
INTRODUCTION
Breast cancer is the most common cancer type and the second leading cause of cancer death in women worldwide and is expected to account for 29% all new cancer diagnoses for female [1]. Besides, breast cancer is a heterogeneous disease that comprises a variety of pathologies and displays a range of histological characteristics and clinical outcomes [2]. Nowadays, the focus of treatment strategies is using chemotherapy to induce cancer cell apoptosis, resistance to hormone therapy and targeted therapy. However, the prognosis of breast cancer patients remains unsatisfactory [3]. Biomarkers play an essential role in the management of patients with invasive breast cancer and may be used to predict outcome and aid adjunct therapy decision-making.
The tyrosine kinase c-Met, also called MET and hepatocyte growth factor receptor (HGFR), is a key regulator of organ development and cancer progression and has been studied in many cancer types such as lung cancer, gastric cancer, prostate cancer and so on [4–7]. c-Met inhibitors also have been tested in many cancers and shown promising results in lung cancer, ovarian cancer and so on [5, 8]. In breast cancer, previous studies have yielded mixed results. Some studies showed favorable association, some reported no significance, while some others reported a negative prognostic effect between c-Met overexpression and prognosis [9–11]. And two previously published meta-analysis with small samples yielded conflicting results of OS for breast cancer patients [12, 13]. Therefore, more systematic studies are needed to acquire high quality evidence-based results of the prognostic value of c-Met to identify patients who would benefit from c-Met targeted therapy and guide future clinical trial.
RESULTS
Description of included studies
507 records were identified in total and then 70 candidate studies were selected. Through further screening, 33 studies were excluded because of in vitro experiment and reviews. Among the remaining studies, three studies were performed in the same institution and only the most recent study was included. Finally, 32 studies were included and the detailed literature search and study selection could be seen in Figure 1.
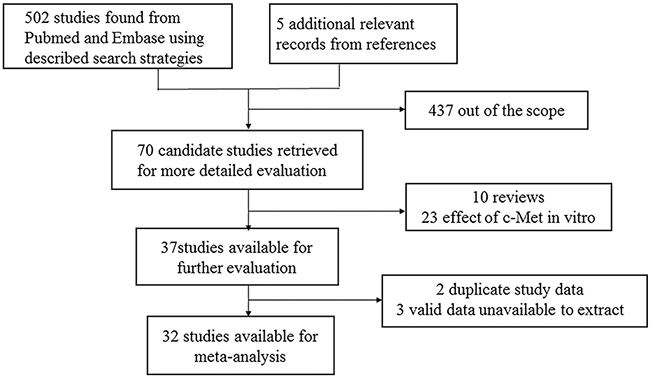
Figure 1: Selection of studies. Flow chart showed selection of the studies in the meta-analysis.
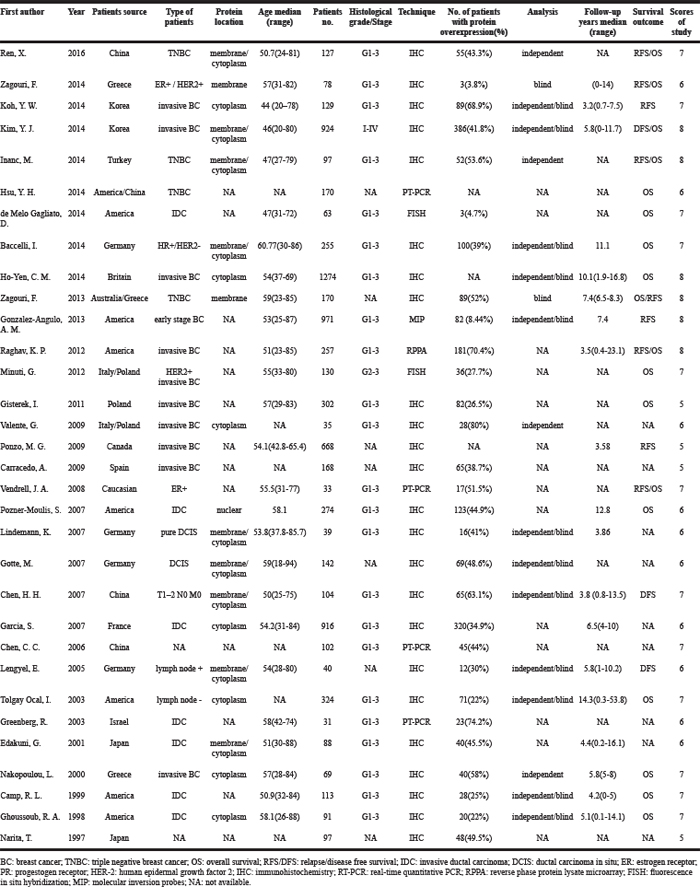
There were 32 studies with 8281 patients in total involved in our meta-analysis. Thereinto, 18 studies with 4751 patients were available for OS survival data and 12 studies with 3598 patients were available for RFS/DFS survival data. There were 24 (75%) articles using immunohistochemistry method to determine the overexpression of c-Met and 8 (25%) articles using RT-PCR, FISH, RPPA and MIP respectively. All the articles included were retrospective. The study quality was assessed using the Newcastle-Ottawa quality assessment scale, generating scores ranging from 5 to 8 with a mean of 6.625 (Table 1).
Table 1: Characteristics of included studies
Data synthesis: clinicopathological features
Our results showed that c-Met overexpression was significantly correlated to large tumor size, OR=1.785 (1.480, 2.153); high histologic grade, OR=1.547 (1.108, 2.158) and distant metastasis, OR=20.431 (1.869, 223.360). However, high c-Met overexpression was not found to be associated with Menopausal status, OR=0.758 (0.529, 1.086); age, OR=1.072 (0.699, 1.645); ER status, OR=1.049 (0.679, 1.619); PR status, OR=1.300 (0.782, 2.161); HER-2 status, OR =1.017 (0.683, 1.516); triple negative breast cancer, OR=0.956 (0.443, 2.063); ki-67 overexpression, OR=1.677 (0.837, 3.362); lymph node status, OR=1.801 (0.991, 3.274); histologic type, OR=1.053 (0.566, 1.960). All the above results could be seen in Table 2.
Table 2: Meta-analysis for the association of c-Met overexpression and clinicopathological features of breast cancer patients
Clinicopathological features |
No.of studies |
No.of patients |
Model |
OR(95% CI) |
P-value |
Heterogeneity |
||
|---|---|---|---|---|---|---|---|---|
I2 |
I2(%) |
P-Value |
||||||
Menopausal status (post vs. pre) |
3 |
1210 |
Fixed |
0.76(0.53,1.09) |
0.13 |
1.51 |
0 |
0.47 |
Age(≤50 vs. >50) |
4 |
1438 |
Random |
1.07(0.70,1.65) |
0.75 |
7.6 |
60.5 |
0.06 |
Size(>2cm vs. ≤2cm) |
9 |
2579 |
Fixed |
1.79(1.48,2.15) |
0 |
7.39 |
0 |
0.5 |
ER status(Negative vs. Positive) |
11 |
2718 |
Random |
1.05(0.68,1.62) |
0.83 |
34.62 |
71.1 |
0 |
PR status(Negative vs. Positive) |
9 |
2533 |
Random |
1.30(0.78,2.16) |
0.31 |
29.02 |
72.4 |
0 |
HER-2(Negative vs. Positive) |
7 |
2402 |
Random |
1.02(0.68,1.52) |
0.93 |
13.38 |
55.1 |
0.04 |
TNBC(yes vs. no) |
4 |
2281 |
Random |
0.96(0.44,2.06) |
0.91 |
25.33 |
88.2 |
0 |
Ki67(≥10% vs. <10%) |
3 |
386 |
Fixed |
1.68(0.84,3.36) |
0.15 |
0.66 |
0 |
0.72 |
Histologic grade(G3 vs.G1-2) |
14 |
2418 |
Random |
1.55(1.11,2.16) |
0.01 |
25.08 |
48.2 |
0.02 |
lymph node status(N1-3 vs.N0) |
11 |
2743 |
Random |
1.80(1.00,3.27) |
0.05 |
74.89 |
86.6 |
0 |
Metastasis (yes vs. no) |
3 |
947 |
Random |
33.60(1.64,689.51) |
0.02 |
48.66 |
95.9 |
0 |
Histologic type(IDC vs. ILC) |
9 |
2633 |
Random |
1.05(0.57,1.96) |
0.87 |
15.1 |
47 |
0.06 |
ER: estrogen receptor; PR: progesterone receptor; HER-2: human epidermal growth factor receptor-2; IDC: infiltrating ductal carcinoma; ILC: infiltrating lobular carcinoma.
Data synthesis: overall survival
OS was analyzed in 18 studies with 4751 patients. Results showed that c-Met overexpression was related to poor OS, HR=1.65 (1.328, 2.051) (Figure 2A). Besides, results of subgroup analysis according to data sources (Figure 2B)/methods (Figure 2C)/ethnicity (Figure 2D) showed that c-Met overexpression was related to poor OS in Given by author, all methods and all ethnicity groups respectively (Table 3).
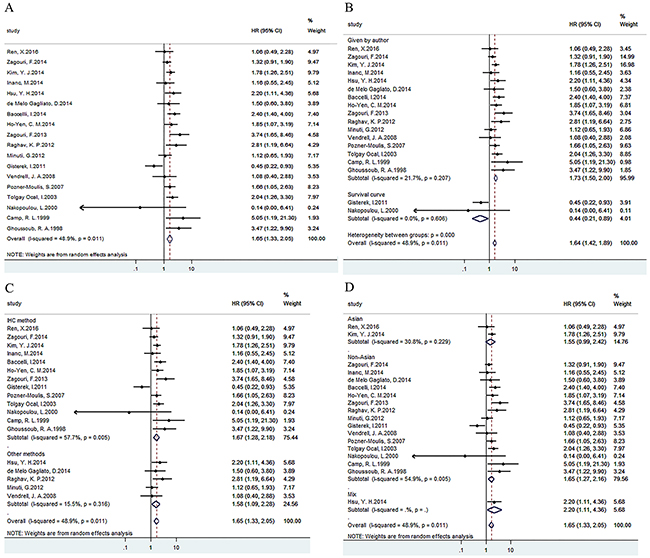
Figure 2: Forest plots of HRs for the association of c-Met overexpression and OS. Survival data were reported as OS (A), as well as subgroup analysis of data sources (B), methods (C) and ethnicity (D) among included studies.
Table 3: Main meta-analysis results
Analysis |
No.of studies |
No.of patients |
Model |
HR(95% CI) |
P-value |
Heterogeneity |
|||
|---|---|---|---|---|---|---|---|---|---|
I2 |
I2(%) |
P-Value |
|||||||
OS |
18 |
4751 |
Random |
1.65(1.33,2.05) |
0 |
33.24 |
48.9 |
0.011 |
|
Data source |
Given by author |
16 |
4380 |
Fixed |
1.75(1.48,2.08) |
0 |
19.15 |
21.7 |
0.207 |
Survival curve |
2 |
371 |
Fixed |
0.44(0.21,0.89) |
0.022 |
0.27 |
0 |
0.606 |
|
Technique |
IHC method |
13 |
4098 |
Random |
1.67(1.28,2.18) |
0 |
28.4 |
57.7 |
0.005 |
Other methods |
5 |
653 |
Fixed |
1.56(1.12,2.17) |
0.009 |
4.74 |
15.5 |
0.316 |
|
Ethnicity |
Asian |
2 |
1051 |
Fixed |
1.63(1.19,2.23) |
0.002 |
1.45 |
30.8 |
0.229 |
Non-Asian |
15 |
3530 |
Random |
1.65(1.27,2.16) |
0 |
31.04 |
54.9 |
0.005 |
|
Mix |
1 |
170 |
- |
2.20(1.11,4.36) |
0.024 |
0 |
- |
- |
|
RFS/DFS |
12 |
3598 |
Random |
1.53(1.20,1.95) |
0.001 |
26.77 |
58.9 |
0.005 |
|
Data source |
Given by author |
11 |
2930 |
Random |
1.56(1.19,2.04) |
0.001 |
26.69 |
62.5 |
0.003 |
Survival curve |
1 |
668 |
- |
1.35(0.87,2.10) |
0.182 |
0 |
- |
- |
|
Technique |
IHC method |
9 |
2337 |
Random |
1.51(1.11,2.06) |
0.008 |
25.32 |
68.4 |
0.001 |
Other methods |
3 |
1261 |
Fixed |
1.63(1.17,2.28) |
0.004 |
0.73 |
0 |
0.693 |
|
Ethnicity |
Asian |
4 |
1284 |
Random |
1.18(0.64,2.17) |
0.59 |
14.44 |
79.2 |
0.002 |
Non-Asian |
8 |
2314 |
Fixed |
1.58(1.33,1.87) |
0 |
8.62 |
18.8 |
0.281 |
|
Data synthesis: disease/relapse free survival
Analysis of 12 studies with 3598 patients indicated overexpression of c-Met was related to poor RFS/DFS, HR=1.53(1.20, 1.95) (Figure 3A). Besides, results of subgroup analysis according to data sources (Figure 3B)/methods (Figure 3C)/ethnicity (Figure 3D) showed that c-Met overexpression was related to poor RFS/DFS in Given by author, all methods and non-Asian groups respectively (Table 3).
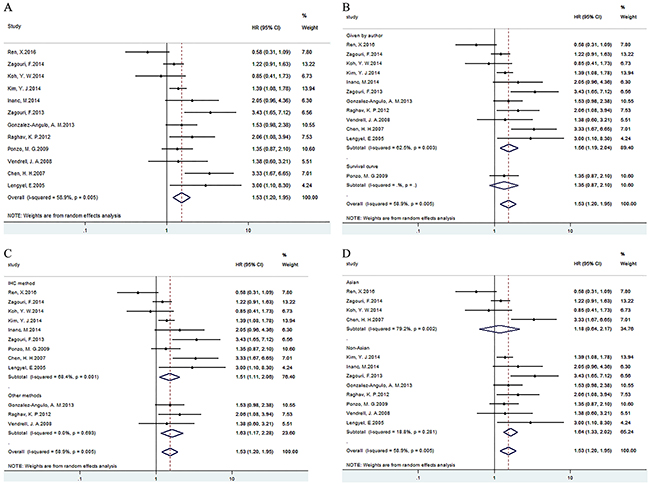
Figure 3: Forest plots of HRs for the association of c-Met overexpression and RFS/DFS. Survival data were reported as OS (A), as well as subgroup analysis of data sources (B), methods (C) and ethnicity (D) among included studies.
Publication bias
Funnel plot and Egger’/Begg’ test was used to evaluate publication bias. Results of Egger’/Begg’ test for OS and RFS/DFS were 0.945/0.520 and 0.270/0.131 respectively. Begg’s funnel plots with pseudo 95% confidence limits of the OS and RFS/DFS were listed in Figure 4A and 4B.
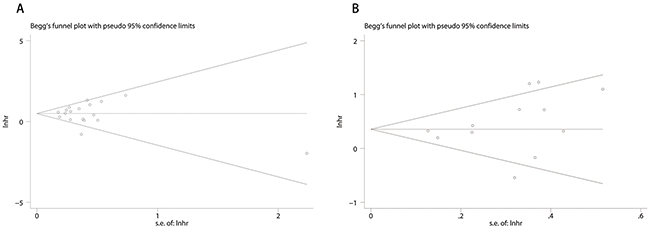
Figure 4: Funnel plots of publication bias of OS and RFS/DFS. Publication bias of OS (A) and RFS/DFS (B) of the meta-analysis showed no statistical signifcance (p > 0.05) using Begg’s test.
Sensitivity analysis
Results of removal of each study at a time could be seen in Figure 5A and 5B. Removal of each study didn’t change HR significantly both for the OS and RFS/DFS analysis.
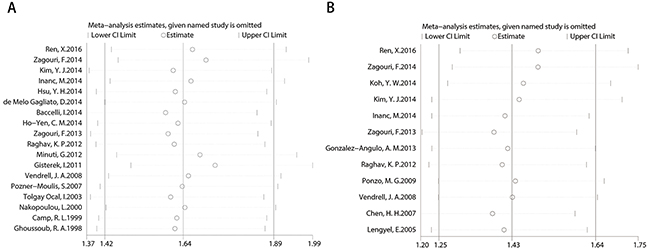
Figure 5: Sensitivity for included studies. The effect of single study was evaluated on the whole results of OS (A) and RFS/DFS (B) in this meta-analysis.
DISCUSSION
The tyrosine kinase c-Met fosters invasive growth, a complex physiological program that signifies concerted activation of cell proliferation, survival, invasion and angiogenesis [4, 14]. In the past years, mountains of clinical studies have described c-Met overexpression and pathway hyperactivation in tissues of breast cancer patients, and found a strong relationship between high HGF/Met signaling and tumor progression [15, 16]. Our results demonstrated that c-Met overexpression was related to poor OS and RFS/DFS for breast cancer patients. Moreover, c-Met overexpression was associated with large tumor size, high histologic grade and distant metastasis. Therefore, c-Met could be a potential target for breast cancer therapy.
In our meta-analysis, the results of OS showed moderate heterogeneity. Then we conducted subgroup analysis and found that data sources were the origin of heterogeneity. The HR value extracted from survival curve of 2 articles showed a favorable prognosis of c-Met overexpression while other 16 articles with HR value given by author indicated a poor prognosis. The difference is mainly because data extracted from survival curve is not as accurate as that given by author and the article quality is relatively low. Subgroup analysis of RFS/DFS was also conducted on the basis of data source. Only one study with HR value derived from survival curve and both the two subgroups showed poor prognosis of c-Met overexpression. And subgroup analysis of methods reached in same conclusion. Subgroup analysis of ethnicity showed c-Met overexpression in non-Asian group rather than Asian group had statistical difference, which might because the significant heterogeneity in Asian group. What’s more, no evidence indicated publication bias for OS and RFS/DFS in regard to c-Met overexpression using Egger’/Begg’ test. And influence analysis of OS and RFS/DFS showed no big difference. All that demonstrated that our results were stable and reliable.
Some studies have investigated the role of c-Met in TNBC and BLBC (basal like breast cancer) and found that c-Met was related to TNBC and BLBC phenotype, which could be exploited as a potential target [2, 9, 17, 18]. Our results showed that c-Met overexpression was independent of hormone receptor status and there was no statistical significance of c-Met overexpression between TNBC and non-TNBC group, which indicated that c-Met could be a target for breast cancer regardless of hormone status. But because of the limited studies, further research is needed to validate the relationship of c-Met overexpression and TNBC/BLBC phenotype.
This study has important implications in breast cancer. Firstly, it demonstrates c-Met overexpression is related to worse OS and RFS/DFS, which indicates that c-Met may be a potential therapeutic target. Secondly, c-Met is involved in malignant biological behavior, such as large tumor size, high histological grade and distant metastasis, and combination therapy with c-Met inhibitor in future will dramatically reduce mortality in invasive breast cancer. However, there are also limitations in this meta-analysis. First of all, identifications of c-Met overexpression of individual studies are not exactly same and as a dichotomous variable, cut-off value may be a source of considerable interstudy heterogeneity. Additionally, although Begg’s and Egger’s test were performed and there was no statistical significance. Results should be interpreted cautiously because we only include studies with available HR value or K-M survival curves with necessary data.
Currently, the most promising approach for disrupting c-Met signaling is to use small molecular inhibitors to target the intracellular kinase domain [19]. The clinical relevance of c-Met inhibitors is now under investigation, phase II and III clinical trials in a variety of malignancies including non-small cell lung cancer [20–22], colorectal cancer [23], gastroesophageal cancer [24] are ongoing. With regard to breast cancer, a phase II trial examining tivantinib in patients with recurrent or metastatic TNBC [25] and a randomized phase II study evaluating the safety and efficacy of onartuzumab and/or bevacizumab in combination with paclitaxel in patients with metastatic TNBC are currently ongoing [26].
Taken together, our analysis shows that overexpression of c-Met in breast cancer tissues is associated with worse prognosis in human breast cancer. Since c-Met inhibitor has already been investigated in numerous clinical trials, the future clinical application will be easier. Combination therapy of c-Met inhibitor will improve the prognosis of breast cancer patients especially invasive breast cancer and TNBC/BLBC, which are types of the poorest prognosis.
MATERIALS AND METHODS
Literature search
This meta-analysis was conducted according to PRISMA guidelines. Studies were identified by searching PubMed and EMBASE databases from 1997 until April, 2016 by using the key words “breast cancer or breast tumor or breast carcinoma” and “hepatocyte growth factor receptor or HGFR or c-Met”. Titles and abstracts were first scanned to exclude irrelevant articles and final inclusion of the articles was determined by reading the full text. The references from identified articles were manually searched for additional relevant records.
Inclusion and exclusion
All studies in this meta-analysis satisfied the following inclusion criteria: 1) full-text studies published in English; 2) proven diagnosis of breast cancer by pathology; 3) considering the relation between c-Met overexpression and OS, RFS/DFS or clinicopathological features among breast cancer patients; 4) provided the HRs and 95% CIs, or Kaplan-Meier survival curves that provided sufficient data to extract HRs and 95% CIs. Exclusion criteria: 1) no data on survival or clinicopathological features and inability to calculate from Kaplan-Meier survival curve; 2) with previous cancer history.
Data extraction
Two reviewers (Zhao XX and Qu JK) performed the search and assessed the studies independently. The following items were extracted from each eligible study, including first author, year, patients source, type of patients, protein location, median age, patients number, technique, c-Met overexpression (%), analysis, median follow up, OS/DFS and clinicopathological features. When the univariate and multivariate analysis were both available, the multivariate results were used. If the above-mentioned data was not reported, items should be treated as “NA (not available)”.
Quality of the studies
The Newcastle-Ottawa Scale was used to assess the quality of each study [27]. The NOS criteria is scored based on three aspects: (1) subject selection, (2) comparability of subject, (3) outcome measurement. NOS scores range from 0 to 9, and a score ≥ 6 indicates a high quality. Two investigators independently assessed the quality of the 32 included studies, and the discrepancies were solved by consensus.
Statistical analysis
HRs and 95% CIs were used to study the association between c-Met overexpression and OS/DFS. If data were only available in the form of figures, we read Kaplan-Meier curves by Engauge Digitizer version 4.1 (free software downloaded from http://sourceforge.net) and extracted survival data HRs and 95%CI [28]. Data of clinicopathological features was extracted in studies available of ORs. The heterogeneity of included studies was assessed by using I2 statistics and P value, and if I2 > 50% or P< 0.1, the results were considered statistically significant and random effects models were employed; otherwise, fixed effects models were employed. Sensitivity analysis, also named influence analysis, was carried out to evaluate the effect of single study on the whole results and meanwhile try to find the origin of heterogeneity. Publication bias was assessed graphically using funnel plots, and funnel plot Symmetry was evaluated by Begg’s and Egger’s linear regression method. P<0.05 was considered statistically significant. Statistical analyses were performed using Stata 13.0 (Stata Corporation, College Station, TX).
ACKNOWLEDGMENTS
The authors would like to acknowledge all the members of clinical research center of The First Affiliated Hospital of Xi’an Jiaotong University
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
This study was supported by grants from National Natural Science Foundation of China (No. 81274136).
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016; 66: 7-30. doi: 10.3322/caac.21332.
2. Kim YJ, Choi JS, Seo J, Song JY, Lee SE, Kwon MJ, Kwon MJ, Kundu J, Jung K, Oh E, Shin YK, Choi YL. MET is a potential target for use in combination therapy with EGFR inhibition in triple-negative/basal-like breast cancer. Int J Cancer. 2014; 134: 2424-36. doi: 10.1002/ijc.28566.
3. Li Z, Yin S, Zhang L, Liu W, Chen B, Xing H. Clinicopathological characteristics and prognostic value of cancer stem cell marker CD133 in breast cancer: a meta-analysis. Onco Targets Ther. 2017; 10: 859-70. doi: 10.2147/ott.s124733.
4. Bahrami A, Shahidsales S, Khazaei M, Ghayour-Mobarhan M, Maftouh M, Hassanian SM, Avan A. C-Met as a potential target for the treatment of gastrointestinal cancer: current status and future perspectives. J Cell Physiol. 2017. doi: 10.1002/jcp.25794.
5. Han K, Chanu P, Jonsson F, Winter H, Bruno R, Jin J, Stroh M. Exposure-response and tumor growth inhibition analyses of the monovalent anti-c-MET antibody onartuzumab (MetMAb) in the second- and third-line non-small cell lung cancer. AAPS J. 2017; 19: 527-33. doi: 10.1208/s12248-016-0029-5.
6. Al-U’datt DG, Al-Husein BA, Qasaimeh GR. A mini-review of c-Met as a potential therapeutic target in melanoma. Biomed Pharmacother. 2017; 88: 194-202. doi: 10.1016/j.biopha.2017.01.045.
7. Wu JC, Wang CT, Hung HC, Wu WJ, Wu DC, Chang MC, Sung PJ, Chou YW, Wen ZH, Tai MH. Heteronemin is a novel c-Met/STAT3 inhibitor against advanced prostate cancer cells. Prostate. 2016; 76: 1469-83. doi: 10.1002/pros.23230.
8. Wang J, Cheng JX. c-Met inhibition enhances chemosensitivity of human ovarian cancer cells. Clin Exp Pharmacol Physiol. 2017; 44: 79-87. doi: 10.1111/1440-1681.12672.
9. Inanc M, Ozkan M, Karaca H, Berk V, Bozkurt O, Duran AO, Ozaslan E, Akgun H, Tekelioglu F, Elmali F. Cytokeratin 5/6, c-Met expressions, and PTEN loss prognostic indicators in triple-negative breast cancer. Med Oncol. 2014; 31: 801. doi: 10.1007/s12032-013-0801-7.
10. Nakopoulou L, Gakiopoulou H, Keramopoulos A, Giannopoulou I, Athanassiadou P, Mavrommatis J, Davaris PS. c-met tyrosine kinase receptor expression is associated with abnormal beta-catenin expression and favourable prognostic factors in invasive breast carcinoma. Histopathology. 2000; 36: 313-25.
11. Zagouri F, Brandstetter A, Moussiolis D, Chrysikos D, Dimitrakakis C, Tsigginou A, Marinopoulos S, Zografos GC, Sergentanis TN, Dimopoulos MA, Filipits M. Low protein expression of MET in ER-positive and HER2-positive breast cancer. Anticancer Res. 2014; 34: 1227-31.
12. Wang F, Li S, Zhao Y, Yang K, Chen M, Niu H, Yang J, Luo Y, Tang W, Sheng M. Predictive role of the overexpression for CXCR4, C-Met, and VEGF-C among breast cancer patients: a meta-analysis. Breast. 2016; 28: 45-53. doi: 10.1016/j.breast.2016.04.016.
13. Yan S, Jiao X, Zou H, Li K. Prognostic significance of c-Met in breast cancer: a meta-analysis of 6010 cases. Diagn Pathol. 2015; 10: 62. doi: 10.1186/s13000-015-0296-y.
14. Gastaldi S, Comoglio PM, Trusolino L. The Met oncogene and basal-like breast cancer: another culprit to watch out for? Breast Cancer Res. 2010; 12: 208. doi: 10.1186/bcr2617.
15. Xing F, Liu Y, Sharma S, Wu K, Chan MD, Lo HW, Carpenter RL, Metheny-Barlow LJ, Zhou X, Qasem SA, Pasche B, Watabe K. Activation of the c-Met pathway mobilizes an inflammatory network in the brain microenvironment to promote brain metastasis of breast cancer. Cancer Res. 2016; 76: 4970-80. doi: 10.1158/0008-5472.can-15-3541.
16. Hultberg A, Morello V, Huyghe L, De Jonge N, Blanchetot C, Hanssens V, De Boeck G, Silence K, Festjens E, Heukers R, Roux B, Lamballe F, Ginestier C, et al. Depleting MET-expressing tumor cells by adcc provides a therapeutic advantage over inhibiting HGF/MET signaling. Cancer Res. 2015; 75: 3373-83. doi: 10.1158/0008-5472.can-15-0356.
17. Ren X, Yuan L, Shen S, Wu H, Lu J, Liang Z. c-Met and ERbeta expression differences in basal-like and non-basal-like triple-negative breast cancer. Tumour Biol. 2016; 37: 11385-95. doi: 10.1007/s13277-016-5010-5.
18. Ho-Yen CM, Green AR, Rakha EA, Brentnall AR, Ellis IO, Kermorgant S, Jones JL. C-Met in invasive breast cancer: is there a relationship with the basal-like subtype? Cancer. 2014; 120: 163-71. doi: 10.1002/cncr.28386.
19. Liu TC, Peng X, Ma YC, Ji YC, Chen DQ, Zheng MY, Zhao DM, Cheng MS, Geng MY, Shen JK, Ai J, Xiong B. Discovery of a new series of imidazo[1,2-a]pyridine compounds as selective c-Met inhibitors. Acta Pharmacol Sin. 2016; 37: 698-707. doi: 10.1038/aps.2016.11.
20. Azuma K, Hirashima T, Yamamoto N, Okamoto I, Takahashi T, Nishio M, Hirata T, Kubota K, Kasahara K, Hida T, Yoshioka H, Nakanishi K, Akinaga S, et al. Phase II study of erlotinib plus tivantinib (ARQ 197) in patients with locally advanced or metastatic EGFR mutation-positive non-small-cell lung cancer just after progression on EGFR-TKI, gefitinib or erlotinib. ESMO Open. 2016; 1: e000063. doi: 10.1136/esmoopen-2016-000063.
21. Scagliotti G, von Pawel J, Novello S, Ramlau R, Favaretto A, Barlesi F, Akerley W, Orlov S, Santoro A, Spigel D, Hirsh V, Shepherd FA, Sequist LV, et al. Phase III multinational, randomized, double-blind, placebo-controlled study of tivantinib (ARQ 197) plus erlotinib versus erlotinib alone in previously treated patients with locally advanced or metastatic nonsquamous non-small-cell lung cancer. J Clin Oncol. 2015; 33: 2667-74. doi: 10.1200/jco.2014.60.7317.
22. Koeppen H, Yu W, Zha J, Pandita A, Penuel E, Rangell L, Raja R, Mohan S, Patel R, Desai R, Fu L, Do A, Parab V, et al. Biomarker analyses from a placebo-controlled phase II study evaluating erlotinib+/-onartuzumab in advanced non-small cell lung cancer: MET expression levels are predictive of patient benefit. Clin Cancer Res. 2014; 20: 4488-98. doi: 10.1158/1078-0432.ccr-13-1836.
23. Bendell JC, Hochster H, Hart LL, Firdaus I, Mace JR, McFarlane JJ, Kozloff M, Catenacci D, Hsu JJ, Hack SP, Shames DS, Phan SC, Koeppen H, et al. A phase ii randomized trial (GO27827) of first-line FOLFOX plus bevacizumab with or without the MET inhibitor onartuzumab in patients with metastatic colorectal cancer. Oncologist. 2017; 22: 264-71. doi: 10.1634/theoncologist.2016-0223.
24. Shah MA, Bang YJ, Lordick F, Alsina M, Chen M, Hack SP, Bruey JM, Smith D, McCaffery I, Shames DS, Phan S, Cunningham D. Effect of fluorouracil, leucovorin, and oxaliplatin with or without onartuzumab in HER2-negative, met-positive gastroesophageal adenocarcinoma: the METGastric randomized clinical trial. JAMA Oncol. 2016. doi: 10.1001/jamaoncol.2016.5580.
25. Tolaney SM, Tan S, Guo H, Barry W, Van Allen E, Wagle N, Brock J, Larrabee K, Paweletz C, Ivanova E, Janne P, Overmoyer B, Wright JJ, et al. Phase II study of tivantinib (ARQ 197) in patients with metastatic triple-negative breast cancer. Invest New Drugs. 2015; 33: 1108-14. doi: 10.1007/s10637-015-0269-8.
26. Dieras V, Campone M, Yardley DA, Romieu G, Valero V, Isakoff SJ, Koeppen H, Wilson TR, Xiao Y, Shames DS, Mocci S, Chen M, Schmid P. Randomized, phase II, placebo-controlled trial of onartuzumab and/or bevacizumab in combination with weekly paclitaxel in patients with metastatic triple-negative breast cancer. Ann Oncol. 2015; 26: 1904-10. doi: 10.1093/annonc/mdv263.
27. Zhao Y, Dai C, Wang M, Kang H, Lin S, Yang P, Liu X, Liu K, Xu P, Zheng Y, Li S, Dai Z. Clinicopathological and prognostic significance of metastasis-associated in colon cancer-1 (MACC1) overexpression in colorectal cancer: a meta-analysis. Oncotarget. 2016; 7: 62966-75. doi: 10.18632/oncotarget.11287.
28. Zhang QW, Liu L, Gong CY, Shi HS, Zeng YH, Wang XZ, Zhao YW, Wei YQ. Prognostic significance of tumor-associated macrophages in solid tumor: a meta-analysis of the literature. PLoS One. 2012; 7: e50946. doi: 10.1371/journal.pone.0050946.