
INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common malignancy and the third leading cause of cancer-related death worldwide [1]. Due to recent advances in diagnosis and surgical technology, curative hepatectomy is now widely considered as the first choice of therapy for HCC with well liver functional reserve, especially early-stage HCC [2]. However, even with these advances, the long-term outcomes of HCC remain unsatisfactory due to the high postoperative recurrence [3]. Approximately 70% of HCC patients have a recurrence within the 5 years after curative hepatectomy [4].
Vascular invasion is generally considered as an important risk factor for the prognosis of HCC patients after curative hepatectomy [5]. Macrovascular invasion, which could be evaluated by macroscopic examination or preoperative imaging, is helpful to provide a basis for selecting rational therapy. However, microvascular invasion (MVI) is difficult to be used for evaluating the prognosis of HCC preoperatively because it is only confirmed after operation by histopathological diagnosis [6]. MVI, defined as the invasion of tumor cells in intrahepatic portal vein or hepatic vein branches, is the beginning of intrahepatic dissemination and metastasis in HCC [5]. The prevalence of MVI ranges from 15% to 57% in HCC specimens [7]. Although the formation mechanism of MVI is not clear, previous researches have identified MVI is associated with poor prognosis of HCC patients after hepatectomy [8, 9]. To our knowledge, MVI is more common in advanced HCC patients presented with large size (tumor size > 5 cm) and multiple lesions [10]. But there are few researches focused on the influence of MVI on the prognosis of early-stage HCC (solitary, tumor size ≤ 5 cm, without macrovascular invasion). In the present research, we aimed to investigate the prognostic outcomes and preoperative predictors of MVI in early-stage HCC patients after curative hepatectomy.
RESULTS
Clinicopathological characteristics and long-term survival
The baseline characteristics of all HCC patients were presented in Table 1. Overall, the median age was 55 years (range 22-87 years). Of 233 HCC patients, 185 patients (79.3%) were male and 48 patients (20.7%) were female respectively. Positive HBsAg and liver cirrhosis were presented in 183 patients (78.5%) and 159 patients (68.2%). The median preoperative ICG-R15 was 5.0% (range 0.5-31.5%). A total of 119 patients (51.1%) received anatomical liver resection and 114 patients (48.9%) received non-anatomical liver resection. The median tumor size was 3.5 cm (range 1.0-5.0 cm). Forty-five patients (19.3%) and 164 patients (70.4%) were diagnosed with well and moderate differentiated HCC, respectively. MVI was found in 87 patients (37.3%). The median follow-up time was 49 months (range 2-142 months). No deaths occurred in hospital. The 1-, 3-, and 5-year overall survival rates for the entire cohort were 91.4%, 73.7%, and 63.5%, respectively. The 1-, 3-, and 5-year recurrence-free survival rates for the entire cohort were 78.0%, 55.8%, and 39.2%, respectively.
Table 1: Clinicopathological characteristics of the overall cohort
Variable |
Overall cohort (n = 233) |
|---|---|
Age (years) a |
55 ± 12 |
Gender |
|
Male |
185 (79.3) |
Female |
48 (20.7) |
HBsAg |
|
Positive |
183 (78.5) |
Negative |
50 (21.5) |
Background liver |
|
Noncirrhosis |
74 (31.8) |
Cirrhosis |
159 (68.2) |
Child–Pugh grade |
|
A |
226 (97.0) |
B |
7 (3.0) |
BCLC staging |
|
0 |
27 (11.6) |
A |
206 (88.4) |
ICG-R15 b |
5.0 (0.5-31.5) |
ALT (U/L) b |
35.5 (7.5-617.1) |
AST (U/L) b |
32.8 (14.5-285.5) |
TB (umol/L) b |
15.9 (3.6-47.7) |
DB (umol/L) b |
4.6 (1.3-27.6) |
GGT (U/L) b |
40.0 (15.3-683.5) |
AKP (U/L) b |
77.5 (32.8-534.6) |
Albumin (g/L) a |
42.2 ± 4.1 |
INR b |
1.1 (0.9-1.8) |
Platelets (109/L) a |
135 ± 53 |
AFP (ng/mL) b |
66.8 (0.7-62593.0) |
Types of resection |
|
Anatomical |
119 (51.1) |
Non-anatomical |
114 (48.9) |
Operation time (min) b |
210 (75-410) |
Blood loss (mL) b |
400 (50-1500) |
Transfusion |
|
Yes |
42 (18.0) |
No |
191 (82.0) |
Tumor size (cm) b |
3.5 (1.0-5.0) |
Tumor differentiation |
|
Well |
45 (19.3) |
Moderate |
164 (70.4) |
Poor |
24 (10.3) |
Microvascular invasion |
|
Yes |
87 (37.3) |
No |
146 (62.7) |
Parenthesis indicates percentage unless indicated.
a median (range); b mean ± standard deviation. AFP, alpha-fetoprotein; AKP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TB, total bilirubin; DB, direct bilirubin; GGT, gamma glutamyl transpeptidase; INR, international normalized ratio.
Univariate and multivariate analysis of prognostic risk factors for the entire cohort
In univariate analysis, Child–Pugh grade, ICG-R15, BCLC staging, tumor size, type of resection and MVI significantly influenced the overall survival rate (Table 2). Additionally, the level of GGT, blood loss, type of resection and MVI significantly influenced the recurrence-free survival rate (Table 3). Cox multivariate regression analysis identified ICG-R15 (HR = 1.081, 95% CI 1.033-1.132, P = 0.001), BCLC staging (HR = 10.244, 95% CI 1.414-74.248, P = 0.021) and MVI (HR = 1.783, 95% CI 1.061-2.997, P = 0.029) as independent risk factors for the overall survival rate. While type of resection (HR = 1.444, 95% CI 1.049-1.988, P = 0.024) and MVI (HR = 1.670, 95% CI 1.212-2.302, P = 0.002) were independent risk factors for the recurrence-free survival rate.
Table 2: Univariate and multivariate analysis of risk factors for overall survival rate
Variable |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
HR (95%CI) |
P-value |
HR (95%CI) |
P-value |
|
Age |
1.010 (0.991-1.029) |
0.303 |
||
Gender (male vs. female) |
1.111 (0.637-1.938) |
0.712 |
||
HBsAg (negative vs. positive) |
0.917 (0.561-1.499) |
0.729 |
||
Background liver (noncirrhosis vs. cirrhosis) |
0.938 (0.585-1.504) |
0.789 |
||
Child–Pugh (B vs. A) |
3.087 (1.248-7.637) |
0.015 |
||
ICG-R15 |
1.084 (1.035-1.135) |
0.001 |
1.081 (1.033-1.132) |
0.001 |
BCLC (A vs. 0) |
4.572 (1.444-14.473) |
0.010 |
10.244 (1.414-74.248) |
0.021 |
ALT |
0.999 (0.995-1.004) |
0.772 |
||
AST |
1.000 (0.996-1.005) |
0.824 |
||
TB |
1.013 (0.994-1.033) |
0.186 |
||
DB |
1.034 (0.975-1.096) |
0.264 |
||
AKP |
1.003 (0.999-1.006) |
0.154 |
||
GGT |
1.002 (1.000-1.004) |
0.084 |
||
Albumin |
0.974 (0.925-1.026) |
0.320 |
||
INR |
4.299 (0.764-24.191) |
0.098 |
||
Platelet |
0.998 (0.994-1.001) |
0.246 |
||
AFP |
1.000 (1.000-1.000) |
0.342 |
||
Tumor size |
1.230 (1.073-1.411) |
0.003 |
||
Operation time |
1.001 (0.999-1.004) |
0.253 |
||
Blood loss |
1.000 (1.000-1.001) |
0.068 |
||
Transfusion (yes vs. no) |
0.808 (0.632-1.034) |
0.090 |
||
Types of resection (non-anatomical vs. anatomical) |
1.619(1.056-2.481) |
0.027 |
||
Tumor differentiation (moderate/poor vs. well) |
0.815 (0.617-1.077) |
0.150 |
||
MVI (yes vs. no) |
1.938 (1.271-2.954) |
0.002 |
1.783 (1.061-2.997) |
0.029 |
AFP, alpha-fetoprotein; AKP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TB, total bilirubin; DB, direct bilirubin; GGT, gamma glutamyl transpeptidase; INR, international normalized ratio.
Table 3: Univariate and multivariate analysis of risk factors for recurrence-free survival rate
Variable |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
HR (95%CI) |
P-value |
HR (95%CI) |
P-value |
|
Age |
1.009 (0.995-1.024) |
0.218 |
||
Gender (male vs. female) |
0.892 (0.604-1.318) |
0.566 |
||
HBsAg (negative vs. positive) |
1.119 (0.754-1.662) |
0.576 |
||
Background liver (noncirrhosis vs. cirrhosis) |
1.038 (0.732-1.473) |
0.833 |
||
Child–Pugh (B vs. A) |
0.582 (0.257-1.319) |
0.195 |
||
ICG-R15 |
1.125 (0.974-1.182) |
0.216 |
||
BCLC (A vs. 0) |
1.473 (0.850-2.553) |
0.168 |
||
ALT |
1.001 (0.999-1.003) |
0.193 |
||
AST |
1.005 (1.003-1.008) |
0.034 |
||
Total bilirubin |
1.003 (0.987-1.020) |
0.693 |
||
Direct bilirubin |
1.016 (0.969-1.064) |
0.514 |
||
AKP |
1.002 (0.999-1.004) |
0.241 |
||
GGT |
1.004 (1.001-1.006) |
0.002 |
||
Albumin |
0.968 (0.930-1.006) |
0.101 |
||
INR |
1.000 (0.208-4.800) |
0.998 |
||
Platelet |
1.000 (0.997-1.003) |
0.986 |
||
AFP |
1.000 (1.000-1.000) |
0.447 |
||
Tumor size |
1.095 (0.987-1.214) |
0.087 |
||
Operation time |
1.001 (1.000-1.003) |
0.116 |
||
Blood loss |
1.000 (1.000-1.001) |
0.032 |
||
Transfusion (yes vs. no) |
0.918 (0.755-1.117) |
0.393 |
||
Types of resection (NAR vs. AR) |
1.408 (1.023-1.937) |
0.006 |
1.444 (1.049-1.988) |
0.024 |
Tumor differentiation (moderate/poor vs. well) |
0.879 (0.718-1.076) |
0.210 |
||
MVI (yes vs. no) |
1.661 (1.206-2.228) |
0.001 |
1.670 (1.212-2.302) |
0.002 |
AFP, alpha-fetoprotein; AKP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TB, total bilirubin; DB, direct bilirubin; GGT, gamma glutamyl transpeptidase; INR, international normalized ratio.
Comparisons of long-term survival according to MVI
In HCC patients with MVI (n = 87), the 1-, 3-, and 5-year overall survival rates were 86.2%, 67.1%, and 50.1%, respectively. Correspondingly, the 1-, 3-, and 5-year recurrence-free survival rates were 72.4%, 47.8%, and 26.9%, respectively. In HCC patients without MVI (n = 146), the 1-, 3-, and 5-year overall survival rates were 94.5%, 77.7%, and 72.0%, respectively. Correspondingly, the 1-, 3-, and 5-year recurrence-free survival rates were 81.4%, 60.6%, and 47.0%, respectively. Kaplan-Meier analysis showed the overall survival and recurrence-free survival rates in patients with MVI were significantly poorer than that in patients without MVI (P = 0.002 and P = 0.001) (Figure 1). In the subgroup analysis according to type of resection, anatomical resection obviously improved the overall survival and recurrence-free survival rates in patients with MVI compared with non-anatomical resection (P = 0.017 and P = 0.009). No significant difference was observed between the two types of resection in patients without MVI (P = 0.380 and P = 0.482) (Figure 2).
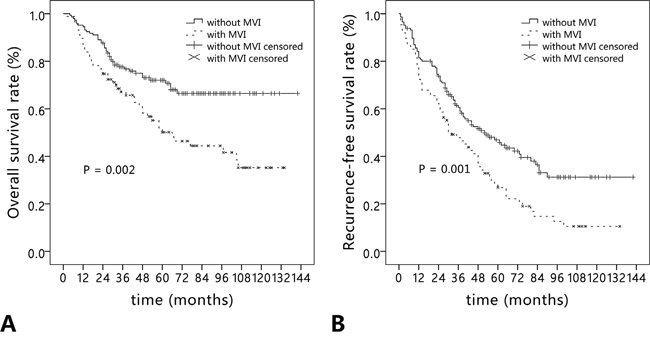
Figure 1: Long-term outcomes in hepatocellular carcinoma patients with (n = 87) and without microvascular invasion (n = 146). (A) Overall survival; (B) recurrence-free survival.
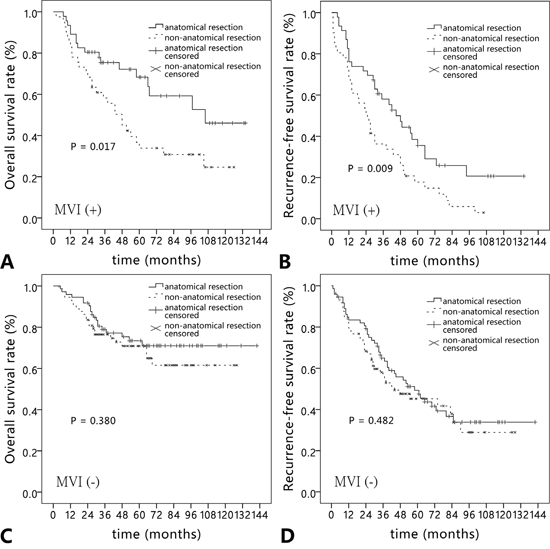
Figure 2: Comparison of (A, C) overall survival rate and (B, D) recurrence-free survival rate in hepatocellular carcinoma patients with and without microvascular invasion according to types of liver resection (anatomical resection vs. non-anatomical resection).
The recurrence patterns of HCC patients with and without MVI
Table 4 summarizes the recurrence patterns of HCC patients with and without MVI. The recurrence rate (79.3%) in patients with MVI was higher than that (56.8%) in patients without MVI (P < 0.001). Compared with patients without MVI, the median time to recurrence in patients with MVI was remarkably shorter (32.0 vs. 52.0 months, P = 0.001). Although there were no significant differences in the intrahepatic recurrence, extrahepatic recurrence and numbers of recurrence between patients with and without MVI, the marginal recurrence was significantly higher in patients with MVI (P = 0.017). On the contrary, the recurrence in contralateral hemiliver was significantly lower in patients with MVI (P = 0.028).
Table 4: The recurrence patterns of hepatocellular carcinoma patients with and without microvascular invasion
MVI (+) (n=87) |
MVI (-) (n=146) |
P-value |
|
|---|---|---|---|
Recurrence |
69 (79.3) |
83 (56.8) |
< 0.001 |
Time to recurrence (months) median (95% CI) |
32.0 (19.9-41.1) |
52.0 (35.1-68.9) |
0.001 |
Site of recurrence |
|||
Intrahepatic |
64 / 69 (92.8) |
79 / 83 (95.2) |
0.775 |
Surgical margin |
21 / 69 (30.4) |
11 / 83 (13.3) |
0.017 |
Ipsilateral hemiliver |
28 / 69 (40.6) |
35 / 83 (42.3) |
0.974 |
Contralateral hemiliver |
15 / 69 (21.7) |
33 / 83 (39.8) |
0.028 |
Extrahepatic |
5 / 69 (7.2) |
4 / 83 (4.8) |
0.775 |
Number of recurrence |
|||
Solitary |
43 / 69 (62.3) |
58 / 83 (69.9) |
0.418 |
Multiple |
26 / 69 (37.7) |
25 / 83 (30.1) |
Predictive value of preoperative clinical factors for MVI
Preoperative clinical factors were performed to predict MVI (Table 5). The significant predictors (P < 0.1) inunivariate analysis were entered into the multivariate logistic regression model to identify the valuable independent predictors for MVI. GGT > 53U/L (OR = 2.360, 95% CI 1.287-4.325, P = 0.005), AFP > 200 ng/ml (OR = 2.544, 95% CI 1.399-4.628, P = 0.002) and tumor size > 3.5cm (OR = 2.938, 95% CI 1.585-5.447, P = 0.001) were independent predictors for MVI.
Table 5: Predictors for microvascular invasion of hepatocellular carcinoma on univariate analysis
Variable |
MVI (+) (n = 87) |
MVI (-) (n = 146) |
Univariate analysis |
|
|---|---|---|---|---|
OR (95%CI) |
P-value |
|||
Age |
||||
> 60 vs. ≤ 60 years |
25 / 62 |
51 / 95 |
0.751 (0.422–1.336) |
0.330 |
Gender |
||||
Male vs. female |
67 / 20 |
118 / 28 |
0.795 (0.416–1.519) |
0.487 |
HBsAg |
||||
Positive vs. negative |
72 / 15 |
111 / 35 |
1.514 (0.772–2.969) |
0.228 |
Child–Pugh grade |
||||
B vs. A |
3 / 84 |
4 / 142 |
0.789 (0.172-3.610) |
0.760 |
ALT |
||||
> 50 vs. ≤ 50 U/L |
25 / 62 |
42 / 104 |
0.998 (0.555-1.795) |
0.996 |
AST |
||||
> 50 vs. ≤ 50 U/L |
19 / 68 |
29 / 117 |
1.127 (0.588-2.162) |
0.718 |
TB |
||||
> 17.1 vs. ≤ 17.1 μmol/L |
41 / 46 |
50 / 96 |
1.711 (0.995-2.943) |
0.052 |
DB |
||||
> 7.0 vs. ≤ 7.0 μmol/L |
13 / 74 |
16 / 130 |
1.427 (0.651-3.131) |
0.375 |
GGT |
||||
> 53 vs. ≤ 53 U/L |
44 / 43 |
42 / 104 |
2.534 (1.458-4.402) |
0.001 |
Albumin |
||||
> 35 vs. ≤ 35 g/L |
83 / 4 |
138 / 8 |
1.203 (0.351-4.118) |
0.769 |
INR |
||||
> 1.1 vs. ≤ 1.1 |
24 / 63 |
27 / 119 |
1.679 (0.895-3.149) |
0.106 |
Platelets |
||||
> 100 vs. ≤ 100 ×109/L |
59 / 28 |
113 / 33 |
0.615 (0.340-1.114) |
0.109 |
AFP |
||||
> 200 vs. ≤ 200 ng/mL |
46 / 41 |
44 / 102 |
2.601 (1.501-4.507) |
0.001 |
Tumor size |
||||
> 3.5 vs. ≤ 3.5 cm |
65 / 22 |
68 / 78 |
3.389 (1.893-6.069) |
< 0.001 |
AFP, alpha-fetoprotein; AKP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TB, total bilirubin; DB, direct bilirubin; GGT, gamma glutamyl transpeptidase; INR, international normalized ratio.
We assigned a prediction score to each independent predictor for MVI according to the β coefficient in multivariate logistic regression model (the β coefficient of each predictor divided by 0.859) (Table 6). The total prediction score of each HCC patient was the sum of the score of each independent predictor, which ranged from 0 to 3 points. Based on ROC curve analysis of the prediction score, the area under receiver operating characteristic (AUROC) was 0.723 (95% CI, 0.655-0.790) in the entire cohort. The optimal cut-off score was 2 on the basis of maximum Youden index value. The sensitivity, specificity, PPV and NPV were 69.0% (95% CI, 58.1-78.5%), 70.6% (95% CI, 62.4-77.8%), 58.3% (95% CI, 48.1-67.9%) and 79.2% (95% CI, 71.2-85.8%) (Figure 3).
Table 6: Predictors for microvascular invasion of hepatocellular carcinoma on multivariate logistic regression analysis
Variable |
β |
OR (95%CI) |
P |
Score |
|---|---|---|---|---|
GGT > 53U/L |
0.859 |
2.360 (1.287-4.325) |
0.005 |
1 |
AFP > 200 ng/mL |
0.934 |
2.544 (1.399-4.628) |
0.002 |
1 |
Tumor size > 3.5 cm |
1.078 |
2.938 (1.585-5.447) |
0.001 |
1 |
OR, odds ratio; CI, confidence interval; β, partial regression coefficient.
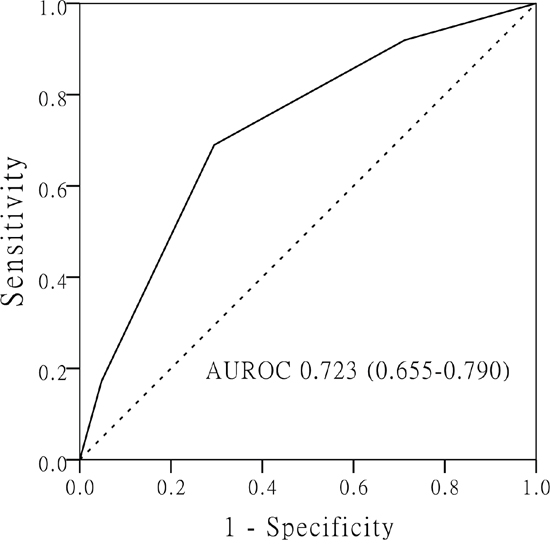
Figure 3: The receiver operating characteristic (ROC) curve of prediction scoring model for microvascular invasion based on the three independent predictors (tumor size > 3.5 cm, AFP > 200 ng/mL and GGT > 53 U/L).
DISSCUSION
Early-stage HCC patients are the main candidates for curative treatments and supposed to have relatively good long-term outcomes [11, 12]. However, even with the progress in surgery techniques, the overall survial and recurrence rates are unsatisfactory. Nathan et al reported the median survival time and 5-year survival rate of early-stage HCC patients were only 45 months and 39% [11]. Cai et al investigated that the 5-year overall survival and recurrence-free survival rates were 77.7% and 59.9% in small HCC patients (maximum tumor size ≤ 3 cm) after resection [3]. Tumor size, vascular invasion, histological grade and treatment strategy have been considered to be independent risk factors influencing the prognosis of early-stage HCC [12–14]. In the present research, we identified a total of 233 early-stage HCC patients (solitary tumor, tumor size ≤ 5 cm and no macrovascular invasion). The 5-year overall survival and recurrence-free survival rates were 63.5% and 39.2%, respectively. Cox multivariate regression analysis showed that ICG-R15, BCLC staging and MVI were independent risk factors for the overall survival rate. While type of resection and MVI were independent risk factors for the recurrence-free survival rate.
A systematic review including 20 observational studies revealed MVI was closely related to poor prognosis of HCC patients [15]. However, the presence of MVI was reported to be associated with tumor size [9, 16]. Ahn et al found that patients with tumor size > 5 cm had higher risk of MVI than those with tumor size ≤ 5 cm [17]. In the previous study of our group, the prevalence of MVI was 55.7% in solitary HCC patients with tumor size > 5 cm [18]. In patients with advanced HCC, it is generally accepted that MVI is the main cause for metastasis and recurrence after hepatectomy [10, 19]. But there is controversial about the significance of MVI on the prognosis of early-stage HCC. Shindoh et al suggested small HCC (≤ 2 cm) was related to a good prognosis without regard to the presence of MVI [20]. Nevertheless, Du et al claimed MVI is a poorer prognostic predictor for small HCC (tumor size ≤ 3 cm) [21]. In our research, the prevalence of MVI was 37.3% in early-stage HCC. The 1-, 3-, 5-year overall survival and recurrence-free survival rates of patients with MVI were significantly poorer than those of patients without MVI. MVI was the only independent risk factor for both the overall survival and recurrence-free survival rates in this study.
We investigated the recurrence patterns of HCC patients with and without MVI in the present research. Though there were no significant differences in the intrahepatic, extrahepatic and numbers of recurrence, the median time to recurrence in patients with MVI after hepatectomy was significantly shorter than that in patients without MVI. Compared with patients without MVI, the marginal recurrence in patients with MVI was higher. These results suggested that HCC patients with MVI were prone to early recurrence and marginal recurrence after hepatectomy. MVI was defined as the invasion of tumor cells in a portal vein, hepatic vein, or a large capsular vessel of the surrounding hepatic tissue [15]. The presence of MVI has been considered to be the first-step of hematogenous metastasis in HCC, which is related to aggressiveness of HCC. Even in the early stage of HCC patients, the invasive tumor cells could spread through invading the intrahepatic vascular system, especially the portal vein and its branches. Futhermore, Shi et al reported MVI usually were found in the normal liver tissue within 2 cm away from the tumor edge [22]. If the extent of liver resection is not adequate, the residual MVI near the surgical margin may be the important cause for intrahepatic early recurrence and marginal recurrence in HCC patients.
The important pathological characteristic of MVI is that tumor cells spread through portal venous and hepatic venous branches. Therefore anatomical resection based on Couinaud’s segment is recommended for HCC patients with MVI. Compared with non-anatomical resection, anatomical resection could remove the portal tributaries bearing the tumor completely, which is more effective to eradicate intrahepatic MVI to reduce the recurrence rate. In our series, anatomical resection significantly improved the overall survival and recurrence-free survival rates in the early-stage HCC patients with MVI. Similar results were not found in patients without MVI. In a multi-center retrospective study from Italy and China, Cucchetti et al investigated that anatomical resection significantly reduced the recurernce rate in 153 early HCC patients with MVI [23]. Shindoh et al aslo revealed the prognostic superiority of anatomical resection was confirmed only in patients with histopathological evidence of MVI [24]. These results supported our conclusion. Thus, if patients has an adequate future liver remnant, anatomical resection should be first taken into consideration in HCC patients with MVI.
Unfortunately, MVI is only confirmed after hepatectomy by histopathological diagnosis, which limits its widespread use in the choice of surgical procedure. Therefore, it is valuable to identify the predictors for MVI preoperatively. By retrospectively investigating preoperative characteristics of patients, We identified three independent predictors for MVI: tumor size > 3.5cm, AFP > 200 ng/ml and GGT > 53U/L. Tumor size is considered as the most valuable predictor for MVI in HCC patients [10, 25]. The risk of MVI continues to rise with the increase of tumor size. Our research showed tumor size was still a strong predictor for MVI, even in solitary HCC patients with tumor size ≤ 5 cm. The significant cut-off value of tumor size was identifed as 3.5 cm. The elevated level of AFP have been reported to be associated with MVI [26, 27]. Schlichtemeier et al investigated 125 HCC patients who underwent liver resection, and showed that a serum AFP level ≥ 400 ng/ml was independently associated with MVI [28]. The cut-off value of AFP was higher than ours because only early-stage HCC patients were included in our research. Circulating tumor cells is considered as one possible mechanism of MVI [29, 30]. Jin et al reported that the high AFP mRNA level of circulating tumor cells was a valuable predictor for vascular invasion of HCC after hepatectomy [31]. The results might explain the relation between high level of AFP and MVI. Aberrant expression of GGT has been found in HCC and plays an important role in tumor formation and metastasis [32]. A previous research by Ju et al demonstrated the high level of GGT was related to vascular invasion, advanced tumor and tumor size [33]. Zhao et al suggested serum GGT > 130 U/L was an independent predictive factor for MVI in multinodular HCC [10]. While in the present research, our results showed GGT > 53U/L was strongly associated with MVI for early-stage HCC. Based on these three predictors, we built up a prediction scoring system for the risk of MVI. According to the ROC curve, the prevalence of MVI in HCC patients with predictive score ≥ 2 was 58.3%, which was obviously lower than those with predictive score < 2 (20.8%).
The present research has some limitations. First, it is a single-center and retrospective research. Therefore, it was subject to potential bias that might preclude definite conclusions to be drawn. The prognostic value and preoperative predictors of MVI require prospective and multicenter validations. Second, thin-slice contrast-enhanced CT and gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid (Gd-EOB-DTPA) MRI have been reported to be helpful for predicting MVI preoperatively [29, 34]. Because these imaging techniques were widely applied in recent years, detailed imaging imformation in early patients of our cohort were not included in the present research.
In conclusion, our study indicated that MVI was an independent risk factor for the overall survival and recurrence-free survival rates of solitary HCC patients with tumor size ≤ 5 cm after hepatectomy. For HCC patients with MVI, anatomical resection could significantly improve the overall survival and recurrence-free survival rates. Based on tumor size > 3.5cm, AFP > 200 ng/ml and GGT > 53U/L, the prediction scoring model are valuable for the preoperative prediction of MVI.
PATIENTS AND METHODS
Study population
A total of 307 consecutive HCC patients (size ≤ 5 cm) underwent curative hepatectomy in the Department of Hepatobiliary Surgery at Nanjing Drum Tower Hospital between January 2004 and December 2013. Patients met the following criteria were enrolled in the present study: (1) no evidence of macroscopic vascular invasion, (2) solitary tumor, (3) Child-Pugh A/B, (4) R0 tumor resection, (5) no any preoperative anticancer treatments, (6) no history of other cancers, (7) complete clinical and pathological data. Eventually, a total of 233 early-stage HCC patients were enrolled. The present study was carried out in accordance with the Declaration of Helsinki revised in 1983. The retrospective study was approved and exempted from the requirement to obtain informed consent by the Committee on Medical Ethics of Nanjing Drum Tower Hospital.
Clinical and pathological characteristics
Preoperative clinical data and operation information were retrospectively reviewed from our HCC database, including age, gender, serum hepatitis B surface antigen (HBsAg), Child-Pugh grade, ICG-R15, BCLC staging, serum alanine aminotransferase (ALT), serum aspartate aminotransferase (AST), gamma glutamyl transpeptidase (GGT), alkaline phosphatase (AKP), serum total bilirubin (TB), direct bilirubin (DB), serum albumin (ALB), alpha-fetoprotein (AFP), platelet count (PLT), international normalized ratio (INR), type of operation, operation time, blood loss and blood transfusions (Table 1). Anatomical resection was charactered as any type of complete excision at least one segment based on Couinaud’s classification, including segmentectomy, sectoriectomy and hemihepatectomy. Non-anatomical resection was defined as local resection or enucleation without regard to the Couinaud’s segmental and sectoral structure. MVI was evaluated based on all the liver slices of resected specimens. MVI was defined as the invasion of tumor cells in a portal vein, hepatic vein, or a large capsular vessel of the surrounding hepatic tissue, partially or totally lined by endothelial cells that were visible only on microscopy [19]. The extent of tumor differentiation was evaluated as well, moderate and poor according to Edmondson-Steiner grading system [35].
Patient follow-up
Patients were followed up systematically by the levels of AFP, liver function and abdominal ultrasonography every 2 month after discharge. Contrast-enhanced computed tomography (CT) or enhanced magnetic resonance imaging (MRI) was performed every 4 months. Recurrence should be confirmed by at least two imaging modalities, such as CT and MRI. The time to recurrence, site of recurrence and number of recurrence were recorded. The site of recurrence was divided into intrahepatic and extrahepatic recurrence. Intrahepatic recurrence was divided into recurrence at surgical margin, ipsilateral hemiliver and contralateral hemiliver. The number of recurrence was divided into solitary and multiple. If the recurrence was detected, further treatment such as second hepatectomy, local ablation, transcatheter arterial chemoembolization (TACE), or other therapeutic modalities, including molecular targeted therapy would be undertaken. Overall survival was defined as the time interval between the operation and the date of the death. Recurrence-free survival was defined as the period after the operation when a recurrence could be detected. Follow-up data were collected until December 31, 2015.
Statistical analysis
Categorical data were compared by the chi-square test or Fisher’s exact test. The survival analyses were performed according to the Kaplan-Meier survival curves and compared by the log-rank test. Prognostic risk factors were analyzed by univariate and multivariate Cox proportional hazards models. The predictors for MVI were identified by univariate logistic regression analysis. Subsequently, the significant predictors (P < 0.10) were evaluated by multivariate logistic regression analysis to identify the valuable independent predictors for MVI. The assigning score of each predictor was determined according to the β coefficient in multivariate logistic regression model [36]. The cut-off value of predictive score was calculated by receiver operating characteristic (ROC) curve. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. For all tests, P < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 21.0 (SPSS Inc., Chicago, IL).
ACKNOWLEDGMENTS
We thank the whole multiple disciplinary team (MDT) in hepatobiliary cancer for their guidance in this study.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
GRANT SUPPORT
This work was supported by the National Natural Science Foundation of China (Grant No. 81470866).
REFERENCES
1. Bosch FX, Ribes J, Diaz M, Cleries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004; 127:S5-S16.
2. Pessaux P. Techniques and innovations in liver surgery. Hepatobiliary Surg Nutr. 2016; 5:277-278.
3. Cai MY, Wang FW, Li CP, Yan LX, Chen JW, Luo RZ, Yun JP, Zeng YX, Xie D. Prognostic factors affecting postoperative survival of patients with solitary small hepatocellular carcinoma. Chin J Cancer. 2016; 35:80.
4. Colecchia A, Schiumerini R, Cucchetti A, Cescon M, Taddia M, Marasco G, Festi D. Prognostic factors for hepatocellular carcinoma recurrence. World J Gastroenterol. 2014; 20:5935-5950.
5. Roayaie S, Blume IN, Thung SN, Guido M, Fiel MI, Hiotis S, Labow DM, Llovet JM, Schwartz ME. A system of classifying microvascular invasion to predict outcome after resection in patients with hepatocellular carcinoma. Gastroenterology. 2009; 137:850-855.
6. Lim KC, Chow PK, Allen JC, Chia GS, Lim M, Cheow PC, Chung AY, Ooi LL, Tan SB. Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Ann Surg. 2011; 254:108-113.
7. Lei Z, Li J, Wu D, Xia Y, Wang Q, Si A, Wang K, Wan X, Lau WY, Wu M, Shen F. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis B virus-related hepatocellular carcinoma within the Milan criteria. JAMA Surg. 2016; 151:356-363.
8. Kluger MD, Salceda JA, Laurent A, Tayar C, Duvoux C, Decaens T, Luciani A, Van Nhieu JT, Azoulay D, Cherqui D. Liver resection for hepatocellular carcinoma in 313 Western patients: tumor biology and underlying liver rather than tumor size drive prognosis. J Hepatol. 2015; 62:1131-1140.
9. Unal E, Idilman IS, Akata D, Ozmen MN, Karcaaltincaba M. Microvascular invasion in hepatocellular carcinoma. Diagn Interv Radiol. 2016; 22:125-132.
10. Zhao WC, Fan LF, Yang N, Zhang HB, Chen BD, Yang GS. Preoperative predictors of microvascular invasion in multinodular hepatocellular carcinoma. Eur J Surg Oncol. 2013; 39:858-864.
11. Nathan H, Schulick RD, Choti MA, Pawlik TM. Predictors of survival after resection of early hepatocellular carcinoma. Ann Surg. 2009; 249:799-805.
12. Suh SW, Lee KW, Lee JM, You T, Choi Y, Kim H, Lee HW, Lee JM, Yi NJ, Suh KS. Prediction of aggressiveness in early-stage hepatocellular carcinoma for selection of surgical resection. J Hepatol. 2014; 60:1219-1224.
13. Tomimaru Y, Eguchi H, Marubashi S, Wada H, Kobayashi S, Tanemura M, Umeshita K, Doki Y, Mori M, Nagano H. Equivalent outcomes after anatomical and non-anatomical resection of small hepatocellular carcinoma in patients with preserved liver function. Dig Dis Sci. 2012; 57:1942-1948.
14. Hsieh CH, Wei CK, Yin WY, Chang CM, Tsai SJ, Wang LY, Chiou WY, Lee MS, Lin HY, Hung SK. Vascular invasion affects survival in early hepatocellular carcinoma. Mol Clin Oncol. 2015; 3:252-256.
15. Rodriguez-Peralvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK. A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol. 2013; 20:325-339.
16. Hirokawa F, Hayashi M, Miyamoto Y, Asakuma M, Shimizu T, Komeda K, Inoue Y, Uchiyama K. Outcomes and predictors of microvascular invasion of solitary hepatocellular carcinoma. Hepatol Res. 2014; 44:846-853.
17. Ahn SY, Lee JM, Joo I, Lee ES, Lee SJ, Cheon GJ, Han JK, Choi BI. Prediction of microvascular invasion of hepatocellular carcinoma using gadoxetic acid-enhanced MR and (18)F-FDG PET/CT. Abdom Imaging. 2015; 40:843-851.
18. Zhao H, Chen C, Fu X, Yan X, Jia W, Mao L, Jin H, Qiu Y. Prognostic value of a novel risk classification of microvascular invasion in patients with hepatocellular carcinoma after resection. Oncotarget. 2017; 8:5474-5486. doi: 10.18632/oncotarget.12547.
19. Iguchi T, Shirabe K, Aishima S, Wang H, Fujita N, Ninomiya M, Yamashita Y, Ikegami T, Uchiyama H, Yoshizumi T, Oda Y, Maehara Y. New pathologic stratification of microvascular invasion in hepatocellular carcinoma: predicting prognosis after living-donor liver transplantation. Transplantation. 2015; 99:1236-1242.
20. Shindoh J, Andreou A, Aloia TA, Zimmitti G, Lauwers GY, Laurent A, Nagorney DM, Belghiti J, Cherqui D, Poon RT, Kokudo N, Vauthey JN. Microvascular invasion does not predict long-term survival in hepatocellular carcinoma up to 2 cm: reappraisal of the staging system for solitary tumors. Ann Surg Oncol. 2013; 20:1223-1229.
21. Du M, Chen L, Zhao J, Tian F, Zeng H, Tan Y, Sun H, Zhou J, Ji Y. Microvascular invasion (MVI) is a poorer prognostic predictor for small hepatocellular carcinoma. BMC Cancer. 2014; 14:38.
22. Shi M, Zhang CQ, Zhang YQ, Liang XM, Li JQ. Micrometastases of solitary hepatocellular carcinoma and appropriate resection margin. World J Surg. 2004; 28:376-381.
23. Cucchetti A, Qiao GL, Cescon M, Li J, Xia Y, Ercolani G, Shen F, Pinna AD. Anatomic versus nonanatomic resection in cirrhotic patients with early hepatocellular carcinoma. Surgery. 2014; 155:512-521.
24. Shindoh J, Hasegawa K, Inoue Y, Ishizawa T, Nagata R, Aoki T, Sakamoto Y, Sugawara Y, Makuuchi M, Kokudo N. Risk factors of post-operative recurrence and adequate surgical approach to improve long-term outcomes of hepatocellular carcinoma. HPB (Oxford). 2013; 15:31-39.
25. Pawlik TM, Delman KA, Vauthey JN, Nagorney DM, Ng IO, Ikai I, Yamaoka Y, Belghiti J, Lauwers GY, Poon RT, Abdalla EK. Tumor size predicts vascular invasion and histologic grade: implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transpl. 2005; 11:1086-1092.
26. McHugh PP, Gilbert J, Vera S, Koch A, Ranjan D, Gedaly R. Alpha-fetoprotein and tumour size are associated with microvascular invasion in explanted livers of patients undergoing transplantation with hepatocellular carcinoma. HPB (Oxford). 2010; 12:56-61.
27. You Z, Chen LP, Ye H. Predictors of microvascular invasion in patients with solitary small hepatitis B related hepatocellular carcinoma. Pak J Med Sci. 2014; 30:331-334.
28. Schlichtemeier SM, Pang TC, Williams NE, Gill AJ, Smith RC, Samra JS, Lam VW, Hollands M, Richardson AJ, Pleass HC, Nozawa S, Albania M, Hugh TJ. A pre-operative clinical model to predict microvascular invasion and long-term outcome after resection of hepatocellular cancer: the Australian experience. Eur J Surg Oncol. 2016; 42:1576-1583.
29. Banerjee S, Wang DS, Kim HJ, Sirlin CB, Chan MG, Korn RL, Rutman AM, Siripongsakun S, Lu D, Imanbayev G, Kuo MD. A computed tomography radiogenomic biomarker predicts microvascular invasion and clinical outcomes in hepatocellular carcinoma. Hepatology. 2015; 62:792-800.
30. Chiba T, Kanai F, Iwama A, Yokosuka O. Circulating cancer stem cells: a novel prognostic predictor of hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2013; 2:4-6.
31. Jin J, Niu X, Zou L, Li L, Li S, Han J, Zhang P, Song J, Xiao F. AFP mRNA level in enriched circulating tumor cells from hepatocellular carcinoma patient blood samples is a pivotal predictive marker for metastasis. Cancer Lett. 2016; 378:33-37.
32. Carr BI, Pancoska P, Branch RA. Low alpha-fetoprotein hepatocellular carcinoma. J Gastroenterol Hepatol. 2010; 25:1543-1549.
33. Ju MJ, Qiu SJ, Fan J, Zhou J, Gao Q, Cai MY, Li YW, Tang ZY. Preoperative serum gamma-glutamyl transferase to alanine aminotransferase ratio is a convenient prognostic marker for Child-Pugh A hepatocellular carcinoma after operation. J Gastroenterol. 2009; 44:635-642.
34. Renzulli M, Brocchi S, Cucchetti A, Mazzotti F, Mosconi C, Sportoletti C, Brandi G, Pinna AD, Golfieri R. Can current preoperative imaging be used to detect microvascular invasion of hepatocellular carcinoma? Radiology. 2016; 279:432-442.
35. Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954; 7:462-503.
36. Sullivan LM, Massaro JM, D'Agostino RB Sr. Presentation of multivariate data for clinical use: the Framingham Study risk score functions. Stat Med. 2004; 23:1631-1660.