
INTRODUCTION
Non-small cell lung cancer (NSCLC) accounts for approximately 80% of lung cancer cases, the majority of which are already unresectable and metastatic at the time of initial diagnosis. Additionally, approximately 40% of patients with advanced NSCLC will present with or develop malignant pleural effusion (MPE) [1]. Pleurodesis is considered a standard procedure for treating MPE. However, this treatment has no effect on the tumor itself and only provides symptomatic relief. Chemical pleurodesis is associated with adverse events, such as fever, chest pain, and acute respiratory distress syndrome. Additionally, the process of intercostal tube insertion itself can cause complications, including hemorrhage, organ injury, and infection. Consequently, optimum strategies for managing recurrent effusions are currently unavailable [2].
Vascular endothelial growth factor (VEGF) is thought to play a principal role in MPE formation by increasing vascular and mesothelial permeability and capillary fluid leakage [3]. As bevacizumab, an anti-VEGF-A agent, was found to effectively control pleural effusion in clinical studies [4, 5], attention has focused on the use of VEGF axis inhibitors to treat patients with MPE. Ramucirumab, a human monoclonal antibody specific for VEGF receptor-2 (VEGFR-2), was recently approved for patients with advanced NSCLC [6]. Bevacizumab and ramucirumab mainly differ with respect to their drug target. Bevacizumab is an antagonist of the VEGF ligand, VEGF-A, whereas ramucirumab is an antagonist of VEGFR-2. However, it remains unclear which of these agents more effectively control MPE in a clinical setting. Herein, we report on a case of MPE that was refractory to ramucirumab plus docetaxel, but responsive to bevacizumab plus docetaxel combination therapy and review the literature.
CASE PRESENTATION
A 68-year-old Japanese man presented at our hospital with dyspnea. A computed tomography (CT) scan revealed right-sided pleural effusion and a pulmonary nodule. Radiographic and pathologic evaluations confirmed a diagnosis of advanced pulmonary adenocarcinoma with MPE (T1aN0M1a, Stage 4). Epidermal growth factor receptor mutation analysis and anaplastic lymphoma kinase fusion gene testing were negative. Carboplatin, paclitaxel, and bevacizumab (15 mg/kg) was administered as first-line chemotherapy, and after 4 cycles, a CT scan indicated the disappearance of the right-sided pleural effusion and a partial tumor response. Bevacizumab maintenance therapy was discontinued due to patient preference.
Three months after the final administration of first-line chemotherapy, progressive disease was detected as an increase in pleural effusion on a CT scan and pleural fluorodeoxyglucose uptake. Despite administering ramucirumab (10 mg/kg, Day 1) plus docetaxel (60 mg/m2, Day 1) as second-line chemotherapy, a CT scan revealed that, after 2 cycles, the pulmonary nodules were unchanged, but the pleural effusion had increased. Therefore, the MPE was considered progressive. Serum VEGF-A levels increased from 143.0 pg/mL before second-line chemotherapy to 511.0 pg/mL after second-line chemotherapy. This high level of serum VEGF-A was maintained after 2 treatment cycles.
Pleurodesis was not considered indispensable at this point, because the patient did not have severe symptoms of MPE after administration of ramucirumab plus docetaxel combination therapy. Subsequently, bevacizumab (15 mg/kg, Day 1) plus docetaxel (60 mg/m2, Day 1) was administered for progressive MPE. After 2 cycles, a CT scan revealed a reduction in the pleural effusion with the pulmonary nodule remaining stable. Moreover, the patient’s serum VEGF-A levels had decreased from 549.0 pg/mL before administration to <15.6 pg/mL on Day 3 of the first treatment course. A response was maintained for 4 months after the administration of bevacizumab plus docetaxel combination therapy and has continued to be maintained.
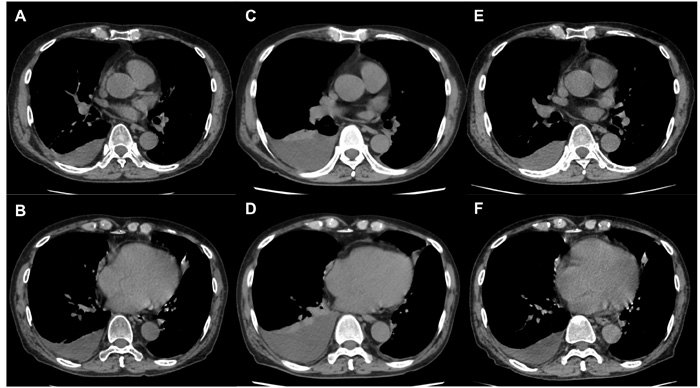
Figure 1: Changes in MPE with treatment. MPE A., B. at initiation of ramucirumab plus docetaxel and C., D. after 2 cycles of ramucirumab plus docetaxel; MPE increased and progressive disease was confirmed. MPE decreased after 2 cycles of bevacizumab plus docetaxel E., F.
DISCUSSION
The family of VEGF ligands comprises VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E, and placental growth factor. VEGF-A is important for vascular permeability and angiogenesis [7]. Its levels are significantly elevated in MPEs relative to pleural effusions associated with benign diseases [8]. Therefore, VEGF-A has been considered the most important VEGF ligand for MPE formation, and this has been supported by several clinical studies [4, 5] that have demonstrated the efficacy of bevacizumab, a VEGF-A inhibitor, for the treatment of MPE.
The family of VEGFRs includes VEGFR-1 (Flt-1), VEGFR-2 (KDR/Flk-1), and VEGFR-3 (Flt-4), among which VEGFR-2 was found to be essential for the induction of VEGF biological responses [7]. Notably, the REVEL trial [6] demonstrated that ramucirumab prolonged overall survival when administered in combination with docetaxel to patients with previously treated NSCLC. Although additional reports [9, 10] have demonstrated the importance of VEGFR-2 in MPE formation in vitro, the functions of the remaining VEGFRs have yet to be fully elucidated [7]. Thus far, it has been shown [11, 12] that VEGFR-1 is also upregulated in MPEs, and it is thought that VEGFR-1 may play a positive regulatory role in angiogenesis under certain conditions.
In the present case, bevacizumab plus docetaxel combination therapy was administered, although this is not considered a standard therapy. However, this therapy was proven to be associated with prolonged progression-free survival compared to docetaxel monotherapy in patients previously treated with bevacizumab-containing platinum-based doublet regimens [13]. Considering the findings of this trial [13], and previous efficacy data for bevacizumab in MPEs, we commenced treatment with this combination therapy in our patient.
In the present case, the MPE was refractory to ramucirumab plus docetaxel, but responsive to bevacizumab plus docetaxel combination therapy. Similar to previous reports [14, 15], our patient exhibited increased serum VEGF-A levels after ramucirumab therapy. We speculate that the inhibition of VEGFR-2 leads to elevated serum VEGF-A, which in turn binds to VEGFRs other than VEGFR-2. Increased MPE during ramucirumab therapy may be maintained via this mechanism. We believe that our report provides scope for improving treatment for MPEs, as well as, important clues to the mechanism(s) of association between VEGF and MPEs.
VEGF-A was not measured in the MPE in our case. Hsu et al. [16] examined serum and pleural effusion VEGF concentrations and reported a statistically significant correlation. Therefore, we believed serum VEGF would be a good surrogate for VEGF concentrations in the MPE in our case.
In conclusion, we demonstrate the efficacy of bevacizumab in a patient with ramucirumab refractory MPE. Although both agents inhibit the VEGF pathway, bevacizumab may be more effective for treating MPE. Further investigations are still warranted to determine the optimal VEGF-targeted agent for MPE.
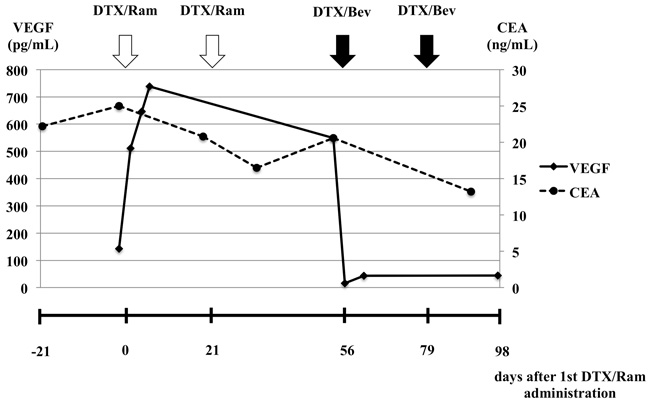
Figure 2: Changes in serum VEGF and carcinoembryonic antigen levels before and after ramucirumab plus docetaxel and bevacizumab plus docetaxel combination therapy.
Abbreviations
CT, computed tomography; MPE, malignant pleural effusion; NSCLC, non-small cell lung cancer; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor.
Conflicts of interest
The authors declare that there are no conflicts of interest.
REFERENCES
1. Porcel JM, Gasol A, Bielsa S, Civit C, Light RW, Salud A. Clinical features and survival of lung cancer patients with pleural effusions. Respirology. 2015; 20:654-659.
2. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ, BTS Pleural Disease Guideline Group. Management of a malignant pleural effusion: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010; 65: ii32-40.
3. Grove CS, Lee YC. Vascular endothelial growth factor: the key mediator in pleural effusion formation. Curr Opin Pulm Med. 2002; 8:294-301.
4. Usui K, Sugawara S, Nishitsuji M, Fujita Y, Inoue A, Mouri A, Watanabe H, Sakai H, Kinoshita I, Ohhara Y, Maemondo M, Kagamu H, Hagiwara K, et al. A phase II study of bevacizumab with carboplatin-pemetrexed in non-squamous non-small cell lung carcinoma patients with malignant pleural effusions: North East Japan Study Group Trial NEJ013A. Lung Cancer. 2016; 99:131-136.
5. Tamiya M, Tamiya A, Yamadori T, Nakao K, Asami K, Yasue T, Otsuka T, Shiroyama T, Morishita N, Suzuki H, Okamoto N, Okishio K, Kawaguchi T, et al. Phase2 study of bevacizumab with carboplatin-paclitaxel for non-small cell lung cancer with malignant pleural effusion. Med Oncol. 2013; 30:676.
6. Garon EB, Ciuleanu TE, Arrieta O, Prabhash K, Syrigos KN, Goksel T, Park K, Gorbunova V, Kowalyszyn RD, Pikiel J, Czyzewicz G, Orlov SV, Lewanski CR, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014; 384:665-673.
7. Hicklin DJ, Ellis LM. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J Clin Oncol. 2005; 23:1011-1027.
8. Jia L, Du Y, Li T, Lv Y, Wang Y, Zhang Y, Zhou X, Liu W. Differential expression of vascular endothelial growth factor-A, -C and -D for the diagnosis and prognosis of cancer patients with malignant effusions. Oncol Lett. 2015; 10:667-674.
9. Verheul HM, Hoekman K, Jorna AS, Smit EF, Pinedo HM. Targeting vascular endothelial growth factor blockade: ascites and pleural effusion formation. Oncologist. 2000; 5:45-50.
10. Yano S, Herbst RS, Shinohara H, Knighton B, Bucana CD, Killion JJ, Wood J, Fidler IJ. Treatment for malignant pleural effusion of human lung adenocarcinoma by inhibition of vascular endothelial growth factor receptor tyrosine kinase phosphorylation. Clin Cancer Res. 2000; 6:957-965.
11. Hiratsuka S, Maru Y, Okada A, Seiki M, Noda T, Shibuya M. Involvement of Flt-1 tyrosine kinase (vascular endothelial growth factor receptor-1) in pathological angiogenesis. Cancer Res. 2001; 61:1207-1213.
12. Hooper CE, Elvers KT, Welsh GI, Millar AB, Maskell NA. VEGF and sVEGFR-1 in malignant pleural effusions: association with survival and pleurodesis outcomes. Lung Cancer. 2012; 77:443-449.
13. Takeda M, Yamanaka T, Seto T, Hayashi H, Azuma K, Okada M, Sugawara S, Daga H, Hirashima T, Yonesaka K, Urata Y, Murakami H, Saito H, et al. Bevacizumab beyond disease progression after first-line treatment with bevacizumab plus chemotherapy in advanced nonsquamous non-small cell lung cancer (West Japan Oncology Group 5910L): An open-label, randomized, phase 2 trial. Cancer. 2016; 122:1050-1059.
14. Zhu AX, Finn RS, Mulcahy M, Gurtler J, Sun W, Schwartz JD, Dalal RP, Joshi A, Hozak RR, Xu Y, Ancukiewicz M, Jain RK, Nugent FW, et al. A phase II and biomarker study of ramucirumab, a human monoclonal antibody targeting the VEGF receptor-2, as first-line monotherapy in patients with advanced hepatocellular cancer. Clin Cancer Res. 2013; 19:6614-6623.
15. Chiorean EG, Hurwitz HI, Cohen RB, Schwartz JD, Dalal RP, Fox FE, Gao L, Sweeney CJ. Phase I study of every 2- or 3-week dosing of ramucirumab, a human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2 in patients with advanced solid tumors. Ann Oncol. 2015; 26:1230-1237.
16. Hsu IL, Su WC, Yan JJ, Chang JM, Lai WW. Angiogenetic biomarkers in non-small cell lung cancer with malignant pleural effusion: correlations with patient survival and pleural effusion control. Lung Cancer. 2009; 65:371-376.