
INTRODUCTION
Variceal rebleeding is a frequent and severe complication in cirrhotic patients. Patients who survive an episode of acute variceal hemorrhage are at increased risk of rebleeding and death. The median rebleeding rate in untreated individuals is approximately 60% and the mortality rate is 33% within 1-2 years of the hemorrhage [1–3]. Pharmacotherapy, endoscopic variceal ligation (EVL), and the transjugular intrahepatic portosystemic shunt (TIPS) are the recommended interventions for the prevention of variceal bleeding. Drug therapy, more specifically nonselective β-blockers or a combination of isosorbide mononitrate (ISMN) and nadolol, has been found to reduce portal pressure and prevent variceal rebleeding [4, 5]. Ligation is reported to be more effective at reducing patient mortality than sclerotherapy [6]. In addition, EVL achieves variceal obliteration with fewer endoscopic sessions and has been found to be effective in controlling active variceal bleeding [7–10]. The TIPS procedure is a minimally invasive, image-guided intervention used for secondary prevention of bleeding and as salvage therapy in acute bleeding [11]. TIPS were created with Wallstents (Schneider, Inc., Plymouth, Minnesota) using standard techniques described elsewhere, and effectively control bleeding in patients with refractory variceal hemorrhage [12, 13].
Several randomized controlled trials (RCTs) have reported the differences in efficacy between these interventions in the control of esophageal variceal bleeding. Although drug therapy was stated to be as effective as EVL in current studies [14, 15], it has also been reported that combination therapy is more effective than EVL or drug therapy alone for reducing the risk of rebleeding, although the effect on mortality was unclear [15, 16]. Moreover, there is evidence to suggest that TIPS is more effective at reducing rebleeding than drug therapy or EVL [17–19]. However, whether the TIPS is more effective than combination therapy (pharmacotherapy and EVL) has not been investigated. Therefore, we performed a meta-analysis of randomized trials to assess the efficacy of combination therapy (pharmacotherapy and EVL) compared with pharmacotherapy, EVL, or TIPS alone in the prevention of rebleeding and mortality in this study.
RESULTS
Characteristics of individual studies
We identified 2153 publications from the electronic databases (Figure 1), of which 516 were excluded as duplicates and 1358 were excluded based on selection criteria. This resulted in 279 articles, which were independently read by two authors. Eventually, ten studies involving 1076 patients were included in our meta-analysis [20–29]. The characteristics of each individual study are presented in Table 1.
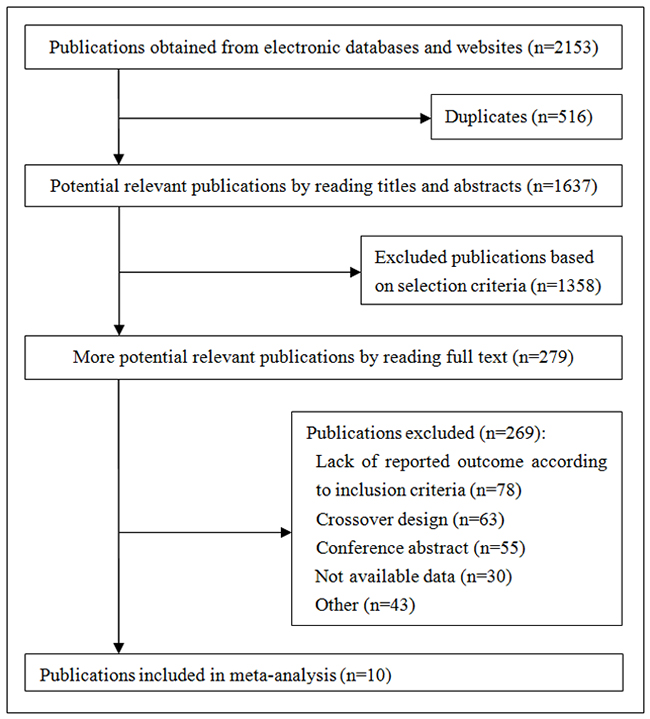
Figure 1: Summary of trial identification and selection.
Table 1: The characteristics of each individual study
Study |
Year |
Country |
Patients (C/M) |
Mean age (C/M) |
Male/female |
Alcohol (C/M) |
Viral (C/M) |
Child score (C/M) |
Combination therapy |
Monotherapy |
Follow-up time (months) |
||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
A |
B |
C |
|||||||||||
Lo [26] |
2000 |
China |
60/62 |
53± 11/51± 12 |
94/28 |
17/20 |
41/41 |
11/12 |
12/18 |
19/22 |
Nadolol 60mg/day, 1-2 bands |
1-2 bands |
22/21 |
De la Pena [27] |
2005 |
Spain |
43/37 |
60/60 |
60/20 |
27/26 |
112/8 |
6/6 |
25/20 |
2/11 |
Nadolol 58mg/day, EVL |
NA |
17.5/17 |
Jain [28] |
2006 |
American |
61/67 |
NA |
NA |
NA |
NA |
26/24 |
23/37 |
12/6 |
Propranolol 114.3mg/day, EVL |
NA |
NA |
Kumar [29] |
2009 |
India |
88/89 |
42(14)/41(14) |
153/24 |
33/30 |
13/20 |
35/26 |
31/34 |
10/15 |
Propranolol 120mg/day, ISMN 40mg/day, 2-10 bands |
2-10 bands |
15/15 |
Lo (a) [30] |
2009 |
Taiwan |
47/46 |
52±11/50±12 |
77/16 |
15/17 |
28/26 |
13/14 |
20/25 |
14/7 |
Terlipressin 4mg/day, 4 bands |
Terlipressin 1 mg/6h for 5 days |
NA |
Lo (b) [31] |
2009 |
Taiwan |
60/60 |
54±10/52±11 |
87/33 |
21/15 |
31/40 |
20/21 |
29/31 |
11/8 |
Nadolol 40 mg/day, ISMN 20mg/day, EVL |
Nadolol 40 mg/day, ISMN 20mg/day |
22.3/22.7 |
Garcia-Pagan [32] |
2009 |
Spain |
80/78 |
57±12/56±11 |
118/40 |
39/42 |
25/18 |
16/18 |
46/42 |
18/18 |
Nadolol 36mg/day, ISMN 36mg/day, EVL |
Nadolol 36mg/day, ISMN 36mg/day |
14.4/15.3 |
Garcia-Pagan [35] |
2010 |
Spain |
31/32 |
49±6/52±10 |
44/19 |
20/22 |
5/4 |
NA |
16/16 |
15/16 |
Propranolol 55mg/day, ISMN 25mg/day, EVL |
e-PTFE–covered stents: 10mm |
14 |
Luo [33] |
2015 |
China |
36/37 |
50.78±13.61/ 49.53±14.02 |
43/30 |
2/4 |
30/26 |
NA |
25/24 |
12/12 |
Propranolol, 65.4 mg/day, 4-6 bands |
e-PTFE–covered stents: 10mm |
20.9/22.8 |
Holster [34] |
2016 |
Netherlands |
35/37 |
54/56 |
41/31 |
18/13 |
1/7 |
13/13 |
18/19 |
4/5 |
Terlipressin 6-12mg/day, 4.3 bands |
Balloon-expandable stent: 8 mm in 21 patients, 10 mm in 10 patients |
23 |
C/M, combination therapy/monotherapy; EVL, endoscopic variceal ligation; ISMN, isosorbide mononitrate; e-PTFE, extended polytetrafluoroethylene; NA, not available.
Quality of the included studies
The risk of bias in the included studies was strictly evaluated. Details of methodological approach are presented in Table 2.
Table 2: The risk of bias in the included studies
Study |
Year |
Random sequence generation |
Allocation concealment |
Blinding of participants and personnel |
Blinding of outcome assessment |
Incomplete outcome data |
Selective reporting |
Other bias |
|---|---|---|---|---|---|---|---|---|
Lo [26] |
2000 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
Low risk |
De la Pena [27] |
2005 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
Low risk |
Jain [28] |
2006 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
Low risk |
Kumar [29] |
2009 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
High risk |
Lo (a) [30] |
2009 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
Low risk |
Lo (b) [31] |
2009 |
Low risk |
Low risk |
Unclear |
Low risk |
Low risk |
Low risk |
Low risk |
Garcia-Pagan [32] |
2009 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
Low risk |
Garcia-Pagan [35] |
2010 |
Low risk |
Low risk |
Unclear |
Unclear |
Low risk |
Low risk |
Low risk |
Luo [33] |
2015 |
Low risk |
Unclear |
Unclear |
Unclear |
Low risk |
Low risk |
Unclear |
Holster [34] |
2016 |
Low risk |
Low risk |
Unclear |
Low risk |
Low risk |
Low risk |
Unclear |
Overall mortality
When assessing the effect on overall mortality (as shown in Figure 2), combination therapy did not significantly differ from EVL alone in a fixed-effects model (RR=0.62, 95%CI: 0.36-1.08, I2=0.0%, P=0.592). Compared to pharmacotherapy alone, combination therapy also had no significant effect on overall mortality in a fixed-effects model (RR=1.05, 95%CI: 0.68-1.63, I2=0.0%, P=0.523). Similarly, combination therapy versus TIPS did not show a statistically significant difference in a random-effects model (RR=1.39, 95%CI: 0.92-2.09, I2=53.7%, P=0.115).
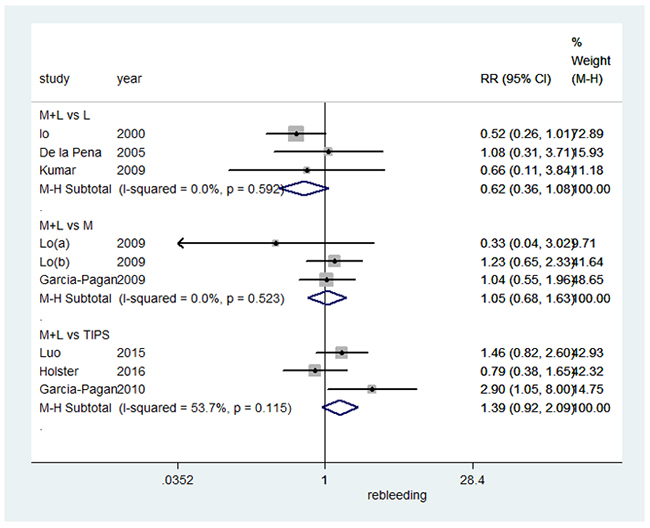
Figure 2: Forest plot of overall mortality.
Mortality caused by variceal bleeding
We also assessed the effect on mortality caused by variceal bleeding (summarized in Figure 3), and found that combination therapy did not significantly differ from EVL alone in a fixed-effects model (RR=0.43, 95%CI: 0.15-1.25, I2=0.0%, P=0.785). Compared to pharmacotherapy alone, combination therapy also had no significant effect on mortality caused by variceal bleedingin a fixed-effects model (RR=0.42, 95%CI: 0.17-1.06, I2=0.0%, P=0.542). However, TIPS resulted in a significant decrease in mortality caused by variceal bleeding when compared to combination therapy in a fixed-effects model (RR=5.66, 95%CI: 1.02-31.40, I2=0.0%, P=0.490).
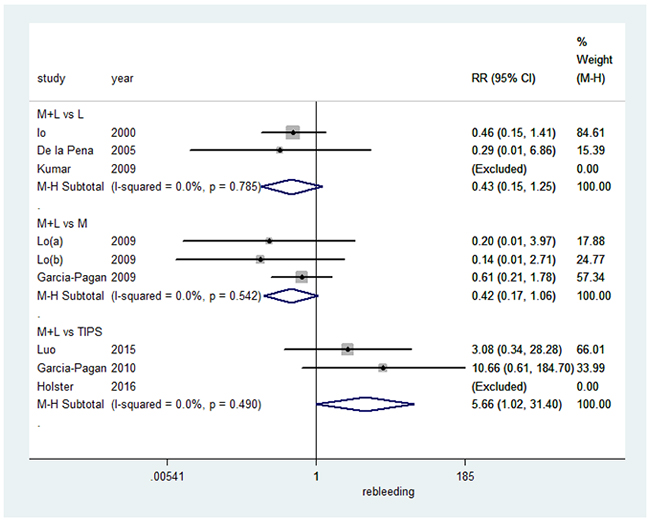
Figure 3: Forest plot of mortality caused by variceal bleeding.
Recurrence of bleeding
We next evaluated the effect on recurrence of bleeding (summarized in Figure 4). Combination therapy resulted in a significant decrease in the recurrence of bleeding (RR=0.57, 95%CI: 0.41-0.79, I2=0.0%, P=0.418), when compared to EVL alone in a fixed-effects model. In comparison to pharmacotherapy alone, combination therapy also significantly decreased the recurrence of bleeding in a random-effects model (RR=0.65, 95%CI: 0.48-0.88, I2=60.7%, P=0.079). However, TIPS significantly decreased bleeding recurrence when compared to combination therapy in a fixed-effects model (RR=9.42, 95%CI: 2.99-29.65, I2=0.0%, P=0.542).
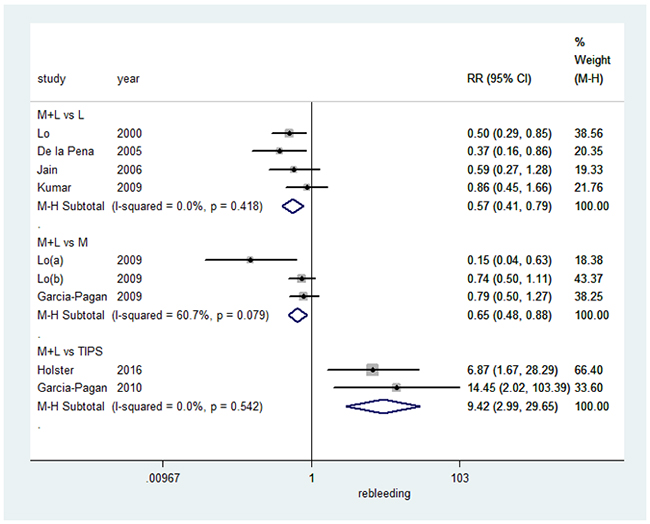
Figure 4: Forest plot of rebleeding.
Recurrence of bleeding from esophageal varices
Finally, we assessed the effect on recurrence of bleeding from esophageal varices (summarized in Figure 5). Combination therapy did not significantly differ from EVL alone in a random-effects model (RR=0.59, 95%CI: 0.33-1.06, I2=63.7%, P=0.064). Compared to pharmacotherapy alone, combination therapy resulted in a significant decrease in the recurrence of bleeding from esophageal varices in a fixed-effects model (RR=0.58, 95%CI: 0.40-0.85, I2=0.0%, P=0.760). However, TIPS significantly decreased esophageal bleeding recurrence in comparison to combination therapy in a random-effects model (RR=2.20, 95%CI: 1.22-3.99, I2=75.1%, P=0.045).
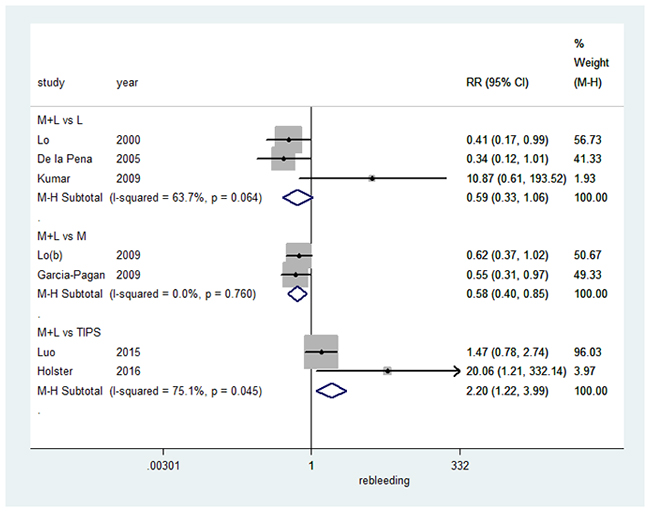
Figure 5: Forest plot of rebleeding from esophageal varices.
Publication bias
No publication bias was observed for any of the outcomes based on the symmetry of the funnel plots, as shown in Supplementary Figures 1–4. The results of the Egger’s test indicated no significant difference in any of the outcomes: overall mortality (Bias=0.514, 95%CI: -3.291-2.263, P=0.675), blood-related mortality (Bias=0.339, 95% CI: -2.393-3.072, P=0.763), recurrence of bleeding (Bias=1.280, 95%CI: -2.257-4.816, P=0.421), and recurrence of bleeding from esophageal varices (Bias=1.724, 95%CI: -1.785-5.233, P=0.262).
DISCUSSION
Despite the administration of vasoactive drugs [30, 31], ligation of varices often combined with drugs [14], or placement of a TIPS, there is still a 15% to 20% mortality rate within 30 days, and an increased risk of rebleeding (up to 25%) within six weeks [32, 33]. Currently in the clinic, most studies have revealed that EVL is an appropriate substitute for endoscopic sclerotheapy, as EVL achieves variceal obliteration quicker, thereby resulting in lower rebleeding rates [16, 34, 35]. The combination of pharmacotherapy and EVL could be more effective than monotherapy (pharmacotherapy and EVL alone). In addition, TIPS is a new therapeutic modality for variceal bleeding with recognized results [36, 37]. Accordingly, this study evaluated the clinical benefit of pharmacotherapy plus EVL compared with pharmacotherapy and EVL alone, and TIPS.
This meta-analysis evaluated the clinical benefit of combination therapy, pharmacotherapy and EVL, compared with that of pharmacotherapy and EVL alone. Combination therapy was found to be more effective than monotherapy (pharmacotherapy and EVL alone) at preventing rebleeding, which was consistent with other studies [15, 38, 39]. The rationale for combining drug therapy with EVL is that they act through different mechanisms; EVL reduces variceal size, and drug therapy lowers portal pressure [20]. However, when assessing rebleeding from esophageal varices, the benefit of combination therapy was only observed in comparison to pharmacotherapy alone, and not with EVL. This could be attributed to the number of patients and events in analysis of the two subgroups. There was no statistically significant difference between combination therapy and monotherapy in the all-course mortality rate or mortality caused by bleeding. Similar findings have been reported by Thiele et al., who suggested that the combination of EVL and medical therapy could reduce the risk of rebleeding, but not overall mortality [38]. Gonzalez et al. provided conflicting evidence, suggesting that combiantion therapy can reduce the risk of mortality [39]. This difference in findings could be attributed to the sample size.
We provide evidence that TIPS was superior to combination therapy in reducing the risk of rebleeding and rebleeding from varices, in our meta-analysis. This is consistent with previous studies where TIPS was found to be more effective in preventing recurrent esophageal variceal bleeding in patients [32, 33, 34]. TIPS involves establishing a direct pathway between the hepatic and portal veins to decompress portal venous hypertension, which is the source of the patient’s bleeding. Accordingly, TIPS is more than 90% effective in controlling bleeding from gastro-esophageal varices [11]. In our study, TIPS reduced mortality caused by bleeding, however, overall mortality was not significantly altered when compared to combination therapy. Holster et al. reported results consistent with this study [33], whereas a study by Garcia-Pagan et al. suggested a decrease in the risk of mortality with TIPS [29]. These contrasting results could be related to the patient follow-up or to the differing grades of cirrhosis inpatients. Sauer et al. demonstrated that TIPS did not improve survival rate associated with an increased risk of encephalopathy and high rates of shunt dysfunction [40]. There is an increase in the rate of development of hepatic encephalopathy after a TIPS procedure [13, 40, 41]. Conversely, other studies indicated that TIPS did not significantly increase the incidence of hepatic encephalopathy, compared other interventions [18, 27, 29, 37]. Although there is no consensus in these studies, TIPS is a widely accepted therapy as a result of extensive clinical validation in recent years. Based on Puente’s study [42], we found that confounding factors including the Child score (Child C >20% and Child C ≤20%) and follow-up time (<15 months and≥15 months) weren’t discovered to influence the results under in the case of the less number.
To our knowledge, TIPS insertion leads to important pathophysiologic circulatory changes; TIPS significantly reduces pressure in the extrahepatic portal venous system secondary to a dramatic drop in intrahepatic vascular resistance to portal flow; therefore, TIPS is potentially useful for patients with portal hypertension [43]. TIPS prevents rebleeding more effectively than drug treatment or endoscopic procedures alone, but it can cause encephalopathy and has no overall survival benefit [44]. Moreover, high-risk patients (those with advanced cirrhosis) experience less rebleeding and have an increased survival rate if TIPS is placed within five days of variceal bleeding [29, 44]. In this meta-analysis, we compare TIPS with combination therapy and show a significant reduction in mortality from variceal bleeding, although there was no overall improvement in survival when TIPS was used, which may be related to hepatic encephalopathy.
An advantage of this meta-analysis is that all included studies were randomized, controlled clinical trials and with large sample sizes [21], however, some limitations in our study should be addressed. Firstly, few clinical trials met the inclusion criteria, therefore, more clinical studies are required to confirm our results. Secondly, the double-blind methods of methodological quality of eligible trials could not be performed, due to the specificity of EVL and TIPS. In addition, heterogeneity of drug dose may also be a concern in our meta-analysis. Finally, the complications associated with TIPS, such as hepatic encephalopathy, are unclear in our study, which may exert influence on mortality.
MATERIALS AND METHODS
Literature search strategy
This systematic review and meta-analysis was reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [45] and conducted in accordance with the Cochrane Collaboration’s systematic review framework [46]. We used the PubMed, EMBASE, and Cochrane Central databases to perform a literature search on articles published up until November 2016, using the following MeSH words and key terms: “esophageal varices”, “variceal rebleeding”, “variceal hemorrhage”, “portal hypertension”, “liver cirrhosis”, “pharmacotherapy”, “endoscopic variceal ligation”, and “transjugular intrahepatic portosystemicshunt”. We also searched the reference lists of the retrieved studies.
Literature selection and exclusion
The inclusion criteria for selection of clinical trials in to the meta-analysis were as follows: (1) randomized, controlled trials comparing pharmacotherapy plus EVL with EVL or pharmacotherapy alone, or TIPS; (2) study participants should be older than 16 years of age with at least one previous episode of esophageal bleeding; and (3) studies needed to have measured at least one of the following outcomes as their endpoints: overall mortality, mortality caused by variceal bleeding, recurrence of bleeding, or recurrence of bleeding from esophageal varices.
Studies comparing these outcomes in the primary prevention of gastroesophageal bleeding, those that included patients with gastric varices alone, or liver cancer, were excluded from our analysis. If that the study was a duplicate or study’s data could not be extracted or obtained through contact with the author, were excluded.
Data extraction
Data was extracted directly from the selected studies by two independent reviewers. In the case of disagreement, a third reviewer was consulted. The relevant information included study design, patient characteristics, interventions, controls, and four outcomes: overall mortality, mortality caused by variceal bleeding, recurrence of bleeding, and recurrence of bleeding from esophageal varices.
Quality assessment of included studies
Two investigators independently evaluated the methodological quality of eligible trials using the Cochrane collaboration tool for assessing risk of bias [47] (random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other sources of bias).
Statistical analysis
This meta-analysis was performed using Stata 12.0. Dichotomous outcomes were expressed as relative risk (RR) with a 95% confidence interval (CI) [46, 48]. Heterogeneity between studies was also analyzed using chi-square tests, with the significance level set to P <0.1 [49]. No heterogeneity is observed when I2 =0%. However, when I2 >50%, studies were considered to have significant heterogeneity and a random-effects model was used to conduct the meta-analysis, whereas when I2 <50%, a fixed-effects model was used instead [46].
The symmetry of a funnel plot was used to qualitatively determine whether there was publication bias [50]. In the funnel plot, larger studies that provide a more precise estimate of an interventions effect from the spout of the funnel, whereas smaller studies with less precision form the cone end of the funnel. Asymmetry in the funnel plot indicates potential publication bias, which is assessed by the Egger’s test for a quantitative detection of bias [51].
Ethical approval
Not required.
CONCLUSIONS
This meta-analysis indicated that a combined therapy of pharmacotherapy plus EVL was more effective in decreasing rebleeding than monotherapy. Furthermore, TIPS was superior to combined therapy in decreasing the risk of rebleeding, rebleeding from varices, and mortality caused by bleeding, although not overall mortality. Accordingly, we recommend TIPS for the prevention of variceal rebleeding in patients with cirrhosis.
Abbreviations
EVB, esophageal varices bleeding; EVL, endoscopic variceal ligation; TIPS, transjugular intrahepatic portosystemic shunt; ISMN, isosorbide mononitrate; RCT, randomized controlled trials; RR, relative risk; CI, confidence interval.
Author contributions
JL and CZ had full access to all of the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis. SMD, HYG and LW designed the study. ZYJ, LLL and YF developed and tested the data collection forms. CZ and XFS acquired the data. SMD and LW conducted the analysis and interpreted the data. JL and CZ drafted the manuscript. All authors critically revised the manuscript. JL and CZ had guarantor.
CONFLICTS OF INTEREST
All authors report there are no conflicts of interest related to the present article.
FUNDING
This study was supported by the Health Department of Hubei Province (No. QJX2012-44). The funders had no roles in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
REFERENCES
1. D’Amico G. Esophageal Varices: From Appearance to Rupture; Natural History and Prognostic Indicators. In: Portal Hypertension in the 21st Century. Groszmann RJ, Bosch J, Editors. Dordretch, the Netherlands: Kluwer Academic. 2004:147-154.
2. D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment of portal hypertension: an evidence-based approach. Semin Liver Dis. 1999; 19:475-505.
3. Bosch J, Garcia-Pagan JC. Prevention of variceal rebleeding. Lancet. 2003; 361:952-954.
4. Pagliaro L, Lebrec D, Poynard T, Hillon P, Benhamou JP. Propranolol for prevention of recurrent gastrointestinal bleeding in patients with cirrhosis. A controlled study. J Hepatol. 2002; 36:148-150.
5. Villanueva C, Balanzo J, Novella MT, Soriano G, Sainz S, Torras X, Cusso X, Guarner C, Vilardell F. Nadolol plus isosorbide mononitrate compared with sclerotherapy for the prevention of variceal rebleeding. N Engl J Med. 1996; 334:1624-1629.
6. Laine L, Cook D. Endoscopic ligation compared with sclerotherapy for treatment of esophageal variceal bleeding. A meta-analysis. Ann Intern Med. 1995; 123:280-287.
7. Stiegmann GV, Goff JS, Michaletz-Onody PA, Korula J, Lieberman D, Saeed ZA, Reveille RM, Sun JH, Lowenstein SR. Endoscopic sclerotherapy as compared with endoscopic ligation for bleeding esophageal varices. N Engl J Med. 1992; 326:1527-1532.
8. Gimson AE, Ramage JK, Panos MZ, Hayllar K, Harrison PM, Williams R, Westaby D. Randomised trial of variceal banding ligation versus injection sclerotherapy for bleeding oesophageal varices. Lancet. 1993; 342:391-394.
9. Laine L, el-Newihi HM, Migikovsky B, Sloane R, Garcia F. Endoscopic ligation compared with sclerotherapy for the treatment of bleeding esophageal varices. Ann Intern Med. 1993; 119:1-7.
10. Sarin SK, Govil A, Jain AK, Guptan RC, Issar SK, Jain M, Murthy NS. Prospective randomized trial of endoscopic sclerotherapy versus variceal band ligation for esophageal varices: influence on gastropathy, gastric varices and variceal recurrence. J Hepatol. 1997; 26:826-832.
11. Loffroy R, Favelier S, Pottecher P, Estivalet L, Genson PY, Gehin S, Krause D, Cercueil JP. Transjugular intrahepatic portosystemic shunt for acute variceal gastrointestinal bleeding: indications, techniques and outcomes. Diagn Interv Imaging. 2015; 96:745-755.
12. LaBerge JM, Ring EJ, Gordon RL, Lake JR, Doherty MM, Somberg KA, Roberts JP, Ascher NL. Creation of transjugular intrahepatic portosystemic shunts with the wallstent endoprosthesis: results in 100 patients. Radiology. 1993; 187:413-420.
13. Rossle M, Haag K, Ochs A, Sellinger M, Noldge G, Perarnau JM, Berger E, Blum U, Gabelmann A, Hauenstein K, Langer M, Gerok W. The transjugular intrahepatic portosystemic stent-shunt procedure for variceal bleeding. N Engl J Med. 1994; 330:165-171.
14. Sarin SK, Wadhawan M, Gupta R, Shahi H. Evaluation of endoscopic variceal ligation (EVL) versus propanolol plus isosorbide mononitrate/nadolol (ISMN) in the prevention of variceal rebleeding: comparison of cirrhotic and noncirrhotic patients. Dig Dis Sci. 2005; 50:1538-1547.
15. Ravipati M, Katragadda S, Swaminathan PD, Molnar J, Zarling E. Pharmacotherapy plus endoscopic intervention is more effective than pharmacotherapy or endoscopy alone in the secondary prevention of esophageal variceal bleeding: a meta-analysis of randomized, controlled trials. Gastrointest Endosc. 2009; 70:658-664.e5.
16. Shi KQ, Liu WY, Pan ZZ, Ling XF, Chen SL, Chen YP, Fan YC, Zheng MH. Secondary prophylaxis of variceal bleeding for cirrhotic patients: a multiple-treatments meta-analysis. Eur J Clin Invest. 2013; 43:844-854.
17. Jalan R, Forrest EH, Stanley AJ, Redhead DN, Forbes J, Dillon JF, MacGilchrist AJ, Finlayson ND, Hayes PC. A randomized trial comparing transjugular intrahepatic portosystemic stent-shunt with variceal band ligation in the prevention of rebleeding from esophageal varices. Hepatology. 1997; 26:1115-1122.
18. Pomier-Layrargues G, Villeneuve JP, Deschenes M, Bui B, Perreault P, Fenyves D, Willems B, Marleau D, Bilodeau M, Lafortune M, Dufresne MP. Transjugular intrahepatic portosystemic shunt (TIPS) versus endoscopic variceal ligation in the prevention of variceal rebleeding in patients with cirrhosis: a randomised trial. Gut. 2001; 48:390-396.
19. Sauerbruch T, Mengel M, Dollinger M, Zipprich A, Rossle M, Panther E, Wiest R, Caca K, Hoffmeister A, Lutz H, Schoo R, Lorenzen H, Trebicka J, et al. Prevention of rebleeding from esophageal varices in patients with cirrhosis receiving small-diameter stents versus hemodynamically controlled medical therapy. Gastroenterology. 2015; 149:660-668.e1.
20. Lo GH, Lai KH, Cheng JS, Chen MH, Huang HC, Hsu PI, Lin CK. Endoscopic variceal ligation plus nadolol and sucralfate compared with ligation alone for the prevention of variceal rebleeding: a prospective, randomized trial. Hepatology. 2000; 32:461-465.
21. de la Pena J, Brullet E, Sanchez-Hernandez E, Rivero M, Vergara M, Martin-Lorente JL, Garcia Suarez C. Variceal ligation plus nadolol compared with ligation for prophylaxis of variceal rebleeding: a multicenter trial. Hepatology. 2005; 41:572-578.
22. Jain A, Kumar A, Tyagi P, Sharma BC, Sarin SK. Endoscopic Variceal Ligation (EVL) Plus Propranolol (P) and Isosorbide Mononitrate (ISMN) Versus Endoscopic Variceal Ligation Alone in Secondary Prophylaxis of Variceal Bleeding: A Prospective Randomized Controlled Trial. Am J Gastroenterol. 2006; 101:S179.
23. Kumar A, Jha SK, Sharma P, Dubey S, Tyagi P, Sharma BC, Sarin SK. Addition of propranolol and isosorbide mononitrate to endoscopic variceal ligation does not reduce variceal rebleeding incidence. Gastroenterology. 2009; 137:892-901, 901.e1.
24. Lo GH, Chen WC, Chan HH, Tsai WL, Hsu PI, Lin CK, Chen TA, Lai KH. A randomized, controlled trial of banding ligation plus drug therapy versus drug therapy alone in the prevention of esophageal variceal rebleeding. J Gastroenterol Hepatol. 2009; 24:982-987.
25. Lo GH, Chen WC, Wang HM, Lin CK, Chan HH, Tsai WL, Cheng LC, Yu HC, Tsay FW. Low-dose terlipressin plus banding ligation versus low-dose terlipressin alone in the prevention of very early rebleeding of oesophageal varices. Gut. 2009; 58:1275-1280.
26. Garcia-Pagan JC, Villanueva C, Albillos A, Banares R, Morillas R, Abraldes JG, Bosch J. Nadolol plus isosorbide mononitrate alone or associated with band ligation in the prevention of recurrent bleeding: a multicentre randomised controlled trial. Gut. 2009; 58:1144-1150.
27. Luo X, Wang Z, Tsauo J, Zhou B, Zhang H, Li X. Advanced cirrhosis combined with portal vein thrombosis: a randomized trial of TIPS versus endoscopic band ligation plus propranolol for the prevention of recurrent esophageal variceal bleeding. Radiology. 2015; 276:286-293.
28. Holster IL, Tjwa ET, Moelker A, Wils A, Hansen BE, Vermeijden JR, Scholten P, van Hoek B, Nicolai JJ, Kuipers EJ, Pattynama PM, van Buuren HR. Covered transjugular intrahepatic portosystemic shunt versus endoscopic therapy + beta-blocker for prevention of variceal rebleeding. Hepatology. 2016; 63:581-589.
29. Garcia-Pagan JC, Bosch J. ACP Journal Club. Early use of TIPS in patients with cirrhosis and variceal bleeding. Ann Intern Med. 2010; 153:JC5-13; author reply JC15-13.
30. Bernard B, Lebrec D, Mathurin P, Opolon P, Poynard T. Beta-adrenergic antagonists in the prevention of gastrointestinal rebleeding in patients with cirrhosis: a meta-analysis. Hepatology. 1997; 25:63-70.
31. Lo GH, Chen WC, Lin CK, Tsai WL, Chan HH, Chen TA, Yu HC, Hsu PI, Lai KH. Improved survival in patients receiving medical therapy as compared with banding ligation for the prevention of esophageal variceal rebleeding. Hepatology. 2008; 48:580-587.
32. Krige JE, Kotze UK, Distiller G, Shaw JM, Bornman PC. Predictive factors for rebleeding and death in alcoholic cirrhotic patients with acute variceal bleeding: a multivariate analysis. World J Surg. 2009; 33:2127-2135.
33. D’Amico G, De Franchis R. Upper digestive bleeding in cirrhosis. Post-therapeutic outcome and prognostic indicators. Hepatology. 2003; 38:599-612.
34. Singh P, Pooran N, Indaram A, Bank S. Combined ligation and sclerotherapy versus ligation alone for secondary prophylaxis of esophageal variceal bleeding: a meta-analysis. Am J Gastroenterol. 2002; 97:623-629.
35. Karsan HA, Morton SC, Shekelle PG, Spiegel BM, Suttorp MJ, Edelstein MA, Gralnek IM. Combination endoscopic band ligation and sclerotherapy compared with endoscopic band ligation alone for the secondary prophylaxis of esophageal variceal hemorrhage: a meta-analysis. Dig Dis Sci. 2005; 50:399-406.
36. Meddi P, Merli M, Lionetti R, De Santis A, Valeriano V, Masini A, Rossi P, Salvatori F, Salerno F, de Franchis R, Capocaccia L, Riggio O. Cost analysis for the prevention of variceal rebleeding: a comparison between transjugular intrahepatic portosystemic shunt and endoscopic sclerotherapy in a selected group of Italian cirrhotic patients. Hepatology. 1999; 29:1074-1077.
37. Halabi SA, Sawas T, Sadat B, Jandali A, Halabi HA, Halabi FA, Kapoor B, Carey WD. Early TIPS versus endoscopic therapy for secondary prophylaxis after management of acute esophageal variceal bleeding in cirrhotic patients: a meta-analysis of randomized controlled trials. J Gastroenterol Hepatol. 2016; 31:1519-1526.
38. Thiele M, Krag A, Rohde U, Gluud LL. Meta-analysis: banding ligation and medical interventions for the prevention of rebleeding from oesophageal varices. Aliment Pharmacol Ther. 2012; 35:1155-1165.
39. Gonzalez R, Zamora J, Gomez-Camarero J, Molinero LM, Banares R, Albillos A. Meta-analysis: combination endoscopic and drug therapy to prevent variceal rebleeding in cirrhosis. Ann Intern Med. 2008; 149:109-122.
40. Sauer P, Theilmann L, Stremmel W, Benz C, Richter GM, Stiehl A. Transjugular intrahepatic portosystemic stent shunt versus sclerotherapy plus propranolol for variceal rebleeding. Gastroenterology. 1997; 113:1623-1631.
41. Burroughs AK, Vangeli M. Transjugular intrahepatic portosystemic shunt versus endoscopic therapy: randomized trials for secondary prophylaxis of variceal bleeding: an updated meta-analysis. Scand J Gastroenterol. 2002; 37:249-252.
42. Puente A, Hernandez-Gea V, Graupera I, Roque M, Colomo A, Poca M, Aracil C, Gich I, Guarner C, Villanueva C. Drugs plus ligation to prevent rebleeding in cirrhosis: an updated systematic review. Liver Int. 2014; 34:823-833.
43. Colombato L. The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension. J Clin Gastroenterol. 2007; 41:S344-351.
44. Parker R. Role of transjugular intrahepatic portosystemic shunt in the management of portal hypertension. Clin Liver Dis. 2014; 18:319-334.
45. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009; 339:b2535.
46. Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions, v.5.1. handbook.cochrane.org/. [Last updated on 2011 Mar 05]. 2011.
47. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011; 343:d5928.
48. Deeks J. Issues in the selection of a summary statistic for meta-analysis of clinical trials with binary outcomes. Stat Med. 2002; 21:1575-1600.
49. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21:1539-1558.
50. Copas J, Shi JQ. Meta-analysis, funnel plots and sensitivity analysis. Biostatistics. 2000; 1:247-262.
51. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629-634.