
Introduction
Postoperative sleep disturbance and fatigue are high risk factors to prolonged convalescence and additional hospital costs. Recent studies reported that aesthesia management may affect postoperative outcomes to promote recovery. For example, clinical trials have found that intraoperative use of dexmedetomidine for general anesthesia, a highly selective alpha-2 adrenergic agonist, was able to attenuate postoperative fatigue, promote recovery, facilitate the analgesic property of PCA morphine, reduce morphine consumption as well as its related adverse effects [1-11]. A more recent study indicated that low-dose infusion of dexmedetomidine are able to promote sleep quality in nonmechanically ventilated elderly patients in the ICU following operations [12]. Dexmedetomidine was also reported to improve postoperative outcomes in breast cancer patients following operations, such as displaying analgesia-promoting effect on acute and chronic pain [4, 10, 11].
Based on the evidence above, we hypothesized that intraoperative use of dexmedetomidine might promote the sleep quality and recovery in breast cancer patients following radical mastectomy under general anesthesia.
materials and Methods
Participants
This study was approved by the Institutional Medical Ethics Committee of The Affiliated Yuntai Yuhuangding Hospital of Qingdao University, and was in accordance with the approved guidelines. Written informed consent was obtained from each patient. The sample size of the study was calculated according to previous studies, and was based on a pilot study. Twenty patients in each group were required to detect a difference of sleep time (primary outcome) with a power of 0.8 and type I error of 0.05. To compensate for dropouts and deviation from normality, a total of 56 patients scheduled for radical mastectomy under general anesthesia were assessed for eligibility. We targeted an 80% probability (β = 0.2) with a significance level of 0.05 and a ~10% dropout rate. Finally, forty-seven patients enrolled were analyzed in Control (n = 23), and DEX (n = 24) based on their treatment. Patients received propofol, remifentanil, and Ringer’s solution or dexmedetomidine for general anesthesia maintenance, respectively. To be blind, the maintenance syringe pump was prepared by a different anesthesiologist. NRS score evaluated by another different anesthesiologist(see Supplementary File-2). Total sleeping time was recorded following operation starting form 8:00PM to 8:00 AM. Patients matching the following criteria were included in this study: American Society of Anesthesiologists (ASA) grade II or III; between 30 and 60 years old; weight 45-75 kg; height 145-175 cm. Patients were excluded if they had a history of opioid addiction, long-term alcohol abuse or smoking history, current use of sedative-hypnotic drug(s); obesity (BMI > 30); sleep disorders, postoperative nausea and vomiting history; or neuropsychiatric diseases and related treatment history.
Anesthesia
Before induction, patients from the DEX group received a fast infusion of 100 ml Ringer solution with or without DEX (1μg/kg) as a loading dose within 15 min. For induction, patients from both groups received midazolam (0.05 mg/kg), remifentanil (2-5 μg/kg), propofol (1.5-2 mg/kg), and cisatracurium (0.2 mg/kg). Immediately after intubation, the patients were ventilated with an oxygen and air mixture (FiO2 = 0.4) with a PetCO2 of 30-35 mmHg. Intravenous infusion was switched to a maintenance syringe pump at rate of 50-80 μg/kg/min for propofol, 0.15-0.2 μg/kg/min for remifentanil, and 0.4 μg/kg/h for dexmedetomidine. Cisatracurium (0.05 mg/kg) was intermittently used for muscle relaxation. Patients were transferred to the PACU after extubation.
Statistics
All data were presented as mean ± SD. or the exact values, and analyzed with GraphPad Prism 6.0 software. Age, weight, height, blood pressure, heart rates, operation time, anesthesia time, PACU time and sleep time were compared with unpaired student’s t test. Recovery and fatigue scores at different time points were compared between the two group with two-way ANOVA followed by Bonferroni post-test. ASA grade and postoperative adverse effects were analyzed with Fisher’s test. P < 0.05 were considered to be significant.
Results
Demographic data of participants
A total of 56 patients scheduled for radical mastectomy under general anesthesia were assessed for eligibility. Nine patients were excluded due to ineligibility. Finally, 47 patients were enrolled in this clinical observation trail and randomized into two groups: Control group (23 patients) and D group (24 patients), which received either propofol/remifentanil and Ringer’s solution or dexmedetomidine (Figure 1). Patients from the two groups were comparable with respect to age, weight, height, BMI, ASA class, baseline MBP, 24 hour MBP, baseline HR, 24 hour heart rate, operation time, anesthesia time, and PACU time (Table 1).
Table 1: Basic demographic data and surgery duration (mean ± SD).
Variables |
Control (n= 23) |
DEX (n = 24) |
Values of P |
Age (years) |
47.74 (8.735) |
49.17 (8.458) |
0.572 |
Weight (Kg) |
53.46 (14.85) |
51.49 (11.18) |
0.609 |
Height |
161.10 (6.324) |
161.3 (6.587) |
0.930 |
BMI (Kg/m2) |
26.44 (2.546) |
25.58 (2.325) |
0.235 |
ASA II/III |
17/6 |
21/3 |
0.287 |
Baseline MBP (mmHg) |
83.41 (4.758) |
83.52 (5.399) |
0.944 |
24 hour MBP (mmHg) |
89.36 (7.832) |
88.67 (8.977) |
0.7812 |
Baseline HR (beats/min) |
70.57 (7.948) |
73.25 (6.469) |
0.2091 |
24 hour HR (beats/min) |
70.57 (7.948) |
73.25 (6.449) |
0.5081 |
Operation time (min) |
140.30 (18.67) |
134.0 (16.05) |
0.214 |
Anesthesia time (min) |
168.10 (22.78) |
166.9 (22.51) |
0.855 |
PACU time (min) |
43.70 (4.733) |
42.04 (4.912) |
0.0447 |
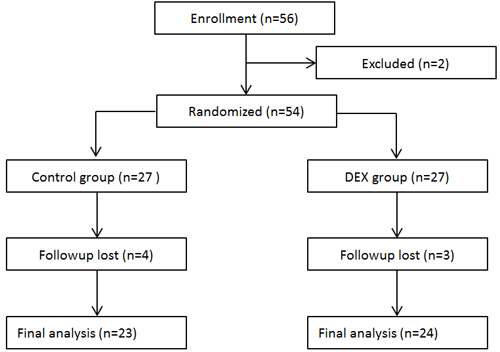
Figure 1: Flow diagram of the study.
Postoperative sleep time of the two groups
Postoperative sleep time was monitored from 8:00 PM on the operation day to next 8:00 AM for 12 hours. During first 12 hours, patients from the DEX group had a longer sleep time as compared with patients from the Control group (Figure 2).
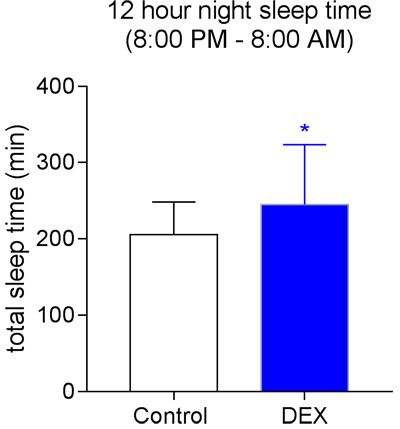
Figure 2: Postoperative 12 hour night sleep time from 8:00 PM to 8:00 AM. *P = 0.0381.
Postoperative recovery and fatigue evaluation
Postoperative recovery was evaluated with the global 40-item quality of recovery questionnaire. Lower scores were observed on day 1 following operation in the two groups. At POD 3 time point, patients in the DEX group shown significantly higher scores compared with their Control group. Patients from the two groups both recovered to their baseline level at POD 7 time point (Figure 3A).
Similarly, Patients in the DEX group had a lower fatigue severity score than those in the Control group at both POD3 and POD7 time points (Figure 3B).
Table 2: Adverse effects.
Variables (+/-) |
Control (n= 23) |
DEX (n= 24) |
Values of P |
Nausea |
13/10 |
8/16 |
0.1468 |
Vomitting |
11/12 |
6/18 |
0.0392 |
Bradycardia |
3/20 |
4/20 |
>0.9999 |
Respiratory depression |
0/23 |
0/24 |
>0.9999 |
Itching |
2/21 |
1/23 |
0.6085 |
+/-: positive patient number/ negative patient number.
Postoperative adverse effects
A decreased incidence vomiting and a trending decrease of nausea were observed during the first 24 hours in the patients from DEX group when compared with those from the Control group (Table 2). No difference was observed in other adverse effects between the two groups.
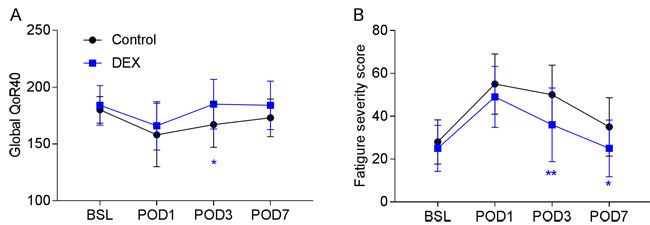
Figure 3: Postoperative recovery in the two groups. A. Global 40-item quality of recovery questionnaire evaluation, *P < 0.05. B. Nine question fatigue scores, *P < 0.05, **P < 0.01. BSL: baseline, POD: post-operative day.
Discussion
The present study have found that general anesthesia maintained with dexmedetomidine improved sleep disturbance and promote recovery following radical mastectomy in patients with breast cancer. The adverse effect of dexmedetomidine on sleep disturbance might be contributed to its recovery-promoting effect.
Radical mastectomy under general anesthesia is a widely-used therapy in patients with breast cancer [13-15]. It has been known that breast cancer patients undergoing radical mastectomy experience severe sleep disturbance and fatigue [16, 17], which might lead to prolonged convalescence and additional hospital costs. There has been a pursuit for novel drugs or for more information regarding combining the currently-available drugs to alleviate these symptoms. Dexmedetomidine is a alpha-2 receptor agonist developed in the 1990s, and it was first introduced into hospital as a sedative in ventilated patient in the intensive care unit [18]. Unexpectedly, it emerged as an adjuvant of local/general anesthetics and opioids for local and general analgesia [19-21] to improve analgesic effects of local anesthetics or general anesthesia.
Clinical trails have recently reported that intraoperative use of dexmedetomidine promoted morphine’s analgesic property in patient-controlled analgesia and postoperative recovery, which might contribute to the recovery-promoting effect of dexmedetomidine following different kinds of operations [1, 6, 22]. In the present study, we further found a novel effect of intraoperative use of dexmedetomidine for general anesthesia maintenance on sleep disturbance: during the first 12 hours of night sleeping, patients from the DEX group spend more time sleeping when compared with the Control groups, which might be a contributor to the recovery-promoting effect of dexmedetomidine. Consistent with recent studies from different centers [6, 23-25], using a global 40-item questionnaire, we observed that the Global QoR-40 score was significantly improved in the DEX group on day 3 after surgery. All of the patients shown higher fatigue level after surgery, but on day 3 and day 7 after surgery, patients in the DEX group reported significantly lower scores for fatigue severity than their controls. Many factors are responsible for slow recovery from surgery, including postoperative acute pain, fatigue, and surgery-induced metabolic, endocrine, and immune changes known as ‘stress responses’. Recently, Dong-Jian Ge and colleagues proposed that the inhibitory effect of dexmedetomidine on the vicious cycle among surgery-induced stress responses, fatigue and acute pain to interpret the recovery-promoting effect of dexmedetomidine [6]. Poor sleep quality was associated high fatigue severity and postoperative stress response [26, 27]. Studies from another group in China recently reported that low-dose dexmedetomidine infusion may improve overall sleep quality in nonmechanically ventilated elderly patients in patients following noncardiac surgery [28, 29].
Thus, improved sleep quality/time might be helpful to reduce fatigue and postoperative stress responses. Collectively, we believe that together with its reversive effect on sleep disturbance, the proposal above will better interpret the recovery-promoting effect of intraoperative use of dexmedetomidine.
There might be limitations in the present study: 1) The study was performed only in female patients, 2) For the observation of sleep conditions, we only studied the total sleep time and did not look at different subtypes of sleep, such as rapid and non-rapid eye movement sleep, 3) To exclude the effect of diurnal rhythm, the total recording time of sleep started from 8:00P M to 8:00 AM, however, the operation time was variable among patients.
Collectively, this study found that general anesthesia combined with dexmedetomidine was useful for promoting postoperative recovery in breast cancer patients following radical mastectomy. Furthermore, the adverse effect of dexmedetomidine on sleep disturbance might be a novel contributor to interpret the recovery-promoting effect of intraoperative use of dexmedetomidine.
Author contributions
C.S. and J.J. conceived of this study, C.S., J.J., Q.P, S.S., K.L., J.M. and T.L. performed the experiments, and C.S. and J.J. analyzed the results and wrote the manuscript. All of the authors reviewed the manuscript.
ConflictS of Interest
There is no conflict of interest.
FUNDING
This work was supported by Traditional Chinese Medicine Science and Technology Development Project of Shandong Province (2015-416) and Natural Science Foundation of Shandong province (ZR2016HL17). This work was supported by Traditional Chinese Medicine Science and Technology Development Project of Shandong Province (2015-416) and Natural Science Foundation of Shandong province (ZR2016HL17 and ZR2014HL109).
References
1. Zhao JN, Kong M, Qi B, Ge DJ. Comparison of the morphine-sparing effect of intraoperative dexmedetomidine with and without loading dose following general anesthesia in multiple-fracture patients: A prospective, randomized, controlled clinical trial. Medicine (Baltimore). 2016; 95: e4576. doi: 10.1097/md.0000000000004576.
2. Wang W, Feng L, Bai F, Zhang Z, Zhao Y, Ren C. The Safety and Efficacy of Dexmedetomidine vs. Sufentanil in Monitored Anesthesia Care during Burr-Hole Surgery for Chronic Subdural Hematoma: A Retrospective Clinical Trial. Front Pharmacol. 2016; 7: 410. doi: 10.3389/fphar.2016.00410.
3. Su S, Ren C, Zhang H, Liu Z, Zhang Z. The Opioid-Sparing Effect of Perioperative Dexmedetomidine Plus Sufentanil Infusion during Neurosurgery: A Retrospective Study. Front Pharmacol. 2016; 7: 407. doi: 10.3389/fphar.2016.00407.
4. Mohta M, Kalra B, Sethi AK, Kaur N. Efficacy of dexmedetomidine as an adjuvant in paravertebral block in breast cancer surgery. J Anesth. 2016; 30: 252-60. doi: 10.1007/s00540-015-2123-8.
5. Li YY, Ge DJ, Li JY, Qi B. Sex Differences in the Morphine-Sparing Effects of Intraoperative Dexmedetomidine in Patient-Controlled Analgesia Following General Anesthesia: A Consort-Prospective, Randomized, Controlled Clinical Trial. Medicine (Baltimore). 2016; 95: e3619. doi: 10.1097/md.0000000000003619.
6. Ge DJ, Qi B, Tang G, Li JY. Intraoperative Dexmedetomidine Promotes Postoperative Analgesia and Recovery in Patients after Abdominal Hysterectomy: a Double-Blind, Randomized Clinical Trial. Sci Rep. 2016; 6: 21514. doi: 10.1038/srep21514.
7. Ren C, Zhang X, Liu Z, Li C, Zhang Z, Qi F. Effect of Intraoperative and Postoperative Infusion of Dexmedetomidine on the Quality of Postoperative Analgesia in Highly Nicotine-Dependent Patients After Thoracic Surgery: A CONSORT-Prospective, Randomized, Controlled Trial. Medicine (Baltimore). 2015; 94: e1329. doi: 10.1097/md.0000000000001329.
8. Ge DJ, Qi B, Tang G, Li JY. Intraoperative Dexmedetomidine Promotes Postoperative Analgesia in Patients After Abdominal Colectomy: A Consort-Prospective, Randomized, Controlled Clinical Trial. Medicine (Baltimore). 2015; 94: e1514. doi: 10.1097/md.0000000000001514.
9. Ge DJ, Qi B, Tang G, Li JY. Intraoperative Dexmedetomidine Promotes Postoperative Analgesia and Recovery in Patients after Abdominal Colectomy: A CONSORT-Prospective, Randomized, Controlled Clinical Trial. Medicine (Baltimore). 2015; 94: e1727. doi: 10.1097/md.0000000000001727.
10. Mohamed SA, Fares KM, Mohamed AA, Alieldin NH. Dexmedetomidine as an adjunctive analgesic with bupivacaine in paravertebral analgesia for breast cancer surgery. Pain Physician. 2014; 17: E589-98.
11. Jain G, Bansal P, Ahmad B, Singh DK, Yadav G. Effect of the perioperative infusion of dexmedetomidine on chronic pain after breast surgery. Indian J Palliat Care. 2012; 18: 45-51. doi: 10.4103/0973-1075.97354.
12. Kim SH, Oh YJ, Park BW, Sim J, Choi YS. Effects of single-dose dexmedetomidine on the quality of recovery after modified radical mastectomy: a randomised controlled trial. Minerva Anestesiol. 2013; 79: 1248-58.
13. Park K, Park S, Jeon MJ, Choi J, Kim JW, Cho YJ, Jang WS, Keum YS, Lee IJ. Clinical application of 3D-printed-step-bolus in post-total-mastectomy electron conformal therapy. Oncotarget. 2016; 8:25660-25668. doi: 10.18632/oncotarget.12829.
14. Wang H, Kong L, Zhang C, Chen D, Zhu H, Yu J. Should all breast cancer patients with four or more positive lymph nodes who underwent modified radical mastectomy be treated with postoperative radiotherapy? A population-based study. Oncotarget. 2016; 7: 75492-502. doi: 10.18632/oncotarget.12260.
15. Zhou N, Liu C, Hou H, Zhang C, Liu D, Wang G, Liu K, Zhu J, Lv H, Li T, Zhang X. Response to apatinib in chemotherapy-failed advanced spindle cell breast carcinoma. Oncotarget. 2016; 7: 72373-9. doi: 10.18632/oncotarget.12568.
16. Berger AM, Kuhn BR, Farr LA, Lynch JC, Agrawal S, Chamberlain J, Von Essen SG. Behavioral therapy intervention trial to improve sleep quality and cancer-related fatigue. Psychooncology. 2009; 18: 634-46. doi: 10.1002/pon.1438.
17. Gerber LH, Stout N, McGarvey C, Soballe P, Shieh CY, Diao G, Springer BA, Pfalzer LA. Factors predicting clinically significant fatigue in women following treatment for primary breast cancer. Support Care Cancer. 2011; 19: 1581-91. doi: 10.1007/s00520-010-0986-7.
18. Rosenzweig AB, Sittambalam CD. A new approach to the prevention and treatment of delirium in elderly patients in the intensive care unit. J Community Hosp Intern Med Perspect. 2015; 5: 27950. doi: 10.3402/jchimp.v5.27950.
19. Marhofer P, Brummett CM. Safety and efficiency of dexmedetomidine as adjuvant to local anesthetics. Curr Opin Anaesthesiol. 2016; 29: 632-7. doi: 10.1097/aco.0000000000000364.
20. Li A, Yuen VM, Goulay-Dufay S, Kwok PC. Pharmacokinetics and pharmacodynamics of dexmedetomidine. Drug Dev Ind Pharm. 2016; 42: 1917-27. doi: 10.1080/03639045.2016.1232727.
21. Gruenbaum SE, Meng L, Bilotta F. Recent trends in the anesthetic management of craniotomy for supratentorial tumor resection. Curr Opin Anaesthesiol. 2016; 29: 552-7. doi: 10.1097/aco.0000000000000365.
22. Bekker A, Haile M, Kline R, Didehvar S, Babu R, Martiniuk F, Urban M. The effect of intraoperative infusion of dexmedetomidine on the quality of recovery after major spinal surgery. J Neurosurg Anesthesiol. 2013; 25: 16-24. doi: 10.1097/ANA.0b013e31826318af.
23. George RB, McKeen DM, Andreou P, Habib AS. A randomized placebo-controlled trial of two doses of pregabalin for postoperative analgesia in patients undergoing abdominal hysterectomy. Can J Anaesth. 2014; 61: 551-7. doi: 10.1007/s12630-014-0147-4.
24. Engelman E, Marsala C. Efficacy of adding clonidine to intrathecal morphine in acute postoperative pain: meta-analysis. Br J Anaesth. 2013; 110: 21-7. doi: 10.1093/bja/aes344.
25. Lambert P, Cyna AM, Knight N, Middleton P. Clonidine premedication for postoperative analgesia in children. Cochrane Database Syst Rev. 2014; 28. doi: 10.1002/14651858.CD009633.pub2.
26. Rodrigue JR, Mandelbrot DA, Hanto DW, Johnson SR, Karp SJ, Pavlakis M. A cross-sectional study of fatigue and sleep quality before and after kidney transplantation. Clin Transplant. 2011; 25: E13-21. doi: 10.1111/j.1399-0012.2010.01326.x.
27. Nerbass FB, Feltrim MI, Souza SA, Ykeda DS, Lorenzi-Filho G. Effects of massage therapy on sleep quality after coronary artery bypass graft surgery. Clinics (Sao Paulo). 2010; 65: 1105-10.
28. Wu XH, Cui F, Zhang C, Meng ZT, Wang DX, Ma J, Wang GF, Zhu SN, Ma D. Low-dose Dexmedetomidine Improves Sleep Quality Pattern in Elderly Patients after Noncardiac Surgery in the Intensive Care Unit: A Pilot Randomized Controlled Trial. Anesthesiology. 2016; 125: 979-91. doi: 10.1097/aln.0000000000001325.
29. Su X, Meng ZT, Wu XH, Cui F, Li HL, Wang DX, Zhu X, Zhu SN, Maze M, Ma D. Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery: a randomised, double-blind, placebo-controlled trial. Lancet. 2016; 388: 1893-902. doi: 10.1016/s0140-6736(16)30580-3.