
INTRODUCTION
Wilms’ tumor (WT) is the most common malignant renal tumor in children [1]. Treatments of WT have improved significantly over the past 40 years, and approximately 90% of patients now achieve a long survival. This progress has been attributed to combining the clinical stage and histological type [2]. However, WT remains to be conquered completely. Only approximately 50% of patients who relapse will survive [3, 4], and hence it is important to identify the prognostic factors associated with the relapse in patients with WT, and more intense treatment may need to be added early to patients with worse prognostic factors.
Some studies have found loss of heterozygosity on chromosome 16q (LOH 16q) to be involved in malignant progression of various tumor types, including WT and those of the breast, prostate, and liver [5–8]. LOH 16q is present in 20–30% of WT patients. The National Wilms Tumor Study (NWTS) first proposed the hypothesis that WT with LOH 16q is associated with relapse based on a study of 232 cases of WT [9], and the findings of several other studies support this conclusion [10, 11]. However, other studies have failed to find a significant role of LOH 16q in recurrence among WT patients [12–15], and so it is still unclear whether LOH 16q is associated with WT relapse.
Our goal was to determine the association between LOH 16q and relapse in WT by conducting a meta-analysis. This is the first meta-analysis to determine this relation, and the findings might further help to predict the prognosis and improve the treatment of WT.
RESULTS
Study selection
In total, 224 relevant studies were identified using PUBMED, EMBASE, and the Cochrane Library, of which 96 duplicates were removed. Scanning the titles and Abstracts resulted in a further 109 studies being excluded because they did not meet the inclusion criteria. The remaining 19 studies were further evaluated by reading the full texts, which resulted in 9 studies being excluded due to a lack of useful data or the presence of duplicate data. Therefore, 10 studies [9–11, 13–19] involving 3385 patients were ultimately included in the meta-analysis. Figure 1 shows the process of study selection.
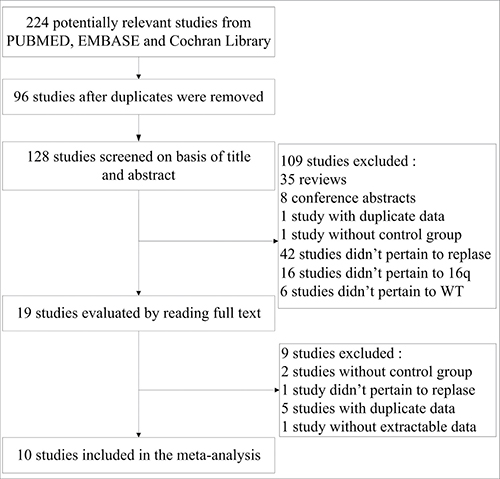
Figure 1: Flow diagram for study selection.
Study characteristics and quality assessment
The 10 included studies were reported on between 1994 and 2017, and all of them were cohort studies. Four of them involved international collaborations [14, 15, 17, 19], five were performed in Europe [9–11, 13, 18], and one was performed in North America [16]. The characteristics of the included studies are presented in Table 1, including the number of patients and their ages, the follow-up period, method to detect LOH 16q, and the quality scores. The quality scores were determined with reference to the Newcastle-Ottawa Scale (NOS) about cohort studies: three studies [14, 15, 19] were of high quality while the other seven [9–11, 13, 16–18] were of moderate quality. The mean with standard deviation of NOS score is 5.8 ± 0.92.
Table 1: Characteristics of included studies
Study |
Country |
Patients |
Age |
Follow-up |
Method to Detect LOH 16q |
NOS score |
|---|---|---|---|---|---|---|
Grundy PE 1994 |
USA and Canada |
206 patients with favorable-histology WT |
Not known |
Median follow-up durations in LOH and non-LOH groups of 1.3 and 1.4 years, respectively |
PCR |
6 |
Klamt B 1998 |
Germany, Austria, and Switzerland |
73 patients with WT |
Mean 3.48 years |
Not known |
PCR |
5 |
Grundy RG 1998 |
UK |
40 patients with sporadic WT |
Not known |
At least 7 years |
PCR |
5 |
Skotnicka KG 2000 |
Poland |
66 patients with WT |
Median 39 months, range 2 days to 13 years |
Median 42 months, range 14 to 139 months |
PCR |
5 |
Kullendorff CM 2003 |
Sweden |
39 patients with WT |
Mean 4.2 years, range 5 months to 15 years |
Range 7 to 160 months |
Not known |
5 |
Grundy PE 2005 |
USA, Canada, Australia, New Zealand, Switzerland, and the Netherlands |
2021 patients younger than 16 years at diagnosis with specific WT |
Younger than 16 years |
4 years |
PCR |
7 |
Messahel B 2009 |
UK |
426 patients with favorable-histology WT |
Not known |
4 years |
Microsatellite markers |
6 |
Spreafico F 2012 |
Italy |
125 patients with nonanaplastic unilateral WT of stages I to IV |
Median 40 months, range 1 to 172 months |
Mean 73 months, range 35 to 97 months |
Microsatellite markers |
5 |
Chagtai T 2016 |
26 countries: 24 in Europe, 1 in Australia, 1 in South America |
586 patients with WT of stages I to IV |
Range 6 months to 18 years |
Median 68 months |
Multiplex Ligation-Dependent Probe Amplification |
7 |
Fernandez CV 2017 |
the United States, Canada, Australia, New Zealand, and Israel |
116 patients with very low risk WT (defined as stage I favorable histology WT with nephrectomy weight < 550 g and age at diagnosis < 2 years) |
11.5 months: 0.1 to 23 months |
80 months: 5 to 97 months |
Multiplex Ligation-Dependent Probe Amplification |
7 |
Abbreviations: LOH, Loss of heterozygosity; WT, Wilms’ tumor.
LOH 16q and relapse
The estimated relative risk (RR) for the association between exposure to LOH 16q and WT relapse is presented in Figure 2. All of the included studies mentioned the RR for relapse. A fixed-effects model was used to pool the data. The pooled estimate showed that the LOH 16q was significantly associated with a higher risk of the relapse compared with that in the control group (RR = 1.74, 95% confidence interval [CI] = 1.43–2.13, P < 0.00001). There was no significant heterogeneity among the studies for this outcome (Pheterogeneity = 0.12, I2 = 35%).
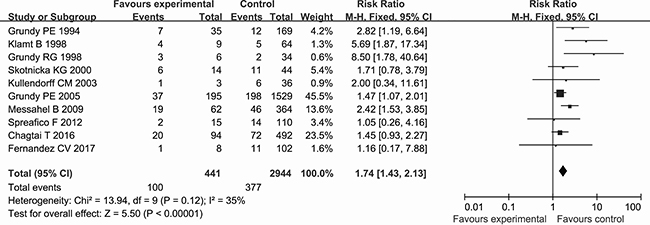
Figure 2: Forest plot of the association between LOH 16q and the relapse of WT using the RR as the effect measure.
The estimated hazard ratio (HR) for the association between exposure to LOH 16q and WT relapse is shown in Figure 3. Six studies investigated the relapse risk of WT based on analyzing the HR. The fixed-effects model was used to calculate the pooled HR due to the absence of significant heterogeneity among the studies (Pheterogeneity = 0.18, I2 = 15%). The pooled estimate showed LOH 16q to be significantly associated with a higher risk of WT relapse (HR = 1.76, 95% CI = 1.38–2.24, P < 0.00001).
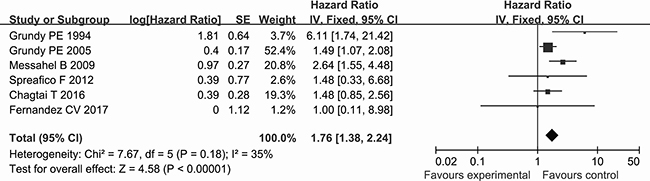
Figure 3: Forest plot of the association between LOH 16q and the relapse of WT using the HR as the effect measure.
Two studies enrolled patients with favorable-histology WT. Subgroup analysis was performed by patients with favorable-histology WT. The pooled RR for favorable-histology WT was 2.52 (95% CI = 1.68–3.78, P < 0.00001, Pheterogeneity = 0.76, I2 = 0%) (Figure 4A). The pooled HR for favorable-histology WT was 2.99 (95% CI = 1.84–4.88, P < 0.0001, Pheterogeneity = 0.23, I2 = 32%) (Figure 4B). The results indicated that LOH 16q was more effective on elevated replase risk in patients with favorable-histology WT.
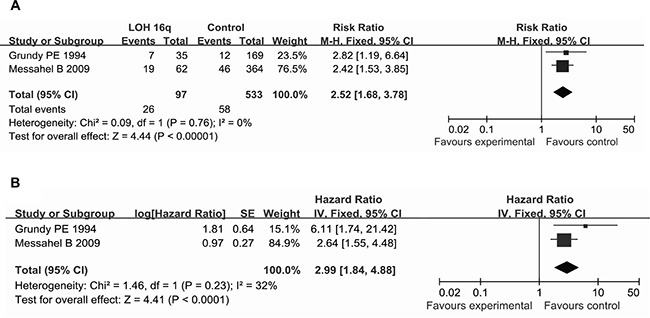
Figure 4: Forest plot of the association between LOH 16q and the relapse in patients with favorable-histology WT (A) using the RR as the effect measure; (B) using the HR as the effect measure.
Publication bias
Funnel plot, Begg’s test and Egger’s test were used to investigate publication bias in the included studies. Visual inspection of the funnel plot did not identify substantial asymmetry (Figure 5), indicating no evidence of substantial publication bias. The Begg’s and Egger’s tests also confirmed the absence of significant publication bias among the included studies (Begg’s test: P = 0.283; Egger’s test: P = 0.053).
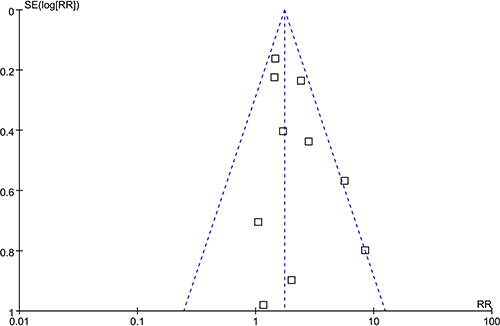
Figure 5: Funnel plot for detecting publication bias.
Sensitivity analysis
Sensitivity analysis showed that a significant association between LOH 16q and relapse in WT was still observable even when any single study was removed (Table 2 and Table 3), which mean the stability of the result that LOH 16q was associated with increased replase risk.
Table 2: Sensitivity analysis of association between LOH 16q and WT relapse risk for the RR by omitting one study in each turn
Study omitted |
Pooled RR |
95% CI |
P |
|---|---|---|---|
Grundy PE 1994 |
1.7 |
1.38–2.08 |
< 0.00001 |
Klamt B 1998 |
1.7 |
1.39–2.08 |
< 0.00001 |
Grundy RG 1998 |
1.69 |
1.38–2.07 |
< 0.00001 |
Skotnicka KG 2000 |
1.75 |
1.42–2.14 |
< 0.00001 |
Kullendorff CM 2003 |
1.74 |
1.43–2.13 |
< 0.00001 |
Grundy PE 2005 |
1.98 |
1.53–2.55 |
< 0.00001 |
Messahel B 2009 |
1.64 |
1.31–2.04 |
< 0.0001 |
Spreafico F 2012 |
1.77 |
1.45–2.16 |
< 0.00001 |
Chagtai T 2016 |
1.83 |
1.47–2.29 |
< 0.00001 |
Fernandez CV 2017 |
1.75 |
1.44–2.14 |
< 0.00001 |
Table 3: Sensitivity analysis of association between LOH 16q and WT relapse risk for the HR by omitting one study in each turn
Study omitted |
Pooled HR |
95% CI |
P |
|---|---|---|---|
Grundy PE 1994 |
1.67 |
1.31–2.14 |
< 0.0001 |
Grundy PE 2005 |
2.1 |
1.48–2.99 |
< 0.0001 |
Messahel B 2009 |
1.58 |
1.2–2.07 |
0.001 |
Spreafico F 2012 |
1.77 |
1.38–2.25 |
< 0.00001 |
Chagtai T 2016 |
1.83 |
1.4–2.4 |
< 0.0001 |
Fernandez CV 2017 |
1.77 |
1.39–2.26 |
< 0.00001 |
DISCUSSION
LOH 16q is present in 20–30% of WT cases [9], and a recent study found that the mean frequency of LOH 16q was 15.1% (95% CI = 12.9–17.2%) [20]. A LOH 16q status has been associated with WT relapse and might consequently play an important role in determining the optimal treatment [5, 21]. This information is being used to stratify patients within NWTS therapeutic protocols to warrant more intensive early drug regimens [19, 22]. However, other studies have found no significant association between LOH 16q and WT relapse [12–15], and hence this relationship remains controversial. The present meta-analysis is, to the best of our knowledge, the first to evaluate whether LOH 16q is associated with the relapse in WT.
Ten cohort studies were included in this meta-analysis. Although cohort studies have many methodological shortcomings in comparison with randomized controlled trials (RCTs), we included cohort studies in the inclusion criteria rather than RCTs based on feasibility. RCT is a kind of intervention trial, and intervention measures involving LOH in patients are technically difficult to implement and they have major ethical problems. Furthermore, it was found that there were no RCTs investigating this topic in the initially searched 224 studies from PUBMED, EMBASE, and the Cochrane Library.
Our meta-analysis revealed that LOH 16q was significantly associated with the relapse in WT using the RR as the effect measure, and that there was no significant heterogeneity among the included studies. Nevertheless, relapses are time-to-event outcomes, and the RR only measures the number of relapses without accounting for when they occur [23]. This may introduce bias into the results and lead to inappropriate conclusions when analyzing time-to-event outcomes such as relapses. In contrast, the HR summarizes the difference between two Kaplan-Meier curves, and represents the overall reduction in the risk of time-to-event outcomes over the follow-up period among patients [24]. It is still defective only to use the HR as the effect measure due to the lnHRs and their standard errors of some included studies were estimated according to the methods of Tierney et al., which also may introduce bias into the results and inappropriate conclusions. We therefore used the RR and the HR as the effect measures to analyze relapses in WT in order to check whether the conclusions were sensitive to different effect measures. It was found that there was still a significant association between LOH 16q and WT relapse when using the HR, and that there was no significant heterogeneity among the included studies. Interestingly, the sample size of 10 included studies involving 3385 cases was imbalanced, since the study of Grundy et al. [19] involved 1724 cases and the weight of this study reached 45.5% and 52.4% (Figures 2 and 3), which imply this study of Grundy et al. may have a greater impact on the results of this meta-analysis. However, the conclusions did not change when we conducted a sensitivity analysis that involved the exclusion of individual studies, even when the study excluded was that of Grundy et al. [19]. In addition, no publication bias was detected by funnel plot and Begg’s and Egger’s tests in our study. These results, no significant heterogeneity among studies and publication bias and the results of sensitivity analysis, mean the meta-analysis are stable and credible.
The mechanism by which LOH 16q increases the recurrence risk in WT may involve the effects of LOH 16q on certain tumor-associated genes such as E2F4, COX4 [25], and CTCF [26, 27]. It is well known that gene distributions vary with race. The 10 studies included in the present analysis were mainly from Europe and North America, and although there are racial variations in these areas, the dominant race is Caucasian. A study that included 206 cases from North America [16] found the frequencies of LOH 16q to be 10%, 19%, 24%, 13%, and 14% in WT of stages I, II, III, IV, and V, respectively. In contrast, the frequencies of LOH 16q were 8%, 20%, 57%, and 0% in WT of stages I, II, III, and IV, respectively, in a study including 30 cases from China [28]. We supposed that factors such as race and tumor stage may affect the distribution of LOH 16q and further affect the relapse risk of WT. Unfortunately, the data available from the included studies were insufficient to perform a subgroup analyses based on race or tumor stage. Moreover, information regarding subclasses including bilateral⁄unilateral and age could not be extracted for most of the included studies to carry out more detailed subgroup analysis. These factors represent limitations of the present meta-analysis, and so future studies need to further explore the significance of LOH 16q in WT replase in various subgroups. Two studies mentioned favorable-histology WT and a subgroup analysis was performed based on the factor. Although subgroup analysis indicated that LOH 16q was more effective on increasing replase risk in patients with favorable-histology WT, further work are needed to confirm this duo to few studies and small sample sizes.
In summary, we have found that LOH 16q increased the relapse risk in WT. The high statistical power of this study has provided more precise and reliable estimates than those reported previously. This information will be helpful when applying early preventive measures in clinical settings according to the existence of LOH 16q. However, more studies are recommended for further assessing the role of LOH 16q in increasing the relapse risk among different subgroups of WT and for identifying the underlying mechanisms.
MATERIALS AND METHODS
Search strategy and selection criteria
We searched PUBMED, EMBASE, and the Cochrane Library in accordance with the PRISMA statement up to March 17, 2017 [29] using the following search terms: (Wilms’ tumor OR renal embryoma OR nephroblastoma) AND (16q OR loss of heterozygosity in 16q OR LOH of 16q). The studies were selected based on the following criteria: (1) cohort studies involving patients with WT, (2) the exposure of interest was LOH 16q, (3) the outcome of interest was relapse, and (4) reporting total numbers and replase numbers of LOH 16q cases and controls (non-LOH 16q) or the natural logarithm of HR (lnHR) and its standard error, or other data sufficient to calculate them. Studies with overlapping data, reviews, nonclinical studies, case observations, and letters were excluded from the present analysis.
Data extraction
Two reviewers independently screened the titles and Abstracts of all studies identified by applying the search strategy and assessed these studies using predetermined selection criteria. The full texts of all potentially relevant studies were retrieved for detailed review, and disagreements were resolved by consensus with the third reviewer. Two reviewers used a predefined data collection form to independently extract the following data from each included study: name of first author, year of publication, country, characteristics of patients, age, duration of follow-up, method to detect LOH 16q, total numbers and replase numbers of LOH 16q cases and controls, and lnHR and its standard error. If the lnHR and its standard error were not reported, they were estimated according to the methods of Tierney et al. [23].
Quality assessment
The quality assessment of each study was assessed based on the NOS about cohort studies [30]. Two reviewers independently performed a methodological quality assessment, and disagreements were resolved by the third reviewer. The included studies were evaluated based on the aspects of selection (4 points), comparability (2 points), and outcomes (3 points), with total scores of 0–3, 4–6, and 7–9 points indicating low, moderate, and high quality, respectively. Average score was presented as mean ± standard deviation.
Statistical analysis
Statistical analysis was performed using Cochrane RevMan 5.1 software. Categorical variables were compared using the RR and HR, and 95% CI values were calculated. The I2 test and Cochran’s Q-test were applied to estimate the heterogeneity among the studies. The heterogeneity was considered to be significant if the P value of the Q-test was < 0.05 or I2 was ≥ 0%. Data with significant heterogeneity were studied using a random-effects model, while a fixed-effects model was applied to other data. Funnel plot and Begg’s test [31] and Egger’s test [32] were used to assess publication bias. A P < 0.05 was considered to be indicative of statistical significance. A sensitivity analysis was performed to test the stability of the results by omitting one study in each turn.
ACKNOWLEDGMENTS AND FUNDING
This study was supported by the National Social Science Foundation of China (No. 16BGL183), the Natural Science Foundation of Shaanxi Province (No. 2015JM8415), the Fundamental Research Funds for the Central Universities of China (No. 2011jdhz55), and the Clinical Research Award of the First Affiliated Hospital of Xi’an Jiaotong University, China (No. XJTU1AF-CRF-2016-021).
CONFLICTS OF INTEREST
The authors declare that there is no conflicts of interests regarding the publication of this paper.
REFERENCES
1. Breslow N, Olshan A, Beckwith JB, Green DM. Epidemiology of Wilms tumor. Med Pediatr Oncol. 1993; 21:172–81.
2. Grosfeld JL. Risk-based management: current concepts of treating malignant solid tumors of childhood. J Am Coll Surg. 1999; 189:407–25.
3. Pritchard-Jones K, Moroz V, Vujanic G, Powis M, Walker J, Messahel B, Hobson R, Levitt G, Kelsey A, Mitchell C. Treatment and outcome of Wilms’ tumour patients: an analysis of all cases registered in the UKW3 trial. Ann Oncol. 2012; 23:2457–63.
4. Kalapurakal JA, Dome JS, Perlman EJ, Malogolowkin M, Haase GM, Grundy P, Coppes MJ. Management of Wilms’ tumour: current practice and future goals. Lancet Oncol. 2004; 5:37–46.
5. Fawzy M, Bahanassy A, Samir A, Hafez H. Profiling Loss of Heterozygosity Patterns in a Cohort of Favorable Histology Nephroblastoma Egyptian Patients: What is Consistent With the Rest of the World. Pediatr Hematol Oncol. 2015; 32:548–56.
6. Sana M, Malik HJ. Current and emerging breast cancer biomarkers. J Cancer Res Ther. 2015; 11:508–13.
7. Kluth M, Runte F, Barow P, Omari J, Abdelaziz ZM, Paustian L, Steurer S, Christina Tsourlakis M, Fisch M, Graefen M, Tennstedt P, Huland H, Michl U, et al. Concurrent deletion of 16q23 and PTEN is an independent prognostic feature in prostate cancer. Int J Cancer. 2015; 137:2354–63.
8. Cheung PF, Yip CW, Ng LW, Lo KW, Wong N, Choy KW, Chow C, Chan KF, Cheung TT, Poon RT, Fan ST, Cheung ST. Establishment and characterization of a novel primary hepatocellular carcinoma cell line with metastatic ability in vivo. Cancer Cell Int. 2014; 14:103.
9. Grundy RG, Pritchard J, Scambler P, Cowell JK. Loss of heterozygosity on chromosome 16 in sporadic Wilms’ tumour. Br J Cancer. 1998; 78:1181–7.
10. Skotnicka-Klonowicz G, Rieske P, Bartkowiak J, Szymik-Kantorowicz S, Daszkiewicz P, Debiec-Rychter M. 16q heterozygosity loss in Wilms’ tumour in children and its clinical importance. Eur J Surg Oncol. 2000; 26:61–6.
11. Messahel B, Williams R, Ridolfi A, A’Hern R, Warren W, Tinworth L, Hobson R, Al-Saadi R, Whyman G, Brundler MA, Kelsey A, Sebire N, Jones C, et al. Allele loss at 16q defines poorer prognosis Wilms tumour irrespective of treatment approach in the UKW1-3 clinical trials: a Children’s Cancer and Leukaemia Group (CCLG) Study. Eur J Cancer. 2009; 45:819–26.
12. Bown N, Cotterill SJ, Roberts P, Griffiths M, Larkins S, Hibbert S, Middleton H, Kelsey A, Tritton D, Mitchell C. Cytogenetic abnormalities and clinical outcome in Wilms tumor: a study by the U.K. cancer cytogenetics group and the U.K. Children’s Cancer Study Group. Med Pediatr Oncol. 2002; 38:11–21.
13. Spreafico F, Gamba B, Mariani L, Collini P, D’Angelo P, Pession A, Di Cataldo A, Indolfi P, Nantron M, Terenziani M, Morosi C, Radice P, Perotti D. Loss of heterozygosity analysis at different chromosome regions in Wilms tumor confirms 1p allelic loss as a marker of worse prognosis: a study from the Italian Association of Pediatric Hematology and Oncology. J Urol. 2013; 189:260–6.
14. Chagtai T, Zill C, Dainese L, Wegert J, Savola S, Popov S, Mifsud W, Vujanic G, Sebire N, Le Bouc Y, Ambros PF, Kager L, O’Sullivan MJ, et al. Gain of 1q As a Prognostic Biomarker in Wilms Tumors (WTs) Treated With Preoperative Chemotherapy in the International Society of Paediatric Oncology (SIOP) WT 2001 Trial: A SIOP Renal Tumours Biology Consortium Study. J Clin Oncol. 2016; 34:3195–203.
15. Fernandez CV, Perlman EJ, Mullen EA, Chi YY, Hamilton TE, Gow KW, Ferrer FA, Barnhart DC, Ehrlich PF, Khanna G, Kalapurakal JA, Bocking T, Huff V, et al. Clinical Outcome and Biological Predictors of Relapse After Nephrectomy Only for Very Low-risk Wilms Tumor: A Report From Children’s Oncology Group AREN0532. Ann Surg. 2017; 265:835–40.
16. Grundy PE, Telzerow PE, Breslow N, Moksness J, Huff V, Paterson MC. Loss of heterozygosity for chromosomes 16q and 1p in Wilms’ tumors predicts an adverse outcome. Cancer Res. 1994; 54:2331–3.
17. Klamt B, Schulze M, Thate C, Mares J, Goetz P, Kodet R, Scheulen W, Weirich A, Graf N, Gessler M. Allele loss in Wilms tumors of chromosome arms 11q, 16q, and 22q correlate with clinicopathological parameters. Genes Chromosomes Cancer. 1998; 22:287–94.
18. Kullendorff CM, Soller M, Wiebe T, Mertens F. Cytogenetic findings and clinical course in a consecutive series of Wilms tumors. Cancer Genet Cytogenet. 2003; 140:82–7.
19. Grundy PE, Breslow NE, Li S, Perlman E, Beckwith JB, Ritchey ML, Shamberger RC, Haase GM, D’Angio GJ, Donaldson M, Coppes MJ, Malogolowkin M, Shearer P, et al. Loss of heterozygosity for chromosomes 1p and 16q is an adverse prognostic factor in favorable-histology Wilms tumor: a report from the National Wilms Tumor Study Group. J Clin Oncol. 2005; 23:7312–21.
20. Deng C, Dai R, Li X, Liu F. Genetic variation frequencies in Wilms’ tumor: A meta-analysis and systematic review. Cancer Sci. 2016; 107:690–9.
21. Wittmann S, Zirn B, Alkassar M, Ambros P, Graf N, Gessler M. Loss of 11q and 16q in Wilms tumors is associated with anaplasia, tumor recurrence, and poor prognosis. Genes Chromosomes Cancer. 2007; 46:163–70.
22. Dome JS, Perlman EJ, Graf N. Risk stratification for wilms tumor: current approach and future directions. Am Soc Clin Oncol Educ Book. 2014: 215–23.
23. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007; 8:16.
24. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998; 17:2815–34.
25. Wen JG, van Steenbrugge GJ, Egeler RM, Nijman RM. Progress of fundamental research in Wilms’ tumor. Urol Res. 1997; 25:223–30.
26. Mummert SK, Lobanenkov VA, Feinberg AP. Association of chromosome arm 16q loss with loss of imprinting of insulin-like growth factor-II in Wilms tumor. Genes Chromosomes Cancer. 2005; 43:155–61.
27. Maschietto M, Charlton J, Perotti D, Radice P, Geller JI, Pritchard-Jones K, Weeks M. The IGF signalling pathway in Wilms tumours—a report from the ENCCA Renal Tumours Biology-driven drug development workshop. Oncotarget. 2014; 5:8014–26. http://doi.org/10.18632/oncotarget.2485.
28. Zhang L, Gao JC, Chen L, Shen YZ, Luo JM. Loss of 16q heterozygosity in Wilms’ tumor and its clinical importance. Chin J Pediatr Surg. 2002; 23:202–4.
29. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009; 6:e1000100.
30. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. (accessed 12 Jul 2017).
31. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994; 50:1088–101.
32. Egger M, Davey SG, Schneider M, Minder C. Bias in metaanalysis detected by a simple, graphical test. BMJ. 1997; 315:629–34.