
INTRODUCTION
Malignant peripheral nerve sheath tumors (MPNSTs) were designated by the World Health Organization in 2002 to replace previous terminologies of “malignant schwannoma”, “malignant neurilemmoma”, “neurogenic sarcoma”, and “neurofibrosarcoma” [1]. MPNST is a rare disease accounting for 6% of soft tissue sarcomas [2]. They occur in three different contexts: sporadic in around 40% of all cases, associated with neurofibromatosis type 1 (NF1), the most frequent autosomal dominant genetic disorder, in 50% of cases [3–7], and as a consequence of previous radiation therapy (RT-induced) in around 10% [5–7]. Patients with NF1 have an estimated 8–12% lifetime risk of developing MPNST, mainly derived from a pre-existing plexiform neurofibroma [8]. MPNST behaves aggressively, with a high rate of local recurrence and a significant propensity to metastasize. Surgical resection represents the mainstay of therapy. The benefit of radiation and systemic chemotherapy, when commonly administered, is undetermined. Despite aggressive combined modality therapy, survival is dismal with 5-year survival rate of 35%–50% [3, 4, 9].
Recently, research data have shown that NF1, surgical margin status, and tumor size are significant predictors of survival in patients with MPNST. Molecular predictors such as TP53 and S-100 are also suggested [4, 10–12]. However, large cohort studies on Chinese MPNST patients are totally absent [11, 12]. Noteworthily, it had been the largest documented retrospective study of MPNST among Chinese populations up to now. Clinical and pathological prognostic predictors affecting local and/or distant recurrence were analyzed.
RESULTS
A total of 159 patients with MPNST were enrolled into the study. Patient characteristics were summarized in Table 1. The median age was 40 (range: 5–76) years. The ratio of male to female patients was 1.04:1. In the series, 69 (43.4%) patients presented with primary tumors only, whereas 76 (47.8%) patients were accompanied with recurrent tumors and 14 (8.8%) with distant metastasis. The percentages of NF1 associated MPNST and sporadic MPNST patients were 44.0% and 47.8%, respectively. The remaining 8.2% of enrolled patients were RT-induced. Similar to the foreign current reports, most NF1 patients in the study showed typical clinical and pathological features, such as cutaneous neurofibromas, multiple café-au-lait spots (Figure 1A), a large, lobulated soft tissue mass with heterogeneous signal intensity in axial T2-weighted magnetic resonance image (Figure 1B) and spindle cell morphology with a fascicular pattern (Figure 1C).
Table 1: Overall patient, tumor, pathologic characteristics and distribution of events in 159 patients with MPNST
Factor |
n |
% of Total |
|---|---|---|
Presentation status |
||
Primary |
69 |
43.4 |
Recurrent |
76 |
47.8 |
Metastasis |
14 |
8.8 |
Age-year |
||
≤ 40 |
80 |
50.3 |
> 40 |
79 |
49.7 |
Gender |
||
Male |
81 |
50.9 |
Female |
78 |
49.1 |
NF1 status |
||
With NF1 |
70 |
44.0 |
Without NF1 |
89 |
56.0 |
Tumor location |
||
Head and neck |
52 |
32.7 |
Trunk |
55 |
34.6 |
Extremity |
52 |
32.7 |
Tumor size |
||
< 5 cm |
62 |
39.0 |
5–10 cm |
64 |
40.2 |
> 10 cm |
53 |
20.8 |
Depth |
||
Superficial to fascia |
81 |
50.9 |
Deep to fascia |
78 |
49.1 |
AJCC stage |
||
I |
35 |
22.0 |
II |
50 |
34.6 |
III |
60 |
37.7 |
IV |
14 |
8.8 |
Survival status |
||
Died of disease |
89 |
56.0 |
Alive with disease |
23 |
14.5 |
Alive without disease |
47 |
29.5 |
Incidence estimates of tumor-free survival and overall survival for all 159 patients
MPNST |
n |
Tumor-free survival rate |
Overall survival rate |
||||||
|---|---|---|---|---|---|---|---|---|---|
1-yr |
2-yr |
3-yr |
5-yr |
1-yr |
2-yr |
3-yr |
5-yr |
||
Overall |
159 |
- |
- |
- |
- |
63.0 |
56.0 |
50.0 |
43.0 |
Presentation status |
|||||||||
Primary |
69 |
37.0 |
37.0 |
37.0 |
29.0 |
58.0 |
50.0 |
45.0 |
36.0 |
Recurrent |
76 |
43.0 |
40.0 |
40.0 |
36.0 |
72.0 |
65.0 |
62.0 |
54.0 |
Metastasis |
14 |
- |
- |
- |
- |
43.0 |
36.0 |
14.0 |
14.0 |
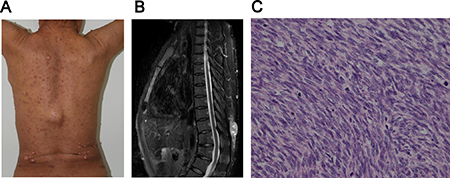
Figure 1: The clinicopathological features of MPNST with NF1.
Among the 159 patients, 19 individuals received no surgery: 14 stage IV cases of the disease with distant metastasis that could not get any obvious benefit from surgery, and 5 patients received palliative treatment for unsuitable health conditions. 140 patients (88.1%) with localized tumors underwent a complete resection. The decision of receiving radiotherapy and/or systemic chemotherapy was made by surgeons, radiologists, physicians, influenced by willingness of patients themselves. In the study, among the 140 patients, 60.7% underwent 15–76 Gy of radiotherapy to primary and/or recurrent lesions before, intra or after surgery. A total of 39 patients were administrated with regimens of doxorubicin and ifosfamide, with or without dacarbazine. 3 patients were stage I and their prognosis were quite well. 36 patients were stage II or stage III. So we conduct the role of chemotherapy among stage II and stage III cases.
The median follow-up time was 31.0 (range: 2.0–199.0) months. The 3- and 5-year overall survival rates of the whole group were 50.0% and 43.0%, respectively (Table 1). 2- and 3-year OS for patients with metastatic disease were 36.0% and 14.0%, which were significantly worse than the localized disease patients (p = 0.002, Figure 2A). NF1 associated MNPST did not show survival advantage compared with those without NF1 presentation (p = 0.671, Figure 2B and p = 0.995, Figure 3D). Additionally, the TFS and the OS of radiation-induced MPNST compared to the sporadic and NF1 -associated are similar (p > 0.05 for both, Table 2).
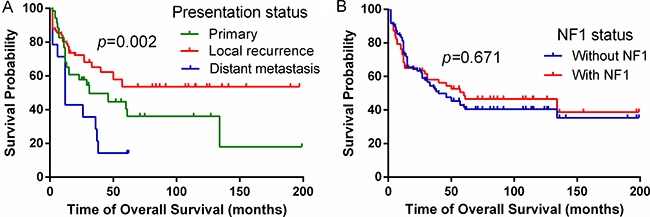
Figure 2: Clinical factors affecting OS in all MPNST patients. (A) Univariable analysis demonstrated that patients presenting with metastasis harbor the worst prognosis (p = 0.002). (B) No difference in outcome was observed when comparing NF1 status (p = 0.671). Kaplan-Meier curves are depicted.
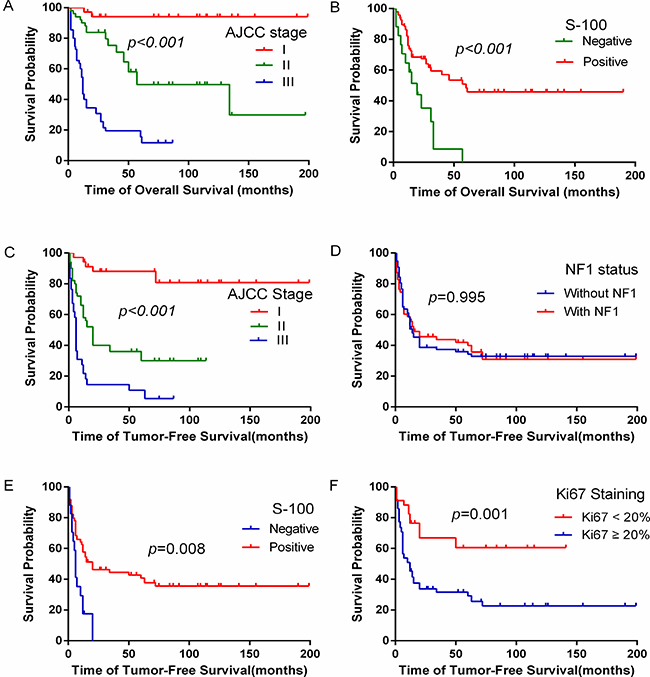
Figure 3: The effect of clinicopathological factors on overall survival and tumor-free survival of MPNST patients. (A) Patients with the late AJCC stage had worse overall survival rate. (B) MPNST patients with S-100 negative had significantly worse overall survival. (C) MPNST patients with the late AJCC stage had lower tumor-free survival. (D) No difference in tumor-free survival was observed when comparing NF1 statuses. (E) MPNST patients with S-100 negative had significantly worse tumor-free survival. (F) MPNST patients with Ki67 ≥ 20% had significantly worse tumor-free survival.
Table 2: Prognostic factors for tumor-free survival and overall survival in 140 completely resected patients with MPNST
Factor |
N |
% |
Tumor-free survival |
Overall survival |
||||
|---|---|---|---|---|---|---|---|---|
HR |
95% CI |
P |
HR |
95% CI |
P |
|||
Age |
||||||||
≤ 40 |
71 |
51.0 |
||||||
> 40 |
69 |
49.0 |
1.085 |
0.708–1.662 |
0.708 |
0.954 |
0.598–1.521 |
0.842 |
Gender |
||||||||
Male |
66 |
47.1 |
||||||
Female |
74 |
52.9 |
0.977 |
0.648–1.473 |
0.913 |
1.177 |
0.747–1.856 |
0.482 |
Tumor location |
||||||||
Head and neck |
51 |
36.4 |
||||||
Trunk |
46 |
32.9 |
0.761 |
0.485–1.193 |
0.233 |
0.569 |
0.338–0.959 |
0.034* |
Extremity |
43 |
30.7 |
0.218 |
0.120–0.397 |
< 0.001* |
0.226 |
0.120–0.426 |
< 0.001* |
Tumor size |
||||||||
≤ 5 cm |
58 |
41.4 |
||||||
> 5 cm |
82 |
58.6 |
2.089 |
1.337–3.263 |
< 0.001* |
1.450 |
0.904–2.324 |
0.123 |
Depth |
||||||||
Superficial to fascia |
67 |
47.9 |
||||||
Deep to fascia |
73 |
52.1 |
4.120 |
2.596–6.539 |
< 0.001* |
3.815 |
2.293–6.348 |
< 0.001* |
NF-1 status |
||||||||
Without NF-1 |
77 |
55.0 |
||||||
With NF-1 |
63 |
45.0 |
0.995 |
0.659–1.501 |
0.980 |
1.024 |
0.649–1.616 |
0.919 |
AJCC stage |
||||||||
I |
35 |
25.0 |
||||||
II |
50 |
35.7 |
6.036 |
2.522–14.446 |
< 0.001* |
11.134 |
2.625–47.217 |
0.001* |
III |
55 |
39.3 |
14.398 |
6.103–33.968 |
< 0.001* |
40.509 |
9.659–169.893 |
< 0.001* |
Margin status |
||||||||
Negative |
123 |
87.9 |
||||||
Positive |
17 |
12.1 |
2.327 |
1.331–4.070 |
0.003* |
2.472 |
1.401–4.362 |
0.002* |
Radiation |
||||||||
Yes |
85 |
60.7 |
||||||
No |
55 |
39.3 |
1.453 |
0.959–2.200 |
0.078 |
2.407 |
1.297–3.233 |
0.002* |
Chemotherapy |
||||||||
Yes |
36 |
34.3 |
||||||
No |
69 |
65.7 |
0.995 |
0.642–1.543 |
0.984 |
1.139 |
0.700–1.848 |
0.603 |
MPNST |
Incidence Estimates of Tumor-free survival and Overall Survival for 140 Completely Resected Patients |
||||||||
|---|---|---|---|---|---|---|---|---|---|
N |
Tumor-free survival rate |
Overall survival rate |
|||||||
1-yr |
2-yr |
3-yr |
5-yr |
1-yr |
2-yr |
3-yr |
5-yr |
||
|
140 |
42.0 |
40.0 |
40.0 |
34.0 |
65.0 |
58.0 |
54.0 |
45.0 |
Median Time (months) |
18.2 |
57.0 |
|||||||
Prognostic factors for overall survival
Till the latest follow-up, 56.0% (89/159) of all patients died of MPNST. Death rate of patients with metastatic disease was much higher than that of patients with localized tumor (85.7% vs. 51.0%, p < 0.05). Since patients with metastases presented significantly worse survival outcomes, these 14 individuals were therefore excluded from further analysis. 5 patients who had inadequate organ functions received no surgery, and they were also excluded. The 5-year OS rate of 140 patients who underwent a complete resection was 45.0%.
To identify additional factors impacting the outcome of MPNST, further analysis was conducted among patients who received surgeries. Univariate analysis showed that the location and the depth of tumor, AJCC stage, margin status, S-100 and Ki67 (Figure 3F) staining independently affected OS (p < 0.05, Tables 2 and 4). However, by multivariate analysis, only AJCC stage (Figure 3A) and S-100 (Figure 3B) were factors associated with prolonged OS (p < 0.05, Table 5).
Prognostic factors for tumor-free survival
The 3-and 5-year TFS rates for the 140 patients were 40.0% and 34.0%, respectively. Most patients experienced local recurrence or distant metastasis during their follow-up. 42.9% experienced local relapse and the median time to relapse was 6.0 months. The 3-year distant relapse rate was 49.3%, and 47.9% developed distant metastases at a median time of 8.0 months. The most common site of distant metastasis was the lungs, which was documented in 35 patients (25.0%). Other common metastatic sites were the bone, brain, and liver, which occurred in 12.1%, 7.1%, and 5.0% of all patients.
Several possible prognostic factors predicting disease progression by analyses of univariable Cox proportions were found. The extremities and the superficial location of MPNST, their early AJCC stage, margin negative, administration of radiotherapy, S-100 positive and Ki67 < 20% were associated with lower recurrence/metastatic rates and prolonged TFS (Table 2). On multivariate analyses, patients with advanced AJCC stage (Figure 3C) and S-100 positive (Figure 3E) had a higher tendency of developing local recurrence and metastases (Table 5).
Biomarker expression in patients with MPNST
It is important to identify MPNST molecular markers for diagnostic value. To achieve this goal, firstly, histologic specimens of 50 NF1 patients diagnosed in the hospital in the same period were collected. Univariate analysis was performed to evaluate possible correlations between biomarker expression and histologic diagnosis (NF1 vs. MPNST). The percentage of NF1 and MPNST specimens exhibiting biomarker positivity (or in case of Ki67 staining, percentage of specimens exhibiting positive staining in ≥ 10% of tumor cells) was calculated (Figure 4). Positive S-100 expression was demonstrated in 84.8% of MPNST samples compared with 98.0% of neurofibroma specimens (Table 3). In summary, the expression of S-100 and Ki67 staining differentiated MPNST from NF1 at a significance of p < 0.05. Though Vimentin, NF and GFAP were slightly higher in positivity in NF1 specimens, they did not reach statistical significance (Table 4).
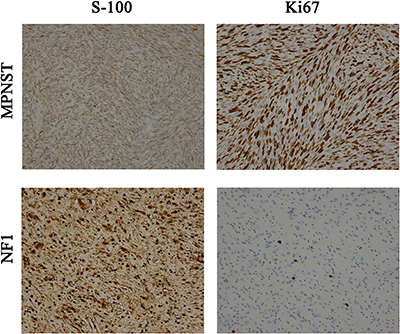
Figure 4: Protein Expression of S-100 and Ki67: in MPNSTs and NF1 (200X), separately.
Table 3: Biomarker distribution and statistical significance in NF1 and MPNST tumor tissues
Marker |
NF1 (n = 50) |
MPNST (n = 112) |
P |
||
|---|---|---|---|---|---|
Staining Negative n (%) |
Staining Positive n (%) |
Staining Negative n (%) |
Staining Positive n (%) |
||
S-100 |
1 (2.0) |
49 (98.0) |
17 (15.2) |
95 (84.8) |
0.014* |
Ki-67 |
29 (96.7) |
1 (3.3) |
34 (42.0) |
47 (58.0) |
< 0.001* |
Vimentin |
1 (6.7) |
14 (93.3) |
3 (4.3) |
66 (95.7) |
0.702 |
NF |
15 (68.2) |
7 (32.8) |
12 (52.2) |
11 (47.8) |
0.273 |
GFAP |
13 (91.9) |
8 (8.1) |
25 (78.1) |
7 (21.9) |
0.200 |
Table 4: Univariable cox proportions analysis for markers associated with MPNST tumor-free survival and overall survival for patients with localized tumors
Prognostic Factor |
N |
% |
Tumor-free survival |
Overall survival |
||||
|---|---|---|---|---|---|---|---|---|
HR |
95% CI |
P |
HR |
95% CI |
P |
|||
S-100 |
||||||||
Positive |
95 |
84.8 |
||||||
Negative |
17 |
15.2 |
2.492 |
1.387–4.479 |
0.002* |
2.903 |
1.572–5.360 |
0.010* |
Ki67 Staining |
||||||||
< 20% |
34 |
42.0 |
||||||
≥ 20% |
47 |
58.0 |
2.244 |
1.153–4.369 |
0.017* |
3.494 |
1.830–6.668 |
< 0.001* |
Vimentin |
||||||||
Positive |
62 |
95.4 |
||||||
Negative |
3 |
4.6 |
1.225 |
0.337–3.268 |
0.692 |
1.532 |
0.343–6.253 |
0.560 |
NF |
||||||||
Positive |
11 |
47.8 |
||||||
Negative |
12 |
52.2 |
0.930 |
0.580–1.520 |
0.734 |
1.004 |
0.336–2.999 |
0.994 |
GFAP |
||||||||
Positive |
7 |
21.8 |
||||||
Negative |
25 |
78.2 |
1.287 |
0.144–11.504 |
0.638 |
0.537 |
0.018–3.203 |
0.520 |
Table 5: Multivariate analysis of prognostic factors for 140 completely resected patients with MPNST
Prognostic Factor |
Tumor-free survival |
Overall survival |
||||
|---|---|---|---|---|---|---|
HR |
95% CI |
P |
HR |
95% CI |
P |
|
Tumor location |
||||||
Head and neck |
1.000 |
1.000 |
||||
Trunk |
0.752 |
0.312–1.814 |
0.526 |
1.149 |
0.474–2.787 |
0.758 |
Extremity |
0.292 |
0.081–1.046 |
0.059 |
0.308 |
0.065–1.455 |
0.137 |
Depth |
||||||
Superficial to fascia |
1.000 |
1.000 |
||||
Deep to fascia |
2.103 |
0.755–5.861 |
0.155 |
3.157 |
0.949–10.505 |
0.061 |
Tumor size |
||||||
≤ 5 cm |
1.000 |
- |
||||
> 5 cm |
1.525 |
0.677–3.435 |
0.308 |
- |
- |
- |
AJCC stage |
||||||
I |
1.000 |
1.000 |
||||
II |
3.784 |
1.268–11.290 |
0.017* |
2.988 |
0.590–15.141 |
0.186 |
III |
16.945 |
4.680–61.350 |
< 0.001* |
35.881 |
7.135–180.442 |
< 0.001* |
S-100 |
||||||
Negative |
1.000 |
1.000 |
||||
Positive |
0.236 |
0.081–0.669 |
0.008* |
0.151 |
0.042–0.542 |
0.004* |
Ki67 |
||||||
< 20% |
1.000 |
1.000 |
||||
≥ 20% |
3.818 |
1.722–8.464 |
0.001* |
1.885 |
0.826–4.304 |
0.132 |
Margin status |
||||||
Negative |
1.000 |
1.000 |
||||
Positive |
1.696 |
0.610–4.716 |
0.311 |
1.892 |
0.650–5.504 |
0.242 |
Radiation |
||||||
Yes |
- |
1.000 |
||||
No |
- |
- |
- |
1.561 |
0.734–3.320 |
0.247 |
DISCUSSION
MPNSTs are rare soft tissue sarcoma. Knowledge of their clinical outcome is limited, which impedes the ability to construct tumor-specific sensitive prognostic paradigms. This is one of the largest studies published within the last 30 years evaluating MPNST populations consisting of at least 100 patients [4, 6, 12, 13]. Data showed the unfavorable outcome of MPNST, as well as the diagnostic value of S-100 and Ki67 in MPNST. Most importantly, it had been the largest retrospective study of Chinese populations to identify clinical and molecular predictors for MPNST to date.
In the study, the 3- and 5-year OS rates were 50.0% and 43.0%, respectively for the whole group, and 54.0% and 45.0%, respectively for patients who received tumor resection. The survival of Chinese patients with MPNST after multidisciplinary treatments was unsatisfactory, which was no difference from the published data with the 5-year survival rates ranging from 35 to 52% [4–6, 12].
The percentages of NF1 associated MPNST and RT-induced were 47.8% and 8.2%, respectively. 44% of patients in the series had NF1. Other studies in the literature reported that it consisted of 22% to 52% of their study samples [4–6, 13]. It is no doubt that patients with NF1 are at increased risk of developing MPNST. There are conflicting reports as to whether malignant MPNST in NF1-patients with have worse prognoses than MPNST in non-NF1 patients. Porter and colleagues found that NF1 (p = 0.007) remained independent predictors of poor outcome and they recommended that NF1 be taken into account during MPNST staging [14]. Kolberg conducted a survival meta-analysis for > 1800 MPNST patients with and without NF1 [10]. The compiled literature from 1963 to 2012 indicated a significantly worse outcome of MPNST in patients with NF1 syndrome compared with that in non-NF1 patients. However, survival for the NF1 patients has improved in the last decade, and the survival difference is diminishing. In the study, there was no significant difference between the survival of patients with and without NF1 (p > 0.05). Additionally, in our study, it has no significance of the TFS and the OS of radiation-induced MPNST compared to the sporadic and NF1 -associated MPNST. However, LaFemina and colleagues reported on 105 patients with MPNST and found that NF1-associated and sporadic MPNSTs may be associated with improved disease specific survival compared to RT-induced tumors [15].
Noteworthily, the study found several prognostic factors for survival of MPNST patients. Data showed that the location, the depth, the size, the AJCC stage of the tumor, and S-100 were associated with the tumor-free survival. Whereas, late AJCC stage and S-100 negative were independent unfavorable factors affecting OS. Local recurrence or distant metastasis were much common in patients whose tumor was deeply located, especially in the head and neck region, tumor size > 5 cm, advanced AJCC stage, and/or Ki67 ≥ 20%. These results from Chinese patients in the report were in accordance with the reported data worldwide.
Some molecules including S-100, Ki67 may be useful in assessing the prognosis of MPNST. S-100 was considered a marker of neural crest differentiation and widely used to identify nerve sheath tumors from other soft-tissue neoplasms [16]. However, S-100 was negative in some MPNST patients as reported previously [12], which was considered the differentiation of Schwann cells [17]. In the series, 15.2% of the tumors were identified as S-100 negative and 84.8% positive. Further, it was found that S-100 negative was an independent prognosis factor, with a 3.24-fold increased risk of recurrence or metastasis, and a 5.62-fold increased risk of mortality. Ki67 was reported as a marker of cell proliferation, and had been used for predicting the prognosis of some tumors, such as breast cancers and lymphomas. Previous studies also confirmed upregulation of Ki67 in MPNST when compared with benign schwannoma [5]. In the report, 58.0% of MPNST tumors were identified as Ki67 ≥ 10%, compared with 3.3% of NF1. In prognostic analysis, Ki67 ≥ 20% was proven to be an independent prognostic factor, with a 2.81-fold increased risk of mortality, compared with Ki67 < 20% MPNST (p = 0.001). The above conclusion was quite similar to the study from Kolarov [18]. It was an agreement that Vimentin was a maker of epithelial-mesenchymal transition. Therefore, it is higher in many malignant tumors, such as prostate cancer, breast cancer and colorectal cancer [19]. In the study, Vimentin, NF, and GFAP did not express significant differences in content between MPNST and NF1. Also, it was confirmed that Vimentin, NF, and GFAP were not prognostic factors for postoperative TFS and OS.
The mainstay of therapy for MPNST is surgical resection with the goal of achieving complete removal with negative margins. Many authors confirmed that total resection with a clear margin could reduce the recurrence rate and improve the prognosis of MPNST [4, 20–22]. In the series, negative margins could improve both the OS (p = 0.002) and the TFS (p = 0.003) on analyses of univariable Cox proportions (Table 4). But it was not an independent prognostic factor via multivariate analysis (p > 0.05, Table 5). Radiation therapy is an important adjunct to surgery in improving local control, and may be administered in the neoadjuvant or adjuvant setting, and as intraoperative therapy in centers with the available resources [23]. Although improvement in rates of local control have been seen with adjuvant radiation therapy, only one study out of Milan, Italy has been able to demonstrate that lack of radiation therapy predicts decreased disease specific survival [4]. In the data, adjuvant radiation therapy (HR: 0.688) could improve the OS rate, but it did not reach statistical significance (p = 0.078). The administration of adjuvant radiation therapy was associated with an improved TFS on univariate analyses (p = 0.002), though it had no impact on OS on multivariate analyses. The role of chemotherapy remains controversial. Some studies supported the effect of chemotherapy in MPNSTs [12, 24], while others considered it as useless [4, 6]. Generally, first-line chemotherapy regimen was doxorubicin-based [25]. Kroep conducted a research analyzing the response and survival of different chemotherapy regimens in patients with advanced MPNST [26]. They came to the conclusion that the doxorubicin-ifosfamide combination had the best response rate (HR: 6.283, 95% CI: 2.342–16.852). In that study, the administration of chemotherapy in MPNST patients had no impact on the survival. That patient sample group was quite small, though (Table 2).
In summary, despite combined multimodality therapy, MPNST behaves as an aggressive sarcoma with a propensity to recur locally or to metastasize to distant sites. It is believed that better survival outcomes were directly related to the high rate of negative margins combined with some certain clinical characteristics. From data of the hospital, tumor complete resection with MPNST patients is encouraged. The role of multidisciplinary approaches including adjuvant chemotherapy and/or radiotherapy need more randomized clinical studies to confirm.
MATERIALS AND METHODS
The clinical data of MPNST patients who were pathologically diagnosed and treated at Cancer Institute & Hospital, Chinese Academy of Medical Science from January 1999 to January 2016 was retrospectively reviewed. The study has been approved by the Ethics Committee in our hospital. For a tumor to be considered a NF1-associated MPNST. Firstly, its presence was determined on the basis of established NIH criteria [4], ie, patients with NF1 had at least 2 of the following: ≥ six cafe-au-lait macules (> 5 mm before puberty, > 15 mm after puberty), skin-fold freckles (groin, axilla, base of neck), ≥ 2 neurofibromas (1 plexiform), skeletal dysplasia (orbital or tibial), Lisch nodules (iris hamartomas), optic gliomas, and family history. For a tumor to be considered a sporadic MPNST, it must have met at least one of the following criteria: [5] (1.) originated in a peripheral nerve; (2.) originated in a pre-existing nerve sheath tumor (rare, other than neurofibroma in NF1); (3.) exhibited ultrastructural features of Schwannian differentiation. Multiple systems of histologic grading have been applied to MPNST with variable success. Grading of MPNST has not been shown to be of clinical utility under the French Federation of Cancer Centers (FNCLCC) system [5]. And It is a pity that grading of MPNST is not routinely performed at our hospital. All patients were verified by two different senior pathologists. Patient clinical data included age, sex, tumor location, largest diameter of tumor, clinical AJCC (American Joint Committee on Cancer) stage of tumor, time to recurrence or metastatic status, treatments and outcomes.
Immunohistochemical methods
The 112 formalin-fixed paraffin-embedded MPNST tissues were sectioned at 4 um and mounted on to charged glass slides for immunohistochemical stainings as previously described with minor modification. The concentrations of the diluted antibodies were 1:75 for S-100 (PL0401286, PLLABS), Ki67 (orb67076, biorbyt), Vimentin (3295s, Cellsignal), neurofilament (NF) (PAB19367, Bio-Swamp), and glial fibrillary acidic protein (GFAP) (orb26155, biorbyt). The protein expressions were estimated by two different senior pathologists.
Statistics
Data were analyzed using SPSS version 19.0 (SPSS, Inc. Chicago, IL, USA). Tumor-free survival (TFS) was calculated from the date of diagnosis to the date of local recurrence, or distant metastasis, or last follow-up, or date of death from any cause. Overall survival (OS) was calculated from the date of diagnosis to the date of death, or last follow-up, whichever occurred first. TFS and OS probabilities were estimated by the Kaplan-Meier methods. Log-rank tests were used to compare the OS probability and TFS probability between groups. Cox proportional-hazards regression (Cox PH) analysis was performed to calculate the hazard ratio and 95% confidence interval. The univariable Cox PH model were fitted to evaluate the predictive effect of clinical characteristics and biomarkers. The significant predictors in univariable models were candidate variables in the multivariable Cox PH model. The cutoff p value was set as 0.05.
Abbreviations
MPNST, malignant peripheral nerve sheath tumors; OS, overall survival; TFS, tumor-free survival; GFAP, glial fibrillary acidic protein; NF, neurofilament; AJCC, American Joint Committee on Cancer; HR, hazard ratio; CI, confidence interval.
ACKNOWLEDGMENTS
We thank the staff from the departments of orthopedics at Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College for their assistance in patient enrollment and sample collection.
CONFLICTS OF INTEREST
The authors disclose no potential conflicts of interest.
REFERENCES
1. Gupta G, Maniker A. Malignant peripheral nerve sheath tumors. Neurosurgical focus. 2007; 22:E12.
2. Doyle LA. Sarcoma classification: an update based on the 2013 World Health Organization Classification of Tumors of Soft Tissue and Bone. Cancer. 2014; 120:1763–1774.
3. Ducatman BS, Scheithauer BW, Piepgras DG, Reiman HM, Ilstrup DM. Malignant peripheral nerve sheath tumors. A clinicopathologic study of 120 cases. Cancer. 1986; 57:2006–2021.
4. Anghileri M, Miceli R, Fiore M, Mariani L, Ferrari A, Mussi C, Lozza L, Collini P, Olmi P, Casali PG, Pilotti S, Gronchi A. Malignant peripheral nerve sheath tumors: prognostic factors and survival in a series of patients treated at a single institution. Cancer. 2006; 107:1065–1074.
5. Zou C, Smith KD, Liu J, Lahat G, Myers S, Wang WL, Zhang W, McCutcheon IE, Slopis JM, Lazar AJ, Pollock RE, Lev D. Clinical, pathological, and molecular variables predictive of malignant peripheral nerve sheath tumor outcome. Annals of surgery. 2009; 249:1014–1022.
6. Stucky CC, Johnson KN, Gray RJ, Pockaj BA, Ocal IT, Rose PS, Wasif N. Malignant peripheral nerve sheath tumors (MPNST): the Mayo Clinic experience. Annals of surgical oncology. 2012; 19:878–885.
7. Dunn GP, Spiliopoulos K, Plotkin SR, Hornicek FJ, Harmon DC, Delaney TF, Williams Z. Role of resection of malignant peripheral nerve sheath tumors in patients with neurofibromatosis type 1. Journal of neurosurgery. 2013; 118:142–148.
8. Evans DG, Baser ME, McGaughran J, Sharif S, Howard E, Moran A. Malignant peripheral nerve sheath tumours in neurofibromatosis 1. Journal of medical genetics. 2002; 39:311–314.
9. Carli M, Ferrari A, Mattke A, Zanetti I, Casanova M, Bisogno G, Cecchetto G, Alaggio R, De Sio L, Koscielniak E, Sotti G, Treuner J. Pediatric malignant peripheral nerve sheath tumor: the Italian and German soft tissue sarcoma cooperative group. Journal of clinical oncology. 2005; 23:8422–8430.
10. Kolberg M, Holand M, Agesen TH, Brekke HR, Liestol K, Hall KS, Mertens F, Picci P, Smeland S, Lothe RA. Survival meta-analyses for > 1800 malignant peripheral nerve sheath tumor patients with and without neurofibromatosis type 1. Neuro-oncology. 2013; 15:135–147.
11. Wang T, Yin H, Han S, Yang X, Wang J, Huang Q, Yan W, Zhou W, Xiao J. Malignant peripheral nerve sheath tumor (MPNST) in the spine: a retrospective analysis of clinical and molecular prognostic factors. Journal of neuro-oncology. 2015; 122:349–355.
12. Fan Q, Yang J, Wang G. Clinical and molecular prognostic predictors of malignant peripheral nerve sheath tumor. Clinical & translational oncology. 2014; 16:191–199.
13. Valentin T, Le Cesne A, Ray-Coquard I, Italiano A, Decanter G, Bompas E, Isambert N, Thariat J, Linassier C, Bertucci F, Bay JO, Bellesoeur A, Penel N, et al. Management and prognosis of malignant peripheral nerve sheath tumors: The experience of the French Sarcoma Group (GSF-GETO). European journal of cancer. 2016; 56:77–84.
14. Porter DE, Prasad V, Foster L, Dall GF, Birch R, Grimer RJ. Survival in Malignant Peripheral Nerve Sheath Tumours: A Comparison between Sporadic and Neurofibromatosis Type 1-Associated Tumours. Sarcoma. 2009; 2009:756395.
15. LaFemina J, Qin LX, Moraco NH, Antonescu CR, Fields RC, Crago AM, Brennan MF, Singer S. Oncologic outcomes of sporadic, neurofibromatosis-associated, and radiation-induced malignant peripheral nerve sheath tumors. Annals of surgical oncology. 2013; 20:66–72.
16. Karamchandani JR, Nielsen TO, van de Rijn M, West RB. Sox10 and S100 in the diagnosis of soft-tissue neoplasms. Applied immunohistochemistry & molecular morphology. 2012; 20:445–450.
17. Perry A, Roth KA, Banerjee R, Fuller CE, Gutmann DH. NF1 deletions in S-100 protein-positive and negative cells of sporadic and neurofibromatosis 1 (NF1)-associated plexiform neurofibromas and malignant peripheral nerve sheath tumors. The American journal of pathology. 2001; 159:57–61.
18. Kolarov V, Stanic J, Eri Z, Zvezdin B, Kojicic M, Hromis S. Intrathoracic malignant peripheral nerve sheath tumor with poor outcome: a case report. Bosnian journal of basic medical sciences. 2010; 10:328–330.
19. Zhao Y, Yan Q, Long X, Chen X, Wang Y. Vimentin affects the mobility and invasiveness of prostate cancer cells. Cell biochemistry and function. 2008; 26:571–577.
20. Ma C, Ow A, Shan OH, Wu Y, Zhang C, Sun J, Ji T, Pingarron Martin L, Wang L. Malignant peripheral nerve sheath tumours in the head and neck region: retrospective analysis of clinicopathological features and treatment outcomes. International journal of oral and maxillofacial surgery. 2014; 43:924–932.
21. Brekke HR, Kolberg M, Skotheim RI, Hall KS, Bjerkehagen B, Risberg B, Domanski HA, Mandahl N, Liestol K, Smeland S, Danielsen HE, Mertens F, Lothe RA. Identification of p53 as a strong predictor of survival for patients with malignant peripheral nerve sheath tumors. Neuro-oncology. 2009; 11:514–528.
22. Ren X, Wang J, Hu M, Jiang H, Yang J, Jiang Z. Clinical, radiological, and pathological features of 26 intracranial and intraspinal malignant peripheral nerve sheath tumors. Journal of neurosurgery. 2013; 119:695–708.
23. Wong WW, Hirose T, Scheithauer BW, Schild SE, Gunderson LL. Malignant peripheral nerve sheath tumor: analysis of treatment outcome. International journal of radiation oncology, biology, physics. 1998; 42:351–360.
24. Moretti VM, Crawford EA, Staddon AP, Lackman RD, Ogilvie CM. Early outcomes for malignant peripheral nerve sheath tumor treated with chemotherapy. American journal of clinical oncology. 2011; 34:417–421.
25. Casali PG, Jost L, Sleijfer S, Verweij J, Blay JY, and ESMO Guidelines Working Group. Soft tissue sarcomas: ESMO clinical recommendations for diagnosis, treatment and follow-up. Annals of oncology. 2009; 20:132–136.
26. Kroep JR, Ouali M, Gelderblom H, Le Cesne A, Dekker TJ, Van Glabbeke M, Hogendoorn PC, Hohenberger P. First-line chemotherapy for malignant peripheral nerve sheath tumor (MPNST) versus other histological soft tissue sarcoma subtypes and as a prognostic factor for MPNST: an EORTC soft tissue and bone sarcoma group study. Annals of oncology. 2011; 22:207–214.