
INTRODUCTION
Chronic hepatitis B (CHB) is a major etiology of cirrhosis and hepatocellular carcinoma (HCC) worldwide, especially in China [1]. The risk factors for the development of cirrhosis in CHB patients have been identified as advanced age, male sex, hepatitis B virus (HBV) DNA load, and viral mutations [2-6]. During the last few decades, nonalcoholic fatty liver disease (NAFLD) has emerged as the most common chronic liver disease in the general population worldwide. The prevalence of NAFLD ranges from 6% to 33% among those with CHB [7]. NAFLD encompasses a spectrum of liver manifestations, ranging from simple hepatic steatosis (HS) to nonalcoholic steatohepatitis, fibrosis, and cirrhosis, which may ultimately progress to HCC. At present, the prevalence of HS in CHB patients reportedly ranges from 13% to 33% [8-10]. Accordingly, with the increasing incidence of NAFLD, the number of patients with concomitant CHB and NAFLD continues to increase rapidly. However, the progression and antiviral outcomes of patients with CHB and HS remain unclear [11, 12]. In this study, we aimed to characterize the effects of HS on the progression of CHB and antiviral response in a prospective cohort. As the limitation of the short time of follow-up and the small number of case, we also evaluated the effect of steatosis induced by oleic acid (OA) on the biological behavior of HCC cells in vitro.
RESULTS
Patient baseline characteristics
A total of 162 patients were enrolled in this study. The demographic, biochemical, virological, and histopathological features of CHB patients with and without HS at baseline are summarized in Table 1. Patients with HS were older (p = 0.034) and had higher BMI (p = 0.000) and higher serum cholesterol (p = 0.003). No significant differences in sex, HBV DNA level, inflammation grade or fibrosis stage were observed between the two groups at the baseline. During follow-up, 133 (82.1%) patients received antiviral treatment with IFN and/or NAs. The NAs included entecavir (ETV), adefovir (ADV), lamivudine (LAM) and telbivudine (LDT).
Table 1: Comparison of demographic, biochemical, virological and histopathological characteristics between CHB patients with and without HS
Steatosis (+) |
Steatosis (-) |
p-value* |
|
|---|---|---|---|
(n = 77) |
(n = 85) |
||
Age, years |
35.27 ± 9.43 |
32.12 ± 9.35 |
0.034 |
Sex, male, n |
59 |
60 |
0.385 |
female, n |
18 |
25 |
|
BMI, kg/m2 |
24.07 ± 2.23 |
22.63 ± 2.22 |
0.000 |
HBV DNA |
0.072 |
||
positive, n (%) |
51 (66.23%) |
67 (78.8%) |
|
negative, n (%) |
26 (33.77%) |
18 (21.2%) |
|
ALT, U/L |
91.84 ± 107.73 |
114.00 ± 91.93 |
0.538 |
AST,U/L |
52.26 ± 49.50 |
62.47 ± 58.53 |
0.232 |
GGT, IU/L |
54.75 ± 46.31 |
58.31 ± 68.08 |
0.093 |
ALP, IU/L |
89.73 ± 25.78 |
94.03 ± 37.58 |
0.665 |
Cholesterol,mmol/L |
4.40 ± 1.08 |
4.05 ± 0.77 |
0.003 |
Inflammation (G) |
|||
0 |
1 (1.30%) |
0 (0) |
0.152 |
1 |
33 (42.85%) |
28 (32.9%) |
|
2 |
29 (37.67%) |
37 (43.5%) |
|
3 |
12 (15.58%) |
19 (22.4%) |
|
4 |
2 (2.60%) |
1 (1.2%) |
|
Fibrosis (S) |
0.270 |
||
0 |
8 (10.39%) |
4 (4.71%) |
|
1 |
32 (41.56%) |
33 (38.82%) |
|
2 |
21 (27.27%) |
29 (34.12%) |
|
3 |
16 (20.78%) |
19 (22.35%) |
|
Hepatic steatosis |
|||
Mild |
59 (76.62%) |
ND |
|
Moderate |
16 (20.77%) |
ND |
|
Severe |
2 (2.61%) |
ND |
CHB, chronic hepatits B; HS, hepatic steatosis; BMI, body mass index; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; GGT, gamma-glutamyl transpeptidase
Noninvasive evaluation of liver fibrosis
In this cohort of 162 patients, cirrhosis developed in 8 (4.9%) patients during the follow-up period, including 4 (5.19%) patients with HS and 4(4.71%) without HS. No statistical difference was determined in the cumulative probability of progression to cirrhosis in patients with or without HS (p = 0.869; Figure 2A). Compared with their baseline, the APRI of both patients with HS and without HS had all decreased during the follow-up period (p< 0.05). However, the APRI of patients without HS decreased more than those with HS (p<0.05; Figure 3A).
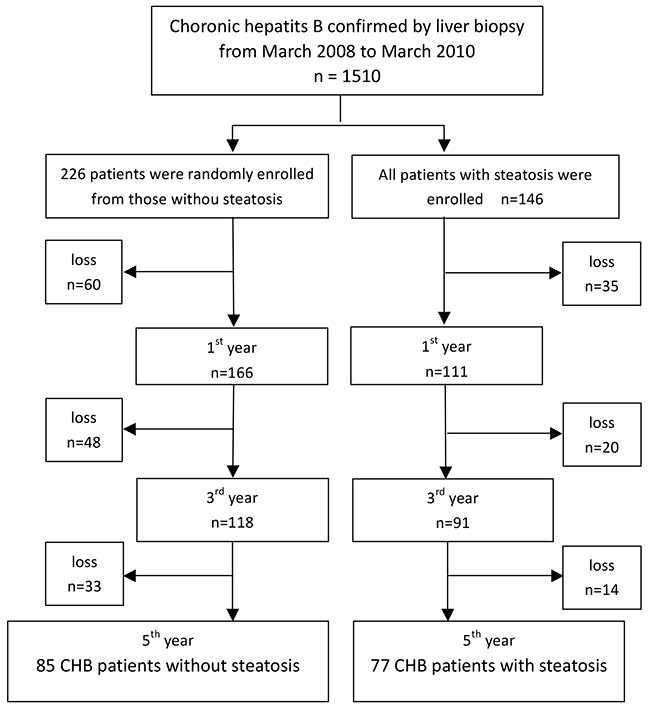
Figure 1: Flow chart of enrolment of chronic hepatitis B patients with or without steatosis.
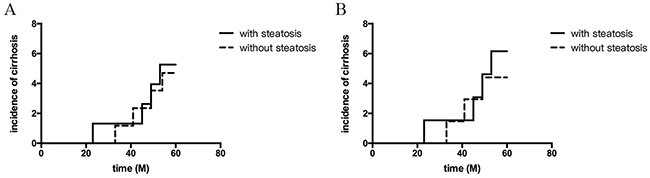
Figure 2: Cumulative probability of developing cirrhosis based on with or without hepatic steatosis. (A) All patients during the follow-up period (by Kaplan–Meier method; log-rank, P>0.05); (B) Patients who received antiviral therapy (by Kaplan–Meier method; log-rank, P>0.05).
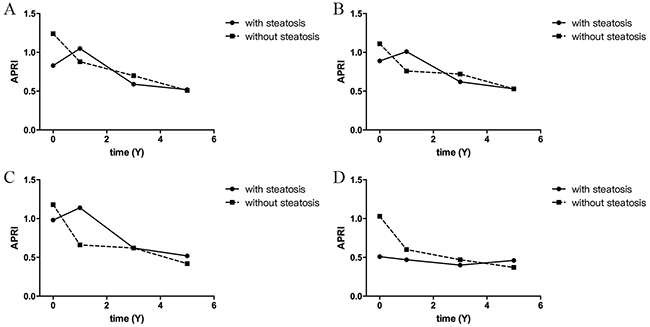
Figure 3: The trends of APRI during the follow-up period. (A) All patients during the follow-up period. The APRI of both patients with and without HS had decreased significantly when they were compared to the baseline (patients with HS: P= 0.344, 0.013, 0.0021 in 1,3,5-year, respectively; without HS: all P<0.001, in 1, 3, 5-year). The APRI of patients without HS had decreased more than that of those with HS (P<0.05, by repeated measures analysis of variance). (B) Patients who received antiviral therapy and (C) patients who achieved CVR. The APRI of both patients with and without HS had decreased when they were compared to the baseline(P<0.05). However, the difference between patients with HS and without was not significant (P>0.05, by repeated measures analysis of variance). (D) Patients without antiviral therapy. In patients without antiviral therapy, the APRI of both patients with and without HS had not changed significantly (P>0.05), and the difference between them was not significant (P>0.05 by repeated measures analysis of variance). (APRI: AST-to-PLT ratio index; CVR, complete virological response)
Evaluation of antiviral therapy outcome
A total of 104 patients achieved a complete virological response (CVR) and 29 patients failed to CVR or relapsed during the follow-up period. The presence of HS did not seem to affect the outcome of antiviral therapy (p = 0.942, Table 2). In patients who received antiviral therapy, the cumulative probability of progression to cirrhosis was not significant between patients with and without HS (p = 0.660, Figure 2B). In patients who received antiviral therapy, the APRI of both patients with HS and without HS had all decreased when compared to the baseline (p< 0.05), and no statistical difference was found between patients with or without HS (p>0.05, Figure 3B). Between patients with and without HS who achieved CVR, the decreased APRI was not significantly during the follow-up period (p>0.05, Figure 3C). In patients without antiviral therapy, the APRI of both patients with and without HS had not changed significantly (p>0.05, Figure 3D), and the difference between them was not significant (p>0.05).
Table 2: The response of antiviral therapy of CHB patients with or without HS
Treatment |
Steatosis (+) (n, %) |
Steatosis (-) (n, %) |
|---|---|---|
Without antiviral therapy |
12 (15.6%) |
17 (20%) |
Failed to respond or relapsed |
14 (18.2%) |
15 (17.6%) |
CVR |
51 (66.2%) |
53 (62.4%) |
IFN+NAs |
15 |
14 |
IFN |
5 |
4 |
ETV |
13 |
13 |
LdT |
2 |
5 |
LAM |
3 |
2 |
ADV |
9 |
7 |
NAs combination |
4 |
8 |
CVR,complete virological response; IFN, pegylated interferon; ETV, entecavir; ADV, adefovir; LAM, lamivudine; LdT, telbivudine; NAs, nucleotide/nucleoside analogues
Risk factor analysis
The multivariate analysis showed that patients who developed to cirrhosis were older (RR 1.07, 95% CI 0.996-1.149, p= 0.065) and had S3 stages of liver fibrosis (RR 3.50, 95% CI 0.812–15.117, p= 0.093). No significant effects of sex, BMI, HBV DNA level, HS, or higher grade of inflammation development on progression to cirrhosis were also observed by univariate analysis (Table 3).
Table 3: Univariate analysis of risk factors for the progression to cirrhosis
Factor |
Cirrhosis (+) |
Cirrhosis (-) |
p-value |
(n = 8) |
(n = 154) |
||
|---|---|---|---|
Age |
40.13±12.32 |
32.25±9.23 |
0.045 |
Males/females, n (%) |
5/3 (62.5%) |
115/39 (74.67) |
0.436 |
BMI |
22.99±1.34 |
23.33±2.38 |
0.688 |
Family history of HBV (yes/no) |
2/6 |
63/91 |
0.585 |
Drinking history (yes/no) |
2/6 |
18/136 |
0.567 |
HBV DNA level (>105/≤105) |
5/3 |
102/52 |
1.000 |
HS (+/-) |
4/4 |
73/81 |
1.00 |
Inflammation, n (%) |
0.219 |
||
G0 |
0 |
1(0.6%) |
|
G1 |
1(12.5%) |
60(39.0%) |
|
G2 |
5(62.5%) |
61(39.6%) |
|
G3 |
2(25%) |
29(18.8%) |
|
G4 |
0(0) |
3(2.0%) |
|
Fibrosis, n (%) |
|||
S0 |
0 |
12 (7.8%) |
0.006 |
S1 |
0 |
65 (42.2%) |
|
S2 |
4 (50%) |
46 (29.9%) |
|
S3 |
4 (50%) |
31 (20.1%) |
BMI, body mass index; HBV DNA, hepatitis B virus deoxyribonucleic acid
OA promotes cell proliferation and migration
The HCC cells steatosis model was successfully established using OA (Figure 4A). The CCK-8 assay showed that proliferation of HepG2 cell was promoted significantly after 24 h at a final concentration of 300 μM (Figure 4B). The scratch assay showed that the migration of four kinds of HCC cells were promoted by OA, but yet reaching significant levels (Figure 4C-4D). Flow cytometer analyses found that cell cycle analyses showed that the S phase was higher in the cells exposed to OA than those without treatment (Figure 4E-4F). The experiments were repeated for three times.
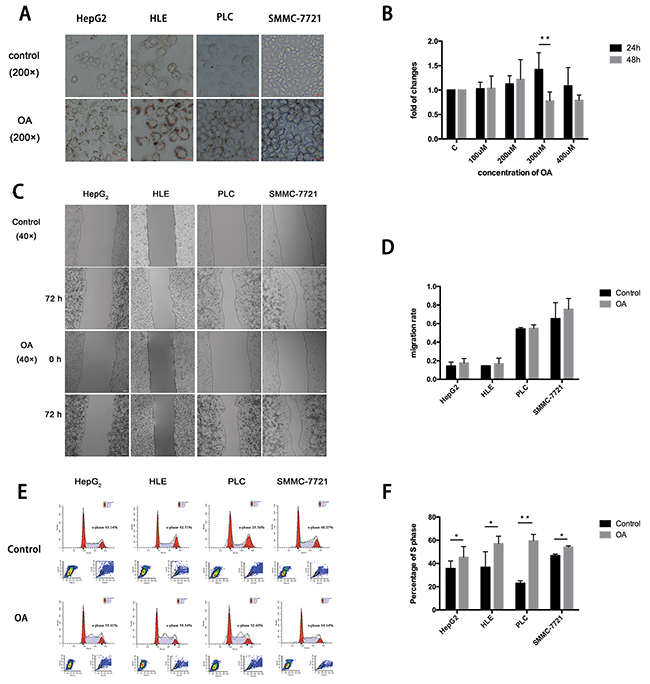
Figure 4: OA promotes HCC cells proliferation, migration. (A) Oil red O staining shows lipid accumulation in HepG2, HLE, PLC and SMMC-7721 cells. (B) CCK-8 assay shows OA promotes the proliferation of HepG2 cell at a final concentration of 300 μM for 24 h. (C) Scratch assay of HCC cells. (D) Statistics of migration rate. (D-E) Flow cytometer analyses shows S phase of cells treated with OA was higher. Each test was repeated in three times (n=3). *P < 0.05 and **P < 0.01. Scale bars: 10 μm (A); 100 μm (C).
DISCUSSION
With the increasing incidence of NAFLD, the existence of concomitant hepatitis B and fatty liver is becoming more common in clinical practice. A study of the prognosis, treatment outcomes, and possible underlying mechanisms by Zheng et al reported that BMI, waist-to-hip ratio, fasting blood glucose, serum triglyceride levels, and serum total cholesterol appeared to be influencing factors of CHB combined with HS. HS in CHB patients was reported to be closely related to changes in anthropometric indices and metabolic factors, but not HBV [13]. It has been widely recognized that the presence of HS accelerates progression of fibrosis in patients with chronic hepatitis C infection [14]. Nevertheless, whether HS is associated with the severity of fibrosis in CHB patients remains to be determined. A study of 5406 patients conducted in Taiwan found that fatty liver with HBV infection has a significant synergistic association with liver damage [15]. In the present study, however, hepatic steatosis had no significant impact on the development of cirrhosis in CHB patients. Our study has the strength of liver biopsy of all patients, which increased the accuracy of fibrosis at baseline. Liver biopsy is the current gold standard to assess hepatic inflammation and fibrosis in patients with CHB. However, it is difficult to repeat liver biopsy over a relatively short follow-up period; therefore, noninvasive markers of liver fibrosis are typically used in clinical practice. In this study, noninvasive marker, APRI, was applied to assess the degree of liver fibrosis. It has been reported that the annual incidence of cirrhosis in CHB patients is 0.7%–2.4%[16-18]. In this study, the cumulative probability of developing cirrhosis was not significant between patients with and without HS, thus HS was not an independent prognostic factor of disease progression by univariate analysis. The rate of progression to cirrhosis during the follow-up period was lower than previous reports because most patients with mild fibrosis are enrolled in this study. This result is likely explained by the small number of cases and the fluctuation of HBV DNA levels during the followed-up period.
The presence of HS is a common finding in CHB infection. However, it remains controversial whether HS influences the efficacy of antiviral therapy. A study carried out by Cindoruk et al. [19] showed that HS was not associated with viral load or treatment outcome in 140 patients with CHB infection. Ben et al. [20] also showed that HS does not seem to influence the progression of liver fibrosis or therapeutic response. However, Shi et al. [21] reported that treatment with polyethylene glycol IFN for 48 weeks had no influence on the virological response of CHB patients with HS, but did alter the biochemical response. Another study by Jin et al. [22] found that HS was significantly associated with failure of ETV treatment. The present study revealed that the HS did not seem to affect the outcome of antiviral therapy. However, the role of HS should be further investigated in prospective longitudinal clinical studies with larger patient populations.
The following features were found to be significant prognostic factors in CHB: the presence of bridging fibrosis, older age, persistence of HBV in serum, HBeAg carrier status, and HBV reactivation. In this study, univariate analysis showed that age and liver fibrosis stage, but not the presence of HS and HBV DNA level, were prognostic factors for the development of cirrhosis. Compared with their baseline, meanwhile, the APRI of both patients with HS and without HS had all decreased after antiviral therapy during the follow-up period. Therefore, the antiviral therapy may also delay the progress of liver fibrosis and cirrhosis.
There are some limitations in our study. One of the limitations is small sample size of patients in this longitudinal cohort despite a follow-up duration of 5 years. In order to address the shortcomings, in vitro cell culture model was used in research of NAFLD with CHB. Recently, OA-induced lipid accumulation in HepG2 cells may act as an in vitro model for studying NAFLD [23]. In this study, the HCC cells steatosis model was successfully established using OA. The biological behavior, proliferation and migration of HCC cells, were promoted in vitro. These results suggested that hepatic steatosis may aggravate liver disease, including the progression of cirrhosis and HCC.
MATERIALS AND METHODS
Patients
A total of 1510 CHB patients were confirmed by liver biopsy from March 2008 to March 2010 in Beijing You’an Hospital. Of these, 162 patients were prospectively followed-up for more than 5 years. According to the results of liver biopsy, the patients were divided into two groups: CHB without HS (n = 85) and CHB with HS (n = 77) (Figure 1). The inclusion criteria were (1) age of 18–65 years, (2) HBsAg positive for more than 6 months without antiviral therapy (3), liver biopsy conducted within 3 months before enrollment, and (4) informed consent was signed to participate in this study. The exclusion criteria of this cohort were: (1) evidence of alcohol addiction (defined as alcohol intake of ≥40g/day for men and ≥20g/day for women for a 5-year period, or alcohol intake of ≥0.80 g/day within 2 weeks); (2) coexisting infection with human immunodeficiency virus (HIV), hepatitis C virus, or other virus-related hepatitis; (3) poorly controlled diabetes (fasting glucose level of > 220 mg/dL); (4) heart failure with grade of III or IV, and (5) definite diagnosis of liver cirrhosis, HCC, or autoimmune or inherited metabolic liver disease. The study protocol was approved by the Beijing You’an Hospital Institutional Review Board and conducted in compliance with the Declaration of Helsinki. The informed consent was obtained from each patient.
Clinical and laboratory data
The symptoms, signs, and components of metabolic syndrome (height, weight, and body mass index, BMI) were retrieved from medical records. A microparticle enzyme immunoassay was used to test for serum markers of hepatitis B (F. Hoffmann-La Roche AG, Basel, Switzerland). HBVDNA levels were measured using the COBAS® AmpliPrep/COBAS® TaqMan® quantitative measurement system (Roche Diagnostics Deutschland GmbH) that has a lower limit of serum HBVDNA detection of 20 IU/mL. Serum markers of human immunodeficiency virus were detected using an electrochemiluminescence immunoassay (Cobas 6000; Roche Diagnostics Deutschland GmbH). Liver function, such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), renal function and serum lipids, were measured with an automatic biochemical analyzer (AU5400; Olympus Corporation, Tokyo, Japan). Blood parameters, including white blood cell (WBC) and platelet (PLT) counts, were measured using an automatic biochemical analyzer (XT-4000i; Sysmex Corporation, Kobe, Japan).
Liver biopsy
Each patient was tested for platelet counts, bleeding time, clotting time, and prothrombin activity before undergoing liver biopsy. Liver biopsy was performed under ultrasound guidance with a disposable 18G biopsy gun and liver puncture needle. Liver tissue sample was conventionally formalin-fixed, paraffin-embedded, and sectioned into thicknesses of 4μm. Histological grading of inflammation (G0–G4) and staging of the liver fibrosis (S0–S4) were carried out according to Metavir classification criteria by a pathologist who was blinded to the clinical data. The degree of fibrosis was staged from 0 to IV (0, no fibrosis; I, mild; II, moderate; III, severe; IV, cirrhosis). In the classification of steatosis, less than 5% was considered normal, 6-33% as mild, 34-66% as moderate, greater than 67% as severe fat deposition [24].
Definition of liver cirrhosis
Cirrhosis was defined as (1) histological conformation, (2) overt cirrhotic findings by ultrasonography or endoscopy, or (3) blood PLT level <100 × 109/L and fibroscan >12.5KPa or AST-to-platelet ratio index (APRI) >2.
APRI for noninvasive evaluation of liver fibrosis
APRI= (AST/ULN*) × 100/PLT [25]
Units: AST(U/L), PLT (109/L), *ULN, upper limit of normal
APRI values of 0.50 or less was defined as no liver fibrosis. While APRI values of 2.00 or more was defined as liver cirrhosis [26].
Definitions of antiviral response
Antiviral failure was defined as detection of resistance-associated mutation or occurrence of HBV DNA rebound (HBV DNA was detective in two consecutive tests following negative testing results) during nucleotide/nucleoside analogues (NAs) and/or pegylated interferon (IFN) therapy. Complete virological response (CVR) was defined as undetectable serum HBV DNA (lower limit of detection = 20 IU/mL) during the period of antiviral therapy.
Follow-up and end-points
All patients had been prospectively followed-up for more than 5 years at outpatients or inpatients department. The end-point of follow-up was a diagnosis of cirrhosis or liver cancer, or death. The APRI as noninvasive markers was dynamically used to assess liver fibrosis progression.
In vitro study
As the limitation of the short time of follow-up and the small number of case, we also evaluated the effect of steatosis induced using OA on the biological behavior of HCC cells. Human HCC cell lines (HepG2, HLE, PLC, and SMMC-7721) were kindly provided by professor DX Chen of Beijing Institute of Hepatology. HepG2, HLE, and PLC cells were cultured in Dulbecco’s modified Eagle’s medium (DMEM, Thermo Fisher Scientific, USA) supplemented with 10% fetal bovine serum (FBS, Sijiqing, China). SMMC-7721 cells were cultured in Roswell Park Memorial Institute (RPMI) 1640 (Thermo Fisher Scientific, USA) with 10% FBS. Four kinds of HCC cells were subcultured with 5 x 105 cells/well at the 37 ºC, 5% CO2 incubator. After 24 h incubation, the culture medium was removed and cells was fixed using 4% paraformaldehyde. Then, the cells were stained using oil red O (Sigma, diluted in double-distilled H2O 3:2) for 30 min at room temperature Lipid droplet accumulation was detected using microscopy.
Cell Counting Kit-8 (CCK-8, Dojindo Laboratories, Kumamoto, Japan) was used to assess cell proliferation. HepG2 cells were taken into 96-well plates with 5000 cells in each well. Different concentrations of OA were added into each well following 24 h or 48 h incubation. The absorbencies were measured at a wave length of 450 nm on a Universal Microplate Reader (EL x800). Cell proliferation was calculated in term of the formula: cell proliferation%= [(A570 or 450sample-background)/ (A570 or 450 control-background)] ×100%. HCC cells migration was assessed using scratch assay. Four kinds of HCC cell lines were pipetted into 6-well microplates with 5 x 105 cells in each well. After completely attachment, the cells were treated using different concentrations of OA. A scratch wound was made across the diameter of each plate using a sterile 10-µl pipette tip. Then, the cells were observed under microscopy at 0, 12, 24, 48, and 72h following treatment. Each test was repeated in three times.
Four kinds of HCC cell lines were cultured in serum-free medium for 24 h before treatment to arrest the cell cycle. Then, the serum-free medium was replaced by fresh DMEM containing 10% FBS. After treated with OA at a final concentration of 300 μM for 24h, the cells were stained by PI at a final concentration of 50 mg/L. DNA content was analyzed with a FACScan-420 flow cytometer (Becton-Dickinso, Germany). The distribution of cells in different cell cycle stages was determined according to the DNA content. Each test was repeated in three times.
Statistical analysis
All statistical tests were performed using SPSS statistical software (version 17.0; IBM-SPSS, Inc., Chicago, IL, USA). Continuous variables are presented as means ± standard deviations and compared using the unpaired t-test and repeated measures analysis of variance, as appropriate. Categorical variables were compared using the chi-squared test. Progression analysis was performed using Kaplan–Meier survival curves and the log-rank test. Multivariate analysis was performed using logistic regression models. A two-sided probability (p) value of < 0.05 was considered statistically significant.
Abbreviations
oleic acid (OA); hepatocellular carcinoma (HCC); aspartate aminotransferase (AST); AST-to-platelet ratio index (APRI); chronic hepatitis B (CHB); nonalcoholic fatty liver disease (NAFLD); hepatic steatosis (HS); nonalcoholic steatohepatitis (NASH); Body mass index (BMI); nucleotide/nucleoside analogues (NAs); hepatitis B virus deoxyribonucleic acid (HBV DNA); Cell Counting Kit-8 (CCK-8); entecavir (ETV); adefovir (ADV); lamivudine (LAM); telbivudine (LDT); Complete virological response (CVR); hepatitis B e antigen (HBeAg); white blood cell (WBC).
Author contributions
Yangqin Chen and Chunlei Fan equally contributed to the data collection, analysis and the cell experiments. Yuhan Chen, Peiling Dong and Lei Li did patients care and follow-up. Hui Liu did histological examination. Shanshan Wang did parts of the cell experiments. Dr. Huiguo Ding was responsible for this project and wrote the final manuscript
ACKNOWLEDGMENTS
This study was supported by grants from the Capital Science and Technology Development Fund (grant no. 2014-1-2181), Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding (grant no. ZYLX201610), Beijing Municipal Administration of Hospitals’Ascent Plan (grant no. DFL20151602) and National Science Fund (grant no. 81672725, 81401970.
CONFLICTS OF INTEREST
The authors declare no conflicts of interests.
REFERENCES
1. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009; 49: S45-55. doi: 10.1002/hep.22898.
2. Zhang X, Ding HG. Key role of hepatitis B virus mutation in chronic hepatitis B development to hepatocellular carcinoma. World J Hepatol. 2015; 7: 1282-6. doi: 10.4254/wjh.v7.i9.1282.
3. Hu HH, Liu J, Lin YL, Luo WS, Chu YJ, Chang CL, Jen CL, Lee MH, Lu SN, Wang LY, You SL, Yang HI, Chen CJ. The rs2296651 (S267F) variant on NTCP (SLC10A1) is inversely associated with chronic hepatitis B and progression to cirrhosis and hepatocellular carcinoma in patients with chronic hepatitis B. Gut. 2015; 65: 1514-21. doi: 10.1136/gutjnl-2015-310686.
4. Shimakawa Y, Yan HJ, Tsuchiya N, Bottomley C, Hall AJ. Association of early age at establishment of chronic hepatitis B infection with persistent viral replication, liver cirrhosis and hepatocellular carcinoma: a systematic review. PLoS One. 2013; 8: e69430. doi: 10.1371/journal.pone.0069430.
5. Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol. 2008; 48: 335-52. doi: 10.1016/j.jhep.2007.11.011.
6. Iloeje UH, Yang HI, Chen CJ. Natural history of chronic hepatitis B: what exactly has REVEAL revealed? Liver Int. 2012; 32: 1333-41. doi: 10.1111/j.1478-3231.2012.02805.x.
7. Demir M, Lang S, Steffen HM. Nonalcoholic fatty liver disease: Current status and future directions. J Dig Dis. 2015; 16: 541-57. doi: 10.1111/1751-2980.12291.
8. Wong VW, Wong GL, Chu WC, Chim AM, Ong A, Yeung DK, Yiu KK, Chu SH, Chan HY, Woo J, Chan FK, Chan HL. Hepatitis B virus infection and fatty liver in the general population. J Hepatol. 2012; 56: 533-40. doi: 10.1016/j.jhep.2011.09.013.
9. Wang MM, Wang GS, Shen F, Chen GY, Pan Q, Fan JG. Hepatic steatosis is highly prevalent in hepatitis B patients and negatively associated with virological factors. Dig Dis Sci. 2014; 59: 2571-9. doi: 10.1007/s10620-014-3180-9.
10. Pais R, Rusu E, Zilisteanu D, Circiumaru A, Micu L, Voiculescu M, Poynard T, Ratziu V. Prevalence of steatosis and insulin resistance in patients with chronic hepatitis B compared with chronic hepatitis C and non-alcoholic fatty liver disease. Eur J Intern Med. 2015; 26: 30-6. doi: 10.1016/j.ejim.2014.12.001.
11. Wang CC, Tseng TC, Kao JH. Hepatitis B virus infection and metabolic syndrome: fact or fiction? J Gastroenterol Hepatol. 2015; 30: 14-20. doi: 10.1111/jgh.12700.
12. Lin CW, Huang XL, Liu HL, Wang Y. Interactions of Hepatitis B Virus Infection with Nonalcoholic Fatty Liver Disease: Possible Mechanisms and Clinical Impact. Dig Dis Sci. 2015; 60: 3513-24. doi: 10.1007/s10620-015-3772-z.
13. Zheng RD, Chen JN, Zhuang QY, Lu YH, Chen J, Chen BF. Clinical and virological characteristics of chronic hepatitis B patients with hepatic steatosis. Int J Med Sci. 2013; 10: 641-6. doi: 10.7150/ijms.5649.
14. Westin J, Nordlinder H, Lagging M, Norkrans G, Wejstal R. Steatosis accelerates fibrosis development over time in hepatitis C virus genotype 3 infected patients. J Hepatol. 2002; 37: 837-42. doi: 10.1016/S0168-8278(02)00299-4.
15. Lin YC, Hsiao ST, Chen JD. Sonographic fatty liver and hepatitis B virus carrier status: synergistic effect on liver damage in Taiwanese adults. World J Gastroenterol. 2007; 13: 1805-10. doi: 10.3748/wjg.v13.i12.1805.
16. Liaw YF, Tai DI, Chu CM, Chen TJ. The development of cirrhosis in patients with chronic type B hepatitis: a prospective study. Hepatology. 1988; 8: 493-6. doi: 10.1002/hep.1840080310.
17. Huo T, Wu JC, Hwang SJ, Lai CR, Lee PC, Tsay SH, Chang FY, Lee SD. Factors predictive of liver cirrhosis in patients with chronic hepatitis B: a multivariate analysis in a longitudinal study. Eur J Gastroenterol Hepatol. 2000; 12: 687-93.
18. Yu MW, Hsu FC, Sheen IS, Chu CM, Lin DY, Chen CJ, Liaw YF. Prospective study of hepatocellular carcinoma and liver cirrhosis in asymptomatic chronic hepatitis B virus carriers. Am J Epidemiol. 1997; 145: 1039-47.
19. Cindoruk M, Karakan T, Unal S. Hepatic steatosis has no impact on the outcome of treatment in patients with chronic hepatitis B infection. J Clin Gastroenterol. 2007; 41: 513-7. doi: 10.1097/01.mcg.0000225586.78330.60
20. Ben Slama Trabelsi A, Ksiaa M, Souguir A, Issaoui D, Sriha B, Ajmi S. Hepatic steatosis in chronic hepatitis B: prevalence, risk factors, and impact on fibrosis and therapeutic response. Tunis Med. 2013; 91: 431-4.
21. Shi JP, Lu L, Qian JC, Ang J, Xun YH, Guo JC, Shi WL, Wang YF, Fan JG. Impact of liver steatosis on antiviral effects of pegylated interferon-alpha in patients with chronic hepatitis B. [Article in Chinese] Zhonghua Gan Zang Bing Za Zhi. 2012; 20: 285-8. doi: 10.3760/cma.j.issn.1007-3418.
22. Jin X, Chen YP, Yang YD, Li YM, Zheng L, Xu CQ. Association between hepatic steatosis and entecavir treatment failure in Chinese patients with chronic hepatitis B. PLoS One. 2012; 7: e34198. doi: 10.1371/journal.pone.0034198.
23. Alkhatatbeh MJ, Lincz LF, Thorne RF. Low simvastatin concentrations reduce oleic acid-induced steatosis in HepG2 cells: An in vitro model of non-alcoholic fatty liver disease. Exp Ther Med. 2016; 11: 1487-92. doi: 10.3892/etm.2016.3069.
24. Brunt EM, Tiniakos DG. Pathology of steatohepatitis. Best Pract Res Clin Gastroenterol. 2002; 16: 691-707. doi: 10.1053/bega.2002.0326.
25. Sterling RK, Lissen E, Clumeck N, Sola R, Correa MC, Montaner J, M SS, Torriani FJ, Dieterich DT, Thomas DL, Messinger D, Nelson M. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006; 43: 1317-25. doi: 10.1002/hep.21178.
26. Chrysanthos NV, Papatheodoridis GV, Savvas S, Kafiri G, Petraki K, Manesis EK, Archimandritis AJ. Aspartate aminotransferase to platelet ratio index for fibrosis evaluation in chronic viral hepatitis. Eur J Gastroenterol Hepatol. 2006; 18: 389-96.