
INTRODUCTION
Pneumocystis carinii pneumonia (PCP) is widely known as an opportunistic infection in patients with acquired immune deficiency syndrome (AIDS). In recent years, the incidence of PCP in AIDS patients is greatly reduced as the introduction of chemoprophylaxis and highly active antiretroviral therapy [1, 2]. However, PCP in human immunodeficiency virus (HIV)-negative patients increased as the number of patients receiving antitumor chemotherapeutic agents, immunosuppressive therapy, and organ transplantation is growing [1]. Moreover, improved diagnostic procedures may also help to increased detection of non- HIV PCP.
In non-HIV infected patients, PCP tends to follow an acute course, and the reported mortality rate range from 19.6 to 52.9% [3–5], which is significantly higher than the mortality for HIV patients with PCP [1, 6, 7]. Several studies have analyzed clinical manifestations of PCP in patients without AIDS [1, 8–10], and others have tried to determine risk factors associated with mortality for PCP in non-HIV patients [11–13]. However, the sample sizes were relatively modest, and the results were inconsistent. This prompts us to conduct a meta-analysis of published articles in order to determine the underlying diseases or conditions associated with PCP and to indentify risk factors associated with mortality in this population.
RESULTS
Study selection
We initially identified 536 articles, of which 513 remained after removing duplicates (Figure 1). A total of 345 articles were excluded as they were irrelevant to the purpose of our meta-analysis, and a further 119 articles were removed after reviewed the abstracts. Therefore, 49 articles were selected for full-text evaluation and 12 met inclusion criteria. We also searched the reference lists of the 12 articles, and a further one study was identified. A total of 13 articles were included in the review.
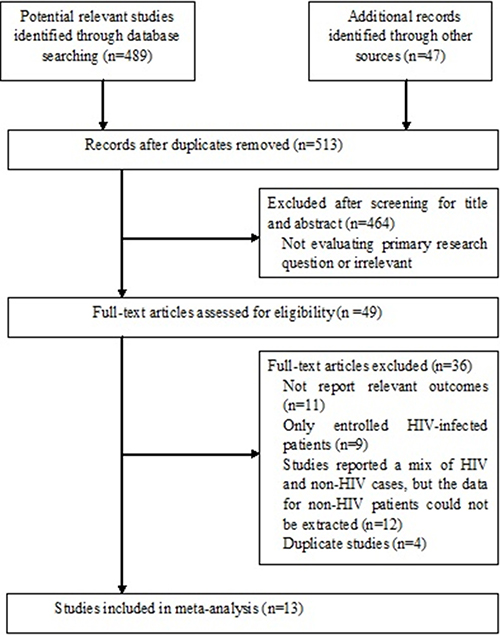
Figure 1: Flow diagram of search strategy and study selection.
Characteristics of included studies
Baseline characteristics of the 13 studies were shown in Table 1. These studies were from a variety of countries, including 4 from Japan [14–17], 2 from France [9, 18], 2 from Korea [13, 19], and one from each of China [8], Greece [10], US [1], Israel [11], and Taiwan [12]. The sample size of these studies varied from 20 to 173, and the mean age of the patients ranged from 39 to 71 years.
Table 1: Characteristics of selected studies
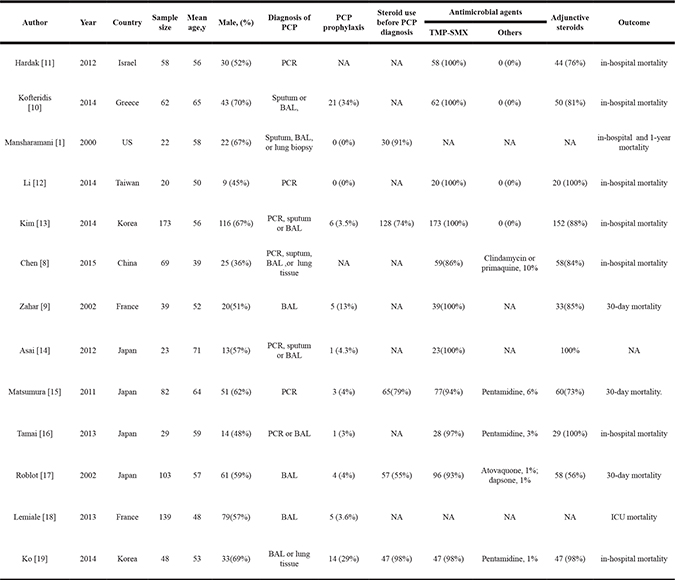
PCP, pneumocystis carinii pneumonia; PCR, polymerase chain reaction; NA, not available; BAL, bronchoalveolar lavage; TMP-SMZ trimethoprim sulphamethoxazole. ICU, Intensive Care Unit; TMP-SMX, Trimethoprim/sulfamethoxazole.
There were some variations in the techniques for diagnosis of PCP. The diagnosis of PCP was based on the microbiological identification of pneumocystis carinii in suptum, BAL fluid or lung biopsy specimens in 6 studies [1, 9, 10, 17–19]. The diagnosis of PCP in 4 studies (all after 2011) was made on basis of a positive polymerase chain reaction (PCR) result from a sputum or BAL fluid sample or positive microbiological test [8, 13, 14, 16], and 3 studies only using PCR assay for PCP diagnosis [11, 12, 15] (Table 1).
As first-line treatment, the majority of the patients in the included studies received trimethoprim-sulfamethoxazole (TMP-SMZ) (ranged from 72 to 100%), and other anti-PCP drugs used including pentamidine, atovaquone, dapsone, and clindamycin. The reported proportion of patients received adjunctive corticosteroids range from 56% to100% (Table 1).
Table 2 summarizes the underlying immunosuppressive conditions in patients who suffered from PCP. A total of 252 patients (29.1%) suffered hematological malignancies, 174 (20.1%) had autoimmune disease /chronic inflammatory disease, 52 (6.0%) with solid tumor, and 121 (14.0%) patients receiving organ or bone marrow transplantations. Regarding the type of immunosuppressive treatment, 152 (17.5%) patients were treated with chemotherapy, 188 (21.7%) had received chemotherapy and steroids and 144 (16.6%) had received corticosteroids only.
Table 2: The underlying immunosuppressive conditions in HIV-negative patients with PCP
Condition |
No of patients (%) |
Proportion (%) |
|---|---|---|
Hematological malignancies, n (%) |
252 |
29.1 |
Acute myeloblastic leukaemia |
37 |
4.3 |
Acute lympoblastic leukaemia |
25 |
2.9 |
Chronic lympocytic leukaemia |
40 |
4.6 |
Chronic myeloblastic leukaemia |
7 |
0.81 |
Lymphoma |
98 |
11.3 |
Multiple myeloma |
19 |
2.2 |
Others |
26 |
3.0 |
Solid tumors |
52 |
6.0 |
Lung cancer |
29 |
3.3 |
Breast cancer |
11 |
1.3 |
Stomach cancer |
1 |
0.12 |
Colon cancer |
5 |
0.58 |
Cervical cancer |
1 |
0.12 |
Others |
5 |
0.58 |
Autoimmune disease/ chronic inflammatory disease, n (%) |
174 |
20.1 |
Systemic lupus erythematosus |
51 |
5.9 |
Wegener’s granulomatosis |
1 |
0.12 |
Reumatoid arthritis |
53 |
6.1 |
Sarcoidosis |
3 |
0.35 |
dermatomyositis |
20 |
2.3 |
Chronic kidney disease |
0 |
0 |
Autoimmune hepatitis |
2 |
0.23 |
Others |
43 |
5.0 |
Organ or bone marrow Transplantation |
121 |
14.0 |
Type of immunosuppressive treatment |
484 |
55.8 |
Chemotherapy alone |
152 |
17.5 |
Steroids + chemotherapy |
188 |
21.7 |
Steroids |
144 |
16.6 |
The synthesis of the main results for the 23 potential risk factors was showed in Table 3. Among the 23 factors included in this study, 13 factors were significantly associated with increased odds of death from PCP, whereas 2 factors were significantly associated with decreased risk of mortality.
Table 3: Synthesis of the main results from this systematic review
Category of risk factor |
Risk factors |
Comparisons |
No of studies included in the meta-analysis |
No of patient include in the meta-analysis |
Pooled OR/WMD (95% CI) |
P |
I2(%) |
|---|---|---|---|---|---|---|---|
Demographic factors |
Age |
Age (years) mean ± SD |
9 |
657 |
6.33 (3.45–9.21) |
< 0.0001 |
0 |
Gender |
Female vs Male |
11 |
1531 |
1.43 (1.12–1.83) |
0.004 |
0 |
|
Respiratory failure |
Yes vs No |
4 |
203 |
6.16 (2.57–14.77) |
< 0.0001 |
0 |
|
ICU admission |
Yes vs No |
2 |
82 |
4.85 (1.28–18.38) |
0.02 |
0 |
|
Smoker |
Yes vs No |
3 |
1066 |
0.97 (0.69–1.38) |
0.88 |
0 |
|
Time from onset of symptoms to diagnosis |
Time (days), mean ± SD |
4 |
16 |
3.53 (0.73–6.33) |
0.01 |
0 |
|
Underlying diseases |
Haematological malignancy |
Yes vs No |
7 |
541 |
0.64 (0.44–0.92) |
0.02 |
32 |
Solid tumor |
Yes vs No |
6 |
548 |
2.66 (1.72–4.13) |
< 0.0001 |
0 |
|
Autoimmune disease |
Yes vs No |
6 |
411 |
1.07 (0.67–1.69) |
0.78 |
67 |
|
Organ transplantations |
Yes vs No |
5 |
369 |
0.38 (0.20–0.74) |
0.004 |
39 |
|
Symptom |
Fever |
Yes vs No |
4 |
1152 |
0.91 (0.63–1.33) |
0.64 |
0 |
Dyspnea |
Yes vs No |
3 |
1070 |
1.50 (1.10–2.04) |
0.01 |
0 |
|
Cough |
Yes vs No |
2 |
235 |
0.68 (0.39–1.18) |
0.17 |
0 |
|
Laboratory findings |
LDH |
LDH (U/L) mean ± SD |
9 |
754 |
151 (90–212) |
< 0.0001 |
7 |
Neutropenia (< 1500/mL) |
Yes vs No |
2 |
120 |
1.43 (0.56–3.66) |
0.45 |
0 |
|
Albumin |
Albumin g/L, mean ± SD |
6 |
463 |
-0.39 (-0.49 - -0.28) |
< 0.0001 |
52 |
|
Presence of co-infection |
Bacterium |
Yes vs No |
7 |
574 |
2.17 (1.34–3.51) |
0.002 |
25 |
Cytomegalovirus |
Yes vs No |
4 |
199 |
2.33 (1.15–4.71) |
0.02 |
40 |
|
Aspergillus |
Yes vs No |
2 |
151 |
10.45 (2.79–40.45) |
0.0007 |
0 |
|
Treatment |
PCP prophylaxis |
Yes vs No |
5 |
1196 |
0.97 (0.69–1.34) |
0.83 |
0 |
Adjunctive steroids |
Yes vs No |
6 |
445 |
1.15 (0.72–1.82) |
0.55 |
0 |
|
Previous Corticosteroid |
Yes vs No |
3 |
254 |
1.05 (0.54–2.03) |
0.88 |
0 |
|
Mechanical ventilation |
Yes vs No |
7 |
558 |
23.46 (14.02–39.28) |
< 0.0001 |
35 |
OR, Odds Ratio; WMD, weighted mean difference; ICU, Intensive Care Unit; PCP, pneumocystis carinii pneumonia; LDH, lactate dehydrogenase.
Demographic variables
Among demographic variables at admission, five variables were significantly associated with increased risk of mortality: old age (MD 6.33 y, 95% CI 3.45 to 9.21 y, P < 0.001); female sex (OR 1.43, 95% CI 1.12 to 1.83, P = 0.004); respiratory failure (OR 6.16, 95% CI 2.57 to 14.77, P < 0.001); ICU admission (OR 4.85, 95% CI 1.28 to 18.38, P = 0.02); and time from onset of symptoms to diagnosis (MD 3.53 d, 95% CI 0.73 to 6.33 days, P = 0.01) (Table 3).
Underlying diseases
Solid tumor was found to be associated with increased risk of death from PCP (OR 2.66, 95% CI 1.72 to 4.13, P < 0.001). Haematological malignancy (OR 0.64, 95% CI 0.44 to 0.92, P = 0.02) and organ transplantations (OR 0.38, 95% CI 0.20 to 0.74, P = 0.004) were associated with significant lower odds of mortality from PCP. Autoimmune disease did not appear to increase the risk of mortality (OR 1.07, 95% CI 0.67 to 1.69, P = 0.78) (Table 3).
Symptoms
The common clinical symptoms reported in patients with PCP were fever, dyspnea and cough. Dyspnea was associated with an increased risk of death (OR 1.50, 95% CI 1.10 to 2.04, P = 0.01). Fever (OR 0.91, 95% CI 0.63 to 1.33, P = 0.64) or cough (OR 0.68, 95% CI 0.39 to 1.18, P = 0.17) was non-significantly associated with mortality risk (Table 3).
Laboratory variables
Among laboratory variables at admission, a higher lactate dehydrogenase (LDH) level (MD 151 U/L, 95% CI 90 to 212 U/L, P < 0.001), and lower serum albumin level (MD −0.39, 95% CI −0.49 to −0.28, P < 0.001) were significantly associated with mortality. Neutropenia (< 1500/mL) did not significantly influence mortality (OR 1.43, 95% CI 0.56 to 3.66, P < 0.001) (Table 3).
Presence of co-infection
Among co-infection recorded during hospitalization, a concomitant infection of bacteria (OR 2.17, 95% CI 1.34 to 3.51, P = 0.002), cytomegalovirus (OR 2.33, 95% CI 1.15 to 4.71 P = 0.02), or aspergillus infection (OR 10.45, 95% CI 2.79 to 40.75, P = 0.0007) was each significantly associated with mortality (Table 3).
Treatment variables
Five studies reported the effect of PCP prophylaxis on mortality. A total of 403 of the 1196 patients (34%) had received TMP-SMZ prophylaxis for PCP before the disease onset. Findings from the pooled analysis suggested there was no significant association between PCP prophylaxis and death (OR 0.97, 95% CI 0.69 to 1.34, P = 0.83) (Figure 2).
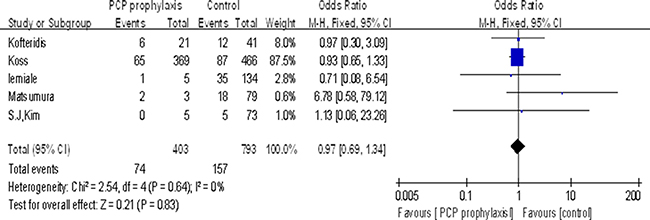
Figure 2: Association between PCP prophylaxis and mortality.
Six studies evaluated the effect of adjuvant steroids for mortality (n = 445). Adjuvant steroids were given to 315 (71%) patients. Findings from this analysis suggested adjuvant steroid therapy did not significantly influence mortality (OR 1.15, 95% CI 0.72 to 1.82, P = 0.55) (Figure 3).
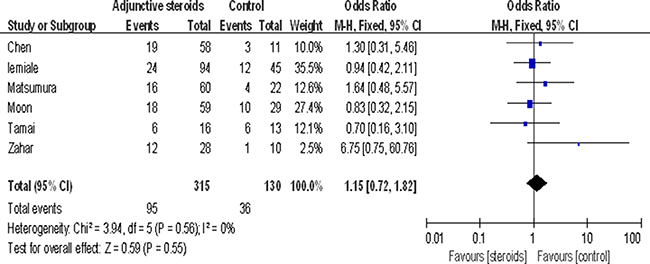
Figure 3: Association between adjuvant steroids and mortality.
The risk of mortality was also not influenced by the steroid treatment before admission (OR 1.05, 95% CI 0.54 to 2.03, P = 0.88). Use of immunosuppressive agents before the diagnosis of PCP was associated with decreased odds of death (OR 0.29, 95% CI 0.12 to 0.73, P = 0.009). Hematologic/oncology patients receiving chemotherapy (OR 4.24, 95% CI 1.81 to 9.92, P = 0.0009), and a need for mechanical ventilation (OR 23.46, 95% CI 14.02 to 39.28, P < 0.0001) were each associated with significantly increased risk of mortality (Table 3).
Risk of bias, sensitivity and subgroup analyses
Supplementary Table 1 reported the risks of bias for the included studies: 4 of the 13 studies were considered to be at high risk of bias, and lack of adjustment for confounding (statistical analysis bias) was the most frequent risk of bias.
In sensitivity analyses, we removed the 4 studies with high risk of bias. Overall, for most of the factors significantly associated with mortality, no substantial change was observed after sensitivity analyses. After removing the studies with high risk of bias, only time from onset of symptoms to diagnosis lost statistical significance (MD 3.50 d, 95% CI −5.77 to 12.77 days, P = 0.46).
In the subgroup analyses, we compared the associations between risk factors and death in subsets of studies grouped by different techniques for PCP diagnosis (PCR method or cytologic identification of pneumocystis carinii) (Supplementary Table 2). The results were not substantially changed by subgroup analysis. Gender, haematological malignancy, lower albumin level and bacterial co-infection were not significantly affect mortality in the subgroup of studies using cytologic method for diagnosis (P > 0.05) (Supplementary Table 2).
Publication bias
Funnel plots and Egger’s tests did not suggest a publication bias for the majority of the risk factors examined with the exception of autoimmune disease, albumin, or chemotherapy.
DISCUSSION
Despite the number of patients with HIV-negative PCP is increasing with widespread chemotherapy and immunosuppressive treatment, the clinical characteristics and the risk factors associated with mortality of non-HIV PCP have not been well defined. Our meta-analysis comprehensively reviewed 13 studies involving 867 patients with non-HIV related PCP which described the clinical courses, and prognosis factors in these patients. The results showed many factors including demographic, underlying diseases, symptomatic, laboratory, presence of co-infection and treatment variables were associated with increased odds for mortality. These clinical factors are easily to be monitored and measured in the primary care setting. To our knowledge, this study is the first systematic review on this topic.
All patients in our meta-analysis had an immunosuppressive condition for PCP. The pooled analysis showed the most common underlying disorder for the development of PCP is hematological malignancies (29.1%) with leukemia (12.6%) or lymphomas (11.3%), followed by autoimmune disease (20.1%) (particularly systemic lupus erythematosus and reumatoid arthritis), organ or bone marrow transplantation (14.0%), and solid tumors (6.0%). The variety of diseases observed suggested that PCP should be suspected in many immunocompromised patients and that special stainings or PCR assays for the detection of pneumocystis DNA should be considerated for diagnosis. The majority of the study population had a history of receiving immunosuppressive treatment (eg, steroids or steroids in combination with anti-malignancy chemotherapy). However, it should be note that 18% of the patients in this study were receiving only chemotherapy, when PCP occurred. This finding is in accordance with previous studies examining PCP in cancer patients and may indicate that chemotherapy or even malignancy only can increase the PCP risk [20, 21].
Our results are consistent with previous data for HIV-positive patients that mortality was influenced by respiratory failure, high lactate dehydrogenase, low serum albumin, concomitant bacterial infection, and a need for mechanical ventilation [4, 6, 7, 22–24]. Many other findings in this meta-analysis were novel and deserve further discussion.
Among demographic variables, old age, female sex, longer time from onset of symptoms to diagnosis was associated with significant increased risk of mortality. Previous study showed the duration between admission and the initialization of PCP treatment was longer in the non-HIV infected group than HIV-infected group [12]. Such a delay in treatment is likely to be related to the delay in the diagnosis of PCP, for which the clinical manifestations and radiologic abnormalities are nonspecific. Improved diagnostic procedures aiming to reduce the delay between symptoms onset and the diagnosis in HIV-negative patients would be important.
Solid tumor was one of the comorbidities associated with increased risk of death from PCP. This result is consistent with a recent study reporting prognosis seems to be worse in patients with solid tumors [9]. In this study, we also found that co-infection, most notably with aspergillosis, was associated with higher mortality. Non-HIV immunocompromised patients are more vulnerable to aspergillosis infection [25], it is possibly because both PCP and aspergillosis develop with the use of immunosuppressive agents [17, 25].
Despite the presence of multiple major risk factors, PCP prophylaxis was not generally implemented for immunocompromised non-HIV patients. Our review showed that 10.4% (34/327) of HIV-negative patients with PCP were on PCP prophylaxis before the onset of disease. Although no significant differences were observed in mortality in the present study between patients with and without TMP-SMX prophylaxis, a previous systematic meta-analysis including 1245 patients who had undergone bone marrow or solid organ transplant or with hematologic cancer showed that there was a 91% reduction in the occurrence of PCP in non-HIV patients who received prophylaxis [26]. In an observational study, it was suggested that PCP prophylaxis should be given to all solid organ transplant recipients for at least 1 year [27]. Indeed, PCP prophylaxis is recommended for all organ transplant recipients for at least 6–12 months post transplantation [28]. However, limited data are available for the efficiency of PCP prophylaxis in solid tumors and immunosuppressed patients with rheumatic diseases. It has been reported that, PCP was most likely to occur during the reduction or withdrawal of chemotherapy or even during clinical remission [3]. Other study showed patients with uncontrolled tumor growth were candidates to develop PCP [9]. Further well-designed prospective research should be undertaken to define the type of solid tumor patients who may benefit from PCP prophylaxis.
For HIV-infected patients with PCP, many studies showed that adjunctive corticosteroid treatment prevented early deterioration [29], and reduced the occurance of respiratory failure and mortality rate [30, 31]. Based on these data, adjunctive corticosteroid is recommended to AIDS patients with PCP, if PaO2 is ≤ 70 mmHg or AaDO2 is ≥ 35 mmHg [32]. However, there is no proof that HIV-negative patients might benefit from adjunctive corticosteroid. Two previous studies analyzed the effect of corticosteroid on non-HIV patients with severe PCP (defined by an PaO2 < 70 mm Hg), which results suggested adjunctive steroid therapy possibly accelerated recovery but failed to reduce the rates of endotracheal mechanical ventilation and in-hospital mortality [33, 34].
Similarly, our pooled analyses of 6 articles support the results of previous studies that adjunctive corticosteroid treatment may not improve the prognosis of PCP in non-HIV patients [33, 34]. However, it should be noted that the non-HIV-immunocompromised patients were not a homogeneous group, and most of them were on corticosteroid treatment at the time they developed PCP. The data on steroid treatment, comorbidity and disease severity can be confounded. More research is needed in this area to better understand how adjunctive corticosteroid influencing the mortality of HIV-negative PCP patients in different settings.
In our study, the pooled overall mortality for non-HIV patients with PCP was 30.6%, which was significantly higher than previously reported mortality rate in HIV-positive patients. The present data confirms the results of previous studies that HIV-negative patients with PCP have different prognosis from the HIV-positive ones [7, 13, 24]. There are several possible explanations for the poorer outcomes in non-HIV PCP. HIV-negative patients were older and had more underlying cardiopulmonary disease than HIV-positive patients. The duration of symptoms onset to the beginning of PCP treatment was much longer in HIV-negative patients. Moreover, AIDS patients with PCP were benefited from adjunctive steroid therapy, but there is no proof that adjunctive corticosteroid is beneficial to HIV-negative patients. This suggests that non-HIV PCP may not benefited from the advances in the management of PCP.
Although we believed that the current study provided useful information, some potential limitations should be noted. Firstly, many studies differed in their study population, era, methods of diagnosis of PCP, and follow-up. The method for PCP diagnosis is a major cause of heterogeneity. When compared with traditional cytological stains, PCR detection of pneumocystis carinii DNA provides greater sensitivity, but carries the risk of false-positive diagnosis of PCP in patients who are not infected, but colonized, with pneumocystis carinii [35]. Colonization with pneumocystis carinii refer to when a patient did not have specific symptoms or history of PCP, and showed a positive nested-PCR result indicating presence of pneumocystis carinii DNA in his or her respiratory secretions [35]. Pneumocystis carinii colonization often occurs in patients with underlying pulmonary diseases and mild immunosuppression [36]. The colonized patients differed from the PCP infected patients, since they presented with lower quantitative PCR assay value [37]. Moreover, recent data demonstrated that the (1,3) ß-D-glucan (BDG) level in bronchoalveolar lavage (BAL) sample from the PCP patients was significantly higher than the colonized patients [38]. For ambiguous PCR results, BDG could be used as a preliminary test for patients with suspected PCP, especially in patients with slightly positive PCR results [39]. Last, most of the studies presented only unadjusted estimates, it was not possible to stratify or adjust for potential confounders in this meta-analysis, which restricted us to obtain more comprehensive results and do further detailed analysis.
In summary, our study suggests all immunocompromised non-HIV patients with symptoms of pulmonary infection should be carefully evaluated for PCP, and the mortality rate is still high in non-HIV infected patients with PCP. Risk factors associated with poor prognosis including old age, female sex, longer time from onset of symptoms to diagnosis, respiratory failure, solid tumors, high LDH, low serum albumin, concomitant infection, etc. The identification of high risk non-HIV patients with PCP has great clinical relevance with respect to patients counsel, and guides the early treatment. Limited data are available for the efficiency of PCP prophylaxis in solid tumors and patients with rheumatic diseases. Further studies evaluate the role of PCP prophylaxis and adjunctive corticosteroid in immunocompromised patients PCP with should be advocated.
MATERIALS AND METHODS
This systematic review and meta-analysis was conducted following the PRISMA statement [40].
Search strategy
We conducted a systematic search of PubMed, Embase, and Scopus Database for articles published until Dec 2016. The text keywords used in searching included: “Pneumocystis Infections ” or “pneumocystis” or “carinii” or “jiroveci” or “PCP ” or “PJP ” combined with “outcome ” or “mortality”’. No language restriction was applied. From the title or abstract, the literature search was reviewed by 2 authors (YL and SJJ) independently to identify potentially relevant studies for full text review. The “related articles” function was used to broaden the search. Moreover, a manual search of references from related articles was performed to identify additional relevant studies.
Study selection
Original articles were considered to be eligible if they investigated the predisposing factors, clinical characteristics and reported mortality data of PCP in HIV-negative patients. Studies restricted to HIV-infected participants or children patients were excluded. Letters, meeting proceedings, and abstracts were also excluded. Studies which reported a mix of HIV and non-HIV infected cases were also included if sufficient data were provided to extract non-HIV infected patients meeting the inclusion criteria. After obtained the full text of candidate studies, the two authors (YL and SJJ) independently assessed eligibility. Disagreements were resolved by reviewing corresponding articles.
Data extraction
Two authors (YL and SJJ) extracted data from included studies. Differences between the two authors were solved by discussion between the two authors and consensus with a third author (LLS). We extracted the following information: first author’s last name, publication year, study design, study population, sample size, methods for PCP diagnosis, potential factors associated with mortality including demographical details, underlying diseases, clinical characteristics, laboratory results, treatment variables and et al.
Statistical analyses
The statistical analyses were performed with Stata (version 12.0; Stata Corporation, College Station, TX, USA) and Revman (version 5.2; Cochrane Collaboration, Oxford, United Kingdom). When meta-analysis was possible, for each risk factor we generated a pooled OR or mean difference (MD) using the inverse-variance weighting method. If both of the univariate and multivariate regression results were reported, we used estimates from the multivariate regression model. As we expected high heterogeneity in the subjects, the diagnosis of PCP, the definition of risk factors, we selected a priori the DerSimonian and Laird random effect model. We tested for heterogeneity with the Cochrane Q test and measured degree of heterogeneity across studies using the I-squared (I2) statistic. The degree of heterogeneity between studies was assessed by I2 statistic with its 95% confidence intervals. Heterogeneity was considered low for I2 values between 25%–50%, moderate for 50%–75%, and high for 75% [41].
The method for PCP diagnosis may be an important source of heterogeneity. In order to analyze the heterogeneity, subgroup analyses were performed by comparing summary results obtained from subsets of studies grouped by different diagnosis methods (PCR method or cytologic identification of pneumocystis organisms). If at least two studies for each subgroup were available, subgroup analyses were performed. We also performed sensitivity analyses were to examine the effect of the risk factors after removing the studies with high risk of bias. We investigated the presence of publication bias by means of funnel plots and Egger’s test.
Author contributions
Y.L. and H.Q. conceived and designed the study; S.-J.J. L.L.S and Y.L. collected the data; L.L.S. and H.Q. analyzed the data; S.-J.J., and L.L.S. contributed analysis tools; Y.L. and H.Q. wrote and revised the manuscript. All authors reviewed and approved the manuscript prior to submission.
CONFLICTS OF INTEREST
The authors declare no competing financial interests.
FUNDING
Financial Support: This work was supported by Key Research & Development Program of Shandong Province (2016GSF202036), and Natural Science Foundation of Shandong Province (ZR2014HQ044).
REFERENCES
1. Mansharamani NG, Garland R, Delaney D, Koziel H. Management and outcome patterns for adult Pneumocystis carinii pneumonia, 1985 to 1995: comparison of HIV-associated cases to other immunocompromised states. Chest. 2000; 118:704–11.
2. Kelley CF, Checkley W, Mannino DM, Franco-Paredes C, Del Rio C, Holguin F. Trends in hospitalizations for AIDS-associated Pneumocystis jirovecii Pneumonia in the United States (1986 to 2005). Chest. 2009; 136:190–197.
3. Roblot F, Le Moal G, Godet C, Hutin P, Texereau M, Boyer E, Prazuck T, Lacroix C, Souala MF, Raffi F, Weinbreck P, Besnier JM, Garo B, et al. Pneumocystis carinii pneumonia in patients with hematologic malignancies: a descriptive study. J Infect. 2003; 47:19–27.
4. Enomoto T, Azuma A, Kohno A, Kaneko K, Saito H, Kametaka M, Usuki J, Gemma A, Kudoh S, Nakamura S. Differences in the clinical characteristics of Pneumocystis jirovecii pneumonia in immunocompromised patients with and without HIV infection. Respirology. 2010; 15:126–131.
5. Pagano L, Fianchi L, Mele L, Girmenia C, Offidani M, Ricci P, Mitra ME, Picardi M, Caramatti C, Piccaluga P, Nosari A, Buelli M, Allione B, et al. Pneumocystis carinii pneumonia in patients with malignant haematological diseases: 10 years’ experience of infection in GIMEMA centers. Br J Haematol. 2002; 117:379–386.
6. Walzer PD, Evans HE, Copas AJ, Edwards SG, Grant AD, Miller RF. Early predictors of mortality from pneumocystis jirovecii pneumonia in HIV-infected patients: 1985–2006. Clin Infect Dis. 2008; 46:625–633.
7. Limper AH, Offord KP, Smith TF, Martin WJ. Pneumocystis carinii pneumonia: differences in lung parasite number and inflammation in patients with and without AIDS. Am Rev Respir Dis. 1989; 140:1204–1209.
8. Chen M, Tian X, Qin F, Zhou J, Liu J, Wang M, Xu KF. Pneumocystis pneumonia in patients with autoimmune diseases: a retrospective study focused on clinical characteristics and prognostic factors related to death. PLoS One. 2015; 10:e0139144.
9. Zahar JR, Robin M, Azoulay E, Fieux F, Nitenberg G, Schlemmer B. Pneumocystis carinii pneumonia in critically ill patients with malignancy: a descriptive study. Clin Infect Dis. 2002; 35:929–934.
10. KIofteridis DP, Valachis A, Velegraki M, Antoniou M, Christofaki M, Vrentzos GE, Andrianaki AM, Samonis G. Predisposing factors, clinical characteristics and outcome of Pneumonocystis jirovecii pneumonia in HIV-negative patients. J Infect Chemother. 2014; 20:412–416.
11. Hardak E, Neuberger A, Yigla M, Berger G, Finkelstein R, Sprecher H, Oren I. Outcome of Pneumocystis jirovecii pneumonia diagnosed by polymerase chain reaction inpatients without human immunodeficiency virus infection. Respirology. 2012; 17:681–686.
12. Li MC, Lee NY, Lee CC, Lee HC, Chang CM, Ko WC. Pneumocystis jiroveci pneumonia in immunocompromised patients: delayed diagnosis and poor outcomes in non-HIV-infected individuals. J Microbiol Immunol Infect. 2014; 47:42–47.
13. Kim SJ, Lee J, Cho YJ, Park YS, Lee CH, Yoon HI, Lee SM, Yim JJ, Lee JH, Yoo CG, Lee CT, Kim YW, Han SK, et al. Prognostic factors of Pneumocystis jirovecii pneumonia in patients without HIV infection. J Infect. 2014; 69:88–95.
14. Asai N, Motojima S, Ohkuni Y, Matsunuma R, Nakashima K, Iwasaki T, Nakashita T, Otsuka Y, Kaneko N. Early diagnosis and treatment are crucial for the survival of Pneumocystis pneumonia patients without human immunodeficiency virus infection. J Infect Chemother. 2012; 18:898–905.
15. Matsumura Y, Shindo Y, Iinuma Y, Yamamoto M, Shirano M, Matsushima A, Nagao M, Ito Y, Takakura S, Hasegawa Y, Ichiyama S. Clinical characteristics of Pneumocystis pneumonia in non-HIV patients and prognostic factors including microbiological genotypes. BMC Infect Dis. 2011; 11:76.
16. Tamai K, Tachikawa R, Tomii K, Nagata K, Otsuka K, Nakagawa A, Otsuka K, Matsumoto T, Monden K, Takeshita J, Tanaka K, Kawamura T, Otoshi T, et al. Prognostic value of bronchoalveolar lavage in patients with non-HIV pneumocystis pneumonia. Intern Med. 2014; 53:1113–1117.
17. Roblot F, Godet C, Le Moal G, Garo B, Faouzi Souala M, Dary M, De Gentile L, Gandji JA, Guimard Y, Lacroix C, Roblot P, Becq-Giraudon B. Analysis of underlying diseases and prognosis factors associated with Pneumocystis carinii pneumonia in immunocompromised HIV-negative patients. Eur J Clin Microbiol Infect Dis. 2002; 21:523–531.
18. Lemiale V, Debrumetz A, Delannoy A, Alberti C, Azoulay E. Adjunctive steroid in HIV-negative patients with severe Pneumocystis pneumonia. Respir Res. 2013; 14:87.
19. Ko Y, Jeong BH, Park HY, Koh WJ, Suh GY, Chung MP, Kwon OJ, Jeon K. Outcomes of Pneumocystis pneumonia with respiratory failure in HIV-negative patients. J Crit Care. 2014; 29:356–361.
20. Torres HA. Chemaly RF, Storey R, Aguilera EA, Nogueras GM, Safdar A, Rolston KV, Raad II, Kontoyiannis DP. Influence of type of cancer and hematopoietic stem cell transplantation on clinical presentation of Pneumocystis jiroveci pneumonia in cancer patients. Eur J Clin Microbiol Infect Dis. 2006; 25:382e8.
21. Ewig S, Bauer T, Schneider C, Pickenhain A, Pizzulli L, Loos U, Lüderitz B. Clinical characteristics and outcome of Pneumocystis carinii pneumonia in HIV-infected and otherwise immunosuppressed patients. Eur Respir J. 1995; 8:1548e53.
22. Wang HW, Lin CC, Kuo CF, Liu CP, Lee CM. Mortality predictors of Pneumocystis jirovecii pneumonia in human immunodeficiency virus-infected patients at presentation: Experience in a tertiary care hospital of northern Taiwan. J Microbiol Immunol Infect. 2011; 44:274–281.
23. Azoulay E, Parrot A, Flahault A, Cesari D, Lecomte I, Roux P. Saidi F, Fartoukh M, Bernaudin JF, Cadranel J, Mayaud C. AIDS-related Pneumocystis carinii pneumonia in the era of adjunctive steroids: implication of BAL neutrophilia. Am J Respir Crit Care Med. 1999; 160:493–499.
24. Armstrong-James D, Copas AJ, Walzer PD, Edwards SG, Miller RF. A prognostic scoring tool for identification of patients at high and low risk of death from HIV-associated Pneumocystis jirovecii pneumonia. Int J STD AIDS. 2011; 22:628–634.
25. Segal BH, Walsh TJ. Current approaches to diagnosis and treatment of invasive aspergillosis. Am J Respir Crit Care Med. 2006; 173:707–717.
26. Green H, Paul M, Vidal L, Leibovici L. Prophylaxis of Pneumocystis pneumonia in immunocompromised non-HIV-infected patients: systematic review and meta-analysis of randomized controlled trials. Mayo Clin Proc. 2007; 82:1052–1059.
27. Gordon SM, LaRosa SP, Kalmadi S, Arroliga AC, Avery RK, Truesdell-LaRosa L, Longworth DL. Should prophylaxis for Pneumocystis carinii pneumonia in solid organ transplant recipients ever be discontinued? Clin Infect Dis. 1999; 28:240–246.
28. Martin SI, Fishman JA, AST Infectious Diseases Community of Practice. Pneumocystis pneumonia in solid organ transplantation. Am J Transplant. 2013; 13:272–9.
29. Moon SM, Kim T, Sung H, Kim MN, Kim SH, Choi SH, Jeong JY, Woo JH, Kim YS, Lee SO. Outcomes of moderate-to-severe Pneumocystis pneumonia treated with adjunctive steroid in non-HIV-infected patients. Antimicrob Agents Chemother. 2011; 55:4613–4618.
30. Anonymous. Consensus statement on the use of corticosteroids as adjunctive therapy for pneumocystis pneumonia in the acquired immunodeficiency syndrome. The National Institutes of Health—University of California Expert Panel for Corticosteroids as Adjunctive Therapy for Pneumocystis Pneumonia. N Engl J Med. 1990; 323:1500–1504.
31. Bozzette SA, Sattler FR, Chiu J, Wu AW, Gluckstein D, Kemper C, Bartok A, Niosi J, Abramson I, Coffman J, Hughlett C, Loya R, Cassens B, et al. A controlled trial of early adjunctive treatment with corticosteroids for Pneumocystis carinii pneumonia in the AIDS. California Collaborative Treatment Group. N Engl J Med. 1990; 323:1451–1457.
32. Kaplan JE, Benson C, Holmes KK, Brooks JT, Pau A, Masur H, Centers for Disease Control and Prevention (CDC), National Institutes of Health, HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR Recommend Rep. 2009; 58:1–207.
33. Delclaux C, Zahar JR, Amraoui G, Leleu G, Lebargy F, Brochard L, Schlemmer B, Brun-Buisson C. Corticosteroids as adjunctive therapy for severe Pneumocystis carinii pneumonia in non-human immunodeficiency virus-infected patients: retrospective study of 31 patients. Clin Infect Dis. 1999; 29:670–672.
34. Moon SM, Kim T, Sung H, Kim MN, Kim SH, Choi SH, Jeong JY, Woo JH, Kim YS, Lee SO. Outcomes of moderate-to-severe Pneumocystis pneumonia treated with adjunctive steroid innon-HIV-infected patients. Antimicrob Agents Chemother. 2011; 55:4613–8.
35. Medrano FJ, Montes-Cano M, Conde M, de la Horra C, Respaldiza N, Gasch A, Perez-Lozano MJ, Varela JM, Calderon EJ. Pneumocystis jirovecii in General Population. Emerg Infect Dis. 2005; 11:245–50.
36. Khodadadi H, Mirhendi H, Mohebali M, Kordbacheh P, Zarrinfar H, Makimura K. Pneumocystis jirovecii Colonization in Non-HIV-Infected Patients Based on Nested-PCR Detection in Bronchoalveolar Lavage Samples. Iran J Public Health. 2013; 42:298–305.
37. Maillet M, Maubon D, Brion JP, François P, Molina L, Stahl JP, Epaulard O, Bosseray A, Pavese P. Pneumocystis jirovecii (Pj) quantitative PCR to differentiate Pj pneumonia from Pj colonization in immunocompromised patients. Eur J Clin Microbiol Infect Dis. 2014; 33:331–6.
38. Lahmer T, da Costa CP, Held J, Rasch S, Ehmer U, Schmid RM, Huber W. Usefulness of 1,3 Beta-D-Glucan Detection in non-HIV Immunocompromised Mechanical Ventilated Critically Ill Patients with ARDS and Suspected Pneumocystis jirovecii Pneumonia. Mycopathologia. 2017; 182:701–708.
39. Damiani C, Le Gal S, Goin N, Di Pizio P, Da Costa C, Virmaux M, Bach V, Stéphan-Blanchard E, Nevez G, Totet A. Usefulness of (1, 3) ß-D-glucan detection in bronchoalveolar lavage samples in Pneumocystis pneumonia and Pneumocystis pulmonary colonization. J Mycol Med. 2015; 25:36–43.
40. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009; 6:e1–e34.
41. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986; 7:177–188.