
INTRODUCTION
Reperfusion strategy, including fibrinolytic therapy or primary percutaneous coronary intervention (PCI), is the key point to reduce mortality in ST-segment elevation myocardial infarction (STEMI). In daily practice, it is not rare that some patients may achieve reopening of the culprit artery without undergoing any reperfusion therapy, which is termed as spontaneous reperfusion (SR).
In previous studies, SR was defined as initial coronary flow of Thrombolysis in Myocardial Infarction (TIMI) [1] grade 3 assessed by emergent angiography [2–4]. Frequency of SR varies around 10%–30% [5–9]. Compared to non-SR (NSR) patients, SR is associated with a lower rate of short-term mortality or heart failure [2–5, 7, 9]. However, the relationship between SR and patient characteristics is still unclear. Moreover, fewer studies have reported the influence of SR on treatment strategy or long-term outcomes.
In the current study, we collected patients diagnosed with STEMI and tried to investigate the relation between clinical features and SR. We also explore the relationship of ST segment resolution and symptom relief and SR. Moreover, in-hospital events and long-term outcomes were compared between SR patients and NSR patients.
MATERIALS AND METHODS
Study population
In this retrospective study, STEMI patients, who had chest pain within 12 h and underwent emergency coronary angiography in one medical center from January 2009 to August 2010, were included. Exclusion criteria: 1) patients received thrombolytic therapy; 2) patients had prior myocardial infarction; 3) Patients refused angiography. Patients were divided into SR group and NSR group. SR referred to the culprit vessel achieved coronary blood flow of TIMI grade 3 identified by initial angiogram.
All patients received 300 mg of aspirin loading dose and 300 mg of clopidogrel, followed by 100 mg of aspirin maintenance dose and 75 mg of clopidogrel per day. Patient characteristics and in-hospital events were collected by questionnaires or medical records. In-hospital events referred to composite of any-cause death, reinfarction, congestive heart failure and cardiogenic shock [10]. Reinfarction was identified as an acute myocardial infarction occurred during the time of in the hospital after an incident myocardial infarction. Reinfarction was considered when ST elevation ≥ 0.1 mV recurs, or new pathognomonic Q waves appear, in at least two contiguous leads, particularly when associated with ischaemic symptoms for 20 min or longer. If the cTn concentration is elevated, but stable or decreasing at the time of suspected reinfarction, the diagnosis of reinfarction requires a 20% or greater increase of the cTn value in the second sample. If the initial cTn concentration is normal, the criteria for new acute myocardial infarction apply [11]. All biochemistry indexes were tested in the center laboratory within 24 hours.
Diagnostic criteria for STEMI
If following criteria were present: the presence of continuous chest pain lasting ≥ 20 minutes; and either 1) ST-segment elevation of ≥ 2 mm in at least 2 contiguous precordial leads, or 2) ST-segment elevation of ≥ 1 mm in at least 2 inferior leads, or 3) new left bundle branch block [11]. It was later confirmed by the elevation of myocardial biomarker (CK-MB or troponin) ≥ 2 folds of normal value.
Chest pain assessment
Chest pain was assessed with a numerical rating scale (NRS). Patients were asked to rate their pain on an 11-point scale, where 0 indicated no pain and 10 indicated the worst imaginable pain [12] at the admission (emergency room or at home). Reduction in pain for each patient was inquired before initiation of emergency coronary angiography. Symptom relief was defined as above 50% easement of pain as compared to the top level of pain for each patient.
ST segment resolution assessment
Electrocardiograms were examined at the admission and initiation of emergency coronary angiography. ST segment resolution was defined as 50–100% reduction in sum ST elevation.
Coronary angiography
Coronary angiography was performed using 5–6 French Judkins catheters through femoral or radial approaches [13]. The decision to perform PCI was made based on the discretion of operators. Usually, if patients in the SR group had significant stenosis in the target vessel or other vessels, we preferred to perform an elective PCI after 7 days of the initial angiography.
Long-term follow up
Follow up information was collected via phone call every 6 months. Primary endpoint was defined as major adverse cardiovascular and cerebrovascular events (MACCE), referring to composite of any-cause death, non-fatal cardiac arrest, acute coronary syndrome, congestive heart failure and stroke [14]. If any event occurred, primary endpoint was reached. This study was approved by the ethics committee of the hospital and the informed consents were obtained from patients. All authors have approved the manuscript and we confirm that all methods were performed in accordance with the relevant guidelines and regulations. The full disclosure of any potential conflict of interest has been declared.
Statistical analysis
Continuous variables are presented as mean ± SD or if not normally distributed as median with interquartile range. Two-sample t-tests or rank-sum tests were used to test group differences. For categorical variables, the data were summarized in percentages and X2 or Fisher exact test was used to assess group differences, where appropriate. Multivariate logistic regression analysis was performed to estimate odds ratios (OR) and 95% confidence intervals (95% CI) to identify independent predictors of SR. Long-term survival of MACCE was estimated with the Kaplan-Meier method. The Cox proportional hazard survival model was used to assess the association between SR and long-term outcomes while adjusting for potential confounders. A value of p < 0.05 was considered significant. All tests were two-sided, with a 5% level of significance. All analyses were performed using SPSS software 13.0 (SPSS Inc; Chicago, IL, USA).
RESULTS
Baseline characteristics
A total of 207 patients were eligible for analysis. Among them, 38 (18.4%) met the criteria of SR. Study flowchart is shown in Figure 1. In the NSR group, 130 (76.9%) patients got a TIMI flow grade 3 after emergent PCI. Patients in the SR group were younger (56.76 ± 12.89 vs. 61.80 ± 11.78, p = 0.020) and more smokers (73.7% vs. 53.3%, p = 0.022). The platelet (266.64 ± 66.91 × 109/L vs. 234.49 ± 66.86 × 109/L, p = 0.010), blood level of uric acid (298.03 ± 74.46 × μmol/L vs. 340.47 ± 106.89 × μmol/L, p = 0.025) and glucose (6.04 × mmol/L vs. 7.98 × mmol/L, p = 0.005) levels were statistically different between SR and NSR group (Table 1).
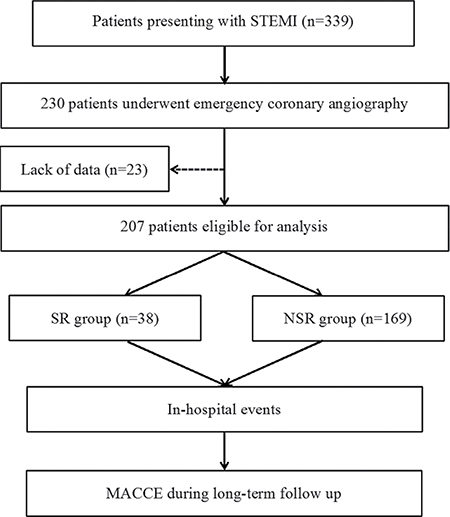
Figure 1: Flow chart of the study. MACCE = major and adverse cardiovascular and cerebrovascular events; NSR = non-spontaneous reperfusion; SR = spontaneous reperfusion; STEMI = ST-segment elevation myocardial infarction.
Table 1: Baseline characteristics
SR Group |
NSR Group |
P |
|
|---|---|---|---|
(n = 38) |
(n = 169) |
||
Age (years) |
56.76 ± 12.89 |
61.80 ± 11.78 |
0.020 |
Gender (Male/Female) |
34/4 |
131/38 |
0.098 |
Hypertension (%) |
18 (47.4) |
85 (50.3) |
0.744 |
Diabetes mellitus (%) |
8 (21.1) |
39 (23.1) |
0.788 |
Smoking (%) |
28 (73.7) |
98 (53.3) |
0.022 |
Anterior wall myocardial infarction (%) |
22 (57.9) |
69 (40.8) |
0.055 |
Systolic blood pressure (mm Hg) [median (Q1, Q3)] |
134 (112–147) |
135 (112–146) |
0.451 |
Diastolic blood pressure (mm Hg) [median (Q1, Q3)] |
79 (70–86) |
78 (66–88) |
0.761 |
Heart rate (/min) [median (Q1, Q3)] |
78 (67–86) |
75 (63–88) |
0.288 |
Time from symptom onset (h) [median (Q1, Q3)] |
4.9 (2.4–6) |
4.5 (2.5–5) |
0.505 |
EF (%) |
59 ± 9 |
56 ± 10 |
0.126 |
Time from symptom onset to PCI (min) [median (Q1, Q3)] |
195 (175–365) |
347 (210–395) |
0.419 |
Killip cardiac functional grading I-II (%) |
36 (94.7) |
162 (95.9) |
0.759 |
GP IIb/IIIa antagonist before procedures (%) |
3 (14.3) |
9 (8.6) |
0.398 |
Admission drug treatment |
|||
Aspirin (%) |
38 (100) |
159 (94.1) |
0.124 |
Clopidogrel (%) |
38 (100) |
158 (93.5) |
0.106 |
Beta-blockers (%) |
33 (86.8) |
123 (76.8) |
0.069 |
ACE inhibitors (%) |
37 (97.4) |
146 (86.45) |
0.056 |
Nitrates (%) |
36 (94.7) |
141 (83.49) |
0.267 |
Low-molecular-weight heparins (%) |
38 (100) |
167 (98.8) |
0.438 |
Platelet (109/L) |
266.64 ± 66.91 |
234.49 ± 66.86 |
0.010 |
Blood glucose (mmol/L) |
6.04 (4.30–7.36) |
7.98 (5.65–8.77) |
< 0.001 |
Uric acid (μmol/L) |
298.03 ± 74.46 |
340.47 ± 106.89 |
0.025 |
High density lipoprotein (mmol/L) |
1.04 ± 0.19 |
1.06 ± 0.24 |
0.687 |
Low density lipoprotein (mmol/L) |
2.62 ± 0.81 |
2.62 ± 0.80 |
0.982 |
Serum creatinine (mol/L) [median (Q1, Q3)] |
69.1 (61.0–77.8) |
76.9 (60.0–82.0) |
0.507 |
Data are presented as percentage or median (25th, 75th centile), Q1 = 25th quartiles, Q3 = 75th quartiles, where appropriate. ACE = angiotensin converting enzyme, EF = ejection fraction, GP = Glycoprotein, NSR = non-spontaneous reperfusion, PCI = percutaneous coronary intervention, SR = spontaneous reperfusion.
In the SR group, 22 (57.9%) patients had severe (≥ 90%) stenosis in culprit artery, while 10 (26.3%) patients with stenosis about 80–89%, 2 (5.3%) with stenosis about 70–79% and 4 (10.5%) with < 70% stenosis.
The culprit lesions were more distal in the SR group than those in the NSR group (26.3% vs. 9.5%, p < 0.005). Stents were placed in 4 (10.5%) patients of the SR group and 143 (84.6%) of the NSR group during the initial procedure (p < 0.001) (Table 2). Number of stents placed in emergent procedure was far less in the SR group than that of the NSR group (0.18 ± 0.61 vs. 1.16 ± 0.70, p < 0.001). After emergent and selective PCI, patients in the SR group still had a lower rate of stent placement than the NSR group (60.5% vs. 86.4%, p = 0.020) (Table 2). The total number of stents used for treating culprit lesions in the SR group was less than that in the NSR group (1.03 ± 1.05 vs. 1.59 ± 1.17, p = 0.007) (Table 2).
Table 2: Angiographic information
SR Group |
NSR Group |
P |
|
|---|---|---|---|
Infarct-related artery |
0.024 |
||
LAD (%) |
21 (55.3) |
71 (42.0) |
|
LCX (%) |
9 (23.7) |
23 (13.6) |
|
RCA (%) |
8 (21.1) |
75 (44.4) |
|
Infarct-related artery was LAD (%) |
21 (55.3) |
71 (42.0) |
0.233 |
Distal lesions (%) |
10 (26.3) |
16 (9.5) |
0.005 |
Vessel disease |
0.510 |
||
One-vessel disease (%) |
18 (47.4) |
74 (43.8) |
|
Two-vessel disease (%) |
12 (31.6) |
44 (26.0) |
|
Three-vessel disease (%) |
8 (21.1) |
51 (30.2) |
|
Number of stents placed in emergent procedure |
0.18 ± 0.61 |
1.16 ± 0.70 |
< 0.001 |
Emergent stent placement |
4 (10.5) |
143 (84.6) |
< 0.001 |
Total number of stents placed |
1.03 ± 1.05 |
1.59 ± 1.17 |
0.007 |
Patients undergoing PCI (%) |
23 (60.5) |
146 (86.4) |
0.020 |
Stent diameter (mm) |
3.44 ± 0.36 |
3.38 ± 0.45 |
0.545 |
Total stent length (mm) |
42.3 ± 18.4 |
45.5 ± 28.0 |
0.740 |
LAD = left anterior descending branch, LCX = left circumflex artery, NSR = non-spontaneous reperfusion, RCA = right coronary artery, PCI = percutaneous coronary Intervention, SR = spontaneous reperfusion.
Clinical predictors for SR
The coincidence rate of patients both with ≥ 70% ST-segment resolution and ≥ 70% relief of chest pain and SR was 100%.
Factors related to SR
Multiple variable analysis showed platelet (OR, 1.007; 95% CI: 1.001–1.013; p = 0.019), blood glucose (OR, 0.750; 95% CI: 0.622–0.905; p = 0.003), uric acid (OR, 0.993; 95% CI: 0.800–0.998; p = 0.011), and culprit lesion in distal lesions (OR, 0.107; 95% CI: 0.029–0.393; p = 0.001) or left anterior descending branch (LAD) (OR, 0.285; 95% CI: 0.105–0.711; p = 0.013) were independently associated with SR (Table 3).
Table 3: Factors related to spontaneous reperfusion
B |
OR (95% CI) |
P |
|
|---|---|---|---|
Age (years) |
−0.012 |
0.988 (0.945–1.033) |
0.592 |
Gender |
0.550 |
1.733 (0.391–7.682) |
0.469 |
EF (%) |
0.010 |
1.011 (0.600–1.060) |
0.677 |
Infarct-related artery was LAD |
−1.256 |
0.285 (0.105–0.711) |
0.013 |
Distal lesions |
−2.239 |
0.107 (0.029–0.393) |
0.001 |
Platelet (109/L) |
0.007 |
1.007 (1.001–1.013) |
0.019 |
Neutrophils (109/L) |
−0.030 |
0.970 (0.833–1.130) |
0.698 |
Blood glucose (mmol/L) |
−0.287 |
0.750 (0.622–0.905) |
0.003 |
Uric acid (μmol/L) |
−0.007 |
0.993 (0.800–0.998) |
0.011 |
High density lipoprotein (mmol/L) |
−0.696 |
0.499 (0.046–5.459) |
0.569 |
Low density lipoprotein (mmol/L) |
0.244 |
1.277 (0.711–2.291) |
0.413 |
Serum creatinine (mol/L) |
0.005 |
1.001 (0.962–1.062) |
0.662 |
CI = confidence interval, EF = ejection fraction, LAD = left anterior descending branch, OR = Odds ratio.
In-hospital events
Patients in the SR group had a significantly lower rate of in-hospital events as compared to the NSR group, including total events (0 vs. 22.5%, p < 0.001), any-cause death (0 vs. 5.9%), reinfarction (0 vs. 3.0%), congestive heart failure (0 vs. 7.1%) and cardiogenic shock (0 vs. 6.5%). The in-hospital mortality of the SR group had no statistically significant difference compared to those in the NSR group (0% vs. 5.9%, p = 0.125).
Long-term outcome
A total of 197 patients were enrolled in the follow up of the study. Median duration of the follow up was 41 months (Quartile 1: 37 months and Quartile 3: 45 months). The longest follow up was 53 months. There were 16 (8.1%) patients lost follow-up (4 patients in the SR group and 16 patients in the NSR group, 10.5% vs. 7.5%, p = 0.546). Patients in the SR group had a non-statistically lower rate of MACCE as compared to the NSR group (2.6% vs. 6.9%, p = 0.302) (Figure 2). Age (OR, 1.077; 95% CI: 1.014–1.143; p = 0.016) and hypertension (OR, 5.201, 95% CI: 1.134–23.855; p = 0.034) were independent predictors of long-term events (Table 4).
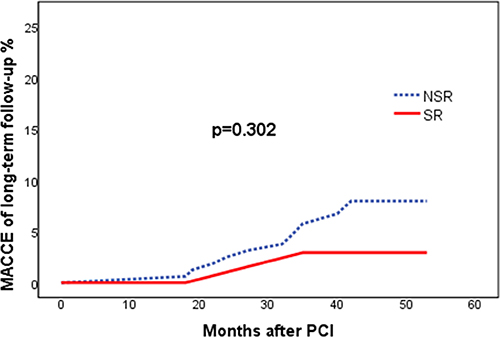
Figure 2: Kaplan-Meier curves for major and adverse cardiovascular and cerebrovascular events. MACCE = major and adverse cardiovascular and cerebrovascular events; NSR = non-spontaneous reperfusion; PCI = percutaneous coronary intervention; SR = spontaneous reperfusion.
Table 4: Cox proportional hazards regression of long-term clinical outcomes
OR (95% CI) |
P |
|
|---|---|---|
Age (years) |
1.077 (1.014–1.143) |
0.016 |
Gender |
1.960 (0.563–6.823) |
0.291 |
Hypertension |
5.201 (1.134–23.855) |
0.034 |
Diabetes mellitus |
0.714 (0.171–2.977) |
0.644 |
Smoking |
1.112 (0.277–4.456) |
0.881 |
SR |
0.232 (0.032–1.669) |
0.304 |
Killip cardiac functional grading I-II |
0.147 (0.064–0.381) |
0.147 |
CI = confidence interval, OR = Odds ratio, SR = spontaneous reperfusion.
As 23.1% of patients in the NSR group did not achieve blood flow of TIMI grade 3 finally, which may attribute to poor outcomes. We therefore analyzed the data again after excluding patients with slow blood flow. Eventually, patients in the SR (n = 38) group still had a lower rate of in-hospital events (0 vs. 16.9%, p = 0.007) compared to the NSR (n = 130) group and the two groups had the similar long-term outcomes (2.6% vs. 6.3%, p = 0.378). Age (OR, 1.095; 95% CI: 1.024–1.171; p = 0.008) and hypertension (OR, 5.818, 95% CI: 1.214–27.878; p = 0.028) were independent predictors of long-term events (Table 5).
Table 5: Cox proportional hazards regression of long-term clinical outcomes after excluding patients with slow blood flow
OR (95% CI) |
P |
|
|---|---|---|
Age (years) |
1.095 (1.024–1.171) |
0.008 |
Gender |
1.405 (0.335–5.899) |
0.642 |
Hypertension |
5.818 (1.214–27.878) |
0.028 |
Diabetes mellitus |
0.188 (0.022–1.650) |
0.132 |
Smoking |
0.773 (0.188–3.173) |
0.721 |
SR |
0.522 (0.062–4.365) |
0.548 |
Killip cardiac functional grading I-II |
0.629 (0.173–2.278) |
0.480 |
CI = confidence interval, OR = Odds ratio, SR = spontaneous reperfusion.
DISCUSSION
In this study, we found the incidence of SR was 18.4%. Combination of ≥ 70% ST-segment resolution with ≥ 70% of relief in pain could clinically predict SR with high accuracy. Platelet count, lower levels of blood glucose and uric acid, distal lesions and LAD as infarct-related artery (IRA) were independently associated with SR. More importantly, SR may result in lower rate of in-hospital events despite less stent placement.
Previous studies [6–8] have suggested that STEMI patients with SR had improved left ventricular function, lower incidence of congestive heart failure and decreased short-term mortality, as compared to patients without SR. In the current study, we also indicated significantly better in-hospital outcome among patients with SR. The possible mechanism could be: 1) SR may be associated with earlier opening time in occluded arteries, resulting in smaller myocardial infarct size. 2) In our study, 23.1% of patients in the NSR group did not achieve blood flow of TIMI grade 3, which may result in poor outcomes. Furthermore, when we only compared patients having TIMI grade 3, SR was still associated with lower in-hospital events. We therefore speculate that the SR group might have more effective reperfusion not only by the reopening of epicardial arteries but also in the microcirculatory level, as compared to patients in the NSR group. 3) Our data demonstrated that stent placement could be safely deferred in the patients with SR. The SR group had a lower rate of stent placement (10.5% vs. 84.6% in emergent procedure and 60.5% vs. 86.4% totally) which might be associated with less procedure-related complications as compared to NSR group. Future studies are needed to confirm our speculations regarding the mechanism of benefit associated with SR.
Although SR was associated with favorable in-hospital events, but no significantly difference was verified with regarding to the long-term follow up. The MACCE were 2.6% in SR group and 6.9% in NSR group, which were relatively lower compared to previous studies [15]. This may somewhat reflect the improvement on management of STEMI and therefore diminish the gap on prognosis between the two groups. Moreover, patient amount was relatively small in the current study, which may impair the power of statistical analysis.
In fibrinolytic era, complete resolution of ST segment elevation, early peaking of biomarkers, reperfusion arrhythmias and relief of chest pain, has been investigated for noninvasive assessment of TIMI grade 3 after thrombolytic therapy, indicating patency of the culprit vessel [16–18]. Even so, clinical features are still considered to be poor markers of reperfusion, without any combinations of them being more able to predictive coronary artery patency more reliably [19]. In our study, when ST segment resolution ≥ 70% and symptom relief ≥ 70% were combined to predict SR, the coincidence rate of patients both with ≥ 70% ST-segment resolution and ≥ 70% relief of chest pain and SR was 100%. Thus, it may be feasible for physicians to accurately identify the restoration of coronary blood flow in patients with STEMI, based on those clinical features.
Since endogenous fibrinolysis or pretreatment with anti-thrombotic agents is regarded to be conducive to SR [2], some clinical characteristics may be associated with SR. Rimar D [10], et al. found the incidence of SR was 4% of STEMI patients, and old age, preinfarction angina, hypertension, non-Q wave myocardial infarction, and Killip class I on admission were independent variables associated with SR. However, Stone GW [2], et al. indicated the rate of SR is 16% but no baseline characteristics clearly predicted SR. In this study, we founded that higher level of uric acid and blood glucose were independently related to SR. Akpek M [20], et al. reported uric acid had a negative relation with TIMI blood flow in STEMI patients undergoing primary PCI. Timmer JR [21], et al. showed hyperglycemia could predict an initial TIMI flow grade 0 to 2 before primary PCI in STEMI patients. Theoretically, uric acid may promote activation of clotting factors, inhibit natural anticoagulant and lead to mural thrombosis through inflammation or platelet pathway, therefore inhibit thrombus autolysis [22–23]. Hyperglycemia could increase activation platelet, damage endothelium-dependent vasodilation and increased inflammatory responses, finally affect platelet function, blood coagulation and fibrinolysis, leading to thrombosis hard to dissolve [24–25]. Interestingly, our data showed patients in SR group had lower platelet levels compared to NSR group. We speculate that these patients may have more severe platelet consumption due to higher thrombotic burden in the culprit lesion. Further studies are needed to elucidate the mechanism.
Study limitations
Limitations of the study include that all data were collected from one institution which may leave selection bias. Moreover, we could not identify the exact duration between coronary blockage and reopening in SR patients. Also, we did not have data about peak levels of CK-MB or troponin to represent and compare the myocardial damage between the SR and NSR groups. Additionally, we speculated that less PCIs might be associated less procedure-related complications, which may partly account for the favorable outcome in the SR group. However, no consolidate data supported it. Further studies are needed to confirm this point. Finally, this study could not reflect influence of new anti-thrombosis agents on SR.
CONCLUSIONS
Spontaneous reperfusion is not rare daily practice. SR is associated with favorable outcomes, despite of less stent usage. Stent placement could be safely deferred in the patients with SR.
CONFLICTS OF INTEREST
There were no potential conflicts of interest.
FUNDING
This study was supported by the grant 81470491 from the National Natural Science Foundation of China to Dr. Li.
REFERENCES
1. Chesebro JH, Knatterud G, Roberts R, Borer J, Cohen LS, Dalen J, Dodge HT, Francis CK, Hillis D, Ludbrook P, Markis JE, Mueller H, Passamani ER, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I: a comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation. 1987; 76:142–54.
2. Stone GW, Cox D, Garcia E, Brodie BR, Morice MC, Griffin J, Mattos L, Lansky AJ, O'Neill WW, Grines CL. Normal flow (TIMI-3) before mechanical reperfusion therapy is an independent determinant of survival in acute myocardial infarction: analysis from the primary angioplasty in myocardial infarction trials. Circulation. 2001; 104:636–41.
3. Cannon CP. Importance of TIMI 3 flow. Circulation. 2001; 104:624–6.
4. Lekston A, Hudzik B, Szkodziński J, Gasior M, Tajstra M, Kalarus Z, Szyguła-Jurkiewicz B, Poloński L. Spontaneous reperfusion before intervention improves immediate but not long-term prognosis in diabetic patients with ST-segment elevation myocardial infarction and multivessel coronary artery disease. Cardiol J. 2013; 20:378–84.
5. Fefer P, Hod H, Hammerman H, Boyko V, Behar S, Matetzky S. Relation of clinically defined spontaneous reperfusion to outcome in ST-elevation myocardial infarction. Am J Cardiol. 2009; 103:149–53.
6. Erden EC, Erden I, Türker Y, Aslantaş Y, Yalçın S, Karabacak A. Amount of ST wave resolution in patients with and without spontaneous coronary reperfusion in the infarct-related artery after primary PCI: an observational study. Anadolu Kardiyol Derg. 2012; 12:30–4.
7. Terkelsen CJ, Kaltoft AK, Nørgaard BL, Bøttcher M, Lassen JF, Clausen K, Nielsen SS, Thuesen L, Nielsen TT, Bøtker HE, Andersen HR. ST changes before and during primary percutaneous coronary intervention predict final infarct size in patients with ST elevation myocardial infarction. J Electrocardiol. 2009; 42:64–72.
8. Bainey KR, Fu Y, Wagner GS, Goodman SG, Ross A, Granger CB, Van de Werf F, Armstrong PW; ASSENT 4 PCI Investigators. Spontaneous reperfusion in ST-elevation myocardial infarction: comparison of angiographic and electrocardiographic assessments. Am Heart J. 2008; 156:248–55.
9. Leibowitz D, Gerganski P, Nowatzky J, Weiss AT, Rott D. Relation of spontaneous reperfusion in ST-elevation myocardial infarction to more distal coronary culprit narrowings. Am Heart J. 2008; 101:308–10.
10. Rimar D, Crystal E, Battler A, Gottlieb S, Freimark D, Hod H, Boyko V, Mandelzweig L, Behar S, Leor J. Improved prognosis of patients presenting with clinical markers of spontaneous reperfusion during acute myocardial infarction. Heart. 2002; 88:352–6.
11. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Thygesen K, Alpert JS, White HD, Jaffe AS, Katus HA, Apple FS, Lindahl B, et al, and Writing Group on the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction, and ESC Committee for Practice Guidelines (CPG). Third universal definition of myocardial infarction. Eur Heart J. 2012; 33:2551–67.
12. Breivik EK, Björnsson GA, Skovlund E. A comparison of pain rating scales by sampling from clinical trial data. Clin J Pain. 2000; 16:22–8.
13. Lavi S, Rihal CS, Yang EH, Fassa AA, Elesber A, Lennon RJ, Mathew V, David HR Jr, Lerman A. The effect of drug eluting stents on cardiovascular events in patients with intermediate lesions and borderline fractional flow reserve. Catheter Cardiovasc Interv. 2007; 70:525–31.
14. Sabaté S, Mases A, Guilera N, Canet J, Castillo J, Orrego C, Sabaté A, Fita G, Parramón F, Paniagua P, Rodríguez A, Sabaté M, Martin B, et al, and ANESCARDIOCAT Group. Incidence and predictors of major perioperative adverse cardiac and cerebrovascular events in non-cardiac surgery. Br J Anaesth. 2011; 107:879–90.
15. Jing Li, Elrashidi MY, Flammer AJ, Lennon RJ, Bell MR, Holmes DR, Bresnahan JF, Rihal CS, Lerman LO, Lerman A. Long-term outcomes of fractional flow reserve-guided vs. angiography-guided percutaneous coronary intervention in contemporary practice. Eur Heart J. 2013; 34:1375–83.
16. Christenson RH, Ohman EM, Topol EJ, Peck S, Newby LK, Duh SH, Kereiakes DJ, Worley SJ, Alosozana GL, Wall TC, Califf RM. Assessment of coronary reperfusion after thrombolysis with a model combining myoglobin, creatine kinase-MB, and clinical variables. TAMI-7 Study Group. Thrombolysis and Angioplasty in Myocardial Infarction-7. Circulation. 1997; 96:1776–82.
17. Califf RM, O'Neil W, Stack RS, Aronson L, Mark DB, Mantell S, George BS, Candela RJ, Kereiakes DJ, Abbottsmith C, Topol EJ. TAMI Study Group. Failure of simple clinical measurements to predict perfusion status after intravenous thrombolysis. Ann Intern Med. 1988; 108:658–62.
18. Remppis A, Scheffold T, Karrer O, Zehelein J, Hamm C, Grünig E, Bode C, Kübler W, Katus HA. Assessment of reperfusion of the infarct zone after acute myocardial infarction by serial cardiac troponin T measurements in serum. Br Heart J. 1994; 71:242–8.
19. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004; 44:E1–E211.
20. Akpek M, Kaya MG, Uyarel H, Yarlioglues M, Kalay N, Gunebakmaz O, Dogdu O, Ardic I, Elcik D, Sahin O, Oguzhan A, Ergin A, Gibson CM. The association of serum uric acid levels on coronary flow in patients with STEMI undergoing primary PCI. Atherosclerosis. 2011; 219:334–41.
21. Timmer JR, Ottervanger JP, de Boer MJ, Dambrink JH, Hoorntje JC, Gosselink AT, Suryapranata H, Zijlstra F, van 't Hof AW. Zwolle Myocardial Infarction Study Group. Hyperglycemia is an important predictor of impaired coronary flow before reperfusion therapy in ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2005; 45:999–1002.
22. Ruggiero C, Cherubini A, Ble A, Bos AJ, Maggio M, Dixit VD, Lauretani F, Bandinelli S, Senin U, Ferrucci L. Uric acid and inflammatory markers. Eur Heart J. 2006; 27:1174–81.
23. Kanellis J, Watanabe S, Li JH, Kang DH, Li P, Nakagawa T, Wamsley A, Sheikh-Hamad D, Lan HY, Feng L, Johnson RJ. Uric acid stimulates monocyte chemoattractant protein-1 production in vascular smooth muscle cells via mitogen-activated protein kinase and cyclooxygenase-2. Hypertension. 2003; 416:1287–93.
24. Esposito K, Nappo F, Marfella R, Giugliano G, Giugliano F, Ciotola M, Quagliaro L, Ceriello A, Giugliano D. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation. 2002; 106:2067–72.
25. Pinto DS, Kirtane AJ, Pride YB, Murphy SA, Sabatine MS, Cannon CP, Gibson CM, and CLARITY-TIMI 28 Investigators. Association of blood glucose with angiographic and clinical outcomes among patients with ST-segment elevation myocardial infarction (from the CLARITY-TIMI-28 study). Am J Cardiol. 2008; 101:303–07.