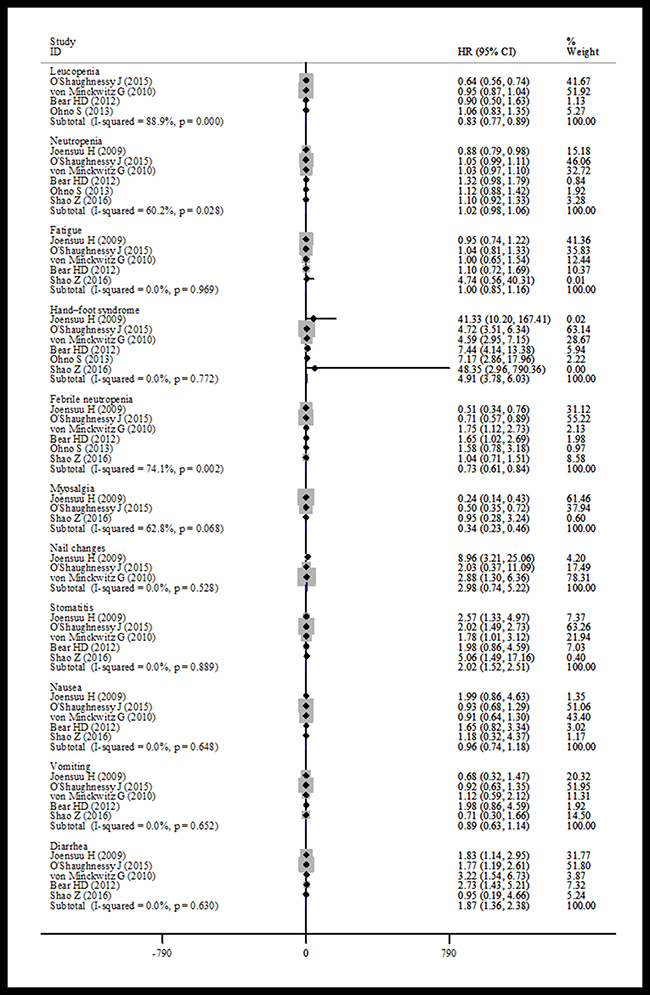
Figure 8: Forest plot of the adverse events for the addition of capecitabine or not.
Publication bias
No publication bias was found between the included studies base on the funnel plots. (Supplementary Figure 1 and Supplementary Figure 2)
DISCUSSION
A primary objective of this meta-analysis was to explore whether capecitabine in addition to an anthracycline-and taxane-based regimen can produce survival benefits in EBC patients. Our meta-analysis demonstrated that patients benefited substantially from capecitabine-anthracycline-taxane combined regimens in terms of DFS (HR = 0.87; 95% CI 0.77–0.97), RFS (HR = 0.79, 95% CI 0.64–0.93) and OS (HR = 0.78, 95% CI 0.66–0.91). In subgroup analysis, we found that capecitabine improved the DFS in hormone receptor negative (HR = 0.72, 95% CI 0.53–0.92) and triple negative (HR = 0.67, 95% CI 0.49–0.86) EBC patients.
Capecitabine is effective only after its conversion to 5-FU, but not by itself and its intermediates. Capecitabine is metabolized in the liver and in tumor tissue after absorption and is converted to 5-FU by sequential enzymatic activity. The final step is the conversion of 5′-deoxy-5-fluorouridine (5′-DFUR) to 5-FU through the enzymatic activity of thymidine phosphorylase (TP), an enzyme over expressed in tumor cells [10]. This tumor cells selective conversion of 5′-DFUR to 5-FU made greater efficacy and more safety than with other fluoropyrimidines. The capecitabine will have a synergistic effect with docetaxel and other cytotoxic drugs that can increase TP levels in the tumors, resulting from the direct chemical precursor of capecitabine being converted to 5-FU [24–25]. This synergistic effect should result in EBC patients benefiting from a capecitabine-taxane combined regimen.
Several studies have confirmed the efficacy of capecitabine treatment for patients with metastatic breast cancer [26–29]. After a median of 6.4 years followed-up, the US Oncology Group study have identified a significant improvement in OS (HR = 0.69, 95% CI 0.53–0.90) rather not in DFS (HR = 0.84, 95% CI 0.68–1.04) [14]. However, the data for 10-year survival from the randomized FinXX trial showed that capecitabine had no statistical significance during 10 years of follow-up in RFS (HR = 0.85 and 95% CI 0.68–1.07) or OS (HR = 0.83, 95% CI 0.65–1.06) [30]. This result was different from the conclusion of our meta-analysis, which may be related to the use of different doses of docetaxel in the control and experimental arms and approximately 24% of patients in the TX group that did not complete all cycles of treatment while about 47% of patients took less than the planned starting dose of capecitabine [14]. Data from a randomized controlled phase III study, GEICAM/2003-10, compared the ET-X (epirubicin and docetaxel followed by capecitabine) versus EC-T (epirubicin and cyclophosphamide followed by docetaxel) as adjuvant therapy for patients with node-positive EBC. The EC-T arm reported better invasive disease-free survival (IDFS) than the ET-X arm (HR = 1.30, 95% CI 1.03–1.64), but there was no significant difference in OS (HR = 1.13, 95% CI 0.81–1.55) [31]. However, this study used different chemotherapy regimens excepted capecitabine between the two arms, and cyclophosphamide was not used in the ET-X group. The authors considered that cyclophosphamide plays an important role in adjuvant BC therapy by its intrinsic antitumor properties or through the induction of amenorrhea in premenopausal patients [31]. All these factors may contribute to the opposite result in our study, and we excluded it in our meta-analysis base on the inclusion criteria. The recent CREAT-X trial also showed that capecitabine would significant improvement in DFS (HR = 0.70, 95% CI 0.53- 0.92) and OS (HR = 0.59, 95% CI 0.39- 0.90). However, capecitabine treatment was given after standard treatments (neoadjuvant chemotherapy and surgery) in the CREAT-X trial, and we excluded it in our meta-analysis base on the exclusion criteria [32].
Our data also showed that HR negative patients would have a DFS benefit with capecitabine over hormone receptor positive patients. Most patients in HR positive group accepted five years of treatment with tamoxifen or an aromatase inhibitor, which provides a significant survival benefits in patients with early-stage breast cancer [33] and reduces the risk of new contralateral breast tumors [34–35]. Moreover, different breast cancer subtypes have different recurrent times, the risk of HR positive breast cancer recurrence is for 8–9 years after surgery, but most included studies of this meta-analysis had failed to follow-up this long, and longer follow-up data are still warrented in future studies. While for HR negative patients, capecitabine would play a therapeutic role. The US Oncology Group study showed that capecitabine could significant improvement OS in HR negative patients (HR = 0.64, 95% CI 0.44–0.95) but not in the HR positive group [14]. The ABCSG24 trial also found that an addition of capecitabine to epirubicin and docetaxel had a greater chance of achieving pCR in the HR negative group [20]. But both the FinXX and US Oncology Group studies failed to indicate that capecitabine could improve DFS in HR negative group. CALGB 49907 trial showed that standard adjuvant chemotherapy with either CMF or doxorubicin plus cyclophosphamide is superior to capecitabine in older EBC patients, and it was pronounced in HR negative patients. These results just indicated that standard adjuvant chemotherapy is superior to capecitabine monotherapy in HR negative older patients with EBC. However, it may be more effective when capecitabine combined with standard adjuvant chemotherapy in HR negative older patients with EBC [36].
Triple negative breast cancer (TNBC) was defined by the absence of ER, PR and HER2. Patients with TNBC were more likely to have distant recurrence and death, and experienced higher risk of recurrence in the first 4 years after diagnosis compared to other breast cancer subtypes [37]. Thus, chemotherapy plays a crucial role for TNBC treatment, and it is the only systemic treatment for these patients. Our data showed that capecitabine combined with an anthracycline-taxane regimen would significantly improve DFS in TNBC patients. This result was similar with the FinXX trials, and after 10 years follow-up, the FinXX trials also showed more favorable RFS (HR = 0.43, 95% CI 0.24–0.79) and OS (HR = 0.55, 95% CI 0.31–0.96) in the capecitabine group [30]. The US Oncology Group study also found an OS benefit from capecitabine in TNBC patients (HR = 0.62, 95% CI 0.41–0.94) [14]. In the ABCSG-24 trial, the addition of capecitabine could significantly improve the pCR rate in TNBC patients (45.3% vs. 30.2% ) [20]. The current study had showed that the expression of TP in TNBC was higher than other subtypes, indicating a better curative effect with capecitabine in patients with TNBC [38]. All these joining evidence demonstrated that TNBC patients would benefit from an anthracycline-taxane-capecitabine combined regimen. While Conversely, Shao Z. reported that the addition of capecitabine in combination with an anthracycline-taxane-based regimen for TNBC patients achieved no significant difference in the DFS between the groups (90.58% vs. 86.8% , p = 0.23), whereas that the RFS would be improved [18]. However, this study only included a 30 mouth follow-up and fewer events occurred. The short follow-up and fewer events may have substantially decreased the power of the study to show the superiority of the capecitabine arm. Our meta-analysis suggests that capecitabine added to anthracycline-taxane will be a appropriate regimen for adjuvant therapy of TNBC.
This meta-analysis suggested that capecitabine would not improve the pCR rate in the neoadjuvant chemotherapy setting(NACT), which was consistent with three of the included trials [17–19] while only the ABCSG study found that capecitabine could significantly improve the pCR rate in the neoadjuvant chemotherapy setting. This indicated that not all subtypes would benefit from capecitabine except for patients with TNBC, perhaps partly on account of a higher TP expression in TNBC [38]. Unfortunately, due to lack of subgroups data in most included trails, subgroups analysis were not available. Current trial-based meta-analyses indicated only a weak correlation between pCR and survival outcomes for patients with neoadjuvant treatment, while the prognostic value of pCR was demonstrated in some subtypes (triple negative, HER2-positive, and hormone receptor negative) [39–40]. And we also found that the DFS or OS were not statistically different between the two groups in the NACT setting. In contrast, several other neoadjuvant trials have reported improved survival outcomes in patients with pCR compared with those without pCR [41–42]. However, because of the lack of survival data in the ABCSG trial, our data only reveal a negative result. Therefore, more clinical trials are still needed to explore and improve the long term outcome data. Different from the other three included trials, [15–17], participants in the ABCSG study received the same dose of docetaxel in both the experimental and the control arms, and most patients (96% ED and 94% EDC) completed all six treatment cycles. These factors may have contributed to the significant benefit observed in the ABCSG trial [20]. Therefore, a appropriate dose of docetaxel and capecitabine is warrented in future studies, and the ABCSG trial might be considered as a reference.
Another result analysis shows that capecitabine would significantly improve both distant-DFS and breast cancer specific survival. A statistical significance was observed in two of these studies focusing on breast cancer specific survival and in one of these concerning about distant-DFS. Our data showed that capecitabine combined with an anthracycline-taxane based regimen would improve OS in EBC compared with the control group. This may due to capecitabine significantly improving distant-DFS and breast cancer specific survival, which indicated a lower rate of systemic recurrence [14].
Some toxicity was also shown in our data analysis. Adding capecitabine to a standard regimen would result in increases in some adverse events. The most frequently increased adverse events were hand-foot syndrome, stomatitis, and diarrhea. These results were consistent with the findings of the FinXX, US Oncology Group, GeparQuattro and NSABP B-40 trials. Although there was a higher incidence of grade 3/4 capecitabine-related adverse events, no new safety related events were found in the capecitabine group, and it has a favorable safety profile [14]. Unfortunately, a statistical heterogeneity was found in these analyses, which might be linked with the use of different dosages of capecitabine and docetaxel because of the toxicity observed in the individual studies. More clinical trials are still necessary to explore and improve the toxicity data.
This meta-analysis has some potential limitations. First, we did not include enough articles in our meta-analysis, because our study has strict execute and inclusion criteria, with one trial available only as a conference abstract. Second, the included trials were varied in their follow-up periods, therapy regimens, and dosages. Third, subgroup analyses were only reported in few trials, future clinical trials with adequate subgroup analyses are needed to report complete data.
Despite the limitations of our meta-analysis, the results strongly indicate that capecitabine combined with an anthracycline-taxane based (neo)adjuvant regimen will improve RFS, DFS and OS, and is well-tolerated by patients with early breast cancer. Moreover, the subgroups analyses also demonstrated that the capecitabine combined with an anthracycline-taxane based (neo)adjuvant regimen may be effective for some high risk early breast cancer subtypes, especially for triple negative breast cancer, and might be a proper clinical choice.
MATERIALS AND METHODS
Search strategy
The literature search was conducted in PubMed, Cochrane library and Google scholar. Conference abstracts were searched in American Society of Clinical Oncology (www.asco.org). The following search terms were used in PubMed and the Cochrane library; “capecitabine”, “adjuvant”, “neoadjuvant”, “chemotherapy” and the expanded MeSH term “breast neoplasms”. In Google scholar, we used the terms; ”capecitabine”, “adjuvant”, “neoadjuvant”, “chemotherapy” and “breast cancer”. Relevant papers that were published before August 2016 were included. Moreover, the references of included literature and the related articles found in PubMed were also screened.
The criteria for inclusion studies were as follows: (a) randomized controlled prospective cohort trials comparing anthracycline-taxane based regimens with or without capecitabine; (b) early breast cancer patients without metastatic; (c) other chemotherapy regimens excepted capecitabine and the cycles of these drugs used were identical; (d) the primary endpoint was either disease-free survival (DFS), overall survival (OS) or pathologic complete response (pCR).
This systematic review excluded the relevant studies based on the following: (a) not a clinical trial; (b) metastasis or local recurrence breast cancer patients; (c) capecitabine treatment was prolonged or given after standard regimens; (d) not reporting the relevant endpoints of this systematic review.
Outcome measures
The primary outcome of this meta-analysis was DFS, defined as the time between randomization and date of diagnosis of disease recurrent or metastatic spread, new primary cancer or any cause of death, whichever occurred first. The OS was defined as death from any cause at the study endpoint. The RFS was defined as the time from randomization to invasive breast cancer recurrence, or death from any cause. The pCR was defined as complete tumor regression with no invasive breast cancer cells in both primary tumors and regional lymph nodes. Other outcomes included distant-DFS (time to systemic metastases and deaths), breast cancer specific survival (time to death due to breast cancer).
Data extraction
Data extraction from each eligible trial was used data extraction form. The following data was extracted: general characteristics of the study (the name of first author, the journal and year of publication, country, study design, the median follow-up time, the number of patients in each group), chemotherapeutic regimens and dose, HRs and 95% CIs for study outcomes, the number of patients with the grade 3 to 4 drug-related toxicities or pCR (the number of patients in each group was directly extracted from the included clinical trials or calculated according to the percentages).
Quality assessment
The Jadad Quality Assessment Scale for cohort studies was used to assess the quality of the inclusive trials in our analysis, and including the follow items: methods of randomization, allocation concealment, blinding status and results (withdrawals and dropouts) [43] (Table 3).
Table 3: The quality evaluation of included clinical trials by Jadad scale
Study |
randomization |
Allocation concealment |
blindness |
result |
score |
|---|---|---|---|---|---|
FinXX |
2 |
1 |
0 |
1 |
4 |
USON |
1 |
1 |
0 |
1 |
3 |
Shao Z |
2 |
1 |
0 |
0 |
3 |
Ohno S |
1 |
1 |
0 |
1 |
3 |
GeparQuattro |
1 |
1 |
0 |
1 |
3 |
NSABP B-40 |
2 |
1 |
0 |
1 |
4 |
ABCSG-24 |
2 |
1 |
0 |
1 |
4 |
Statistical analysis
The primary efficacy outcome of our meta-analysis was DFS. And the secondary endpoints were OS, RFS, pCR. Outcomes measures were based on the intention-to-treat (ITT) analysis. Efficacy and adverse events analysis was compared between the two groups used the pooled log hazard ratios (HRs), and their 95% confidence intervals (CI) were also provided. The subgroup analyses were performed by including the HR status, HER2 status, triple negative status, distant-DFS, and breast cancer specific survival. A random effects model was used for drawing forest plots which are designed to demonstrate data distribution of the included articles. It was considered statistically significant if the 95% CI did not include the value 1. The between-study heterogeneity was tested with I-squared statistic and p values. When the I-squared was greater than or equal to 50%, or the p value was less than 0.05, we considered the presence of a high level of heterogeneity.
The probability of publication bias was assessed with the funnel plots and the Egger’s test with statistical significance set at p < 0.05. All statistical analyses were performed using Stata (version 12.0).
Author contributions
Jiantang Zhang, Fangmeng Fu and Chuan Wang conceived and wrote the protocol of the study, Jiantang Zhang, Yazhen Chen, Minjun Lu and Peodong Yang performed the search, assessed the references for inclusion and extracted data from the studies. Meng Huang performed the statistical calculation. Jiantang Zhang produced the manuscript, which was critically revised by Fangmeng Fu, Yuxiang Lin and Minyan Chen.
ACKNOWLEDGMENTS
The authors would like to thank Wenhui Guo, Lili Chen, Weibin Lian, Na Wu for valuable comments in preparation of the manuscript.
CONFLICTS OF INTEREST
The authors have declared no conflicts of interest.
FUNDING
The study was supported by grants from National Nature Science Foundation (No.81302320), Medical-care System Excellent Youth Foundation Program (2015-ZQN-ZD-14#) and Sci-Tech Key Program of Fujian Province (2015J01473 and 2016J01549).
REFERENCES
1. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer. 2015; 136:E359–386.
2. Servick K. Breast cancer. Breast cancer: a world of differences. Science. 2014; 343:1452–1453.
3. Verma S, Lavasani S, Mackey J, Pritchard K, Clemons M, Dent S, Latreille J, Lemieux J, Provencher L, Verma S, Chia S, Wang B, Rayson D. Optimizing the management of HER2-positive early breast cancer: the clinical reality. Current Oncology. 2010; 17:20–33.
4. Early Breast Cancer Trialists’ Collaborative G. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005; 365:1687–1717.
5. Polychemotherapy for early breast cancer: an overview of the randomised trials. Early Breast Cancer Trialists’ Collaborative Group. Lancet. 1998; 352:930–942.
6. De Laurentiis M, Cancello G, D’Agostino D, Giuliano M, Giordano A, Montagna E, Lauria R, Forestieri V, Esposito A, Silvestro L, Pennacchio R, Criscitiello C, Montanino A, et al. Taxane-based combinations as adjuvant chemotherapy of early breast cancer: A meta-analysis of randomized trials. Journal of Clinical Oncology. 2008; 26:44–53.
7. Mamounas EP, Bryant J, Lembersky B, Fehrenbacher L, Sedlacek SM, Fisher B, Wickerham DL, Yothers G, Soran A, Wolmark N. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: results from NSABP B-28. Journal of Clinical Oncology. 2005; 23:3686–3696.
8. Sparano JA, Wang M, Martino S, Jones V, Perez EA, Saphner T, Wolff AC, Sledge GW Jr, Wood WC, Davidson NE. Weekly paclitaxel in the adjuvant treatment of breast cancer. The New England Journal of Medicine. 2008; 358:1663–1671.
9. Bear HD, Anderson S, Smith RE, Geyer CE Jr, Mamounas EP, Fisher B, Brown AM, Robidoux A, Margolese R, Kahlenberg MS, Paik S, Soran A, Wickerham DL, et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer:National Surgical Adjuvant Breast and Bowel Project Protocol B-27. Journal of Clinical Oncology. 2006; 24:2019–2027.
10. Miwa M, Ura M, Nishida M, Sawada N, Ishikawa T, Mori K, Shimma N, Umeda I, Ishitsuka H. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. European Journal of Cancer. 1998; 34:1274–1281.
11. O’Shaughnessy JA, Kaufmann M, Siedentopf F, Dalivoust P, Debled M, Robert NJ, Harbeck N. Capecitabine monotherapy: review of studies in first-line HER-2-negative metastatic breast cancer. The Oncologist. 2012; 17:476–484.
12. O’Shaughnessy J, Miles D, Vukelja S, Moiseyenko V, Ayoub JP, Cervantes G, Fumoleau P, Jones S, Lui WY, Mauriac L, Twelves C, Van Hazel G, Verma S, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: phase III trial results. Journal of Clinical Oncology. 2002; 20:2812–2823.
13. Miles D, Vukelja S, Moiseyenko V, Cervantes G, Mauriac L, Van Hazel G, Liu WY, Ayoub JP, O’Shaughnessy JA. Survival benefit with capecitabine/docetaxel versus docetaxel alone: analysis of therapy in a randomized phase III trial. Clinical Breast Cancer. 2004; 5:273–278.
14. O’Shaughnessy J, Koeppen H, Xiao Y, Lackner MR, Paul D, Stokoe C, Pippen J Jr, Krekow L, Holmes FA, Vukelja S, Lindquist D, Sedlacek S, Rivera R, et al. Patients with Slowly Proliferative Early Breast Cancer Have Low Five-Year Recurrence Rates in a Phase III Adjuvant Trial of Capecitabine. Clinical Cancer Research. 2015; 21:4305–4311.
15. Shao Z, Li J, Pang D, Wang C, Jiang J, Yang S, Liu Y, Fu P, Sheng Y, Zhang G, Cao L, He Q, Cui S, et al. Cbcsg-10: Adjuvant capecitabine in combination with docetaxel and cyclophosphamide plus epirubicin for triple negative breast cancer. Journal of Clinical Oncology. 2016; 34: abstr 1012.
16. Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, Kokko R, Ahlgren J, Auvinen P, Paija O, Helle L, Villman K, Nyandoto P, Nilsson G, et al. Adjuvant capecitabine, docetaxel, cyclophosphamide, and epirubicin for early breast cancer: final analysis of the randomized FinXX trial. Journal of Clinical Oncology. 2012; 30:11–18.
17. von Minckwitz G, Rezai M, Fasching PA, Huober J, Tesch H, Bauerfeind I, Hilfrich J, Eidtmann H, Gerber B, Hanusch C, Blohmer JU, Costa SD, Jackisch C, et al. Survival after adding capecitabine and trastuzumab to neoadjuvant anthracycline-taxane-based chemotherapy for primary breast cancer (GBG 40-GeparQuattro). Annals of Oncology. 2014; 25:81–89.
18. Bear HD, Tang G, Rastogi P, Geyer CE Jr, Liu Q, Robidoux A, Baez-Diaz L, Brufsky AM, Mehta RS, Fehrenbacher L, Young JA, Senecal FM, et al. Neoadjuvant plus adjuvant bevacizumab in early breast cancer (NSABP B-40 [NRG Oncology]): secondary outcomes of a phase 3, randomised controlled trial. The Lancet Oncology. 2015; 16:1037–1048.
19. Ohno S, Chow LW, Sato N, Masuda N, Sasano H, Takahashi F, Bando H, Iwata H, Morimoto T, Kamigaki S, Nakayama T, Nakamura S, Kuroi K, et al. Randomized trial of preoperative docetaxel with or without capecitabine after 4 cycles of 5-fluorouracil-epirubicin-cyclophosphamide(FEC) in early-stage breast cancer: exploratory analyses identify Ki67 as a predictive biomarker for response to neoadjuvant chemotherapy. Breast Cancer Research and Treatment. 2013; 142:69–80.
20. Steger GG, Greil R, Lang A, Rudas M, Fitzal F, Mlineritsch B, Hartmann BL, Bartsch R, Melbinger E, Hubalek M, Stoeger H, Dubsky P, et al. Epirubicin and docetaxel with or without capecitabine as neoadjuvant treatment for early breast cancer: final results of a randomized phase III study (ABCSG-24). Annals of Oncology. 2014; 25:366–371.
21. Bear HD, Tang G, Rastogi P, Geyer CE Jr, Robidoux A, Atkins JN, Baez-Diaz L, Brufsky AM, Mehta RS, Fehrenbacher L, Young JA, Senecal FM, et al. Bevacizumab added to neoadjuvant chemotherapy for breast cancer. The New England Journal of Medicine. 2012; 366:310–320.
22. von Minckwitz G, Rezai M, Loibl S, Fasching PA, Huober J, Tesch H, Bauerfeind I, Hilfrich J, Eidtmann H, Gerber B, Hanusch C, Kühn T, du Bois A, et al. Capecitabine in addition to anthracycline/taxane-based neoadjuvant treatment in patients with primary breast cancer: The Phase III GeparQuattro Study. Journal of Clinical Oncology. 2010; 28:2015–2023.
23. Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, Asola R, Kokko R, Ahlgren J, Auvinen P, Hemminki A, Paija O, Helle L, Nuortio L, et al. Adjuvant capecitabine in combination with docetaxel and cyclophosphamide plus epirubicin for breast cancer: an open-label, randomised controlled trial. The Lancet Oncology. 2009; 10:1145–1151.
24. Kurosumi M, Tabei T, Suemasu K, Inoue K, Kusawake T, Sugamata N, Higashi Y. Enhancement of immunohistochemical reactivity for thymidine phosphorylase in breast carcinoma cells after administration of docetaxel as a neoadjuvant chemotherapy in advanced breast cancer patients. Oncology Reports. 2000; 7:945–948.
25. Fujimoto-Ouchi K, Tanaka Y, Tominaga T. Schedule dependency of antitumor activity in combination therapy with capecitabine/5›-deoxy-5-fluorouridine and docetaxel in breast cancer models. Clinical Cancer Research. 2001; 7:1079–1086.
26. Daniele G, Gallo M, Piccirillo MC, Giordano P, D’Alessio A, Del Giudice A, La Porta ML, Perrone F, Normanno N, De Luca A. Pharmacokinetic evaluation of capecitabine in breast cancer. Expert Opinion on Drug Metabolism & Toxicology. 2013; 9:225–235.
27. Molteni LP, Rampinelli I, Cergnul M, Scaglietti U, Paino AM, Noonan DM, Bucci EO, Gottardi O, Albini A. Capecitabine in breast cancer: the issue of cardiotoxicity during fluoropyrimidine treatment. The Breast Journal. 2010; 16:S45–48.
28. Naughton M. Evolution of capecitabine dosing in breast cancer. Clinical Breast Cancer. 2010; 10:130–135.
29. Dellapasqua S, Bertolini F, Bagnardi V, Campagnoli E, Scarano E, Torrisi R, Shaked Y, Mancuso P, Goldhirsch A, Rocca A, Pietri E, Colleoni M. Metronomic cyclophosphamide and capecitabine combined with bevacizumab in advanced breast cancer. Journal of Clinical Oncology. 2008; 26: 4899–4905.
30. Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, Kokko R, Auvinen P, Lahdenperä O, Villman K, Nyandoto P, Nilsson G, Murashev M, Poikonen-Saksela P, et al. Adjuvant capesitabine in combination with docetaxel (T), epirubicin (E), and cyclophosphamide (C) in the treatment of early breast cancer (BC): 10-year survival results from the randomized FinXX trial. Journal of Clinical Oncology. 2016; 34: abstr 1001.
31. Martín M, Ruiz Simón A, Ruiz Borrego M, Ribelles N, Rodríguez-Lescure Á, Muñoz-Mateu M, González S, Margelí Vila M, Barnadas A, Ramos M, Del Barco Berron S, Jara C, Calvo L, et al. Epirubicin Plus Cyclophosphamide Followed by Docetaxel Versus Epirubicin Plus Docetaxel Followed by Capecitabine As Adjuvant Therapy for Node-Positive Early Breast Cancer: Results From the GEICAM/2003–10 Study. Journal of Clinical Oncology. 2015; 33:3788–3795.
32. Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, Kuroi K, Im SA, Park BW, Kim SB, Yanagita Y, Ohno S, Takao S, et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. The New England Journal of Medicine. 2017; 376:2147–2159.
33. Tamoxifen for early breast cancer: an overview of the randomised trials. Early Breast Cancer Trialists› Collaborative Group. Lancet. 1998; 351:1451–1467.
34. Fisher B, Dignam J, Bryant J, DeCillis A, Wickerham DL, Wolmark N, Costantino J, Redmond C, Fisher ER, Bowman DM, Deschênes L, Dimitrov NV Margolese RG, et al. Five versus more than five years of tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen receptor-positive tumors. Journal of the National Cancer Institute. 1996; 88:1529–1542.
35. Fisher B, Costantino JP, Wickerham DL, Redmond CK, Kavanah M, Cronin WM, Vogel V, Robidoux A, Dimitrov N, Atkins J, Daly M, Wieand S, Tan-Chiu E, et al. Tamoxifen for prevention of breast cancer: Report of the national surgical adjuvant breast and bowel project P-1 study. Journal of the National Cancer Institute. 1998; 90: 1371–1388.
36. Muss HB, Berry DA, Cirrincione CT, Theodoulou M, Mauer AM, Kornblith AB, Partridge AH, Dressler LG, Cohen HJ, Becker HP, Kartcheske PA, Wheeler JD, Perez EA, et al. Adjuvant chemotherapy in older women with early-stage breast cancer. The New England Journal of Medicine. 2009; 360:2055–65.
37. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P, Narod SA. Triple-negative breast cancer: clinical features and patterns of recurrence. Clinical Cancer Research. 2007; 13:4429–4434.
38. Umemura S, Shirane M, Takekoshi S, Tokuda Y, Mori K, Osamura RY. High expression of thymidine phosphorylase in basal-like breast cancers: Stromal expression in EGFR- and/or CK5/6-positive breast cancers.Oncology Letters. 2010; 1:261–266.
39. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L, Valagussa P, Swain SM, Prowell T, Loibl S, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014; 384:164–172.
40. von Minckwitz G, Untch M, Nuesch E, Loibl S, Kaufmann M, Kummel S, Fasching PA, Eiermann W, Blohmer JU, Costa SD, Mehta K, Hilfrich J, Jackisch C, et al. Impact of treatment characteristics on response of different breast cancer phenotypes: pooled analysis of the German neo-adjuvant chemotherapy trials. Breast Cancer Research and Treatment. 2011; 125:145–156.
41. Feldman LD, Hortobagyi GN, Buzdar AU, Ames FC, Blumenschein GR. Pathological assessment of response to induction chemotherapy in breast cancer. Cancer Research. 1986; 46: 2578–2581.
42. von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, Gerber B, Eiermann W, Hilfrich J, Huober J, Jackisch C, Kaufmann M, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. Journal of Clinical Oncology. 2012; 30: 1796–1804.
43. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary. Controlled Clinnical Trials. 1996; 17:1–12.