
INTRODUCTION
The unstable intertrochanteric femur fracture (IFFs) is a major orthopaedic challenge, and associated with high rates of complications and poor prognosis [1, 2]. Intramedullary and extramedullary fixation methods are commonly used for treating unstable IFFs [3, 4]. Currently, a variety of implants of internal fixation have been employed for unstable intertrochanteric femur fractures include proximal femoral locking compression plate (PFLCP), PFNA (proximal femoral nails anti-rotation), InterTan nail, Dynamic Hip Screw (DHS), et al [5–7]. However, the optimal management of unstable IFFs still remains controversial. Gotfried Y first emphasized the importance of lateral trochanteric wall and certainly suggested that an intact lateral trochanteric wall played a key role in the stabilization of unstable IFFs [8]. Subsequently, Palm H et al showed that a postoperative fracture of the lateral wall was closely related with a reoperation after an intertrochanteric fracture and pointed out intertrochanteric fractures should be classified according to the integrity of the lateral wall, especially in trials comparing fracture implants. Moreover, IFF with lateral wall fractures are a challenge for orthopedic surgeons. The optimal internal fixation for treating this type of unstable intertrochanteric fractures remains controversial. Thus, this study aimed to compare DHLPs with PFNA-IIs in the management of IFF with lateral wall fractures.
RESULTS
19 were male, 24 were female and the average age was 77 years old (ranging between 65 and 93). 17 patients were treated with DHLP fixation device and 26 patients were treated with PFNA-II fixation device (Figure 1a, 1b). The mean follow-up period was 11 months (ranging from 6 to16 months). Both the groups were comparable for demographic data before surgery (Table 1). The PFNA-II group had less operation time, time of full weight bearing and healing time of fracture in comparison with the DHLP group (p<0.05). Compared with the DHLP group, the PFNA-II group had larger blood loss (p<0.05). Internal fixation failure was significantly more in the DHLP group than in the PFNA-II group (Table 2). The failure type of these four failure cases were internal fixation screw loosening or withdraw. Two of four internal fixation failure in the DHLP group received delayed mobilization. The other two patients required revision. But only one finally received total hip joint replacement (Figure 2a, 2b) and one was lost during follow-up.
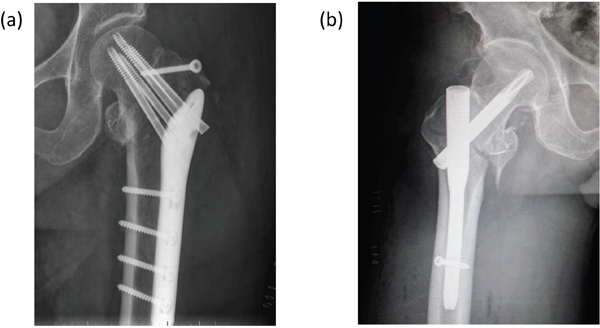
Figure 1: (a) patient treated with DHLP fixation device; (b) patient treated with PFNA-II fixation device.
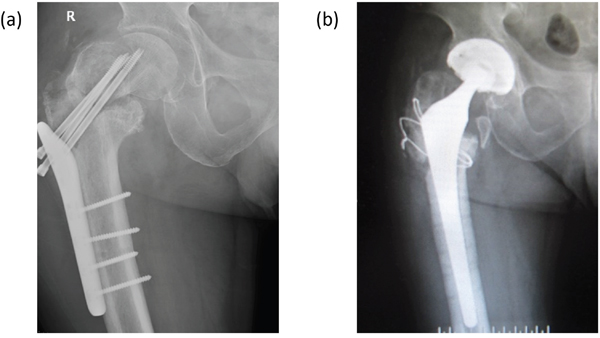
Figure 2: (a) Aggravating hip varus, withdrawal of screw, and no sign of fracture healing at nearly four months postoperatively; (b) Removal of internal fixation and total hip arthroplasty.
Table 1: Comparison of characteristics of the patients before surgery in two groups
Group |
Number |
Age(years) |
Sex (number) |
Fractured side (n) |
Time for preoperative preparation |
||
|---|---|---|---|---|---|---|---|
Male |
Female |
Left |
Right |
||||
DHLP |
17 |
75.77±7.22 |
8 |
9 |
6 |
11 |
5.41±3.57 |
PFNA-II |
26 |
77.58±6.95 |
11 |
15 |
10 |
16 |
4.50±1.21 |
P value |
0.415 |
0.76 |
0.83 |
0.702 |
|||
Table 2: Comparison of intraoperative variables and clinical results after surgery in two groups
Group |
Number |
Operation time(mins) |
Total blood loss(ml) |
Time of full weight bearing (w) |
Healing time of fracture(w) |
Internal fixation failure (n) |
Revision demand (n) |
|---|---|---|---|---|---|---|---|
DHLP |
17 |
64.19±11.30 |
525.88±56.69 |
12.88±2.00 |
14.53±2.03 |
4 |
2 |
PFNA-II |
26 |
45.35±6.81 |
711.15±63.71 |
8.04±1.34 |
11.73±1.56 |
0 |
0 |
P value |
0.00 |
0.00 |
0.00 |
0.00 |
0.02 |
0.15 |
The results of HHS after surgery were shown in (Tables 3 and 4). The mean HHS in the PFNA-II group was significantly higher than that in the DHLP group both in third month after surgery (p<0.05). Additionally, the rate of good-to-excellent in the PFNA-II group was also significantly higher than that in the DHLP group in third month after surgery (p<0.05). However, no statistically significant difference was found in the rate of good-to-excellent between two groups in sixth month after surgery (p<0.05).
Table 3: Comparison of HHS in third month after surgery between two groups
Group |
Excellent |
Good |
Fair |
Poor |
Good-to-excellent (%) |
Mean in points |
|---|---|---|---|---|---|---|
DHLP |
3 |
4 |
6 |
3 |
43.75 |
75.25±11.23 |
PFNA-II |
5 |
15 |
5 |
1 |
76.92 |
83.96±7.78 |
P value |
0.03 |
0.01 |
Table 4: Comparison of HHS in sixth month after surgery between two groups
Group |
Excellent |
Good |
Fair |
Poor |
Good-to-excellent (%) |
Mean in points |
|---|---|---|---|---|---|---|
DHLP |
3 |
7 |
4 |
2 |
62.50 |
81.94±8.08 |
PFNA-II |
5 |
16 |
4 |
1 |
80.76 |
85.19±6.49 |
P value |
0.28 |
0.16 |
DISCUSSION
Management of unstable IFFs requires stable fixation that allows early mobilization and remains a challenge to orthopaedic surgeons. Recently, lateral wall reconstruction is seen as an important component in stabilization and fixation of unstable IFFs by providing a lateral buttress for the proximal fragment. The fracture of lateral wall can lead to collapse, which is a major cause of postoperative morbidity [8]. So, intertrochanteric fractures should be classified according to the integrity of the lateral wall. The study was initiated to compare PFNA-II and DHLP for differences in outcomes of IFF with lateral wall fractures.
IFF with lateral wall fractures represent a challenge for internal fixation. Palm et al [9]thought that a sliding compression hip screw was not sufficient for treatment of fractures involving the lateral wall and more methods should be needed to manage this condition. Using sliding hip screw in fractures with broken lateral wall could result in collapse, limb length shortening and poorer functional outcome [10, 11]. Gupta RK et al showed that lateral wall reconstruction using a trochanteric stabilising plate (TSP) in combination with a dynamic hip screw (DHS) can be successful [12]. Proximal femoral nail anti-rotation (PFNA) and locking compression plate (LCP) have good effectiveness in the treatment of intertrochanteric fractures with the lateral unsubstantial femoral wall in the elderly patients. Each has its own advantages and disadvantages [7]. However, Haq RU et al found that PFN (proximal femoral nail) was a better implant than reverse-DFLCP (reverse distal femoral locking compression plate) for IFFs with compromised lateral wall because of favourable intraoperative variables, better functional outcome and lower failure rates [13]. Additionally, Hu et al [14] thought that anatomic locking plate could be used for IFF with lateral wall fractures especially for severe comminuted fractures, difficult for intramedullary nailing to avoid re-injury of lateral wall.
Currently, there is no consensus regarding which type of internal fixation is the better option for unstable IFFs especially for IFF with lateral wall fractures. In our study, the PFNA-II group had less operation time, time of full weight bearing and healing time of fracture in comparison with the DHLP group. Moreover, internal fixation failure was significantly more in the DHLP group than in the PFNA-II group. Regarding functional outcomes, the mean HHS and the rate of good-to-excellent in the PFNA-II group was significantly higher than that in the DHLP group in third month after surgery. But no significant difference was observed in the mean HHS and the rate of good-to-excellent in the sixth month between two groups. Thus, PFNA-II is a more suitable option for early rehabilitation in patients with IFF with lateral wall fractures. Additionally, compared with the DHLP group, the PFNA-II group had larger blood loss (p<0.05). So, more attention should be paid on bleeding when performing PFNA-II for IFF with lateral wall fractures. To conclude, PFNA-II is more effective than DHLP in internal fixation of IFF with lateral wall fractures and can reduce complications and improve clinical outcomes.
MATERIALS AND METHODS
Between December 2009 and March 2015, 43 elder patients of IFF with lateral wall fracture (AO/OTA type-31-A2, A3) operated at the Second Affiliated Hospital, School of Medicine, Zhejiang University, were investigated and completely followed up. These cases were performed by senior doctors in one team. DHLP fixation devices were from Tianjin Walkman Biomaterial Company Limited, China. PFNA-II fixation devices were from Trauson Medical Instrument Company Limited, China. Detailed clinical and radiological examination were performed on all patients. Demographic characteristics of the patients before surgery were compared between two groups. Fracture healing was assessed by X-ray reexamination. The function of the hip joint was assessed according to the Harris Hip Score (HHS). Out of a total of 100 points, 100 to 90 points were rated excellent; 89 to 80, good; 79 to 70, fair; and less than 70, poor [15, 16]. One patient in DHLP group did not receive further treatment after internal fixation failure. So, this patient was not included in the comparison of HHS after surgery.
The operation time, total blood loss [17], time of full weight bearing, healing time of fracture, number of internal fixation failure, number of revision and HHS in third and sixth month after surgery were compared between the two groups. The operation time refers to the duration from skin incision to skin suture (minutes).
The statistical analysis was performed using SPSS 23.0 software for all statistical analyses. Data were expressed as Mean ± SD (standard deviation). Student t test was used for quantitative variables between two groups. Categorical variables were analysed by the chi-square test where appropriate. P<0.05 was taken as significant. Under varied distributional conditions, Wilcoxon rank sum test was used for time for preoperative preparation and time of full weight bearing between two groups. Fisher exact test was used for internal fixation failure, revision and good-to-excellent between two groups.
ACKNOWLEDGMENTS
The authors would like to thank Xingzhi Zhou for discussions, Weijing Fang for editorial help, and Haiqing Lin for critically reading the manuscript.
CONFLICTS OF INTEREST
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
GRANT SUPPORT
No.
Consent
This study was approved by the local ethical. Written informed consent was obtained from the patients for publication of this study and any accompanying images.
REFERENCES
1. Ahrengart L, Tornkvist H, Fornander P, Thorngren KG, Pasanen L, Wahlstrom P, Honkonen S, Lindgren U. A randomized study of the compression hip screw and Gamma nail in 426 fractures. Clin Orthop Relat Res. 2002; 209-22.
2. Sonmez MM, Camur S, Erturer E, Ugurlar M, Kara A, Ozturk I. Strategies for proximal femoral nailing of unstable intertrochanteric fractures: lateral decubitus position or traction table. J Am Acad Orthop Surg. 2017; 25:e37-e44. https://doi.org/10.5435/JAAOS-D-15-00691.
3. Singh AK, Narsaria N, G RA, Srivastava V. Treatment of unstable trochanteric femur fractures: proximal femur nail versus proximal femur locking compression plate. Am J Orthop (Belle Mead NJ). 2017; 46:E116-23.
4. Socci AR, Casemyr NE, Leslie MP, Baumgaertner MR. Implant options for the treatment of intertrochanteric fractures of the hip: rationale, evidence, and recommendations. Bone Joint J. 2017; 99-b:128-33. https://doi.org/10.1302/0301-620X.99B1.BJJ-2016-0134.R1.
5. Ma JX, Wang J, Xu WG, Yu JT, Yang Y, Ma XL. Biomechanical outcome of proximal femoral nail antirotation is superior to proximal femoral locking compression plate for reverse oblique intertrochanteric fractures: a biomechanical study of intertrochanteric fractures. Acta Orthop Traumatol Turc. 2015; 49:426-32. https://doi.org/10.3944/AOTT.2015.14.0306.
6. Yu W, Zhang X, Zhu X, Hu J, Liu Y. A retrospective analysis of the InterTan nail and proximal femoral nail anti-rotation-Asia in the treatment of unstable intertrochanteric femur fractures in the elderly. J Orthop Surg Res. 2016; 11:10. https://doi.org/10.1186/s13018-016-0344-7.
7. Shi Y, Li F, Tan W, Liu J. Effectiveness comparison of proximal femoral nail anti-rotation and locking compression plate for intertrochanteric fractures with lateral unsubstantial femoral wall in elderly patients. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014; 28:1199-203.
8. Gotfried Y. The lateral trochanteric wall: a key element in the reconstruction of unstable pertrochanteric hip fractures. Clin Orthop Relat Res. 2004; 82-6.
9. Palm H, Jacobsen S, Sonne-Holm S, Gebuhr P. Integrity of the lateral femoral wall in intertrochanteric hip fractures: an important predictor of a reoperation. J Bone Joint Surg Am. 2007; 89:470-5. doi:10.2106/JBJS.F.00679.
10. Haidukewych GJ. Intertrochanteric fractures: ten tips to improve results. J Bone Joint Surg Am. 2009; 91:712-9.
11. Watson JT, Moed BR, Cramer KE, Karges DE. Comparison of the compression hip screw with the Medoff sliding plate for intertrochanteric fractures. Clin Orthop Relat Res. 1998; 79-86.
12. Gupta RK, Sangwan K, Kamboj P, Punia SS, Walecha P. Unstable trochanteric fractures: the role of lateral wall reconstruction. Int Orthop. 2010; 34:125-9. https://doi.org/10.1007/s00264-009-0744-y.
13. Haq RU, Manhas V, Pankaj A, Srivastava A, Dhammi IK, Jain AK. Proximal femoral nails compared with reverse distal femoral locking plates in intertrochanteric fractures with a compromised lateral wall; a randomised controlled trial. Int Orthop. 2014; 38:1443-9. https://doi.org/10.1007/s00264-014-2306-1.
14. Hu YG, Han L, Fang WL, Jin B. Comparison of anatomical locking plate and Gamma nail for the treatment of intertrochanteric fracture with external wall fractures. Zhongguo Gu Shang. 2016; 29:496-501.
15. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969; 51:737-55.
16. Kavanagh BF, Fitzgerald RH Jr. Clinical and roentgenographic assessment of total hip arthroplasty. A new hip score. Clin Orthop Relat Res. 1985; 133-40.
17. Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery. 1962; 51:224-32.