
INTRODUCTION
Surgery is a treatment option for certain NSCLC patients, including those with localized (i.e. Stage I-II) and few patients locally advanced (i.e. Stage IIIA) disease. Currently, the NCCN recommends post-surgical observation only in pT1ab R0 or pT2a R0 patients. In contrast, the vast majority of post-operative NSCLC patients are recommended to receive POCT, with or without PORT. POCT is indicated in patients with T2a+ and N1+ disease. PORT is indicated if there is presence of pN2 disease, a positive margin (R+; e.g. R1 or R2), or ECE [1].
In patients with R0 disease who have indications for POCT and PORT, POCT is typically delivered prior to PORT (termed “late PORT” in this manuscript) because these patients are thought to likely harbor micrometastatic disease with a relatively low risk of locoregional disease that would cause a LRR. moreover, such patients would still receive PORT after POCT to prevent LRR. In contrast, the only subsets of patients where PORT is delivered concurrently with POCT or prior to POCT (termed “early PORT”). In these patients, the burden of local disease is theorized to outweigh the risk of micrometastatic disease; PORT is theorized to minimize further micrometastatic dissemination and prevent LRR. Nonetheless, the exact timing of PORT in relationship to POCT has not been investigated in R0 patients.
The aim of this study was to evaluate the ideal timing of PORT in the management of completely resected (R0) Stage IIIA-N2 NSCLC. We hypothesized that the delivery of early PORT in R0 patients would improve patient outcomes.
RESULTS
Patient characteristics
A total of 112 patients treated between January 1, 2008 and December 30, 2015 were included by a multidisciplinary tumor board from multiple hospitals. Of all eligible patients whose records were examined, 41 (36.6%) and 71 (63.4%) patients were assigned to the early PORT and late PORT, respectively. There were no significant differences in gender, age, smoking history, COPD history, ECOG PS score, tumor location, tumor histology, type of surgery, T classification, number of positive N2 MLNs, positive N2 MLN ratio, number of N2 MLN stations, the interval between surgery and POCT, and total dose of PORT between the two groups (all p > 0.05). Differences were observed for the interval between surgery and PORT, the number of POCT cycles and POCT regimens (p <0.05). The selection of patients and the baseline characteristics of all patients are shown in Figure 1 and Table 1.
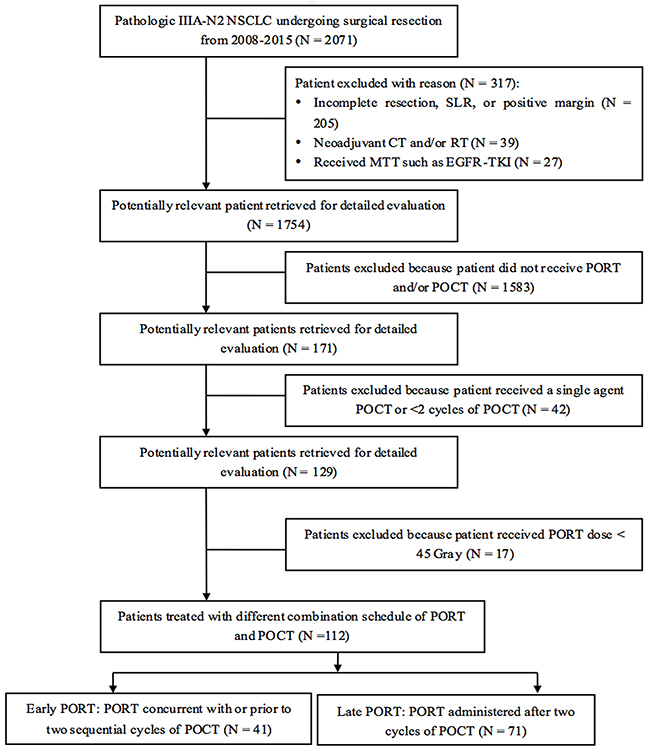
Figure 1: Patient selection. NSCLC: non-small cell lung cancer; SLR: sublobar lung resection; CT: chemotherapy; RT: radiotherapy; MTT: molecular targeted therapies; EGFR-TKI: epidermal growth factor tyrosine kinase inhibitors; MLN: mediastinal lymph node; PORT: postoperative radiotherapy; POCT: postoperative chemotherapy.
Table 1: Patient characteristics
Characteristics |
N (%) |
χ2 values |
p values |
||
|---|---|---|---|---|---|
Overall (N = 112) |
Early PORT (N = 41) |
Late PORT (N =71) |
|||
Gender |
|||||
Male |
77 (68.8) |
32 (78.1) |
45 (63.4) |
2.60 |
0.11 |
Female |
35 (31.2) |
9 (21.9) |
26 (36.6) |
||
Age (median years) |
|||||
≤ 58 |
59 (52.7) |
19 (46.3) |
40 (56.3) |
1.04 |
0.31 |
> 58 |
53 (47.3) |
22 (53.7) |
31 (43.7) |
||
Smoking history |
|||||
Yes |
69 (61.6) |
29 (70.7) |
40 (56.3) |
2.28 |
0.13 |
No |
43 (38.4) |
12 (29.3) |
31 (43.7) |
||
COPD history† |
|||||
Yes |
4 (3.6) |
2 (4.9) |
2 (2.8) |
0.32 |
0.57 |
No |
108 (96.4) |
39 (95.1) |
69 (97.2) |
||
ECOG-PS score† |
|||||
0-1 |
111 (99.1) |
40 (97.6) |
71 (100) |
2.03 |
0.16 |
2 |
1 (0.9) |
1 (2.4) |
0 |
||
Tumor location |
|||||
RUL |
30 (26.8) |
12 (29.3) |
18 (25.4) |
2.23 |
0.69 |
RML |
5 (4.5) |
2 (4.9) |
3 (4.2) |
||
RLL |
24 (21.4) |
7 (17.1) |
17 (23.9) |
||
LUL |
32 (28.5) |
10 (24.4) |
22 (31.0) |
||
LLL |
21 (18.8) |
10 (24.3) |
11 (15.5) |
||
Tumor histology |
|||||
Squamous cell |
42 (37.5) |
18 (43.9) |
24 (33.8) |
4.58 |
0.10 |
Adenocarcinoma |
55 (49.1) |
15 (36.6) |
40 (56.3) |
||
Others |
15 (13.4) |
8 (19.5) |
7 (9.9) |
||
Type of surgery† |
|||||
Lobectomy |
111 (99.1) |
41 (100) |
70 (98.6) |
0.92 |
0.34 |
Ipsilateral pneumonectomy |
1 (0.9) |
0 |
1 (1.4) |
||
T classification |
|||||
T1 |
32 (28.6) |
14 (34.2) |
18 (25.4) |
2.08 |
0.56 |
T2 |
55 (49.1) |
17 (41.5) |
38 (53.5) |
||
T3 |
17 (15.2) |
6 (14.6) |
11 (15.5) |
||
T4 |
8 (7.1) |
4 (9.7) |
4 (5.6) |
||
Number of dissected N2 nodes |
|||||
< 9 |
41 (36.6) |
15 (36.6) |
26 (36.6) |
0.00001 |
1.00 |
≥ 9 |
71 (63.4) |
26 (63.4) |
45 (63.4) |
||
Number of positive N2 MLNs |
|||||
Single |
45 (40.2) |
15 (36.6) |
30 (42.3) |
0.35 |
0.56 |
Multiple |
67 (59.8) |
26 (63.4) |
41 (57.7) |
||
Positive N2 MLN ratio |
|||||
< 25% |
54 (48.2) |
23 (56.1) |
31 (43.7) |
1.61 |
0.21 |
≥ 25% |
58 (51.8) |
18 (43.9) |
40 (56.3) |
||
Number of N2 MLN positive stations |
|||||
Single |
59 (52.7) |
21 (51.2) |
38 (53.5) |
0.06 |
0.81 |
Multiple |
53 (47.3) |
20 (48.8) |
33 (46.45) |
||
Interval between surgery and POCT (months) |
1.3 ± 0.6 |
1.4 ± 0.8 |
1.2 ± 0.5 |
1.14 |
0.26 |
Interval between surgery and PORT (months) |
4.9 ± 2.6 |
3.2 ± 1.1 |
5.9 ± 2.8 |
4.99 |
0.0001 |
Total dose of PORT |
|||||
< 50 Gy |
5 (4.4) |
0 |
5 (7.0) |
3.02 |
0.08 |
≥ 50 Gy |
107 (95.6) |
41 (100) |
66 (93.0) |
||
POCT regimen‡ |
|||||
TP/DP |
53 (47.3) |
26 (63.4) |
27 (38.0) |
14.16 |
0.003 |
CP |
40 (25.7) |
14 (34.2) |
26 (36.6) |
||
GP/GC |
18 (16.1) |
1 (2.4) |
17 (23.9) |
||
NP |
1 (0.9) |
0 |
1 (1.5) |
||
# of POCT cycles |
|||||
< 4 |
15 (13.4) |
15 (36.6) |
0 |
29.99 |
0.0001 |
≥ 4 |
97 (86.6) |
26 (63.4) |
71 (100) |
||
Gene expression status |
|||||
EGFR mutation |
9 (8.0) |
2 (4.9) |
7 (9.9) |
1.49 |
0.47 |
ALK positive |
1 (0.9) |
0 |
1 (1.4) |
||
N/A |
102 (91.1) |
39 (95.1) |
63 (88.7) |
||
Molecular targeted therapy |
|||||
Erlotinib |
2 (1.8) |
1 (2.4) |
1 (1.4) |
2.35 |
0.50 |
Gefitinib |
7 (6.3) |
1 (2.4) |
6 (8.5) |
||
Crizotinib |
1 (0.9) |
0 |
1 (1.4) |
||
None |
102 (91.0) |
39 (95.2) |
63 (88.7) |
||
Treatment strategies after progression |
|||||
RT |
12 (10.7) |
3 (7.3) |
9 (12.7) |
2.91 |
0.41 |
S |
20 (17.9) |
1 (2.4) |
0 |
||
CT |
9 (8.0) |
9 (22.0) |
19 (26.8) |
||
BSC |
71 (63.4) |
28 (68.3) |
43 (60.5) |
||
Note: Bold-face denotes p-value < 0.05.
†Subgroups have less than five patients.
‡ Platinum-based CT regimens included cisplatin, carboplatin, or oxaliplatin.
COPD: chronic obstructive pulmonary disease; ECOG-PS: the Eastern Cooperative Oncology Group scale-performance status; RUL: right upper lobe; RML: right middle lobe; RLL: right lower lobe; LUL: left upper lobe; LLL: left lower lobe; TP/DP: paclitaxel or docetaxel + platinum included cisplatin, carboplatin, or oxaliplatin; CP: pemetrexed + platinum included cisplatin, carboplatin, or oxaliplatin; GP/GC: gemcitabine + platinum included cisplatin, carboplatin, or oxaliplatin; NP: vinorelbine + platinum included cisplatin, carboplatin, or oxaliplatin; PORT: postoperative radiotherapy; POCT: postoperative chemotherapy; EGFR: epidermal growth factor receptor; ALK: anaplastic lymphoma kinase; N/A: not report; RT: radiotherapy; CT: chemotherapy; S: surgery; BSC: best supportive care.
OS, LRRFS, and DMFS
For the whole cohort, the median OS, LRRFS, and DMFS were not reached during the median follow-up was 29.6 months (range, 4.7–93.5 months) (Figure 2). The 3- and 5-year OS rates were 79.1% and 73.1% in the early PORT, respectively; these were statistically significantly higher than those of late PORT group, with the respective rates of 63.2% and 53.4%. The 3- and 5-year LRFFS rates were 80.5% and 80.5% in the early PORT and 65.9% and 62.4% in the late PORT, respectively, and the differences in LRFFS rates between the two groups trended toward significance. The 3- and 5-year DMFS rates were 76.1% and 69.2% in the early PORT as well as 49.0% and 46.1% in late PORT, respectively, and the differences in DMFS rates between the two groups also were significant (all p < 0.05).
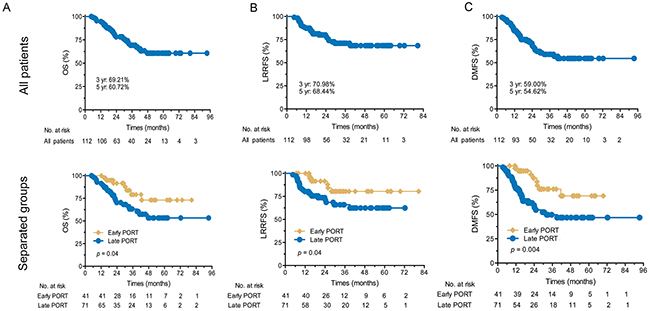
Figure 2: Kaplan–Meier survival curves. (A) OS for all patients and separate groups; (B) LRRFS for all patients and separate groups; (C) DMFS for all patients and separate groups. OS: overall survival; yr: year; LRRFS: locoregional recurrence-free survival; DMFS: distant metastasis-free survival; PORT: postoperative radiotherapy; POCT: postoperative chemotherapy.
Patterns of failure and the first failure
Up to the last follow-up, treatment failure was observed in 50 (44.6%) patients, LR occurred in 24 (21.4%) patients, DM occurred in 44 (39.3%) patients, and both LR and DM occurred in 18 (16.1%) patients. LR occurred as the first failure site in 6 (14.6%) and 15 (21.1%) patients in the early and late PORT groups, respectively (p = 0.40). DM occurred as the first failure site in 13 (31.7%) patients in the early PORT versus 26 (36.6%) patients in the late PORT (p = 0.21). Both LR and DM occurred as the first failure site in 3 (7.3%) and 7 (9.9%) patients in the early and late PORT groups, respectively (p = 0.65). In addition, of 44 (39.3%) patients who had DM, the most frequent sites were lung, bone, lung pleura, central nervous system, adrenal gland, liver, and others sequentially. The cumulative incidences of LR and DM are listed in Table 2.
Table 2: Pattern of failure and the first failure
Parameters |
N (%) |
χ2 values |
p values |
||
|---|---|---|---|---|---|
All (N = 112) |
Early PORT (N = 41) |
Late PORT (N = 71) |
|||
LR as first site of failure |
|||||
Yes |
21 (18.8) |
6 (14.6) |
15 (21.1) |
0.72 |
0.40 |
No |
91 (81.2) |
35 (85.4) |
56 (78.9) |
||
All LR failure |
|||||
Yes |
24 (21.4) |
8 (39.0) |
16 (22.5) |
0.14 |
0.71 |
No |
88 (78.6) |
33 (61.0) |
55 (77.5) |
||
DM as first site of failure |
|||||
Yes |
39 (34.8) |
13 (31.7) |
26 (36.6) |
1.56 |
0.21 |
No |
73 (65.2) |
28 (68.3) |
45 (63.4) |
||
All DM failure |
|||||
Yes |
44 (39.3) |
13 (31.7) |
31 (43.7) |
1.56 |
0.21 |
No |
68 (60.7) |
28 (68.3) |
40 (56.3) |
||
Both LR and DM as first site of failure |
|||||
Yes |
10 (8.9) |
3 (7.3) |
7 (9.9) |
0.21 |
0.65 |
No |
102 (91.1) |
38 (92.7) |
64 (90.1) |
||
Both LR and DM failure |
|||||
Yes |
18 (16.1) |
5 (12.2) |
13 (18.3) |
0.72 |
0.39 |
No |
94 (83.9) |
36 (87.8) |
58 (81.7) |
||
Site of DM† |
|||||
Lung |
20 (17.9) |
7 (17.1) |
13 (18.3) |
- |
- |
Bone |
14 (12.5) |
3 (7.3) |
11 (15.5) |
||
Lung pleura |
7 (6.3) |
3 (7.3) |
4 (5.6) |
||
Central nervous system |
6 (5.4) |
2 (4.9) |
4 (5.6) |
||
Adrenal gland |
4 (3.5) |
1 (2.4) |
3 (4.2) |
||
Liver |
4 (3.5) |
2 (4.9) |
2 (2.8) |
||
Others |
6 (5.4) |
1 (2.4) |
5 (7.0) |
||
Note: some patients had more than one site of LR or/and DM failure at the same time.
PORT: postoperative radiotherapy; LR: locoregional recurrence; DM: distant metastasis.
†Fifteen patients concurrent with multiple metastases including lung, bone, lung pleura, central nervous system, adrenal gland, liver, or others.
Prognostic factors associated with OS, LRRFS, and DMFS
The results of univariate analyses for clinical factors affecting OS are presented in Table 3. The patients with ≥ 4 CT cycles of POCT and those who received early PORT experienced significantly greater OS, LRRFS, and DMFS (all p < 0.05). In addition, age (p = 0.01), smoking history (p = 0.02), the number of POCT cycles (p = 0.007), and the combination schedule of PORT and POCT (p = 0.04) were significant factors affecting OS; simultaneously, tumor histology (p = 0.02 and p = 0.03), the number of POCT cycles (p = 0.02 and p = 0.03), and the combination schedule of PORT and POCT (p = 0.04 and p = 0.004) were statistically significant clinical factors affecting LRRFS and DMFS, respectively.
Table 3: Univariate analyses for clinical variables affecting OS, LRRFS, and DMFS
Variable |
OS |
LRRFS |
DMFS |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
3-yr |
5-yr |
χ2 |
p |
3-yr |
5-yr |
χ2 |
p |
3-yr |
5-yr |
χ2 |
p |
|
Patient inclusion site |
||||||||||||
A |
70.4% |
65.0% |
1.31 |
0.73 |
74.0% |
74.0% |
3.25 |
0.35 |
65.7% |
60.3% |
4.30 |
0.23 |
B |
64.1% |
46.1% |
59.8% |
59.8% |
44.7% |
44.7% |
||||||
C |
63.5% |
63.5% |
61.5% |
61.5% |
53.6% |
53.6% |
||||||
D |
76.2% |
76.2% |
83.1% |
83.1% |
60.6% |
60.6% |
||||||
Gender |
||||||||||||
Male |
63.8% |
57.0% |
2.02 |
0.16 |
73.1% |
68.8% |
0.01 |
0.92 |
54.8% |
51.4% |
0.66 |
0.42 |
Female |
71.9% |
67.1% |
65.8% |
65.8% |
66.3% |
59.7% |
||||||
Age |
||||||||||||
≤ 58 years |
81.1% |
70.7% |
6.27 |
0.01 |
68.0% |
68.0% |
0.04 |
0.84 |
57.5% |
53.7% |
0.02 |
0.88 |
> 58 years |
52.8% |
47.5% |
76.1% |
69.2% |
60.5% |
55.0% |
||||||
Smoking history |
||||||||||||
Yes |
58.1% |
54.5% |
5.27 |
0.02 |
71.0% |
71.0% |
0.14 |
0.71 |
53.4% |
53.4% |
0.61 |
0.44 |
No |
84.1% |
69.1% |
71.7% |
66.9% |
65.7% |
56.8% |
||||||
COPD history† |
||||||||||||
Yes |
75.0% |
0 |
1.84 |
0.18 |
100% |
100% |
1.04 |
0.31 |
50.0% |
50.0% |
0.14 |
0.71 |
No |
70.2% |
61.6% |
70.1% |
67.5% |
58.7% |
54.3% |
||||||
ECOG-PS score† |
||||||||||||
0-1 |
68.5% |
60.1% |
0.17 |
0.68 |
71.8% |
69.2% |
3.39 |
0.07 |
59.0% |
54.6% |
3.25 |
0.07 |
2 |
100% |
100% |
0 |
0 |
0 |
0 |
||||||
Tumor location |
||||||||||||
RUL |
74.0% |
64.1% |
9.31 |
0.05 |
53.6% |
53.6% |
2.50 |
0.65 |
57.2% |
49.0% |
4.79 |
0.31 |
RML |
100% |
100% |
80.0% |
80.0% |
80.0% |
80.0% |
||||||
RLL |
60.0% |
25.0% |
59.1% |
59.1% |
43.2% |
43.2% |
||||||
LUL |
75.0% |
75.0% |
72.5% |
72.5% |
51.8% |
51.8% |
||||||
LLL |
77.9% |
77.9% |
85.7% |
85.7% |
82.7% |
68.9% |
||||||
Tumor histology |
||||||||||||
Sqa |
78.0% |
78.0% |
3.28 |
0.19 |
88.2% |
88.2% |
8.43 |
0.02 |
75.5% |
75.5% |
7.13 |
0.03 |
Ade |
61.6% |
55.4% |
59.5% |
59.5% |
46.3% |
46.3% |
||||||
Others |
81.8% |
56.1% |
72.9% |
72.9% |
66.3% |
53.0% |
||||||
Type of surgery† |
||||||||||||
Lobectomy |
68.2% |
59.6% |
0.51 |
4.73 |
70.6% |
68.0% |
0.38 |
0.54 |
57.9% |
53.5% |
0.62 |
0.43 |
Ipsilateral pneumonectomy |
100% |
100% |
100% |
100% |
100% |
100% |
||||||
T classification |
||||||||||||
T1 |
82.9% |
76.0% |
2.96 |
0.40 |
74.4% |
74.4% |
0.60 |
0.90 |
62.9% |
62.9% |
1.78 |
0.62 |
T2 |
62.1% |
55.2% |
67.9% |
67.9% |
52.2% |
48.2% |
||||||
T3 |
61.9% |
46.5% |
81.1% |
54.1% |
69.3% |
52.0% |
||||||
T4 |
85.7% |
0 |
70.0% |
70.0% |
87.5% |
87.5% |
||||||
Number of N2 MLN positive nodes |
||||||||||||
Single |
73.2% |
55.8% |
0.02 |
0.90 |
74.5% |
74.5% |
0.11 |
0.74 |
61.8% |
56.6% |
0.04 |
0.84 |
Multiple |
64.6% |
64.6% |
68.6% |
63.7% |
55.6% |
51.6% |
||||||
Positive N2 MLN ratio |
||||||||||||
≤ 25% |
67.6% |
58.7% |
0.001 |
0.97 |
74.4% |
69.1% |
0.68 |
0.41 |
61.1% |
56.4% |
1.69 |
0.19 |
> 25% |
69.5% |
61.5% |
67.4% |
67.4% |
55.8% |
51.5% |
||||||
Number of N2 MLN positive stations |
||||||||||||
Single |
79.2% |
79.2% |
3.71 |
0.04 |
74.1% |
74.1% |
0.004 |
0.95 |
60.1% |
55.8% |
0.25 |
0.62 |
Multiple |
61.2% |
48.0% |
70.4% |
65.0% |
57.2% |
52.5% |
||||||
Total dose of PORT† |
||||||||||||
< 50 Gy |
80.0% |
80.0% |
0.01 |
0.91 |
80.0% |
80.0% |
0.02 |
0.90 |
66.7% |
66.7% |
0.14 |
0.71 |
≥ 50 Gy |
68.3% |
59.7% |
70.6% |
67.9% |
58.3% |
53.8% |
||||||
Number of POCT cycles |
||||||||||||
< 4 |
45.6% |
45.6% |
7.41 |
0.007 |
56.8% |
56.8% |
5.94 |
0.02 |
49.1% |
49.1% |
4.38 |
0.03 |
≥ 4 |
73.0% |
63.1% |
74.0% |
71.1% |
60.2% |
57.2% |
||||||
The combination schedule |
||||||||||||
Early PORT |
79.1% |
73.1% |
4.19 |
0.04 |
80.5% |
80.5% |
4.12 |
0.04 |
76.1% |
69.2% |
8.16 |
0.004 |
Late PORT |
63.2% |
53.4% |
65.9% |
62.4% |
49.0% |
46.1% |
||||||
Note: Bold-face denotes p-value < 0.05.
† Subgroups have less than five patients.
OS: overall survival; LRRFS: locoregional recurrence-free survival; DMFS: distant metastasis-free survival; MST: median survival time; mo: months; yr: year; COPD: chronic obstructive pulmonary disease; ECOG-PS: the Eastern Cooperative Oncology Group scale-performance status; RUL: right upper lobe; RML: right middle lobe; RLL: right lower lobe; LUL: left upper lobe; LLL: left lower lobe; Sqa: squamous cell; Ade: adenocarcinoma; MLN: mediastinal lymph node; PORT: postoperative radiotherapy; POCT: postoperative chemotherapy.
On multivariate analyses, the statistically significant prognostic factors for OS included tumor histology (HR = 2.186, p = 0.04), number of POCT cycles (HR = 0.235, p = 0.005), and the combination schedule of PORT and POCT (HR = 0.183, p = 0.001). Significant prognostic factors for LRRFS and DMFS included ECOG-PS score (HR = 72.343, p = 0.02; HR = 36.565, p = 0.004), tumor histology (HR = 2.176, p = 0.054; HR = 2.011, p = 0.04), number of POCT cycles (HR = 0.131, p = 0.0001; HR = 0.292, p = 0.009), and the combination schedule of PORT and POCT (HR = 0.196, p = 0.005; HR = 0.167, p = 0.0001), respectively (Table 4).
Table 4: Multivariable analyses for clinical variables affecting OS, LRRFS, and DMFS
Variable |
OS |
LRRFS |
DMFS |
||||||
|---|---|---|---|---|---|---|---|---|---|
HR |
95% CI |
p value |
HR |
95% CI |
p value |
HR |
95% CI |
p value |
|
Patient inclusion site (A vs. B vs. C vs. D) |
0.944 |
0.642-1.387 |
0.944 |
0.901 |
0.570-1.423 |
0.654 |
1.193 |
0.823-1.729 |
0.351 |
Gender (female vs. male) |
1.155 |
0.361-3.690 |
0.808 |
1.288 |
0.409-4.057 |
0.665 |
0.760 |
0.303-1.907 |
0.559 |
Age (≤ 58 vs. > 58) |
1.771 |
0.795-3.946 |
0.162 |
0.701 |
0.289-1.700 |
0.432 |
0.901 |
0.453-1.793 |
0.901 |
Smoking history (yes vs. no) |
0.289 |
0.091-0.920 |
0.036 |
0.733 |
0.232-2.318 |
0.597 |
0.735 |
0.298-1.813 |
0.503 |
COPD history (yes vs. no)† |
0.322 |
0.059-1.762 |
0.191 |
302.604 |
0.0001- |
0.986 |
1.181 |
0.148-9.397 |
0.875 |
ECOG-PS score (0-1 vs. 2)† |
0 |
0 |
0.992 |
72.343 |
4.712-1110.747 |
0.002 |
36.565 |
3.151-424.359 |
0.004 |
Tumor location (RUL vs. RML vs. RLL vs. LUL vs. LLL) |
0.954 |
0.725-1.254 |
0.734 |
0.944 |
0.706-1.262 |
0.697 |
1.065 |
0.835-1.358 |
0.612 |
Tumor histology (Sqa vs. Ade vs. others) |
2.186 |
1.036-4.616 |
0.040 |
2.176 |
0.988-4.793 |
0.054 |
2.011 |
1.031-3.922 |
0.040 |
Type of surgery (lobectomy vs. Ipsilateral pneumonectomy)† |
0 |
0 |
0.981 |
0.0001 |
0.0001- |
0.993 |
0.0001 |
0.0001- |
0.977 |
T classification (T1 vs. T2 vs. T3 vs. T4) |
1.393 |
0.871-2.229 |
0.167 |
1.125 |
0.675-1.873 |
0.652 |
1.127 |
0.728-1.744 |
0.592 |
Number of N2 MLN positive stations (single vs. multiple) |
0.461 |
0.191-1.114 |
0.085 |
0.747 |
0.309-1.802 |
0.516 |
1.041 |
0.517-2.096 |
0.911 |
Total dose of PORT (< 50 Gy vs. ≥ 50 Gy) |
8.364 |
0.748-93.488 |
0.085 |
6.951 |
0.632-76.416 |
0.113 |
5.047 |
0.603-42.208 |
0.135 |
Number of POCT cycles (≥ 4vs. < 4) |
0.235 |
0.086-0.640 |
0.005 |
0.131 |
0.043-0.400 |
0.0001 |
0.292 |
0.117-0.732 |
0.009 |
The combination schedule (early PORT vs. late PORT) |
0.183 |
0.066-0.511 |
0.001 |
0.196 |
0.063-0.611 |
0.005 |
0.167 |
0.064-0.434 |
0.0001 |
† Subgroups have less than five patients.
Note: Bold-face denotes p-value < 0.05.
OS = overall survival; LRRFS: locoregional recurrence-free survival; DMFS: distant metastasis-free survival; HR: hazard ratio; CI: confidence interval; COPD: chronic obstructive pulmonary disease; ECOG-PS: the Eastern Cooperative Oncology Group scale-performance status; Sqa: squamous cell; Ade: adenocarcinoma; RUL: right upper lobe; RML: right middle lobe; RLL: right lower lobe; LUL: left upper lobe; LLL: left lower lobe; MLN: mediastinal lymph node; PORT: postoperative radiotherapy; POCT: postoperative chemotherapy.
Toxicities
Twelve patients (10.7%) experienced CTCAE v4.0 Grade 1 to 2 acute toxicities including pneumonitis, esophagitis, chest pain, agranulocytosis, and throm-bocytopenia. Five patients (4.5%) experienced Grade 3 acute toxicities including esophagitis and tracheitis. Almost all of these acute toxicities occurred in the early PORT group, and they were generally transient and resolved with conservative management. Late radiation toxicities were observed in two patients (1.8%) including pulmonary fibrosis, and both patients were in the early PORT. None of the patients died from Grade 5 late toxicities.
DISCUSSION
With improvements in radiotherapy equipment and techniques, several clinicians have investigated the efficacy and safety of PORT for patients with resected NSCLC and demonstrated decreased survival in the subset of N0-1 NSCLC patients who received PORT. However, in patient with pathologic N2 disease, the use of PORT was associated with a significant improvement in OS without serious toxicities [2-7]. Although it has yet to be proven in randomized trials, the NCCN recommends a sequence of POCT and PORT for patients with pathologic Stage IIIA-N2 NSCLC, because PORT has been incorporated into multidisciplinary management to improve locoregional control in resected Stage IIIA-N2 NSCLC, which may further translate into a survival benefit. However, the optimal schedule of PORT and POCT remains poorly understood and warrants further investigation for patients with pathologic stage IIIA-N2 NSCLC.
There has been no study comparing the optimal sequencing of POCT and PORT among patients with pathologic Stage IIIA-N2 R0 NSCLC [8]. In the absence of randomized data, we sought to answer this question in a multi-institutional retrospective study of high-quality data to provide insight into the relationship between the PORT and POCT combination schedule and survival. In this study, we found that pathologic Stage IIIA-N2 R0 NSCLC patients treated with early PORT had better OS, LRRFS, and DMFS than those treated with late PORT. Thus, early PORT is associated with improved outcomes in pathologic Stage IIIA-N2 R0 NSCLC. Our study provides new evidence to optimize the postoperative treatment strategy for patients with pathologic Stage IIIA-N2 NSCLC. Prospective studies must be performed to confirm the optimal schedule of PORT and POCT in the treatment of patients with pathologic Stage IIIA-N2 NSCLC.
In the definitive treatment for locally advanced NSCLC, concurrent POCT and PORT has been proven to be superior to RT alone [9], as well as to sequential chemotherapy followed by RT [10]. Some phase II studies have shown that postoperative concurrent POCT and PORT provide promising results both in terms of treatment-related toxicities and survival [11-13]. However, other studies report no improvement in outcomes with concurrent POCT and PORT vs either treatment alone [13-14]. Further, the IAEA stated that PORT represents a form of elective nodal irradiation (ENI), and this concept has been abandoned gradually in clinical practice despite a lack of clear evidence for such an approach [15-16]. These results led us to presume that a suboptimal timing of POCT and PORT cause their inefficacy in these patients.
The ACR guidelines recommend delivering PORT sequentially after completion of POCT because POCT would address micrometastatic disease, and DMs are a prevailing failure pattern among these patients [17]. For example, Dautzenberg et al. reported on 267 patients (259 with Stage II and III disease) who were randomized to PORT with 60 Gray or POCT followed by PORT [18]. There was no difference in DFS or OS between the two arms; DMs occurred more frequently in the RT group (p = 0.09) whereas LR occurred similarly in both groups (p = 0.27). Additionally, in a retrospective study of 105 patients with Stage IIIA-N2 NSCLC, a PORT-first strategy after surgery appeared not to compromise the clinical outcomes. The benefit of POCT on OS, with or without PORT first [19]. Together, these previous findings indicate that the optimal combination schedule of PORT and POCT remains poorly understood and warrants further investigation.
Our multi-institutional retrospective study showed that the median OS was longer for those who received early PORT than for those who received late PORT. The rationale for early PORT comes from multiple factors. First, locoregional tumor burden is assumed to be higher than that of distant micrometastases in patients with pN2 disease [20]. Second, PORT tends to achieve a better tumor response rate when compared to historical trials using POCT [21-23]; thus, delaying PORT may lead to the loss of optimal time for controlling the locoregional residual tumor. Third, the addition of POCT after surgery for patients with operable NSCLC improves OS, irrespective of whether POCT was adjuvant to surgery alone or adjuvant to surgery plus PORT [24].
Recently, Lee et al. demonstrated that the PORT followed by POCT might be more effective in terms of locoregional control without compromising OS for Stage IIIA-N2 NSCLC [19]. The 5-year OS of the early PORT in the present study was 60.7%, which is similar to their reported value of 61.3%. In the study by Lee et al., one of the most important questions about sequential PORT followed by POCT was whether postponing POCT might be deleterious to survival. In our study, there were 15 patients who received fewer than 4 cycles of POCT (Table 1), and this may compromise its efficacy. Therefore, the combination schedule of PORT and POCT warrant further investigation for patients with pathologic Stage IIIA-N2 NSCLC.
Detailed investigation of the patterns of failure after treatment enables the identification of optimum treatments. In the present study, the combined event rate for LR and DM of almost 44.6% (50 patients), and the plurality of failures were DMs (Table 2). This failure pattern is likely reflective of the relatively large number of patients with adenocarcinoma as the primary histologic subtype (Table 1). There were no differences between the two groups in terms of LR, DM, and both LR and DM as relapse or the first site of relapse (all p > 0.05, Table 2); nonetheless, our analysis revealed that early PORT, compared with late PORT, was associated with improved OS, LRRFS, and DMFS (all p < 0.05, Table 3). One possible reason might be that early PORT exterminated the existing small tumors and reduced the possibility of these small tumors to spread to remote locations. Furthermore, multivariate analyses showed that ≥ 4 cycles of POCT and early PORT were favorable prognostic factors for OS, LRRFS, and DMFS (all p < 0.05, Table 4).
The appropriate dose in the PORT has not been addressed in a randomized trial. The required dose for sites of potential occult disease may vary depending on the probability of residual disease, the number of sites at risk, and the desired control rate. Together, the results of our study along with those of previous studies suggest that PORT doses of 45 Gy or higher are well tolerated when given with two different combination schedules of PORT and POCT. It should be noted that the older randomized trials using this dose found no survival benefit, presumably due to excess toxicity related to PORT. By comparison, modern radiotherapy equipment and techniques including 3D-CRT, IMRT, and VMAT have been widely adapted in several clinical areas in an effort to improve dose homogeneity and target coverage, and to decrease normal tissue exposure in comparison to outdated radiation equipment and techniques.
In addition, although growing evidence suggests that PORT administered using the modern PORT technique has a favorable effect on the survival of patients with N2 disease, there exists significant heterogeneity within the reported studies with respect to the irradiation fields employed for PORT and the consensus guidelines regarding the dose and CTV [25-28]. Recently, Feng et al. designed a patterns-of-failure study after R0 surgery in resected N2 disease to evaluate the rationale of the proposed PORT CTVs based on the most likely sites of nodal failure, and the institutional standard CTV delineation for PORT was developed in their hospital [29-30]. Similar to these studies, our CTV encompassed the bronchial stump and involved mediastinal nodal stations and their next draining stations.
The present study does have potential weakness. First, the study carries with it all of the limitations inherent to a retrospective analysis. Second, the sample size of the present study was relatively small; however, patients with pathologic Stage IIIA-N2 R0 NSCLC treated with PORT were rare during the past decades when the PORT meta-analysis was published. Third, this study did analyze RT dose (<50 Gy and ≥50 Gy) as a variable for OS, LRRFS, and DMFS in uni- and multivariate analyses, and the effect of the RT dose did not seem to be significant. However, more specific RT details such as dose to normal tissues need to be reported. Additionally, these are more heterogeneity in the IIIA-N2 patients. Some patients are optional to fail in distant metastases, others patients more in local-regional regions. For example, the late PORT group included more adenocarcinoma patients with more DM. This may explain the more DM in late PORT group. Finally, we acknowledge that the method by which patients were chosen to receive the different combination schedule of PORT and POCT was not random but rather influenced by patients’ and physicians’ preferences, baseline characteristics, and practice patterns; therefore, it may have contributed to study bias.
PATIENTS AND METHODS
Study design and eligible patients
We queried a retrospective database of patients with known histologies of pathologic Stage IIIA-N2 NSCLC from multiple hospitals. Patients were treated between January 1, 2008 and December 30, 2015. All patients were examined in a multidisciplinary setting by surgical, medical, and radiation oncologists at the time of diagnosis, and their cases were re-presented in front of the tumor board on an as-needed basis (e.g., postoperatively).
The inclusion criteria were defined as follows: (I) any age; (II) KPS ≥ 70 (assessed pre- and post-operatively); (III) pathologic Stage IIIA-N2 NSCLC with histologic confirmation (assessed post-operatively); (IV) life expectancy >6 months in order to exclude perioperative mortality (assessed pre-operatively); (V) receipt of surgical resection with negative margins (R0) plus complete MLN dissection, PORT, and POCT; and (VI) written informed consent for the treatment and inclusion in the database.
The exclusion criteria were as follows: (I) non pathological Stage IIIA-N2 NSCLC; (II) sublobar lung resection, no radical resection, or incomplete MLN dissection; (III) use of neoadjuvant chemotherapy and/or radiotherapy; (IV) use of molecular targeted therapies such as epidermal growth factor tyrosine kinase inhibitors (EGFR-TKIs), etc.; (V) receipt of single agent of POCT or <2 cycles of POCT; (VI) PORT dose < 45 Gray and/or with palliative RT intent; (VII) evidence of metastatic disease; (VII) contraindication to receiving combination therapy (e.g. change in performance status); and (VIII) uncontrolled comorbid conditions (metabolic or psychiatric). The study protocol was designed in accordance with the ethical guidelines of the Declaration of Helsinki and was approved by the independent ethics committees at all participating hospitals.
Treatment schedule
The treatment schedule and definitions of early vs. late PORT are shown in Figure 3. For baseline staging, bronchoscopy, computed tomography scanning of the chest and upper abdomen, brain MRI with enhancement, and bone scintigraphy or PET-CT were routinely performed. All patients underwent lobectomy or ipsilateral pneumonectomy as well as complete MLN dissection. In addition, the administration of PORT for a patient with pathologic Stage IIIA-N2 disease was based on the attending radiation oncologist’s decision and, partially, the referring surgeon’s suggestion.
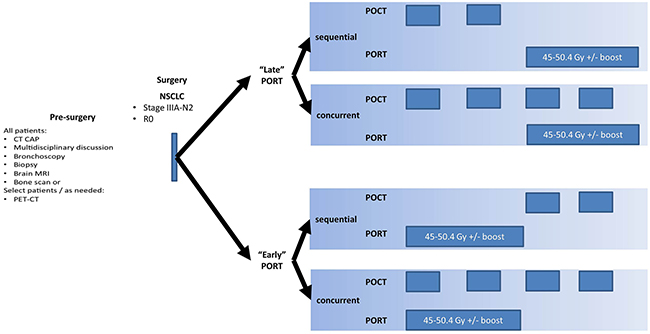
Figure 3: Treatment scheme and definition of “early” and “late” PORT.
PORT treatment was per our institutional guidelines, which were applicable to all patients fitting inclusion criteria. PORT was administered with 3D-CRT, IMRT, or VMAT. The initial CTV encompassed a bronchial stump, involved the mediastinal nodal stations and the next draining stations. The boost CTV included a bronchial stump and involved nodal stations only. The PTV was extended in all directions from the CTV by a margin of 1–1.5 cm. The tumor bed was included only if invasion of the parietal pleura was documented in the operative report. Neither the contralateral hilum nor the supraclavicular fossae were included on a routine basis. If, however, it was necessary to treat the tumor bed for a lesion of the upper lobe, the supraclavicular fossae were included. Conventional fractionation (1.8–2.0 Gray/day) was used with a dose of 45–50.4 Gray for the initial volume, and the boost volume was irradiated up to 60 Gray according to the risk of recurrence.
Data gathered for POCT included agent(s) used and the number of POCT cycles, and the combination schedule of PORT and POCT was extracted for each patient. Per Figure 2, included patients were divided (1) “early PORT,” which was defined by a regimen in which patients received PORT concurrent with POCT, or following two cycles of POCT; (2) and “late PORT,” which was defined by a regimen in which patients received two cycles of POCT without PORT, and then received PORT (with or without concurrent chemotherapy).
Follow-up
Patients were seen in clinic at 1 month after completion of treatment, then every 3 months for the first year, and then, every 6 months until April 20, 2016. Imaging, adverse events, and the compliance of all patients were monitored during the follow-up period using our clinical databases.
Endpoints
The primary aim was OS. The secondary aims were: (i) pattern of the first failure; (ii) locoregional recurrence-free survival (LRRFS); (iii) distant metastasis-free survival (DMFS); and (iv) toxicity according to the CTCAE v4.0. OS was defined as the time between the date of diagnosis and the date of death or the date of the last follow-up for censored patients. The LRRFS and DMFS were defined as the time between the date of the post-operation and the date of the locoregional recurrence and/or distant metastases or the last follow-up for censored patients. To prevent immortal time bias, all patients needed to receive a minimum of 2 cycles of POCT and must have been alive for at least 1 month after surgery [31]. All toxicities were assessed in a multidisciplinary setting. Locoregional failure was defined as tumor regrowth in the hilar, mediastinal, or supraclavicular lymph nodes or at the bronchial margin of resection, as visualized by computed tomography or PET-CT scanning. Recurrences beyond these sites were deemed distant metastases. In addition, PET-CT scanning was employed to assist with differentiating radiation-related changes with recurrence and/or metastasis.
Statistical analysis
The χ2 test or Fisher’s exact test was performed for qualitative data. OS, LRRFS, and DMFS curves were estimated by using the Kaplan–Meier technique and compared by the stratified log-rank test. Uni- and multi-variate analyses were performed using a Cox regression model. Data were analyzed using Intercooled Stata, version 8.2 for Windows (Stata Corporation, College station, Texas, USA), with a p value of < 0.05 considered significant.
Abbreviations
PORT: postoperative radiotherapy; NSCLC: non-small cell lung cancer; OS: overall survival; LRRFS: locoregional recurrence-free survival; DMFS: distant metastasis-free survival; POCT: postoperative chemotherapy; NCCN: national comprehensive cancer network; ECE: extracapsular extension; LRR: locoregional recurrence; KPS: karnofsky performance score; MLN: mediastinal lymph node; EGFR-TKIs: epidermal growth factor tyrosine kinase inhibitors; MRI: magnetic resonance imaging; PET: positron emission tomography; 3D-CRT: three-dimensional conformal radiotherapy; IMRT: intensity-modulated radiotherapy; VMAT: volumetric modulated arc therapy; CTV: clinical target volume; PTV: planning target volume; HR: hazard ratio; IAEA: international atomic energy agency; ENI: elective nodal irradiation; ACR: The American college of radiology; CTCAE: common terminology criteria for adverse events.
Author contributions
Conception and design: Mao-Bin Meng.
Administrative support: Nicholas G. Zaorsky, Yang-Yang Shi, Wei Wang, and Bo Jiang.
Provision of study materials or patients: Huan-Huan Wang, Lei Deng, Qing-Lian Wen, Chun-Ze Zhang, Bai-Lin Zhang, Jie Chen, Xian-Liang Zeng, Yao-Li Cui, Hai-Ling Hou, Jun Wang, Qing-Song Pang, Lu-Jun Zhao, Zhi-Yong Yuan and Ping Wang
Collection and assembly of data: Mao-Bin Meng, Huan-Huan Wang, Lei Deng, Qing-Lian Wen and Chun-Ze Zhang.
Data analysis and interpretation: Mao-Bin Meng, Huan-Huan Wang, Lei Deng, Qing-Lian Wen, Chun-Ze Zhang, and Nicholas G. Zaorsky.
Manuscript writing: Mao-Bin Meng, Lei Deng, Huan-Huan Wang, Nicholas G. Zaorsky, and Yang-Yang Shi.
Final approval of manuscript: Mao-Bin Meng, Huan-Huan Wang, Lei Deng, Qing-Lian Wen, Chun-Ze Zhang, Nicholas G. Zaorsky, Bai-Lin Zhang, Jie Chen, Xian-Liang Zeng, Yao-Li Cui, Yang-Yang Shi, Hai-Ling Hou, Wei Wang, Bo Jiang, Jun Wang, Qing-Song Pang, Lu-Jun Zhao, Zhi-Yong Yuan and Ping Wang.
ACKNOWLEDGMENTS
We are indebted to Dr. Yue Hu at Department of Oncology, Affiliated Hospital of Southwest Medical University who provided the assistances for this study. We also thank the anonymous referee for his/her very helpful comments, which remarkably improved the quality of this paper.
CONFLICTS OF INTEREST
We have no conflicts of interests.
FUNDING
This work was supported by the National Natural Science Foundation of China (No. 81201754). No benefits in any form have been or will be received from a commercial party directly or indirectly related to the subject of this article.
REFERENCES
1. NCCN Clinical Practice Guidelines in Non-small cell lung cancer (Version 2. 2016). Available at www.nccn.org.
2. Lally BE, Zelterman D, Colasanto JM, Haffty BG, Detterbeck FC, Wilson LD. Postoperative radiotherapy for stage II or III non-small cell lung cancer using the surveillance, epidemiology, and end results database. J Clin Oncol. 2006; 24: 2998-3006.
3. Mikell JL, Gillespie TW, Hall WA, Nickleach DC, Liu Y, Lipscomb J, Ramalingam SS, Rajpara RS, Force SD, Fernandez FG, Owonikoko TK, Pillai RN, Khuri FR, et al. Postoperative radiotherapy is associated with better survival in non-small cell lung cancer with involved N2 lymph nodes: results of an analysis of National Cancer Data Base. J Thoracic Oncol. 2015; 10: 462-471.
4. Corso CD, Rutter CE, Wilson LD, Kim AW, Decker RH, Husain ZA. Re-evaluation of the role of postoperative radiotherapy and the impact of radiation dose for non-small-cell lung cancer using the National Cancer Database. J Thoracic Oncol. 2015; 10: 148-155.
5. Dai H, Hui Z, Ji W, Liang J, Lu J, Ou G, Zhou Z, Feng Q, Xiao Z, Chen D, Zhang H, Yin W, He J, Wang L. Postoperative radiotherapy for resected pathological stage IIIA-N2 non-small cell lung cancer: a retrospective study of 221 cases from a single institution. Oncologist. 2011; 16: 641-650.
6. Zou B, Xu Y, Li T, Li W, Tang B, Zhou L, Li L, Liu Y, Zhu J, Huang M, Wang J, Ren L, Gong Y, et al. A multicenter retrospective analysis of survival outcome following postoperative chemoradiotherapy in non-small-cell lung cancer patients with N2 nodal disease. Int J Radiat Oncol Biol Phys. 2010; 77: 321-328.
7. Bonner JA, Spencer SA. Postoperative radiotherapy in non-small-cell lung cancer warrants further exploration in the era of adjuvant chemotherapy and conformal radiotherapy. J Clin Oncol. 2006; 24: 2978-2980.
8. Kepka L, Socha J, Rucinska M, Wasilewska-Tesluk E, Komosinska K. Sequencing postoperative radiotherapy and adjuvant chemotherapy in non-small cell lung cancer: unanswered questions on the not evidence-based approach. J Thorac Dis. 2016; 8: 1381-1385.
9. Auperin A, Le Pechoux C, Pignon JP, Koning C, Jeremic B, Clamon G, Einhorn L, Ball D, Trovo MG, Groen HJ, Bonner JA, Le Chevalier T, Arriagada R. Meta-Analysis of Cisplatin/carboplatin based Concomitant Chemotherapy in non-small cell Lung Cancer (MAC3-LC) Group. Concomitant radio-chemotherapy based on platin compounds in patients with locally advanced non-small cell lung cancer (NSCLC): a meta-analysis of individual data from 1764 patients. Ann Oncol. 2006; 17: 473-483.
10. Auperin A, Le Pechoux C, Rolland E, Curran WJ, Furuse K, Fournel P, Belderbos J, Clamon G, Ulutin HC, Paulus R, Yamanaka T, Bozonnat MC, Uitterhoeve A, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010; 28: 2181-2190.
11. Bradley JD, Paulus R, Graham MW, Ettinger DS, Johnstone DW, Pilepich MV, Machtay M, Komaki R, Atkins J, Curran WJ. Radiation Therapy Oncology Group. Phase II trial of postoperative adjuvant paclitaxel/carboplatin and thoracic radiotherapy in resected stage II and IIIA non-small-cell lung cancer: promising long-term results of the Radiation Therapy Oncology Group-RTOG 9705. J Clin Oncol. 2005; 23: 3480-3487.
12. Feigenberg SJ, Hanlon AL, Langer C, Goldberg M, Nicolaou N, Millenson M, Coia LR, Lanciano R, Movsas B. A phase II study of concurrent carboplatin and paclitaxel and thoracic radiotherapy for completely resected stage II and IIIA non-small cell lung cancer. J Thorac Oncol. 2007; 2: 287-292.
13. Shen WY, Ji J, Zuo Y, Pu J, Xu Y, Zong CD, Tao GZ, Chen XF, Ji FZ, Zhou XL, Han JH, Wang CS, et al. Comparison of efficacy for postoperative chemotherapy and concurrent radiochemotherapy in patients with IIIA-pN2 non-small cell lung cancer: an early closed randomized controlled trial. Radiother Oncol. 2014; 110: 120-125.
14. Keller SM, Adak S, Wagner H, Johnson DH. Mediastinal lymph node dissection improves survival in patients with stages II and IIIa non-small cell lung cancer. Eastern Cooperative Oncology Group. Ann Thorac Surg. 2000; 70: 358-365.
15. Belderbos JS, Kepka L, Spring Kong FM, Martel MK, Videtic GM, Jeremic B. Report from the International Atomic Energy Agency (IAEA) consultants' meeting on elective nodal irradiation in lung cancer: non-small-Cell lung cancer (NSCLC). Int J Radiat Oncol Biol Phys. 2008; 72: 335-342.
16. Kępka L, Bujko K, Bujko M, Matecka-Nowak M, Salata A, Janowski H, Rogowska D, Cieślak-Żerańska E, Komosińska K, Zawadzka A. Target volume for postoperative radiotherapy in non-small cell lung cancer: results from a prospective trial. Radiother Oncol. 2013; 108: 61-65.
17. Gopal RS, Dubey S, Rosenzweig KE, Chang JY, Decker R, Gewanter RM, Kong FM, Lally BE, Langer CJ, Lee HK, Movsas B. ACR Appropriateness Criteria® on Induction and Adjuvant Therapy for Stage N2 Non-Small-Cell Lung Cancer: expert panel on radiation oncology-lung. Int J Radiat Oncol Biol Phys. 2010; 78: 969-974.
18. Dautzenberg B, Chastang C, Arriagada R, Le Chevalier T, Belpomme D, Hurdebourcq M, Lebeau B, Fabre C, Charvolin P, Guérin RA. Adjuvant radiotherapy versus combined sequential chemotherapy followed by radiotherapy in the treatment of resected nonsmall cell lung carcinoma. A randomized trial of 267 patients. GETCB (Groupe d'Etude et de Traitement des Cancers Bronchiques). Cancer. 1995; 76: 779-786.
19. Lee HW, Noh OK, Oh YT, Choi JH, Chun M, Kim HI, Heo J, Ahn MS, Park SY, Park RW, Yoon D. Radiation therapy-first strategy after surgery with or without adjuvant chemotherapy in stage IIIA-N2 non-small cell lung cancer. Int J Radiat Oncol Biol Phys. 2016; 94: 621-627.
20. Robinson CG, Patel AP, Bradley JD, DeWees T, Waqar SN, Morgensztern D, Baggstrom MQ, Govindan R, Bell JM, Guthrie TJ, Colditz GA, Crabtree TD, Kreisel D, et al. Postoperative radiotherapy for pathologic N2 non-small-cell lung cancer treated with adjuvant chemotherapy: a review of the National Cancer Data Base. J Clin Oncol. 2015; 33: 870-876.
21. Pisters KM, Vallieres E, Crowley JJ, Franklin WA, Bunn PA Jr, Ginsberg RJ, Putnam JB Jr, Chansky K, Gandara D. Surgery with or without preoperative paclitaxel and carboplatin in early-stage non-small-cell lung cancer: Southwest Oncology Group Trial S9900, an intergroup, randomized, phase III trial. J Clin Oncol. 2010; 28: 1843-1849.
22. Scagliotti GV, Pastorino U, Vansteenkiste JF, Spaggiari L, Facciolo F, Orlowski TM, Maiorino L, Hetzel M, Leschinger M, Visseren-Grul C, Torri V. Randomized phase III study of surgery alone or surgery plus preoperative cisplatin and gemcitabine in stages IB to IIIA non-small-cell lung cancer. J Clin Oncol. 2012; 30: 172-178.
23. Felip E, Rosell R, Maestre JA, Rodriguez-Paniagua JM, Moran T, Astudillo J, Borro JM, González-Larriba JL, Torres A, Camps C, Guijarro R, Isla D, Aguiló R, et al. Preoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J Clin Oncol. 2010; 28: 3138-3145.
24. NSCLC Meta-analyses Collaborative Group, Arriagada R, Auperin A, Burdett S, Higgins JP, Johnson DH, Le Chevalier T, Le Pechoux C, Parmar MK, Pignon JP, Souhami RL, Stephens RJ, Stewart LA, et al. Adjuvant chemotherapy with or without postoperative radiotherapy in operable non-small cell lung cancer: two meta-analyses of individual patient data. Lancet. 2010; 375: 1267-1277.
25. Rodrigues G, Choy H, Bradley J, Rosenzweig KE, Bogart J, Curran WJ Jr, Gore E, Langer C, Louie AV, Lutz S, Machtay M, Puri V, Werner-Wasik M, Videtic GM. Definitive radiation therapy in locally advanced non-small cell lung cancer: executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based clinical practice guideline. Pract Radiat Oncol. 2015; 5: 141-148.
26. Rodrigues G, Choy H, Bradley J, Rosenzweig KE, Bogart J, Curran WJ Jr, Gore E, Langer C, Louie AV, Lutz S, Machtay M, Puri V, Werner-Wasik M, Videtic GM. Adjuvant radiation therapy in locally advanced non-small cell lung cancer: Executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based clinical practice guideline. Pract Radiat Oncol. 2015; 5: 149-155.
27. Bezjak A, Temin S, Franklin G, Giaccone G, Govindan R, Johnson ML, Rimner A, Schneider BJ, Strawn J, Azzoli CG. Definitive and adjuvant radiotherapy in locally advanced non-small-cell lung cancer: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation Oncology Evidence-Based Clinical Practice Guideline. J Clin Oncol. 2015; 33: 2100-2105.
28. Decker RH, Langer CJ, Rosenzweig KE, Chang JY, Gewanter RM, Ginsburg ME, Kong FM, Lally BE, Videtic GM, Movsas B. ACR Appropriateness Criteria® postoperative adjuvant therapy in non-small cell lung cancer. Am J Clin Oncol. 2011; 34: 534-544.
29. Feng W, Fu XL, Cai XW, Yang HJ, Wu KL, Fan M, Xiang JQ, Zhang YW, Chen HQ. Patterns of local-regional failure in completely resected stage IIIA (N2) non-small cell lung cancer cases: implications for postoperative radiation therapy clinical target volume design. Int J Radiat Oncol Biol Phys. 2014; 88: 1100-1107.
30. Feng W, Zhang Q, Fu XL, Cai XW, Zhu ZF, Yang HJ, Xiang JQ, Zhang YW, Chen HQ. The emerging outcome of postoperative radiotherapy for stage IIIA (N2) non-small cell lung cancer patients: based on the three-dimensional conformal radiotherapy technique and institutional standard clinical target volume. BMC Cancer. 2015; 15: 348.
31. Park HS, Gross CP, Makarov DV, Yu JB. Immortal time bias: a frequently unrecognized threat to validity in the evaluation of postoperative radiotherapy. Int J Radiat Oncol Biol Phys. 2012; 83: 1365-1373.