
Human papillomaviruses (HPVs)
Human papillomaviruses (HPVs) are small double-stranded DNA viruses that comprise a heterogeneous family consisting of more than 130 different HPV types [1]. Different HPV types have been detected in the anogenital tract, urethra, skin, larynx, tracheo-bronchial and oral mucosa and can cause a wide range of infections, including common warts, genital warts, recurrent respiratory papillomatosis, low-grade and high-grade squamous intraepithelial lesions (SILs), anal cancer, vaginal cancer and cervical cancer. Based on their association with cervical cancer, HPV types are classified as high-risk (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 and 82) or low-risk (HPV-26, 30, 34, 53, 66, 67, 69, 70, 73, 82, 85) [2]. Evidence of the potential role of HPV in other tumor types has been shown, as well [3-8]. High-risk HPV types contribute significantly to viral associated neoplasms, accounting for approximately 600,000 cases (5%) of cancers worldwide annually [9]. In particular, HPV-16 accounts for approximately 50% of cervical carcinomas and more than 90% of HPV(+) carcinomas of the oropharynx (and the other ano-genital sites). Low-risk HPVs have been associated with benign warts of oral and urogenital epithelium in adults as well as children and they are only rarely found in malignant tumors. HPV has also been associated with several other types of SCC and their precursors at different sites, such as skin, vulva, vagina, penis, esophagus, conjunctiva, paranasal sinuses, and bronchus; but its role in the pathogenesis of the lesions is less clear than in cervical cancer. The similarity of the morphologic features of genital and oral HPV associated lesions was one of the early findings that raised the possibility that HPV might be involved in oral and laryngeal SCCs [10, 11]. Until recently, however, the role of HPV in the pathogenesis of head and neck squamous-cell carcinoma (HNSCC) has been quite uncertain.
HPV infections are mainly sexually transmitted through direct skin or mucosa contact and represent the most common sexually transmitted infections worldwide. The probability of transmission is very high, with an estimated life-time risk of cervical HPV infection in sexually active women of up to 80%. Exposure to HPV is determined by well known risk factors for most sexually transmitted infections, while determinants of susceptibility and infectivity are much less established [12]. Knowledge on the natural history of HPV infection derives from studies on cervical infection. The large majority of infections clear spontaneously within 24 months, although the time depends on the HPV type and the immune status. Clearing an infection does not always create immunity if there is a new or continuing source of infection [13]. The virus can either be completely cleared or remain in a latent form which can be later reactivated. Only a small fraction of infections cause clinical lesions; spontaneous regression occurs in most low grade lesions and in a fraction of high grade ones, while progression to invasive cancer is a very rare event and is preventable by surgical treatment of high grade lesions [14].
Epidemiological data of head and neck carcinomas and HPV involvement
Head and neck carcinomas (HNCs) is the sixth most common cancer with an annual incidence of ~400.000 cases [15] and represents about 3.5% of all malignant tumors in the western societies [16, 17] and other parts of the world. HNC is quite heterogeneous and most of the tumors arise in the oral cavity, oropharynx, hypopharynx and larynx. Nearly 90% of these cancers are HNSCCs. The disease is associated with a poor prognosis, with a 5-year survival rate less than 50%. The most well-established risk factors for HNSCC are tobacco and alcohol abuse [18].
HPV involvement in head and neck carcinogenesis was initially reported 30 years ago [10, 11]; however, it was just recently recognized as an emerging risk factor for oropharyngeal squamous cell carcinoma (OSCC) [19]. OSCC begins in the oropharynx, the middle part of the throat that includes the soft palate, the base of the tongue, the tonsils and the side and back wall of the throat. Incidence of HPV(+) OSCC varies greatly worldwide from 25-80% and it is predicted to increase in the near future. OSCC now represents a significantly higher proportion of HNSCCs. This rise in incidence is mostly occurring in individuals aged 40-55 years, without environmental risk factors, and is associated with persistent infection with high-risk HPVs [20]. HPV(+) OSCC patients tend to be younger than HPV(-) ones [21]. Tonsil and oropharyngeal cancers increased in male predominance over the last 30 years, despite a decline in smoking, which may be linked to the decreasing proportion of HPV(-) cancers; while changes in sexual activity may be reflected in increasing proportion of HPV(+) cancers [20]. Recently, HPV-associated OSCC represents about 60% of OSCC cases compared to 40% in the previous decade [22]. In the USA, Sweden, Finland and Czech Republic an increasing incidence of OSCC has been observed during the last decade [23-26].
Nevertheless, the actual incidence of high-risk HPV infection in sites outside the oropharynx, as well as what is the best HPV detection method in HNSCC, have not yet been answered with confidence. Among the other extra-oropharyngeal subsites, HPV might have a role in the supraglottic larynx [27], whose marginal region is contiguous with the oropharynx, and it may account for the high-risk HPV infection rate reported in laryngeal SCCs [28, 29]. HPV detection rates were recently found to range between 12.6-90.9% in oropharyngeal carcinoma [30]. Only in one study the HPV detection rate was <20%; whereas in 34 other investigations it ranged between 20-40%. Also in 2 studies it ranged between 20-30% and in 15 studies HPV was detected in >40% of the tested samples. HPV detection rates, including high risk HPV viral load, were found to be significantly higher in tonsillar cancers than in other head and neck carcinomas [31, 32]. As for the oral cavity SCCs, many authors reported frequent high-risk HPV involvement by considering the over-expression of p16INK4A as equivalent to HPV infection [33, 34]. Nevertheless, recent data in oral cancers indicate that p16INK4A over-expression is due to different mechanisms and high-risk HPV infection is very rarely detectable in oral SCCs [27, 35].
Among the many high-risk HPV types, HPV-16 is the most common, found in almost 90% of the HPV(+) oropharyngeal cancers. At present, HPV-16 remains the only HPV type that is classified as cancer-causing in the head and neck [2, 36]. In addition, there is a more diverse spectrum of other high-risk HPV types with a less important role and a putatively different behavior than that of HPV-16 [37]. Of these, HPV-33, HPV-35, HPV-45 and HPV-58 have been detected in lower frequencies, representing 10-15% of HPV(+) OPC [38-41]. Therefore, HPV(+) OSCCs belong to a distinct clinical and molecular entity with a looser association with tobacco and alcohol.
Molecular mechanisms through which HPVs induce carcinogenesis
The HPV genome is composed of six early (E1, E2, E4, E5, E6, and E7), two late (L1 and L2) open reading frames, and a non-coding long control region (LCR) [42]. E5, E6 and E7 genes encode three viral onco-proteins. E6/E7 proteins function as the dominant onco-proteins of high-risk HPVs inactivating the tumor suppressor proteins, p53 and pRb, respectively. E6 and E7 genes [43] can modify the cell cycle so as to retain the differentiating host keratinocyte in a state that is favorable to the amplification of viral genome replication and consequent late gene expression.
HPV E6 in association with host ubiquitin ligase E6-associated protein (E6AP) acts to ubiquitinate p53, leading to its proteasomal degradation [44]. P53 is a well-studied transcription factor that induces cell cycle arrest or apoptosis in response to cellular stress or DNA damage, and has been attributed the roles of “guardian of the genome” and “policeman of the oncogenes”. The first role consists in sensing and reacting to DNA damage through the ATM/ATR and Chk1/Chk2 kinases, and the second in responding to oncogenic signaling through the p53-stabilizing protein ARF [45].While in most cancers p53 malfunction is determined by p53 mutations, in HPV-associated carcinomas wild-type functional p53 is degraded by E6 oncoprotein. Moreover, cells expressing HPV-16 E6 show chromosomal instability [46, 47]. HPV E7 on the other hand inactivates pRb, which controls the G1-S phase transition of the cell cycle by binding the transcription factor E2F. As a consequence, E2F is released with consequent promotion of cell G1-S phase transition [48, 49] and transcription of genes, such as cyclin E and cyclin A, which are required for cell cycle progression. This functional inactivation of pRb results in a reciprocal over-expression of p16INK4A. The HPV(+) tonsillar SCC share a disruption of the pRb pathway as a common biological marker. By immunohistochemistry (IHC), most HPV(+) HNSCCs show p16INK4A over-expression. In non-HPV-related HNSCC, continuous tobacco and alcohol exposure can lead to mutational loss of the p16INK4A and p53 genes. These early neoplastic events are detected in 80% of HNSCCs and cause uncontrolled cellular growth [50]. The expression of p53 and bcl-2 is not associated with HPV(+) oral cavity SCC [51] and mutations in p53 are rarely seen in HPV(+) tumors compared with HPV(-) tumors [52]. Furthermore, there seems to be an inverse relationship between epidermal growth factor receptor (EGFR) expression and HPV status. For patients with OSCC, high p16INK4A and low EGFR were associated with improved outcome, suggesting a predictive role in surgically treated patients [53]. All HPVs can induce transient proliferation, but only HPV-16 and HPV-18 can immortalize cell lines in vitro. Carcinogenic mechanisms in HPV-associated OSCCs may be similar to those in cervical cancers. However, since the oral cavity and the oropharynx are exposed to higher levels of chemical carcinogens compared to the genital tract, it is likely that different mechanisms are implicated in cervical and oropharyngeal carcinogenesis.
HPV detection methods in OSCC
Although the management of OSCC does not require evaluation of HPV status, HPV-testing in OSCC patients is increasingly becoming the standard of care. HPV-induced OSCC constitutes a separate tumor entity with distinct clinical and histopathological features, improved performance status and better prognosis. Nevertheless, heterogeneity both in biological and clinical behavior among HPV(+) cases has been well observed [54]. This heterogeneity highlights the need to assess the presence of HPV in the tumor using an algorithm that can detect just the biologically active virus, and identify the cases with improved clinical outcome. Molecular detection of HPV DNA is the gold standard for the identification of HPV in tissue and exfoliated cell samples using several assays with different sensitivity and specificity, including Southern transfer hybridization, dot blot hybridization, in situ hybridization (ISH), hybrid capture and polymerase chain reaction (PCR) [55]. All the limitations and advantages of each method have been previously described in detail [55].
p16INK4A immunostaining in conjunction with HPV DNA detection is a useful tool to establish a diagnosis of HPV-related OSCC
HPV-related and HPV-unrelated OSCCs show different genetic signatures which most likely underlie differences in tumor development and progression [56]. These differences may also have implications for the management of patients [57]. The detection of elevated p16INK4A protein levels by IHC is the most well-known biomarker for the detection of biologically active HPV infection in HNSCC [58]. p16INK4A is a cyclin-dependent kinase (CDK) inhibitor, encoded by the CDKN2A locus, which arrests the cell cycle in the G1 stage [59, 60]. pRb inactivation by HPV E7 is associated with up-regulation of CDKN2A and consequent protein over-expression. Conversely, in HPV-unrelated, environment-related HNSCC, perturbation of the pRb-pathway is uncommon and CDKN2A expression is usually low. Therefore, p16INK4A immunostaining in conjunction with HPV DNA detection is very a useful tool to establish a diagnosis of HPV-related OSCC [53]. Weinberger et al. [61] demonstrated that HPV(+) and p16INK4A(+) tumors had favorable prognosis and the presence of HPV in the tumors per se did not have a substantial positive impact on prognosis. As p16INK4A expression lacks specificity for high-risk HPV and does not distinguish p16INK4A up-regulation due to E7-mediated pRb loss from that sustained by other so far unidentified mechanisms (e.g., stress, aging, senescence, etc.), and given the different outcomes in the p16INK4A(+)/HPV(-) subgroups, in the context of personalized treatments, p16INK4A(+)/HPV(-) OSCCs should be considered as a distinct subset. For this reason, it is recommended that HPV should be assessed both by ISH and p16INK4A [62].
In the Danish Head and Neck Cancer Group (DAHANCA) 5 trial [63] p16INK4A was evaluated as prognostic marker of treatment response and survival in a cohort of patients treated solely with conventional radiotherapy. p16INK4A positivity was detected in 22% of the tumors; however, no substantial difference was observed between p16INK4A(+) and p16INK4A(-) tumors. Specifically, p16INK4A(+) tumors seemed to be more closely associated with poor histopathologic differentiation compared with the p16INK4A(-) ones, but the difference was not statistically significant, indicating that p16INK4A alone is not an adequate marker. The weakness of this study is that the authors included many p16INK4A(+) tumors that were not HPV(+) in the analysis as if they were HPV(+).
Preclinical data for HNSCC cell lines and xenografts showed more antitumor activity when treated with the anti-EGFR monoclonal antibody panitumumab combined with radiotherapy, than when treated with radiotherapy alone. Furthermore, phase 1 response data for panitumumab plus chemotherapy suggested that additional investigation of panitumumab in HNSCC is needed [64]. In the Study of Panitumamub Efficacy in Patients With Recurrent and/or Metastatic Head and Neck Cancer (SPECTRUM), panitumumab plus cisplatin and fluorouracil was compared with chemotherapy in patients with recurrent or metastatic HNSCC. Overall survival did not significantly improve with the addition of panitumumab to the chemotherapy regimen; however, improvements were recorded in progression-free survival and objective response. Furthermore, in a retrospective analysis, a negative HPV tumor status predicted overall and progression-free survival after treatment with cisplatin and fluorouracil plus panitumumab. Moreover, a p16INK4A(+) status was a favorable prognostic marker in patients who received only chemotherapy, suggesting a potential prognostic effect in this population of patients. The authors reported that the p16INK4A status of the tumor, regional differences in overall survival, as well as other factors including the intensity and amount of previous treatment, might be important considerations in the design of future global trials in recurrent or metastatic HNSCC. However, the drawback of this study is that conclusions about EGFR inhibition were erroneously drawn based on the patients’ p16INK4A status, since half of the tumors were rated as HPV(+), just by p16INK4A(+) test.
The conclusion of these two studies is that presence of HPV DNA in tissue biopsies is not always sufficient to attribute a cancer of the oropharynx to HPV, depending on the different sensitivity of the various assays relying on DNA detection (especially in tobacco/alcohol exposed patients). Appropriate algorithms should be used to define an HPV-induced tumor. Assessment of HPV status is indicated in patients with oropharyngeal carcinomas, particularly when no environmental risk factors are present and in patients with neck metastasis and carcinoma of unknown primary as HPV detection in metastatic lymph node samples is strongly indicative of a primary in the tonsils or in the base of the tongue [65].
Prognosis of HPV-induced carcinomas
The first line of evidence of the impact of HPV in prognosis comes from various small single-institutional retrospective case series, showing that patients with HPV(+) HNSCC (particularly those with oropharyngeal primary) treated by radiotherapy, chemoradiotherapy, surgery or combined modality therapy, have better outcome than those with HPV-uninduced cancer [66, 67]. HPV(+) SCC patients were estimated to have up to an 80% reduction in risk of disease failure compared to HPV(-) patients. Furthermore, retrospective analyses of archival tumor specimens from patients enrolled in phase II and III trials, which received more specific treatment regimens [68, 69] and meta-analyses [70, 71], confirmed that HPV(+) HNSCC is a separate biologic entity and that these patients have significantly better prognosis than patients with HPV-unrelated tumors. In these studies, the survival benefit was most predominant or restricted in patients with an oropharyngeal primary tumor. Furthermore, patients with HPV(+) HNSCCs, OSCCs and tonsillar SCCs have lower disease specific mortality and are less likely to experience progression or recurrence of their cancer than HPV(-) patients [72]. The reason why patients with HPV-induced HNSCC have better prognosis than those with HPV-unrelated cancer remains to be explained. Robust data indicate that cigarette smoking may modify the clinical behavior of HPV(+) SCC, adversely affecting the prognosis of these neoplasms [73]. Recently, a recursive partitioning analysis showed that the combination of tumor HPV status, smoking and TN category segregates patients with stage III and IV OSCCs into 3 groups with different prognoses: patients with HPV-induced SCCs were considered to be at low risk, with the exception of smokers with advanced nodal category, who were considered to be at intermediate risk; patients with HPV(-) SCCs were considered to be at high risk, with the exception of non-smokers with tumors of stage T2 or T3, who were considered to be at intermediate risk [74]. Some authors have argued that HPV status may reduce the overall prognostic significance of nodal category [75]. As mentioned above, the high-risk HPV E6 and E7 oncoproteins are prognostic factors in HNSCC. The E7-mediated inactivation of pRb is associated with CDKN2A/p16INK4A up-regulation [76]. The absence of p53 mutations is significantly associated with better overall survival. Also, p16INK4A positivity is associated with better outcomes, regardless of HPV positivity. As a consequence, the survival benefit observed in HPV-induced HNSCC may not be the result of HPV positivity per se, but rather the result of the absence of p53 gene mutations or p16INK4A deletion in HPV(+) tumors, which are responsible for poor prognosis in HPV(-) patients [77]. Another unclear aspect is whether HPV status is a prognostic marker, a predictive marker for response to a specific treatment, or both. So far, the data support the hypothesis that HPV positivity results in a survival benefit, independently of treatment. However, large randomized clinical trials including the stratification of patients according to HPV status are needed to provide a definite response.
New immunotherapy drugs anti-CTLA-4 and anti-PD-L1 block co-inhibitory signaling
Both in environmental-induced carcinogenesis and HPV oncogene-induced transformation, HNSCC is associated with a fundamental failure of immune surveillance, where tumor cells have escaped recognition and lysis by the cytotoxic T lymphocytes (CTLs) of adaptive immunity. The critical effector cells of adaptive antitumor immunity are the activated CD8(+) CTLs. Activation of the naïve, antigen-restricted CD8(+) CTLs first requires binding of the T cell receptor (TCR) to its cognate tumor antigen (TA) in complex with human leukocyte antigen (HLA) I. Although the engagement between a tumor antigen and a T cell receptor (TA-TCR engagement) is necessary, it is not sufficient for CTL activation and tumor cytolysis. Initial activation also depends upon the balance between co-stimulatory and co-inhibitory signaling by dendritic cells (DCs) and CD4(+) helper T cells, as well as freedom from suppression caused by CD4(+) regulatory T cells (Tregs). HNSCC elicits T cell anergy in both peripheral and tumor-infiltrating lymphocytes (TILs). Functional defects in TILs include low production and response to IL-2 [78]; vulnerability to spontaneous apoptosis, mediated by the Fas/Fas-ligand pathway [79]; low expression of CD3-f, OX40, and 4-1BB, co-stimulatory molecules required for signaling by the TCR [78, 80]; and high expression of co-inhibitory receptors, cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed-death 1 (PD-1) [78, 81] (Figure 1).
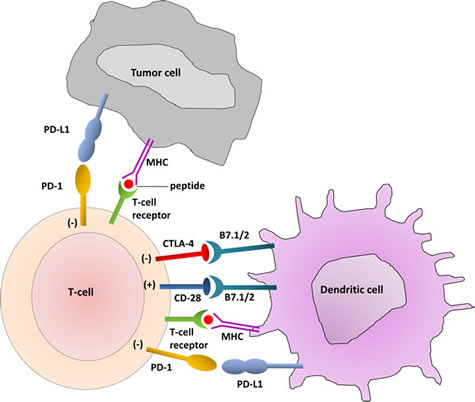
Figure 1: T-Cell Interaction with dendritic cells and tumor cells. The immune checkpoints CTLA-4 and PD-1/PD-L1 are highlighted in the interactions among T-cells, dendritic cells and tumor cells.
Successful activation of the CTL following the binding of TA-TCR depends upon predominance of co-stimulatory versus co-inhibitory signaling by accessory receptors. The co-inhibitory receptors CTLA-4 and PD-1 down-modulate CTL response in the setting of chronic antigen stimulation - a useful adaptation for resolving the inflammatory response following infection and in preventing auto-immunity. However, in the setting of cancer these receptors induce pathologic tolerance. A new therapeutic paradigm is the design of mAbs to block co-inhibitory signaling, releasing the CTL from anergy. The first in class is ipilimumab, an IgG1 mAb against the CTLA-4 co-inhibitory receptor expressed on activated CTLs and Tregs. CTLA-4 and the major co-stimulatory receptor CD28 compete for the same ligand on antigen-presenting cells (APCs), B7. The blockade of CTLA-4, releases B7 to bind CD28, thus propagating the B7-CD28 co-stimulatory signal that is required for TA-specific TCR activation. Ipilimumab has been FDA-approved in melanoma [82]. Release from CTLA-4 co-inhibitory signaling appears to up-regulate TA-specific CTLs and mediate therapeutic response. Blockade of constitutive CTLA-4 signaling in Tregs also potentiates response [83]. However, non-specific up-regulation of CTLs can lead to significant autoimmune adverse events [84]. A similar drug, the IgG2 mAb tremelimumab, is also under development [84]. CTLA-4 checkpoint inhibitors have striking potential to release T-cell immune-suppression in HNSCC, where the immune microenvironment is characterized by CTL anergy and Treg infiltration.
PD-1 is a second inhibitory member of the CD28/CTLA-4 family of co-receptors. It is expressed on CTLs, NK cells, B cells and macrophages, and it is thought to be a broader negative regulator of immune response than CTLA-4. PD-1 has two ligands: PD-L1 and PD-L2. PD-L1 is up-regulated on DCs and macrophages in response to chronic antigen stimulation, as is the case in the tumor microenvironment; many tumors including HNSCC co-opt expression of PDL1 to induce CTL and NK anergy. Therapeutic mAbs against both PD-1 and PD-L1 are entering advanced stages of clinical development [85, 86]. A phase I trial of BMS-936558, a humanized IgG4 anti-PD-1 mAb, was conducted in patients with advanced solid tumors including NSCLC, renal carcinoma and melanoma. There were 31 responses; 20 of these were durable, lasting greater than one year. Immune adverse events, including pneumonitis, vitiligo, colitis, hepatitis, did not limit treatment. Of note, objective responses correlated with PD-L1 expression on tumor. Similarly, a large phase I study of a humanized IgG4 anti-PD-L1 mAb (BMS-936559), documented durable objective responses in 6-17% of patients with advanced solid tumors. Given the expression of PD-L1 in the majority of HPV(-) and HPV(+) HNSCC, these therapeutic antibodies are of particular interest in HNSCC - as monotherapy, or as adjuncts to conventional therapies including cetuximab.
Therapeutic cancer vaccines
Enthusiasm for the development of head and neck tumor vaccines is motivated by the observation of nascent CTL responses against unique tumor antigens (TAs); the existence of this thwarted immune response implies the potential to harness and amplify adaptive immunity. Fundamentally, the goal of therapeutic cancer vaccination is inculcation of a persistent, TA-specific T cell response which kills tumor cells - abating tumor progression or even resulting in cure. In general, an effective vaccine will require successful TA presentation by professional APCs and a consequent TA-specific CTL response. Vaccines may target two forms of TAs: tumor-specific antigens (TSAs), or tumor-associated antigens (TAAs) [87]. TSAs are oncoproteins unique to the tumor not occurring in normal host cells (e.g. mutated p53 protein or the E6/E7 HPV oncoproteins). Targeting TSAs may be advantageous as these proteins are often central to tumorigenesis and their specificity would avoid auto-immune sequelae for normal tissue. However, a TSA-targeting vaccine may be applicable to only a small minority, whose tumor bears the candidate somatic mutation. This can be particularly prohibitive when the target is a tumor suppressor gene inactivated by a variety of point mutations, frameshifts or deletions - as is the case for p53 mutation, the most common genetic mutation in HNSCC [88]. TAAs are proteins over-expressed in tumor cells; however, they are also expressed in normal tissues (e.g. wild type EGFR). While TAA over-expression is prevalent in tumors with a common histology, making them a broadly applicable target, they are limited by weak immunogenicity and self-tolerance.
Ultimately, cancer vaccines must deliver antigenic peptides to professional APCs for presentation in association with MHC to the cognate CTLs. Various vaccination methods exist in HNSCC, each with their own particular advantages and drawbacks: 1) protein-based or peptide vaccines, consisting of pre-assembled proteins; 2) DNA vaccines, consisting of recombinant, TA-encoding DNA in a plasmid backbone; and 3) recombinant vector-based vaccines, where a viral, bacterial or yeast vector is loaded with recombinant DNA encoding the TA of interest. In peptide vaccines, for example HPV oncoprotein peptide vaccines, oncogenic activity must be inactivated while maintaining sufficient peptide length to stimulate CTL response. Advantages to this approach include ease of production and the ability to target TSA, whereas disadvantages include host proteolysis, weak immunogenicity, HLA restriction and poor long-lasting immunity [89]. DNA vaccines are more stable than peptides, however DNA uptake by APC associated with effective antigen expression is limited. Delivery methods, such as by electroporation or gene gun, can enhance uptake and immunogenicity [90]. Vector-based vaccines may overcome the poor antigenicity of naked DNA vaccines, due to a cross-over effect from the robust inflammatory response against vector antigens.
HPV is an ideal vaccine target, due to the expression of non-host TSAs and constitutive expression of these viral oncoproteins to maintain the transformed state. Proof-of-principle has been demonstrated by the successful development of HPV prevention vaccines, Cervarix® and Gardasil®. While these marketed vaccines prevent anogenital HPV infection, their impact on the natural history of oral HPV is still unknown. Regardless, the capsid antibodies triggered by these L1 peptide vaccines are useful only for primary prevention; humoral blockade of the viral entry step is not relevant for established, HPV-transformed malignancies. Therapeutic vaccines for HPV-related cancers are of substantial interest in HNSCC. Five promising vaccination strategies have entered clinical development in HPV-induced neoplasia including two peptide vaccines, a detoxified E7 DNA vaccine, and two vector vaccines: 1) The HPV 16 E6 and E7 long peptide vaccine with incomplete freund’s adjuvant was studied in 20 women with HPV-16 associated vulvar intraepithelial neoplasia. All patients had vaccine-induced CTL responses; 15 out of 19 patients had clinical responses [91]. 2) In a phase I study of a Trojan peptide vaccine containing HLA-I and HLA-II restricted Melanoma Antigen E (MAGE-A3) and HPV-16 derived peptides, immunogenicity was documented in 4 out of 5 patients with advanced HNSCC, however none exhibited an objective response [92]. 3) The HPV pNGVL4a-CRT/E7 (Detox) DNA vaccine contains the HPV 16 E7 gene engineered to disrupt the retinoblastoma binding site, thereby abrogating oncogenicity, embedded in the pNGVL-4a plasmid backbone [93]. This vaccine is under phase I study in patients with HPV-associated HNSCC following definitive multimodality therapy (NCT01493154). 4) TG4001, a modified vaccinia virus expressing the HPV-16 oncoproteins E6 and E7 as well as human interleukin- 2 (IL-2), has been studied in 21 patients with cervical intraepithelial neoplasia (CIN). HPV-16 clearance was associated with cytologic regression in 7/10 clinical responders. Additionally, 7/8 patients cleared HPV infection without conization and had no residual suspicion of CIN2/3 [94]. 5) The Lm-LLO-E7 vaccine harnesses a live-attenuated Listeria monocytogenes bacterium engineered to secrete the HPV-16 E7 antigen fused to listeriolysin O, the virulence factor permitting cytosolic replication in APCs [95]. This vaccine was evaluated for safety in 15 patients with advanced cervical carcinoma [96]. Dose-limiting toxicities consisted of pyrexia and diastolic hypotension; assessment of CTL response was technically limited. This vaccine is current under phase I investigation in patients with HPV-associated HNSCC with no evidence of disease after completion of standard therapy (NCT 01598792).
In HPV(-) HNSCCs, over-expressed wild type (wt) TAAs, such as p53, are potential vaccine targets. Although p53 mutation is the most commonly identified mutation in HPV(-) HNSCCs, most mutations result in the accumulation of p53; non-mutated portions of the protein are susceptible to degradation into wt peptide sequences appropriate for immune presentation. A phase I trial (NCT00404339) examining p53 multiple-epitope/dendritic cell vaccine in HNSCC patients was reported in 2009. Following definitive therapy, patients with locally advanced HNSCC were vaccinated with wt p53 sequences pre-loaded onto autologous dendritic cells. At 15-month follow up 11/16 patients were alive without disease. Analysis of immunogenicity indicated p53-specific CTLs in 5/16 patients [97].
Current management of HPV-induced HNSCCs
Despite treatment intensification for patients with HNSCC, including altered radiation fractionation and the addition of chemotherapy to radiation, physicians and patients still face the significant challenge of recurrent or second tumors arising within or in close proximity to previously irradiated tissues. Locoregional recurrences develop in ~20% of patients treated with definitive chemoradiation for larynx preservation [98] or with post-operative chemoradiation for high-risk HNSCC [99, 100] and 17-33% of patients treated with definitive chemoradiation for locally advanced un-resectable disease [101, 102]. Locally recurrent tumors may arise from residual neoplastic cells that survive initial treatment, perhaps because of biological parameters that confer radio-resistance [103] or insufficiencies in initial treatment parameters such as radiation dose, volume, fractionation and treatment duration. Second cancers may arise from underlying field cancerization [104], as a radiation-induced malignancy, or as a de novo process and may be indistinguishable from a local recurrence of the primary tumor [105, 106].
Patients with recurrent HNSCC after prior radiation are a heterogeneous group. Differences in the location and extent of recurrent tumor, initial radiation treatment parameters, elapsed time since prior treatment, and extent of normal tissue sequelae, as well as relatively sparse data on acute and late normal tissue recovery from prior treatment and tolerance to re-irradiation [107], pose a significant challenge to the formulation of widely applicable schemata for re-irradiation. The optimal treatment volume for re-irradiation is uncertain. In an effort to limit the toxicity of re-treatment, many reported experiences with re-irradiation have targeted the recurrent gross disease with limited margin and not added elective nodal re-irradiation.
Despite the absence of evidence from randomized, controlled trials to support a de-escalation of treatment intensity in HPV(+) oropharyngeal carcinomas, some investigators argue that intensive concomitant chemoradiation regimens may represent overtreatment [108, 109]. Actually, an aggressive multimodality strategy, which may result in high rates of acute and long-term severe toxicity, would be not appropriate for HPV(+) patients who are younger and have prolonged survival. In this context, most efforts are targeted toward de-escalation of treatment intensity in HPV(+) SCCs with the intent to reduce toxicity and thereby improve the long-term quality of life, while maintaining efficacy. Recommended treatment de-escalation can be achieved by reducing the total dose of radiotherapy in a concurrent chemoradiotherapy setting, by using radiotherapy and EGFR inhibitors instead of cis-platinum based chemoradiotherapy or radiotherapy alone instead of chemoradiotherapy, and primary surgery +/- de-intensified adjuvant treatment instead of up-front chemoradiotherapy.
Aside from the Phase II Eastern Cooperative Oncology Group (ECOG) study and the Phase III Quarterback Trial, there are no active trials addressing radiotherapy dose. The Phase II ECOG study [110] confirmed the improved survival outcomes for patients with HPV(+) HNSCC observed in retrospective survival analyses. Also, these improved survival outcomes were consistent with an increased sensitivity of these cancers to chemotherapy and chemoradiation.
Nevertheless, a de-escalation strategy is not without concerns. A phase III non-inferiority trial for HPV(+) patients is considered difficult to conduct due to the large number of patients required [111]. Moreover, although HPV positivity results in a platform-independent survival benefit, the absolute superiority of any given platform is not yet known. Currently, several randomized controlled clinical trials specifically designed to test the efficacy of a de-intensification strategy in HPV(+) patients are on-going. These de-escalation protocols are mainly based on decreasing the intensity of the radiotherapy or on substituting cis-platinum with cetuximab in concurrent chemotherapy regimens. Treatment de-escalation strategies carry a risk of negatively impacting the overall favorable outcome of the patients. Several investigators sustain that the more favorable prognosis in HPV(+) SCCs may be attributable to better compliance to chemoradiotherapy strategies. Furthermore, emerging data suggest that cetuximab-radiotherapy may not be the preferred therapy in patients with HPV(+) cancers [112]. Very recently, a single-institutional experience with definitive radiation alone for HPV(+) HNSCC confirmed the inherent radio-sensitivity of these tumors [113]. Overall, there is insufficient evidence to treat HPV(+) SCCs with a de-intensified treatment strategy. This option should be restricted to controlled clinical trial settings with closely monitored safety assessments. Undoubtedly, it seems reasonable to exclude non-smoker patients with HPV(+) SCC from clinical trials using intensification of standard treatment. To date, the treatment of patients with HPV(+) OSCC should not be different from standard treatment of patients with HPV(-) tumors. It should be based on stage of disease and the general conditions of the patient, maximizing the probability to treat early stage SCCs with a single modality therapy [114].
Patients with head and neck cancer experience significant changes in their quality of life (qol) associated with disease and the adverse effects of treatment. Frequent problems the patients have to face are usually difficulties with speech, respiration and eating, apart from the psychological impact of loss of function and physical mutilation. These concerns associated with traditional trans-cervical surgical exposure approaches were principal in the clinical development of non-surgical treatment approaches based on fractionated radiotherapy. Over the past 30 years, multiple randomized trials have now established that treatment intensification with the addition of concurrent chemotherapy and altered radiotherapy fractionation schedules [115] can improve locoregional disease control rates and survival. It is also clear that these treatment intensification approaches can also contribute to an increased risk of late swallowing complications, raising concerns that such treatment approaches are also compromising qol and function [116]. As new treatment approaches are developed, prospective qol and function assessment are integral to the assessment in addition to traditional oncologic outcome measures. Development of the trans-oral robotic surgery (TORS) has greatly facilitated the trans-oral surgical approach for oropharyngeal carcinomas, evading many technical restraints [117].
Nevertheless, the optimal treatment for HPV(+) HNSCC patients remains uncertain. HPV(+) cancers appear more sensitive to chemoradiation as patients with low risk HPV(+) oropharyngeal cancers have almost double the overall survival as patients high risk HPV(-) cancers. This benefit in HPV(+) patients results from improved locoregional control rather than decreased distant metastasis. Since concurrent chemoradiation at least doubles the rate of acute and long term toxicities, less intense treatment regimens maximizing cure and decreasing toxicities are being investigated. To de-intensify the current standard of care would require reducing the current radiation dose and/or the chemotherapy regimens.
To this end, the ECOG Phase II trial (E1308) addressed these questions by testing the efficacy of decreasing the radiation dose. Patients achieving a complete response to induction chemotherapy were treated with lower dose radiation and cetuximab. The fact that cetuximab is an antibody targeting the cancer cell membrane and is thus associated with lower toxicity, renders radiation with cetuximab or bioradiotherapy distinct from chemoradiotherapy. Nevertheless, it remains unclear whether bioradiotherapy provides as good locoregional control as chemoradiotherapy. A retrospective analysis showed that bioradiotherapy may not be as effective as chemoradiation, especially in patients with HPV(+) cancers [118]. Similarly, a recent trial suggested that bioradiotherapy has more local failures than chemoradiotherapy in patients with laryngeal cancers [119]. Nevertheless, the ECOG trial is a major advance towards treatment de-intensification even though there was no direct comparison between bioradiotherapy and chemoradiotherapy.
References
1. zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nat Rev Cancer. 2002, 2:342-350.
2. Bouvard V, Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, Benbrahim-Tallaa L, Guha N, Freeman C, Galichet L, Cogliano V. A review of human carcinogens--Part B: biological agents. Lancet Oncol. 2009, 10:321-322.
3. Lyronis ID, Baritaki S, Bizakis I, Krambovitis E, Spandidos DA. K-ras mutation, HPV infection and smoking or alcohol abuse positively correlate with esophageal squamous carcinoma. Pathol Oncol Res. 2008, 14:267-273.
4. Radojicic J, Zaravinos A, Spandidos DA. HPV, KRAS mutations, alcohol consumption and tobacco smoking effects on esophageal squamous-cell carcinoma carcinogenesis. Int J Biol Markers. 2012, 27:1-12.
5. Sarchianaki E, Derdas SP, Ntaoukakis M, Vakonaki E, Lagoudaki ED, Lasithiotaki I, Sarchianaki A, Koutsopoulos A, Symvoulakis EK, Spandidos DA, Antoniou KM, Sourvinos G. Detection and genotype analysis of human papillomavirus in non-small cell lung cancer patients. Tumour Biol. 2014, 35:3203-3209.
6. Zaravinos A, Bizakis J, Spandidos DA. Prevalence of human papilloma virus and human herpes virus types 1-7 in human nasal polyposis. J Med Virol. 2009, 81:1613-1619.
7. Zaravinos A, Kanellou P, Spandidos DA. Viral DNA detection and RAS mutations in actinic keratosis and nonmelanoma skin cancers. Br J Dermatol. 2010, 162:325-331.
8. Ragin C, Obikoya-Malomo M, Kim S, Chen Z, Flores-Obando R, Gibbs D, Koriyama C, Aguayo F, Koshiol J, Caporaso NE, Carpagnano GE, Ciotti M, Dosaka-Akita H, Fukayama M, Goto A, Spandidos DA, Gorgoulis V, Heideman DA, van Boerdonk RA, Hiroshima K, Iwakawa R, Kastrinakis NG, Kinoshita I, Akiba S, Landi MT, Eugene Liu H, Wang JL, Mehra R, Khuri FR, Lim WT, Owonikoko TK, Ramalingam S, Sarchianaki E, Syrjanen K, Tsao MS, Sykes J, Hee SW, Yokota J, Zaravinos A, Taioli E. HPV-Associated Lung Cancers: an International Pooled Analysis. Carcinogenesis 2014.
9. Moore PS, Chang Y. Why do viruses cause cancer? Highlights of the first century of human tumour virology. Nat Rev Cancer. 2010, 10:878-889.
10. Syrjanen K, Syrjanen S, Pyrhonen S. Human papilloma virus (HPV) antigens in lesions of laryngeal squamous cell carcinomas. ORL J Otorhinolaryngol Relat Spec. 1982, 44:323-334.
11. Syrjanen K, Vayrynen M, Castren O, Mantyjarvi R, Pyrhonen S, Yliskoski M. Morphological and immunohistochemical evidence of human papilloma virus (HPV) involvement in the dysplastic lesions of the uterine cervix. Int J Gynaecol Obstet. 1983, 21:261-269.
12. Veldhuijzen NJ, Snijders PJ, Reiss P, Meijer CJ, van de Wijgert JH. Factors affecting transmission of mucosal human papillomavirus. Lancet Infect Dis. 2010, 10:862-874.
13. Hernandez BY, Wilkens LR, Zhu X, Thompson P, McDuffie K, Shvetsov YB, Kamemoto LE, Killeen J, Ning L, Goodman MT. Transmission of human papillomavirus in heterosexual couples. Emerg Infect Dis. 2008, 14:888-894.
14. Schiffman M, Wentzensen N, Wacholder S, Kinney W, Gage JC, Castle PE. Human papillomavirus testing in the prevention of cervical cancer. J Natl Cancer Inst. 2011, 103:368-383.
15. Duray A, Descamps G, Decaestecker C, Remmelink M, Sirtaine N, Lechien J, Ernoux-Neufcoeur P, Bletard N, Somja J, Depuydt CE, Delvenne P, Saussez S. Human papillomavirus DNA strongly correlates with a poorer prognosis in oral cavity carcinoma. Laryngoscope. 2012, 122:1558-1565.
16. Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer. 2010, 46:765-781.
17. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012, 62:10-29.
18. Osei-Sarfo K, Tang XH, Urvalek AM, Scognamiglio T, Gudas LJ. The molecular features of tongue epithelium treated with the carcinogen 4-nitroquinoline-1-oxide and alcohol as a model for HNSCC. Carcinogenesis. 2013, 34:2673-2681.
19. World Health Organization. IARC monographs on the evaluation of carcinogenic risks to humans: volume 100B-Biological Agents. A review of human carcinogens. Lyon: International Agency for Research on Cancer 2012.
20. Chaturvedi AK, Engels EA, Pfeiffer RM, Hernandez BY, Xiao W, Kim E, Jiang B, Goodman MT, Sibug-Saber M, Cozen W, Liu L, Lynch CF, Wentzensen N, Jordan RC, Altekruse S, Anderson WF, Rosenberg PS, Gillison ML. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol. 2011, 29:4294-4301.
21. Lajer CB, von Buchwald C. The role of human papillomavirus in head and neck cancer. Apmis. 2010, 118:510-519.
22. Mehanna H, Jones TM, Gregoire V, Ang KK. Oropharyngeal carcinoma related to human papillomavirus. Bmj. 2010, 340:c1439.
23. Hong AM, Grulich AE, Jones D, Lee CS, Garland SM, Dobbins TA, Clark JR, Harnett GB, Milross CG, O’Brien CJ, Rose BR. Squamous cell carcinoma of the oropharynx in Australian males induced by human papillomavirus vaccine targets. Vaccine. 2010, 28:3269-3272.
24. Nasman A, Attner P, Hammarstedt L, Du J, Eriksson M, Giraud G, Ahrlund-Richter S, Marklund L, Romanitan M, Lindquist D, Ramqvist T, Lindholm J, Sparén P, Ye W, Dahlstrand H, Munck-Wikland E, Dalianis T. Incidence of human papillomavirus (HPV) positive tonsillar carcinoma in Stockholm, Sweden: an epidemic of viral-induced carcinoma? Int J Cancer. 2009, 125:362-366.
25. Syrjanen S: HPV infections and tonsillar carcinoma. J Clin Pathol. 2004, 57:449-455.
26. Tachezy R, Klozar J, Salakova M, Smith E, Turek L, Betka J, Kodet R, Hamsikova E. HPV and other risk factors of oral cavity/oropharyngeal cancer in the Czech Republic. Oral Dis. 2005, 11:181-185.
27. Bussu F, Sali M, Gallus R, Vellone VG, Zannoni GF, Autorino R, Dinapoli N, Santangelo R, Martucci R, Graziani C, Miccichè F, Almadori G, Galli J, Delogu G, Sanguinetti M, Rindi G, Valentini V, Paludetti G. HPV infection in squamous cell carcinomas arising from different mucosal sites of the head and neck region. Is p16 immunohistochemistry a reliable surrogate marker? Br J Cancer. 2013, 108:1157-1162.
28. Almadori G, Cadoni G, Cattani P, Posteraro P, Scarano E, Ottaviani F, Paludetti G, Maurizi M. Detection of human papillomavirus DNA in laryngeal squamous cell carcinoma by polymerase chain reaction. Eur J Cancer. 1996, 32A:783-788.
29. Almadori G, Galli J, Cadoni G, Bussu F, Maurizi M. Human papillomavirus infection and cyclin D1 gene amplification in laryngeal squamous cell carcinoma: biologic function and clinical significance. Head Neck. 2002, 24:597-604.
30. Mammas IN, Sourvinos G, Zaravinos A, Spandidos DA. Vaccination against human papilloma virus (HPV): epidemiological evidence of HPV in non-genital cancers. Pathol Oncol Res. 2011, 17:103-119.
31. Venuti A, Badaracco G, Rizzo C, Mafera B, Rahimi S, Vigili M. Presence of HPV in head and neck tumours: high prevalence in tonsillar localization. J Exp Clin Cancer Res. 2004, 23:561-566.
32. Koskinen WJ, Chen RW, Leivo I, Mäkitie A, Bäck L, Kontio R, Suuronen R, Lindqvist C, Auvinen E, Molijn A, Quint WG, Vaheri A, Aaltonen LM. Prevalence and physical status of human papillomavirus in squamous cell carcinomas of the head and neck. Int J Cancer. 2003, 107:401-406.
33. Sethi S, Ali-Fehmi R, Franceschi S, Struijk L, van Doorn LJ, Quint W, Albashiti B, Ibrahim M, Kato I. Characteristics and survival of head and neck cancer by HPV status: a cancer registry-based study. Int J Cancer. 2012, 131:1179-1186.
34. Heath S, Willis V, Allan K, Purdie K, Harwood C, Shields P, Simcock R, Williams T, Gilbert DC. Clinically significant human papilloma virus in squamous cell carcinoma of the head and neck in UK practice. Clin Oncol. (R Coll Radiol) 2012, 24:e18-23.
35. Harris SL, Thorne LB, Seaman WT, Hayes DN, Couch ME, Kimple RJ. Association of p16(INK4a) overexpression with improved outcomes in young patients with squamous cell cancers of the oral tongue. Head Neck. 2011, 33:1622-1627.
36. Stransky N, Egloff AM, Tward AD, Kostic AD, Cibulskis K, Sivachenko A, Kryukov GV, Lawrence MS, Sougnez C, McKenna A, Shefler E, Ramos AH, Stojanov P, Carter SL, Voet D, Cortés ML, Auclair D, Berger MF, Saksena G, Guiducci C, Onofrio RC, Parkin M, Romkes M, Weissfeld JL, Seethala RR, Wang L, Rangel-Escareño C, Fernandez-Lopez JC, Hidalgo-Miranda A, Melendez-Zajgla J, Winckler W, Ardlie K, Gabriel SB, Meyerson M, Lander ES, Getz G, Golub TR, Garraway LA, Grandis JR. The mutational landscape of head and neck squamous cell carcinoma. Science. 2011, 333:1157-1160.
37. Bosch FX, Lorincz A, Muñoz N, Meijer CJ, Shah KV. The causal relation between human papillomavirus and cervical cancer. J Clin Pathol. 2002, 55:244–265.
38. Glombitza F, Guntinas-Lichius O, Petersen I. HPV status in head and neck tumors. Pathology –ResearchandPractice. 2010, 206:229–234.
39. Deng Z, Hasegawa M, Yamashita Y, Matayoshi S, Kiyuna A, Agena S, Uehara T, Maeda H, Suzuki M. Prognostic value of human papillomavirus and squamous cell carcinoma antigen in head and neck squamous cell carcinoma. Cancer Sci. 2012, 103:2127-2134.
40. Koskinen WJ, Chen RW, Leivo I, Mäkitie A, Bäck L, Kontio R, Suuronen R, Lindqvist C, Auvinen E, Molijn A, Quint WG, Vaheri A, Aaltonen LM. Prevalence and physical status of human papillomavirus in squamous cell carcinomas of the head and neck. Int J Cancer. 2003, 107:401–406.
41. Soria-Céspedes D, Canchola Aguilar G, Lara-Torres CO, Sánchez-Marle JF, Hernández-Peña RE, Ortiz-Hidalgo C. Metastatic oropharyngeal squamous cell carcinoma in cervical lymph nodes associated to HPV infection type 16 and 45; clinical, morphological and molecular study of two cases. Gac Med Mex. 2013, 149:673-679.
42. Ganguly N, Parihar SP. Human papillomavirus E6 and E7 oncoproteins as risk factors for tumorigenesis. J Biosci. 2009, 34:113-123.
43. Munger K, Howley PM. Human papillomavirus immortalization and transformation functions. Virus Res. 2002, 89:213-228.
44. Ault KA. Epidemiology and natural history of human papillomavirus infections in the female genital tract. Infect Dis Obstet Gynecol. 2006, 2006 Suppl:40470.
45. Efeyan A, Serrano M. p53: guardian of the genome and policeman of the oncogenes. Cell Cycle. 2007, 6:1006-1010.
46. Lee D, Kwon JH, Kim EH, Kim ES, Choi KY. HMGB2 stabilizes p53 by interfering with E6/E6AP-mediated p53 degradation in human papillomavirus-positive HeLa cells. Cancer Lett. 2010, 292:125-132.
47. Tomaic V, Pim D, Thomas M, Massimi P, Myers MP, Banks L. Regulation of the human papillomavirus type 18 E6/E6AP ubiquitin ligase complex by the HECT domain-containing protein EDD. J Virol. 2011, 85:3120-3127.
48. Classon M, Harlow E. The retinoblastoma tumour suppressor in development and cancer. Nat Rev Cancer. 2002, 2:910-917.
49. Masciullo V, Khalili K, Giordano A. The Rb family of cell cycle regulatory factors: clinical implications. Int J Oncol. 2000, 17:897-902.
50. Califano J, van der Riet P, Westra W, Nawroz H, Clayman G, Piantadosi S, Corio R, Lee D, Greenberg B, Koch W, Sidransky D. Genetic progression model for head and neck cancer: implications for field cancerization. Cancer Res. 1996, 56:2488-2492.
51. Oliveira MC, Soares RC, Pinto LP, Souza LB, Medeiros SR, Costa Ade L. High-risk human papillomavirus (HPV) is not associated with p53 and bcl-2 expression in oral squamous cell carcinomas. Auris Nasus Larynx. 2009, 36:450-456.
52. Fallai C, Perrone F, Licitra L, Pilotti S, Locati L, Bossi P, Orlandi E, Palazzi M, Olmi P. Oropharyngeal squamous cell carcinoma treated with radiotherapy or radiochemotherapy: prognostic role of TP53 and HPV status. Int J Radiat Oncol Biol Phys. 2009, 75:1053-1059.
53. Liang C, Marsit CJ, McClean MD, Nelson HH, Christensen BC, Haddad RI, Clark JR, Wein RO, Grillone GA, Houseman EA, Halec G, Waterboer T, Pawlita M, Krane JF, Kelsey KT. Biomarkers of HPV in head and neck squamous cell carcinoma. Cancer Res. 2012, 72:5004-5013.
54. Reimers N, Kasper HU, Weissenborn SJ, Stutzer H, Preuss SF, Hoffmann TK, Speel EJ, Dienes HP, Pfister HJ, Guntinas-Lichius O, Klussmann JP. Combined analysis of HPV-DNA, p16 and EGFR expression to predict prognosis in oropharyngeal cancer. Int J Cancer. 2007, 120:1731-1738.
55. Zaravinos A, Mammas IN, Sourvinos G, Spandidos DA. Molecular detection methods of human papillomavirus (HPV). Int J Biol Markers. 2009, 24:215-222.
56. Jung AC, Briolat J, Millon R, de Reynies A, Rickman D, Thomas E, Abecassis J, Clavel C, Wasylyk B. Biological and clinical relevance of transcriptionally active human papillomavirus (HPV) infection in oropharynx squamous cell carcinoma. Int J Cancer. 2010, 126:1882-1894.
57. Lohavanichbutr P, Houck J, Fan W, Yueh B, Mendez E, Futran N, Doody DR, Upton MP, Farwell DG, Schwartz SM, Zhao LP, Chen C. Genomewide gene expression profiles of HPV-positive and HPV-negative oropharyngeal cancer: potential implications for treatment choices. Arch Otolaryngol Head Neck Surg. 2009, 135:180-188.
58. Chandarana SP, Lee JS, Chanowski EJ, Sacco AG, Bradford CR, Wolf GT, Prince ME, Moyer JS, Eisbruch A, Worden FP, et al: Prevalence and predictive role of p16 and epidermal growth factor receptor in surgically treated oropharyngeal and oral cavity cancer. Head Neck. 2013, 35:1083-1090.
59. Kanellou P, Zaravinos A, Zioga M, Spandidos DA. Deregulation of the tumour suppressor genes p14(ARF), p15(INK4b), p16(INK4a) and p53 in basal cell carcinoma. Br J Dermatol. 2009, 160:1215-1221.
60. Kanellou P, Zaravinos A, Zioga M, Stratigos A, Baritaki S, Soufla G, Zoras O, Spandidos DA. Genomic instability, mutations and expression analysis of the tumour suppressor genes p14(ARF), p15(INK4b), p16(INK4a) and p53 in actinic keratosis. Cancer Lett. 2008, 264:145-161.
61. Weinberger PM, Yu Z, Haffty BG, Kowalski D, Harigopal M, Brandsma J, Sasaki C, Joe J, Camp RL, Rimm DL, Psyrri A. Molecular classification identifies a subset of human papillomavirus–associated oropharyngeal cancers with favorable prognosis. J Clin Oncol. 2006, 24:736-747.
62. Perrone F GA, Cortelazzi B, Bossi P, Licitra L, Pilotti S. Isolating p16-positive/HPV-negative oropharyngeal cancer: an effort worth making. Am J Surg Pathol. 2011, 35:774-777.
63. Lassen P, Eriksen JG, Hamilton-Dutoit S, Tramm T, Alsner J, Overgaard J. Overgaard: Effect of HPV-Associated p16INK4A Expression on Response to Radiotherapy and Survival in Squamous Cell Carcinoma of the Head and Neck. J Clin Oncol. 2009, 27:1992-1998.
64. Wirth LJ, Posner MR, Haddad RI, et al. Phase I study of panitumumab + chemoradiotherapy (CRT) for head and neck cancer (HNC). Proc Am Soc Clin Oncol. 2008, 26:32360 (abstr.).
65. Tribius S, Hoffmann AS, Bastrop S, Gorogh T, Haag J, Rocken C, Clauditz T, Grob T, Wilczak W, Tennstedt P, Borcherding A, Petersen C, Hoffmann M. HPV status in patients with head and neck of carcinoma of unknown primary site: HPV, tobacco smoking, and outcome. Oral Oncol. 2012, 48:1178-1184.
66. Licitra L, Perrone F, Bossi P, Suardi S, Mariani L, Artusi R, Oggionni M, Rossini C, Cantù G, Squadrelli M, Quattrone P, Locati LD, Bergamini C, Olmi P, Pierotti MA, Pilotti S. High-risk human papillomavirus affects prognosis in patients with surgically treated oropharyngeal squamous cell carcinoma. J Clin Oncol.2006, 24:5630-5636.
67. Ritta M, De Andrea M, Mondini M, Mazibrada J, Giordano C, Pecorari G, Garzaro M, Landolfo V, Schena M, Chiusa L, Landolfo S. Cell cycle and viral and immunologic profiles of head and neck squamous cell carcinoma as predictable variables of tumor progression. Head Neck. 2009, 31:318-327.
68. Posner MR, Lorch JH, Goloubeva O, Tan M, Schumaker LM, Sarlis NJ, Haddad RI, Cullen KJ. Survival and human papillomavirus in oropharynx cancer in TAX 324: a subset analysis from an international phase III trial. Ann Oncol. 2011, 22:1071-1077.
69. Rischin D, Young RJ, Fisher R, Fox SB, Le QT, Peters LJ, Solomon B, Choi J, O’Sullivan B, Kenny LM, McArthur GA. Prognostic significance of p16INK4A and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III trial. J Clin Oncol. 2010, 28:4142-4148.
70. Dayyani F, Etzel CJ, Liu M, Ho CH, Lippman SM, Tsao AS. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol. 2010, 2:15.
71. Ragin CC, Taioli E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: review and meta-analysis. Int J Cancer. 2007, 121:1813-1820.
72. O’Rorke MA, Ellison MV, Murray LJ, Moran M, James J, Anderson LA. Human papillomavirus related head and neck cancer survival: a systematic review and meta-analysis. Oral Oncol. 2012, 48:1191-1201.
73. Granata R, Miceli R, Orlandi E, Perrone F, Cortelazzi B, Franceschini M, Locati LD, Bossi P, Bergamini C, Mirabile A, Mariani L, Olmi P, Scaramellini G, Potepan P, Quattrone P, Ang KK, Licitra L. Tumor stage, human papillomavirus and smoking status affect the survival of patients with oropharyngeal cancer: an Italian validation study. Ann Oncol. 2012, 23:1832-1837.
74. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tân PF, Westra WH, Chung CH, Jordan RC, Lu C, Kim H, Axelrod R, Silverman CC, Redmond KP, Gillison ML. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010, 363:24-35.
75. Genden EM, Sambur IM, de Almeida JR, Posner M, Rinaldo A, Rodrigo JP, Strojan P, Takes RP, Ferlito A. Human papillomavirus and oropharyngeal squamous cell carcinoma: what the clinician should know. Eur Arch Otorhinolaryngol. 2013, 270:405-416.
76. Wiest T, Schwarz E, Enders C, Flechtenmacher C, Bosch FX. Involvement of intact HPV16 E6/E7 gene expression in head and neck cancers with unaltered p53 status and perturbed pRb cell cycle control. Oncogene. 2002, 21:1510-1517.
77. Leemans CR, Braakhuis BJ, Brakenhoff RH. The molecular biology of head and neck cancer. Nat Rev Cancer. 2011, 11:9-22.
78. Baruah P, Lee M, Odutoye T, Williamson P, Hyde N, Kaski JC, Dumitriu IE. Decreased levels of alternative costimulatory receptors OX40 and 4-1BB characterise T cells from head and neck cancer patients. Immunobiology. 2012, 217:669–675.
79. Hoffmann TK, Dworacki G, Tsukihiro T, Meidenbauer N, Gooding W, Johnson JT, Whiteside TL. Spontaneous apoptosis of circulating T lymphocytes in patients with head and neck cancer and its clinical importance. Clin Cancer Res. 2002, 8:2553–2562.
80. Reichert TE, Scheuer C, Day R, Wagner W, Whiteside TL. The number of intratumoral dendritic cells and zeta-chain expression in T cells as prognostic and survival biomarkers in patients with oral carcinoma. Cancer Epidemiol Biomarkers Prev. 2001, 91:2136–2147.
81. Badoual C, Hans S, Merillon N, Van Ryswick C, Ravel P, Benhamouda N, Levionnois E, Nizard M, Si-Mohamed A, Besnier N, Gey A, Rotem-Yehudar R, Pere H, Tran T, Guerin CL, Chauvat A, Dransart E, Alanio C, Albert S, Barry B, Sandoval F, Quintin-Colonna F, Bruneval P, Fridman WH, Lemoine FM, Oudard S, Johannes L, Olive D, Brasnu D, Tartour E. PD-1-expressing tumor-infiltrating T cells are a favorable prognostic biomarker in HPV-associated head and neck cancer. Cancer Res. 2013, 73:128–138.
82. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbé C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010, 363:711–723.
83. Peggs KS, Quezada SA, Chambers CA, Korman AJ, Allison JP. Blockade of CTLA-4 on both effector and regulatory T cell compartments contributes to the antitumor activity of anti-CTLA-4 antibodies. J Exp Med. 2009, 206:1717–1725.
84. Dillman RO: Cancer immunotherapy. Cancer Biother Radiopharm 2011, 26:1–64.
85. Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ, Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, Pitot HC, Hamid O, Bhatia S, Martins R, Eaton K, Chen S, Salay TM, Alaparthy S, Grosso JF, Korman AJ, Parker SM, Agrawal S, Goldberg SM, Pardoll DM, Gupta A, Wigginton JM. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012, 366:2455–2465.
86. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, Horn L, Drake CG, Pardoll DM, Chen L, Sharfman WH, Anders RA, Taube JM, McMiller TL, Xu H, Korman AJ, Jure-Kunkel M, Agrawal S, McDonald D, Kollia GD, Gupta A, Wigginton JM, Sznol M. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012, 366:2443–2454.
87. Schlom J. Therapeutic cancer vaccines: current status and moving forward. J Natl Cancer Inst. 2012, 104:599–613.
88. Stransky N, Egloff AM, Tward AD, Kostic AD, Cibulskis K, Sivachenko A, Kryukov GV, Lawrence MS, Sougnez C, McKenna A, Shefler E, Ramos AH, Stojanov P, Carter SL, Voet D, Cortés ML, Auclair D, Berger MF, Saksena G, Guiducci C, Onofrio RC, Parkin M, Romkes M, Weissfeld JL, Seethala RR, Wang L, Rangel-Escareño C, Fernandez-Lopez JC, Hidalgo-Miranda A, Melendez-Zajgla J, Winckler W, Ardlie K, Gabriel SB, Meyerson M, Lander ES, Getz G, Golub TR, Garraway LA, Grandis JR. The mutational landscape of head and neck squamous cell carcinoma. Science. 2011, 333:1157–1160.
89. Vergati M, Intrivici C, Huen NY, Schlom J, Tsang KY. Strategies for cancer vaccine development. J Biomed Biotechnol. 2010, 2010. pii: 596432.
90. Best SR, Peng S, Juang CM, Hung CF, Hannaman D, Saunders JR, Wu TC, Pai SI. Administration of HPV DNA vaccine via electroporation elicits the strongest CD8+ T cell immune responses compared to intramuscular injection and intradermal gene gun delivery. Vaccine. 2009, 27:5450–5459.
91. Kenter GG, Welters MJ, Valentijn AR, Lowik MJ, Berends-van der Meer DM, Vloon AP, Essahsah F, Fathers LM, Offringa R, Drijfhout JW, Wafelman AR, Oostendorp J, Fleuren GJ, van der Burg SH, Melief CJ. Vaccination against HPV-16 oncoproteins for vulvar intraepithelial neoplasia. N Engl J Med. 2009, 361:1838–1847.
92. Voskens CJ, Sewell D, Hertzano R, DeSanto J, Rollins S, Lee M, Taylor R, Wolf J, Suntharalingam M, Gastman B, Papadimitriou JC, Lu C, Tan M, Morales R, Cullen K, Celis E, Mann D, Strome SE. Induction of mage-A3 and HPV-16 immunity by Trojan vaccines in patients with head and neck carcinoma. Head Neck Oncol. 2012, 34:1734-1746.
93. Peng S, Lyford-Pike S, Akpeng B, Wu A, Hung CF, Hannaman D, Saunders JR, Wu TC, Pai SI. Low-dose cyclophosphamide administered as daily or single dose enhances the antitumor effects of a therapeutic HPV vaccine. Cancer Immunol Immunother. 2013, 62:171–182.
94. Brun JL, Dalstein V, Leveque J, Mathevet P, Raulic P, Baldauf JJ, Scholl S, Huynh B, Douvier S, Riethmuller D, Clavel C, Birembaut P, Calenda V, Baudin M, Bory JP. Regression of high-grade cervical intraepithelial neoplasia with TG4001 targeted immunotherapy. Am J Obstet Gynecol. 2011, 204:169.e1-8.
95. Wallecha A, French C, Petit R, Singh R, Amin A, Rothman J. Lm-LLO-based immunotherapies and HPV-associated disease. J Oncol. 2012, 2012:542851.
96. Maciag PC, Radulovic S, Rothman J. The first clinical use of a live-attenuated Listeria monocytogenes vaccine: a Phase I safety study of Lm-LLO-E7 in patients with advanced carcinoma of the cervix. Vaccine. 2009, 27:3975–3983.
97. Andrade P, Deleo A, Visus C, Butterfield L, Argiris A, Ferris RL, University of Pittsburgh Cancer Institute, Pittsburgh, PA. Phase I adjuvant trial of multi-epitope p53 vaccine for patients with squamous cell carcinoma of the head and neck (SCCHN): a preliminary report. J Clin Oncol. 2009, 27:15s, (suppl; abstr 3012).
98. Forastiere AA, Goepfert H, Maor M, Pajak TF, Weber R, Morrison W, Glisson B, Trotti A, Ridge JA, Chao C, Peters G, Lee DJ, Leaf A, Ensley J, Cooper J. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003, 349:2091-2098.
99. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefèbvre JL, Greiner RH, Giralt J, Maingon P, Rolland F, Bolla M, Cognetti F, Bourhis J, Kirkpatrick A, van Glabbeke M; European Organization for Research and Treatment of Cancer Trial 22931. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004, 350:1945-1952.
100. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, Kish JA, Kim HE, Cmelak AJ, Rotman M, Machtay M, Ensley JF, Chao KS, Schultz CJ, Lee N, Fu KK; Radiation Therapy Oncology Group 9501/Intergroup. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004, 350:1937-1944.
101. Brockstein B, Haraf DJ, Rademaker AW, Kies MS, Stenson KM, Rosen F, Mittal BB, Pelzer H, Fung BB, Witt ME, Wenig B, Portugal L, Weichselbaum RW, Vokes EE. Patterns of failure, prognostic factors and survival in locoregionally advanced head and neck cancer treated with concomitant chemoradiotherapy: A 9-year, 337-patient, multi-institutional experience. Ann Oncol. 2004, 15:1179–1186.
102. Denis F, Garaud P, Bardet E, Alfonsi M, Sire C, Germain T, Bergerot P, Rhein B, Tortochaux J, Calais G. Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol. 2004, 22:69–76.
103. Hedman M, Bjork-Eriksson T, Mercke C, West C, Hesselius P, Brodin O. Comparison of predicted and clinical response to radiotherapy: A radiobiology modelling study. Acta Oncol. 2009, 48:584-590.
104. Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer. 1953, 6:963–968.
105. Braakhuis BJ, Tabor MP, Kummer JA, Leemans CR, Brakenhoff RH. A genetic explanation of Slaughter’s concept of field cancerization: Evidence and clinical implications. Cancer Res 2003, 63:1727-1730.
106. Cooper JS, Pajak TF, Rubin P, Tupchong L, Brady LW, Leibel SA, Laramore GE, Marcial VA, Davis LW, Cox JD, et al. Second malignancies in patients who have head and neck cancer: Incidence, effect on survival and implications based on the RTOG experience. Int J Radiat Oncol Biol Phys. 1989, 17:449–456.
107. Nieder C, Milas L, Ang KK. Tissue tolerance to reirradiation. Vaccine. 2000, 10:200–209.
108. Forastiere AA. Chemotherapy in the treatment of locally advanced head and neck cancer. J Surg Oncol. 2008, 97:701-707.
109. Leclerc M, Maingon P, Hamoir M, Dalban C, Calais G, Nuyts S, Serre A, Gregoire V. A dose escalation study with intensity modulated radiation therapy (IMRT) in T2N0, T2N1, T3N0 squamous cell carcinomas (SCC) of the oropharynx, larynx and hypopharynx using a simultaneous integrated boost (SIB) approach. Radiother Oncol. 2013, 106:333-340.
110. Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, Forastiere A, Gillison ML. Improved survival of patients with human papillomavirus - positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008, 100:261-269.
111. Psyrri A, Licitra L, Lacombe D, Schuuring E, Budach W, Ozsahin M, Knecht R, Vermorken JB, Langendijk JA. Strategies to promote translational research within the European Organisation for Research and Treatment of Cancer (EORTC) Head and Neck Cancer Group: a report from the Translational Research Subcommittee. Ann Oncol. 2010, 21:1952-1960.
112. Eriksen JG, Lassen P, Overgaard J. Do all patients with head and neck cancer benefit from radiotherapy and concurrent cetuximab? Lancet Oncol. 2010, 11:312-313.
113. Chen AM, Zahra T, Daly ME, Farwell DG, Luu Q, Gandour-Edwards R, Vaughan AT. Definitive radiation therapy without chemotherapy for human papillomavirus-positive head and neck cancer. Head Neck. 2013, 35:1652-1656.
114. Boscolo-Rizzo P, Gava A, Baggio V, Marchiori C, Stellin M, Fuson R, Lamon S, Da Mosto MC. Matched survival analysis in patients with locoregionally advanced resectable oropharyngeal carcinoma: platinum-based induction and concurrent chemoradiotherapy versus primary surgical resection. Int J Radiat Oncol Biol Phys. 2011, 80:154-160.
115. Bourhis J, Overgaard J, Audry H, Ang KK, Saunders M, Bernier J, Horiot JC, Le Maître A, Pajak TF, Poulsen MG, O’Sullivan B, Dobrowsky W, Hliniak A, Skladowski K, Hay JH, Pinto LH, Fallai C, Fu KK, Sylvester R, Pignon JP; Meta-Analysis of Radiotherapy in Carcinomas of Head and neck (MARCH) Collaborative Group. Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet. 2006, 368:843–854.
116. Machtay M, Moughan J, Trotti A, Garden AS, Weber RS, Cooper JS, Forastiere A, Ang KK. Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis. J Clin Oncol. 2008, 26:3582–3589.
117. Leonhardt FD, Quon H, Abrahão M, O’Malley BW Jr, Weinstein GS. Transoral robotic surgery for oropharyngeal carcinoma and its impact on patient-reported quality of life and function. Head Neck. 2012, 34:146–154.
118. Koutcher L, Sherman E, Fury M, Wolden S, Zhang Z, Mo Q, Stewart L, Schupak K, Gelblum D, Wong R, Kraus D, Shah J, Zelefsky M, Pfister D, Lee N. Concurrent cisplatin and radiation versus cetuximab and radiation for locally advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2011, 81:915-922.
119. Lefebvre JL, Pointreau Y, Rolland F, Alfonsi M, Baudoux A, Sire C, et al. Induction chemotherapy followed by either chemoradiotherapy or bioradiotherapy for larynx preservation: the TREMPLIN randomized phase II study. J Clin Oncol. 2013, 31:853-859.