
INTRODUCTION
Blockade of immune checkpoints has recently emerged as a novel treatment for various cancers. In particular, monoclonal antibodies targeting programmed cell death 1 (PD-1) or its ligand (PD-L1) have been extensively studied in lung cancer, and their roles as first-line [1] or second-line [2-6] treatment in the management of advanced non-small cell lung cancer (NSCLC) patients are well established. The reports from high-profile clinical trials have shown an association of PD-L1 expression determined by immunohistochemistry (IHC) with overall response rates which suggested that PD-L1 expression may be a clinically applicable predictive biomarker [1, 2, 7].
The recent clinical series had reported various degrees of PD-L1 expression in lung cancers ranging from 7.4% to 72.7%, which was well reviewed by Mino-Kenudson [8]. The same series have correlated PD-L1 expression with clinicopathologic characteristics, molecular variables, and survival but the results vary greatly [8-13]. Each PD-1 or PD-L1 inhibitor is developed with a companion diagnostic biomarker using a different PD-L1 antibody (clones SP263, SP142, 22C3, 28-8, and etc.), IHC platforms, and scoring systems, which make a head-to-head comparison between studies difficult. Among the PD-L1 antibodies, only the PD-L1 IHC 22C3 pharmDx assay has obtained regulatory approval as a companion diagnostic, which is linked to the use of pembrolizumab [1, 2, 7]. Clinical application of the 22C3-PD-L1 biomarker was essentially confined to patients with advanced NSCLC and there is only limited information on patients with early stage resectable lung cancer. Recently, commercial 22C3-PD-L1 IHC diagnostic assays became available. However, to our knowledge, the clinical data linked to clinicopathologic factors and survival are very limited and the results also inconsistent, even using the FDA approved standard 22C3 PD-L1 antibody [12, 14, 15].
Primary mechanism of PD-L1 on tumors is innate immune resistance and adaptive immune resistance. Interferon gamma (IFN-γ) is released by CD8+ T-cells and is a major inducer of PD-L1 expression in vivo [16, 17]. In addition, PD-L1 expression was up-regulated secondary to constitutive oncogenic signaling within tumor cells, which is evidenced by the small fraction of human cancers that lack tumor infiltrating lymphocytes (TILs) in the tumor microenvironment but still express high levels of PD-L1 [11, 16, 18-22]. Recently, multiple studies of various malignancies have shown that PD-L1 expression is associated with significant TIL infiltration of the tumor microenvironment. However, a standardized methodology for evaluating TILs in lung cancer is still unavailable and several studies with NSCLC cohorts have investigated TILs in association with PD-L1 expression, again, producing conflicting results [8].
To address the issue, we investigate association with clinicopathologic characteristics and the prognostic value of PD-L1 expression measured by a commercial 22C3-PD-L1 immunohistochemistry diagnostic assay with a Dako platform in patients with surgically resectable NSCLC. We have also explored the immune microenvironment by studying the association between PD-L1 expression and tumor lymphocyte infiltration.
RESULTS
Patient characteristics
A total of 170 patients were eligible for study and their characteristics are summarized in Table 1. Median age at diagnosis was 56 years (range, 34-78 years) and 118/170 (69.4%) patients were male. The ECOG performance status was 0 in all patients. Adenocarcinoma and squamous carcinoma accounted for 94/170 (55.3%) and 76/170 (44.7%), respectively. Fifty patients (29.4%), 43 (25.3%), and 77 (45.3%) had stage I, stage II and stage III disease, respectively (Table 1). The EGFR and ALK status were not routinely detected in China between 2008 and 2010 and data is not always available in the medical records. As a result, only 13 patients had their EGFR status known (10 EGFR mutations, 5 wild-type), and 13 patients had known ALK status (12 negative, 1 positive). Ninety-six of 120 (80.0%) patients with stage II and stage III disease have been offered adjuvant chemotherapy.
Table 1: Association between 22C3-PD-L1 protein expression and clinicopathological factors
Subgroup |
N |
PD-L1 expression N(%) |
Univariate analysis |
Multivariate analysis |
|||
|---|---|---|---|---|---|---|---|
TPS <1% |
1 to 49% |
≥50% |
OR(95%CI) P value |
OR(95%CI) P value |
|||
Overall |
170 |
110(64.7%) |
42(24.7%) |
18(10.6%) |
|||
Gender |
|||||||
Female |
52 |
38(73.1%) |
12(23.1%) |
2(3.8%) |
1.73 (0.85-3.55) |
||
Male |
118 |
72(61.0%) |
30(25.4%) |
16(13.6%) |
0.132 |
||
Age |
|||||||
≤60y |
99 |
63(63.6%) |
27(27.3%) |
9(9.1%) |
0.89 (0.47-1.70) |
||
>60y |
71 |
47(66.2%) |
15(21.1%) |
9(9.3%) |
0.730 |
||
Smoking status |
|||||||
Never-smoke |
97 |
68(70.1%) |
20(20.6%) |
9(9.3%) |
1.73 (0.92-3.27) |
||
Smokers |
73 |
42(57.5%) |
22(30.1%) |
9(12.3%) |
0.091 |
||
Histology |
|||||||
AD |
94 |
69(73.4%) |
19(20.2%) |
6(6.4%) |
2.36 (1.24-4.48) |
2.02 (1.01-4.01) |
|
SCC |
76 |
41(53.9%) |
23(30.3%) |
12(15.8%) |
0.009 |
0.045 |
|
Tumor location |
|||||||
Peripheral |
74 |
53(71.6%) |
16(21.6%) |
5(6.8%) |
1.73 (0.90-3.31) |
||
Central |
96 |
57(59.4%) |
26(27.1%) |
13(13.5%) |
0.099 |
||
TNM stage |
|||||||
I |
50 |
40(80.0%) |
7(14.0%) |
3(6.0%) |
Reference |
Reference |
|
II |
43 |
25(58.1%) |
8(18.6%) |
10(23.3%) |
2.88 (1.15-7.23) |
2.68 (1.03-7.02) |
|
III |
77 |
45(58.4%) |
27(35.1%) |
5(6.5%) |
2.84 (1.24-6.51) |
3.53 (1.48-8.42) |
|
0.031 |
0.016 |
||||||
TILs |
|||||||
Absence |
29 |
25(86.2%) |
4(13.8%) |
0(0.0%) |
4.12 (1.36-12.47) |
5.32 (1.69-16.68) |
|
Presence |
141 |
85(60.3%) |
38(27.0%) |
18(12.8%) |
0.012 |
0.004 |
|
AD, adenocarcinoma; SCC, squamous carcinoma.
PD-L1 expression and correlation with clinicopathological characteristics
PD-L1 was commonly expressed at the cell membrane of cancer cells, and only in selective cases in the cytoplasm. Heterogeneous distribution of PD-L1 staining was observed within a single section of tumor tissue, with some areas being dominated by cells with strong PD-L1 expression, whereas other areas were characterized by cells lacking PD-L1 expression. Representative examples of PD-L1 Tumor Proportion Score (TPS) <1%, TPS 1 to 49%, and TPS ≥50% are shown in Figure 1. The PD-L1 TPS ≥50% and TPS 1 to 49% were observed in 10.6% and 24.7% of patient tumors. Among the 60 cases that were considered PD-L1 positive (TPS ≥1%), the median percentage of tumor cells with positive staining was 30% (interquartile range, 2%-50%).
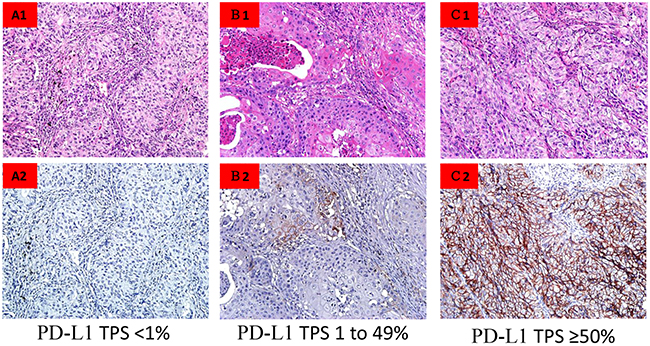
Figure 1: PD-L1 immunohistocehmistry labeling in NSCLC tumor specimens. (A) PD-L1 TPS <1%. (B) PD-L1 TPS 1 to 49%. (C) PD-L1 TPS ≥50%.
Expression of PD-L1 was correlated with the clinicopathological characteristics by univariate analysis in a two-level classification of tumors that were negative (TPS <1%) vs. positive (TPS ≥1%) for PD-L1 expression (Table 1). There was no statistically significant association between PD-L1 expression and gender, age, smoking status and primary tumor location in the univariate analysis (Table 1).
Histology is strongly correlated with PD-L1 expression. Incidence of positive PD-L1 expression in squamous carcinoma tumors was 46.1% comparing to 26.6% in adenocarcinoma tumors (OR 2.36; 95%CI, 1.24-4.48, p=0.009). In this study, higher tumor stage was significantly associated with PD-L1 expression in univariate analysis, stage I 20.0%, stage II 41.9%, and stage III 41.6%, p=0.031. In the multivariate binary logistic analysis, squamous carcinoma tumors and higher TNM stage was confirmed as significantly independent factors for higher incidence of PD-L1 expression (Table 1).
TILs and classification of tumor immune microenvironment
TILs were observed in 141 (82.9%) of the tumors (Table 1). Representative examples of different types of tumor immune microenvironments are shown in Figure 2. In the present study, we found 56 (39.8%) PD-L1 positive tumors and 85 (60.3%) PD-L1 negative tumors among the tumors with TILs present. The tumors without TILs included four (13.8%) tumors that were PD-L1 positive and 25 tumors (86.2%) that were PD-L1 negative. Furthermore, there were no cases of the subtype of PD-L1 TPS ≥50% detected in the tumors without TILs. The odds ratio (OR) was 4.12 (95% CI, 1.36-12.47), p=0.012, by univariate analysis and OR 5.32 (95% CI, 1.69-16.68), p=0.004, by multivariate analysis (Table 1).
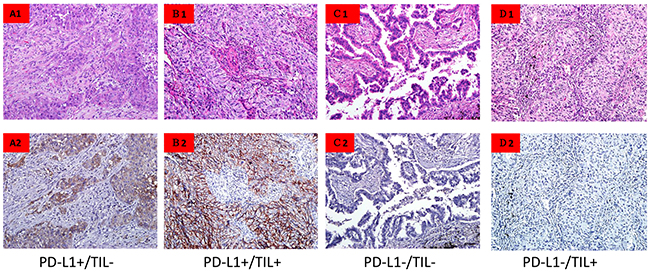
Figure 2: Tumor cell PD-L1 expression and lymphocytic infiltration. (A) PD-L1+TILs-. (B) PD-L1+TILs+. (C) PD-L1-TILs-. (D) PD-L1-TILs+. TILs showed PD-L1 positive expression in (D). 20X.
Prognostic value of PD-L1 expression and TILs
Survival data in this study were censored on January 07, 2017. The median follow-up time was 53.8 months (m) (range: 1.4 to 104 m) and 89 patients had cancer-related deaths.
In the univariate survival analysis the PD-L1 negative expression group had a tendency to have a longer overall survival than the PD-L1 positive expression group, median overall survival 67.6 months (95%CI, 60.2-74.9) vs. 57.9 months (95%CI, 47.4-68.4), HR 1.32 (95%CI, 0.86-2.02), p=0.202 (Figure 3A). Using the TNM stage as a stratification factor (Stage III vs. Stage I+II), PD-L1 expression was still not associated with overall survival in the population (Figure 3E, 3F). Similarly, there was no significant difference in OS between patients with TILs and without TILs, HR 0.86; 95%CI, 0.50-1.48; p=0.586 (Figure 3B). Furthermore, TIL status was not an independent prognostic factor for overall survival using 50% stromal TILs as the cut-off (Table 2). The patients were divided into four subgroups; PD-L1+TILs+, PD-L1+TILs-, PD-L1-TILs+ and PD-L1-TILs-. Kaplan-Meier graphical analysis demonstrated that OS was not significantly different among the four subgroups, HR 0.85; 95%CI, 0.67-1.06, p=0.148 (Figure 3C). The unadjusted survival curves show a statistically significant association between TNM stage and survival, which also confirmed in the multivariate Cox regression analysis after controlling for covariates (Figure 3D; Table 2).
Table 2: Univariate and multivariate analyses of OS in all patients using the 1% cutoff value
Variables |
Reference |
Univariate analyses |
Multivariate analyses |
||
|---|---|---|---|---|---|
HR(95% CI) |
P value |
HR(95% CI) |
P value |
||
Gender |
Male |
1.12 (0.71-1.77) |
0.626 |
||
Age |
≤60y |
1.20 (0.79-1.83) |
0.391 |
||
Histology |
Squamous |
1.05 (0.69-1.59) |
0.83 |
||
Smoking status |
Never smokers |
1.26 (0.83-1.90) |
0.286 |
||
|
TNM stage |
I (reference) |
<0.001 |
<0.001 |
||
II |
3.24 (1.54-6.82) |
0.002 |
3.58 (1.69-7.56) |
0.001 |
|
III |
6.18 (3.14-12.16) |
<0.001 |
5.11(2.49-10.48) |
<0.001 |
|
PD-L1 expression |
Negative |
1.32 (0.86-2.02) |
0.202 |
||
PD-L1 expression in Stage I and II |
Negative |
1.15 (0.56-2.38) |
0.700 |
||
PD-L1 expression in Stage III |
Negative |
1.22 (0.72-2.06) |
0.470 |
||
TILs |
Absence |
0.86 (0.50-1.48) |
0.586 |
||
TILs |
>50% TILs |
0.71 (0.43-1.18) |
0.189 |
||
PD-L1 expression* TILs |
0.85 (0.67-1.06) |
0.148 |
|||
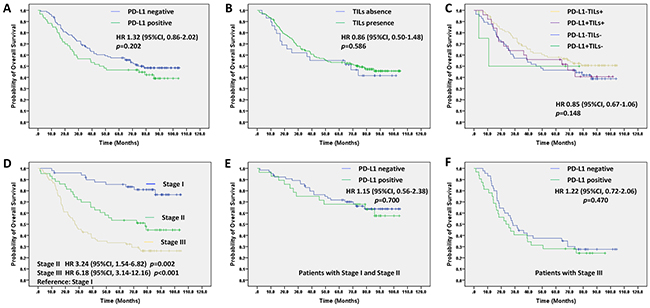
Figure 3: Prognostic value of PD-L1 expression and TILs status and interaction between them in the univariate survival analysis. (A) for PD-L1 expression and OS. (B) for TILs status and OS. (C) for interaction between PD-L1 and TILs status and OS. (D) for TNM stage and OS. (E) for PD-L1 expression in patients with Stage I and stage II and OS. (F) for PD-L1 expression in patients with Stage III and OS.
DISCUSSION
We studied PD-L1 expression and TILs in 170 patients with resectable NSCLC and found neither the PD-L1 expression, TILs status, nor their combination to be an independent prognosis biomarker. The incidence of positive PDL1 expression is lower than expected. This could be related to the early stage of disease.
We noticed that many clinical series of lung cancers had reported various amounts of PD-L1 expression and correlate expression with clinicopathologic characteristics and/or survival leading to conflicting results [8]. One of interpretation of the discrepancy could be different antibodies, platforms, and cut-off values when comparing the experimental positives used in the different studies. Hirsch et al. studied the concordance between four PD-L1 antibodies (SP142, SP263, 22C3 and 28-8) and found similar analytical performance for three assays (SP263, 22C3 and 28-8). There were cases of misclassification of PD-L1 status comparing SP142 to the other three [23, 24]. Echoing Hirsch, another study compared the performance of four PD-L1 platforms, including the 28-8 antibody on the Dako Link 48 platform, the 22c3 antibody on the Dako Link 48 platform, the SP142 antibody on the Ventana Benchmark platform, and the E1L3N antibody on the Leica Bond platform. Results showed that the assay using the SP142 antibody was an outlier that detected significantly less PD-L1 expression in tumor cells and immune cells. The assay using antibody 22C3 showed slightly yet significantly less staining than either 28-8 or E1L3N [25].
Among the above PD-L1 antibodies, it is only the PD-L1 IHC 22C3 pharmDx assay that has obtained regulatory status as a companion diagnostic. We performed a literature search in PubMed for studies using the 22C3-PD-L1 assay published before Mar 1, 2017 [1, 2, 7, 12, 14, 15, 26] that had an association with clinicopathologic characteristics and/or survival (summarized in Table 3). The prevalence of 22C3-PD-L1 positive expression appears to be different between advanced NSCLC and early stage NSCLC. Three clinical trials (KEYNOTE-001, KEYNOTE-010 and KEYNOTE-024) have shown that the TPS ≥50% in patients with advanced NSCLC was between 23.2% and 30.2% and TPS (1 to 49%) was reported in 37.6% to 37.9% [1, 2, 7]. We found a lower incidence of positive PD-L1 expression in our cohort of patients with early stage NSCLC. Furthermore, our study showed that the PD-L1 expression is more likely influenced by disease stage, which indicated that the induction of PD-L1 expression was not an initial event in the development of cancer. A recent study echoes our finding, which report the incidence TPS ≥50% at 7.4% and TPS 1-49% at 20.8% [12]. We also found squamous carcinoma tumors to be strongly associated with PD-L1 expression. The biological determinants and potential clinical implications of these observations are unknown and require further study.
Table 3: Summary of recent studies investigating 22C3-PD-L1 expression in NSCLC
Author |
N |
PD-L1 (%) |
Histology (%) |
Stage (%) |
Correlation with |
Prognosis of |
|---|---|---|---|---|---|---|
1-49%/ >50% |
ADs/Sq/others |
I/II/III/IV |
||||
Reck M1 |
1653 |
-/30.2 |
- |
0/0/0/100 |
- |
- |
Herbst RS2 |
2222 |
37.9/28.5 |
- |
0/0/0/100 |
- |
- |
Garon EB7 |
824 |
37.6/23.2 |
81.0*/17.2/1.8 |
0/0/0/100 |
KRAS mutation |
- |
Cooper WA12 |
678 |
20.8/7.4 |
40.7/40.0/19.3 |
50/50(II+III)/0 |
Younger: High tumor grade |
Better |
He Y14 |
139 |
-/18.0 |
28.8/58.3/12.9 |
41.7/25.2/28.1/5.0 |
NS |
Poor |
Sorensen SF15 |
204 |
50/25 |
72/21.6/6.4 |
-/-/-/88 |
NS |
NS |
Rangachari D26 |
71 |
28.2/29.6 |
100/0/0 |
25.4(I-III)/74.6 |
Smoking |
- |
Present study |
170 |
24.7/10.6 |
55.3/44.7 |
29.4/25.3/45.3/0 |
Histology; TILs; tumor stage |
NS |
-, data not shown; NS, not significant; *, nonsquamous.
Recent studies, including ours, have investigated the prognostic impact of PD-L1 expression in NSCLC. However, the results are conflicting [8]. Differences in PD-L1 antibody clones used in the various studies could contribute to the conflicting results. In fact, the results were inconsistent even in three studies using the same 22C3 PD-L1 antibody [12, 14, 15]. One study found high PD-L1 expression was associated with early postoperative recurrence in a Korean population of early and advanced stage NSCLC, particularly in adenocarcinoma [14]. In contrast, PD-L1 high expression appears to be a favorable prognostic factor in a cohort of 678 patients with early stage disease [12]. In another study, PD-L1 expression is not a strong prognostic indicator in a European population of patients with advanced stage NSCLC treated with chemotherapy [15], which was similar to our results. Based on our study, PD-L1 expression is more likely influenced by tumor stage, therefore, the dynamics of PD-L1 expression may also limit its use as a prognostic biomarker.
A framework was previously proposed to stratify the tumor microenvironment into different types based on the presence or absence of TILs and PD-L1 expression [16, 27, 28]. We observed TILs presence in most patients with positive PD-L1 expression. All patients with PD-L1 TPS ≥50% were found to have presence of TILs. Brambilla et al. found intense TILs (>50% stromal TILs) in a minority of tumors that was a favorable prognostic marker for survival in resected non-small-cell lung cancer [9]. However, our analysis showed the contrary. One of reason is that pathologists have shown poor agreement of the scoring of immune cells probed with different antibodies [25]. In addition, it is not surprising using that TILs as a single factor has been found to produce paradoxical results for survival. The role of TILs in cancer growth is complex, and TILs may both promote or suppress tumor progression [29]. For the immediate future, it is critical to focus on a specific cell subsets within TILs and delve deeply into the details of the TILs present and to characterize them in relation to genetic and microenvironment characteristics.
In conclusion, incidence of PD-L1 expression (by 22C3) in patients with resectable NSCLC is relatively lower than in patients with advanced NSCLC. Our findings do not support PD-L1 expression, TILs, or the combination of both as a significant prognostic factor for resectable NSCLC.
MATERIALS AND METHODS
Patients and materials
Primary tumor samples were from the archive of patients with surgically resectable NSCLC and pathologically confirmed adenocarcinoma or squamous cell carcinoma at the Fujian Cancer Hospital in China between January 2008 and December 2010. None of the patients had prior anti-PD-1/PD-L1 therapies, neo-adjuvant chemotherapy or EGFR/ALK-targeted therapy. The clinicopathologic information of patients was collected from the clinical records and pathology reports. The pathological TNM stage was reassigned according to the 8th TNM staging [30] and lung tumor histology were reclassified according to the 2015 World Health Organization (WHO) classification for lung tumors [31]. Patients with stage II/III disease may have been offered adjuvant chemotherapy and patients with recurrent disease received chemotherapy and/or EGFR-targeted therapy. The study design was approved by the Ethical Committee of Fujian Cancer Hospital; and written informed consent was obtained from all patients.
PD-L1 immunohistochemistry
We conduct the study on PD-L1 expression at the Chinese University of Hong Kong, using automated staining by the Autostainer Link 48 with the murine 22C3 anti-human PD-L1 antibody (Code SK006, Merck & Co., Inc., Hong Kong) according to the manufacturer’s protocol. Each staining run contained positive and negative controls along with a negative isotype-matched antibody control for each sample. Two board-certified pathologists (CL, DH) independently evaluated all stained slides for PD-L1 membrane staining. All areas in a tissue section were observed to appropriately evaluate the expression of PD-L1 on tumor cells. Following the standard recommendation as per prior publications, PD-L1 expression was determined by the TPS and classified into TPS <1%, TPS 1 to 49% and TPS ≥50%. [1, 2, 7]. Using PD-L1 TPS ≥1% as the cut off, PD-L1 expression were classified into positive (TPS ≥1%) and negative (TPS <1%) groups.
Evaluation of tumor infiltrating lymphocytes
The independent scoring of TILs was performed in hematoxylin & eosin stained formalin fixed paraffin embedded tissue sections by two pathologists (CL, DH). Due to the lack of a standardized methodology for evaluating TILs in lung cancer, we adopted a recently reported system for standardized evaluation of TILs in breast cancer, which is also adopted in lung cancer [32]. Briefly, TILs were classified into three groups as no/minimal immune cells (0-10% stromal TILs), intermediate/heterogeneous infiltrates (10-40% stromal TILs), and high immune infiltrates (40-90% stromal TILs). The agreement analysis showed that the kappa varied from 0.40 to 0.76 for three groups and from 0.67 to 0.86 for two groups, TILs absent vs. TILs present with >10% stromal TILs as the cut off. The discordant cases were reviewed to reach a final consensus classification. After the concordance analysis, the lymphocyte infiltration was considered as a binary marker (TILs absent vs. TILs present) for the statistical analysis.
Classification of tumor immune microenvironment
Based on PD-L1 expression and TILs status, we classified the tumor immune microenvironment into four categories: 1) PD-L1 positive expression and TILs present (PD-L1+TILs+), 2) PD-L1 positive expression and TILs absent (PD-L1+TILs-), 3) PD-L1 negative and TILs present (PD-L1-TILs+), 4) PD-L1 negative and TILs absent (PD-L1-TILs-).
Statistical analysis
Using PD-L1 TPS ≥1% as the cut off, PD-L1 expression were classified into positive (TPS ≥1%) and negative (TPS <1%) groups. The level of PD-L1 positive expression was compared in subgroups based on age (≤60yr or >60yr), gender (male or female), smoking status (never smoker or former/current smoker), primary tumor location (central or peripheral), histology (adenocarcinoma or squamous carcinoma), TNM stage (I, II, or III) and TILs (absence or presence) using the binary logistic analysis. Adjustment was made for age, gender, smoking status, primary tumor location, histology, TNM stage and TILs in multivariate binary logistic analysis.
Overall survival (OS) was defined as the time from the date of diagnosis to the date of death or the last follow-up. The Kaplan-Meier method and a log-rank test were used for univariate survival analysis. Survival rate correlation of PD-L1 expression with, age, gender, smoking status, histology, TNM stage, PD-L1 expression, TILs and interaction between PD-L1 expression and TILs were estimated by the Kaplan-Meier method and survival curves were compared with the log-rank test. Cox proportional hazard models were used for multivariate survival analysis that controlled for the above factors and the hazard ratio (HR) and 95% CI were estimated.
Statistical analyses were performed using SPSS16.0 software. All tests were two-sided. Statistical significance was set at p<0.05.
Abbreviations
PD: L1: programmed death ligand 1; NSCLC: non-small cell lung cancer; TILs: tumor infiltrating lymphocytes; TPS: Tumor Proportion Score; PD-1: programmed cell death 1; IHC: immunohistochemistry; IFN-γ: interferon gamma; AD: adenocarcinoma; SCC: squamous carcinoma; NS: not significant; WHO: World Health Organization; OS: overall survival; HR: hazard ratio; FDA: Food and Drug Administration; CI: confidence interval.
Author contributions
Gen lin and Chao Li designed experiments, analyzed data and wrote the manuscript; Gen lin, Xirong Fan, Weifeng Zhu and Dan Hu conducted experiments, Cheng Huang, Wu Zhuang, Haipeng Xu, Xiandong Lin, Yunjian Huang, Kan Jiang and Qian Miao contributed to clinical data collection and analysis; and all authors approved the final manuscript before submission.
ACKNOWLEDGMENTS
The authors are grateful to Tony S. Mok for critical advice.
CONFLICTS OF INTEREST
The authors do not have any conflicts of interest.
FUNDING
This work was supported by the National Natural Science Foundation of China (grant number 81372599); the Fujian Provincal health systemic youth backbone training projects (grant number 2015-ZQN-ZD-9); Natural Science Foundation of Fujian province (grant number 2015J01434) and the National Clinical Key Specialty Construction Program of China (2014).
REFERENCES
1. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O’Brien M, Rao S, Hotta K, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016; 375:1823-1833.
2. Herbst RS, Baas P, Kim DW, Felip E, Perez-Gracia JL, Han JY, Molina J, Kim JH, Arvis CD, Ahn MJ, Majem M, Fidler MJ, de Castro GJ, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016; 387:1540-1550.
3. Rizvi NA, Mazieres J, Planchard D, Stinchcombe TE, Dy GK, Antonia SJ, Horn L, Lena H, Minenza E, Mennecier B, Otterson GA, Campos LT, Gandara DR, et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol. 2015; 16:257-265.
4. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, Barlesi F, Kohlhaufl M, Arrieta O, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015; 373:1627-1639.
5. Brahmer J, Reckamp KL, Baas P, Crino L, Eberhardt WE, Poddubskaya E, Antonia S, Pluzanski A, Vokes EE, Holgado E, Waterhouse D, Ready N, Gainor J, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015; 373:123-135.
6. Gettinger SN, Horn L, Gandhi L, Spigel DR, Antonia SJ, Rizvi NA, Powderly JD, Heist RS, Carvajal RD, Jackman DM, Sequist LV, Smith DC, Leming P, et al. Overall survival and long-term safety of nivolumab (anti-programmed death 1 antibody, BMS-936558, ONO-4538) in patients with previously treated advanced non-small-cell lung cancer. J Clin Oncol. 2015; 33:2004-2012.
7. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M, Horn L, Carcereny E, Ahn MJ, Felip E, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015; 372:2018-2028.
8. Mino-Kenudson M. Programmed cell death ligand-1 (PD-L1) expression by immunohistochemistry: could it be predictive and/or prognostic in non-small cell lung cancer? Cancer Biol Med. 2016; 13:157-170.
9. Brambilla E, Le Teuff G, Marguet S, Lantuejoul S, Dunant A, Graziano S, Pirker R, Douillard JY, Le Chevalier T, Filipits M, Rosell R, Kratzke R, Popper H, et al. Prognostic effect of tumor lymphocytic infiltration in resectable non-small-cell lung cancer. J Clin Oncol. 2016; 34:1223-1230.
10. Kim MY, Koh J, Kim S, Go H, Jeon YK, Chung DH. Clinicopathological analysis of PD-L1 and PD-L2 expression in pulmonary squamous cell carcinoma: comparison with tumor-infiltrating T cells and the status of oncogenic drivers. Lung Cancer. 2015; 88:24-33.
11. Velcheti V, Schalper KA, Carvajal DE, Anagnostou VK, Syrigos KN, Sznol M, Herbst RS, Gettinger SN, Chen L, Rimm DL. Programmed death ligand-1 expression in non-small cell lung cancer. Lab Invest. 2014; 94:107-116.
12. Cooper WA, Tran T, Vilain RE, Madore J, Selinger CI, Kohonen-Corish M, Yip P, Yu B, O’Toole SA, McCaughan BC, Yearley JH, Horvath LG, Kao S, et al. PD-L1 expression is a favorable prognostic factor in early stage non-small cell carcinoma. Lung Cancer. 2015; 89:181-188.
13. Koh J, Go H, Keam B, Kim MY, Nam SJ, Kim TM, Lee SH, Min HS, Kim YT, Kim DW, Jeon YK, Chung DH. Clinicopathologic analysis of programmed cell death-1 and programmed cell death-ligand 1 and 2 expressions in pulmonary adenocarcinoma: comparison with histology and driver oncogenic alteration status. Mod Pathol. 2015; 28:1154-1166.
14. He Y, Yu H, Rozeboom L, Rivard CJ, Ellison K, Dziadziuszko R, Suda K, Ren S, Wu C, Hou L, Zhou C, Hirsch FR. LAG-3 protein expression in non-small cell lung cancer and its relationship with PD-1/PD-L1 and tumor-infiltrating lymphocytes. J Thorac Oncol. 2017; 12:814-823.
15. Sorensen SF, Zhou W, Dolled-Filhart M, Georgsen JB, Wang Z, Emancipator K, Wu D, Busch-Sorensen M, Meldgaard P, Hager H. PD-L1 expression and survival among patients with advanced non-small cell lung cancer treated with chemotherapy. Transl Oncol. 2016; 9:64-69.
16. Taube JM, Anders RA, Young GD, Xu H, Sharma R, McMiller TL, Chen S, Klein AP, Pardoll DM, Topalian SL, Chen L. Colocalization of inflammatory response with B7-H1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci Transl Med. 2012; 4:127r-137r.
17. Spranger S, Spaapen RM, Zha Y, Williams J, Meng Y, Ha TT, Gajewski TF. Up-regulation of PD-L1, IDO, and T(regs) in the melanoma tumor microenvironment is driven by CD8(+) T cells. Sci Transl Med. 2013; 5:116r-200r.
18. Akbay EA, Koyama S, Carretero J, Altabef A, Tchaicha JH, Christensen CL, Mikse OR, Cherniack AD, Beauchamp EM, Pugh TJ, Wilkerson MD, Fecci PE, Butaney M, et al. Activation of the PD-1 pathway contributes to immune escape in EGFR-driven lung tumors. Cancer Discov. 2013; 3:1355-1363.
19. Ota K, Azuma K, Kawahara A, Hattori S, Iwama E, Tanizaki J, Harada T, Matsumoto K, Takayama K, Takamori S, Kage M, Hoshino T, Nakanishi Y, et al. Induction of PD-L1 expression by the EML4-ALK oncoprotein and downstream signaling pathways in non-small cell lung cancer. Clin Cancer Res. 2015; 21:4014-4021.
20. Parsa AT, Waldron JS, Panner A, Crane CA, Parney IF, Barry JJ, Cachola KE, Murray JC, Tihan T, Jensen MC, Mischel PS, Stokoe D, Pieper RO. Loss of tumor suppressor PTEN function increases B7-H1 expression and immunoresistance in glioma. Nat Med. 2007; 13:84-88.
21. Marzec M, Zhang Q, Goradia A, Raghunath PN, Liu X, Paessler M, Wang HY, Wysocka M, Cheng M, Ruggeri BA, Wasik MA. Oncogenic kinase NPM/ALK induces through STAT3 expression of immunosuppressive protein CD274 (PD-L1, B7-H1). Proc Natl Acad Sci U S A. 2008; 105:20852-20857.
22. Chen N, Fang W, Zhan J, Hong S, Tang Y, Kang S, Zhang Y, He X, Zhou T, Qin T, Huang Y, Yi X, Zhang L. Upregulation of PD-L1 by EGFR activation mediates the immune escape in EGFR-driven NSCLC: implication for optional immune targeted therapy for NSCLC patients with EGFR mutation. J Thorac Oncol. 2015; 10:910-923.
23. Ratcliffe MJ, Sharpe A, Midha A, Barker C, Scott M, Scorer P, Al-Masri H, Rebelatto M, Walker J. Agreement between programmed cell death ligand-1 diagnostic assays across multiple protein expression cut-offs in non-small cell lung cancer. Clin Cancer Res. 2017; 23:3585-3591.
24. Hirsch FR, McElhinny A, Stanforth D, Ranger-Moore J, Jansson M, Kulangara K, Richardson W, Towne P, Hanks D, Vennapusa B, Mistry A, Kalamegham R, Averbuch S, et al. PD-L1 immunohistochemistry assays for lung cancer: results from phase 1 of the blueprint PD-L1 IHC assay comparison project. J Thorac Oncol. 2017; 12:208-222.
25. Rimm DL, Han G, Taube JM, Yi ES, Bridge JA, Flieder DB, Homer R, West WW, Wu H, Roden AC, Fujimoto J, Yu H, Anders R, et al. A prospective, multi-institutional, pathologist-based assessment of 4 immunohistochemistry assays for PD-L1 expression in non-small cell lung cancer. JAMA Oncol. 2017; 3:1051-1058.
26. Rangachari D, VanderLaan PA, Shea M, Le X, Huberman MS, Kobayashi SS, Costa DB. Correlation between classic driver oncogene mutations in EGFR, ALK, or ROS1 and 22C3-PD-L1 >/=50% expression in lung adenocarcinoma. J Thorac Oncol. 2017; 12:878-883.
27. Sznol M, Chen L. Antagonist antibodies to PD-1 and B7-H1 (PD-L1) in the treatment of advanced human cancer. Clin Cancer Res. 2013; 19:1021-1034.
28. Teng MW, Ngiow SF, Ribas A, Smyth MJ. Classifying cancers based on T-cell infiltration and PD-L1. Cancer Res. 2015; 75:2139-2145.
29. Kataki A, Scheid P, Piet M, Marie B, Martinet N, Martinet Y, Vignaud JM. Tumor infiltrating lymphocytes and macrophages have a potential dual role in lung cancer by supporting both host-defense and tumor progression. J Lab Clin Med. 2002; 140:320-328.
30. Detterbeck FC, Chansky K, Groome P, Bolejack V, Crowley J, Shemanski L, Kennedy C, Krasnik M, Peake M, Rami-Porta R. The IASLC lung cancer staging project: methodology and validation used in the development of proposals for revision of the stage classification of NSCLC in the forthcoming (eighth) edition of the TNM classification of lung cancer. J Thorac Oncol. 2016; 11:1433-1446.
31. Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JH, Beasley MB, Chirieac LR, Dacic S, Duhig E, Flieder DB, Geisinger K, Hirsch FR, Ishikawa Y, et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015; 10:1243-1260.
32. Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, Wienert S, Van den Eynden G, Baehner FL, Penault-Llorca F, Perez EA, Thompson EA, Symmans WF, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann Oncol. 2015; 26:259-271.