
INTRODUCTION
Esophageal cancer (EC) is one of the most common and aggressive malignancies globally, resulting in more than 400,000 deaths each year [1]. Despite the significant improvement in its diagnosis and treatment in recent decades, the prognosis of EC patients remains poor. Radical esophagectomy and subsequent lymph node (LN) dissection are considered the best option for potentially curable EC patients. The status of LN metastasis is a key factor that closely relates with the long-term survival of EC patients who underwent surgery [2-5]. Both involved LN and retrieved LN count are prognostic [6, 7]. However, insufficient LN retrieval would happen because of various factors such as physical condition of each patient, surgical or pathological diagnosing skills in clinical practice, and the number of the pathologically involved lymph nodes is significantly influenced by the number of the removed LNs.
Recent studies have proposed a superior prognostic factor, the positive lymph node ratio (LNR), for EC patients especially when insufficient LN retrieval happened [8-10]. LNR, also known as metastatic lymph node ratio (MLNR), is the ratio of the number of positive lymph nodes to the total number of dissected lymph nodes. LNR has been proposed to be used to assess the prognoses of several other solid cancers, such as colorectal cancer, non-small-cell lung cancer and pancreatic adenocarcinoma [11-13]. However, its prognostic significance in EC patients is still controversial as the existed evidence did not completely agree with each other. We sought to examine the relationship between LNR and prognosis of EC by integrating all available published data.
RESULTS
Eligible studies
We identified 1,448 potentially relevant records according to the search strategy. 1,376 studies were excluded after checking the corresponding title and abstract. Then the full texts of 72 articles were carefully reviewed. A total of 18 studies [8, 9, 14-29] were finally included in this meta-analysis according to the eligible criteria. Figure 1 summarized the flow chart.
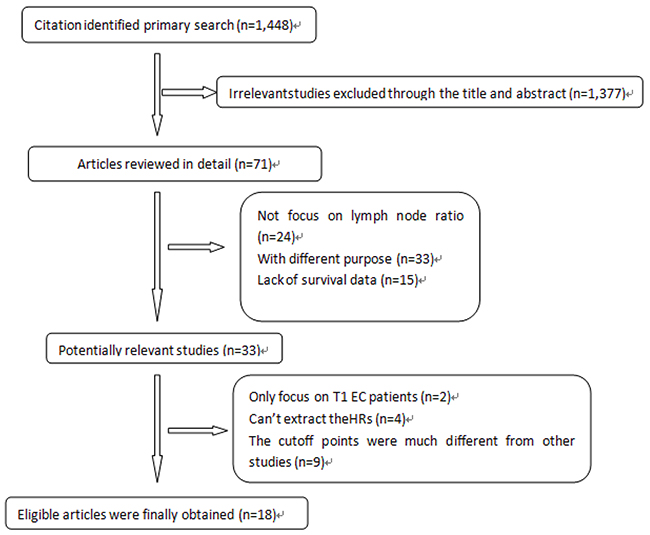
Figure 1: Profile summarizing the trial flow.
Characteristics of the included studies
Our meta-analysis was composed of 18 studies including 7,664 EC patients. These studies were conducted between 2000 and 2016. The characteristics of all included studies were summarized in Table 1. We listed the HRs and their 95% CIs under specific cut-off values of the LNRs of the collected studies in Table 2. Since the determined cut-off values of the LNRs varied from study to study, we uniformed the cutoffs for the LNRs according to the selection in the majority of studies. Therefore, 0.3(representing the range from 0.2 to 0.4) and 0.5(representing the range from 0.4 to 0.6) were selected as the cutoff values of LNR in our study.
Table 1: Characteristic of the included studies
First author |
Year |
Patient age |
T-stage |
N-stage |
Case number(n) |
Country |
Cut-off point |
Resected nodes (median/average) |
Surgical approach |
|---|---|---|---|---|---|---|---|---|---|
Castigliano |
2012 |
- |
Ttis-4 |
N0-3 |
347 |
USA |
0.1,0.2,0.3 |
14 |
Thoracotomy/Nonthoracotomy |
Chen |
2015 |
56 |
T1-4 |
N0-3 |
496 |
China |
0.15,0.3 |
7 |
_ |
Zhang |
2014 |
62 |
T1-4 |
N0-3 |
337 |
China |
0.3,0.6 |
_ |
_ |
Lagergren |
2015 |
64 |
T0-4 |
_ |
606 |
England |
0.14,0.37 |
_ |
transhiatal or transthoracic esophagectomy |
Wang |
2015 |
60.6 |
_ |
N0-3 |
209 |
China |
0.2 |
_ |
_ |
Wu |
2013 |
_ |
T0-4a |
_ |
205 |
China |
0.1,0.2,0.3, 0.4,0.5 |
10.2 |
two-field lymph node dissection/three-field lymph node dissection |
Tang |
2013 |
_ |
T1-4 |
_ |
170 |
China |
0.32 |
_ |
_ |
Sandick |
2001 |
_ |
T1-4 |
N0-3 |
111 |
Netherlands. |
0.3 |
12 |
transhiatal technique |
Wijnhoven |
2007 |
63 |
T1-4 |
_ |
292 |
Australia |
0.2 |
11 |
transhiatal technique |
Zhang |
2016 |
_ |
T1-4 |
N0-3 |
389 |
China |
0.3,0.6 |
17.5 |
_ |
Liu |
2010 |
54.8 |
_ |
_ |
1325 |
China |
0.25,0.5 |
21.2 |
transhiatal or transthoracic esophagectomy |
Shao |
2016 |
_ |
T0-4a |
N0-3 |
916 |
China |
0.1,0.35 |
12 |
transthoracic esophagectomy |
Zafirellis |
2002 |
_ |
T0-4 |
N1-2 |
156 |
China |
0.2 |
13 |
thoracoabdominal incision |
Tan |
2014 |
57 |
T0-4 |
N0-3 |
700 |
China |
0.25 |
16.4 |
tri-incisional approach |
Bogoevski |
2008 |
61 |
T1-4 |
N0-1 |
235 |
Germany |
0.11,0.33 |
18 |
transhiatal or transthoracic esophagectomy |
Hsu |
2009 |
63.8 |
T1-4 |
N0-1 |
488 |
Taiwan |
0.2 |
22 |
Tri-incisional/Transhiatal/Thoracoabdominal/IVOR Lewis |
Mariette |
2008 |
58 |
T1-3 |
N0-1 |
509 |
Australia |
0.2 |
_ |
transthoracic en bloc esophagectomy |
Wilson |
2008 |
62 |
T1-3 |
N0-3 |
173 |
USA |
0.25,0.5 |
_ |
Tri-incisional/Transhiatal/Thoracoabdominal/IVOR Lewis |
Table 2: Summary table of HRs (95% CI) and HR calculation
First author |
Year |
HR |
LL |
UL |
Cut-point |
|---|---|---|---|---|---|
Castigliano |
2012 |
2.04 |
0.06 |
67.5 |
0.3 |
Chen |
2015 |
2.35 |
1.64 |
3.78 |
0.3 |
Zhang |
2014 |
2.25 |
1.03 |
4.91 |
0.3 |
2.564 |
1.33 |
4.942 |
0.6 |
||
Lagergren |
2015 |
2.22 |
1.31 |
3.76 |
0.37 |
Wang |
2015 |
3.059 |
2.114 |
4.426 |
0.2 |
Wu |
2013 |
2.72 |
1 |
7.38 |
0.3 |
2.315 |
0.775 |
6.912 |
0.5 |
||
Tang |
2013 |
2.44 |
1.79 |
3.33 |
0.32 |
Sandick |
2001 |
1.87 |
0.72 |
4.81 |
0.3 |
Wijnhoven |
2007 |
1.98 |
1.029 |
3.79 |
0.2 |
Zhang |
2016 |
2.36 |
1.0135 |
5.5 |
0.3 |
2.82 |
1.578 |
5.04 |
0.6 |
||
Liu |
2010 |
1.584 |
1.05 |
2.38 |
0.25 |
1.644 |
1.143 |
2.363 |
0.5 |
||
Shao |
2016 |
2.08 |
1.31 |
3.3 |
0.35 |
Zafirellis |
2002 |
4.55 |
2.94 |
7.14 |
0.2 |
Tan |
2014 |
1.94 |
1.45 |
2.59 |
0.25 |
Bogoevski |
2008 |
1.656 |
0.98 |
2.81 |
0.33 |
Hsu |
2009 |
2.97 |
2.096 |
4.196 |
0.2 |
Mariette |
2008 |
2.65 |
2.02 |
3.48 |
0.2 |
Wilson |
2008 |
1.11 |
0.54 |
2.27 |
0.25 |
1.53 |
0.8 |
2.94 |
0.5 |
Quantitative data synthesis
As shown in Figure 2, patients with an LNR of 0.3 or greater had an increased risk of long-term deaths compared to those with a LNR less than 0.3(HR=2.33; 95% CI 2.03-2.68; P<0.01). There was no significant heterogeneity (I2=32.2%, P=0.09). As shown in Figure 3, patients with an LNR of 0.5 or greater was also associated with decreased OS (HR=1.95; 95% CI 1.52-2.50; P<0.01; heterogeneity test, I2=0.0%, P=0.45). Sensitivity analyses did not change the trends. After the exclusion of results from studies using multivariate analysis, patients with an LNR of 0.3 or greater also had an increased risk of deaths compared to those with an LNR less than 0.3 (HR=2.27; 95% CI 1.93-2.26; P<0.05). All studies using an LNR of 0.5 as cut-off were multivariate setting, thus sensitivity analysis was unavailable.
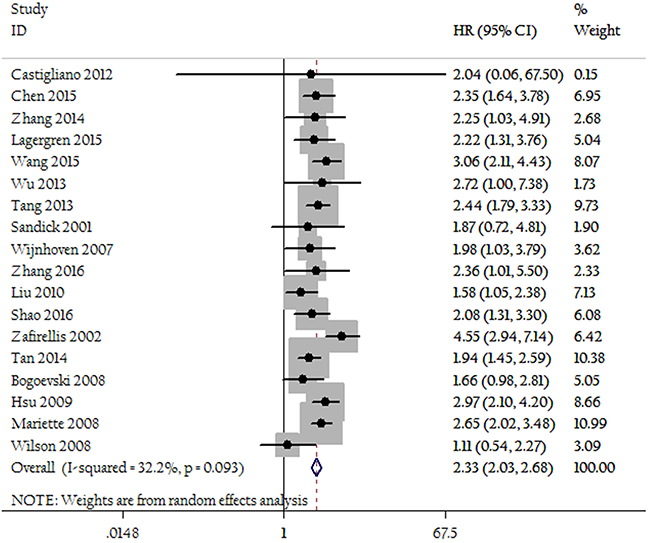
Figure 2: Forest plots show the association between LNR of 0.3 and overall survival.
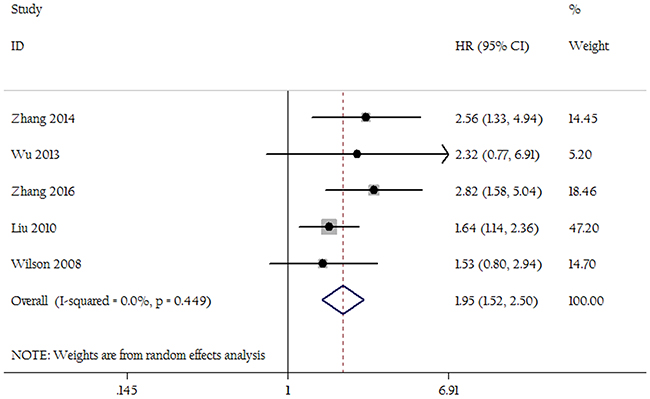
Figure 3: Forest plots show the association between LNR of 0.5 and overall survival.
Publication bias
The funnel plot and Egger’s test were performed for the overall comparison. No obvious visual asymmetry was observed in funnel plots (Figures 4 and 5) for OS, and the P values of the Egger’s test were all greater than 0.05.
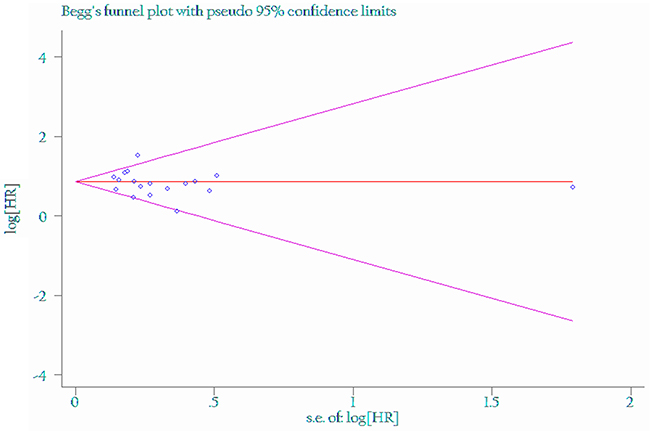
Figure 4: Funnel plot of the association between LNR of 0.3 and overall survival.
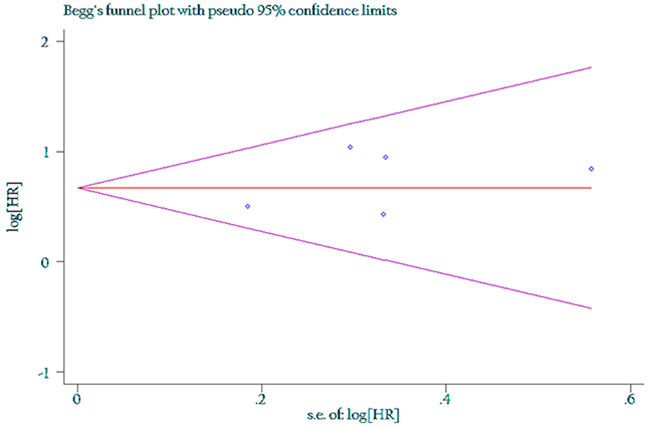
Figure 5: Funnel plot of the association between LNR of 0.5 and overall survival.
DISCUSSION
Tumor staging system has multiple roles: prognosis prediction, determination of treatment strategy, and the adjustment for the comparison of treatment effects. The status of LN metastasis in patients with esophageal cancer has been considered a pivotal prognostic factor [30, 31]. Since the accuracy of the number of metastatic LNs depends on the number of nodes removed, the 7th edition AJCC TNM staging system suggested more than 12 nodes should be sampled. To allow best predictive outcome, Peyre et al. have suggested that the number of removed nodes should range from 23 to 29 [32]. Considering the total number of LNs retrieved may be affected by many factors, LNR emerged as a more simple strategy to make up for insufficient LN retrieval. Furthermore, emerging evidence indicates that LNR showed better prognostic value than metastatic LN number for esophageal cancer [17, 33, 34].
Combining the available data of 18 studies, our results confirmed that no matter the cutoff point was 0.3 or 0.5, higher LNR is significantly associated with a poorer survival of esophageal cancer. Observations on other malignancies from many other studies were consistent with ours that LNR could be a prognostic factor. Sun and his coworkers [35] published a meta-analysis involving12 observational studies, showing that higher LNR was significantly associated with a poorer survival of NSCLC(OS HR=1.93; 95% CI 1.64-2.28, DDS HR=1.82; 95% CI 1.55-2.14). A previous meta-analysis also indicated that LNR was a prognostic factor with regard to overall survival for breast cancer and colorectal cancer [36, 37].
Since the different extent of lymph node dissection and the pathological type of esophageal cancer, various cutoffs of LNR have been used in different studies. For breast cancer, Liu et al. suggested that the suitable cutoff point were 0.2 and 0.65 [36]. In the present study, we determined 0.3 and 0.5 as cutoff values since they were used in most of the articles.
This is the first study to comprehensively answer the prognostic role of LNR in EC patients. However, there are several limitations. First, it was based on retrospective analyses; prospective analysis is needed to further clarify these issues. Second, the different cutoff values for defining high LNR may have contributed to heterogeneity. Third, we can’t rule out the effects of the chemotherapeutic agents or radiotherapy after surgery or concurrent radiochemotherapy (CRT) before surgery as such information was not provided in the original reports. In addition, we cannot study adenocarcinoma and squamous cell carcinoma, or the location of the tumor separately for insufficient information provided by primary studies; we can distinguish the prognostic roles of LNR on these subtypes. Further studies are warranted.
In conclusion, this meta-analysis confirmed that LNR was a strong predictor of survival in patients with EC. The appropriate incorporation of LNR into the prognostic system or the treatment determination (such as postoperative radiotherapy) of EC should be discussed.
MATERIALS AND METHODS
Literature search
All relevant articles were retrieved by searching PubMed, Embase and the Central Registry of Controlled Trials of the Cochrane Library using a combination of the terms: (“EC or “esophageal carcinoma” or “esophageal cancer”) and ratio. No restriction by language or year was set in the search. The last research time was October 23, 2016. References from relevant articles, including review papers, were also reviewed.
Inclusion criteria and exclusion criteria
Eligible studies should meet the following criteria: (1) studies which evaluated the association between LNR and prognosis of EC. (2) studies published in English or Chinese regardless of publication time.(3) the original papers containing enough data. Studies failed to meet the inclusion criteria will be excluded.
Data collection
Two authors searched eligible studies and extracted information independently and finally negotiate to reach consensus. Details of publication characteristics such as first author’s name, publication year, middle/mean age of study sample, sample size, T stage, N stage, cutoff point and hazard ratio (HR) and the corresponding 95% CI were collected from each eligible publication. If the results of univariate and multivariate analysis were both reported in a study, the former was chosen. If precise HR (95% CI) were provided in the study, we used them directly, otherwise we used Engauge Digitizer version 2.11 software to extract relevant numerical value from survival curves and calculate the HR(95% CI) when only Kaplan-Meier survival curves were provided [38, 39].
Statistical analysis
Cochran’s Q-statistic test and I2 test were used to calculate the heterogeneity. As to Q-statistic, P < 0.05 was considered to have statistical significance. For I2 statistics, I2 < 25% indicated no heterogeneity; I2 = 25–50% indicated moderate heterogeneity; and I2 > 50% indicated strong heterogeneity [40, 41]. A random effects model was applied to minimize the impact of any potential bias. Subgroup analysis and sensitivity analysis were performed. Sensitivity analyses were conducted to assess the strength of our findings by excluding one study at a time. Publication bias was investigated by funnel plots and by Egger’s test. All statistical analyses were performed with STATA 11.0 software.
Of note, patients with LNR=0 was the reference group in many studies. We used LNR=0 as the link to calculate relevant HR and the standard error for the log HR was , in which log HRAC was the log HR for the direct comparison of patients who with LNR equal to or greater than the cut-points versus those who with LNR=0, and log HRBC were log HR for the direct comparison of patients who with LNR between 0 and a number less than the cut-points versus those who with LNR=0. SE (logHR) was the standard error of the log HR for the direct comparisons.
CONFLICTS OF INTEREST
We declare no conflicts of interests.
REFERENCES
1. Amini N, Spolverato G, Kim Y, Squires MH, Poultsides GA, Fields R, Schmidt C, Weber SM, Votanopoulos K, Maithel SK, Pawlik TM. Clinicopathological features and prognosis of gastric cardia adenocarcinoma: a multiinstitutional US study. J Surg Oncol. 2015; 111:285-292.
2. Peyre CG, Hagen JA, DeMeester SR, Van Lanschot JJ, Hölscher A, Law S, Ruol A, Ancona E, Griffin SM, Altorki NK, Rice TW, Wong J, Lerut T, DeMeester TR. Predicting systemic disease in patients with esophageal cancer after esophagectomy: a multinational study on thesignificance of the number of involved lymph nodes. Ann Surg. 2008; 248:979-985.
3. Purwar P, Bambarkar S, Jiwnani S, Pramesh CS. Prognostic significance of lymph node counts in operable esophageal cancer. Ann Thorac Surg. 2014; 97:2229.
4. Kawahara K, Maekawa T, Okabayashi K, Shiraishi T, Yoshinaga Y, Yoneda S, Hideshima T, Shirakusa T. The number of lymph node metastases influences survival in esophageal cancer. J Surg Oncol. 1998; 67:160-163.
5. Zhang HL, Chen LQ, Liu RL, Shi YT, He M, Meng XL, Bai SX, Ping YM. The number of lymph node metastases influences survival and International Union Against Cancer tumor-node-metastasis classification for esophageal squamous cell carcinoma. Dis Esophagus. 2010; 23:53-58.
6. Altorki NK, Zhou XK, Stiles B, Port JL, Paul S, Lee PC, Mazumdar M. Total number of resected lymph nodes predicts survival in esophageal cancer. Ann Surg. 2008; 248:221–226.
7. Sisic L, Blank S, Weichert W, Jager D, Springfeld C, Hochreiter M, Buchler M, Ott K. Prognostic impact of lymph node involvement and the extent of lymphadenectomy (LAD) in adenocarcinoma of the esophagogastric junction (AEG). Langenbecks Arch Surg. 2013; 398:973-981.
8. Tan Z, Ma G, Yang H, Zhang L, Rong T, Lin P. Can lymphnode ratio replace pn categories in the tumor-node metastasis classification system for esophageal cancer? J Thorac Oncol. 2014; 9:1214–1221.
9. Mariette C, Piessen G, Briez N, Triboulet JP. The number of metastatic lymph nodes and the ratio between metastatic and examined lymph nodes are independent prognostic factors in esophageal cancer regardless of neoadjuvant chemoradiation or lymphadenectomy extent. Ann Surg. 2008; 247:365–371.
10. Kelty CJ, Kennedy CW, Falk GL. Ratio of metastatic lymphnodes to total number of nodes resected is prognostic for survival in esophageal carcinoma. J Thorac Oncol. 2010; 5:1467–1471.
11. Costi R, Beggi F, Reggiani V, Ricco M, Crafa P, Bersanelli M, Tartamella F, Violi V, Roncoroni L, Sarli L. Lymph node ratio improves TNM and Astler- Coller’s assessment of colorectal cancer prognosis: an analysis of 761 node positive cases. J Gastrointest Surg. 2014; 18:1824–1836.
12. Wang CL, Li Y, Yue DS, Zhang LM, Zhang ZF, Sun BS. Value of the metastatic lymph node ratio for predicting the prognosis of non-small-cell lung cancer patients. World J Surg. 2012; 36:455–462.
13. Liu ZQ, Xiao ZW, Luo GP, Liu L, Liu C, Xu J, Long J, Ni QX, Yu XJ. Effect of the number of positive lymph nodes and lymph node ratio on prognosis of patients after resection of pancreatic adenocarcinoma. Hepatobiliary Pancreat Dis Int. 2014; 13:634–641.
14. Bhamidipati CM, Stukenborg GJ, Thomas CJ, Lau CL, Kozower BD, Jones DR. Pathologic lymph node ratio is a predictor of survival in esophageal cancer. Ann Thorac Surg. 2012; 94:1643-1651.
15. Chen W, Deng WY, Li N, Shen W, Zhang C, Liu JY, Luo SX. Lymph node ratio as an alternative to the number of metastatic lymph nodes for the prediction of esophageal carcinoma patient survival. Dig Dis Sci. 2015; 60:2771-2776.
16. Zhang H, Chen C, Yue J, Ma M, Ma Z, Yu Z. Effect of number of metastatic lymph nodes and metastatic lymph node ratio on the prognosis in patients with adenocarcinoma of the esophagogastric junction after curative resection. Zhonghua Zhong Liu Za Zhi. 2014; 36:141-146.
17. Lagergren J, Mattsson F, Zylstra J, Chang F, Gossage J, Mason R, Lagergren P, Davies A. Extent of lymphadenectomy and prognosis after esophageal cancer surgery. JAMA Surg. 2016; 151:32-39.
18. Wang N, Jia Y, Wang J, Wang X, Bao C, Song Q, Tan B, Cheng Y. Prognostic significance of lymph node ratio in esophageal cancer. Tumour Biol. 2015; 36:2335-2341.
19. Wu N, Chen Z, Pang L, Ma Q, Chen G. Prognostic significance of lymph node characteristics on survival in esophageal squamous cell carcinomas. Wien Klin Wochenschr. 2013; 125:26-33.
20. Tang P, Zhang HD, Yu ZT. Risk factors of early recurrence and prognosis for patients with adenocarcinoma of gastroesophageal junction after curative resection. Zhonghua Yi Xue Za Zhi. 2013; 93:3594-3597.
21. vanSandick JW, van Lanschot JJ, ten Kate FJ, Tijssen JG, Obertop H. Indicators of prognosis after transhiatal esophageal resection without thoracotomy for cancer. J Am Coll Surg. 2002; 194:28-36.
22. Wijnhoven BP, Tran KT, Esterman A, Watson DI, Tilanus HW. An evaluation of prognostic factors and tumor staging of resected carcinoma of the esophagus. Ann Surg. 2007; 245:717-725.
23. Zhang H, Shang X, Chen C, Gao Y, Xiao X, Tang P, Duan X, Yang M, Jiang H, Yu Z. Lymph node ratio-based staging system as an alternative to the current TNM staging system to assess outcome in adenocarcinoma of the esophagogastric junction after surgical resection. Oncotarget. 2016; 7:74337-74349. doi: 10.18632/oncotarget.11188.
24. Liu YP, Ma L, Wang SJ, Chen YN, Wu GX, Han M, Wang XL. Prognostic value of lymph node metastases and lymph node ratio in esophageal squamous cell carcinoma. Eur J Surg Oncol. 2010; 36:155-159.
25. Shao Y, Geng Y, Gu W, Ning Z, Huang J, Pei H, Jiang J. Assessment of lymph node ratio to replace the pN categories system of classification of the TNM system in esophageal squamous cell carcinoma. J Thorac Oncol. 2016; 11:1774-1784.
26. Zafirellis K, Dolan K, Fountoulakis A, Dexter SP, Martin IG, Sue-Ling HM. Multivariate analysis of clinical, operative and pathologic features of esophageal cancer: who needs adjuvant therapy? Dis Esophagus. 2002; 15:155-159.
27. Bogoevski D, Onken F, Koenig A, Kaifi JT, Schurr P, Sauter G, Izbicki JR, Yekebas EF. Is it time for a new TNM classification in esophageal carcinoma? Ann Surg. 2008; 247:633-641.
28. Hsu WH, Hsu PK, Hsieh CC, Huang CS, Wu YC. The metastatic lymph node number and ratio are independent prognostic factors in esophageal cancer. J Gastrointest Surg. 2009; 13:1913-1920.
29. Wilson M, Rosato EL, Chojnacki KA, Chervoneva I, Kairys JC, Cohn HE, Rosato FE Sr, Berger AC. Prognostic significance of lymph node metastases and ratio in esophageal cancer. J Surg Res. 2008; 146:11-15.
30. Yamasaki M, Miyata H, Miyazaki Y, Takahashi T, Kurokawa Y, Nakajima K, Takiguchi S, Mori M, Doki Y. Evaluation of the nodal status in the 7th edition of the UICC-TNM classification for esophageal squamous cell carcinoma: proposed modifications for improved survival stratification: impact of lymph node metastases on overall survival after esophagectomy. Ann Surg Oncol. 2014; 21:2850-2856.
31. Hsu PK, Huang CS, Wang BY, Wu YC, Hsu WH. Survival benefits of post operative chemoradiation for lymph node positive esophageal squamous cell carcinoma. Ann Thorac Surg. 2014; 97:1734-1741.
32. Peyre CG, Hagen JA, DeMeester SR, Van Lanschot JJ, Hölscher A, Law S, Ruol A, Ancona E, Griffin SM, Altorki NK, Rice TW, Wong J, Lerut T, DeMeester TR. Predicting systemic disease in patients with esophageal cancer after esophagectomy: a multinational study on the significance of the number of involved lymph nodes. Ann Surg. 2008; 248:979-985.
33. Wei C, Deng WY, Li N, Shen W, Zhang C, Liu JY, Luo SX. Lymph node ratio as an alternative to the number of metastatic lymph nodes for the prediction of esophageal carcinoma patient survival. Dig Dis Sci. 2015; 60:2771-2776.
34. Cao J, Yuan P, Ma H, Ye P, Ye P, Wang Y, Yuan X, Bao F, Lv W, Hu J. Log odds of positive lymph nodes predicts survival in patients after resection for esophageal Cancer. Ann Thorac Surg. 2016; 102:424-432.
35. Sun G, Xue L, Wang M, Zhao X. Lymph node ratio is a prognostic factor for non-small cell lung cancer. Oncotarget. 2015; 6:33912-33918. doi: 10.18632/oncotarget.5669.
36. Liu D, Chen Y, Deng M, Xie G, Xie G, Wang J, Zhang L, Liu Q, Yuan P, Feng X. Lymph node ratio and breast cancer prognosis: a meta-analysis. Breast Cancer. 2014; 21:1-9.
37. Zhang MR, Xie TH, Chi JL, Li Y, Yang L, Yu YY, Sun XF, Zhou ZG. Prognostic role of the lymph node ratio in node positive colorectal cancer: a meta-analysis. Oncotarget. 2016; 7:72898-72907. doi: 10.18632/oncotarget.1213.
38. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998; 17:2815–2834.
39. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to event data in meta-analysis. Trials. 2007; 8:16.
40. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557-560.
41. Geller N, Freedman L, Lee YJ, DerSimonian R. Conference on meta-analysis in the design and monitoring of clinical trials. Stat Med. 1999; 18:753–754.