
INTRODUCTION
Spinal anesthesia is commonly used in cesarean section surgery. Apart from being economical and easy to administer, spinal anesthesia provides both analgesia and muscular relaxation with rapid onset of action [1]. However, the administration of local anesthetics alone has a short duration of effect, and is insufficient for preventing visceral pain and nausea especially at an earlier stage [2–4]. Visceral pain is common during spinal anesthesia with mini dose local anesthetics. It is especially uncomfortable in cesarean surgery as the surgeons need to lift the uterus and suture the peritoneal during surgery. Moreover, there remains a lack of long lasting postoperative analgesia [5]. To overcome the defects of local anesthetics, joint administration of adjuvant drugs has become an widely accepted practice in clinical work.
Adjuvant drugs added to the intrathecal bupivacaine can decrease the dose of local anesthetics and guarantee sensory and motor block. Intrathecal adjuvants include opioids, agonist, magnesium, neostigmine, ketamine and midazolam etc. Clonidine and dexmedetomidine are receptor agonists which have sedative, analgesic, perioperative sympatholytic, anesthetic-sparing, and hemodynamic-stabilizing properties [6]. Clonidine provides a dose-dependent increase in the duration of sensory and motor block, besides antinociceptive properties [7]. Furthermore, evidence from animal study indicates that dexmedetomidine produces spinal analgesia as efficiently as clonidine [8]. Intrathecal α2-receptor agonists are found to have antinociceptive action for both somatic and visceral pain [9]. Intrathecal dexmedetomidine has been used in the dose of 3, 5, 10 and 15 μg along with bupivacaine in surgeries such as lower limbs, transurethral prostatectomy [9–14]. Intrathecal dexmedetomidine has also been used in cesarean section. Sun Y et al. demonstrated that addition of 10 μg dexmedetomidine into bupivacaine provided better intraoperative and postoperative analgesia [15]. Li Z et al. showed the same data that dexmedetomidine at the dose of 10μg adjunt to bupivacaine is sufficient to provide adequate anesthesia and postoperative analgesia [16]. It remains unknown whether addition of lower doses of dexmedetomidine to bupivacaine could produce satisfactory decrease of visceral pain in cesarean surgery. Therefore, in the current study we aimed to test whether adjunct use of lower doses (3 and 5 μg) of dexmedetomidine with bupivacaine intrathecally could improve somato-visceral block characteristcs and decrease postoperative pain without affecting the infants.
RESULTS
Demographic and surgical characteristics
The demographic profiles of the patients in all the 3 groups were comparable with regard to age, weight, height, gestation age, mean duration of surgery (P > 0.05). There were no significant difference between duration of surgery, surgery starting time and fetal delivery time among groups (Table 1).
Table 1: Demographic and surgical characteristics
Bup |
Bup+Dex(3) |
Bup+Dex(5) |
F/χ2 |
P value |
|
|---|---|---|---|---|---|
Age (year) |
29.5±3.9 |
32.1±4.9 |
31.3±3.7 |
2.04 |
0.1398 |
Height(cm) |
161.2±5.4 |
161.2±3.6 |
162.0±3.7 |
0.23 |
0.7944 |
Weight(kg) |
74.9±8.4 |
75.9±7.3 |
72.9±9.6 |
0.65 |
0.5266 |
Gestational weeks |
38.5(37.0,39.0) |
39.0(38.0,39.0) |
39.0(38.0,40.0) |
4.51 |
0.1051 |
Duration of surgery(min) |
48.0±8.8 |
47.3±11.5 |
53.8±12.7 |
1.91 |
0.1570 |
Onset time of operation (min) |
13.1±3.4 |
14.7±3.8 |
13.6±3.1 |
0.71 |
0.4960 |
Fetal delivery time(min) |
19.6±20.0 |
23.1±6.9 |
21.9±4.1 |
2.42 |
0.0981 |
Spinal block characteristics and analgesia
The spinal block characteristics are presented in Table 2. The cases with supplemental lidocaine reduced to 7 and 5 in Bup+Dex(3) and Bup+Dex(5) groups (p<0.05), respectively. The supplemental lidocaine dose was higher in Bup group than Bup+Dex(3) and Bup+Dex(5) groups (p<0.05 vs Bup). The cases with visceral pain and received fentanyl administration were 9 in Bup group, 2 in Bup+Dex(3) group and 6 in Bup+Dex(5) group (p<0.05 vs Bup). Fentanyl dose was higher in Bup group than the other two groups. The abdominal muscle relax satisfactory cases were 7 in Bup group, 15 in Bup+Dex(3) group and 16 in Bup+Dex(5) group. The time to highest sensory block was similar among the 3 groups. Duration of motor block was significantly prolonged from 3.56±1.02h in Bup group to 5.82±0.95h in Bup+Dex(3) group and 5.14±0.88h Bup+Dex(5) group. The other spinal block characteristics including highest sensory block level among groups.
Table 2: Spinal block characteristics
Bup |
Bup+Dex(3) |
Bup+Dex(5) |
F/χ2 |
P value |
|
|---|---|---|---|---|---|
Time to Max sensory level(min) |
15.0(10.0,15.0) |
15.0(12.5,20.5) |
15.0(10.0,17.5) |
1.21 |
0.5468 |
Supplemental lidocaine cases |
14(70.0)ab |
7(35.0)a |
5(25.0)b |
9.10 |
0.0110 |
Supplemental 2%lidocaine dose(ml) |
5.0(2.5,10.0)ab |
5.0(0.0,11.0)a |
2.5(0.0,5.0)b |
11.58 |
0.0031 |
Fentanyl cases(%) |
9(45.0)ab |
2(10.0)a |
6(30.0)b |
6.07 |
0.0480 |
Fentanyl dose(mg) |
0.0(0.0,0.1)ab |
0.0(0.0,0.0)a |
0.0(0.0,0.05)b |
6.69 |
0.0352 |
Visceral pain cases(%) |
9(45.0)ab |
2(10.0)a |
6(30.0)b |
6.07 |
0.0480 |
Visceral pain time(min) |
37.0(35.0,40.0) |
38.5(37.0,40.0) |
42.5(40.0,45.0) |
5.27 |
0.0716 |
Muscle relaxation satisfaction cases(%) |
7(35.0)ab |
15(75.0)a |
16(80.0)b |
10.48 |
0.0053 |
Duration of motor block(h) |
3.6±1.0ab |
5.8±1.0a |
5.1±0.9b |
29.88 |
<0.0001 |
a,b suggest groups labeled by the same letter have statistical significance. Data in accordance with normal distribution were showed by mean ± standard deviation. Data not in accordance with normal distribution were showed by median.
The VAS at 6h after surgery was higher in Bup group than in Bup+Dex(3) and Bup+Dex(5) groups (Table 3). No difference of VAS was observed at 12h after surgery. There was no difference in uterine contraction pain after surgery and supplement postoperative analgesia time (Table 3).
Table 3: Postoperative pain and analgesia
Bup n (%) |
Bup+Dex(3) n (%) |
Bup+Dex(5) n (%) |
F/χ2 |
P value |
|
|---|---|---|---|---|---|
VAS |
|||||
6h |
0.0(1.5,2.5)ab |
0.0(0.0,0.0)a |
0.0(0.0,1.5)b |
11.50 |
0.0032 |
12h |
4.0(5.5,6.5) |
5.0(2.5,7.5) |
3.8(2.5,5.3) |
2.08 |
0.3533 |
Uterine Contraction Pain |
|||||
6h |
0.0(0.0,0.0) |
0.0(0.0,0.0) |
0.0(0.0,0.0) |
1.72 |
0.4239 |
12h |
1.0(1.0,1.0) |
1.0(0.5,1.0) |
1.0(0.5,1.0) |
1.84 |
0.3978 |
Supplement postoperative analgesia case(%) |
5(25.0) |
4(20.0) |
8(40.0) |
2.13 |
0.3440 |
Postoperative supplement drug time(h) |
22.3±3.4 |
24.8±3.0 |
23.8±5.4 |
0.35 |
0.7096 |
Postoperative promethazine |
0.0(0.0,0.0) |
0.0(0.0,0.0) |
0.0(0.0,0.0) |
0.00 |
1.0000 |
a,b suggest groups labeled by the same letter have statistical significance. Data in accordance with normal distribution were showed by mean ± standard deviation. Data not in accordance with normal distribution were showed by median.
Fetal characteristcs
In all three groups newborns have no signs of fetal distress, evidenced by Apgar score 9 and 10 at 1 and 5 min, respectively (Table 4). There was no difference in umbilical oxygen partial pressure, dioxide partial pressure, glucose and lactate among three groups (Table 4).
Table 4: Apgar scores and umbilical artery gas analysis
Factor |
Bup |
Bup+Dex(3) |
Bup+Dex(5) |
F |
P value |
|---|---|---|---|---|---|
Apgar score |
|||||
1min |
9.0(8.0,9.0) |
9.0(8.0,9.0) |
9.0(8.0,9.0) |
0.59 |
0.7450 |
5min |
10.0(9.0,10.0) |
10.0(9.0,10.0) |
10.0(9.5,10.0) |
0.31 |
0.8556 |
Umbilical oxygen partial pressure(mmHg) |
24.8±10.3 |
25.7±8.4 |
27.6±9.0 |
0.48 |
0.6217 |
Umbilical dioxide partial pressure(mmHg) |
41.9±5.1 |
43.1±5.4 |
43.6±5.9 |
0.49 |
0.6162 |
Umbilical glucose(mmol/L) |
3.5±0.6 |
3.6±0.4 |
3.6±0.6 |
0.12 |
0.8838 |
Umbilical lactate(mmol/L) |
1.5(1.4,1.6) |
1.5(1.3,1.7) |
1.4(1.2,1.6) |
1.33 |
0.5136 |
Umbilical blood PH |
7.4±0.0 |
7.3±0.0 |
7.3±0.0 |
1.99 |
0.1460 |
Hemodynamics and side effects
There was no difference among three groups in SP, DP and HR (Figures 1 and 2).
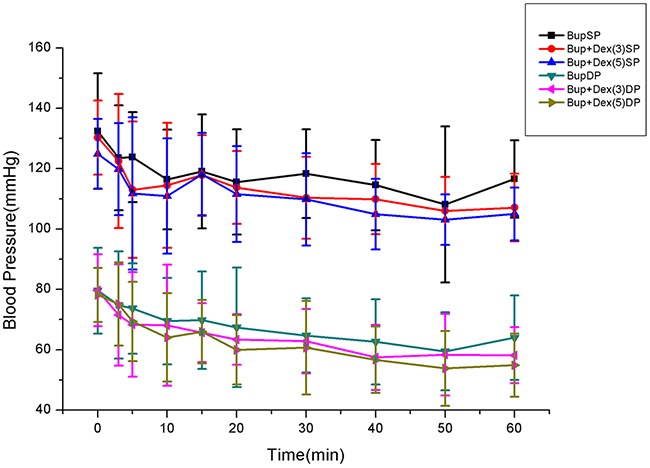
Figure 1: Comparison of SP, DP among groups.
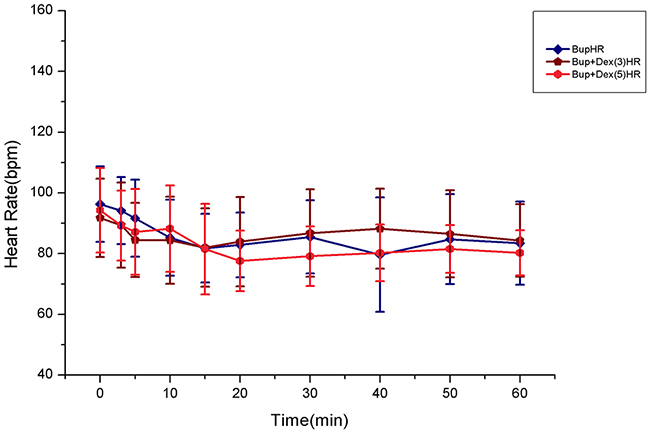
Figure 2: Comparison of HR among groups.
The phenylephrine dose at 10min after spinal anesthesia was 190.0±88.4 μg in Bup+Dex(5), which is higher than in Bup group 133.0±39.1 μg and Bup+Dex(3) group 130.0±43.3μg (Table 5). The phenylephrine dose at 20min after spinal anesthesia was 308.0±111.5μg in Bup+Dex(5) group, 229.5±59.6 μg in Bup group and 241.0±64.1 μg in Bup+Dex(3) group (P<0.05 vs Bup+Dex(5)). No difference was observed between Bup and Bup+Dex(3) groups (Table 5). There were no significant difference between nausea and vomiting intraoperation, postoperation, shiver, pruritus, exaust time and tramadol dose among groups (Table 6).
Table 5: Phenylephrine dose
Factor |
Bup |
Bup+Dex(3) |
Bup+Dex(5) |
F |
P value |
|---|---|---|---|---|---|
Phenylephrine dose(μg) |
|||||
10min |
133.0±39.1a |
130.0±43.3b |
190.0±88.4ab |
6.12 |
0.0039 |
20min |
229.5±59.6a |
241.0±64.1b |
308.0±111.5ab |
5.37 |
0.0073 |
a, b suggest groups labeled by the same letter have statistical significance.
Table 6: Comparison of incidence of side effects, first anal aerofluxus time and tramadol dose
Bup n(%) |
Bup+Dex(3) n(%) |
Bup+Dex(5) n(%) |
F/χ2 |
P value |
|
|---|---|---|---|---|---|
Nausea and vomiting intraoperation |
0(0.0) |
4(20.0) |
3(15.0) |
4.47 |
0.1442 |
Nausea and vomiting postoperation |
0(0.0) |
1(5.0) |
1(5.0) |
1.28 |
1.0000 |
Shivering postoperation |
11(55.0) |
8(40.0) |
9(45.0) |
0.94 |
0.6258 |
Pruritus postoperation |
2(10.0) |
3(15.0) |
3(15.0) |
0.42 |
1.0000 |
First anal aerofluxus time(h) |
35.5±9.9 |
35.4±9.1 |
34.8±6.7 |
0.04 |
0.9644 |
Tramadol case intraoperation |
3(15.0) |
3(15.0) |
1(5.0) |
1.24 |
0.5375 |
Stress response
There was no difference in the maternal baseline IL-6 level among groups. The postoperative IL-6 level was lower in Bup+Dex(3) and Bup+Dex(5) groups than Bup group (Table 7). Baseline maternal cortisol levels were similar among Bup, Bup+Dex(3), and Bup+Dex(5) groups (87.6±10.3μg/L, 86.8±10.0μg/L, 93.4±9.5μg/L, respectively). After surgery, cortisol level was lower in Bup+Dex(3) and Bup+Dex(5) groups than Bup group (Table 7).
Table 7: Compare the stress response effect
Bup |
Bup+Dex(3) |
Bup+Dex(5) |
F/χ2 |
P value |
|
|---|---|---|---|---|---|
Preoperative IL-6 (μg/L) |
50.8±7.2 |
50.4±6.5 |
50.9±4.9 |
0.03 |
0.9711 |
Postoperative IL-6 (μg/L) |
107.3±6.2ab |
87.3±4.7a |
88.2±6.1b |
78.61 |
<0.0001 |
Preoperative cortisol (μg/L) |
87.6±10.3 |
86.8±10.0 |
93.4±9.5 |
2.67 |
0.0778 |
Postoperative cortisol (μg/L) |
157.7±18.4ab |
124.7±11.1a |
128.1±7.4b |
38.18 |
<0.0001 |
a, b suggest groups labeled by the same letter have statistical significance.
DISCUSSION
The selection of different combination and suitable doses when using adjuvant with local anesthetics is a critical process and signifies the consideration of factors such as the formation and duration of sensory and motor block, the quality and duration of postoperative analgesia, and the side effects that might be observed in the mothers and the newborns [17]. Over the years, many drugs have been used intrathecally as an adjuvant to local anesthetic to prolong the intraoperative as well as postoperative analgesia with variable effects [18].
Dexmedetomidine is a new and more selective α2 receptor agonist compared to clonidine, with higher sedative and analgesic effects. Dexmedetomidine provides stable hemodynamic conditions, good sedation, and good quality of intraoperative and prolonged postoperative analgesia with minimal side effects [19]. Our study indicates that in comparison to 5μg intrathecal dexmedetomidine, 3μg dexmedetomidine prolonged and intensified sensory and motor block of bupivacaine without causing any significant side effects. Dexmedetomidine prolonged the pain free period and improved postoperative analgesia. The results are in consistent with previous findings [9, 10], which indicated that the addition of dexmedetomidine demonstrated effective spinal block. The difference is that the dose employed in this study is lower than previous ones. The reason for prolongation of spinal anesthesia in case of dexmedetomidine is due to its supra-spinal action at locus ceruleus and dorsal raphe nucleus. Moreover, dexmedetomidine is more selective to α2 receptor than clonidine, with more sedative and analgesic effects. The prolongation of the motor block of dexmedetomidine with bupivacaine can be explained by the binding of agonists to motor neurons in the dorsal horn [20] and the synergism between local anesthetic and agonists [21].
Hypotension is very common in neuroaxial blocks for cesarean section. This is particularly due to sympathetic block and tends to be treated with ephedrine, phenylephrine and crystalloid-colloid solution infusion [22, 23]. In this study, addition of 5μg dexmedetomidine to hyperbaric bupivacaine produced unstable hemodynamics after spinal anesthesia. However, low dose dexmedetomidine(3μg) adding into bupivacaine exerted stable hemodynamics. Addition of 5μg dexmedetomidine caused lower systolic pressure and diastolic pressure than bupivacaine alone or addition of 3μg dexmedetomidine at all time after spinal anesthesia. Therefore, more phenylephrine(190.0±88.3μg) was administered to maintain blood pressure in patients giving adjuvant 5μg dexmedetomidine than bupivacaine alone (133.0±39.1μg) or addition of 3μg dexmedetomidine (130.0±41.3μg) groups at 10 min after spinal anesthesia. These data indicated that low dose dexmedetomidine(3μg) added into hyperbaric bupivacaine could prolong its sensory and motor block effect with stable blood pressure. The benefits of the use of minidose dexmedetomidine is that it provides prolonged postoperative analgesia and avoided hemodynamic instability such as hypotension and bradycardia produced by larger dose of dexmedetomidine or a prolonged motor blockade.
Several studies have shown blunting of the cardiovascular responses to operation, surgical stimulation and extubation with the use of dexmedetomidine for abdominal hysterectomy on the stress response during caesarean delivery [24]. Nasr and Abdelhamid researched the effect of caudal dexmedetomidine versus fentanyl and bupivacaine on the stress response and postoperative analgesia in pediatric cardiac surgery, and found that dexmetomidine attenuated the stress response and produced better analgesia [25].
Kang et al. reported that dexmedetomidine administration during surgery reduced intraoperative and post-operative secretion of cytokines, including the pro-inflammatory cytokines tumour necrosis factor-α, interleukin-1β and IL-6 and anti-inflammatory cytokines IL-4 and CRP level in their study [26]. Nour EM et al. also found that epidural administration of dexmedetomidine adjunct to bupivacaine inhibited the increment of plasma interleukin-6 [27]. Similarly, in this study the postoperative IL-6 level was lower in Bup+Dex(3) and Bup+Dex(5) groups than Bup group in our study. Preoperative anxiety, fear, sleeplessness, anesthesia, surgery and postoperative pain could elevate cortisol level which is the terminal hormone of pituitary-adrenal cortex axis dramatically. In our study we found that cortisol secretion was suppressed by low dose dexmedetomidine.
Dexmedetomidine and clonidine prevent postoperative shivering by inhibiting central thermoregulation and attenuation of hyperadrenergic response to perioperative stress [28]. Previous studies reported that the incidence of shivering is 10-30 % in control group and there is no occurrence of shivering in dexmedetomidine group [29, 30]. In our study, shivering occurred in 40% and 45% of the patients in the dexmedetomidine(3μg) and dexmedetomidine(5μg) groups, and 55% in control group. The reasons for the difference may be that the small dose of dexmedetomidine (3μg and 5μg) given intrathecally is not as effective as intravenous application to prevent shivering, and parturients are prone to lose more heat and blood than other surgery.
In all three groups, the newborns have no signs of fetal distress, evidenced by Apgar score 9 and 10 at 1 and 5 min, respectively, which infers the advantageous use of dexmedetomidine over other adjuvants. The results were parallel to those reported in literature [15, 31]. Furthermore in our study on significant difference in the incidence of side effects such as pruritus, nausea and vomiting were noted across the three groups. Similar results were reported in previous studies [10, 32, 33]. There has been much debate regarding problems with breastfeeding after anesthesia. Unfortunately, there are no published studies on the safety of breastfeeding after epidural dexmedetomidine when used as an adjunct in labor analgesia. According to the data of previous study [34], we recommended that breastfeeding should be avoided during the 24h immediately after surgery.
In summary, the use of low dose of dexmedetomidine (3μg) as an adjuvant to bupivacaine in cesarean surgery provides better intraoperative somato-visceral block characteristcs and postoperative analgesia without significant impact on Apgar scores or incidence of side effects and decreases stress response level.
MATERIALS AND METHODS
Design
We designed a prospective, randomized, double-blind study to determine whether intrathecal bupivacaine with dexmedetomidine could improve block characteristcs and decrease stress response for cesarean section, and to find out the minimal dose of dexmedetomidine for parturients.
Subjects and setting
The study was approved by the institutional ethics committee with written informed consent (the ethics number:ChiCTR-IIR-16008497. Sixty parturients at the age 18-40 years old with American Society of Anesthesiologists (ASA) physical status I or II undergoing elective cesarean section were enrolled in this study. Exclusion criteria included a long history of opioid analgesic use or NSAIDS, psychiatric disorders, preoperative heart rate less than 50 bpm with cardiac conduction or rhythm abnormalities, neuromuscular and endocrine diseases or allergic reactions to α2-adrenergic agonist.
Study protocol
An 18-gauge intravenous cannula was inserted into a peripheral vein. Standard intraoperative monitoring was used, consisting of ECG, pulse oximetry and non-invasive arterial blood pressure. An intravenous infusion of Lactated Ringer’s Solution 500ml was administered. Lumber epidural anesthesia was induced with 18 gauge Tuohy needle with parturients in lateral position in lumber 3 -4 or lumber 2-3 interspace. Location of epidural space was confirmed by loss of resistance techniques. The spinal injection was performed with a 25 gauge pencil point needle. A computer-generated randomization table was used to divide parturients into three groups: intrathecal 10mg bupivacaine alone(Bup group), 10mg bupivacaine with 3μg dexmedetomidine (Bup+Dex(3) group), 10mg bupivacaine with 5μg dexmedetomidine (Bup+Dex(5) group). All solutions were at room temperature and diluted with 0.9% saline to a final volume of 2.0 ml. Study drugs were injected at a rate of 1ml/15s by the same anesthesiologist. Epidural catheter was secured 3-5 cm into the epidural space, then parturients were placed supine with a Crawford wedge displacing the uterus to the left until birth. The allocation to one of three combinations was done by a computer-generated randomization scheme. The prescriptions of the study medication were kept in sealed numbered envelopes and stored near the operation room. A registered anesthetic nurse who was not involved in the study prepared the solutions, using the consecutive envelopes, a few minutes before starting the procedure. All employees contributing to the study were blinded for the spinal medication. In cases where sensory block did not reached T6 within 20 min after the injection, a general anesthetic was administered. If spinal anesthesia failed, the patients were given epidural drugs, and be excluded from this study. If the patients experienced any discomfort such as back pain, stomach discomfort after the fetal delivery, intravenous fentanyl 0.05mg would be given immediately. If not relieved, another fentanyl 0.05mg would be given. If the patients felt pain around surgery area or the surgeons felt abdominal muscle relaxant not enough, 2% lidocaine 5ml would be given through epidural catheter. If not effective, 2% lidocaine 5ml would be given after 5min. Rescue lidocaine dose with time and fentanyl total dose would be recorded. When the surgeon closed peritoneum, morphine 2.5mg would be given by epidural route as postoperative analgesia. Blood collection finished before anesthesia and after operation. If shivering happened, tramadol 100mg were given intraoperation.
If the patient’s VAS was more than 4 after surgery, the surgeon would give them diclofenac sodium and lidocaine hydrochloride injection. If the patient was shivering later on postoperatively, promethazine 12.5mg would be given.
Measurements
Sensory block was evaluated every 5 min with a pinprick test. Motor block was evaluated with the Bromage scale (0 = no motor loss, 1 = inability to flex the hip, 2 = inability to flex the knee, and 3 = inability to flex the ankle). The following parameters were observed immediately after the administration of spinal block: Maximum sensory level, time to maximum sensory level, duration of motor block (two lower limbs bromage score return to 0), the onset time of operation, fetal delivery time, supplemental lidocaine dose and time intraoperation, supplemental fentanyl dose, visceral pain, abdominal muscle relaxation, patients VAS 6, 12 hour after surgery, first rescue analgesia drug time and the first anal aerofluxus time (the first anal aerofluxus time, anus exhausting time. It reflected the recovery time of gastrointestinal function recovery.). Side effects include shivering, nausea and vomiting, hypotension, pruritus etc.
The hemodynamic parameters include systolic pressure(SP), diastolic pressure (DP), heart rate (HR), the saturation of pulse oximetry at 0, 3, 5, 10, 15, 20, 30, 40, 50, 60 minutes after spinal anesthesia, and dose of phenylephrine at 10, 20 minutes after the spinal anesthesia. If the systolic pressure decreases 20%, or less than 100mmHg, phenylepherine 60-80μg would be given. Umbilical blood gas analysis includes fetal blood pH, oxygen partial pressure, carbon dioxide partial pressure, lactate and Apgar scores.
Statistic analysis
Data are expressed as mean±SD. Statistical analysis was performed using SAS9.1. ANOVA and χ2 test were used for analysis of the standard characteristics, the degree of motor block, sensory block level, maternal side effects, fetal delivery and postoperative analgesia. Analysis of variance for repeated data was used to compare hemodynamic characteristics. P-value less than 0.05 was considered statistically significant for all comparisons.
Aurthor contributions
All authors contributed equally.
ACKNOWLEDGMENTS
We thank Dr. Xuan Chen for great support in obstetric surgery as well as Xiaohai Xu and others for assistance with arterial blood gas analysis.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Gupta R, Verma R, Bogra J, Kohli M, Raman R, Kushwaha JK. A comparative study of intrathecal dexmedetomidine and fentanyl as adjuvants to bupivacaine. J Anaesthesiol Clin Pharmacol. 2011; 27: 339-343. doi: 10.4103/0970-9185.83678.
2. Bremerich DH, Fetsch N, Zwissler BC, Meininger D, Gogarten W, Byhahn C. Comparison of intrathecal bupivacaine and levobupivacaine combined with opioids for caesarean section. Curr Med Res Opin. 2007; 23: 3047-3054. doi: 10.1185/030079907X242764.
3. Hamber EA, Viscomi CM. Intrathecal lipophilic opioids as adjuncts to surgical spinal anesthesia. Reg Anesth Pain Med. 1999; 24: 255-263. doi: 10.1016/S1098-7339(99)90139-6.
4. Bogra J, Arora N, Srivastava P. Synergistic effect of intrathecal fentanyl and bupivacaine in spinal anesthesia for cesarean section. BMC Anesthesiol. 2005; 5: 5. doi: 10.1186/1471-2253-5-5.
5. Sapate M, Sahu P, Thatte WS, Dubey R. A randomized, double blind, control study of the effects of adding nalbuphine to spinal bupivacaine for lower abdominal surgeries in elderly patients. Anaesth Pain &Intensive Care. 2013; 17: 145-148.
6. Shukry M, Miller JA. Update on dexmedetomidine: use in nonintubated patients requiring sedation for surgical procedures. Ther Clin Risk Manag. 2010; 6: 111-121.
7. Elia N, Culebras X, Mazza C, Schiffer E, Tramèr MR, Phil D. Clonidine as an adjuvant to intrathecal local surgery: systematic review of randomized trials. Reg Anesth Pain Med. 2008; 33: 159-167. doi: 10.1016/j.rapm.2007.10.008.
8. Ishii H, Kohno T, Yamakura T, Ikoma M, Baba H. Action of dexmedetomidine on the substantia gelatinosa neurons of the rat spinal cord. Eur J Neurosci. 2008; 27: 3182-3190. doi: 10.1111/j.1460-9568.2008.06260.x.
9. Kalso EA, Pöyhiä R, Rosenberg PH. Spinal antinociception by dexmedetomidine, a highly selective a2-adrenergic agonist. Pharmacol Toxicol. 1991; 68: 140-143. doi: 10.1111/j.1600-0773.1991.tb02052.x.
10. Kanazi GE, Aouad MT, Jabbour-Khoury SI, Jabbour-Khoury SI, Al-Jazzar MD, Alameddine MM, Al-Yaman R, Bulbul M, Baraka AS. Effect of low-dose dexmedetomidine or clonidine on the characteristics of bupivacaine spinal block. Acta Anaesthesiol Scand. 2006; 50: 222-227. doi: 10.1111/j.1399-6576.2006.00919.x.
11. Kim JE, Kim NY, Lee HS, Kil HK. Effects of intrathecal dexmedetomidine on low-dose bupivacaine spinal anesthesia in elderly patients undergoing transurethral prostatectomy. Biol Pharm Bull. 2013; 36: 959-965.
12. Al-Mustafa MM, Abu-Halaweh SA, Aloweidi AS, Murshidi MM, Ammari BA, Awwad ZM, Al-Edwan GM, Ramsay MA. Effect of dexmedetomidine added to spinal bupivacaine for urological procedures. Saudi Med J. 2009; 30: 365-370.
13. Mahendru V, Tewari A, Katyal S, Grewal A, Singh MR, Katyal R. A comparison of intrathecal dexmedetomidine, clonidine, and fentanyl as adjuvants to hyperbaric bupivacaine for lower limb surgery: a double blind controlled study. J Anaesthesiol Clin Pharmacol. 2013; 29: 496-502. doi: 10.4103/0970-9185.119151.
14. Sarma J, Narayana PS, Ganapathi P, Shivakumar MC. A comparative study of intrathecal clonidine and dexmedetomidine on characteristics of bupivacaine spinal block for lower limb surgeries. Anesth Essays Res. 2015; 9: 195-207. doi: 10.4103/0259-1162.153763.
15. Sun Y, Xu Y, Wang GN. Comparative evaluation of intrathecal bupivacaine alone, bubivacaine-fentanyl, and bupivacaine-dexmedetomidine in cesarean section. Drug Res (Stuttg). 2015; 65: 468-472. doi: 10.1055/s-0034-1387740.
16. Li Z, Tian M, Zhang CY, Li AZ, Huang AJ, Shi CX, Xin DQ, Qi J, Li KZ. A randomized controlled trial to evaluate the effectiveness of intrathecal bupivacaine combined with different adjuvants (fentanyl, clonidine and dexmedetomidine) in caesarean section. Drug Res. 2014; 65: 581-586. doi: 10.1055/s-0034-1395614.
17. Vercauteren M. Obstetric spinal analgesia and anesthesia. Curr Opin Anesthesol. 2003; 16: 503-507. doi: 10.1097/01.aco.0000094509.08873.53.
18. Shetty PS, Picard J. Adjuvant agents in regional anaesthesia. Anesth Intensive Care Med. 2006; 7: 407-410. doi: 10.1053/j.mpaic.2006.08.004.
19. Al-Ghanem SM, Massad IM, Al-Mustafa MM, Al-Zaben KR, Qudaisat IY, Qatawneh AM, Abu-Ali HM. Effect of adding dexmedetomidine vesus fentanyl to intrathecal bupivacaine on spinal block characteristics in gynecological procedures: a double blind controlled study. Am J Appl Sci. 2009; 6: 882-887. doi: 10.3844/ajassp.2009.882.887.
20. Harada Y, Nishioka K, Kitahata LM, Kishikawa K, Collins JG. Visceral antinociceptive effects of spinal clonidine combined with morphine, [D-Pen2,D-Pen5] enkephalin, oR U50,488H. Anesthesilology. 1995; 83: 344-352. doi: 10.1007/s002560100351.
21. Civantos Calzada B, Aleixandre de Artinano A. Alpha-adrenoceptor subtypes. Pharmacol Res. 2001; 44: 195-208. doi: 10.1006/phrs.2001.0857.
22. McKinlay J, Lyons G. Obstetric neuraxial anesthesia: which presser agents should we be using. Int J Obstet Anesth. 2002; 11: 117- 121. doi: 10.1054/ijoa.2001.0926.
23. Lee A, Ngan Kee WD, Gin T. A quantitative systematic review of randomized controlled trials of epherdrine verus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery. Anesth Analg. 2002; 94: 920-926. doi: 10.1097/00000539-200204000-00028.
24. El-Tahan MR, Mowafi HA, Al Sheikh IH, Khidr AM, Al-Juhaiman RA. Efficacy of dexmedetomidine in suppressing cardiovascular and hormonal responses to general anesthesia for cesarean delivery: a dose response study. Int J Obstet Anesth. 2012; 21: 222-229. doi: 10.1016/j.ijoa.2012.04.006.
25. Nasr DA, Abdelhamid HM. The efficacy of caudal dexmedetomidine on stress response and postoperative pain in pediatric cardiac surgery. Ann Card Anesth. 2013; 16: 109-114. doi: 10.410310971-9784.1044.
26. Kang SH, KimYS, HongTH, Chae MS, Cho ML, Her YM, Lee J. Effects of dexmedetomidine on inflammatory responses in patients undergoing laparoscopic cholecystectomy. Acta Anaesthesiol Scand. 2013; 57: 480-487. doi: 10.1111/aas.12039.
27. Nour EM, Othman MM, Karrouf GI, Zaghloul AE. Comparative evaluation of the epidural dexmedetomidine, ketamine or fentanyl in combination with bupivacine in dogs undergoing castration. Life Sci J. 2013; 10: 1051-1057.
28. Talke P, Tayefeh F, Sessler DI, Jeffrey RB, Noursalehi M, Richardson C. Dexmedetomidine does not alter the sweating threshold, but comparably and linearly decreases the vasoconstriction and shivering thresholds. Anesthesiology. 1997; 87: 835-841. doi: 10.1097/00000542-199710000-00017.
29. Tekin M, Kati I, Tomak Y, Kisli E. Effect of dexmedetomidine IV on the duration of spinal anesthesia with Prilocaine: a double-blind, prospective study in adult surgical patients. Curr Ther Res Clin Exp. 2007; 68: 313-324. doi: 10.1016/j.curtheres.2007.10.006.
30. Dinesh CN, Sai Tej NA, Yatish B, Pujari VS, Mohan Kumar RM, Mohan CV. Effects of intravenous dexmedetomidine on hyperbaric bupivacaine spinal anesthesia: a randomized study. Saudi J Anaesth. 2014; 8: 202-208. doi: 10.4103/1658-354X.130719.
31. Paech MJ, Pavy TJ, Orlikowski CE, Yeo ST, Banks SL, Evans SF, Henderson J. Postcesarean analgesia with spinal morphine, clonidine, or their combination. Anesth Analg. 2004; 98: 1460-1466. doi: 10.1213101.ANE.0000111208.08867.3C.
32. Al-Mustafa MM, Badran IZ, Abu-Ali HM, Al-Barazangi BA, Massad IM, Al-Ghanem SM. Intravenous dexmedetomidine prolongs bupivacaine spinal analgesia. Middle East J Anesthesiol. 2009; 20: 225-231.
33. Nethra SS, Sathesha M, Dixit A, Dongare PA, Harsoor SS, Devikarani D. Intrathecal dexmedetomidine as adjuvant for spinal anaesthesia for perianal ambulatory surgeries: a randomized double-blind controlled study. Indian J Anaesth. 2015; 59: 177-181. doi: 10.4103/0019-5049.153040.
34. Bajwa SJ, Bajwa SK. Impact of epidural analgesia on breast feeding: a possible relation and the existing controversies. J Obstet Anaesth Crit Care. 2012; 2: 57-59. doi: 10.4103/2249-4472.99337.