
INTRODUCTION
First-line treatment using folinic acid, fluorouracil, and oxaliplatin (FOLFOX) or folinic acid, 5-fluorouracil, and irinotecan (FOLFIRI) combined with target therapy prolongs the overall survival (OS) of patients with metastatic colorectal cancer (mCRC) patients compared with dual chemotherapy, particularly when administered to patients without RAS or BRAF mutations [1–7]. A study that used a regression model to analyze the correlation between the percentages of patients treated with triplet chemotherapy and the outcomes, found that OS is prolonged [8]. However, this model was derived using the data of a single arm of a study of patients with mCRC who were administered chemotherapy as first-line treatment. Moreover, the dose intensities of chemotherapy and targeted therapy were not considered.
Randomized controlled trials (RCTs) compared the efficacy and toxicities of triple chemotherapy (folinic acid, 5-fluorouracil, oxaliplatin and irinotecan [FOLFOXIRI]) plus target therapy with those of triple or double chemotherapy (FOLFOX or FOLFIRI) plus target therapy [9–11]. The efficacies and toxicities of triple and double chemotherapy were compared as well. However, whether dose intensity is the most important prognostic factor is controversial. We asked therefore whether FOLFOXIRI plus target therapy administered as first-line treatment improves the prognosis of patients with mCRC and if there is a significant difference in efficacy between FOLFOXIRI and double chemotherapy plus target therapy?
RESULTS
The titles and abstracts of 248 studies were reviewed. After the initial screen, we performed a detailed assessment of potentially eligible papers and selected 11 papers and 2 abstracts of 10 randomized controlled trials (RCT) [1–7, 9–14] (Figure 1). FIRE3 study [15], PEAK study [16] and CALGB 80405 study [17] were not included because the regimens both in the experimental groups and the control groups were recognized as FOLFOX or FOLFIRI plus target therapy in our network meta-analysis. And the survival of these three studies were consistent with the studies included. Table 1 shows the characteristics of these 10 RCTs. The patients with mCRC (n = 2,506) were randomized into treatment vs control groups (Table 1). Methodological quality assessment was performed according to the latest guidelines in the Cochrane Handbook for Systematic Reviews of Interventions. The quality of each included study was high (Table 2).
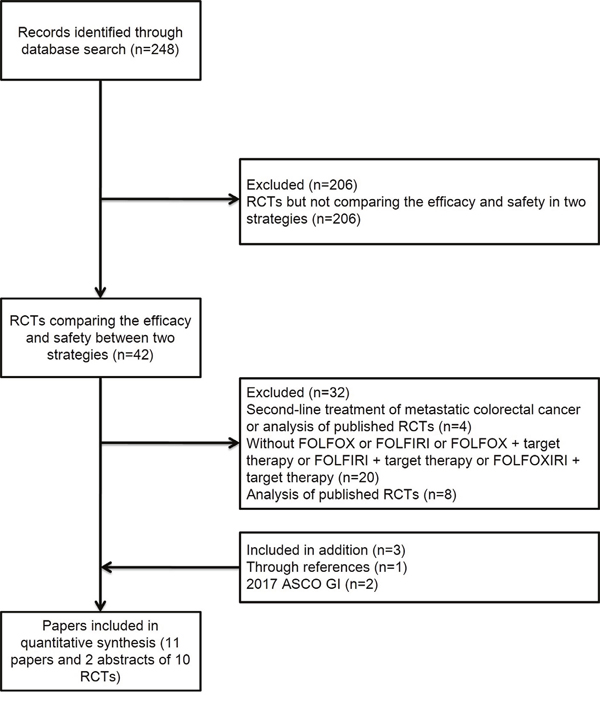
Figure 1: Literature search and selection of studies. Abbreviation: RCT, randomized controlled trial.
Table 1: Characteristics of the included randomized control trials
Study |
Study design |
Treatment schedule |
|---|---|---|
OPUS 2011, 2015 |
FOLFOX4+Cetux. |
Cetux.: initial dose 400 mg/m2 and 250 mg/m2/week thereafter, Q2W. |
|
FOLFOX4 |
FOLFOX4: oxaliplatin 85 mg/m2; folinic acid 200 mg/m2; 5-FU 400 mg/m2 IV bolus and 600 mg/m2 22-hour continuous infusion on days 1 and 2, Q2W. |
CRYSTAL 2011, 2015 |
FOLFIRI+Cetux. |
Cetux.: initial dose 400 mg/m2 and 250 mg/m2/week thereafter, followed after 1 hour by FOLFIRI, Q2W. |
|
FOLFIRI |
FOLFIRI: irinotecan 180 mg/m2, on day 1, infused over 30–90 minutes; leucovorin 200 mg/m2 L-form, or 400 mg/m2 racemic, infused over 2 hours; fluorouracil 400 mg/m2 IV bolus and 2400 mg/m2 46-hour continuous infusion, Q2W. |
PRIME 2010, 2013 |
FOLFOX4+Panit. |
Panit.: IV over 1 hour, 6 mg/kg on day 1 before FOLFOX4, Q2W |
|
FOLFOX4 |
FOLFOX4: oxaliplatin 85 mg/m2 IV infusion on day 1; leucovorin 200 mg/m2 IV infusion; fluorouracil 400 mg/m2 IV bolus and 600 mg/m2 22-hour continuous infusion on days 1 and 2, Q2W. |
TRIBE 2015 |
FOLFOXIRI+bevacizumab. |
Bevacizumab: 5 mg/kg, Q2W. |
|
FOLFIRI+bevacizumab. |
Bevacizumab: 5 mg/kg, Q2W. |
OLIVIA 2015 |
FOLFOXIRI+bevacizumab. |
Bevacizumab: 5 mg/kg, Q2W. |
|
mFOLFOX-6+bevacizumab. |
Bevacizumab: 5 mg/kg, Q2W. |
AVF2107 2009 |
IFL+bevacizumab. |
Bevacizumab |
|
IFL+placebo. |
Placebo |
GONO 2007 |
FOLFOXIRI |
Irinotecan 165 mg/m2 on day 1; Oxaliplatin 85 mg/m2 on day 1; Leucovorin 200 mg/m2 on day 1; 5-fluorouracil 3200 mg/m2 48-hour continuous infusion starting on day 1. Repeated every 2 weeks. |
|
FOLFIRI |
Irinotecan 180 mg/m2 on day 1; Leucovorin 100 mg/m2 on day 1 and day 2; 5-fluorouracil 400 mg/m2 bolus followed by 5-fluorouracil 600 mg/m2 22-hour continuous infusion on day 1 and day 2. Repeated every 2 weeks. |
HORG 2006 |
FOLFOXIRI |
CPT-11 at the dose of 150 mg/m2 as a 30 min IV infusion on day 1; LV was given at the dose of 200 mg/m2 as a 2 h IV infusion, followed by 5FU 400 mg/m2 as IV bolus, and then, 600 mg/m2 as a 22 h continuous IV infusion, on days 2 and 3; L-OHP was administered on day 2 at the dose of 65 mg/m2 as a 2 h IV infusion in parallel with LV but using different lines. |
|
FOLFIRI |
CPT-11 at the dose of 180 mg/m2 as a 30 min IV infusion on day 1; LV was given at the dose of 200 mg/m2 as a 2 h IV infusion, followed by 5FU 400 mg/m2 as IV bolus, and then, 600 mg/m2 as a 22 h continuous IV infusion, on days 1 and 2. |
STEAM 2017 |
FOLFOXIRI + bevacizumab |
Bevacizumab: 5 mg/kg Q2W. |
|
FOLFOX + bevacizumab |
Bevacizumab: 5 mg/kg Q2W. |
CHARTA 2017 |
FOLFOXIRI + bevacizumab |
Bevacizumab: 5 mg/kg, Q2W. |
|
FOLFOX + bevacizumab |
Bevacizumab: 5 mg/kg Q2W. |
Abbreviations: Q2W, every 2 weeks; IV, intravenous.
Table 2: Methodological quality of included RCTs
study |
Sequence generation |
Allocation sequence concealment |
Blinding of participants and personnel |
Blinding of outcome assessment |
Incomplete outcome data |
Selective outcome reporting |
Other risk of bias |
|---|---|---|---|---|---|---|---|
OPUS 2011 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
OPUS 2015 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
CRYSTAL 2011 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
CRYSTAL 2015 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
PRIME 2010 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
PRIME 2013 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
TRIBE 2015 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
OLIVIA 2015 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
AVF2107 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
GONO 2007 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
HORG 2006 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
STEAM 2017 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
CHARTA 2017 |
adequate |
adequate |
Not report |
yes |
no |
no |
no |
ITT, intention to treat. Unclear reporting of allocation was considered inadequate.
The network of the comparisons is shown in Figure 2. Four regimens from 10 trails were included in the network. Four studies compared double chemotherapy plus target therapy with double chemotherapy. Four studies compared double chemotherapy plus target therapy with triple chemotherapy plus target therapy. Two studies compared triple chemotherapy with double chemotherapy.
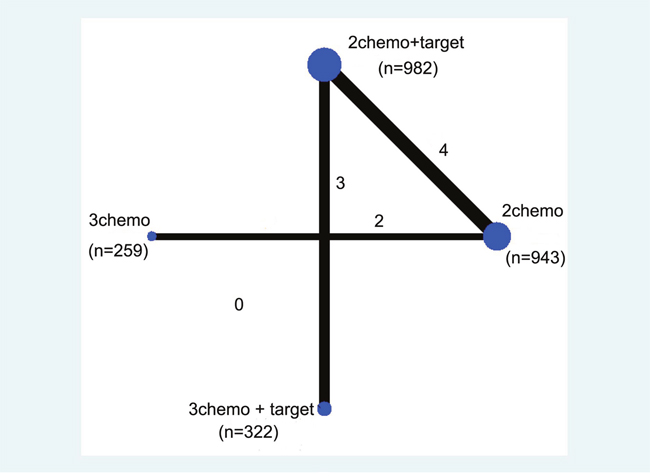
Figure 2: Network of the comparisons included in the network meta-analysis. The sizes of the nodes are proportional to the numbers of patients (in parentheses) randomized to receive the treatment. The width of the lines is proportional to the number of trials (next to the line) comparing the connected treatments.
The pooled HRs of PFS of patients administered an individual regimen compared with FOLFOX or FOLFIRI plus target therapy in the network meta-analysis shows that the PFS of patients administered FOLFOXIRI plus target therapy was longer compared with that of FOLFOX or FOLFIRI plus target therapy (HR 0.71, 95% CI 0.59–0.86) (Figure 3A). There was no difference between FOLFOXIRI and FOLFOX or FOLFIRI plus target therapy (HR 1.23, 95% CI 0.87–1.72) (Figure 3A). Pooled HRs of OS of patients administered individual regimens compared with FOLFOX or FOLFIRI plus target therapy in the network meta-analysis shows that the OS of patients for FOLFOXIRI plus target therapy was longer compared with that of FOLFOX or FOLFIRI plus target therapy (HR 0.81, 95% CI 0.69–0.94) (Figure 3B). There was no difference between FOLFOXIRI and FOLFOX or FOLFIRI plus target therapy (HR 0.94, 95% CI 0.66–1.35) (Figure 3B).
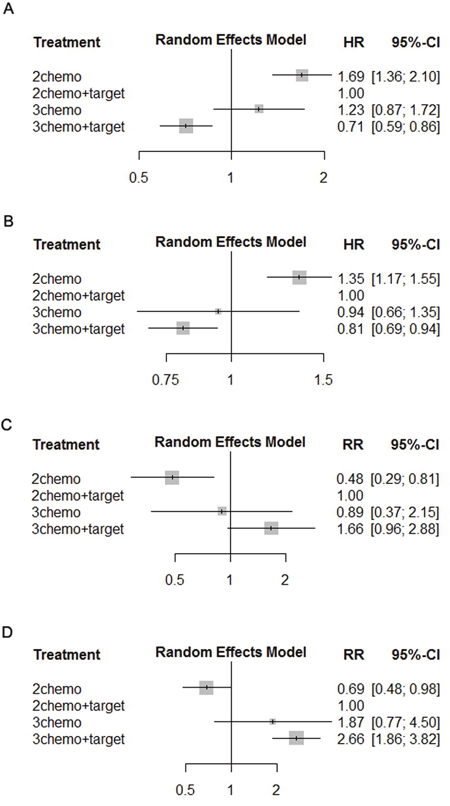
Figure 3: Pooled HRs of PFS (A) and OS (B), pooled RRs of ORR (C), and R0-resection rate (D) determined using network meta-analysis. Abbreviations: HR, hazard ratio, PFS, progression-free survival; OS, overall survival; ORR, objective response rate.
The pooled RRs of ORR of patients administered individual regimens compared with FOLFOX or FOLFIRI plus target therapy in the network meta-analysis shows that the ORR of patients administered FOLFOXIRI plus target therapy was higher compared with that of FOLFOX or FOLFIRI plus target therapy (RR 1.66, 95% CI 0.96–2.88) (Figure 3C). There was no difference between FOLFOXIRI and FOLFOX or FOLFIRI plus target therapy (RR 0.89, 95% CI 0.37–2.15) (Figure 3C). The pooled RRs of the R0 resection rate of patients administered individual regimens compared with FOLFOX or FOLFIRI plus target therapy in the network meta-analysis shows that the R0 resection rate of patients administered FOLFOXIRI plus target therapy was higher compared with that of FOLFOX or FOLFIRI plus target therapy (RR 2.66, 95% CI 1.86–3.82) (Figure 3D). There was no significant difference between FOLFOXIRI and FOLFOX or FOLFIRI plus target therapy (RR 1.87, 95% CI 0.77–4.50) (Figure 3D).
The pooled RRs of toxicities of patients administered individual regimens compared with double chemotherapy plus targeted therapy in the network meta-analysis shows no increase in toxicities between FOLFOXIRI and FOLFOX or FOLFIRI plus target therapy (Figure 4). Further, FOLFOXIRI plus target therapy did not increase toxicities compared with FOLFOX or FOLFIRI plus target therapy (Figure 4B).
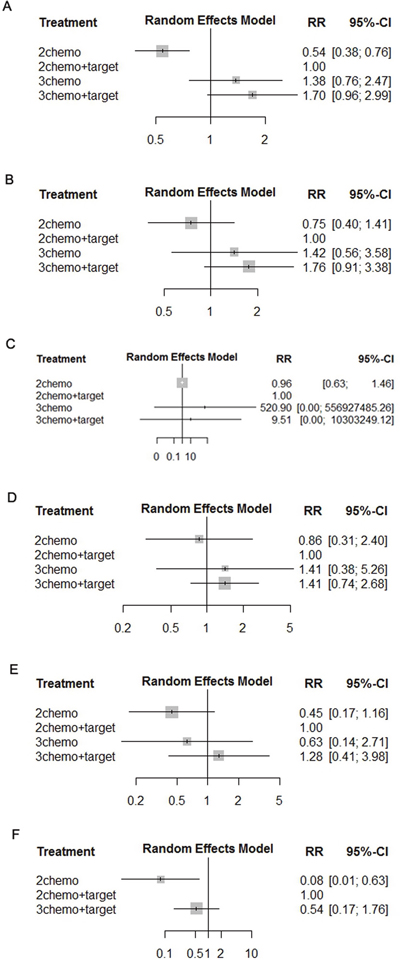
Figure 4: Pooled RRs of toxicities determined using network meta-analysis. Diarrhea (A), Neutropenia (B), Neurologic toxicities (C), Febrile neutropenia (D), Fatigue (E), and Venous thrombosis (F).
We also performed the subgroup analysis for the patients with RAS/BRAF mutations and the patients without RAS mutations. For the patients with RAS mutations (n = 454), FOLFOXIRI plus Bevacizumab (Bev) significantly prolonged the PFS compared with FOLFOX or FOLFIRI plus Bev (HR 0.75, 95% CI 0.62–0.92). For the patients with BRAF mutations (n = 54), FOLFOXIRI plus Bev prolonged the PFS compared with FOLFOX or FOLFIRI plus Bev, but the difference was not significant (HR 0.64, 95% CI 0.36–1.15). For the patients without RAS mutations (n = 292), FOLFOXIRI plus Bev significantly prolonged the PFS compared with FOLFOX or FOLFIRI plus Bev (HR 0.73, 95% CI 0.57–0.94) (Supplementary Figure 1).
DISCUSSION
The results of this network meta-analysis show that first-line treatment using FOLFOXIRI plus target therapy prolonged PFS and OS and improved the ORR and R0 resection rate of patients with mCRC without a significant increase in toxicities. The patients with RAS/BRAF mutations could benefit from FOLFOXIRI plus Bev compared with FOLFOX or FOLFIRI plus Bev. Triple chemotherapy used in some studies was as effective as double chemotherapy plus target therapy and was associated with acceptable toxicities. Therefore, patients who cannot afford target therapy may have the option of choosing FOLFOXIRI as their first-line treatment.
This study is the first to our knowledge to conduct a network meta-analysis that ranks the efficacy and toxicities of intensive therapy strategies. NCCN 2017 version 2 guidelines recommend a choice of FOLFOX, FOLFIRI, CapeOx, infusion 5-FU/LV or capecitabine, or FOLFOXIRI, with or without targeted agents as initial therapy for mCRC patients appropriate for intensive therapy. But which one is the best choice was still controversial. The 2016 ESMO guidelines recommend that the goal for treating patients with potentially resectable or nonresectable mCRC who have the ability to withstand intensive therapy should achieve shrinkage of clinically relevant tumors to the maximum extent possible [18]. Further, the 2016 ESMO guidelines state that for patients who are candidates for therapies that maximize tumor shrinkage or for those with BRAF mutations, the cytotoxic triplet FOLFOXIRI plus Bev is an option. But the grade of this evidence was IIB [18].
Considering the absence of sufficient evidence, the application of intensive therapeutic strategies for treating patients with mCRC is limited. The results of our network meta-analysis suggest that patients with mCRC may benefit from FOLFOXIRI plus target therapy as first-line treatment. Therefore, FOLFOXIRI or FOLFOXIRI plus Bev may be a more suitable option for patients able to withstand intensive treatment. Moreover, the analysis of toxicities presented here show that FOLFOXIRI did not significantly increase toxicities compared with those associated with FOLFOX or FOLFIRI plus target therapy. And FOLFOXIRI plus target therapy also did not increase toxicities compared with those associated with FOLFOX or FOLFIRI plus target therapy, except for neutropenia.
The number of patients with mCRC who can afford target treatment is limited, and the efficacies and toxicities of triple chemotherapy and double chemotherapy plus target chemotherapy were not determined by RCTs. The results of our indirect comparison using network meta-analysis suggest that patients treated with FOLFOXIRI achieved similar PFS, OS, ORR, and R0 resection rates compared with patients treated with double chemotherapy plus target chemotherapy. Therefore, patients with mCRC who cannot afford target therapy may choose FOLFOXIRI as their first-line treatment.
This study did not analyze patients’ ages or their performance status because only some certain criteria for the patients administered FOLFOXIRI with or without target therapy were referred in the included studies but not consistent. For example, in the STEAM study [11], patients aged 18–75 years were required to meet Eastern Cooperative Oncology Group (ECOG) performance status ≤1. The inclusion criteria of the OLIVIA [10], TRIBE [9], and GONO [12] studies were age ≥18 years and ECOG performance status ≤1; age 18–70 years, ECOG performance status ≤2; and age 71–75-years, ECOG performance status = 0; respectively. In the HORG study [13], which did not impose an age limit, 56% of patients treated with FOLFOXIRI were aged ≥65 years.
Our network meta-analysis has certain limitations. First, target therapy has been used as first-line treatment for mCRC since 2004. Thus, target therapy was not administered to study and control groups in the GONO study [12], which may have biased the present data. Second, testing for RAS and BRAF mutations is not currently required for treatment using Bev, and the HRs of all patients without data for RAS mutational status included in the studies were administered bevacizumab but not an anti-EGFR antibody. Third, the number of eligible studies was small. Therefore, future RCTs must include larger numbers of subjects.
We conclude that FOLFOXIRI plus target therapy administered as first-line treatment is the best choice for patients with mCRC, because it is not significantly associated with increased toxicities. The patients with RAS/BRAF mutations could benefit from FOLFOXIRI plus Bev. Further, FOLFOXIRI is as effective as double chemotherapy plus target therapy.
MATERIALS AND METHODS
Search strategy
This network meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19]. We searched the abstracts of RCTs to evaluate the efficacies and toxicities of intensive therapies administered as first-line treatment of patients with mCRC. The resources searched included PubMed, the Cochrane Collaboration Central Register of Controlled Clinical Trials, Cochrane Systematic Reviews, ClinicalTrials.gov, and the databases of the European Society for Medical Oncology and American Society of Clinical. The search included articles dated from the inception of these resources until March 31, 2017 (the list of search terms is included in the Supplementary Data). We reviewed the bibliographies of these reports as well as related reviews to identify articles. These papers were subjected to manual searches. Our network meta-analysis included studies that compared different intensive therapies.
Quality assessment and data extraction
Two investigators (Z-MY, Y-P) independently reviewed the entire text of eligible studies. Information was extracted and inserted into an electronic database that included patient characteristics, inclusion and exclusion criteria, treatment protocols, and outcomes. Any disagreement between reviewers was discussed with the other coauthors until a consensus was reached.
Data synthesis and analysis
Outcomes of this study included progression-free survival (PFS), OS, ORR, and the R0 resection rate. Random-effects models were used to account for the heterogeneity among studies. Standard meta-analysis was performed using Stata 12.1 (StataCorp, College Station, TX, USA). Network meta-analysis was performed using a netmeta package developed according to the theories of a classical frequentist setting included in the R language framework.
CONFLICTS OF INTEREST
There is no conflicts of interest.
FUNDING
This work was supported by the Educational Commission of Liaoning Province of China (No. 20060973), and the Science and Technology Planning Project of Liaoning Province of China (No. 2007225009-1, 2011404013-9, 2011225019, 2013225079), and the National Natural Science Foundation of China (No. 81372532), and the Science and Technology Planning Project of Shenyang (No. F15-139-9-27).
REFERENCES
1. Van Cutsem E, Köhne CH, Láng I, Folprecht G, Nowacki MP, Cascinu S, Shchepotin I, Maurel J, Cunningham D, Tejpar S, Schlichting M, Zubel A, Celik I, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol. 2011; 29:2011–19.
2. Van Cutsem E, Lenz HJ, Köhne CH, Heinemann V, Tejpar S, Melezínek I, Beier F, Stroh C, Rougier P, van Krieken JH, Ciardiello F. Fluorouracil, leucovorin, and irinotecan plus cetuximab treatment and RAS mutations in colorectal cancer. J Clin Oncol. 2015; 33:692–700.
3. Bokemeyer C, Bondarenko I, Hartmann JT, de Braud F, Schuch G, Zubel A, Celik I, Schlichting M, Koralewski P. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: the OPUS study. Ann Oncol. 2011; 22:1535–46.
4. Bokemeyer C, Köhne CH, Ciardiello F, Lenz HJ, Heinemann V, Klinkhardt U, Beier F, Duecker K, van Krieken JH, Tejpar S. FOLFOX4 plus cetuximab treatment and RAS mutations in colorectal cancer. Eur J Cancer. 2015; 51:1243–52.
5. Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham D, Jassem J, Rivera F, Kocákova I, Ruff P, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol. 2010; 28:4697–705.
6. Douillard JY, Oliner KS, Siena S, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham D, Jassem J, Rivera F, Kocákova I, Ruff P, et al. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med. 2013; 369:1023–34.
7. Hurwitz HI, Yi J, Ince W, Novotny WF, Rosen O. The clinical benefit of bevacizumab in metastatic colorectal cancer is independent of K-ras mutation status: analysis of a phase III study of bevacizumab with chemotherapy in previously untreated metastatic colorectal cancer. Oncologist. 2009; 14:22–28.
8. Grothey A, Sargent D. Overall survival of patients with advanced colorectal cancer correlates with availability of fluorouracil, irinotecan, and oxaliplatin regardless of whether doublet or single-agent therapy is used first line. J Clin Oncol. 2005; 23:9441–42.
9. Cremolini C, Loupakis F, Antoniotti C, Lupi C, Sensi E, Lonardi S, Mezi S, Tomasello G, Ronzoni M, Zaniboni A, Tonini G, Carlomagno C, Allegrini G, et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015; 16:1306–15.
10. Gruenberger T, Bridgewater J, Chau I, García Alfonso P, Rivoire M, Mudan S, Lasserre S, Hermann F, Waterkamp D, Adam R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: the OLIVIA multinational randomised phase II trial. Ann Oncol. 2015; 26:702–08.
11. Bendell JC, Tan BR, Reeves JA, Xiong H, Somer BG, Lenz HJ, Hochster HS, Scappaticci F, Sommer N, Bann-mo D, Hurwitz H. Overall response rate (ORR) in STEAM, a randomized, open-label, phase 2 trial of sequential and concurrent FOLFOXIRI-bevacizumab (BEV) vs FOLFOX-BEV for the first-line (1L) treatment (tx) of patients (pts) with metastatic colorectal cancer (mCRC). J Clin Oncol. 2016; 34:4_suppl, 492-492.
12. Falcone A, Ricci S, Brunetti I, Pfanner E, Allegrini G, Barbara C, Crinò L, Benedetti G, Evangelista W, Fanchini L, Cortesi E, Picone V, Vitello S, et al, and Gruppo Oncologico Nord Ovest. Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: the Gruppo Oncologico Nord Ovest. J Clin Oncol. 2007; 25:1670–76.
13. Souglakos J, Androulakis N, Syrigos K, Polyzos A, Ziras N, Athanasiadis A, Kakolyris S, Tsousis S, Kouroussis C, Vamvakas L, Kalykaki A, Samonis G, Mavroudis D, Georgoulias V. FOLFOXIRI (folinic acid, 5-fluorouracil, oxaliplatin and irinotecan) vs FOLFIRI (folinic acid, 5-fluorouracil and irinotecan) as first-line treatment in metastatic colorectal cancer (MCC): a multicentre randomised phase III trial from the Hellenic Oncology Research Group (HORG). Br J Cancer. 2006; 94:798–805.
14. Schmoll HJ, Garlipp B, Junghanss C, Leithaeuser M, Vogel A, Schaefers M, Kaiser U, Hoeffkes HG, Florschütz A, Rüssel J, Kanzler S, Edelmann T, Forstbauer H, et al. CHARTA: FOLFOX bevacizumab /- irinotecan in advanced colorectal cancer (CRC)—Final results of the randomized phase II trial of the AIO (KRK 0209). J Clin Oncol. 2017; 35:4_suppl, 658-658.
15. Heinemann V, von Weikersthal LF, Decker T, Kiani A, Vehling-Kaiser U, Al-Batran SE, Heintges T, Lerchenmüller C, Kahl C, Seipelt G, Kullmann F, Stauch M, Scheithauer W, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014; 15:1065–75.
16. Schwartzberg LS, Rivera F, Karthaus M, Fasola G, Canon JL, Hecht JR, Yu H, Oliner KS, Go WY. PEAK: a randomized, multicenter phase II study of panitumumab plus modified fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab plus mFOLFOX6 in patients with previously untreated, unresectable, wild-type KRAS exon 2 metastatic colorectal cancer. J Clin Oncol. 2014; 32:2240–47.
17. Venook AP, Niedzwiecki D, Lenz HJ, Innocenti F, Mahoney MR, O’Neil BH, Shaw JE, Polite BN, Hochster HS, Atkins JN, Goldberg RM, Mayer RJ, Schilsky RL, et al. CALGB/SWOG 80405: phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC). J Clin Oncol. 2014; 32:15_suppl, LBA3-LBA3.
18. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, Aranda Aguilar E, Bardelli A, Benson A, Bodoky G, Ciardiello F, D’Hoore A, Diaz-Rubio E, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016; 27:1386–422.
19. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009; 339:b2535.